Diagnosing Tuberculosis Old and new tools Anne Detjen, The Union.
56
Diagnosing Tuberculosis Old and new tools Anne Detjen, The Union
-
date post
22-Dec-2015 -
Category
Documents
-
view
213 -
download
0
Transcript of Diagnosing Tuberculosis Old and new tools Anne Detjen, The Union.
Diagnosing TuberculosisOld and new tools
Anne Detjen, The Union

MicroscopyAcid-fast bacilli (AFB)
Ziehl andNeelsen (1892)
Tuberculin-Skin TestRobert Koch 1890 (Tuberculin)
Mendel (1909), Mantoux (1910)
Diagnosis of active TBDiagnosis of M. tuberculosis
infection (LTBI)
Over 100 years ago….

Microscopy remains the frontline tool for diagnosing active TB
But
New and exciting developments
Today

Microscopy
o Certain amount of bacilli needed for visibility
Diagnostic delay
Morbidity
Transmission
Sputum smear microscopy
Advantages
o Can be used at district levelo Simple and inexpensiveo Rapid detection of
infectious cases
o Smear positivity = Basis for recording and reporting of TB cases
Disadvantages
o Diagnostic delay: 5000-10,000 bacilli/ml
o Sensitivity 60-70% in HIV-uninfected adults
o Suboptimal in o HIV-infectedo Children 20%o Extrapulmonary TB (EPTB)
o Cannot distinguisho M. tuberculosis versus NTMo Dead or live M. tuberculosiso Drug-sensitive or resistant
Microscopy
o Sensitivity = correctly identified ‘sick’ peoplenumber of true positives
number of true positives plus number of false negatives
o Specificity = correctly identified healthy people
number of true negativesnumber of true negatives plus number of false positives
Measures of diagnostic accuracy

o Symptomso Chest radiography (or other imaging)o Immune response to M. tuberculosis
o Tuberculin Skin Testo Interferon-gamma Release Assayso Antibody tests
o Bacteriologic confirmation = gold standardand Drug susceptibility testing (DST) o Smear microscopyo Cultureo Nucleic acid amplicfication tests (NAATs)
What else?Approaches to diagnose TB
o Non-remitting cougho Night sweats o Fevero Fatigueo Organ-specific symptoms
Symptoms

Advantages
o Cheapo Can be done anywhere
Disadvantages
o Unspecifico No diagnosis
BUT: index of suspicion
Symptoms
o Unspecifico Certain characteristic features
o Cavitieso Lymph node enlargement in childrenoMiliary tuberculosis
o Remains pillar in diagnosis of TB in children
Chest radiography ~1910

Advantages
o Diagnosis of extent of disease and complications
Disadvantages
o Unspecifico Often difficult to accesso Equipment and personnelo Training in interpretation
Chest radiography

= Indirect assaysDetection of the host response to M. tuberculosis
o Cannot differentiate between active TB and M. tuberculosis infection (LTBI)
Immune-based Tests - Concept
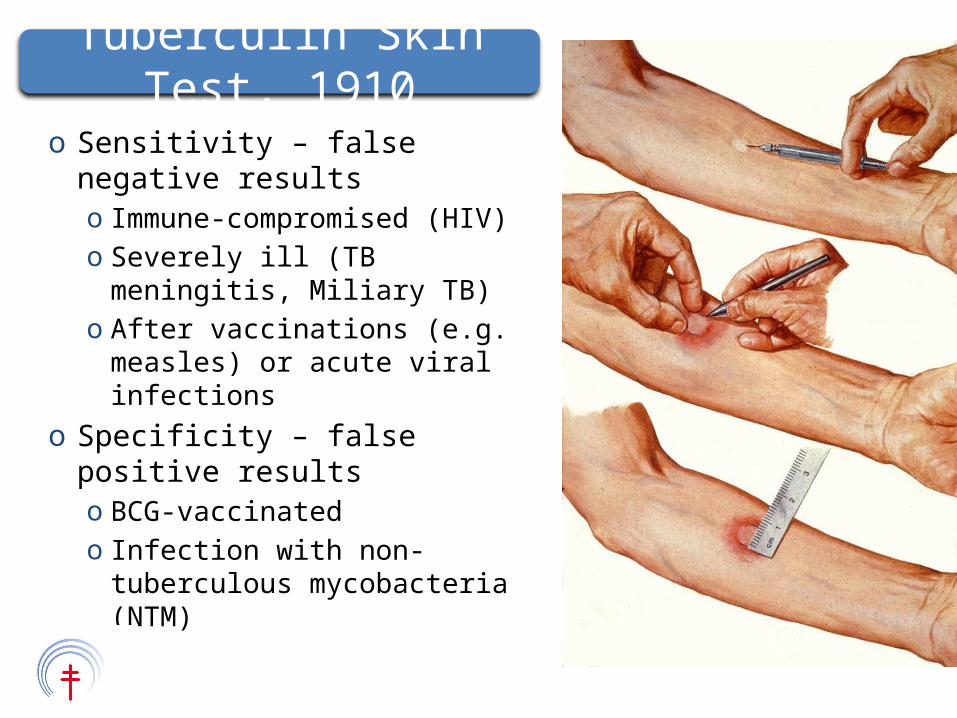
o Sensitivity – false negative resultso Immune-compromised (HIV)o Severely ill (TB meningitis,
Miliary TB)o After vaccinations (e.g. measles)
or acute viral infectionso Specificity – false positive results
o BCG-vaccinatedo Infection with non-tuberculous
mycobacteria (NTM)
Tuberculin Skin Test, 1910
Advantages
o Basic test for M. tuberculosis infection
o Used for contact tracingo Risk assessment for active
TB
Disadvantages
o Not widely availableo Feasibility: Return visit
necessaryo Cross-reactivity
Tuberculin Skin Test
o Developed for detection of LTBIo Sensitized T-cells produce interferon-gamma after
stimulation with TB-specific antigenso Interferon-gamma/Interferon-gamma producing cells can be
measuredo Sensitivity similar to TST (70-90%)
o Increased in HIV-infected?o Children?
o Specificity superior to TST (>95%)o No cross-reactivity with BCG or
common NTM
Interferon-gamma Release Assays (IGRAs)
Advantages
o HIC: Superiority over TST (?)o LMIC: Value in HIV-infected,
children?
Recommended in many high income countries for detection of LTBI
Disadvantages
o Costo HR and lab requirementso No value for detection of
active TBWHO 25 October 2010:
Negative policy recommendation for low and middle income countries 2010
T SPOT TM.TB QuantiFERON®-Tb Gold In-Tube
Interferon-gamma Release Assays (IGRAs)

o Would be ideal point of care test (similar to HIV rapid test)
o Current commercial versions have suboptimal accuracy(and are yet widely used e.g. India)
First negative policy recommendation WHO 2011
Antibody Detection Tests

o Solid mediao Egg-based (Löwenstein-Jensen),
Agar-based (Middlebrook)o Time to detection: 3-4 weeks
o Liquid media (WHO 2007) o E.g. Bactec 460 (radiolabelled CO2) or Mycobacterial growth
indicator tube (MGIT) 960 (fluorescent indicator)o Time to detection: 10-14 dayso Yield +10% over solid mediao More prone to contamination
o Strain specification needed (Phenotypic, Genotypic)
Bacteriologic confirmation - Culture methods
o ‘Conventional’ = Culture of M. tuberculosis in the presence of anti-TB drugs to detect growth (resistant) or inhibition of growth (susceptible)o Direct DST = from specimeno indirect DST = from positive culture
= gold standard
Drug Sensitivity Testing
Advantages
o Gold standardo Increases case-finding (30-
50%)o Earlier detection than
microscopy (10-100 bacteria/ml)
Disadvantages
o Time (incl. DST)o Costo Lab and HR requirementso Biosafety requirementso Trainingo Maintenance of equipment
Bacteriologic confirmation
o Microscopy ~ 90 Million patient examinations/year (6% in high income countries)
o 50 Million chest radiographies (2/3 in Asia)o Culture:
o 17 Million cultures, 1/3 in HICo Of cultures performed in 22 high burden countries: 75%
are done in Brazil, Russian Federationo South Africa: > 90% of cultures on African continento 2.5% of incident TB cases in Asian and African HBC
receive DST
Use of current TB diagnostics

o Existing diagnostic tools are suboptimalo Accuracy (microscopy)
oHIV-infectedoChildren
o Time to diagnosis = Transmission o Feasibility in settings with limited resources
o FinancialoHumano Infrastructure
New diagnostics are urgently needed
Conclusion

NDWG 2009
Pathway for the development of new diagnostics

o Case detectiono Diagnosis of drug resistanceo Treatment follow-upo Diagnosis of latent TB infection
Development of new tools – What will a new test be used for?

Reference Laboratory
Regional/Referral Laboratory
Microscopy Laboratory
Health clinicSoph
istic
ation
of d
iagn
ostic
Patient accessWhere in the health system?
o Depends on the epidemiologic setting and health system contexto Add-on or replacement?
Each of these indications has different needs for a test – no ‘one-fits all’ solution
Desirable: o High accuracy in all patient groups
(smear positive, smear negative, HIV-infected, children, EPTB)o Easy to perform
o Little training, user-friendlyo Biosafety
o Close to the patient – point of care
Needs assessment

The diagnostic pipeline
o Fluorescent microscopyo 10% increased yieldo Recommended for intermediate level laboratories
(100+ smears)o Light-emitting diode (LED) fluorescence
microscopyo Accuracy comparable to conventional fluorescenceo Less power, can run on batteries, bulbs long half lifeo Alternative to conventional microscopy at high- and
low-volume laboratories
Improved microscopy
LAM = Lipoarrabinomannano Cell wall component of M. tuberculosiso Promising marker of active TB, found in urineo Potential for simple, non-invasive and safe
point-of care test?o Commercial assay available
Point of care diagnostic within reach?Urinary LAM Antigen detection
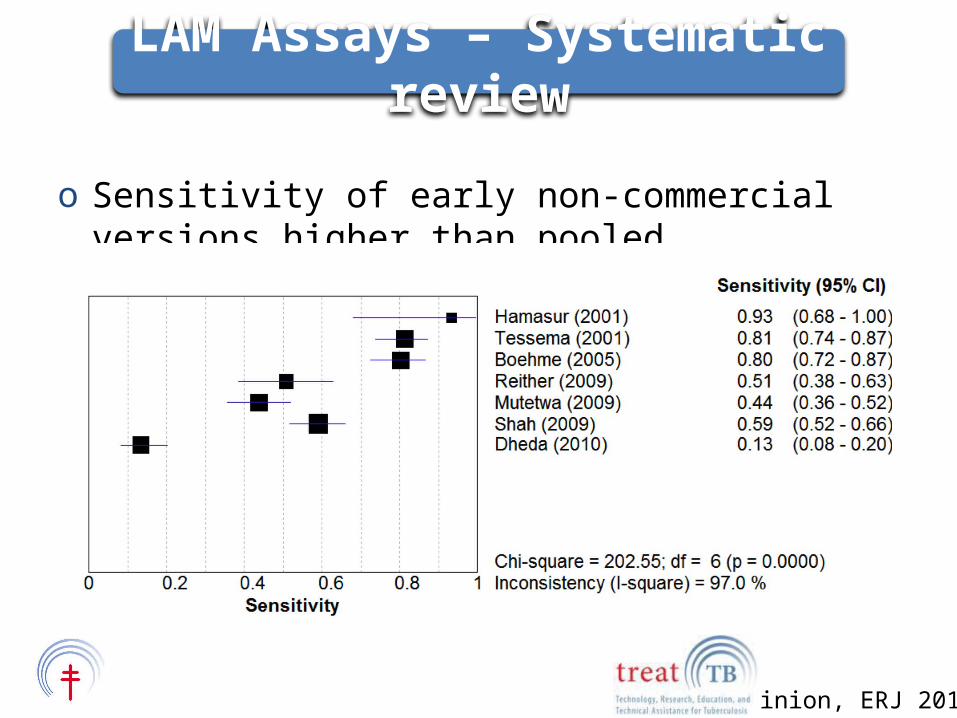
Minion, ERJ 2011
o Sensitivity of early non-commercial versions higher than pooled sensitivity of commercial versions
LAM Assays – Systematic review
o Microscopic Observation Drug Susceptibility (MODS)
o Using liquid mediumo Non-commercial, manual culture methodo Detection of
oM. tuberculosiso INH and RIF resistance
o Time to detection 7-14 days
www.modsperu.org
Simplified culture methods
o Simpleo Less expensiveo Modest training
requirementso Combines detection of
M. tuberculosis and DST
o Not standardizedo Local variations in
methodologyo Quality assuranceo Biosafety
WHO 2011: Recommended for MDR suspects as interim alternative
MODS
o Genotypic detection of M. tuberculosiso Allows for screening of common resistance-
causing mutationso Various commercial and
non-commercial NAATs have beenaround for >15 yearso Excellent specificityo Clinical sensitivity depends on bacterial
concentration: 50-80% in smearnegative
Nucleic Acid Amplification Tests (NAAT)

o Manual NAATo Detection of
oM. tuberculosiso INH and RIF resistance
o based on DNA strip technology. Three steps: DNA extraction, PCR and reverse hybridization
Recommended for detection of MDR TB on smear+ samples
Line Probe Assays (WHO 2008)

Advantages
o Results within hourso Fast detection of INH, RIF
resistanceo Excellent sensitivity and
specificity compared to conventional culture
Disadvantages
o Biosafety level 2 or 3o Limited use in
o HIV-infectedo Childreno (on positive cultures)
o Conventional culture (and DST) still needed for smear negative
Line Probe Assays
o Real-time PCR assayo Fully automated: No prior specimen processing
and DNA extraction neededo Detects M. tuberculosis and RIF resistanceo Highly accurate in smear + (99%) and smear -
(>80%) as well as HIV-infectedo Sensitivity for RIF resistance 95.1%, Specificity
98.4%o Results within 2 hours
Xpert MTB/RIF (WHO 2010)
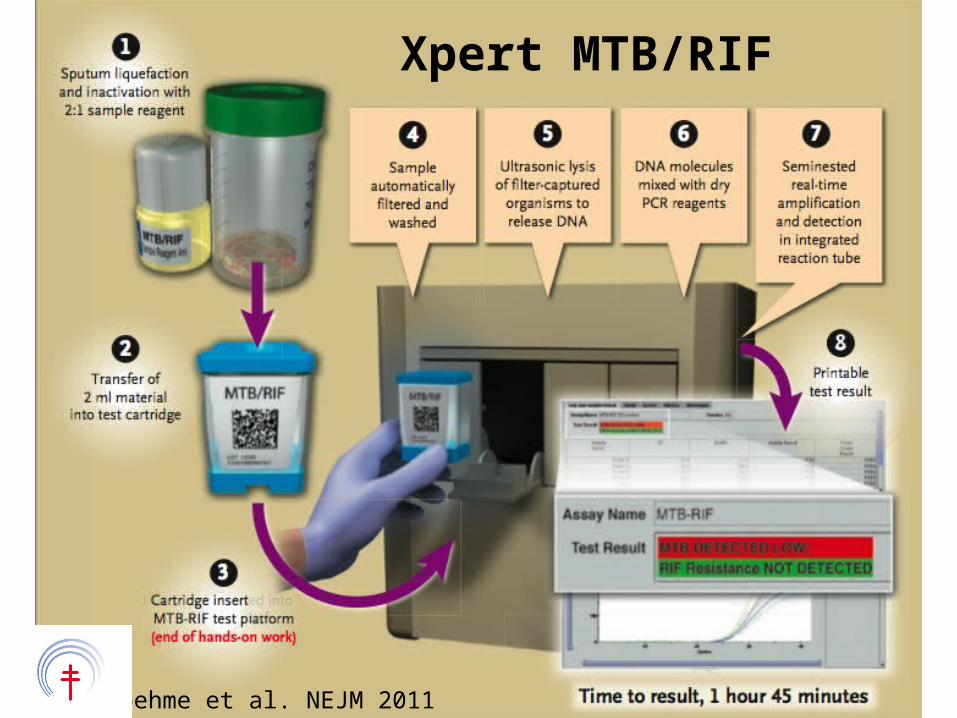
Xpert MTB/RIF
Boehme et al. NEJM 2011

Potential for point of care test?• Cost• Electric supply
WHO policy statement:• Xpert MTB/RIF as initial diagnostic test in MDR suspects
or HIV-infected TB suspects• Follow-on test to microscopy in MDR or HIV low-burden
settings, further testing of smear negative samples District, Sub-district Level
Xpert MTB/RIF
• Exciting development in the area of new diagnostics
• Challenges:– Cost– Adoption at country level– Implementation and scale up
Still not optimal for– Vulnerable populations: Children– Extrapulmonary TB
Conclusions
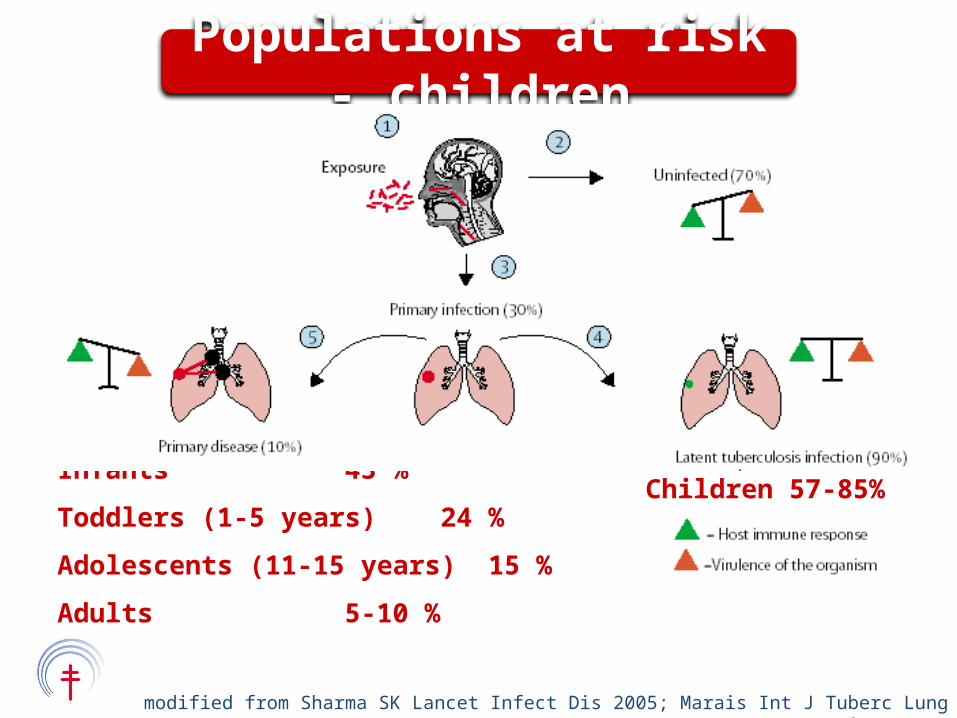
Infants 43 %
Toddlers (1-5 years) 24 %
Adolescents (11-15 years) 15 %
Adults 5-10 %
Children 57-85%
modified from Sharma SK Lancet Infect Dis 2005; Marais Int J Tuberc Lung Dis 2004
Populations at risk - children
o Children account for approximately 15% of the annual incident cases globallyo Up to 40% of caseload in some areas
o TB in children contributes to global child morbidity and mortality
TB in children – a global challenge

Diagnostic challenges:o Different disease presentationo Difficulty to produce sputum
Alternative: gastric acido Paucibacillary TB
Diagnosis relies on composite of exposure history, symptoms, X-ray
TB diagnosis in children
Method Characteristics adults
Fluorescence microscopy/LED FM
• Improved sensitivity compared to light microscopy (5-10%)
MODS • Simple, rapid, inexpensive
NAAT• Multiple Commercial/In-house assays• Variable performance
LPA•High accuracy•Recommended in smear positive
Xpert MTB/RIF
Good performance in smear negative
Urine LAM•Highly variable•Improved sensitivity in HIV-infected
Volatile organic compounds
• Few data• Sub-optimal accuracy in adults (breath)
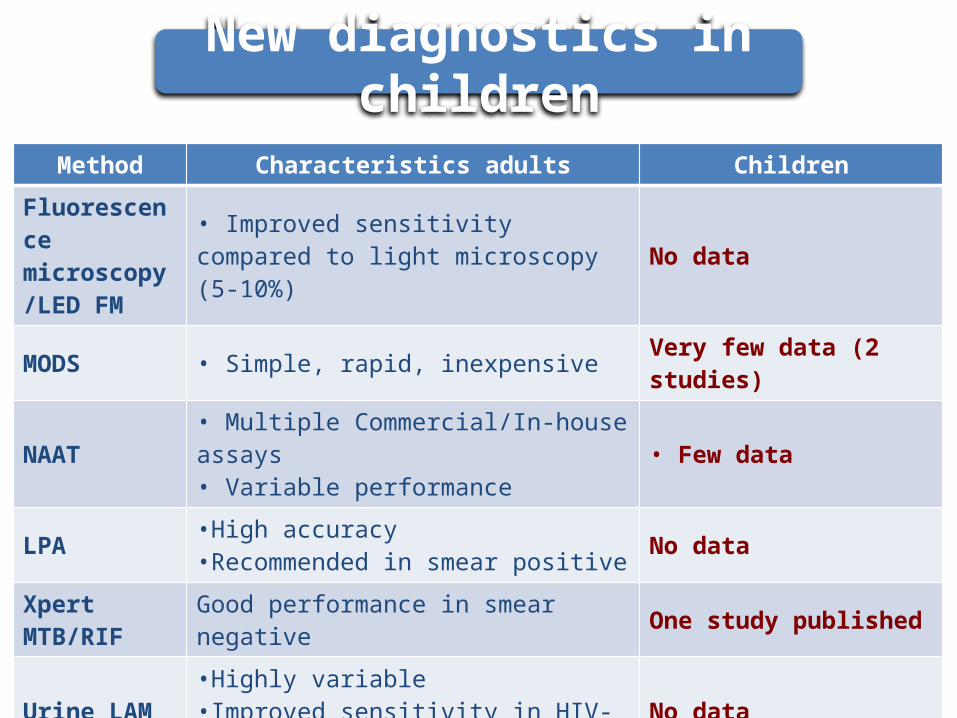
Method Characteristics adults Children
Fluorescence microscopy/LED FM
• Improved sensitivity compared to light microscopy (5-10%)
No data
MODS • Simple, rapid, inexpensive Very few data (2 studies)
NAAT• Multiple Commercial/In-house assays• Variable performance
• Few data
LPA•High accuracy•Recommended in smear positive
No data
Xpert MTB/RIF
Good performance in smear negative One study published
Urine LAM•Highly variable•Improved sensitivity in HIV-infected
No data
Volatile organic compounds
• Few data• Sub-optimal accuracy in adults (breath)
No data
New diagnostics in children

Policy
NDWG 2009
New diagnostics –from concept to public health implementation

WHO
WHO policy formulation
New diagnostics recent WHO policy recommendations
o 2007: Liquid culture and DST o 2008: Line probe Assayo 2010: Xpert MTB/RIFo 2011:
oNon-commercial culture and DST (MODS)o LED microscopyoNegative recommendation commercial
serodiagnostic tests o IGRAs
Limited data on patient outcomes and impact
High accuracy ≠ positive changes in outcomes
Challenges in developing policy guidance
o Functioning of new tool in different epidemiologic settings
o Functioning of new tool within diagnostic algorithms
o Cost effectivenesso Impact on health system and patientso Operational issues: training, maintenance, ,
supply chains, storage, waste management
Little information on
o WHO recommendation as basis for consideration
o Data from own or similar epidemiologic setting e.g. Brazil requests in-country validation and cost-effectiveness data
o Question remains: which tool or which combination of new tools
o Will there be another, better tool soon?
vanKampen PLoS One 2010
How does a country decide what to do?

o Negotiated reduced cost (WHO & FIND)o Rapid implementation documento Interim algorithmso Close monitoring of roll-out
http://www.who.int/tb/laboratory/mtbrifrollout/en/index.html
o TREAT TB: Monitoring of research
Global support – example Xpert
o Each policy document lists a number of open research questionso Test-specifico General related to implementation and impact
oCost effectivenesso Functioning of new test within health systemso Functioning within diagnostic algorithms (combination
of steps and tools)o Impact on patients (Cost, access)
Research – open questions

o Delay policy process?o Accompanying implementation process
o Optimize implementationo Inform national and global policy
o Different risk groups and disease manifestationso HIV-infectedo Childreno Extrapulmonary TB
Research
A framework for policy-relevant research – impact assessment
o Evaluation of new tools o under program conditionso as part of diagnostic strategies
o The impact of new diagnostic approaches should be measured on their ability to increase case detection. o Acceptable levels of sensitivity and specificityo Affordability (to the health system – and patients)o Accessibility (e.g. to all TB suspects)
o Impact on the society
Support decision making process for National TB Programs on which, when and how to implement new tools
Layer of Assessment
Layer 1:EFFICACY
ANALYSIS
Layer 2:EQUITY ANALYSIS
Layer 3:HEALTH SYSTEM
ANALYSIS
Layer 4: SCALE UP
ANALYSIS
Layer 5: POLICY ANALYSIS
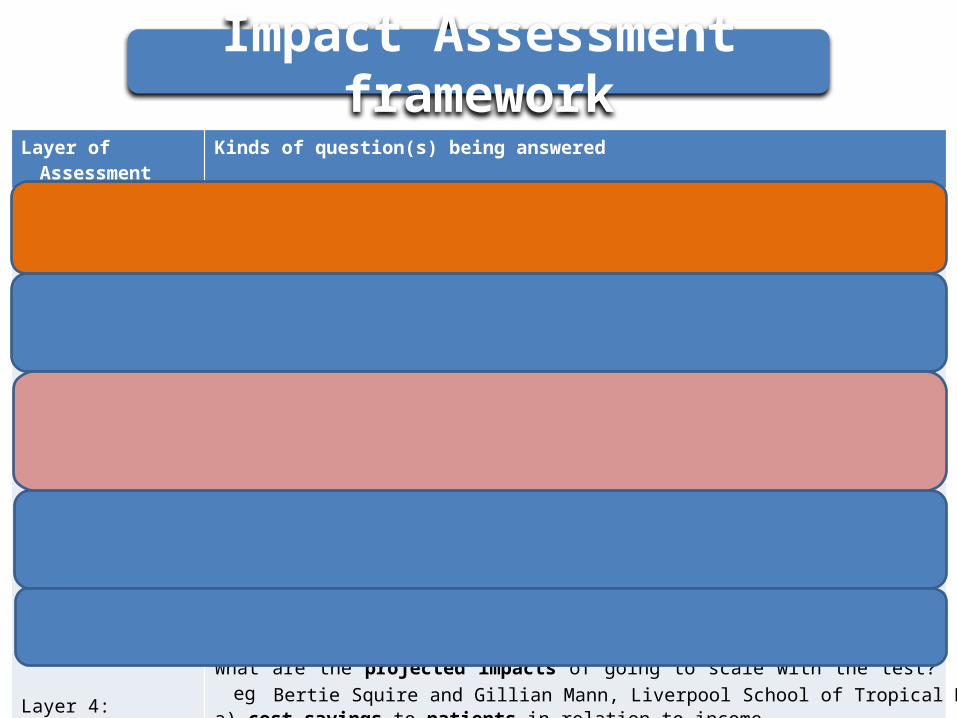
Layer of Assessment
Kinds of question(s) being answered
Layer 1:EFFICACY
ANALYSIS
How well does new test work in terms of accuracy? How many additional cases will be identified?How many additional cases will actually start treatment / achieve cure / avoid
death?
Layer 2:EQUITY ANALYSIS
Who benefits from new test? (ambulant vs hospitalised, poor/less poor, men/women, adults/children)
Why do these benefits accrue? (level health system in which tests are deployed, change time to issue of results, change in patient costs)
Layer 3:HEALTH SYSTEM
ANALYSIS
What are the human resource implications of introducing the test? (training, number and cadre of staff)
What are the infrastructure implications? (equipment, lab layout, safety installations)What are the procurement implications? (reagents, consumables, documentation)What are the implications for quality assurance? (internal and external)
Layer 4: SCALE UP
ANALYSIS
What are the projected impacts of going to scale with the test? ega) cost savings to patients in relation to incomeb) cost savings to health providers / the health systemd) Effects on transmission of improved infection control as a result of test introduction
Layer 5: POLICY ANALYSIS
What other similar technologies are available or likely to become available?How do similar existing or emerging technologies compare in their projected
performance within each of the layers above?
Bertie Squire and Gillian Mann, Liverpool School of Tropical Medicine
Impact Assessment framework
o Exciting new diagnostics have been developedo Many open questions remain as to
o how these new diagnostics work in health systemso how they influence patient outcomes
o Need for more researcho Still needed:
o point of care diagnostics testo Better diagnostics for
Conclusions

Thank you!