Diabetes Nation for Iowa 2015 - s3.amazonaws.com Diabetes Care, Risk Medical Solutions, Vision...
20
10/4/15 1 Diabetes Nation Where Are We & Where Do We Go From Here? A. Paul Chous, MA, OD, FAAO Tacoma, WA Disclosures I am or have been a consultant for, been on advisory boards of, or spoken on behalf of: Bausch & Lomb, Freedom Meditech, GlaxoSmithKline, Kestrel, Kowa, LifeMed Media, Prodigy Diabetes Care, Risk Medical Solutions, Vision Service Plan, ZeaVision None of these affiliations have affected the content of this presentation 29.1 million Americans have diabetes 8 million Americans with diabetes haven’t yet been diagnosed 86 million more are at high risk 2014 ADA Diabetes Fact Sheet Further Increases in the Prevalence of Diabetes Are Expected 0 5,000,000 10,000,000 15,000,000 20,000,000 25,000,000 30,000,000 35,000,000 2005 2010 2025 2050 Projected Number of Persons With Diagnosed Diabetes Based on diabetes prevalence rates predicted from 1980-1998 trends from the National Health Interview Survey and predicted US Census Bureau’s population projections. Boyle JP, et al. Diabetes Care. 2001;24:1936-1940. Diagnosed Diabetes 2014 Diabetes – A “Growth Industry” 86 million Americans have pre-diabetes Diabetes & pre-diabetes affect 1/2 of US Adults JAMA. 2015;314(10):10211029. Diabetes Myths Diabetes only occurs in obese people Not taking medications to control diabetes means the disease is less serious Having type 2 diabetes is ‘better’ than having type 1 diabetes Type 2 diabetes is not hereditary
Transcript of Diabetes Nation for Iowa 2015 - s3.amazonaws.com Diabetes Care, Risk Medical Solutions, Vision...

10/4/15
1
Diabetes Nation
Where Are We & Where Do We Go
From Here?
A. Paul Chous, MA, OD, FAAO Tacoma, WA
Disclosures I am or have been a consultant
for, been on advisory boards of, or spoken on behalf of:
Bausch & Lomb, Freedom Meditech, GlaxoSmithKline, Kestrel, Kowa, LifeMed Media, Prodigy Diabetes Care, Risk Medical Solutions, Vision Service Plan, ZeaVision
None of these affiliations have affected the content of this presentation
29.1 million Americans have
diabetes
8 million Americans with
diabetes haven’t yet been
diagnosed
86 million more are at high risk 2014 ADA Diabetes Fact Sheet
Further Increases in the Prevalence of Diabetes Are Expected
0
5,000,000
10,000,000
15,000,000
20,000,000
25,000,000
30,000,000
35,000,000
2005 2010 2025 2050
Proje
cted N
umbe
r of P
erso
ns W
ith
Diag
nose
d Diab
etes
Based on diabetes prevalence rates predicted from 1980-1998 trends from the National Health Interview Survey and predicted US Census Bureau’s population projections. Boyle JP, et al. Diabetes Care. 2001;24:1936-1940.
Diagnosed Diabetes
2014
Diabetes – A “Growth Industry”
86 million Americans have
pre-diabetes Diabetes & pre-diabetes affect
1/2 of US Adults
JAMA. 2015;314(10):1021-‐1029.
Diabetes Myths
n Diabetes only occurs in obese people
n Not taking medications to control diabetes means the disease is less serious
n Having type 2 diabetes is ‘better’ than having type 1 diabetes
n Type 2 diabetes is not hereditary
10/4/15
2
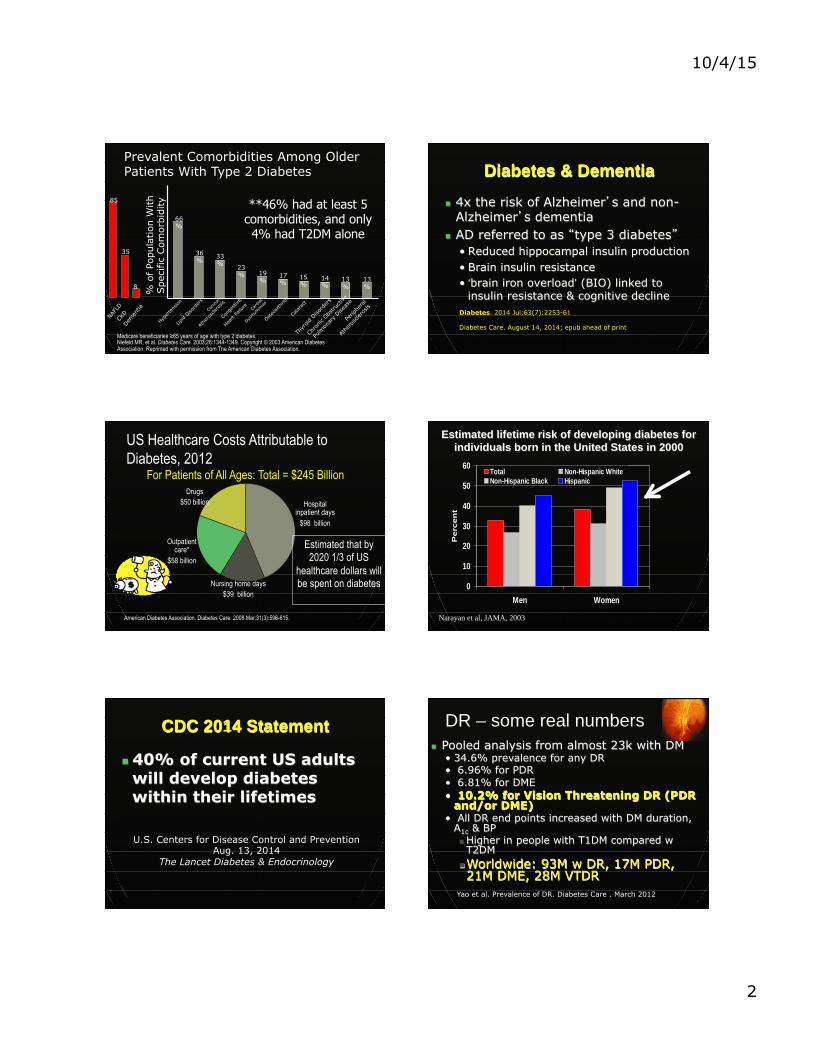
Prevalent Comorbidities Among Older Patients With Type 2 Diabetes
Niefeld MR, et al. Diabetes Care. 2003;26:1344-1349. Copyright © 2003 American Diabetes Association. Reprinted with permission from The American Diabetes Association.
Medicare beneficiaries ≥65 years of age with type 2 diabetes.
66%
36% 33
% 23% 19
% 17%
15%
14%
13% %
of Po
pula
tion
With
Spe
cific
Com
orbi
dity
Hyper
tens
ion
Lipid
Disord
ers
Coro
nary
Athe
rosc
leros
is
Cong
estive
Heart
Failu
re
Card
iac
Dysrh
ythm
ias
Osteoa
rthrit
is
Catara
ct
Thyr
oid D
isord
ers
Chro
nic O
bstru
ctive
Pulm
onar
y Dise
ase
Perip
hera
l
Athe
rosc
leros
is
13%
**46% had at least 5 comorbidities, and only 4% had T2DM alone
NAF
LD
CKD
Dem
entia
85
35
8
Diabetes & Dementia
n 4x the risk of Alzheimer’s and non-Alzheimer’s dementia
n AD referred to as “type 3 diabetes” • Reduced hippocampal insulin production • Brain insulin resistance • ‘brain iron overload’ (BIO) linked to
insulin resistance & cognitive decline Diabetes. 2014 Jul;63(7):2253-61 Diabetes Care. August 14, 2014; epub ahead of print
US Healthcare Costs Attributable to Diabetes, 2012
American Diabetes Association. Diabetes Care. 2008 Mar;31(3):596-615.
Hospital inpatient days
$98 billion
Outpatient care*
$58 billion
For Patients of All Ages: Total = $245 Billion Drugs
$50 billion
Nursing home days $39 billion
Estimated that by 2020 1/3 of US
healthcare dollars will be spent on diabetes 0
10
20
30
40
50
60
Men Women
Perc
en
t
Total Non-Hispanic WhiteNon-Hispanic Black Hispanic
Narayan et al, JAMA, 2003
Estimated lifetime risk of developing diabetes for individuals born in the United States in 2000
CDC 2014 Statement
n 40% of current US adults will develop diabetes within their lifetimes
U.S. Centers for Disease Control and Prevention Aug. 13, 2014
The Lancet Diabetes & Endocrinology
DR – some real numbers n Pooled analysis from almost 23k with DM
• 34.6% prevalence for any DR • 6.96% for PDR • 6.81% for DME • 10.2% for Vision Threatening DR (PDR
and/or DME) • All DR end points increased with DM duration,
A1c & BP n Higher in people with T1DM compared w T2DM
n Worldwide: 93M w DR, 17M PDR, 21M DME, 28M VTDR
Yao et al. Prevalence of DR. Diabetes Care . March 2012

10/4/15
3
What This Means for the US
• 9.65 million with any DR
• 2.85 million Americans with Sight-threatening diabetic retinopathy
How is The World Doing?
Source: Organisa6on for Economic Coopera6on and Development (OECD) 2011
USA
500,000,000 People Will Have Diabetes
By 2030
Source: IDF 2013
Percent Change in Diabetes Prevalence Amongst Adults from 1995 to 2010
10/4/15
4
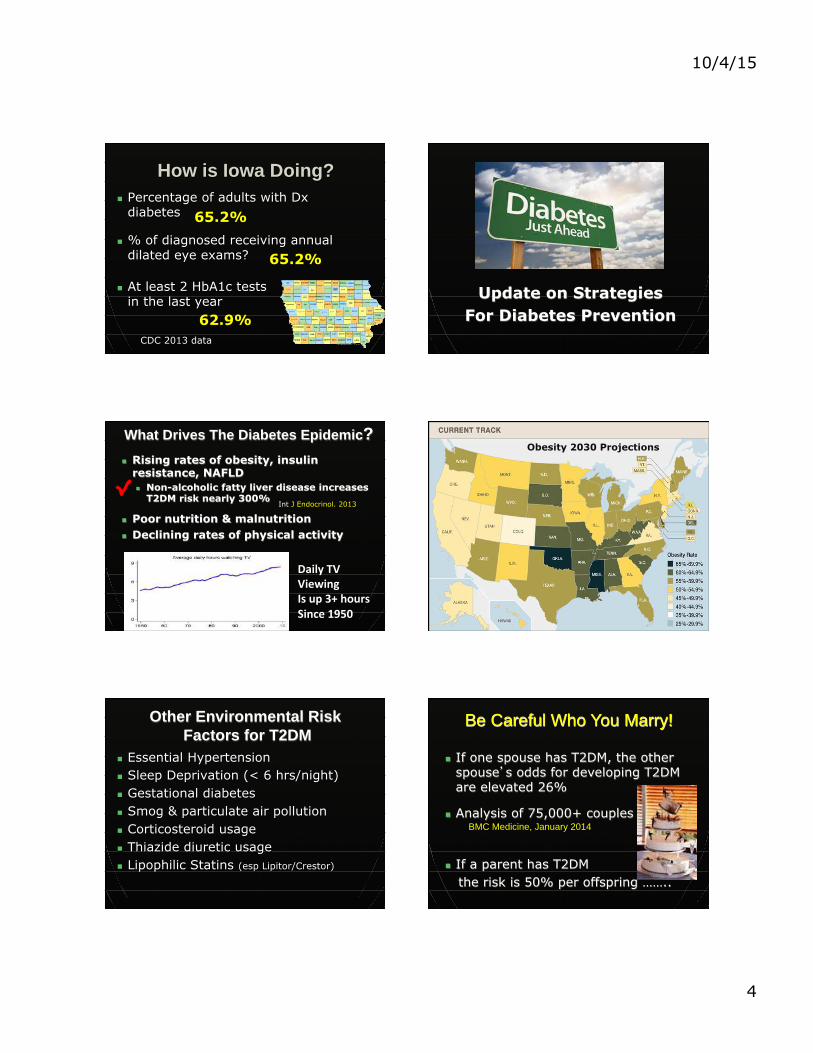
How is Iowa Doing? n Percentage of adults with Dx
diabetes
n % of diagnosed receiving annual dilated eye exams?
n At least 2 HbA1c tests in the last year
CDC 2013 data
65.2%
65.2%
62.9%
Update on Strategies For Diabetes Prevention
What Drives The Diabetes Epidemic? n Rising rates of obesity, insulin
resistance, NAFLD n Non-alcoholic fatty liver disease increases
T2DM risk nearly 300%
n Poor nutrition & malnutrition n Declining rates of physical activity
Int J Endocrinol. 2013
Daily TV Viewing Is up 3+ hours Since 1950
Obesity 2030 Projections
Other Environmental Risk Factors for T2DM
n Essential Hypertension n Sleep Deprivation (< 6 hrs/night) n Gestational diabetes n Smog & particulate air pollution n Corticosteroid usage n Thiazide diuretic usage n Lipophilic Statins (esp Lipitor/Crestor)
Be Careful Who You Marry!
n If one spouse has T2DM, the other spouse’s odds for developing T2DM are elevated 26%
n Analysis of 75,000+ couples
n If a parent has T2DM the risk is 50% per offspring ……..
BMC Medicine, January 2014

10/4/15
5
Diabetes Among Youth n By 2050, cases of both type 1 and type 2 diabetes in Americans < 20 will rise dramaFcally • T1DM to triple (179K to 587K) • T2DM to quadruple (22.8K to 82.1K) • Majority of increased rates to be seen in Hispanic, Asian and African American youth)
Diabetes Care. 2012;35:2515-‐2520
T2DM in Kids Insulin resistance progresses faster in kids with T2DM aged 10-‐17
4x faster decline in pancreaFc beta cell mass compared with adults (20-‐35% decline v. 7-‐11% decline per year)
Triple the rate of early Diabetes Care May 2013
kidney disease
T2DM in Young People is WORSE than T1DM
n T2DM diagnosed between 15-‐30 years of age is TWICE as likely to result in death • AZer controlling for age at diagnosis, duraFon of disease and HbA1c (n = 824; mean A1c = 8.1% in both groups)
• 20+ year follow-‐up • 5X the rate of ischemic heart disease & 6X the rate of stroke
• 30% worse nerve funcFon but equivalent DR rates (37% vs 41%) Diabetes Care. 2013 Dec;36(12):3863-9
Strategies to Prevent Diabetes
Exercise…a DIRTY word!!

10/4/15
6
The DPP n Diabetes Prevention Program
n The Diabetes Prevention Program (DPP) conducted at 13 US centers showed that “lifestyle modification” (walking 30 minutes each day, five days each week) lowered the risk of developing T2DM in those with prediabetes (IGT or IFG) by 58% over a four year period
Twice as effecFve as medormin (GlucophageTM)
What About Metformin + Exercise?
n Several studies show that add-on metformin lessens the insulin sensitizing effects of exercise in pre-diabetes
n Pioglitazone reduced conversion to T2DM by 72% (weight gain & edema common)
Diabetes Care. 2012 January; 35(1): 131–136. Obesity (Silver Spring). 2013 January; 21(1)
N Engl J Med. 2011 Mar 24;364(12):1104-15
Act Now Study
VITAMIN D STATUS AND DIABETES
Incidence of Diabetes NHANES: 8.5/1,000 person-‐years US D*ac6on: 0.9/1,000 person-‐years
Average Serum Level NHANES: 22 ng/ml US D*ac6on: 53 ng/ml
Equivalent Mean BMI NO adjustments for Age Fam Hx HTN
80% risk reducFon Over 5 yrs aZer all adjustments
Primary PrevenFon of T2DM Unpublished data
Diabetologia 2008; June 12

10/4/15
7
Vitamin D Summary
n Reasonably good evidence for benefit n Evidence shows inverse relationship
between DR severity & serum vit D
n Associations, positive or negative, do not establish causality
n Most experts agree that 2000 IU vitamin D3/day is safe and that serum 25-OH D > 50 ng/ml is preferable
2009 Vitamin D Cosensus Panel Univ of Toronto Schhol of Medicine
Endocr Pract. 2012 Mar-Apr;18(2):185-93
What Diet Is Best to Prevent DM? ¨ Multiple observational studies link
high meat intake to more diabetes
¨ FFQ of 41,387 patients showed lowest risk for vegans, especially in African-Americans – hazard ratios: ¡ Vegan: 0.43
¡ Lacto-ovo Vegetarian: 0.68
¡ Vegan: 0.30 ¡ Lacto-ovo Vegetarian: 0.47
Non-Black Race
Black Race
Nutrition, Metabolism & Cardiovascular Diseases. 2013;23:292-299
Too Many Calories, but…..
Not All Calories Are The Same
Are All Calories Equal?
n Probably NOT ü Fructose forms intra-hepatic fat and AGEs at a higher (7X) rate than does glucose
ü Fructose and HFCS raise uric acid & are causally linked to diabetes and Met Synd
Int J Mol Sci. 2013 Nov 5;14(11):21873-86
Diabetes. 2013 Oct;62(10):3307-15.
Hide not thy poison with such sugar'd words
- Henry VI Part 2
Myth or Fact: High Sugar Intake Causes Diabetes?
Econometric analysis of 175 countries
Every 150kcal/person/day sugar consumpFon increases populaFon diabetes prevalence 1.1%
Equivalent to 1 can of soda per day
PLoS One. 2013;8(2):e57873

10/4/15
8
• “Differences in sugar availability statistically explain variations in diabetes prevalence rates at a population level that are not explained by physical activity, overweight or obesity”
National obesity rates are NOT totally synchronous with rates of diabetes
Sugar Availability and Increased Diabetes
Total Sugar Intake 1700 to 2000
Am J Clin Nutr
Consumption of Sugared Soda and Fruit Juice 1977-2006 WHO 2014 Recommendations
for Sugar Consumption n Added sugars, sugar from fruit juices
& honey should be less than 5% of total calories
n < 25 grams/day
WHO Guideline: Sugar intake for adults and children, March 5, 2014
40 gm 3 gm 24 gm

10/4/15
9
Smoking Gun n 2014 Surgeon General Report concludes
that cigarette smoking is causally linked to T2DM based on meta-analysis
Surgeon General’s 5oth Annual Report on Smoking US Department of Health & Human Services, Jan 20, 2014
Independent Of all other Diabetogenic Factors 54% ñ risk For 1+ pack/d
Other Steps to Avoid Diabetes
n Significant Risk Reductions Associated With: • Mediterranean-type Diet • Avoidance of beta-cell toxicity from
nitrate/nitrate preservatives • Higher variety of vegetables (> 14/wk) • Drinking coffee or tea • Moderate use of cannibis
Am J Med. 2013 Jul;126(7):583-9
Arch Int Med 2009;169(22): 2053-63 Am J Clin Nutr. 2011 Aug 10, epub
Diabetes Care. 2012 Apr 3.
Diabetes Res Clin Pract. 2010 Aug;89(2):97-102
Practical Tips To Avoid Diabetes
n Exercise 30 minutes each day (soon after waking) n Eat a Mediterranean type diet n Eat breakfast n Eat a variety of fruits and vegetables and more
vegetables n Minimize processed meats n Drink coffee or tea Don’t Smoke n Sleep > 6 hours per night n Get your serum vitamin D checked n Breast feed *Turn down the thermostat
* Live away from smog
Update on Diabetes Diagnosis
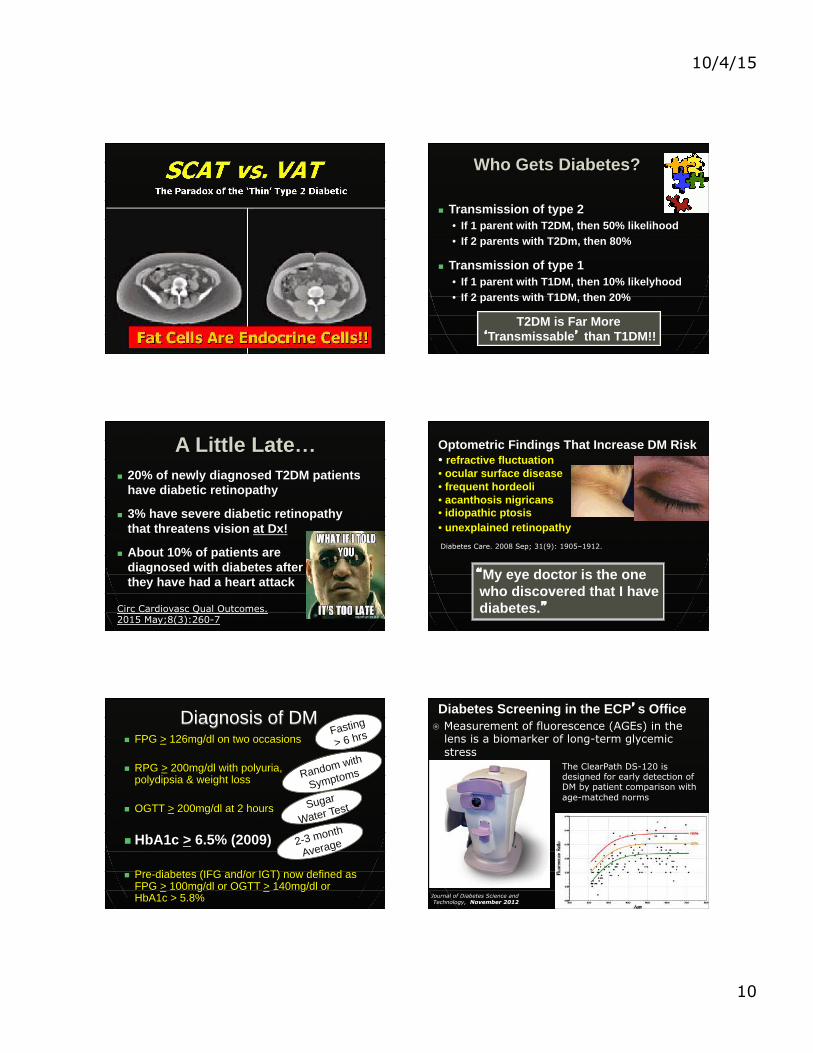
Who Gets Diabetes
n Older pts > Younger pts n Men > Women in mid-life n People with a strong family history n People with essential HTN n People who are physically inactive n African, Latino and Pacific Island
Americans > European Americans n Those with increased abdominal fat
Visceral Adipose Tissue: Bad Fat Releases Bad Hormones
n Visceral fat releases substances that cause insulin resistance and mobilize non-esterified fatty acids (Free Fatty Acids)
n High Abdominal Fat is BAD
10/4/15
10
Who Gets Diabetes?
n Transmission of type 2 • If 1 parent with T2DM, then 50% likelihood • If 2 parents with T2Dm, then 80%
n Transmission of type 1 • If 1 parent with T1DM, then 10% likelyhood • If 2 parents with T1DM, then 20%
T2DM is Far More ‘Transmissable’ than T1DM!!
A Little Late… n 20% of newly diagnosed T2DM patients
have diabetic retinopathy
n 3% have severe diabetic retinopathy that threatens vision at Dx!
n About 10% of patients are diagnosed with diabetes after they have had a heart attack
Circ Cardiovasc Qual Outcomes. 2015 May;8(3):260-7
“My eye doctor is the one who discovered that I have diabetes.”
Optometric Findings That Increase DM Risk • refractive fluctuation • ocular surface disease • frequent hordeoli • acanthosis nigricans • idiopathic ptosis • unexplained retinopathy Diabetes Care. 2008 Sep; 31(9): 1905–1912.
Diagnosis of DM n FPG > 126mg/dl on two occasions
n RPG > 200mg/dl with polyuria, polydipsia & weight loss
n OGTT > 200mg/dl at 2 hours
n HbA1c > 6.5% (2009)
n Pre-diabetes (IFG and/or IGT) now defined as FPG > 100mg/dl or OGTT > 140mg/dl or HbA1c > 5.8%
Fasting
> 6 hrs
Random with
Symptoms
Sugar
Water Test
2-3 month
Average
Diabetes Screening in the ECP’s Office � Measurement of fluorescence (AGEs) in the
lens is a biomarker of long-term glycemic stress
The ClearPath DS-120 is designed for early detection of DM by patient comparison with age-matched norms
Journal of Diabetes Science and Technology, November 2012

10/4/15
11
Significance of AGEs? n Long-term biomarkers of glucose toxicity
n Implicated in virtually ALL diabetes complications, Alz Dis, as well as AMD
n Inhibit the SIRT1 gene -> shorten lifespan
n Found in foods cooked at high temperatures and low humidity • Methylglyoxal found in grilled meats worsens
human cognition and insulin sensitivity
J Gerontol A Biol Sci Med Sci. 013 Jan;68(1):68-73. Proc Natl Acad Sci U S A. 2012 Sep 25;109(39):15888-93 Microvasc Res. 2014 Jun 28;95C:1-6.
Update on Trends in Diabetes Treatment
Metabolic Control in US Diabetes Patients
n 50% have A1c > 7% & 33% have A1c > 8%
n Per AACE guidelines, half of patients with T2DM are on inappropriate meds Arch Intern Med. 2008 Oct 27;168(19):2088-94
n Up to 70% of patients with diabetes have blood pressure levels above target J Gen Intern Med. 2008 May;23(5):588-94
J Clin Hypertens 2010 Oct;12(10):826-32. 2014 NIDDKD Fact Sheet
Treatment Trends n Most patients with T2DM are put on
metformin, followed by a sulfonylurea
n Data shows a shift toward combination therapy and incretin drugs (-gliptins & -tides)
Diabetes Care. 2003 Jun;26(6):1847-51 Adv Ther. 2007 Jul-Aug;24(4):803-13
Postgrad Med. 2011 Jan;123(1):53-65
Surprising Me[ormin Fact
n 33-‐50% of non-‐insulin diabetes medica6ons are NOT being prescribed with me[ormin
n Counter to Clinical Prac6ce Guideline recommenda6ons of AACE, ADA, AAFP to use me[ormin as first-‐line agent with all other agents being ADDITIVE
Hampp, C. et al. "Use of AnDdiabeDc Drugs in the U.S., 2003-‐2012" Diabetes Care. 2014; 38: 8p
Benefits of Incretins
n Victoza & Byetta/Bydureon, Trulicity (injected)
n Januvia, Tradjenta, Onglyza (oral)
n Weight loss with the former (10-20 lbs) n Better preservation of beta cells with
both
n Early data shows improved cardiovascular outcomes with GLP-1 analogs
Postgrad Med. 2013 May;125(3):7-20 Adv Exp Med Biol. 2010;654:515-35

10/4/15
12
InvokanaTM (canigliflozin) • First FDA approved SGLT2-‐inhibitor agent causing glycosuria – excess glucose eliminated in urine – lowers HbA1c 0.7%-‐1% – increased risk of UTI – 5-‐10 lbs weight loss – approved in T2DM – Lowers BP
Diabetes Obes Metab. 2013;15(4):372-‐82
FarxigaTM (dapagliflozin)
Victoza/Byetta + metformin + Actos
Early triple therapy results in better everything: n A1c, fasting glucose, post-prandial glucose n Beta cell mass & function n Weight, BP, Lipids
Need longer RCTs
AACE Presentation, 2013
Diabetes Meds Are Expensive
n 40+% increase in filled diabetes Rxs from 2003-2012
n Amongst non-specialty medications, diabetes meds are the most expensive
n Patient costs rose 14% in 2013, while lipid and BP med costs declined modestly
n Out of pocket costs may easily exceed $500/month
Express Scripts Survey, April 2014
Bariatric Surgery for DM
Rou-en Y Gastric Bypass
Laparoscopic Adjustable
Gastric Band Gastric Sleeve
Surgery is Effective…
n STAMPEDE 3-year study shows far superior A1c results than intensive medical therapy (IMT) - mean BMI = 36.7
• 38% of gastric by-pass pts had A1c < 6% and 94% were off insulin at year 3
• 25% and 92% of gastric sleeve pts
• 5% and 45% with IMT
Bariatric surgery versus intensive medical therapy for diabetes -- 3-year outcomes, NEJM 2014
Bariatric Surgery & Progression of Retinopathy (n = 148)
n 56% of mild NPDR regressed and 45% was stable (none progressed)
n 1 pt with moderate NPDR and 2 with severe NPDR progressed
n Those with progression had higher pre-surgical A1c and larger A1c drop post-surgery
n “Euglycemic re-entry phenomena”
n Pts with moderate or worse NPDR prior to undergoing bariatric surgery need close F/U
J Diabetes Complications 2014 Mar-Apr;28(2):191-5.

10/4/15
13
Latest Research on Tight Metabolic Control in Higher
Risk Patients
n Is Lower Always Better?
How Low Should You Go? n Kids – fear that hypoglycemia
impairs cognitive development & increases risk of death Pediatr Endocrinol Rev.
2004 Aug;1 Suppl 3:530-6. n Adults with CVD – some studies
show risk of CV events may increase with tight control
Diabetes Care. 2008 May;31(5):952-7 N Engl J Med. 2008 Jun 12;358(24):2545-59
High Risk Patients with CVD & Poor Glycemic Control
n ACCORD: US study showed a 22% increased risk of death with tight BS control (A1c of 6.5% vs. 7.4%)
n ADVANCE: European study showed a small decrease in CV events and death (A1c of 6.5% vs. 7.3%)
n VADT: Smaller US study showed no difference (A1c of 6.9% vs. 8.4%)
N Engl J Med. 2008 Jun 12;358(24):2545-59
Diabetes Care. 2008 May;31(5):952-7
HbA1c Take Home Messages
n Lower A1c lowers risk of microvascular complications (DR)
n Lower A1c improves CV outcomes if • Dx < 15 years • A1c target achieved readily
n If pts with CVD have had T2DM > 20 years and/or don’t readily achieve A1c levels < 7%, back off!!
Continuous Glucose Monitoring
n Only used for patients on insulin n SC sensor implanted Q7 days
n Alarms for hypo- and hyperglycemic thresholds (e.g. < 70 and > 170)
Emerging Therapies for T1DM n Immune therapy
• Anti-CD3 monoclonal antibody vaccines • GAD65 auto-antigen therapy • TB vaccine (T cell death x 1 wk)
n Micro-encapsulated beta cells • ViaCyte Encaptra system

10/4/15
14
What’s Wrong With Insulin Delivery?
Pancreatic insulin is secreted directly into the hepatic portal vein
n “Rapid Acting” insulins (NovologTM,
HumalogTM) do not exert significant activity for 30-60 minutes given S/C • Guarantees significant post-meal
hyperglycemia
Solutions?
n Inhaled insulin • ExuberaTM pulled from the market • AfreezaTM now has FDA approval
n Glucose responsive Insulin (GRI) • pH sensitive polymer or membrane
releases insulin only when glucose elevated (JDRF GRI Prize)
Insulin Pros & Cons The Good
n Early use preserves beta cell function
n Early use may promote protective metabolic memory
n Allows correction of mild to profound hyperglycemia
The Bad
n Weight gain
n Hypoglycemia
n Poorer survival in pts with cancer
Diabetologia. 2014 May;57(5):927-34.
In T1DM, insulin pump use i mortality 29% vs injections over 15 years after all controls
EASD 2014 Vienna
A Few Trends in Managing Diabetic Retinopathy
Out, damned spot! out, I say! - Macbeth
Lipid Agents & ReFnopathy SimvistaFn + Fenofibrate therapy lowers the
risk of DR progression by 35% (and need for laser by 31%) compared to simvista6n alone in pts with T2DM and high cardiovascular risk (n = 2856)
Consistent with FIELD Study showing reduced progression of DR and need for laser Tx Lancet 2007 370(9600):687-‐97
ACCORD Eye Study, N Engl J Med. 2010 Jul 15;363(3):233-‐44
Add-‐on Fenofibrate lowers risk of DR progression in T2DM
Fenofibrate
n Approved first-line therapy for NPDR in Australian adults with T2DM
n NNT = 14 for prevention of CSME/PDR
n Decreases total macular volume in DME
n Reduces CV events 30% in women and 13% in men
Ophthalmic Epidemiol. 2014 Oct;21(5):307-17
Ophthalmology. 2014 Aug 26. Curr Med Chem. 2013;20(26):3258-66
Diabetologia 2014; DOI: 10.1007/s00125-014-3344-3. Diabetologia 2014; DOI: 10.1007/s00125-014-3344-3. Diabetologia 2014; DOI: 10.1007/s00125-014-3344-3. Diabetologia 2014; DOI: 10.1007/s00125-014-3344-3. Diabetologia 2014; DOI: 10.1007/s00125-014-3344-3. Diabetologia 2014; DOI: 10.1007/s00125-014-3344-3. Diabetologia 2014; DOI: 10.1007/s00125-014-3344-3. Diabetologia 2014; DOI: 10.1007/s00125-014-3344-3. Diabetologia 2014; DOI: 10.1007/s00125-014-3344-3.
Diabetologia 2014

10/4/15
15
ACEIs/ARBs Vasotec® (enalapril) and Cozaar® (losartan) reduce the risk of DR progression by 65% and 70% in T1DM NEJM 2009;361: 40-‐51
Captopril reduces DR progression 40% and DME 30% by OCT in T2DM
Should these agents become standard treatment of DR?
-‐prils and –sartans lower DR Risk of Progression
Chin Med J (Engl) 2012 Jan;125(2):287-‐92
Does This Patient Have CSME?
n Hard exudate within 1 DD of the fovea is highly sensitive (75- 94%) and specific (84%) for CSME in diabetes (n = 103)
OVS March 2014
Is Telescreening Valuable?
n PROS n Good reliability with
expert interpretation (JVN)
n Cheaper, mass access for underserved populations
n Improved public health
n CONS n Does not ID all ocular
complications of diabetes
n Does not emphasize education or prevention
n Human interaction results in better outcomes
n Possible misuse
Evolution of Clinical Imaging
Adaptive Optics IU School of Optometry
Biomedical Optics Express, 2014; 5 (3): 961
RESTORE & READ
n Lucentis versus Laser for Vision loss from CSME (20/40 to 20/200 BCVA)
n Percent achieving > 20/40 ETDRS acuity at 12 months: n Lucentis – 53% n Lucentis + Laser – 44.9% n Laser alone – 26.3%
n Benefit of Lucentis maintained at 3 years n No increased MI or CVA with Lucentis
Ophthalmology. 2011 Apr;118(4):615-25.
JAMA Ophthalmol. 2013 Feb;131(2):139-45
5

10/4/15
16
EyleaTM in Diabetes (Regeneron)
l Aflibercept vs. laser for CSME l Blocks all VEGF-A isoforms, IgG1 &
placental growth factors (PIGF) l Long half-life = fewer injections
l Better reductions in macular thickness and improvements in VA versus laser l +8.4 - +12.7 letters vs. +0.1 - +2.5 letters
Ophthalmology. 2011 Sep;118(9):1819-26
FDA Approved For DME 7/2014
Ophthalmology. 2014 Jul 8. pii: S0161-6420(14)00426
Avastin in DME
n Bevacizumab Or Laser Therapy in DME (BOLT) • Small study (n=80) showing better VA
over 24 mos with Avastin • Mean change +8.6 letters vs -0.5 letters
Arch Ophthalmol. 2012 Aug;130(8):972-9
Take Home for DME: n anti-VEGF treatments are
superior to macular laser for VA and OCT
• Earlier treatment and more injections appear to result in better vision • Bevacizumab (AvastinTM) + Laser most cost-effective comparing laser, steroid, Lucentis, Avastin or any combination
Ophthalmology. 2013 May 1. epub
Is It Safe????
n Meta-analysis of 2500 patients shows no significantly increased
risk of CVA, MI, vascular death or mortality with Lucentis for DME (but 95% CIs = 0.37 to 4.73)
n There is a dose-dependent increased risk of mortality (p = 0.04) that dissipates when Lucentis is used pro en reta (as needed) to p = 0.133 Retina. 2014 Apr;34(4):629-35
What anti-VEGF is Best for DME?
n Avastin, Lucentis & Eylea have now been studied head-to-head n (DRCR.net Protocol T)
n Cost-effectiveness is best with Avastin
n Adverse events with Avastin are under-reported
Int J Technol Assess Health Care. 2013 Oct;29(4):392-401
Protocol T – Published Results n Aflibercept yielded 5-7 additional
ETDRS letters when baseline VA was 20/50 or worse • Fewer pts needed rescue laser • 1 fewer injection
n Few adverse events in all 3 groups • No difference for serious events,
hospitalization or death
n Still only 1-year data N Engl J Med. 2015 Feb 18. [Epub ahead of print]

10/4/15
17
Intravitreal Steroid Implants
n Slow release
n Dexamethasone (OzurdexTM) • Lasts up to 6 mos
n Fluocinolone (IluvienTM) • Lasts up to 3 years Can We Predict Who is Going
to Develop Sight-threatening Diabetic Retinopathy?
A1c Variability Matters!
• 5 year cumulative incidence of laser Tx for DR in 1459 T1DM pts with highest (19%) vs lowest (10%) A1c variability controlling for mean A1c, duration, BP, kidney status, gender
• 70% increase risk of PDR in hi SD group
Diabetologia. 2013 Jan 13
Obstructive Sleep Apnea Syndrome
� OSAS is independently associated with risk of DR and its progression
Br J Ophthalmol. 2012 Dec;96(12):1535 Retina. 2012 Oct;32(9):1791-8.
Jpn J Ophthalmol. 2011 Nov;55(6):638-42 Am J Ophthalmol. 2011 Apr;151(4):604-9
Mil Med. 2010 Nov;175(11):913-6 Diabet Med. 2010 Apr;27(4):423-30
Am J Ophthalmol. 2009 Jun;147(6):1017-21
SNPs Increase Risk n Like AMD, gene single nucleotide
polymorphisms (SNPS) may confer significantly increased risk for severe DR
n No commercially available test………Yet
Invest Ophthalmol Vis Sci. Apr 2012; 53(4): 2377–2381.
Hum Mol Genet. Jun 15, 2011; 20(12): 2472–2481.
Invest Ophthalmol Vis Sci. 2014 Mar 19;55(3):1666-71.
Keys to Risk
n Diabetes duraFon n HbA1c n Blood Pressure n Diabetes sub-‐type n Gender n ReFnal Status at baseline
80% of All Risk is
determined By these 6 factors

10/4/15
18
www.RetinaRisk.com
• Algorithm recently validated in a multi-cultural UK cohort (> 15,000)
• Launched at AOA Convention, San Diego, 2013
• Free 30 day trial – check it out
Current Algorithm For Preventing Diabetic Retinopathy
• Keep blood glucose, blood pressure and blood lipids as close to normal as possible
• Get annual dilated retinal examinations • Get treatment if/when you develop
STR
Is There Anything More We Can Do?
STAY TUNED

10/4/15
19
SO……..Where Are We?
n In big trouble
n Diabetes and co-morbidities will bankrupt the US health care system
n Research suggests provider reimbursement for “Optimal Care” of DM patients must increase 19% for providers to break even!!!
n Boutique health care is on the rise
Diabetes Care. 2013;36(11): 3843-3849
Diabetes care 2013; 36(11):3843-9.
Slipping through the cracks n 44 yo male with T1DM 16 years
• A1c = 11%
n Dx with high-risk PDR 8/2013 with stat referral to retinology • BCVA 20/25 and 20/20
n Received Avastin OD and asked to return x 1 week • Upset about co-pay • Never returned for more Tx • Came to see me Sept 2014
9/11/2014
20/80 HM
● What the Endocrinologist/PCP should be communicating:
● What is this patient’s individualized A1c goal?
o What are the reasons of concern (if any) with the specific A1c goal?
o What is the treatment and follow-up plan?
Roundtable discussion with 5 endocrinologists July 17, 2014
● What Optometrists should be communicating: o What are the retinal findings? (No
abbreviations) o Comparison of current findings to
previous exam. o What is the surveillance
recommendation? o Is the patient being referred to a
Retinal Specialist, if so why? o What education points were touched
on at the visit?
Some Good News

10/4/15
20
n After 30 years, < 1% of patients in the DCCT on intensive management have suffered amputation, ESRD, or legal blindness
n Rates of acute MI and stroke in patients with T2DM have dropped by 60% over the last 20 years
Arch Intern Med. 2009 Jul 27;169(14):1307-16.
N Engl J Med. 2014;370(16):1514-1523.
New Diabetes n Increased incidence of diabetes
appears to be plateauing in the US JAMA. 2014;312(12):1218-1226
Where Do We Go From Here?
n We need to develop high quality, efficient, collaborative health care teams to manage diabetes
n We need to incentivize good self-care and prevention of diabetes
n Optometrists can play a vital role by being proactive & collaborative
Thank You! A. Paul Chous














![PatientPopGE Reflux CANCER: Where: C] NONE NONE Others: OPERATIONS: Others: FAMILY HISTORY (OTHER THAN YOU): Explain who and what kind C) Stroke Cl Diabetes C) Psychiatric Disorder](https://static.fdocuments.us/doc/165x107/5f7a115f4322132a773addb3/patientpop-ge-reflux-cancer-where-c-none-none-others-operations-others-family.jpg)