
Diabetes Management in the Hospital Bruce W. Bode, MD, FACE Atlanta Diabetes Associates Atlanta,...
61
-
Upload
raymond-haynes -
Category
Documents
-
view
213 -
download
0
Transcript of Diabetes Management in the Hospital Bruce W. Bode, MD, FACE Atlanta Diabetes Associates Atlanta,...


Diabetes Management in the Hospital
Bruce W. Bode, MD, FACE
Atlanta Diabetes Associates
Atlanta, Georgia

Diabetes in Hospitalized Patients1997
• 3.5 Million US Hospitalizations
15% of Admissions
• 14 Million Hospital Days
20% of All Hospital Days
• 36% First Diagnosed in Hospital 66% No Documentation by Physician 27% Labeled Hyperglycemia 2% Diagnosed on Chart

Diabetes in Hospitalized Patients1997 Costs
•$$23,500 Each Diabetes Patient vs.23,500 Each Diabetes Patient vs. $12,200 for Non-Diabetes Patient$12,200 for Non-Diabetes Patient
•60% of All Diabetes-Related Costs60% of All Diabetes-Related Costs
•Only 5% DKA, HHNKCOnly 5% DKA, HHNKC
•48% Diabetes Complications48% Diabetes Complications
•52% Other Conditions52% Other Conditions

Diabetes in Hospitalized PatientsDiabetes in Hospitalized PatientsReason for Higher CostsReason for Higher Costs
Higher Rate of HospitalizationHigher Rate of Hospitalization
Longer StaysLonger Stays
More Procedures, MedicationsMore Procedures, Medications
Chronic ComplicationsChronic Complications
More Arteriosclerotic DiseaseMore Arteriosclerotic Disease
More InfectionsMore Infections
Complicated PregnanciesComplicated Pregnancies

Diabetes in Hospitalized PatientsDiabetes in Hospitalized Patients
• High-risk for Bacterial Infection– Surgery– Catheters– Intravenous Access– Anaesthesia
Problems with wound healing
Problems with tissue and organ perfusion

InfectionsInfections in Diabetesin Diabetes
More FrequentMore Frequent
Bacteremia Bacteremia
Septic ShockSeptic Shock
PyelonephritisPyelonephritis
CandidaCandida
TPNTPN
UniqueUnique
Necrotizing FasciitisNecrotizing Fasciitis
Fournier’s GangreneFournier’s Gangrene
MucoromycosisMucoromycosis
Emphysematous GB Emphysematous GB
Malignant External OtitisMalignant External Otitis

Infections in Diabetes
One BG >220 mg/dl results in 5.8 times increase in nosocomial infection rate
Two hours hyperglycemia results in impaired WBC function for weeks
Pomposelli, New England Deaconess,
J Parenteral and Enteral Nutrition 22:77-81,1998

TPN In DiabetesTPN In DiabetesVA Cooperative TrialVA Cooperative Trial
Benefit NegatedBenefit Negated
Increased InfectionsIncreased Infections
Related to HyperglycemiaRelated to Hyperglycemia
Buzby et al. NEJM 325:525-531, 1991Buzby et al. NEJM 325:525-531, 1991

Side Effects of BG >200 mg/dl Side Effects of BG >200 mg/dl
Reduced Intravascular VolumeReduced Intravascular Volume
DehydrationDehydration
Electrolyte FluxesElectrolyte Fluxes
Impaired WBC FunctionImpaired WBC Function
Immunoglobulin InactivationImmunoglobulin Inactivation
Complement DisablingComplement Disabling
Increased Collagenase, Decreased Wound Increased Collagenase, Decreased Wound CollagenCollagen

Psychology of Diabetes in HospitalPsychology of Diabetes in Hospital
Patients expect good glycemic control as part of Patients expect good glycemic control as part of hospital carehospital care
They strive for recommended goals at homeThey strive for recommended goals at home
Difficult to understand staff’s casual approach to BG’s Difficult to understand staff’s casual approach to BG’s >150>150

Evidence for Immediate Benefit of Evidence for Immediate Benefit of Normoglycemia in Hospitalized PatientsNormoglycemia in Hospitalized Patients
Numerous Publications on in Vitro EvidenceNumerous Publications on in Vitro Evidence
– Neutrophil DysfunctionNeutrophil Dysfunction
– Complement InhibitionComplement Inhibition
– Altered Redox State (Pseudohypoxia)Altered Redox State (Pseudohypoxia)
– Glucose Rich Edema as Culture MediaGlucose Rich Edema as Culture Media
Six Recent Clinical Publications supporting good glucose Six Recent Clinical Publications supporting good glucose control in the hospital settingcontrol in the hospital setting

Open Heart Surgery in DiabetesPortland St. Vincent Medical Center
Control Group
N=968
1987-1991
SubQ Insulin q 4 h
Goal 200 mg/dl
Standard Deviation 36
All Mean BG’s <200 47%
Study Group
N=1499
1991-1997
IV Insulin
Goal 150-200 mg/dl
Standard Deviation 26
All Mean BG’s <200 84%
Furnary et al, The 34th Meeting of The Society of Thoracic Surgeons New Orleans, LA January 26, 1998

Open Heart Surgery in DiabetesOpen Heart Surgery in DiabetesPortland CII ProtocolPortland CII Protocol
DemographicsDemographics
Total Open Heart Surgery Patients 14,468Total Open Heart Surgery Patients 14,468
Diabetes at Admission 2467 (17%)Diabetes at Admission 2467 (17%)
Age 65 SD 10Age 65 SD 10
Males 62%Males 62%
Insulin Rx 36%Insulin Rx 36%
OHA 48%OHA 48%

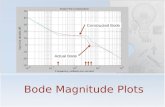
170
190
210
230
250
DOS POD 1 POD 2 POD 3
SQI
CII
Open Heart Surgery in DiabetesPortland St. Vincent Medical Center Perioperative Blood Glucose
Furnary et al, The 34th Meeting of The Society of Thoracic Surgeons New Orleans, LA January 26, 1998

Incidence of DSWI: 1987-1997
0.0%
1.0%
2.0%
3.0%
4.0%
87 88 89 90 91 92 93 94 95 96 97
Year
DS
WI DM Pts.
Non-DM
CII
Furnary, et al, The 34th Meeting of The Society of Thoracic Surgeons New Orleans, LA January 26, 1998

Open Heart Surgery in DiabetesOpen Heart Surgery in DiabetesPortland CII ProtocolPortland CII Protocol
Infectious ComplicationsInfectious Complications
DiabetesDiabetes
31/2467 (1.3%) Deep Sternal Wound Infection (DSWI)31/2467 (1.3%) Deep Sternal Wound Infection (DSWI)
23/31 Required Second Admission23/31 Required Second Admission
22 Micrococcus22 Micrococcus
0 Anaerobes, fungal, yeast0 Anaerobes, fungal, yeast
Non-DiabetesNon-Diabetes
40/12,005 (0.3%)40/12,005 (0.3%)

Open Heart Surgery in DiabetesOpen Heart Surgery in DiabetesPortland CII ProtocolPortland CII Protocol
MortalityMortality AllAll (99/2467) 4.0%(99/2467) 4.0%
SQI SQI 6.1% 6.1%
CIICII 3.0% 3.0%
DSWIDSWI 19.0% 19.0%
No DSWI 3.8%No DSWI 3.8%
Recent ExperienceRecent Experience
1994-1997 DSWI as in non-diabetics1994-1997 DSWI as in non-diabetics
1996-7 No DSWI in last 15 mo.1996-7 No DSWI in last 15 mo.

Open Heart Surgery in DiabetesOpen Heart Surgery in DiabetesPortland CII ProtocolPortland CII Protocol
Comparison of GroupsComparison of GroupsHigher Risk Patients in CII GroupHigher Risk Patients in CII Group
SQI CII P Value
Hypertension (% ) 54 67 0.0001
BMI 28.4 29.6 0.0001
Urgent Status (% ) 51 75 0.0001
ITA /CABG (% ) 64 71 0.001
LOS (Days ) 10.7 8.5 0.0001
Mortality (% ) 6.1 3.0 0.03

Open Heart Surgery in DiabetesOpen Heart Surgery in DiabetesPortland CII ProtocolPortland CII Protocol
Univariate Analysis of DSWIUnivariate Analysis of DSWI
No DSW I
DSW I P value
POD #1 >200 mg/d l (% )
34 42 0.04
LOS (Days) 9.5 25 0.001
Mortality (% ) 3.8 19 0.001

Variable SQI CII Savings# DSWI 2,968 1009 1,959
Additional LOS 47,488 16,416 31,342
Additional $ $78.4M $26.6M $51.7M
# Deaths 564 192 372
Estimated USA Socioeconomic Savings
Assumes 742K cases*, 20% prevalence of DM& 2% DSWI with SQI
*1998 Heart & Stroke Statistical update, AHA

Open Heart Surgery in DiabetesOpen Heart Surgery in DiabetesPortland CII ProtocolPortland CII Protocol
Weakness of StudyWeakness of Study
Not RandomizedNot Randomized
Temporal Sequential NatureTemporal Sequential Nature
Subtle Cumulative Improvements in TechniquesSubtle Cumulative Improvements in Techniques

Open Heart Surgery in DiabetesOpen Heart Surgery in DiabetesPortland CII ProtocolPortland CII Protocol
ConclusionsConclusions
Magnitude and Strength of Study is CompellingMagnitude and Strength of Study is Compelling
Ethics of Confirming Study Would be QuestionableEthics of Confirming Study Would be Questionable
Application of CII is Simple and SafeApplication of CII is Simple and Safe
Hyperglycemia Predicts DSWIHyperglycemia Predicts DSWI
CII Prevents DSWICII Prevents DSWI

Open Heart Surgery in DiabetesJohn Hopkins
Prospective Cohort Study of 411 OHS pts with Diabetes 1990 – 1995
Diabetes based on history (42% insulin treated, 45% oral agents)
SMBG 4x/day with sliding scale
Measured relationship between peri-operative control and risk of all infections

Open Heart Surgery in DiabetesJohn Hopkins
24.3% with infections
BG divided into quartiles Relative Odds
Q1 121-206 20.1%
Q2 207-229 21.6% 1.17
Q3 230-252 29.8% 1.86*
Q4 252-352 25.7% 1.72*
Golden SH Diabetes Care 22: 1408, 1999 * P < 0.01

DIGAMI StudyDiabetes, Insulin Glucose Infusion in Acute Myocardial Infarction(1997)
Acute MI With BG > 200 mg/dl Intensive Insulin Treatment IV Insulin For > 24 Hours Four Insulin Injections/Day For > 3 Months Reduced Risk of Mortality By:
28% Over 3.4 Years
51% in Those Not Previous Diagnosed
Malmberg BMJ 1997;314:1512Malmberg BMJ 1997;314:1512

Cardiovascular RiskMortality After MI Reduced by Insulin Therapy in the DIGAMI Study
Malmberg, et al. BMJ. 1997;314:1512-1515.
All Subjects
(N = 620)Risk reduction (28%)
P = .011
Standard treatment
0
.3
.2
.4
.7
.1
.5
.6
0 1Years of Follow-up
2 3 4 5
Low-risk and Not Previously on Insulin
(N = 272)Risk reduction (51%)
P = .0004
IV Insulin 48 hours, then 4 injections daily
0
.3
.2
.4
.7
.1
.5
.6
0 1Years of Follow-up
2 3 4 5
6-11

ICU Survival
1548 Patients (mostly OHS pts.)
All with BG >200 mg/dl
Randomized into two groups
– Maintained on IV insulin
– Conventional group (BG 180-200)
– Intensive group (BG 80-110)
Conventional Group had 1.74 X mortality
Van den Berghe et al, NEJM 2001;345(19):1359

ICU IV Insulin Protocol
If > 100 mg/dl, 2 U/h If > 200 mg/dl, 4 U/h
If > 140 mg/dl, increase by 1 – 2 U/h
If 121 to 140 mg/dl, increase by 0.5 – 1 U/h
If 111 to 120 mg/dl, increase by 0.1 – 0.5 U/h
If 81 to 110 mg/dl, no change
If 61 to 80 mg/dl, change back to prior rate
Van den Berghe et al, NEJM 2001;345(19):1359

ICU Survival
Blood glucose control:
Convetional Intensive
Mean AM BG 153 103
% Receiving Insulin 39% 100%
BG < 40 mg/dl 6 39
Van den Berghe et al, NEJM 2001;345(19):1359
In no instance was hypoglycemia considered to be a serious event

ICU Survival
Intensive Therapy (80 to 110 mg/dL) resulted in:
34% reduction in mortality
46% reduction in sepsis
41% reduction in dialysis
50% reduction in blood transfusion
44% reduction in polyneuropathy
Van den Berghe et al, NEJM 2001;345(19):1359

Conclusion
All hospital patients should have normal glucose

Insulin
The agent we have
to control glucose
only
most powerfulpowerful

Comparison of Human Insulins / Analogues
Insulin Onset of Duration ofpreparations action Peak action
Regular 30–60 min 2–4 h 6–10 h
Lispro/aspart 5–15 min 1–2 h 4–6 h
NPH/Lente 1–2 h 4–8 h 10–20 h
Ultralente 2–4 h Unpredictable 16–20 h
Glargine 1–2 h Flat ~24 h

4:004:00
2525
5050
7575
8:008:00 12:0012:00 16:0016:00 20:00 20:00 24:0024:00 4:004:00
BreakfastBreakfast LunchLunch DinnerDinner
Pla
sma
insu
lin
(P
lasm
a in
suli
n (µ U
/ml)
U
/ml)
TimeTime
8:008:00
Physiological Serum Insulin Secretion Profile

4:00 16:00 20:00 24:00 4:00
Breakfast Lunch Dinner
8:0012:008:00
Time
Glargineor
Detemir
Lispro Lispro Lispro
Aspart Aspart Aspartor oror
Pla
sma
insu
lin
Basal/Bolus Treatment Program withRapid-acting and Long-acting Analogs

Methods For Managing Hospitalized Persons with Diabetes
Continuous Variable Rate IV Insulin Drip
Major Surgery, NPO, Unstable, MI, DKA, Hyperglycemia, Steroids, Gastroparesis, Delivery, etc
Basal / Bolus Therapy (MDI) when eating

Continuous Variable Rate IV Insulin Drip
Mix Drip with 125 units Regular Insulin into
250 cc NS Starting Rate Units / hour = (BG – 60) x 0.02
where BG is current Blood Glucose
and 0.02 is the multiplier Check glucose every hour and adjust drip Adjust Multiplier to keep in desired glucose
target range (100 to 140 mg/dl)

Continuous Variable Rate IV Insulin Drip
Adjust Multiplier (initially 0.02) to obtain glucose in target range 100 to 140 mg/dL
If BG > 140 mg/dL, increase by 0.01
If BG < 100 mg/dL, decrease by 0.01
If BG 100 to 140 mg/dL, no change in Multiplier
If BG is < 80 mg/dL, Give D50 cc = (100 – BG) x 0.3
Give continuous rate of Glucose in IVF’s
Once eating, continue drip till 1 hour post SQ insulin

Glucose Management System

Glucommander
Based on 15 Year Experience with a Computer Based Algorithm for the Administration of IV Insulin
Developed for Marketing by MiniMed and Roche
GMS System
Shelved Pending FDA Approval of IV Use of Insulin
Useful and Safe for Any Application of IV Insulin


Glucommander Effectiveness
Initial blood glucose
– Median 292 mg/dl
– Range 181-1,568 Time to achieve glucose < 180 mg/dl
– Median 3 hours
– Range 0.3 - 19.7 Time to achieve three consecutive glucose results between 60 - 180
mg/dL
– Median 3. 1 hours
– Range 0.3 - 22.5

Converting to SQ insulin Establish Daily Insulin Requirement
– IV Insulin First Night
– (BG - 60) x Multiplier = Ins/hr Targeted to 120
– 60 x Multiplier x 24 = Daily Insulin Requirement
Give One-Half Amount As Basal
Give p.c. Boluses Based on CHO Intake
– Start at CHO/Ins 1 CHO = 1.5 units Rapid-acting
Monitor a.c. tid, hs, and 3 am
Supplement All BG >150
– (BG-100)/(1700/Daily Insulin Requirement)

Protocol for SQ Insulin in Hospitalized Patient
Bedtime: Wt (kg) x 0.2 = Units of Glargine Meals Eaten: 1.5 units per 15 Gm CHO eaten BG >150: (BG-100) / CF
CF = 3000 / Wt (kg) Do Not Use Sliding Scale Only Any BG <80: D50 = (100-BG) x 0.3 ml
Maintain INT Do Not Hold Insulin When BG Normal

How to Initiate MDI Starting dose = 0.4 to 0.5 x weight in kilograms
Bolus dose (aspart/lispro) = 20% of starting dose at each meal
Basal dose (glargine) = 40% of starting dose given at bedtime or anytime
Correction bolus = (BG - 100)/ Correction Factor, where CF = 1700/total daily dose

How to Initiate MDI
starting dose = 0.45 x wgt. in kg
Wt. is 80 kg; 0.45 x 80 = 36 units
Bolus dose (aspart / lispro) = 20% of starting dose at each meal; 0.2 x 36 = 7 units ac (tid)
Basal dose (glargine) = 40% of starting dose at HS; 0.4 x 36 = 14 units at HS
Correction bolus = (BG - 100)/ CF, where CF = 1700/total daily dose; CF = 50

Correction Bolus Formula
Example:
–Current BG: 250 mg/dl
– Ideal BG: 100 mg/dl
–Glucose Correction Factor: 50 mg/dl
Current BG - Ideal BGGlucose Correction factor
250 - 100 50
=3.0u

Piedmont Diabetes PlanPiedmont Diabetes PlanWhat Can We Do For Patients Admitted To Hospital?What Can We Do For Patients Admitted To Hospital?
NPO Pathway For All Diabetes PatientsNPO Pathway For All Diabetes Patients
Finger Stick BG ac qid on ALL AdmissionsFinger Stick BG ac qid on ALL Admissions
Check All Steroid Treated PatientsCheck All Steroid Treated Patients
Diagnose DiabetesDiagnose Diabetes
FBG >126 mg/dlFBG >126 mg/dl
Any BG >200 mg/dlAny BG >200 mg/dl

Piedmont Diabetes PlanPiedmont Diabetes PlanWhat Can We Do For Patients Admitted To Hospital?What Can We Do For Patients Admitted To Hospital?
Document Diagnosis in ChartDocument Diagnosis in Chart
Hyperglycemia Is Diabetes Until Proven Hyperglycemia Is Diabetes Until Proven
Bring to All Physician’s AttentionBring to All Physician’s Attention
Note on Problem List and Face SheetNote on Problem List and Face Sheet
Check Hemoglobin A1CCheck Hemoglobin A1C
Hold Metformin; Hold TZD with CHF, Liver DysfunctionHold Metformin; Hold TZD with CHF, Liver Dysfunction
Start Insulin in All Hospitalized Patients Not Start Insulin in All Hospitalized Patients Not Already on InsulinAlready on Insulin

Piedmont Diabetes PlanPiedmont Diabetes PlanWhat Can We Do For Patients Admitted To Hospital?What Can We Do For Patients Admitted To Hospital?
Get Diabetes Education ConsultGet Diabetes Education Consult
Instruct Patient in Monitoring and RecordingInstruct Patient in Monitoring and Recording
See That Patient Has Meter on DischargeSee That Patient Has Meter on Discharge
Decide on Case Specific Program for DischargeDecide on Case Specific Program for Discharge
Arrange Early F/U with PCPArrange Early F/U with PCP

Piedmont Diabetes PlanPiedmont Diabetes PlanWhat Can We Do For Patients Admitted To Hospital?What Can We Do For Patients Admitted To Hospital?
Follow Guidelines For Endocrinology ConsultFollow Guidelines For Endocrinology Consult
Any Hypoglycemia Requiring InterventionAny Hypoglycemia Requiring Intervention
DKA or HHNCDKA or HHNC
Patient on Insulin PumpPatient on Insulin Pump
Diabetes in PregnancyDiabetes in Pregnancy
Glucocorticoid Therapy in DiabetesGlucocorticoid Therapy in Diabetes
Progressive Diabetes ComplicationsProgressive Diabetes Complications
A1C >8%, Microalbuminuria >30 mgA1C >8%, Microalbuminuria >30 mg

Treat Any Patient With BG > 150 With InsulinTreat Any Patient With BG > 150 With Insulin
– Treat Any BG >150 with Rapid-acting Insulin Treat Any BG >150 with Rapid-acting Insulin (BG-100) / (5000 / wt #) or (3000 / wt kg) (BG-100) / (5000 / wt #) or (3000 / wt kg)
– Treat Any Recurrent BG >200 with IV InsulinTreat Any Recurrent BG >200 with IV Insulin
If More than 0.5 u/hr IV Insulin Required with Normal If More than 0.5 u/hr IV Insulin Required with Normal BG Start Long Acting InsulinBG Start Long Acting Insulin
Protocol for Insulin in Hospitalized PatientProtocol for Insulin in Hospitalized Patient

Protocol for Insulin in Hospitalized PatientProtocol for Insulin in Hospitalized Patient
Daily Total: Pre-Admission or Weight (#) x 0.2 uDaily Total: Pre-Admission or Weight (#) x 0.2 u
– 40 % as Glargine (Basal)40 % as Glargine (Basal)
– 60% as Rapid-acting insulin (Bolus)60% as Rapid-acting insulin (Bolus)
• Give in Proportion to Meal’s CHO EatenGive in Proportion to Meal’s CHO Eaten
BG >150: (BG-100) / CFBG >150: (BG-100) / CF
CF = 5000 / Wt(#) or 3000 / Wt(kg)CF = 5000 / Wt(#) or 3000 / Wt(kg)
Do Not Use Sliding Scale As Only Diabetes Do Not Use Sliding Scale As Only Diabetes ManagementManagement

Protocol for Insulin in Hospitalized PatientProtocol for Insulin in Hospitalized Patient
Treatment of HypoglycemiaTreatment of Hypoglycemia
Any BG <80 mg/dl: D50 = (100-BG) x 0.3 ml IVAny BG <80 mg/dl: D50 = (100-BG) x 0.3 ml IV
Do Not Hold Insulin When BG NormalDo Not Hold Insulin When BG Normal

Diabetes at Piedmont HospitalDiabetes at Piedmont Hospital
ConclusionsConclusions
Any BG >200 mg/dl Is Diabetes (Fasting >126 mg/dl)Any BG >200 mg/dl Is Diabetes (Fasting >126 mg/dl)
Most Diabetes Is Type 2Most Diabetes Is Type 2
All DM patients Must Self-Monitor BG’s and RecordAll DM patients Must Self-Monitor BG’s and Record
No BG >150 mg/dl Should Go UntreatedNo BG >150 mg/dl Should Go Untreated
Most Hospitalized DM [atients Should Be on InsulinMost Hospitalized DM [atients Should Be on Insulin
IV Insulin is Most Effective, Efficient, Safest Rx in Acute Illness IV Insulin is Most Effective, Efficient, Safest Rx in Acute Illness (Glucommander)(Glucommander)

Diabetes at Piedmont HospitalDiabetes at Piedmont HospitalConclusions 2Conclusions 2
Type 2 Diabetics Are Resistant to Insulin ReactionsType 2 Diabetics Are Resistant to Insulin Reactions
Treat Insulin Reactions in Hospital With IV GlucoseTreat Insulin Reactions in Hospital With IV Glucose
Do Not Be Hold Insulin for Normal BG, i.e. 80-120 mg/dlDo Not Be Hold Insulin for Normal BG, i.e. 80-120 mg/dl
A1C Values A1C Values >>7% Indicates Sub-optimal Care7% Indicates Sub-optimal Care

Diabetes at Piedmont HospitalDiabetes at Piedmont HospitalConclusions 3Conclusions 3
Discharge Plan For BG ControlDischarge Plan For BG Control
You Are the Link Between the Best You Are the Link Between the Best Diabetes Care and the PatientDiabetes Care and the Patient
Use Your Diabetes ResourcesUse Your Diabetes Resources
Diabetes Education Center Diabetes Education Center EndocrinologistsEndocrinologists

The Paradigm for the MilleniumThe Paradigm for the MilleniumHyperglycemia: A Mortal SinHyperglycemia: A Mortal Sin
A blood glucose over 200 in a hospitalized patient A blood glucose over 200 in a hospitalized patient causes increased morbidity and mortality.causes increased morbidity and mortality.
In the 21st Century Neglecting a BG >200 Will Be In the 21st Century Neglecting a BG >200 Will Be MalpracticeMalpractice

Conclusion
Intensive therapy is
the best way to treat
patients with diabetes

QUESTIONS
For a copy or viewing of these slides, contact
WWW.adaendo.com














![[XLS] · Web viewAMCR INSTITUTE INC 0000222920 ATLANTA DIABETES ASSOCIATES 0000222921 BANNER HEALTH 0000222922 0000222924 BEND MEMORIAL CLINIC 0000222925 BILLINGS CLINIC DIABETES CENTER](https://static.fdocuments.us/doc/165x107/5aa581c07f8b9a2f048d8046/xls-viewamcr-institute-inc-0000222920-atlanta-diabetes-associates-0000222921-banner.jpg)
