Innovation in the Manufacture ofSalt in Eastern Australia ...

214 POSTGRADUATE MEDICAL JOURNAL April 1950BIBLIOGRAPHY
ALBRIGHT, F., SMITH, P. H., and FRASER, R. (1942), J. Clin.Endocrinology, 2, 37.
ATKINSON, F. R. B. (193I), Brit. J. of Children's Diseases, 28,121.
BAUER, W., and AUB, J. C. (1941), . Clin. Invest., 20, 295.CHUTE, A. L., ROBINSON, G. C., and DONOHUE, W. L.
(I949), . Paediatrics, 34, I.COGGESHALL, C., and ROOT, H. F. (1940), Endocrinology,
26, I.CROOKE, A. C., and CALLOW, R. K. (I939), Quart.7. Med.,
8, 233.CUSHING, H. (1912), 'The Pituitary Body and its Disorders,'
J. B. Lippincott & Co. Philadelphia.CUSHING, H., and DAVIDOFF, L. M. (1927), 'Rockefeller
Institute for Medical Research Monographs,' New York.DAVIDOFF, L. M. (1926), Endocrinology, 10, 461.DAVIS, A. C. (1940), 'Transactions of Amer. Assoc. for Study
of Goitre.ELLINGER, P., HARE, D. C., and SIMPSON, S. L. (I937),
Quart. Y. Med., 6, 241.ELLIS F. (949), Proc. Roy. Soc. Med., 42, 853.FORBES, J. E., GUSTINA, F. G., and POSTOLOFF, A. V.
(I943), Amer. J. Dis. Child., 45, 593.
GO]LDB)ERG, M. B., and LISSER, H. (1942), J. Ciin. Endo-crinology, 2, 477.HURXTHAL, L. M., HARE H. F. E., HORRASE, G., andPOPPEN J. L. (1949) .. Clin. Endocrinology, 9, 126.
JOSEPHSON, B. (1936), Acta. Med. Scand., go, 38s.KINSELL, L. W., MICHAELS, G. D., LI, C. H., and LARSEN
W. E. (1948), J. Clin. Endocrinology, 8, 1013.LI, C. H. (I950), Lancet, , 213.MAINZER, F., and YALAUSIS, E. (I937), Folia Clin. Orient.,
I, 37.McNEE J. W. (95o), Brit. Med. J., I, 113.NORTHFIELD,D . W. C. (949), Proc. Roy. Soc. Med., 42. 84OPPENHEIMER, B. S., and FISHBERG, A. M. (I924), Arch.
Int. Med., 34, 631.SCHRIRE, J., and SHARPEY-SCHAFER, E. P. (1938), Clinical
Science, 3, 413.SCHRIRE, J. (1948), J. Endocrinology (Gt. Britain), 5, 274.SIMPSON, S. L. (1948), 'Major Endocrine Disorders,' Oxford
University Press, London.TURNER, H. H. (1938), Endocrinology, 23 566.WALTERS, W., WILDER, M., and KEPLER, E. J. (1934),
Annals of Surgery Oct. p. 670.YOUNG, F. G. (1937), Lancet, 2, 372.
DIABETES INSIPIDUSBy A. A. G. LEWIS, B.Sc., M.D., M.R.C.P.
Saltwell Research Fellow, the Royal College of PhysiciansFrom the Medical Professorial Unit, The Middlesex Hospital
Thomas Willis, in I682, distinguished betweensaccharine and non-saccharine diabetes. Frank (in1794) defined diabetes insipidus as a long-continued,abnormally-increased secretion of non-saccharineurine, not caused by renal disease. It is nowknown to be due to a failure of water reabsorptionby the renal tubules as the result of an ineffectivelevel of circulating anti-diuretic hormone (ADH).Cases where the renal tubules can be shown to beinsensitive to the action of the hormone occurextremely rarely (Williams, I946).Clinical Picture
Diabetes insipidus may occur at any age, but ismore common in the young. In Jones' series of42 cases (I944), 17 occurred in the first ten years oflife. Males are more often affected thanfemales.The onset is usually insidious, the patient
noticing a tendency to thirst and dryness of themouth, with polyuria and nocturia. There maybe some loss of appetite, and the dryness of themouth may make mastication difficult and foodless appetizing. Loss of weight may occur, thoughsome cases gain. Loss of appetite and exhaustionfrom loss of sleep may lead to emaciation in severecases. Occasionally the appetite is increased.
In a few cases the onset is sudden and dramaticwith intense, unquenchable thlrst and polyuria.These patients may remember for years exactly
when and where their illness began and may saythat the thirst occurred after some particularfood had been eaten. Sometimes a shock or anaccident may be blamed.
In severe cases the thirst is extreme, the patientdeveloping a dry mouth if he abstains from fluidfor more than an hour or so. Very often thethirst seems to be abnormal in quality as well. Itmay be described in dramatic terms, the patientemphasizing the 'burning sensation' in themouth and throat. Sipping water is only a tem-porary palliative however; the patient often feelscompelled to drink a large quantity of water-he feels he must' drain the glass to the dregs' or'get it right down inside.' Water is often pre-ferred to all other fluids and some patients be-come connoisseurs of water, preferring that fromone source to that from another in flavour. Manyfind iced water more satisfying.
Deprived of water, the sufferer may go to anylengths to get fluid, drinking from flower vases,puddles or fountains, or filling his mouth withsnow, or even drinking his own urine. It is notsurprising that some of these patients, constantlytortured by thirst, unable to follow any normaloccupation on account of the polyuria and pre-vented from sleeping for more than an hour or soat a time, should develop neurotic symptoms.Headaches, apathy, weakness, inability to con-centrate, irritability and insomnia may be com-
copyright. on January 8, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.294.214 on 1 April 1950. D
ownloaded from

April 1950 LEWIS: Diabetes Insipidus 25I
plained of, though in some cases these symptomsare probably associated with loss of salt.
In severe cases the urine volume may exceedio litres a day and much higher figures have beenrecorded. Trousseau's famous case passed 43litres in 24 hours. While it is probably true thatthe more severe cases tend to have a more constantoutput of urine, variations do occur from time totime. The day volume is greater than the nightand may be increased by anxiety or reduced in anintercurrent infection. Since the renal tubulescannot concentrate the urine in the absence ofADH, any call for the increased excretion ofosmotically active substances (especially salt andurea) will increase the volume of urine (Beaser,1947).The specific gravity of the urine is always low,
usually below o005. The significance of thevariations in urine volume and specific gravitywhich occur with fluid restriction will be discussedlater.
Diabetes insipidus is a symptom complex andthe underlying cause must be carefully sought.Hyperparathyroidism should be remembered asan occasional cause of polyuria.The Anti-Diuretic Hormone
This is formed by the neurohypophysis. It isgenerally believed to be identical with vasopressin,and it is doubtful whether this has any otheraction normally in the body, though Heller (1940)has reported separating the anti-diuretic from thepressor effect. Pitressin is the proprietary namegiven to a preparation of vasopressin which is saidto be practically free of the oxytocic factor.The hormone can be adsorbed and inactivated
by blood and tissue extracts. It is probably re-moved from the blood stream partly by destructionin the liver and, to a lesser extent, by excretion inthe urine, in which it can be assayed by suitabletechniques (Bur, 1931; Heller and Urban, I935;Grollman and Woods, 1949). In cirrhosis of theliver it has been suggested that slow destruction ofthe hormone may be partly responsible for waterretention (Ralli, et al., I945).The NeurohypophysisThe terminology introduced by Rioch, Wislocki
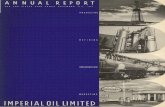
and O'Leary (I940) for the more accurate descrip-tion of the pituitary gland is now being generallyadopted. The gland is divided into adeno-hypophysis and neurohypophysis, the latter con-sisting of the median eminence of the tubercinereum, the infundibular stem and the in-fundibular process, which together form, histo-logically and functionally, a single unit (see fig.).A dense bundle of unmyelinated fibres (the supra-
:) ... PARAVENTRICULAR.' NUCLEUS
NCLEUS MAMILLAY
OPTIC
supraoptico-hypophysial tracts in man.
CHIASMA P E W\ INFUNDIBULAR STEM
TUBERCINEREM \
IFWUNDIWULARPROCESS
ADENOHYPOPHYSIS
Diagrammatic representation of the course of thesupraoptico-hypophysial tracts in man.
(Drawn bi' Professor E. W. Walls.)
optico-hypophysial tract) passes from the supra-optic nucleus in the hypothalamus, with somefibres from the paraventricular nucleus, to theneurohypophysis. The mode of termination ofthese fibres is uncertain. It is thought that thepituicytes, large glial cells found throughout theneurohypophysis, may actually elaborate the hor-mone. They degenerate after section of thesupraoptico-hypophysial tracts, and retrograde de-generation occurs in the two hypothalamic nuclei.
The von Hann Theory (x918)In spite of the fact that posterior pituitary ex-
tracts were shown to control the polyuria ofdiabetes insipidus in 1913, the role of the hypo-thalamus and of the anterior lobe remained indispute for many years. In I9I8 von Hann firstreconciled the conflicting results of animal ex-periments, suggesting that some continued func-tion of the anterior lobe, in the absence of thesecretion of the posterior lobe, was necessary forthe maintenance of the polyuria. Complete hypo-physectomy does not lead to diabetes insipidus,nor, clinically, does Simmond's disease, in whichthe water exchange is reduced. Exactly how theanterior lobe is responsible for this is not known.It may produce an actively diuretic principle, butit seems more likely that it is the maintenance ofnormal metabolism and activity, by the thyroidand the adrenals, that is essential. Thus thyroid-ectomy greatly reduces the severity of the polyuriain diabetes insipidus, and there is a failure of thenormal response to the ingestion of water inadrenal insufficiency. This has been further in-vestigated in dogs by Pickford and Ritchie (I945).
copyright. on January 8, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.294.214 on 1 April 1950. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
The HypothalamusThe confusion as to the role of the hypothalamus
in the causation of diabetes insipidus was finallyended by the work of Fisher, Ingram and Ranson(1938) who conclusively proved that bilateral in-terruption of the supraoptico-hypophysial tractsproduces the disease in the cat and monkey. Noother lesion has consistently been shown to do this.Nearly complete destruction of the gland or tractsis necessary to produce diabetes insipidus; in thecat subtotal lesions produce less severe degrees ofthe disease. This appears to be true in man also.A temporary phase of polyuria and a brief normalinterval occur before the polyuria becomes per-manently established.
The Normal Processes of Urine FormationThe nephrons elaborate urine by a process of
glomerular filtration, followed by the reabsorptionof the greater part of this filtrate by the tubules.In a normal man about I,ooo to I,400 cc. of bloodflow through the kidneys per minute, the glomerulifiltering off I30 cc. of plasma water with its dis-solved crystalloids. Of this, more than I00 cc. arealways reabsorbed, probably in the proximal halfof the tubule (Smith, I947). It is believed that thefinal concentration of the urine takes place in thedistal tubule (probably mainly in the thin segmentof Henle's loop) where varying quantities of waterare reabsorbed under the control of ADH re-leased into the blood stream by the neuro-hypophysis.Under ordinary conditions the glomerular
filtration rate (measured by the inulin or sodiumthiosulphate clearances) remains remarkably con-stant and variations in the rate of urine flow arethought to be effected by varying blood levels ofADH, to which the renal tubules are extremelysensitive. Secretion of urine ceases if theglomerular filtration rate falls to very low levels(as with very low arterial pressures) and at veryhigh rates of urine flow the filtration rate rises,possibly from dilution of the plasma proteins bythe large water load ingested. Between these ex-tremes, however, there is no evidence that varia-tions in renal blood flow or glomerular filtrationrate affect the urine flow. It is possible thatADH, by acting on the glomerular arterioles, mayproduce small changes in the filtration rate butthese probably play no part in its essential action.The greater the tubular reabsorption of water
the more concentrated does the urine become. Itsspecific gravity and osmotic pressure rise, thoughnot all the constituents are equally affected. Moreurea is reabsorbed for instance (this is probably aprocess of passive back-diffusion) so that less ureais removed from the blood per minute at low ratesof urine flow (that is, the urea clearance falls). On
the other hand, the concentration of chloride inthe urine rises until it reaches a maximum of about1,200 mg. per cent. (as CI), which implies thatfor every cc. of water reabsorbed less chloridepasses back. This appears to be the specificeffect of the hormone but it is often said that itincreases the output of chloride by the humankidney. This question has recently been furtherinvestigated and it has been shown that in normalmen the hormone increases the concentration ofchloride in the urine leaving the minute output un-changed, or reducing it slightly (Chalmers, Lewisand Pawan, 1950). There is in fact no evidencethat ADH has any other action in normal menthan to stimulate the renal tubule to reabsorb morewater. The factor that limits the tubular re-absorption of water, and therefore determines theminimum urine flow that can occur under theaction of ADH, appears to be the total osmoticpressure exerted by the urine solutes.
Suggestions that the posterior pituitary hor-mones might have other actions, e.g. on a hypo-thetical water regulating centre in the mid-brain or hypothalamus, on the hydration of thetissues or on the osmotic pressure of the plasmaproteins are not supported by the evidence.
Renal function has been investigated in diabetesinsipidus by Winer (1942) who found the filtrationrate to be normal before and after treatment withpituitrin, though there was a sharp, temporary de-crease just after the injection.Factors Influencing the Production of ADH(Pickford, 1945; O'Connor, I947)
Claude Bernard showed that emotion could in-hibit the flow of urine. Emotional changes seem tobe responsible for the release of ADH broughtabout by exercise (Rydin and Verney, I938) and bypain (Kelsall, 1949). Various sensory stimuli willinhibit a water diuresis in animals, and thestimulus can be so conditioned that the inhibitioncan be produced by the mere preparation of theanimal for the experiment, or even by a musicalnote. In man, a water diuresis can be initiated bysuggestion under hypnosis (Marx, 1926).
Pickford (I947) has shown that acetylcholinewill cause the release of ADH in the dog when in-jected into the supraoptic nucleus, and Burn,Truelove and Bur (I945) showed that in manintravenous injections of nicotine, or smokingcigarettes, will do so (Walker, I949). Estimationsof the inulin clearance in this laboratory haveshown that this is due to increased tubular re-absorption of water.
Dehydration appears to be the 'normal'stimulus increasing the output of hormone. Ithas frequently been shown that the urine of de-hydrated animals contains an anti-diuretic sub-
2I6 April I950copyright.
on January 8, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.294.214 on 1 A
pril 1950. Dow
nloaded from

LEWIS: Diabetes Insipidus
stance. This disappears after destruction of thesupraoptico-hypophysial tracts. (These resultsshould not all be accepted without reserve. Otheranti-diuretic substances might be present inurine, and the methods of assay have not alwaysbeen above criticism. As an example, the urine ofsmokers contains nicotine, which will inhibit awater diuresis when injected into rats unless careis taken to remove it.)
It is this stimulus that has been so fully in-vestigated by Verney and his co-workers at Cam-bridge (Verney, 1946). They have shown in dogsthat it is the osmotic pressure exerted by some ofthe plasma crystalloids which controls the releaseof the hormone. Changes can be brought about,with subsequent inhibition of a water diuresis,by injections of hypertonic solutions into thecommon carotid artery, and the amount liberatedcan be estimated by comparing the duration ofinhibition with that produced by injecting aknown quantity of hormone. Changes in theosmotic pressure of the carotid blood of about 2per cent. are effective. Verney believes thatspecial ' osmoreceptors' are responsible for con-trolling the output of ADH from moment tomoment, and has very tentatively suggested thatthe small vesicles which can be seen in sectionsthrough the supraoptic nucleus may be the re-ceptors themselves. According to Verney, a waterdiuresis only occurs when, following the ingestionof water, dilution of the blood leads to the cessa-tion of the activity of the osmoreceptors (' physio-logical diabetes insipidus '). There is a time lagof some 15 minutes after the peak of the waterload before the maximum rate of urine flow isattained, presumably because this is the time takenfor the circulating hormone to be removed orinactivated.
Thirst in Diabetes InsipidusThere is no doubt that this experimental work
offers a very convincing explanation of the natureof the clinical condition, and there might seem tobe little room for further argument. It deals,however, solely with the factors controlling wateroutput and only indirectly with that sensationwhich must ultimately regulate the organism'swater exchange, namely, thirst. If water loss didnot rapidly lead to thirst and the ingestion of water,death would soon follow, while diabetes insipidus,as defined above, would certainly be the result ifsome prolonged and abnormal increase in thirstwere to occur.The problem of thirst has been discussed by
'Gregersen (I94I). The older view is that it is asensation arising centrally, from changes in thehydration of the tissues. Cannon suggested thatit is purely local in origin, arising from dryness of
the mouth and throat. If this were true, extirpa-tion of the salivary glands should lead to increaseddrinking, but Montgomery (I931) found that thisdid not follow in dogs. Gregersen and Cannon(1932) repeated this work, drying the buccalmucosa as well by exposing it to warm air, buteven then the dogs only drank twice as much asbefore. Cannon found that atropine made himthirsty when it made his mouth dry: most peoplewho have tried this would probably say that thedryness leads to a desire to wet the mouth, not todrink large quantities of water. Nervous womenwith xerostomia, or patients with ureo-parotidtuberculosis or with Sj6gren's syndrome (Ellmanand Parkes Weber, I949) do not develop diabetesinsipidus, though they may drink more often thanother people.
Gilman (I937) has suggested that thirst is theresult of the loss of intracellular fluid, which is theolder view in modern terminology, and this doesnot seem inconsistent with the known facts. Itwould explain why thirst should occur afterhaemorrhage, which reduces the extracellular fluidvolume, and after infusions of hypertonic saline,which increase it. It seems probable that thirstarises from intracellular dehydration, while extra-cellular fluid loss, by reducing the blood flowthrough the salivary glands (Gregersen), reducesthe salivary flow. Usually, of course, the twooccur together.Holmes and Gregersen (1948) investigated the
origin of the thirst in diabetes insipidus by study-ing the weight, thirst, salivary flow, plasmavolume, ' thiocyanate available fluid' and plasmaproteins and sodium in five cases under three setsof conditions: (I) when fluids were allowed ad lib.(2) when pitressin was given to control thepolyuria, and (3) when fluids were forced untilthirst disappeared and the salivary flow approachedthat observed in period (2). In the last twoperiods, compared with the first, changes wereconsistently observed identical with those foundin dehydrated men after the ingestion of water-the weight, salivary flow, plasma volume and'thiocyanate space' rose, while the plasma pro-teins and sodium fell. They believed thatCannon's theory of thirst could be applied todiabetes insipidus, the dehydration leading to adry mouth and so to thirst. These results do notrule out the possibility of over-hydration inperiods (2) and (3), as no figures for normalestimations are given. They believed this wasexcluded since pitressin and forced fluids will notincrease the salivary flow in normally hydratedmen. Theobald (I934), however, found that if awater diuresis in a hydrated dog were inhibited bypituitrin, excessive salivation did occur. Thatpitressin can lead to chronic over-hydration is
April I950 217copyright.
on January 8, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.294.214 on 1 A
pril 1950. Dow
nloaded from

POSTGRADUATE MEDICAL JOURNAL
shown by the results of fluid restriction in a casereported recently at the Royal Society of Medicine(Lewis, Ward and Bishop, I949). Fluids were re-stricted on two occasions, once after daily dosesof pitressin or pituitrin snuff and once four cleardays after any treatment had been given. On thefirst occasion, in the course of the 12 hours thatfollowed the end of the anti-diuresis produced bythe last dose of pituitrin, nearly 5 litres of fluidwere lost, yet the urine flow remained above 5 cc.per minute and the specific gravity was less thanI005' On the second occasion 19 hours' de-privation reduced the urine flow to less than i cc.per minute with a specific gravity of Io1o.5, inspite of a total loss of less than 3 litres of fluid.The mouth was not really dry on either occasion,though thirst was great (see also Thorn and Stein,I941).The Role of PolydipsiaThe view that thirst is the cause and not the
result of diabetes insipidus, in spite of the im-pressive weight of evidence to the contrary, cannotbe lightly dismissed. This was certainly theopinion of many of the older clinicians, who con-sidered the disease as psychopathic in origin orreferred to it as 'nervous polyuria.' Later,hysterical thirst was considered in France to be aseparate condition and was termed ' potomanie.'Cushny (1926) and Cushing (I932) both suggestedthat the polydipsia was primary. Many patientsare absolutely convinced that their thirst beganbefore their polyuria, and there are several casereports in the literature (Nothnagel, I88I;Futcher, I904; Kennaway and Mottram, I9I9;Weir, Larson and Rowntree, 1922; Kourilsky,1947). In Dandy's case (1940), the pituitary stalkwas deliberately cut at operation: thirst appearedsoon after the return of consciousness and wasquickly followed by a very high output of urine.The water intake greatly exceeded the urinevolume for ten days.
Other clinical evidence sometimes advanced tosupport the theory of primary polydipsia is per-haps less convincing. Patients will often maintainthat injections of pituitrin relieve their thirst veryrapidly, long before much effect on body hydrationcould have occurred, or declare that pituitrinpromptly increases their salivation. Both theseeffects may be psychological, however, and evencontrol water injections may not decide this, forpatients can sometimes tell from bladder sensationswhen the injection' begins to work.'
Experimental evidence in favour of the theory ofpolydipsia was given by Bailey and Bremer (I921)who believed that polydipsia and polyuria occurredsimultaneously and independently, by Curtis(1924) and by Swann (i939). These findings have
been criticized by Fisher, Ingram and Ranson(I938). Bellows and van Wagenen (1938) repeatedan earlier experiment of Claude Bernard, makingoesophageal fistulas in dogs so that the water in-take could be completely dissociated from the out-put, the dogs being given a measured quantity offluid into the lower end of the oesophagus.Diabetes insipidus was then produced by bperationon the hypothalamus or pituitary. In the tem-porary phase a marked polydipsia occurred, withpolyuria only on the first day. In the permanentphase polydipsia was the sole abnormality, thedogs suffering no ill effects from losing, throughthe fistula, all the excess water drunk. If theywere given more water into the stomach, thepolydipsia was reduced but not abolished. Thedogs could, however, pass a fairly concentratedurine. Though there was no obvious evidence ofdehydration, there may have been sufficient tostimulate both the thirst and the production ofADH from some residual tissue. The findings inDandy's case might be explained along similarlines, for there may have been a greatly increasedextra-renal fluid loss following the operation.The view that there might be two types of
diabetes insipidus was put forward by Veil (I9I6).He believed that polydipsic and polyuric formsexisted, but his final division was into hypo-chloraemic and hyperchloraemic types. In France,Veil's earlier view has been greatly extended byKourilsky (I947) who has studied the effects ofprolonged fluid deprivation on 30 patients. Hedivided them into:--(I) Pure polydipsia: fivecases. The urine is reduced in volume andnormally concentrated if the fluid deprivation isprolonged. The symptoms and signs arise fromexcessive water ingestion (see below). Twoshowed a normal hypothalamo-hypophysial systemat necropsy (Roussy, Kourilsky and Mosinger,I946). (2)Pure polyuria: six cases. This corres-ponds in every respect to the disease produced incats by Fisher, Ingram and Ranson. There isconstant polyuria of low specific gravity, littleaffected by fluid restriction, the gravity remainingbelow IOIO even when a fluid deficit of 3 litreshas developed. Dehydration and haemocon-centration occur. (3) Mixed forms: 19 cases.These may be due to partial lesions of the neuro-hypophysis. Here the urine volume and specificgravity can be influenced to some extent by theintake, but the thirst seems to be the dominantsymptom and the effects of excessive fluid intakecomplicate the picture.The effects of excessive water drinking have
been studied by Veil and by Kourilsky, the latteremphasizing that different changes in the bloodchemistry occur in different subjects. Kunst-mann, for example, in 1933 drank between IO and
2I8 April 1950copyright.
on January 8, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.294.214 on 1 A
pril 1950. Dow
nloaded from

LEWIS: Diabetes Insipidus
I8 litres a day for 127 days. After the first eightdays there was an active desire for water and he hadto drink during the night, even if he had done sobefore retiring. If water was not drunk, drynessof the mouth and difficulty in mastication occurred.His weight remained constant and the plasmachloride rose in spite of a negative chloridebalance. At the end of the experiment he hadgreat difficulty in reducing his water intake. It is,of course, well known that continuous drinkinghas a dehydrating effect (Wolf, I945; see alsothe references to earlier literature by Schemm,I944, who based his treatment of oedema on thisprinciple). This may be due to loss of sodiumand of extra cellular fluid. It is difficult to believethat Kunstmann was dehydrated during this ex-periment, as his weight remained constant. Therise in plasma chloride, with a negative chloridebalance, indicates a marked loss of extra cellularwater, which might have reduced the salivary flow.
Kourilsky maintains that the polydipsia in hiscases was not a hysterical manifestation, though hedoes not deny the existence of' potomanie.' Thisis bound to be the subject of controversy, thoughrecent additions to our knowledge of the controlof autonomic functions by specific cortical areasmake this view seem less improbable than itwould have done a few years ago. One of hiscases was a young girl with a subarachnoid cystwhich was stretching the pituitary stalk. Whilethis was being aspirated she suddenly exclaimedthat her thirst had gone. This resembles resultssometimes produced by leucotomy.Whether or not it is accepted that pathological
thirst may be the result of lesions elsewhere than inthe neuro-hypophysis or may arise from its partialdestruction, the experiments of Kunstmannand others show that the excessive ingestion ofwater can produce a symptom complex identicalwith diabetes insipidus.Diagnostic TestsThe tendency in Britain and America has been
to divide these cases into two groups-diabetesinsipidus and 'psychogenic polydipsia.' Carterand Robbins (1947) suggested that a rapid intra-venous infusion of hypertonic saline, after pre-liminary hydration, will reduce the urine flow inthe second group. This begs the question of theorigin of the polydipsia, but they claim that thethree cases so diagnosed were freed of theirsymptoms by psychotherapy.
Prolonged restriction of fluid is the usualdiagnostic procedure. Sucking small pieces of iceor decicaine lozenges makes the ordeal moretolerable, but the patient will still complain ofthirst. Severe cases become obviously dehydratedin a few hours, with little rise in the urinary
specific gravity or fall in the urine flow. Thegravity never exceeds ioio and rarely reaches eventhis figure. Cases of polydipsia will be able toform a much more concentrated urine without anysigns of dehydration, though the urine flow falls tomuch lower levels than in the first group and thetest may therefore have to be prolonged for morethan 24 hours. There remains a number of inter-mediate cases where there is probably sufficienthypophysial function left to form small amounts ofADH when dehydration is moderate; in thesethere may be a rise of urinary specific gravityabove ioio when some litres of fluid have beenlost. The thirst and dryness of the mouth maybe misleading indications of the degree of de-hydration, as noted earlier. It is the urine flowand specific gravity considered against the fluiddeficit that are of diagnostic importance.
Nicotine may also be valuable as a diagnosticaid. In the case previously referred to (Lewis,Ward and Bishop, I950) there was no response tohypertonic saline but smoking a cigarette pro-duced a marked anti-diuresis. Further work onthis test is now in progress in this unit.
Lesions Associated with Diabetes InsipidusCases occur where other signs of damage to the
hypothalamus are present-emotional changes,adiposo-genital dystrophy, impotence, dis-turbances of sleep or of sweating and diabetesmellitus. The polyuria found in acromegaly maysometimes be due to pressure on the neuro-hypophysis by the enlargement in the anteriorlobe.These symptoms are the exception, however,
and in the majority of cases diabetes insipidus is anisolated finding.
Fink (1928) analysed 107 post-mortem reportsof cases with diabetes insipidus. In 63 per cent.there was a tumour at the base or in the posteriorfossa, in 13 per cent. basal syphilitic meningitis orgumma, in 6 per cent. tuberculous meningitis or atuberculoma and in 8 per cent. some other in-flammatory process in this area, while in io percent. trauma was responsible.
Jones (1944) reviewed the records of 42 casestreated in the University of Michigan Hospitalbetween 1926 and 1943. Tumours involved thepituitary gland in 11; one was a medulloblastoma,four were cystic adamantinomas and the otherssecondary deposits. There was a tumour involv-ing the hypothalamus in two. Four suffered fromHand-Schiiller-Christian disease, seven fromchronic encephalitis, three from syphilis, threefrom the effects of head injury and three possiblyfrom the results of vascular accidents. No causecould be found in eight, which were classed as' idiopathic.'
April 1950 219copyright.
on January 8, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.26.294.214 on 1 A
pril 1950. Dow
nloaded from

220 POSTGRADUATE MEDICAL JOURNAL April 1950
Kourilsky (I947) has emphasized the importanceof upper respiratory tract infections as a cause, andcases following sphenoidal sinusitis have been re-ported (Yaskin, Lewey and Schwarz, 1942;Ball and Thackray, 1948).
Bollack, et al. (i937), found 15 cases of diabetesinsipidus among 129 of chiasmal arachnoiditis.Sinusitis or rhinitis were noted in 15 of the latter.
Colover (1948), reviewing the reports of II5cases of sarcoidosis involving the central nervoussystem, states that polydipsia and polyuria werepresent in 20. Several showed other. symptomsdue to lesions of the hypothalamus.
Porter and Miller (1948) have reviewed thecases occurring at the Head Injury Centre atOxford. They reported I8 cases, 13 occurring in5,ooo admissions with non-fatal closed head in-juries. The majority had severe injuries withmore than seven days' post-traumatic amnesia.Symptoms were noticed between the ninth andthirty-first day after the injury. Of the I8 cases,only 12 had fractured skulls and these were notall basal. 'Eleven cases recovered within ninemonths.Warkany and Mitchell (1939) have reviewed
the condition in childhood.Blotner (1942) and Williams (1946) have re-
ported families with hereditary diabetes insipidus.Idiopathic Diabetes InsipidusThe diagnosis of this condition calls for an ex-
tremely detailed case history and clinical examina-tion, with X-rays of the skull and sinuses, lumbarpuncture and perhaps encephalography to deter-mine the underlying condition. In a small num-ber, no evidence of one will be .found and theseare usually termed 'idiopathic.' A progressivelesion may declare itself even in some of theseafter time has elapsed. A primary growth wasfound in one of Jones' cases six years after theonset of polyuria, and in this unit a case hasrecently been seen to develop papilloedema afterseven years. It has even been suggested (Bern-stein, Moore and Fishback, 1938) that 'idio-pathic' cases should be given deep X-ray therapyto the pituitary area on an empirical basis.
Isolated lesions destroying the supraopticnuclei have been reported (Baker and Craft, I940)
and it is possible that some cases have a selectivedegeneration of the supraoptico - hypophysialtracts.The number of cases for which no cause at all
can be found at any time must be comparativelysmall. A few of these may be found to be re-sistant to pitressin. The remainder probably in-cludes those cases described by Kourilskv aspure polydipsias,l if it is indeed the case that they
are not wholly psychological in origin.Treatment
Apart from the treatment of the underlyingcondition, the polyuria can be controlled by re-placement therapy.
Implantations of pellets and grafts of animalglands have been made, but have been un-successful.
Injections of posterior pituitary extracts willcontrol the polyuria in the majority of cases, butthis effect only lasts for a few hours. Occasionallythey cause such unpleasant sensations, particu-larly abdominal cramps, that they have to beabandoned.
Intramuscular injection of pitressin tannate inoil, which delays the absorption, is usually muchmore successful. Many patients need only i or2 cc. every two or three days and unpleasant sideeffects are fewer (Court and Taylor, I943).
Nasal insufflations of the dried gland are alsoeffective for short periods. Patients can take apinch of this snuff when they need to control thepolyuria for a few hours and can judge the quantitywithout having to measure it accurately, or theymay prefer to have it measured out in capsules.Some find it too irritating to the mucousmembrane.
Thyroidectomy has been recommended, par-ticularly for those cases associated with post-encephalitic Parkinsonism (Blotner and Cutler,I941). Thiouracil was given to one ' idiopathic'case in the Middlesex Hospital by Dr. K. P. Ball,but without effect.
Restriction of salt and protein in the diet willreduce the polyuria and increase the effectivenessof pituitary extracts, but it must not be forgottenthat salt deficiency may occur and be responsiblefor some of the symptoms in untreated cases.
BIBLI:;OG:RAPHY
BAILEY, P., and BREMER, F. (I921), Arch. Int. Med., 28, 773.BAKER, A. B., and CRAFT, C. B. (1940), Endocrinology, 26, 8ox.BALL, K. P., and THACKRAY, A. C. (1948), Lancet, I, 637.BEASER, S. B. (I947), Amer. J. Med. Sci., 213, 441.BELLOWS, R., and Van WAGENEN, W. P. (1938), J. Nerv.
Ment. Dis., 88, 417.BERNSTEIN, M., MOORE, M. T., and FISHBACK, D. B.
(1938), Arch. Ijt. Med., 62, 604.BLOTNER, H. (1942), Amer. J. Med. Sd., 204, 261.
BLOTNER, H., and CUTLER, E. C. (I941), J. Amer. Med. Ass.,ir6, 2739.
BOLLACK, J., DAVID, M., and PUECH, P. (I937), 'Lesarachnoidites optochiasmatiques,' Paris.
BURN, J. H. (I931), Quart. J. Pharm., 4, 57.BURN, J. H., TRUELOVE, L. H., and BURN, I. (I945), Brit.
Med. Y., I, 403.CANNON, W. B. (19I8), Proc. Roy. Soc. B., 90, 283.CARTER, A. C., and ROBBINS, J. (1947), J. Clin. Endo., 7,752.
copyright. on January 8, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.294.214 on 1 April 1950. D
ownloaded from

April 1950 LEWIS: Diabetes Insipidus 221
CHALMERS, T. M., LEWIS, A. A. G., and PAWAN, G. L.( 95o), Y. Physiol. (in press).
COLOVER, J. (I948), Brain, 71, 45I.COUTT, D., and TAYLOR, S. (1943), Lancet, I, 265.CURTIS, G. M. (1921), Arch. Int. Med., 34, 8oi.CUSHING, H. (1932), 'Papers relating to the Pituitary Body,
Hypothalamus and Parasympathetic Nervous System,'Charles C. Thomas, Springfield.
CUSHNY, A. R. (I926), ' The Secretion of the Urine,' Longman'sGreen & Co., London.
DANDY, W. E. (I940), J. Amer. Med. Ass., 114, 3I2.ELLMAN. P., and PARKES WEBER. F. (I949), Brit. Med. J.,
1, 304.FINK, E. B. (1928), Arch. Path., 6, Io2.FISHER, C., INGRAM, W. R., and RANSON, S. W. (1938),
'Diabetes Insipidus and the Neuro-Hormonal Control ofWater Balance,' Edwards Bros., Ann. Arbor.
FUTCHER, T. B. (I904), Tr. A. Amer. Physicians, 19, 247.GILMAN, A. (I937), Amer. J. Physiol., 120, 323.GREGERSEN, M. I. (I94I), in Macleod's 'Physiology in Modern
Medicine,' 9th edition, Henry Kimpton, London.GREGERSEN, M. I., and CANNON, W. B. (I932), Amer. J.
Physiol., o02, 336.GROLLMAN, A., and WOODS, B. (1949), Endocrinology, 44, 409.VON HANN, F. (I918), Ztschr. f. Path., 21, 337.HELLER, H., and URBAN, F. (1935), J. Physiol., 85, 502.HOLMES, J. H., and GREGERSEN, M. (1948), Amer. J. Med.,
4, 503.JONES, G. M. (1944), Arch. Int. Med., 74, 8I.KELSALL, A. R. (1949), J. Physiol., 109, 150.KENNAWAY, E. L., and MOTTRAM, J. C. (1919), Quart. J.
Med., 12, 225.KOURILSKY, R. (I947), Ann. Med., 48, 288.KUNSTMANN, R. (1933), Arch. J Erp. Path., 170, 701.LEWIS, A. A. G., WARD, C. S., and BISHOP, P. M. F. (1950),
J. Endocrinol. (in press).
MARX, H. (1926), Klin. Wchnschr., 5, 92MONTGOMERY, M. (193I), Amer. J. Physiol., 96,'221.NOTHNAGEL, H. (1887), Virchow's Arch., 86, 435.O'CONNOR, W. J. (I947), Biol. Rev., 22, 30.PICKFORD, M. (1945), Physiol. Rev., 25, 573.PICKFORD, M. (I947), .. Physiol., xo6, 264.PICKFORD, M., and RITCHIE, A. E. (1945), J. Physiol., 04,.
o05.PORTER, R. J., and MILLER, R. A. (1948), 7. Neurol., Neurosurg.
and Psychiat., I,, 258.RALLI, E., ROBSON, J. G., CLARK, D., and HOAGLAND,
C. L. (I945), J. Clin. Invest., 24, 316.RIOCH, D., WISLOCKI, G. B., and O'LEARY, J. L. (1940),
Res. Publ. Ass. Nerv. Ment. Dis., 20, 3.ROUSSY, G., KOURILSKY, R., and MOSINGER, M. (I946),
Rev. Neurol., 78, 313.RYDIN, H., and VERNEY, E. B. (1938), Quart. J. exper. Physiol.,
27, 343.SCHEMM, F. R. (1944), Ann. Int. Med., 21, 937.SMITH, HOMER W. (1947), Bull. N.Y. Acad. Med., 23, I77.SWANN, H. G. (1939), Endocrinology, 25, 288.THEOBALD, G. W. (1934), J. Physiol., 81, 243.THORN, G. W., and STEIN, K. E. (I941), .7 Clin. Endoc., I,.
680.VEIL, R. (I916), Deutch. Arch. f. Klin. Med., 119, 376.VERNEY, E. B. (1946), Lancet, 2, 739 and 781.WALKER, J. M. (I949), Quart. J. Med., I8, 5I.WARKANY, J., and MITCHELL, A. G. (1939), Amer. J. Dis.
Child., 57, 603.WEIR, J. F., LARSON, E. E., and ROWNTREE, L. G. (1922),Arch. Int. Med., 29, 306.WILLIAMS, R. H. (1946), J. Clin. Invest., 25, 937.WINER, N. J. (1942), Arch. Int. Med., 70, 6I.WOLF, A. V. (1945), Amer. J. Physiol., 143, 567.YASKIN, J. C., LEWEY, F. H., and SCHWARZ, G. (1942),Arch. Neurol. and Psychiat., 48, 19.
*NUN-----RNRRUMENMEMRMuU MNE Nn mmuERREMNEN
Ribena is bemg increasingly prescribed in the treatment ofPeptic Ulcer because controlled clinical tests have clearlyW indicated that natural vitamin C, in the form of black-currant syrup, accelerated disappearance of symptoms and
q X-ray evidence of ulcer. Detailed information on this workwill be gladly sent to physicians.bena Ribena is the pure undiluted juice of fresh ripe black-currants with sugar, in the form of a delicious syrup. Beingfreed from all cellular structure of the fruit, it will not upsetthe most delicate stomach. It is particularly rich in naturalvitamin C (not less than 20 mgm. per fluid ounce) andassociated factors.
PepticUlcer? NIGIABLACKCURRANT SYRUP
H. W. Carter & Co. Ltd. (Dept. 5.K), The Royal Forest Factory, Coleford, GlosEire.-Inquiries should be addressed to Proprietaries (Eire) Ltd.,I7/22, Parkgate Street, Dublin.
EKE ME*n ME3 EEEEEEEEMEEMEM *************EE***EM***********EE****»E»«
copyright. on January 8, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.294.214 on 1 April 1950. D
ownloaded from