
Diabetes in Pregnancy - UCSF CME
23
4/12/2018 1 Diabetes in Pregnancy Ingrid Block-Kurbisch, MD, Associate Clinical Professor of Medicine Associate Physician, OB/GYN, UCSF April 12, 2018 Disclosures I have nothing to disclose
Transcript of Diabetes in Pregnancy - UCSF CME
4/12/2018
1
Diabetes in Pregnancy
Ingrid Block-Kurbisch, MD,
Associate Clinical Professor of Medicine
Associate Physician, OB/GYN, UCSF
April 12, 2018
Disclosures
I have nothing to disclose
4/12/2018
2
Objectives
Definitions: GDM, Pre-GDM 1 & 2
Epidemiology
Implications of GDM and PEDM on outcomes
Pre-conception Care
Populations at high risks for adverse outcomes
Screening for GDM
Treatment and questions about oral agents
Monitoring
Delivery planning
Post-conception Care
Definitions
Hyperglycemia first detected in pregnancy:
- Gestational DM (GDM)
- Diabetes in pregnancy (DIP)
Pre-gestational DM (PEDM):
- Type 1
- Type 2
- Other (Monogenic DM, CF, other)
GDM
- A1GDM: diet controlled
- A2GDM: medication + Diet controlled
4/12/2018
3
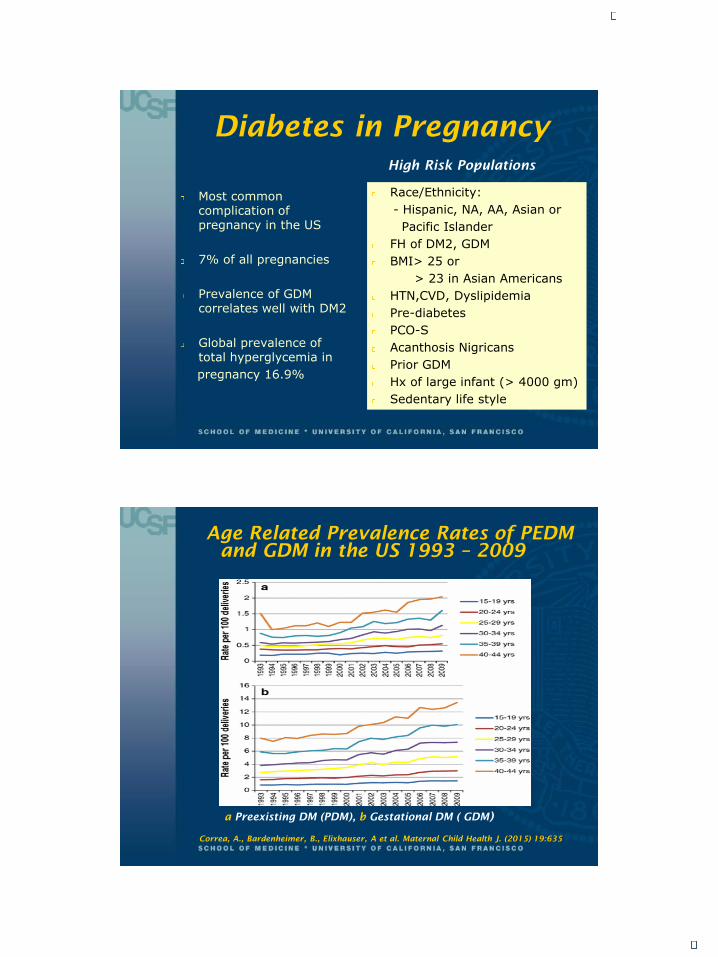
Diabetes in Pregnancy
Most common complication of pregnancy in the US
7% of all pregnancies
Prevalence of GDM correlates well with DM2
Global prevalence of total hyperglycemia in
pregnancy 16.9%
Race/Ethnicity:
- Hispanic, NA, AA, Asian or
Pacific Islander
FH of DM2, GDM
BMI> 25 or
> 23 in Asian Americans
HTN,CVD, Dyslipidemia
Pre-diabetes
PCO-S
Acanthosis Nigricans
Prior GDM
Hx of large infant (> 4000 gm)
Sedentary life style
High Risk Populations
Age Related Prevalence Rates of PEDM
and GDM in the US 1993 – 2009
a Preexisting DM (PDM), b Gestational DM ( GDM)
Correa, A., Bardenheimer, B., Elixhauser, A et al. Maternal Child Health J. (2015) 19:635
4/12/2018
4
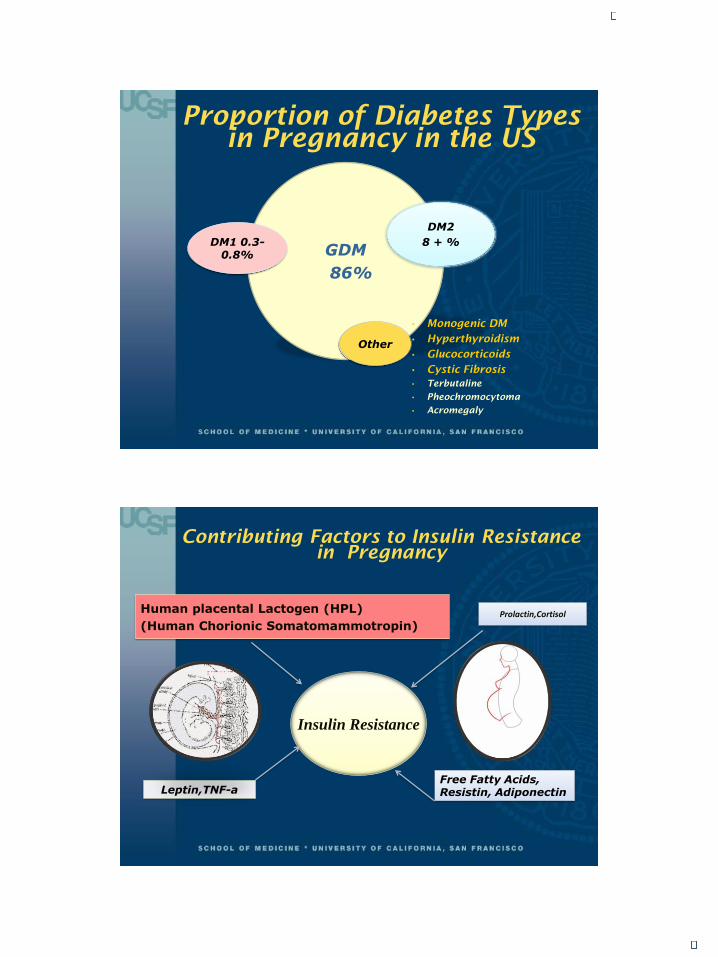
Proportion of Diabetes Types
in Pregnancy in the US
GDM
86%
DM1 0.3-0.8%
DM2
8 + %
Other
• Monogenic DM
• Hyperthyroidism
• Glucocorticoids
• Cystic Fibrosis
• Terbutaline
• Pheochromocytoma
• Acromegaly
Contributing Factors to Insulin Resistance
in Pregnancy
Insulin Resistance
Human placental Lactogen (HPL)
(Human Chorionic Somatomammotropin)Prolactin,Cortisol
Leptin,TNF-aFree Fatty Acids, Resistin, Adiponectin
4/12/2018
5
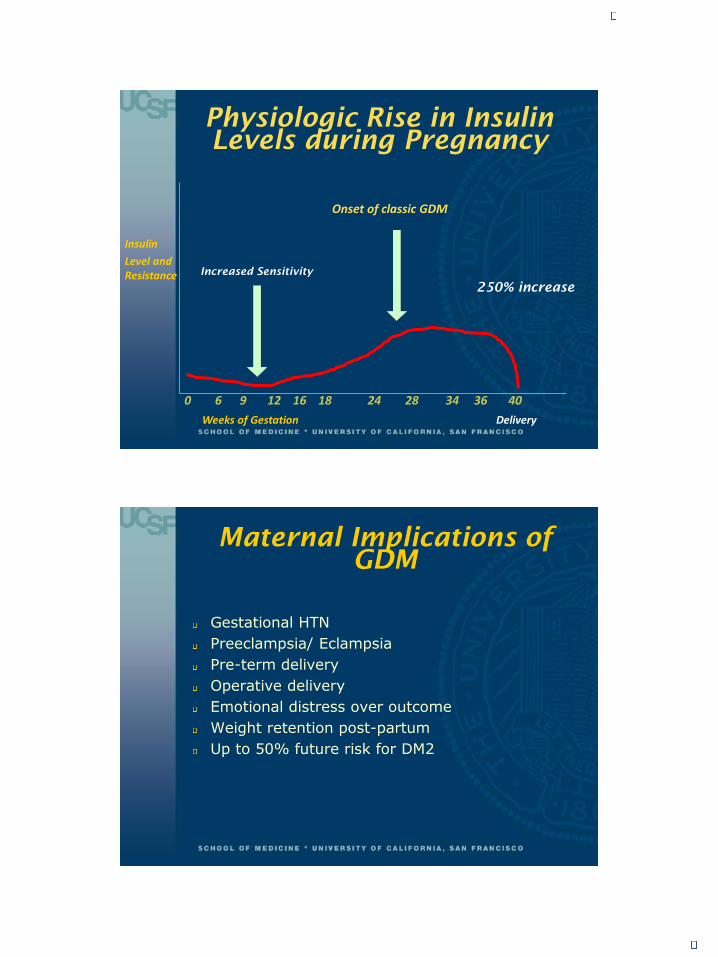
Physiologic Rise in Insulin
Levels during Pregnancy
0 6 9 12 16 18 24 28 34 36 40
Weeks of Gestation Delivery
Insulin
Level and Resistance
Onset of classic GDM
250% increase
Increased Sensitivity
Maternal Implications of
GDM
Gestational HTN
Preeclampsia/ Eclampsia
Pre-term delivery
Operative delivery
Emotional distress over outcome
Weight retention post-partum
Up to 50% future risk for DM2

4/12/2018
6
Fetal Implications of GDM
Fetal/Neonatal/Child and Adult:
LGA / Macrosomia
Stillbirth
Shoulder dystocia
Neonatal hypoglycemia ( NICU stay )
Childhood obesity
DM2
GDM in female offspring
Implications of PEDM
Maternal Risks
Severe hypoglycemia (especially first trimester)
Progression of advanced chronic complications
- Proliferative retinopathy
- Proteinuria/CKD
- Gastroparesis
Pregnancy induced HTN
Cardiovascular event if longstanding DM and AMA
Preeclampsia and Eclampsia
Operative delivery
Anxiety and emotional distress over fetal outcomes
AMA: Advanced maternal age

4/12/2018
7
Implications of PEDM
Fetal Risks
Congenital Anomalies due to - Hyperglycemia- Teratogenic drugs- Lack of folic acid supplementation
SAB and StillbirthMacrosomiaShoulder Dystocia Delayed Lung MaturationPerinatal metabolic Abnormalities:- Hyperbilirubinemia- HypoglycemiaIncreased risk of childhood obesity and DM 2
Postnatal and future Risks
due to GDM and PMD
Macrosomic Neonate•Hypoglycemia
•Hyperbilirubinemia
•Polycythemia
•Respiratory Distress
•Cardiomyopathy
•Brachial Plexus injuries
Long-term Sequelae
•Congenital anomalies (if early GDM)
•Delayed cognitive and motor development
•Increased risk for type 2 DM
•Childhood Obesity
4/12/2018
8
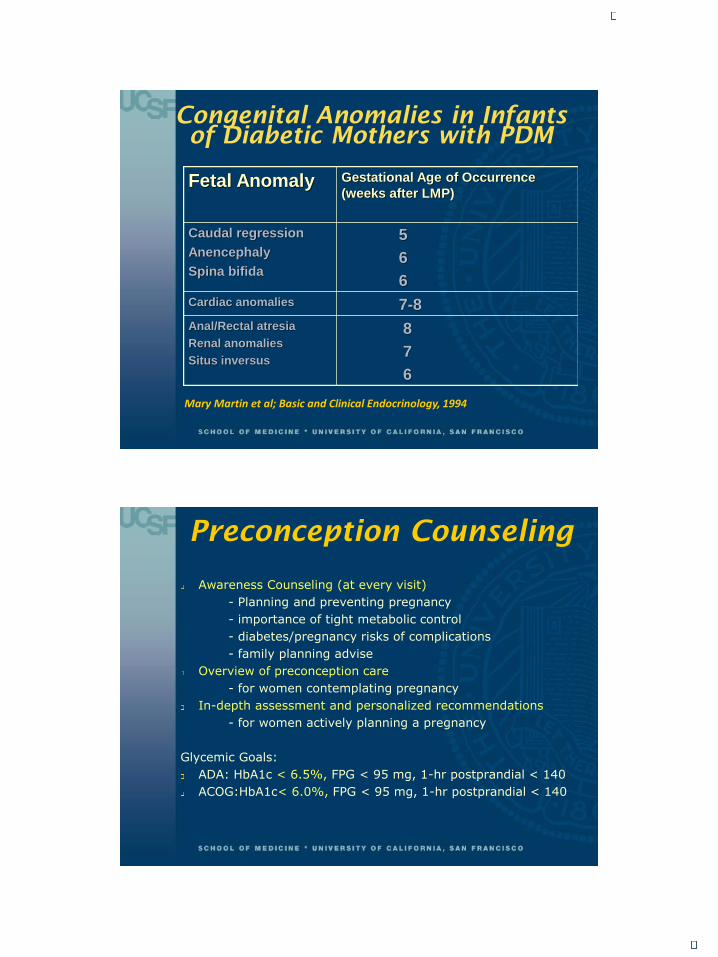
Congenital Anomalies in Infants
of Diabetic Mothers with PDM
Fetal Anomaly Gestational Age of Occurrence
(weeks after LMP)
Caudal regression
Anencephaly
Spina bifida
5
6
6
Cardiac anomalies 7-8
Anal/Rectal atresia
Renal anomalies
Situs inversus
8
7
6
Mary Martin et al; Basic and Clinical Endocrinology, 1994
Preconception Counseling
Awareness Counseling (at every visit)
- Planning and preventing pregnancy
- importance of tight metabolic control
- diabetes/pregnancy risks of complications
- family planning advise
Overview of preconception care
- for women contemplating pregnancy
In-depth assessment and personalized recommendations
- for women actively planning a pregnancy
Glycemic Goals:
ADA: HbA1c < 6.5%, FPG < 95 mg, 1-hr postprandial < 140
ACOG:HbA1c< 6.0%, FPG < 95 mg, 1-hr postprandial < 140
4/12/2018
9
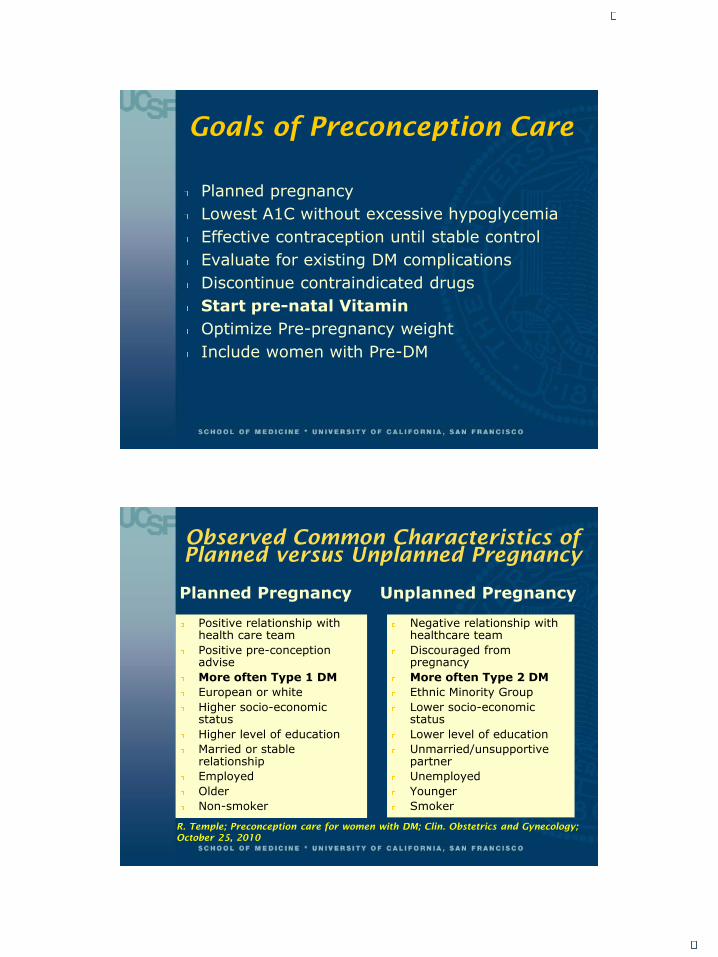
Goals of Preconception Care
Planned pregnancy
Lowest A1C without excessive hypoglycemia
Effective contraception until stable control
Evaluate for existing DM complications
Discontinue contraindicated drugs
Start pre-natal Vitamin
Optimize Pre-pregnancy weight
Include women with Pre-DM
Observed Common Characteristics of
Planned versus Unplanned Pregnancy
Planned Pregnancy
Positive relationship with health care team
Positive pre-conception advise
More often Type 1 DM
European or white
Higher socio-economic status
Higher level of education
Married or stable relationship
Employed
Older
Non-smoker
Unplanned Pregnancy
Negative relationship with healthcare team
Discouraged from pregnancy
More often Type 2 DM
Ethnic Minority Group
Lower socio-economic status
Lower level of education
Unmarried/unsupportive partner
Unemployed
Younger
Smoker
R. Temple; Preconception care for women with DM; Clin. Obstetrics and Gynecology;
October 25, 2010
4/12/2018
10
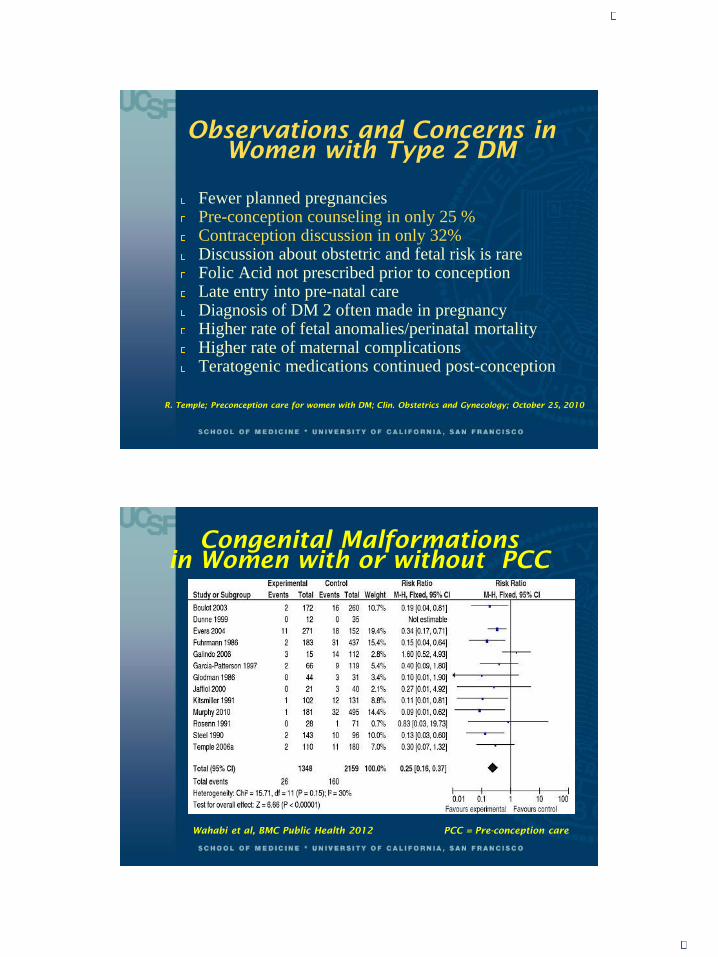
Observations and Concerns in
Women with Type 2 DM
Fewer planned pregnanciesPre-conception counseling in only 25 % Contraception discussion in only 32% Discussion about obstetric and fetal risk is rare Folic Acid not prescribed prior to conception Late entry into pre-natal care Diagnosis of DM 2 often made in pregnancyHigher rate of fetal anomalies/perinatal mortalityHigher rate of maternal complications Teratogenic medications continued post-conception
R. Temple; Preconception care for women with DM; Clin. Obstetrics and Gynecology; October 25, 2010
Congenital Malformations
in Women with or without PCC
PCC = Pre-conception care Wahabi et al, BMC Public Health 2012
4/12/2018
11
Who to Refer to High Risk OB
for Preconception counseling
Longstanding PEDM
Established micro vascular complications
Chronic HTN
Hypoglycemia unawareness or DKA
Uncontrolled hyperglycemia
Advanced maternal age ( > 35 yrs)
Prior history of preeclampsia or pregnancy complications
History of moderate to severe obesity
Preconception Care
and Planning
DM Self care
Pregnancy planning
Education
PMD
Endocrinologist
Obstetrician
Ophthalmologist
Nephrologist
Cardiologist
CDE
RD
Support at Home
Support at work
4/12/2018
12
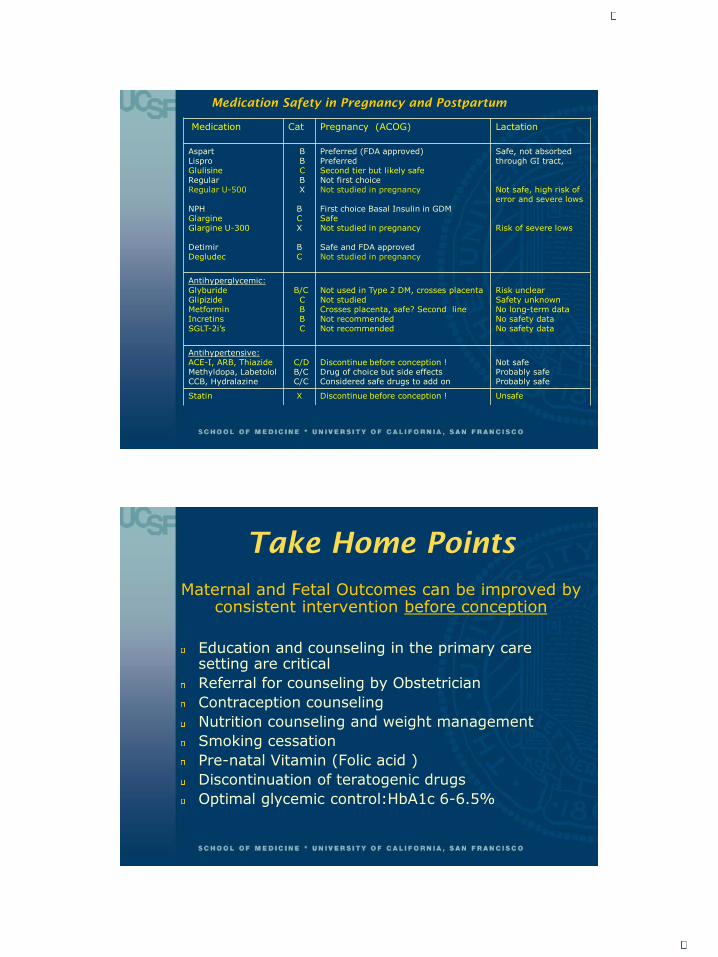
Medication Safety in Pregnancy and Postpartum
Medication Cat Pregnancy (ACOG) Lactation
AspartLisproGlulisineRegular Regular U-500
NPHGlargineGlargine U-300
Detimir Degludec
BBCBX
BCX
BC
Preferred (FDA approved) Preferred Second tier but likely safe Not first choiceNot studied in pregnancy
First choice Basal Insulin in GDMSafe Not studied in pregnancy
Safe and FDA approved Not studied in pregnancy
Safe, not absorbedthrough GI tract,
Not safe, high risk of error and severe lows
Risk of severe lows
Antihyperglycemic:Glyburide GlipizideMetforminIncretins SGLT-2i’s
B/CCBBC
Not used in Type 2 DM, crosses placenta Not studied Crosses placenta, safe? Second lineNot recommended Not recommended
Risk unclearSafety unknownNo long-term dataNo safety data No safety data
Antihypertensive:ACE-I, ARB, Thiazide Methyldopa, LabetololCCB, Hydralazine
C/DB/CC/C
Discontinue before conception !Drug of choice but side effectsConsidered safe drugs to add on
Not safe Probably safe Probably safe
Statin X Discontinue before conception ! Unsafe
Take Home Points
Maternal and Fetal Outcomes can be improved by consistent intervention before conception
Education and counseling in the primary care setting are critical
Referral for counseling by Obstetrician
Contraception counseling
Nutrition counseling and weight management
Smoking cessation
Pre-natal Vitamin (Folic acid )
Discontinuation of teratogenic drugs
Optimal glycemic control:HbA1c 6-6.5%
4/12/2018
13
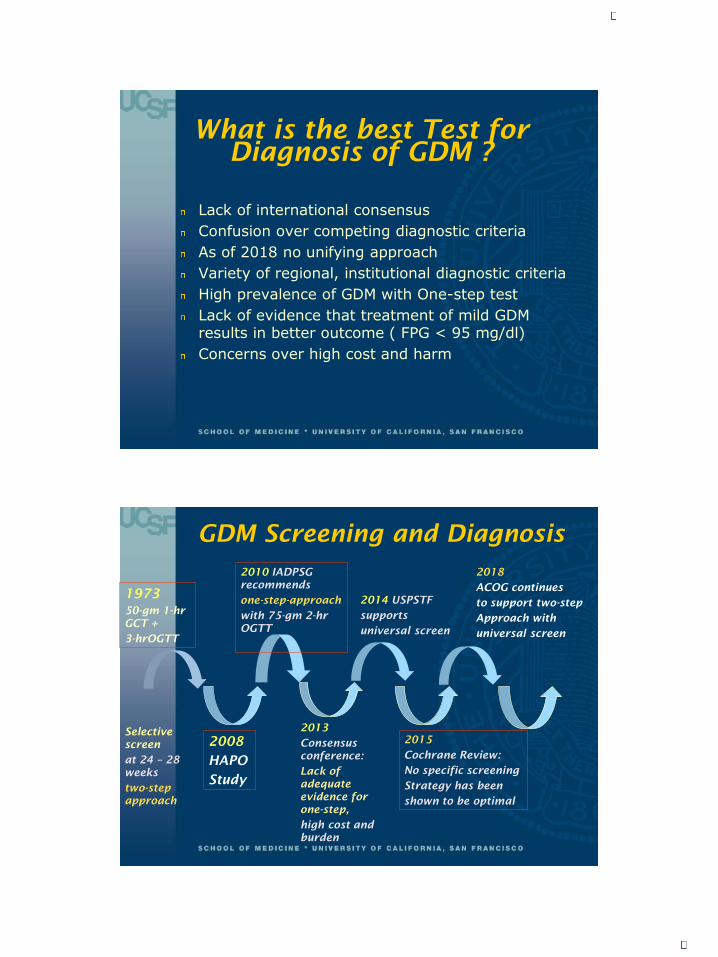
What is the best Test for
Diagnosis of GDM ?
Lack of international consensus
Confusion over competing diagnostic criteria
As of 2018 no unifying approach
Variety of regional, institutional diagnostic criteria
High prevalence of GDM with One-step test
Lack of evidence that treatment of mild GDM results in better outcome ( FPG < 95 mg/dl)
Concerns over high cost and harm
GDM Screening and Diagnosis
1973
50-gm 1-hr
GCT +
3-hrOGTT
Selective
screen
at 24 – 28
weeks
two-step
approach
2014 USPSTF
supports
universal screen
2010 IADPSG
recommends
one-step-approach
with 75-gm 2-hr
OGTT
2013
Consensus
conference:
Lack of
adequate
evidence for
one-step,
high cost and
burden
2015
Cochrane Review:
No specific screening
Strategy has been
shown to be optimal
2018
ACOG continues
to support two-step
Approach with
universal screen
2008
HAPO
Study
4/12/2018
14
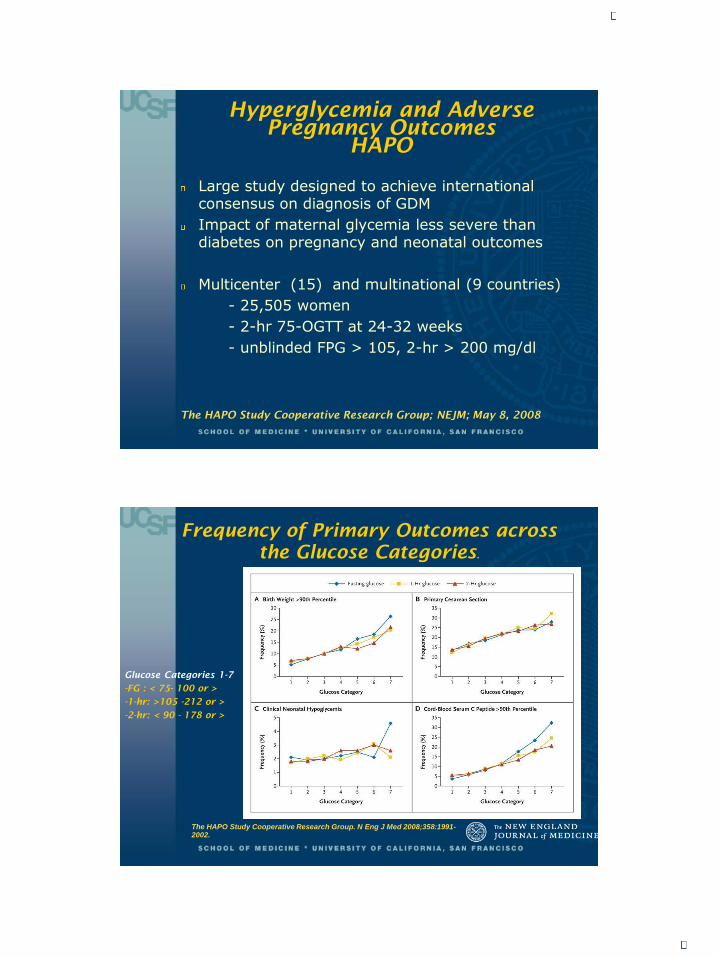
Hyperglycemia and Adverse
Pregnancy Outcomes
HAPO
Large study designed to achieve international consensus on diagnosis of GDM
Impact of maternal glycemia less severe than diabetes on pregnancy and neonatal outcomes
Multicenter (15) and multinational (9 countries)
- 25,505 women
- 2-hr 75-OGTT at 24-32 weeks
- unblinded FPG > 105, 2-hr > 200 mg/dl
The HAPO Study Cooperative Research Group; NEJM; May 8, 2008
Frequency of Primary Outcomes across
the Glucose Categories.
The HAPO Study Cooperative Research Group. N Eng J Med 2008;358:1991-2002.
Glucose Categories 1-7
-FG : < 75- 100 or >
-1-hr: >105 -212 or >
-2-hr: < 90 - 178 or >
4/12/2018
15
Secondary Outcomes
of HAPO Study
Preeclampsia: strongest association with maternal glycemia: OR: 1.21- 1.28
Other positive associations:
Shoulder dystocia or birth injury: OR 1.20
Delivery before 37 weeks
Hyperbilirubinemia
Neonatal ICU stay
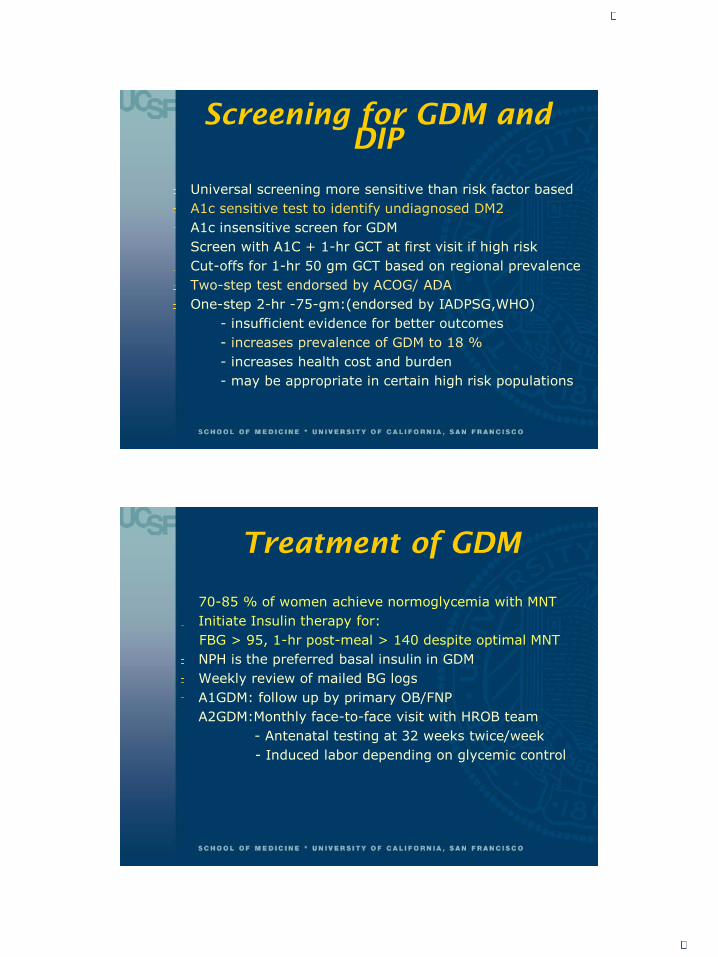
Current Screening Modalities
IADPSG /WHO 2013
One Step Screen:
ACOG/ADA
Two Step Screen:
Fasting 92 mg/dl
1-hr 180 mg/dl
2-hr 153 mg/dl
1) 50-gm, 1hrOGCT
Plasma130-140
2) 3-hr OGTT
Fasting 95 mg/dl
1-hr 180 mg/dl
2-hr 155 mg/dl
3-hr 140 mg/dl1 abnormal value = GDM
Increases prevalence to 18%
2 abnormal values on OGGT = GDM
(Carpenter and Coustan criteria)
IADPSG: International Association of Diabetes Study Group, WHO: World Health Organization
ACOG: American College of Obstetrics and Gynecology, ADA: American
4/12/2018
16
Screening for GDM and
DIP
Universal screening more sensitive than risk factor based
A1c sensitive test to identify undiagnosed DM2
A1c insensitive screen for GDM
Screen with A1C + 1-hr GCT at first visit if high risk
Cut-offs for 1-hr 50 gm GCT based on regional prevalence
Two-step test endorsed by ACOG/ ADA
One-step 2-hr -75-gm:(endorsed by IADPSG,WHO)
- insufficient evidence for better outcomes
- increases prevalence of GDM to 18 %
- increases health cost and burden
- may be appropriate in certain high risk populations
Treatment of GDM
70-85 % of women achieve normoglycemia with MNT
Initiate Insulin therapy for:
FBG > 95, 1-hr post-meal > 140 despite optimal MNT
NPH is the preferred basal insulin in GDM
Weekly review of mailed BG logs
A1GDM: follow up by primary OB/FNP
A2GDM:Monthly face-to-face visit with HROB team
- Antenatal testing at 32 weeks twice/week
- Induced labor depending on glycemic control

4/12/2018
17
Risk Reduction with
Treatment for GDM
Decreases Preeclampsia risk (3 trials)
Reduces rate of Macrosomia (5 trials)
Reduces Shoulder Dystocia (3 trials)
Medical Nutrition Therapy
MNT
Goals:
Achieve optimal pre and post meal BG’s
FBG < 95 mg/dl
1- hr post prandial < 140 mg/dl
2- hr post prandial < 120 mg/dl
Prevent ketosis
Promote fetal well-being
Individualize caloric intake based on BMI and weight goals ( 12-40 kcal/Kg, 33-40% CHO)
Teach CHO counting
Promote physical activity
Post-partum counseling on weight management
4/12/2018
18
Medical Nutrition Therapy
Recommended CHO distribution
Breakfast: 30 - 45 gm
Snack: 15 – 30 gm
Lunch: 45 – 60 gm
Snack: 15 – 30 gm
Dinner: 45 – 60 gm
Bedtime Snack: 15 -30 gm
Total minimum CHO intake: 175 gm/ day
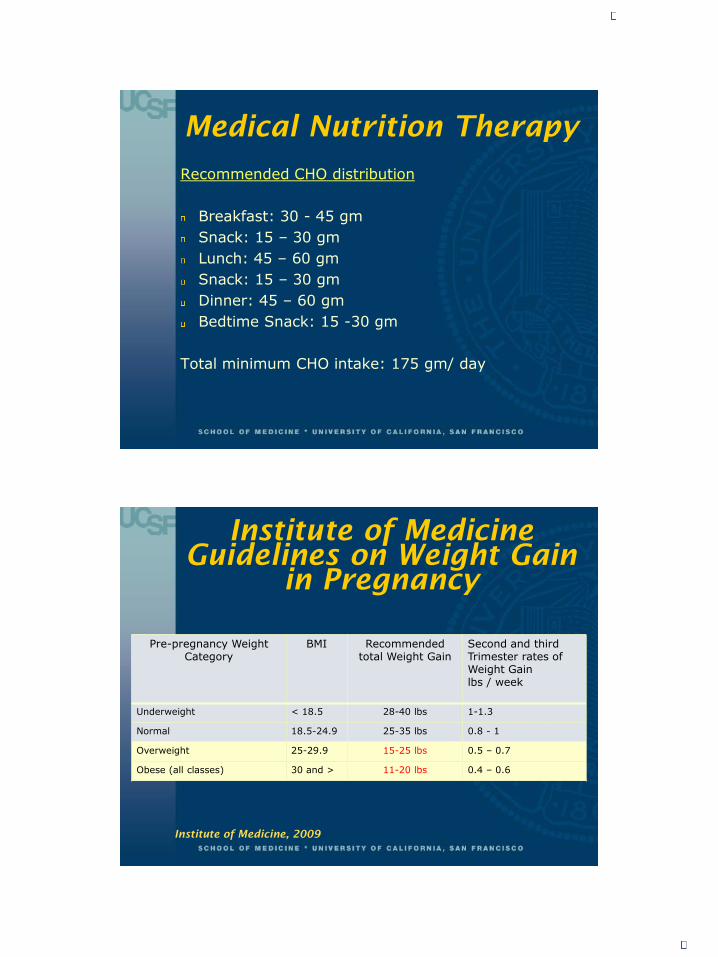
Institute of Medicine
Guidelines on Weight Gain
in Pregnancy
Pre-pregnancy Weight Category
BMI Recommendedtotal Weight Gain
Second and third Trimester rates of Weight Gain lbs / week
Underweight < 18.5 28-40 lbs 1-1.3
Normal 18.5-24.9 25-35 lbs 0.8 - 1
Overweight 25-29.9 15-25 lbs 0.5 – 0.7
Obese (all classes) 30 and > 11-20 lbs 0.4 – 0.6
Institute of Medicine, 2009
4/12/2018
19
Treatment of GDM with
oral Agents
Glyburide:
-Higher rated of Macrosomia and neonatal hypoglycemia:
-Not first line drug
Metformin: Failure rate up to 40 %
- Safe ? Crosses the placenta in significant amounts.
- long term safety data not yet available
MiG-TOFU trial: 2011
- Large RCT (New Zealand National Women’s Health Database)
- Compared Metformin and insulin
- Slightly earlier delivery and less neonatal hypoglycemia in
Metformin group
-Two year follow up in offspring: no difference in total body fat
mass. Awaiting results of 9 yr follow up
If using Metformin must counsel patient !
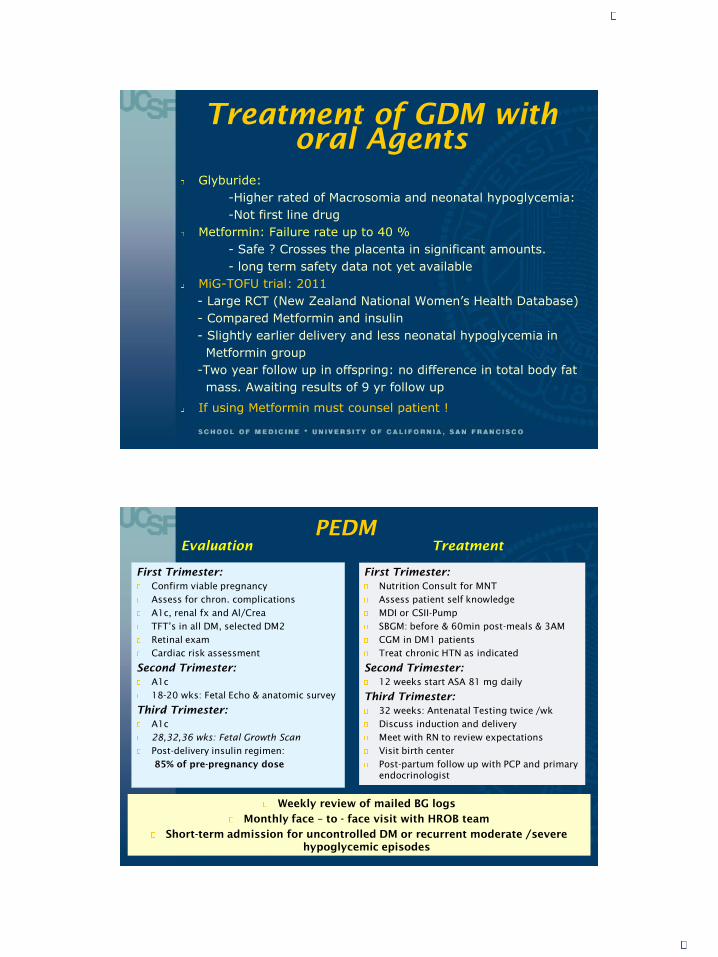
PEDM
First Trimester:
Confirm viable pregnancy
Assess for chron. complications
A1c, renal fx and Al/Crea
TFT’s in all DM, selected DM2
Retinal exam
Cardiac risk assessment
Second Trimester:
A1c
18-20 wks: Fetal Echo & anatomic survey
Third Trimester:
A1c
28,32,36 wks: Fetal Growth Scan
Post-delivery insulin regimen:
85% of pre-pregnancy dose
First Trimester:
Nutrition Consult for MNT
Assess patient self knowledge
MDI or CSII-Pump
SBGM: before & 60min post-meals & 3AM
CGM in DM1 patients
Treat chronic HTN as indicated
Second Trimester:
12 weeks start ASA 81 mg daily
Third Trimester:
32 weeks: Antenatal Testing twice /wk
Discuss induction and delivery
Meet with RN to review expectations
Visit birth center
Post-partum follow up with PCP and primary
endocrinologist
Weekly review of mailed BG logs
Monthly face – to - face visit with HROB team
Short-term admission for uncontrolled DM or recurrent moderate /severe
hypoglycemic episodes
Evaluation Treatment
4/12/2018
20
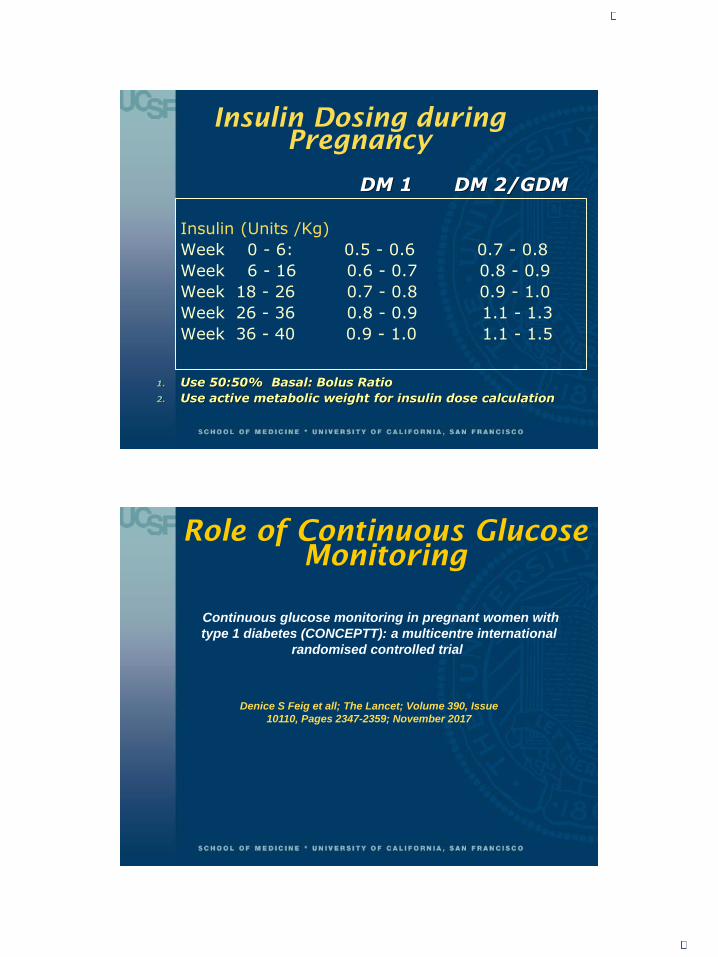
Insulin Dosing during
Pregnancy
Insulin (Units /Kg)
Week 0 - 6: 0.5 - 0.6 0.7 - 0.8
Week 6 - 16 0.6 - 0.7 0.8 - 0.9
Week 18 - 26 0.7 - 0.8 0.9 - 1.0
Week 26 - 36 0.8 - 0.9 1.1 - 1.3
Week 36 - 40 0.9 - 1.0 1.1 - 1.5
1. Use 50:50% Basal: Bolus Ratio
2. Use active metabolic weight for insulin dose calculation
DM 1 DM 2/GDM
Continuous glucose monitoring in pregnant women with
type 1 diabetes (CONCEPTT): a multicentre international
randomised controlled trial
Denice S Feig et all; The Lancet; Volume 390, Issue
10110, Pages 2347-2359; November 2017
Role of Continuous Glucose
Monitoring
4/12/2018
21
CONCEPTT
Assessed effectiveness of CGM on maternal glucose control and obstetric and neonatal outcomes
31 Hospitals (Canada, Europe, USA)
325 women, 18-40 years old, Type 1 DM
planning pregnancy or
< 13 weeks pregnant
12 month duration
Primary outcome: change in A1c
Secondary outcome: obstetric and neonatal health
Denice S Feig et all; The Lancet; Volume 390, Issue 10110, Pages 2347-2359; November 2017
CONCEPTT
Results:
Increased time in glucose target in CGM group
Comparable hypoglcycemia
Small difference in A1c
Lower incidence of LGA (NNT: 6)
Lower rate of neonatal hypoglycemia (NNT: 8)
Lower admission rate to NICU (NNT: 6)
One day shorter hospital stay
Less significant outcomes in women planning pregnancy
Costeffectiveness will need further study
Denice S Feig et all; The Lancet; Volume 390, Issue 10110, Pages 2347-2359; November 2017

4/12/2018
22
Postpartum Follow up and
Interconception Care for GDM
75-g 2-hr OGTT at
4-12 weeks
Diabetes Mellitus
Pre-DM Normal
Follow up with
PMD
Screen for DM every 1-3 years &
Before next conception
Exercise, Weight loss
Family Planning
Preconception Counseling and care
Screen for DM annually & Before next conception
Exercise, Diet, Weight loss
Nutrition counseling
Consider Metformin
Family Planning Preconception Care and Counseling
Treat for DM
Nutrition consult
Diabetes Education
Family Planning Preconception Care and Counseling
Endocrine Referral
References
1. Correa, A.,Bardenheimer, B., Elixhauser, A et al. Mat. Child Health J. (2015)
2. ACOG Practice Bulletin, Number 190, February 2018
3. Epidemiology of Diabetes in Pregnancy; David Simmons
A practical Manual of DM in Pregnancy Second Edition. 2018 John Wiley & Sons
4. The HAPO Study Cooperative Research Group. Hyperglycemia and Adverse
Pregnancy Outcome NEJM, May 8, 2008;358:1991-2002
5. F. M. Brown, J. Wyckoff; Application of One-Step IADPSG versus Two-step
6. Diagnostic Criteria for GDM in the Real World: Impact on Health Services, Clinical Care and Outcomes. Curr Diab Rep (2017)17:85, August 2017
7. Hartling L. Dryden et al. Benefits and harms of treating gestational diabetes
mellitus: a systematic review and meta-analysis for the U.S. Preventive Task
Force and the National Institutes of Health Office of Medical Applications of
Research. Ann Intern Med 2013; 159:123
8. J. Rowan et al Metformin in gestational diabetes: The offspring follow-up (MiG-
TOFU): body composition at 2 years of age; Diabetes Care. 2011;34(10); 2279
9. E. Buschur, F. Brown, J. Wyckhoff, Using Oral Agents to manage Gestational Diabetes: What have we learned?, Curr Diab Rep, (2015) 15:4
10. Denise S Feig et al. Continuous Glucose Monitoring in Pregnant Women with Type 1 Diabetes (CONCEPTT): A Multicentre Randomised Controlled Trial; The Lancet, 15 September 2017
11. Institute of Medicine Guidelines on Weight Gain in Pregnancy, IOM 2009
12. F. Peterson-Burch et al: Preconception Counseling for Adolescents and Young Adults with Diabetes; 02/15/2018; A literature review of the past 10 years.
Current Diabetes Reports( 2018) 18:11
4/12/2018
23
Thank you !
Thank you!


















