Clinical Practice Guideline on management of patients with diabetes and chronic kidney disease

of 46
Upload
lansoprazoleCategory
view
220download
0description
American Diabetes Association
STANDARDS OF MEDICAL CAREIN DIABETES2015
Standards of Medical Care in Diabetes2015 comprises all of the current and key clinical practice recommendations of the American Diabetes Association (ADA)These Standards of Care are revised annually by the ADAs multidisciplinary Professional Practice Committee (PPC)For the current revision, PPC members systematically searched Medline for human studies related to each subsection and published since 1 January 2014Recommendations were revised based on new evidence or, in some cases, to clarify the prior recommendations or match the strength of the word to the strength of the evidentA table linking the changes in the recommendations to new evidence can be reviewed at http://professional.diabetes.org/SOCAs for all position statements, the Standards of Care were reviewed and approved by the Executive Committee of ADAs Board of Directors, which includes health care professionals, scientists, and lay peopleFeedback from the larger clinical community was valuable for the 2014 revision of the Standards of Care; readers who wish to comment on the Standards of Medical Care in Diabetes2015 are invited to do so at http://professional.diabetes.org/SOCADA funds development of the Standards of Care and all ADA position statements out of its general revenues and does not use industry support for these purposesThe slides are organized to correspond with sections within the Standards of Medical Care in Diabetes2015While not every section in the document is represented, these slides do incorporate the most salient points from the Position Statement1ReferenceAmerican Diabetes Association. Standards of medical care in diabetes2014. Diabetes Care 2014;37(suppl 1):S1 2. CLASSIFICATION AND DIAGNOSIS OF DIABETESSection 2. Classification and Diagnosis of Diabetes Classification of DiabetesCriteria for the Diagnosis of DiabetesPrediabetes: IFG, IGT, Increased A1C2Classification of DiabetesType 1 diabetes-cell destructionType 2 diabetesProgressive insulin secretory defectOther specific types of diabetesGenetic defects in -cell function, insulin actionDiseases of the exocrine pancreasDrug- or chemical-inducedGestational diabetes mellitus (GDM)ADA. 2. Classification and Diagnosis. Diabetes Care 2015;38(suppl 1):S8The classification of diabetes includes four clinical categoriesType 1 diabetes (due to -cell destruction, usually leading to absolute insulin deficiency)Type 2 diabetes (due to a progressive insulin secretory defect on the background of insulin resistance)Other specific types of diabetes due to other causes; e.g., genetic defects in -cell function, genetic defects in insulin action, diseases of the exocrine pancreas (such as cystic fibrosis), and drug- or chemical-induced diabetes (such as in the treatment of HIV/AIDS or after organ transplantation)Gestational diabetes mellitus (GDM)(diabetes diagnosed during pregnancy that is not clearly overt diabetes)Some patients cannot be clearly classified as having type 1 or type 2 diabetesClinical presentation and disease progression vary considerably in both types of diabetesOccasionally, patients who otherwise have type 2 diabetes may present with ketoacidosisChildren with type 1 diabetes typically present with the hallmark symptoms of polyuria/polydipsia and occasionally with diabetic ketoacidosis (DKA)However, difficulties in diagnosis may occur in children, adolescents, and adults, with the true diagnosis becoming more obvious over time3ReferenceAmerican Diabetes Association. Standards of medical care in diabetes2014. Diabetes Care 2014;37(suppl 1):S14peripheralglucose uptake
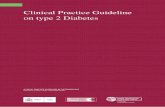
hepatic glucose productionpancreatic insulinsecretion
pancreatic glucagonsecretion
gutcarbohydratedelivery &absorption incretineffect HYPERGLYCEMIA
?Adapted from: Inzucchi SE, Sherwin RS in: Cecil Medicine 2011
Multiple, Complex Pathophysiological Abnormalities in T2DM__+renal glucose excretion
4This slide provides a broad overview of the main pathophysiological defects in type 2 diabetes. Insulin resistance is demonstrated in peripheral tissues, such as skeletal muscle and adipocytes. The pancreas develops relative insulin secretory failure and is no longer provide the amount of insulin required for normal glucose. The pancreas also demonstrates a failure of the normal suppression of glucagon after meals. This may be mediated through abnormalities in the incretin axis. Hepatic glucose production is also increased. Renal glucose output is set at a higer threshold than normal. Many of these defects may be influenced by abnormal central control of metabolism. Criteria for the Diagnosis of DiabetesA1C 6.5%ORFasting plasma glucose (FPG)126 mg/dL (7.0 mmol/L)OR2-h plasma glucose 200 mg/dL(11.1 mmol/L) during an OGTTORA random plasma glucose 200 mg/dL (11.1 mmol/L)ADA. 2. Classification and Diagnosis. Diabetes Care 2015;38(suppl 1):S9; Table 2.1Table 2, current diagnostic criteria for the diagnosis of diabetes, is divided into five slidesOn this slide, all four criteria are included:A1C 6.5%ORFasting plasma glucose (FPG) 126 mg/dL (7.0 mmol/L)OR2-hour plasma glucose 200 mg/dL (11.1 mmol/L) during an OGTTORA random plasma glucose 200 mg/dL (11.1 mmol/L), in patients with classic symptoms of hyperglycemia or hyperglycemic crisis The subsequent four slides examine each of the four criteria in greater detail
5ReferenceAmerican Diabetes Association. Standards of medical care in diabetes2014. Diabetes Care 2014;37(suppl 1):S15; Table 2Criteria for the Diagnosis of DiabetesA1C 6.5%
The test should be performed in a laboratory using a method that isNGSP certified and standardizedto the DCCT assay**In the absence of unequivocal hyperglycemia, result should be confirmed by repeat testing.ADA. 2. Classification and Diagnosis. Diabetes Care 2015;38(suppl 1):S9; Table 2A1CRecently, an International Expert Committee added the A1C, (threshold 6.5%) as a third option to diagnose diabetes 1,2The A1C test should be performed using a method certified by the National Glycohemoglobin Standardization Program (NGSP) and standardized or traceable to the Diabetes Control and Complications Trial (DCCT) reference assay3Although point-of-care (POC) assays may be NGSP-certified, proficiency testing is not mandated for performing the test, so use of these assays for diagnostic purposes may be problematic2The A1C has several advantages to the FPG and OGTT, including greater convenience (fasting not required), possibly greater preanalytical stability, and less day-to-day perturbations during periods of stress and illness2These advantages must be balanced by greater cost, the limited availability of A1C testing in certain regions of the developing world, and the incomplete correlation between A1C and average glucose in certain individuals2A1C levels may vary with patients race/ethnicity3,4Interpreting A1C levels in the presence of certain anemias and hemoglobinopathies is particularly problematic (see www.ngsp.org/interf.asp for an updated list)6ReferencesInternational Expert Committee: International Expert Committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care 2009;32:13271334American Diabetes Association. Standards of medical care in diabetes2014. Diabetes Care 2014;37(suppl 1):S15; Table 2Ziemer DC, Kolm P, Weintraub WS, et al. Glucose-independent, black-white differences in hemoglobin A1c levels: a cross-sectional analysis of 2 studies. Ann Intern Med 2010;152:770777Kumar PR, Bhansali A, Ravikiran M, et al. Utility of glycated hemoglobin in diagnosing type 2 diabetes mellitus: a community-based study. J Clin Endocrinol Metab 2010;95:28322835Criteria for the Diagnosis of DiabetesFasting plasma glucose (FPG)126 mg/dL (7.0 mmol/L)
Fasting is defined as no caloric intakefor at least 8 h**In the absence of unequivocal hyperglycemia, result should be confirmed by repeat testing.ADA. 2. Classification and Diagnosis. Diabetes Care 2015;38(suppl 1):S9; Table 2.1Fasting Plasma Glucose (FPG)In addition to the A1C test, the FPG and 2-h PG may also be used to diagnose diabetes1Concordance between the FPG and 2-h PG tests is