Factors Affecting Compliance with Diabetes Hypertension Guidelines

American Journal of EpidemiologyCopyright © 1999 by The Johns Hopkins University School of Hygiene and Public HealthAll rights reserved
Vol. 149, No. 11Printed in U.S.A.
Diabetes and Hypertension in Mexican American Families: Relation toCardiovascular Risk
Braxton D. Mitchell,1 Laura A. Almasy,1 David L. Rainwater,1 Jennifer L. Schneider,1 John Blangero,1 Michael P.Stern,2 and Jean W. MacCluer1
There is a strong familial predisposition to type 2 diabetes, hypertension, and cardiovascular disease. Theauthors evaluated the association between a family history of these diseases and a large panel of cardiovascularrisk factors in 1,431 Mexican American subjects who were enrolled in the San Antonio Family Heart Study inSan Antonio, Texas. The baseline phase of the study covered 1992-1996. Diabetes and hypertension werediagnosed according to standard clinical criteria, while cardiovascular disease was defined as a history of heartattack or heart surgery. The prevalence of diabetes, hypertension, and cardiovascular disease in this populationwas 15%, 12%, and 3%, respectively. For each unaffected subject, the authors computed a family history scorebased on the presence or absence of disease in parents and older siblings, and correlations betweencardiovascular risk factors and family history scores were estimated by using likelihood-based variancecomponent methods. Diabetes family history score was significantly correlated with a broad panel ofcardiovascular risk factors, including glucose and insulin, obesity, blood pressure, triglycerides, and totalcholesterol. Hypertension family history score was significantly correlated with glucose, blood pressure, bodymass index, waist circumference, total cholesterol, and triglycerides. These results support the idea that genesthat confer a risk for diabetes, and to a lesser extent hypertension, adversely alter the cardiovascular risk profilelong before the manifestation of clinical disease. Am J Epidemiol 1999; 149:1047-56.
cardiovascular diseases; diabetes mellitus; family; genetics; hypertension; risk; risk assessment; risk factors
Cardiovascular disease is the leading cause of deathamong adults in the United States and is a major causeof morbidity (1). A family history of early heart dis-ease is an important risk factor for cardiovascular dis-ease, and relatives of patients with diabetes and hyper-tension are also at increased risk, partly because theserelatives tend to have elevated glucose and blood pres-sure levels. However, a family history of diabetesand/or hypertension may also be associated with otheralterations in the cardiovascular risk profile. For exam-ple, numerous studies have reported that relatives ofdiabetic subjects tend to be more insulin resistant thancontrol subjects (2-8), and insulin resistance has beenreported in nonhypertensive offspring of subjects withessential hypertension (9-12). Moreover, prospectivestudies have established that an atherogenic cardiovas-cular risk profile, including elevations in body mass
Received for publication January 29,1998, and accepted for pub-lication September 25, 1998.
Abbreviations: LDL, low density lipoprotein; Lp(a), lipoprotein(a);OR, odds ratio.
1 Department of Genetics, Southwest Foundation for BiomedicalResearch, San Antonio, TX.
2 Department of Medicine/Epidemiology, University of TexasHealth Science Center, San Antonio, TX.
Reprint requests to Dr. Braxton D. Mitchell, Department ofGenetics, Southwest Foundation for Biomedical Research, PO Box760549, San Antonio, TX 78245-0549.
index, triglyceride concentrations, and blood pressure,begins to emerge long before the onset of clinical dia-betes (13, 14). This pattern of risk factor clustering iscommonly referred to as the multiple metabolic syn-drome, or syndrome X. Clustering of these risk factorsis consistent with the idea that genes associated withdiabetes and/or hypertension may have pleiotropiceffects on cardiovascular risk that are independent ofthe secondary changes that occur as a consequence ofthe diabetic (and/or hypertensive) state.
The goal of this study was to evaluate the relationbetween a family history of diabetes, hypertension,and cardiovascular disease and a broad panel of car-diovascular risk factors, including measures of adipos-ity, lipids and lipoproteins, and blood pressure. Thestudy population consisted of persons with large,multigenerational pedigrees. A unique feature of thispopulation is that the families represented a popula-tion-based sample, which were not selected for anyparticular disease or phenotype.
MATERIALS AND METHODS
The San Antonio Family Heart Study was designedto investigate the genetics of heart disease and itsdeterminants in Mexican American families from San
1047

1048 Mitchell et al.
Antonio, Texas. Probands for the study were identi-fied, without regard to health status or family healthhistory, from low-income neighborhoods, and all first-,second-, and third-degree relatives of the proband andspouse aged 16 years or older were invited to partici-pate. A total of 1,431 persons from 42 extended fami-lies were recruited into the baseline phase of the study,which was conducted between 1992 and 1996. Detailsof the sampling design and recruitment procedureshave been described previously (15).
Probands and participating family members receiveda medical examination in our clinic. Pregnant womenwere not eligible to participate; women who reportedthat they were pregnant were recontacted followingtheir pregnancies to reschedule the examination.Examinations took place in the morning following a12-hour fast. An anthropometric assessment was con-ducted that included measurement of height andweight, skinfold thicknesses, and waist and hip circum-ferences. Systolic (first phase) and diastolic (fifthphase) blood pressures were measured to the nearesteven digit by using a random-zero sphygmomanometer(Hawksley-Gelman, London, England) on the right armof the seated participant. Three readings were recordedfor each person, whose blood pressure was defined asthe average of the second and third readings.
A 75 g glucose equivalent load was also adminis-tered, and glucose and insulin levels were determinedfrom a blood sample obtained 2 hours following theglucose challenge. Plasma glucose was measured byusing an Abbott V/P Analyzer (Diagnostic ProductsCorp., Los Angeles, California) and serum insulin andleptin by radioimmunoassay. Lipid and lipoproteinconcentrations were determined from fasting bloodsamples by using methods described previously (15).Low density lipoprotein (LDL) size was measured byusing nondenaturing gradient gel electrophoresis inlaboratory-made gels (16). LDL cholesterol wasstained with Sudan black B; median diameter, thediameter that splits the LDL absorbance profile in two,was determined as described by Rainwater et al. (17).Median diameter is similar to LDL particle score asmeasured by other laboratories (18, 19).
Diabetes was diagnosed according to the plasma glu-cose criteria of the World Health Organization (20).Subjects were also considered to have diabetes if theywere currently taking antidiabetic medications.Hypertension was defined as a systolic blood pressureof >160 mmHg, a diastolic blood pressure of >95mmHg, or current use of antihypertensive medications.Overt heart disease was defined as a self-reported his-tory of heart attack ("Have you ever been told by a doc-tor that you had a heart attack?") or a history of heartsurgery ("Have you ever had surgery on your heart?").
A medical history interview was administered, inwhich information was obtained on a variety of otherfactors potentially related to diabetes, hypertension,and heart disease. These variables included years ofeducation, current smoking status, alcohol consump-tion (converted to g/day), menopausal status, oral con-traceptive use, and postmenopausal estrogen use.Women were considered postmenopausal if theyreported having had both ovaries removed or if at least12 months had elapsed since their last menstrual period.These variables were used as covariates in the regres-sion analyses.
The extent to which diabetes, hypertension, andovert heart disease clustered in study subjects wasevaluated by comparing the prevalence of each disor-der in those with and without a second disorder. Forexample, we compared the prevalence of hypertension(and overt heart disease) in those subjects with andwithout diabetes. These analyses were performed formen and women separately. Odds ratios were computedby using multiple logistic regression to describe theassociation between each pair of disorders whileadjusting for the effects of age.
In a preliminary analysis, we compared mean levelsof cardiovascular risk factors between subjects withand without a parental history of diabetes, hyperten-sion, and overt heart disease. Only unaffected subjectswere included in these analyses. For example, we com-pared cardiovascular risk factors between nondiabeticoffspring of diabetic parents and nondiabetic off-spring of nondiabetic parents (and between nonhy-pertensive offspring of hypertensive parents and non-hypertensive offspring of nonhypertensive parents).Parental history was considered positive if either par-ent was affected and negative if both parents wereexamined and found to be unaffected. Offspring of oneunaffected parent were not included in this analysis ifthe other parent was not examined. Age-adjustedmeans for the cardiovascular risk factors were com-puted by using the analysis of variance procedure inSYSTAT (SPSS Inc., Chicago, Illinois). This analyticapproach was deemed preliminary because it makesonly limited use of the known information about dis-ease status in ancestors (i.e., parental disease status isdichotomized, and information about other relatives isnot considered). In addition, the analysis does not takeinto account the nonindependence of offspring withinsibships and between related sibships.
To incorporate into the analysis information aboutwhether additional family members were affected, wecomputed a family history score for each participantand estimated its effect on each quantitatively distrib-uted risk factor. The family history score was designedto summarize the burden of disease (diabetes, hyper-
Am J Epidemiol Vol. 149, No. 11, 1999

Diabetes, Hypertension, and Cardiovascular Risk in Families 1049
tension, and heart disease) in each participant's imme-diate family members. Scores were calculated byadding 1 for each affected parent and older sibling and-1 for each unaffected parent and older sibling.Unexamined family members did not contribute anyinformation to the family history score. Thus, althoughthey were excluded from the preliminary "parental his-tory" analysis, subjects who had one examined unaf-fected parent and one unexamined parent could beincluded in this analysis. This scoring is analogous tothat described by Bonney in his class D regressivemodels, in which each subject's phenotype is depen-dent on the phenotype of his or her parents and allolder siblings (21). In the context of our study, a sig-nificant effect of this family history score occurs onlywhen the familial correlation between the discrete traitand the quantitative risk factor does not equal 0.
A virtue of this scoring function is that the scores areinfluenced largely by the "density" of disease in a fam-ily, since information from both affected and unaffectedrelatives is included. In contrast, scores based on thenumbers of affected relatives only are heavily depen-dent on family size; larger families may include moreaffected persons than smaller families do merelybecause of their size. The problem is not remediedsimply by considering the proportion of affected per-sons in the family. This approach introduces the prob-lem that scores generated from small families may behighly variable but will be assigned weights equal tothose scores generated from large families. Our scor-ing function places more weight on larger families,because extremely high (or extremely low) scores can-not be generated from small, and less informative,families. Obviously, the scores among siblings are cor-related, but these familial correlations are accountedfor in the analysis by conditioning on the pedigreestructures, described below.
We modeled each risk factor as a function of age,age squared, sex, and family history score. The fol-lowing covariates were also included in the model:years of education, alcohol consumption (g/day), cur-rent smoking (yes/no), menopausal status (post-menopausal vs. other), oral contraceptive use (currentuse vs. other), and postmenopausal estrogen use (cur-rent use vs. other). Although genetic influences sharedamong relatives can also be incorporated as an addi-tional component of variance, we chose not to modelthem because we hypothesized that any associationsbetween the cardiovascular risk factor and a familyhistory of disease are largely due to the transmission ofgenes from parents to offspring. In fact, we demon-strated previously that genetic factors account formuch more of the phenotypic variability in cardiovas-cular risk factors in this population than do environ-
mental influences shared among relatives (15).Maximum likelihood estimates of the means and vari-ances were obtained by using the FISHER softwareprogram (22), which conditions parameter estimationson the family relationships.
We accounted for nonindependence among siblingsby conditioning the analysis on the pedigree data.Briefly, we used FISHER software to compute thelikelihood of the pedigree data in models that bothincluded and excluded the family history score. Thesignificance of the family history score was assessedby using the likelihood ratio test, which compares thelikelihood of a full model (e.g., age, sex, covariates,and family history score) with that of a nested model(e.g., age, sex, and covariates only). The likelihoodratio statistic is distributed asymptotically as a chi-square statistic with degrees of freedom equal to thedifference in the numbers of parameters included inthe two models being compared (23). No adjustmentwas made for multiple comparisons, in part becausewe hypothesized that many of the outcomes wereinterdependent.
We tested for the presence of interactions betweensex and family history score by estimating the effect offamily history score independently for men andwomen. The sex interaction term was interpreted asstatistically significant if the likelihood of this modelwith sex-specific regression coefficients was signifi-cantly larger than that of the nested model, in whichthe sex correlations were constrained to be identical.
Persons who were currently taking antilipid medica-tions were excluded from the analyses involving lipidand lipoprotein concentrations, and diabetic personswere excluded from analyses involving insulin.Insulin, triglyceride, and lipoprotein(a) (Lp(a)) con-centrations were logarithm-transformed prior to analy-sis to remove skewness, and the distribution of LDLsizes was transformed by using the reciprocal of thesquare root.
RESULTS
The mean age (standard deviation) of the 1,431 per-sons examined in this study was 39.3 (16.8) years. Theprevalence of diabetes, hypertension, and self-reportedheart disease, according to age and sex, is shown intable 1. More than 20 percent of the men and womenhad at least one of these three conditions. The overallprevalence of diabetes was 14.0 and 15.7 percent inmen and women, respectively. Approximately 57 per-cent of the diabetic subjects were currently takingantidiabetic medications (either insulin or oral agents).Hypertension was present in 9.0 percent of the menand 14.0 percent of the women. Of those affected, 79.0percent reported that they were currently taking anti-
Am J Epidemiol Vol. 149, No. 11, 1999

1050 Mitchell et al.
TABLE 1. Prevalence of diabetes, hypertension, andFamily Heart Study, San
Age(years)
16-2930-3940-4950-5960-69>70
Overall prevalence
Antonio,
No.
223104100724736
582f
Texas, 1992-1996
Diabetes
1.48.8
21.429.628.640.0
14.0
Men
Hypertensior
0.04.8
10.319.422.237.1
9.0
self-reported
Self-reported
heartdisease
0.41.04.0
15.314.35.7
4.4
heart disease,* according to age and sex,
Anyclinicaldisease
1.814.927.845.144.262.9
21.0
No.
278170193976347
849t
Diabetes
1.46.0
20.033.347.640.9
15.7
Women
Hypertension
0.73.0
14.630.246.053.2
14.0
the San
Self-reported
heartdisease
0.01.21.62.14.8
15.6
2.0
Antonio
Anyclinicaldisease
2.28.5
30.050.066.771.1
23.9
* Per 100 persons,t Total sample size.
hypertensive medications (82.4 percent of the men and77.6 percent of the women). A total of 4.4 percent ofthe men and 2.0 percent of the women reported thatthey had previously been told by a physician that theyhad had a heart attack or that they had undergone heartsurgery in the past.
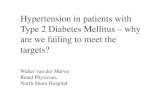
The prevalence of hypertension and heart disease inmen and women, according to diabetes status, isshown in figure 1. Hypertension was present in 33.3and 5.1 percent of diabetic and nondiabetic men,respectively, and in 42.0 and 8.7 percent of diabeticand nondiabetic women, respectively. Heart disease
was present in 13.8 and 2.9 percent of diabetic andnondiabetic men, respectively, and in 6.2 and 1.3 per-cent of diabetic and nondiabetic women, respectively.After adjustment for age, the association between dia-betes and hypertension was highly significant in bothmen (adjusted odds ratio (OR) = 4.00, p < 0.001) andwomen (adjusted OR = 2.78, p < 0.001). The associa-tion between diabetes and heart disease was statisticallysignificant in men (adjusted OR = 2.76, p < 0.05) butnot women (adjusted OR = 1.52, p = 0.46). The preva-lence of heart disease was higher in hypertensives thanin nonhypertensives, but the association was not statis-
45
40
35 -
30 -
ID 25 -u0« 20 -I
15 -
10 -
5 -
0
Diabetic
Nondiabetic
MEN
Age-adjustedodds ratio = 4 0095% Cl 2.03 - 7.89
Age-adjustedodds ratio = 2.7695% Cl 1.15-6.62
I
WOMEN
Age-adjustedodds ratio = 2 7895% Cl 1.69-4.58
Age-adjustedodds ratio = 1 5295% CIO 50 -4 .60
Hypertension Heart disease Hypertension Heart disease
FIGURE 1. Prevalence (percentages) of hypertension and heart disease in diabetic and nondiabetic men and women who participated in theSan Antonio Family Heart Study, San Antonio, Texas, 1992-1996. Odds ratios, adjusted for age by using multiple logistic regression, and their95% confidence intervals (Cl) are also shown.
Am J Epidemiol Vol. 149, No. 11, 1999

Diabetes, Hypertension, and Cardiovascular Risk in Families 1051
tically significant in either men (adjusted OR = 2.25, p =0.11) or women (adjusted OR = 2.19, p = 0.16).
The distribution of cardiovascular risk factors innondiabetic subjects, according to a parental history ofdiabetes, is shown in table 2. In men, those with aparental history of diabetes had a significantly higherbody mass index and subscapular-triceps ratio, a sig-nificantly larger waist circumference, and significantlyhigher serum leptin concentrations and triglyceridelevels (p < 0.05 for each comparison). In women, aparental history of diabetes was associated with signif-icantly higher levels of fasting (p< 0.01) and 2-hour (p< 0.001) glucose, fasting (p < 0.05) and 2-hour (p <0.01) insulin, and triglycerides (p < 0.01); a signifi-cantly higher body mass index (p < 0.001) and waist-hip ratio (p < 0.01); a significantly larger waist cir-cumference (p < 0.001); a significantly smaller LDLsize (p < 0.05); and significantly lower concentrationsof Lp(a) (p < 0.05).
The distribution of cardiovascular risk factors innonhypertensive subjects with and without a parentalhistory of hypertension is shown in table 3. Men whohad a parental history of hypertension had significant-ly higher concentrations of leptin (p < 0.05), whilewomen with a parental history of hypertension had sig-nificantly higher systolic blood pressure (p < 0.01) andtriglyceride levels (p < 0.05). Two-hour insulin con-centrations were also significantly lower in women
with a parental history of hypertension than in thosewithout such a history (p < 0.05).
The distribution of cardiovascular risk factors insubjects free of overt heart disease, with and without aparental history of heart disease, is shown in table 4.For men, fasting insulin and apolipoprotein B concen-trations were significantly lower in those with a posi-tive parental history compared with those without sucha history; for women, those with a positive parentalhistory had significantly higher levels of fastinginsulin (p < 0.05), a significantly higher body massindex (p < 0.001), a significantly larger waist circum-ference (p < 0.05), and significantly lower concentra-tions of Lp(a) (p < 0.01).
The results of the variance component analyses areshown in table 5. The family history scores rangedfrom -11 to 5 for diabetes, -13 to 3 for hypertension,and -13 to 2 for heart disease. Diabetes family historyscore was significantly correlated with fasting and 2-hour glucose (p < 0.001 for both), fasting (p < 0.05)and 2-hour (p < 0.001) insulin, and several differentmeasures of obesity, including body mass index (p <0.01), waist circumference (p < 0.01), leptin concen-trations (p < 0.05), and waist-hip ratio (p < 0.05).Diabetes family history score was also significantlycorrelated with both systolic and diastolic blood pres-sure (p < 0.05), higher concentrations of total choles-terol (p < 0.05) and triglycerides (p < 0.01), and lower
TABLE 2. Age-adjusted levels of cardiovascular risk factors in nondiabetic subjects with and without aparental history of diabetes, the San Antonio Family Heart Study, San Antonio, Texas, 1992-1996
Riskfactor
Fasting glucose (mg/dl)2-hour glucose (mg/dl)In (fasting insulin (|itl/ml))In (2-hour insulin (|iU/ml))Leptin (ng/ml)Body mass index (kg/m2)Waist circumference (cm)Waist-hip ratioSubscapular-triceps ratioSystolic blood pressure (mmHg)Diastolic blood pressure (mmHg)Total cholesterol (mg/dl)HDLt cholesterol (mg/dl)Apolipoprotein A-l (mg/dl)Apolipoprotein A-ll (mg/dl)Apolipoprotein B (mg/dl)In (triglycerides (mg/dl))In (lipoprotein(a) (mg/dl))Median LDLt size (nm)
No parentalhistory(n = 82)
85.889.82.313.567.3
25.889.0
0.9031.705
117.269.3
175.648.4
136.957.6
105.24.661.94
26.68
Men
Confirmedparental history
(n= 137)
88.694.72.293.68
10.0*27.8*93.3*
0.9171.909*
118.071.0
182.245.3
134.857.7
111.44.85*2.00
26.52
No parentalhistory
(n=108)
82.592.62.183.84
25.627.085.3
0.8231.185
109.066.9
181.852.7
144.056.7
106.84.542.49
26.88
Women
Confirmedparental history
(n=178)
86.1**106.0***
2.39*4.12**
28.730.5***93.6***0.855**1.279
111.468.6
181.550.7
144.256.3
106.84.72**2.14*
26.77*
* p< 0.05; ** p < 0.01; *** p < 0.001.t HDL, high density lipoprotein; LDL, low density lipoprotein.
Am J Epidemiol Vol. 149, No. 11, 1999

1052 Mitchell et al.
TABLE 3. Age-adjusted levels of cardiovascular risk factors in nonhypertensive subjects with andwithout a parental history of hypertension, the San Antonio Family Heart Study, San Antonio, Texas,1992-1996
Risk
factor
Fasting glucose (mg/dl)2-hour glucose (mg/dl)In (fasting insulin (n.U/ml))In (2-hour insulin (nil/ml))Leptin (ng/ml)Body mass index (kg/m2)Waist circumference (cm)Waist-hip ratioSubscapular-triceps ratioSystolic blood pressure (mmHg)Diastolic blood pressure (mmHg)Total cholesterol (mg/dl)HDLf cholesterol (mg/dl)Apolipoprotein A-l (mg/dl)Apolipoprotein A-ll (mg/dl)Apolipoprotein B (mg/dl)In (triglycerides (mg/dl))In (lipoprotein(a) (mg/dl))Median LDLf size (nm)
No parentalhistory
(n=124)
96.0112.0
2.243.567.6
26.791.30.9181.750
117.070.2
182.247.0
136.959.0
110.44.822.12
26.58
Men
Confirmedparental history
(n=116)
98.2106.3
2.343.58
10.3*28.094.00.9161.899
120.071.6
185.448.1
139.057.3
113.74.801.74
26.59
No parentalhistory
(77=131)
88.0106.8
2.354.10
26.428.889.20.8371.252
110.167.7
181.150.9
143.256.9
107.54.612.22
26.77
Women
Confirmedparental history
(n=163)
95.7122.4
2.293.88*
26.029.291.30.8551.232
113.6**69.5
187.153.2
148.657.5
109.64.74*2.25
26.77
* p < 0.05; * * p < 0.01.t HDL, high density lipoprotein; LDL, low density lipoprotein.
TABLE 4. Age-adjusted levels of cardiovascular risk factors in subjects free of overt heartdisease, with and without a parental history of overt heart disease, the San Antonio FamilyHeart Study, San Antonio, Texas, 1992-1996
Risk
factor
Fasting glucose (mg/dl)2-hour glucose (mg/dl)In (fasting insulin (n.U/ml))In (2-hour insulin (nil/ml))Leptin (ng/ml)Body mass index (kg/m2)Waist circumference (cm)Waist-hip ratioSubscapular-triceps ratioSystolic blood pressure (mmHg)Diastolic blood pressure (mmHg)Total cholesterol (mg/dl)HDLt cholesterol (mg/dl)Apolipoprotein A-l (mg/dl)Apolipoprotein A-ll (mg/dl)Apolipoprotein B (mg/dl)In (triglycerides (mg/dl))In (lipoprotein(a) (mg/dl))Median LDLt size (nm)
No parentalhistory
(n =161)
96.9110.5
2.363.589.3
27.493.0
0.9161.819
117.469.9
183.146.0
136.858.2
113.24.841.96
26.57
Men
Confirmedparental history
(n = 38)
98.9112.3
2.04*3.338.6
27.590.40.8971.728
119.670.7
176.848.7
134.054.6
101.5*4.731.65
26.66
No parentalhistory
(n=187)
89.4107.7
2.253.89
25.828.088.4
0.8401.261
109.867.8
179.352.0
145.656.6
104.04.612.35
26.82
Women
Confirmedparental history
(n = 45)
90.0114.2
2.50*4.13
30.731.8***95.0*0.8391.183
111.266.9
186.651.9
140.655.6
110.84.661.69**
26.86
* p < 0.05; ** p < 0.01; *** p < 0.001.t HDL, high density lipoprotein; LDL, low density lipoprotein.
Am J Epidemiol Vol. 149, No. 11, 1999

Diabetes, Hypertension, and Cardiovascular Risk in Families 1053
TABLE 5. Linear regression coefficientst representing the effects of family history scores for diabetes,hypertension, and heart disease on cardiovascular risk factors, the San Antonio Family Heart Study,San Antonio, Texas, 1992-1996
Risk factor(dependent variable)
Fasting glucose (mg/dl)2-hour glucose (mg/dl)In (fasting insulin (|iU/ml))In (2-hour insulin (u.U/ml))Leptin (ng/ml)Body mass index (kg/m2)Waist circumference (cm)Waist-hip ratioSubscapular-triceps ratioSystolic blood pressure (mmHg)Diastolic blood pressure (mmHg)Total cholesterol (mg/dl)HDLt cholesterol (mg/dl)Apolipoprotein A-l (mg/dl)Apolipoprotein A-ll (mg/dl)Apolipoprotein B (mg/dl)In (triglycerides (mg/dl))In (lipoprotein(a) (mg/dl))Median LDLt size (nm)
Diabetes
0.90***2.63***0.035*0.084***0.35*0.35**1.03**0.004*0.0140.66*0.44*1.63*
-0.14-0.19
0.280.860.034**
-0.075*0.022
Family history score
Hypertension
1.15*2.96*0.0200.0300.240.25*0.71*0.0020.0060.79**0.53**1.72*0.13
-0.160.080.920.021*
-0.073*0.019
Heart disease
1.12*1.970.0180.041*0.210.210.56*0.001
-0.0060.420.111.140.08
-0.44-0.03
0.400.010
-0.077**0.011
* p < 0.05; ** p < 0.01; *** p < 0.001.t Adjusted for age, age squared, sex, education, alcohol consumption, smoking, menopausal status, oral
contraceptive use, and postmenopausal estrogen use.$ HDL, high density lipoprotein; LDL, low density lipoprotein.
concentrations of Lp(a) (p < 0.05). Hypertension fam-ily history score was significantly correlated withhigher concentrations of fasting and 2-hour glucose,serum total cholesterol, and triglycerides (p < 0.05 foreach); higher systolic and diastolic blood pressure (p <0.01) and body mass index (p < 0.05); a larger waistcircumference (p < 0.05); and lower concentrations ofLp(a) (p < 0.05). Family history scores for heart dis-ease were significantly correlated with higher fastingglucose (p < 0.05) and 2-hour insulin (p < 0.05) levels,a larger waist circumference (p < 0.05), and lower con-centrations of Lp(a) (p < 0.01). For none of these vari-ables was there any evidence of an interaction betweensex and family history score.
DISCUSSION
A major conclusion of this study is that a family his-tory of type 2 diabetes, and to a lesser extent hyper-tension, is associated with an atherogenic cardiovascu-lar risk profile, as reflected by greater adiposity, highertriglyceride and total cholesterol concentrations, andelevated blood pressure. This atherogenic profile isapparent even for unaffected persons in the pedigree,only some of whom will presumably develop overtdiabetes and/or hypertension. These results are notunexpected, since many previous studies have shown
that nondiabetic relatives of diabetics are insulin resis-tant (2-8). Indeed, the associations that we found prob-ably can be considered a manifestation of the multiplemetabolic syndrome. However, few studies havedemonstrated the extent of the atherogenic changesthat we observed, nor have they evaluated the impactof the multiple metabolic syndrome within a popula-tion-based sample of families.
The heritability of the cardiovascular risk factors thatwe analyzed in this study is moderately high (15,24). Ina previous study of this Mexican American population,we estimated that the additive effects of genes (i.e.,poly genes) accounted for 18^46 percent of the pheno-typic variance in glucose, insulin, blood pressure, adi-posity, and concentrations of various lipid and lipopro-tein measures; in contrast, age, sex, and other covariatesaccounted for generally less than 5 percent of the totalvariance in these traits (15). In the present study, theassociations we observed between a family history ofdiabetes and many of these risk factors are consistentwith the commonly held idea that the genes that influ-ence variation in cardiovascular risk factors ultimatelyinfluence the risk for overt disease. If true, then identi-fication of such genes may lead to insights about futuredirections for therapy and disease prevention.
The correlations in these data between a family his-tory of diabetes and obesity are particularly striking.
Am J Epidemiol Vol. 149, No. 11, 1999

1054 Mitchell et al.
An elevated body mass index and a parental history ofdiabetes have long been recognized as important riskfactors for type 2 diabetes. The independent contribu-tions of these two risk factors to diabetes risk weredefinitively demonstrated by Knowler et al., whoshowed that diabetes incidence in Pima Indiansincreased with increasing levels of body mass indexindependently of whether one or both parents wereaffected and, conversely, that at any given level ofbody mass index, diabetes incidence increased with anincreasing number of diabetic parents (from 0 to 1 to2) (25). The one exception to this trend was that bodymass index was not associated with diabetes incidencein subjects who did not have a parental history ofdiabetes. More recently, Hanson et al. observed thatdiabetes prevalence was higher in offspring of lean dia-betics than in offspring of heavy diabetics, and theyhypothesized that a higher genetic load was requiredfor a lean person to become diabetic (26). Many haveused these observations to reinforce the belief thatbody mass index and a family history of diabetes areetiologically distinct risk factors. However, this inter-pretation may be at least partially incorrect, sincecommon genes may predispose to both diabetes andobesity. In other words, obesity should be regarded aspart of the pathogenic process of diabetes, and it maybe equally as valid to consider that persons becomeobese because they have inherited diabetes suscepti-bility genes as it is to consider that they become dia-betic because they get fat.
Because it is largely unknown which genes influ-ence both obesity and diabetes risk, it is difficult toproject the relative importance of pleiotropic genes inthe etiology of these disorders. However, recent resultsfrom the Pima Diabetes Genes Group suggest thatsome pleiotropic genes may have relatively majoreffects on both traits. In a genome-wide screen to iden-tify genes for susceptibility to diabetes and relatedtraits, these investigators have used linkage analysis tomap a locus to the long arm of chromosome 11 thatinfluences both susceptibility to diabetes and, in non-diabetic persons, variation in body mass index (27).
In our data, a family history of hypertension was high-ly correlated with systolic and diastolic blood pressurebut only weakly correlated with (a few) other cardiovas-cular risk factors. We interpret this finding to indicatethat the pleiotropic effects of hypertension susceptibilitygenes on other cardiovascular risk factors are relativelyweak. Supporting this interpretation is the fact that theepidemiologic evidence for an association betweenhypertension and insulin resistance, at least in MexicanAmericans and Pima Indians, is relatively weak (28-30).Moreover, we previously reported from our own studythat the genetic correlation (which reflects the degree of
pleiotropy) for insulin concentrations with body massindex, high density lipoprotein cholesterol, and triglyc-eride concentrations is much higher than it is for insulinconcentrations with blood pressure (31).
The association of a family history of cardiovasculardisease with cardiovascular risk factors was not strongin our study. The most likely explanation is that weused a relatively crude definition of cardiovascular dis-ease that relied on a self-reported history of heartattack and/or heart surgery, and we were unable to ver-ify disease endpoints. Furthermore, the sensitivity ofour case definition was low, further reducing ourpower to detect associations. It is possible that addi-tional associations would have been identified had webroadened our case definition to include subclinicalmeasures of atherosclerotic vessel disease, such asthose obtained from ultrasonography of the carotidarteries or electron-beam computed tomography of thecoronary arteries.
The inverse association between diabetes family his-tory score and Lp(a) agrees with our earlier studies thatreported significantly lower Lp(a) concentrations indiabetic subjects (32, 33). More recently, we foundthat Lp(a) concentrations are inversely correlated withserum insulin concentrations (34). However, the obser-vation that Lp(a) concentrations were inversely corre-lated with family history scores for cardiovascular dis-ease was unexpected, since most studies report apositive association between Lp(a) and cardiovasculardisease (35, 36) or no association at all (37, 38).However, the frequency of insulin resistance is high inthis population, and the inverse association betweenLp(a) and a family history of heart disease may be sec-ondary to insulin resistance. Supporting this interpre-tation is the fact that in this population, 2-hour insulinconcentrations were also inversely associated withfamily history score for heart disease.
The impact of diabetes on cardiovascular risk is dis-proportionately worse for diabetic women than for dia-betic men; the risk for cardiovascular mortality isincreased threefold to fourfold in diabetic women butonly twofold in diabetic men (39). In a longitudinalstudy of Mexican Americans also from San Antonio,Haffner et al. extended these observations to show thatprediabetic women have a relatively more atherogeniccardiovascular risk profile than prediabetic men do, asreflected by their concentrations of fasting insulin,triglycerides, and high density lipoprotein cholesteroland by their diastolic blood pressure (40). However,our study found no evidence that a family history ofdiabetes was more strongly correlated with cardiovas-cular risk in women than in men.
The prevalence of type 2 diabetes is increasingrapidly in the United States, particularly in low-income
Am J Epidemiol Vol. 149, No. 11, 1999

Diabetes, Hypertension, and Cardiovascular Risk in Families 1055
ethnic populations such as Mexican Americans (41).The cause of this rapid increase has been attributed tobehavioral changes, including an increase in sedentarylifestyle, with diabetes risk accentuated in those whohave an underlying genetic susceptibility (42). Anoverlooked consequence of this diabetes epidemicmay be an accompanying increase in cardiovascularrisk that will occur even in many who will neverdevelop overt diabetes. Although some studies haveobserved a paradoxical lower prevalence of cardiovas-cular disease in Mexican Americans (in whom diabetesand obesity occur relatively frequently) compared withnon-Hispanic Whites (43), other studies have suggestedthat the burden of cardiovascular disease actually maybe higher in Mexican Americans. For example, in theCorpus Christi Heart Project, the incidence of personshospitalized with myocardial infarction was 1.5 and1.3 times higher in Mexican American women andmen, respectively, than in their non-Hispanic Whitecounterparts (44). The discrepancy between the resultsof these prevalence and incidence studies is possiblyexplained by a lower survival rate among MexicanAmericans with cardiovascular disease, as suggestedby the observation that 28-day case fatality amongthose in the Corpus Christi Heart Project who werehospitalized for a definite or possible myocardialinfarction was 1.5 times higher in Mexican Americansthan in non-Hispanic Whites (45).
In summary, we detected significant associationsbetween a family history of diabetes, and to a lesserextent hypertension, and a range of cardiovascular riskfactors. These associations probably reflect thepleiotropic effects of genes that are transmitted fromaffected persons to their offspring. In populations suchas Mexican Americans, in whom the incidence of dia-betes is increasing rapidly, there is likely to be anaccompanying increase in cardiovascular risk.
ACKNOWLEDGMENTS
This work was supported by grant PO1-HL45522 fromthe National Institutes of Health.
REFERENCES
1. National Center for Health Statistics. Health, United States,1996-97. Hyattsville, MD: Public Health Service, 1997.
2. Eriksson J, Franssila-Kallunki A, Ekstrand A, et al. Earlymetabolic defects in persons at increased risk for non-insulin-dependent diabetes mellitus. N Engl J Med 1989;321:337-43.
3. Elbein SC, Maxwell TM, Schumacher MC. Insulin and glu-cose levels and prevalence of glucose intolerance in pedigreeswith multiple diabetic siblings. Diabetes 1991;40:1024-32.
4. Gulli G, Ferrannini E, Stem MP, et al. The metabolic profile ofNIDDM is fully established in glucose-tolerant offspring oftwo Mexican-American NIDDM parents. Diabetes 1992;41:1575-86.
5. Haffner SM, Stem MP, Hazuda HP, et al. Increased insulinconcentrations in nondiabetic offspring of diabetic parents.N Engl J Med 1988;319:1297-301.
6. Ho LT, Chang ZY, Wang JT, et al. Insulin insensitivity in off-spring of parents with type 2 diabetes mellitus. Diabet Med1 9 9 0 7 3 1 t
7. Laws A, Stefanick ML, Reaven GM. Insulin resistance andhypertriglyceridemia in nondiabetic relatives of patients withnon-insulin-dependent diabetes mellitus. J Clin EndocrinolMetab 1989;69:343-7.
8. Stewart MW, Humphriss DB, Berrish TS, et al. Features ofsyndrome X in first-degree relatives of NIDDM patients.Diabetes Care 1995;18:1020-2.
9. Beatty OL, Harper R, Sheridan B, et al. Insulin resistance inoffspring of hypertensive parents. BMJ 1993;307:92-6.
10. Ferrari P, Weidmann P, Shaw S, et al. Altered insulin sensitiv-ity, hyperinsulinemia, and dyslipidemia in individuals with ahypertensive parent. Am J Med 1991 ;91:589-96.
11. Facchini F, Chen YD, Clinkingbeard C, et al. Insulin resis-tance, hyperinsulinemia, and dyslipidemia in nonobese indi-viduals with a family history of hypertension. Am J Hypertens1992;5:694-9.
12. Grunfeld B, Balzareti M, Romo M, et al. Hyperinsulinemia innormotensive offspring of hypertensive parents. Hypertension1994;23(suppl):I12-15.
13. McPhillips JB, Barrett-Connor E, Wingard DL. Cardiovasculardisease risk factors prior to the diagnosis of impaired glucosetolerance and non-insulin-dependent diabetes mellitus in acommunity of older adults. Am J Epidemiol 1990; 131:443—53.
14. Haffner SM, Stem MP, Hazuda HP, et al. Cardiovascular riskfactors in confirmed prediabetic individuals. Does the clockfor coronary heart disease start ticking before the onset of clin-ical diabetes? JAMA 1990;263:2893-8.
15. Mitchell BD, Kammerer CM, Blangero J, et al. Genetic andenvironmental contributions to cardiovascular risk factors inMexican Americans: the San Antonio Family Heart Study.Circulation 1996;94:2159-70.
16. Singh ATK, Rainwater DL, Haffner SM, et al. Effect of dia-betes on lipoprotein size. Arterioscler Thromb Vase Biol1995;15:1805-ll.
17. Rainwater DL, Moore PH Jr, Shelledy WR, et al.Characterization of a composite gradient gel for the elec-trophoretic separation of lipoproteins. J Lipid Res 1997;38:1261-6.
18. Campos H, Blijlevens E, McNamara JR, et al. LDL particlesize distribution: results from the Framingham OffspringStudy. Arterioscler Thromb 1992;12:1410-19.
19. Tchernof A, Moorjani S, Lamarche B, et al. The dense LDLphenotype. Association with plasma lipoprotein levels, visceralobesity, and hyperinsulinemia in men. Diabetes Care 1996;19:629-37.
20. World Health Organization Expert Committee. Second reporton diabetes mellitus. Geneva, Switzerland: World HealthOrganization, 1980. (Technical report series, no. 646).
21. Bonney GE. Regressive logistic models for familial diseaseand other binary traits. Biometrics 1986;42:611—25.
22. Lange K, Weeks DE, Boehnke M. Programs for pedigreeanalysis: MENDEL, FISHER, and dGENE. Genet Epidemiol1988;5:471-2.
23. Edwards AWF. Likelihood. Expanded ed. Baltimore, MD: TheJohns Hopkins University Press, 1992.
24. Peyser PA. Genetic epidemiology of coronary artery disease.Epidemiol Rev 1997; 19:80-90.
25. Knowler WC, Pettitt DJ, Savage PJ, et al. Diabetes incidencein Pima Indians: contributions of obesity and parental diabetes.Am J Epidemiol 1981;113:144-56.
26. Hanson RL, Pettitt DJ, Bennett PH, et al. Familial relation-ships between obesity and NIDDM. Diabetes 1995;44:418-22.
27. Hanson R. The Pima Diabetes Genes Group. Genomic scan for
Am J Epidemiol Vol. 149, No. 11, 1999

1056 Mitchell et al.
markers linked to type II diabetes in Pima Indians. (Abstract).Diabetes 1997;46(suppl 1):51A.
28. Saad MF, Knowler WC, Pettitt DJ, et al. Insulin and hyper-tension. Relationship to obesity and glucose intolerance inPima Indians. Diabetes 1990;39:1430-5.
29. Saad MF, Lillioja S, Nyomba BL, et al. Racial differences inthe relation between blood pressure and insulin resistance. NEngl J Med 1991;324:733-9.
30. Mitchell BD, Haffner SM, Hazuda HP, et al. The relationbetween serum insulin levels and 8-year changes in lipid,lipoprotein, and blood pressure levels. Am J Epidemiol1992;136:12-22.
31. Mitchell BD, Kammerer CM, Mahaney MC, et al. Geneticanalysis of the IRS. Pleiotropic effects of genes influencinginsulin levels on lipoprotein and obesity measures.Arterioscler Thromb Vase Biol 1996;16:281-8.
32. Rainwater DL, MacCluer JW, Stern MP, et al. Effects ofNIDDM on lipoprotein(a) concentration and apolipoprotein(a)size. Diabetes 1994;43:942-6.
33. Rainwater DL, Kammerer CM, VandeBerg JL, et al.Characterization of the genetic elements controlling lipopro-tein(a) concentrations in Mexican Americans. Evidence for atleast three controlling elements linked to LPA, the locus encod-ing apolipoprotein(a). Atherosclerosis 1997;128:223—33.
34. Rainwater DL, Haffner SM. Insulin and 2-hour glucose levelsare inversely related to Lp(a) concentrations controlled for LPAgenotype. Arterioscler Thromb Vase Biol 1996; 18:1335^1.
35. Hajjar KA, Nachman RL. The role of lipoprotein(a) in athero-genesis and thrombosis. Annu Rev Med 1996;47:423^2.
36. Kronenberg F, Steinmetz A, Kostner GM, et al. Lipoprotein(a)in health and disease. Crit Rev Clin Lab Sci 1996;33:495-543.
37. Jauhiainen M, Koskinen P, Ehnholm C, et al. Lipoprotein (a)and coronary heart disease risk: a nested case-control study ofthe Helsinki Heart Study participants. Atherosclerosis 1991;89:59-67.
38. Ridker PM, Hennekens CH, Stampfer MJ. A prospectivestudy of lipoprotein(a) and the risk of myocardial infarction.JAMA 1993;270:2195-9.
39. Mitchell BD. Macrovascular disease in diabetes. In: LeslieRDG, Robbins DC, eds. Diabetes: clinical science in practice.Cambridge, United Kingdom: Cambridge University Press,1995:222-36.
40. Haffner SM, Miettinen H, Stern MP. Relatively more athero-genic coronary heart disease risk factors in prediabetic womenthan in prediabetic men. Diabetologia 1997;40:711-17.
41. Centers for Disease Control and Prevention. Trends in theprevalence and incidence of self-reported diabetes mellitus—United States, 1980-1994. JAMA 1997;278:1564-5.
42. Groop LC, Tuomi T. Non-insulin-dependent diabetes melli-tus—a collision between thrifty genes and an affluent society.Ann Med 1997;29:37-53.
43. Mitchell BD, Hazuda HP, Haffner SM, et al. Myocardialinfarction in Mexican Americans and non-Hispanic whites:the San Antonio Heart Study. Circulation 1991;83:45-51.
44. Goff DC, Nichaman MZ, Chan W, et al. Greater incidence ofhospitalized myocardial infarction among Mexican Americansthan non-Hispanic whites. The Corpus Christi Heart Project,1988-1992. Circulation 1997;95:1433-40.
45. Goff DC Jr, Ramsey DJ, Labarthe DR, et al. Greater case-fatality after myocardial infarction among Mexican Americansand women than among non-Hispanic whites and men. TheCorpus Christi Heart Project. Am J Epidemiol 1994;139:474-83.
Am J Epidemiol Vol. 149, No. 11, 1999