Surveillance Guidelines for Smallpox Vaccine (vaccinia) Adverse

CHAPTER 7
DEVELOPMENTS INVACCINATION AND CONTROL
BETWEEN 1900 AND 1966
Contents
INTRODUCTION
By the year 1900 vaccination was inwidespread use throughout the industrializedcountries as well as in some cities in what werethen the colonies of various Europeanpowers. Although variolation was no longerpractised in Europe and North America, itwas still widely employed in many parts ofAfrica and Asia . Smallpox persisted as anendemic disease in virtually every country ofthe world (see Chapter 8, Fig. 8 .16), althoughits incidence in the industrialized countrieswas lower than in previous centuries .
277
The latter half of the 19th century saw theemergence of microbiology and immunologyas scientific disciplines . Because of theirfamiliarity with vaccination, many of thepioneers in these new sciences used vacciniavirus for their studies (see Chapter 2) . Inconsequence, the empirical practices of Jennerand his early followers were placed on a morescientific basis . Vaccine production was nolonger the province of the local physician,who had maintained the virus by arm-to-armtransmission, and small local "vaccine parks",but was taken over by factory-type lab-oratories, the precursors of the great bio-
Page
Introduction 277Vaccine production and quality control before 1967 278
Production of vaccine lymph 279Preparation of liquid vaccine 282Preparation of dried vaccine 283Quality control 289
Vaccination techniques before 1967 291Vaccination site 291Methods of vaccination 292Age for primary vaccination 293Interpretation of the results of vaccination 294
Complications of vaccination 296Types of complication 299Frequency of complications 302Contraindications to vaccination 307Prevention and treatment of complications 308Reconsideration of vaccination policies in non-endemic
countries 309Complications : the overall picture 310
Programmes for vaccination and revaccination 311Vaccination and revaccination of the general public 311Simultaneous vaccination with several antigens 311Vaccination of international travellers 312

278
logical products supply houses of the 20thcentury .
There was a steady improvement in thequality of the vaccine, the methods for itsdistribution, and the public health infrastruc-ture, which had reached such a level that bythe early 1950s endemic smallpox had beeneliminated from the industrialized countriesof Europe and North America (see Chapter 8) .In the decade after the end of the SecondWorld War, several major advances weremade in the production and methods ofdelivery of the vaccine, but further changeand innovation were necessary before globaleradication was feasible. This chapter sum-marizes the state of the art of vaccine produc-tion and inoculation, and the results ofinvestigations into the complications of vac-cination, as these stood in the period betweenthe end of the Second World War and 1967,when the Intensified Smallpox EradicationProgramme was initiated .During the middle years of the 20th
century quarantine measures, which had ear-lier operated on a national basis in somecountries (see Chapter 6), were elaborated andapplied on a global scale, with the develop-ment of the International Health Regulationsby the World Health Organization . The
SMALLPOX AND ITS ERADICATION
Cowpox Virus and Vaccinia Virus
All orthopoxviruses exhibit cross-protection in laboratory animals . Among theorthopoxviruses that infect humans, cowpox and vaccinia viruses usually produce onlylocal lesions, with minimal systemic disturbance, whereas variola and monkeypox virusescause serious systemic diseases . Jenner's original "variolae vaccinae" was cowpox virus, andduring the 19th century, on many occasions, virus for vaccination was derived from lesionsin cows and sometimes horses in several European countries . Since the description of thebiological characteristics of cowpox virus by Downie (1 939a,b), it has been recognized thatsmallpox vaccines in use then, and probably for many years before the 1930s, consisted notof cowpox virus, but of another orthopoxvirus which had long been called "vaccine virus",but was shown by Downie to have biological properties different from those of cowpoxvirus (see Chapter 2) . Although some smallpox vaccines were still said to be made fromcowpox virus during the 1960s, it is doubtful, in the light of evidence from contemporaryvirological studies, whether this was so .
The origins of vaccinia virus are unknown . It may have arisen as a hybrid betweencowpox virus and variola virus, it may have been derived from cowpox virus or some otherorthopoxvirus by serial passage under artificial conditions of culture, or, as Baxby (1981)has suggested, it may be the laboratory survivor of a virus that is now extinct in nature .Whatever its origin, vaccinia virus is clearly a distinct species of Orthopoxvirus, and DNAmaps of different strains of vaccinia virus are remarkably similar to each other anddifferent from those of all other orthopoxviruses, including cowpox and variola virus (seeChapter 2, Fig. 2.7, 2 .9 and 2 .10, and Chapter 29, Fig . 29.1). However, like cowpox virus inthe hands of Jenner and his followers, it provided inoculated subjects with a high degree ofprotection against smallpox, with little risk to either the individual or the community .
present chapter concludes with an account ofthe introduction and eventual demise, in1981, of the International Certificate ofVaccination or Revaccination againstSmallpox.
VACCINE PRODUCTION ANDQUALITY CONTROL BEFORE 1967
Jennerian vaccination was the tool withwhich the incidence of smallpox was reducedand the disease eliminated from many coun-tries of Europe and the Americas during thefirst half of the 20th century. However, atsome time during the 19th century, forreasons which are obscure, the nature of thevirus used for vaccination changed, in mostparts of the world, from cowpox virus toanother orthopoxvirus, which came to beknown as vaccinia virus.
As scientific virology developed during the20th century, it was applied to the study ofsmallpox vaccine and vaccination, and newmethods of preparing, distributing and ino-culating the vaccine were developed. Thedescriptions which follow refer to the bestmethods and procedures in use for vaccineproduction before 1967. However, because

I
7 . DEVELOPMENTS IN VACCINATION AND CONTROL, 1900-1966
smallpox vaccine was produced in manycountries, in which there were wide differ-ences in the degree of scientific and industrialexperience and skill, the procedures employedin some countries were much less satisfactorythan those described here . Modifications totraditional production and assay methods,and most important the internationalquality control of vaccines, were introducedshortly after the Intensified Smallpox Eradi-cation Programme began operations in 1967(see Chapter 11) .
Production of Vaccine Lymph
During the first half of the 19th centuryvaccine was usually made available by arm-to-arm transfer but was sometimes dispatchedover long distances dried on threads, ivorytips, or glass slides (see Chapter 6) . Cows werefirst used for the production of vaccine inItaly early in the 19th century ; this practicegradually spread around Europe and wasuniversal by the end of the century. Over theyears, changes were made in the mode ofpreparation of both liquid and dried vaccine,but the initial production of vaccine pulp wasthe same for each .
Choice of vaccinifer
For historical reasons, calves were first usedfor vaccine production. During the First
Vaccine Pulp and Vaccine Lymph
By the end of the 19th century arm-to-arm vaccination had been made illegal in manycountries and smallpox vaccine was obtained from animal skin. However, technicalknowledge of vaccine production was still extremely poor . For example, even in anadvanced industrialized country it was recommended that seed lymph could be obtainedfrom (1) "smallpox direct", (2) cowpox, (3) horsepox, sheep-pox, goatpox, swinepox, or (4)vaccinia in the human body (England and Wales, Ministry of Health, 1928a) .
Looked at with modern eyes, the production of smallpox vaccine, even in 1966, was aprimitive operation. The method of production, in animal skin, made bacterialcontamination inevitable, something that would not have been tolerated in a new viralvaccine in the 1950s .
A number of traditional expressions were used to describe the product obtained atdifferent stages of the process : the animal in which the vaccine was produced was called thevaccinifer, the material used for its inoculation the seed, the material reaped from the scarifiedskin the vaccine pulp, and the clarified suspension obtained from this the vaccine lymph. Thepulp was a mixture of epidermal cells and leukocytes, plasma, hair, bacteria and the virus .Clarification removed some of the coarser debris, but the vaccine lymph was milky inappearance on account of contamination with fragments of cells and bacteria . Purifiedvirus, at the concentration found in the lymph, would have been a water-clear suspension .
279
World War, the Lister Institute of PreventiveMedicine, in Elstree, Hertfordshire, England,introduced the use of sheep, a practice subse-quently adopted in some other countries .Because of their ready availability, water-buffaloes were sometimes used in India,Indochina and Indonesia, and W . A. Collier(1953) considered them to be superior toother species for vaccine production . At-tempts were made in several countries toproduce smallpox vaccine in chick embryosand in cultured cells, to avoid the bacterialcontamination that was inevitable when pro-duction was carried out by scarification of theskin of large animals . However, chick embryovaccines were produced on a commercial scaleonly in Brazil, Sweden and the state of Texasin the USA, and only in Brazil were they inwidespread use in an eradication campaign(see Chapter 12) . Except on a very limitedscale, tissue culture vaccines were neverproduced commercially.
During the 1920s the concept was de-veloped that biological products prepared foruse in man should be bacteriologically sterile .Legislation was introduced in some of theindustrialized countries to regulate the pro-duction of vaccines and similar products . Atthat time smallpox vaccine grown on theflank of calves was already in wide use .Inevitably, it contained some bacteria, butthere was no other practicable method ofproduction . Thus smallpox vaccine was the

280
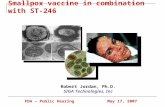
Plate 7 .1 . The preparation of smallpox vaccine at the Vaccine Production Institute, Dhaka, Bangladesh .A: Calves to be used for vaccination were held in quarantine for 7 days. B: Four days after scarification, theskin was scraped with a sharpened stainless-steel spoon and the vaccine pulp collected in a jar, for subsequentgrinding and centrifugation to yield the vaccine lymph .
only vaccine for which both the public andthe health authorities accepted the fact ofcontamination by exogenous microorgan-isms. Since bacterial contamination was inevi-table, the aim in preparing vaccine lymph wasto exclude pathogenic bacteria completelyand reduce the level of contamination withthe normal skin bacteria of the vaccinifer .Choice of a healthy vaccinifer was clearly ofmajor importance. The requisite veterinaryinspection was practised in some countries,but in others animals were bought in themarket, or even rented to be returned after-wards to their owners . This last procedurecircumvented one of the important precau-tions recommended by producers in de-veloped countries-namely, that a thoroughpostmortem examination should be conduct-ed when the animal was killed at the end ofthe incubation period and the pulp discardedif serious disease was found .
Under optimum conditions, every animalused for vaccine production was subjected toan examination by a veterinarian to ensurethat it was free from tuberculosis, skininfection and ectoparasites . Only animalswhich had been free of fever and any sign ofdisease for at least 2 weeks were used, andduring this observation period the animalswere clipped and washed .
SMALLPOX AND ITS ERADICATION
Preparation of the vaccinifer
The proper preparation of the skin of thevaccinifer was one of the most importantsteps in obtaining a vaccine of low bacterialcontent. After being anaesthetized or tran-quillized, the animals were washed on an areaon the flank or belly, preferably one not liableto soiling by excretions, and then shavedextensively enough to permit a reasonablylarge area to be scarified. Some producerstreated the skin with an efficient skin disin-fectant, such as a quaternary ammoniumcompound, and before vaccination the pre-pared area was well rinsed with sterile dis-tilled water .
Scarication
The skin was prepared for vaccination byscarification, using the same principle as forthe vaccination of humans (see below)-namely, to bring the virus into contact withcells in the Malpighian layer of the epidermis .However, the operation was on a much largerscale, the aim being to produce a confluenttake on a large area of the flank and abdomen .The usual procedure was to make a series ofparallel scratches about 1 cm apart on thecleansed flank and abdomen of the vaccinifer,

7. DEVELOPMENTS IN VACCINATION AND CONTROL, 1900-1966
followed by a similar series of scratches atright angles to the first . A wide variety ofinstruments was used in different laborato-ries, sufficient force being exerted to produceobvious erythema of the skin, but not bleed-ing. The prepared skin was then inoculated byrubbing seed virus of high infectivity into thesuperficial scarifications. Practical consider-ations limited the extent of the area scarified,because in some countries animals in ratherpoor health were used, and too extensivescarification might have caused their death .
Two important features which were subjectto a great deal of variation in differentcountries, and sometimes even among differ-ent producers in the same country, were thechoice of the strain of vaccinia virus and themode of preparation and maintenance of theseed virus (see below) .
Incubation period
Methods of maintaining the vacciniferuntil the lesions were ready for harvestdiffered considerably . Ideally, the scarifiedarea was loosely covered with a cotton cloth,which was changed at least once each day . Inthe better laboratories, the pen in which theanimal was housed was so constructed that thevaccinated animal could not lie down . It hadwalls that could be washed frequently and ahard floor on which was placed a slattedwooden platform the length of the animal andsloping gently from front to back ; the penwas cleaned thoroughly and often. In somecountries, however, the vaccinifers werehoused in ordinary stables and sometimesthey were even turned out to pasture .
The pulp was harvested before crustsformed on the vaccinated area, at a time whenboth the viral titre and the quantity of pulpwere at their maximum. Workers at the ListerInstitute found in the 1920s that the viralyield was about the same on the 4th and 5thdays after inoculation, but preferred the 4-dayincubation period because the opportunityfor bacterial contamination and hair growthwas reduced by a day .
Harvest
The skin was rinsed with warm water, withor without soap, and the pulp was scrapedfrom the skin with a curette, one form ofwhich was made by sharpening the edge of ahemispherical stainless-steel spoon (Plate 7 .1B). If the animals were killed, exsanguination
281
before scraping ensured a less blood-stainedproduct ; if they were not killed, they wereusually anaesthetized before scraping . Har-vests from individual animals were keptseparately in sterile containers closed tightlyenough to prevent drying by evaporation,and stored below 0 °C except when beingprocessed .
Seed virus used for inoculation
The seed viruses used in various laborato-ries differed with regard to the strain of virusemployed and the titre of the inoculum, aswell as the methods by which they weremaintained.
Strain of vaccinia virus . With a procedurethat had been in use in many countries forover a hundred years, and with no effort atinternational standardization, it was not sur-prising that the strains of virus employed forvaccination in different countries differed intheir biological properties. The choice of aparticular strain was arbitrary, being basedon the history of the vaccine productionlaboratory concerned . An examination of thesituation in 1967 showed that many differentstrains were then in use (see Chapter 11) . Thiscan be understood when it is realized thatduring the 19th century vaccine productionwas an unregulated activity, undertaken by alarge number of "backyard" producers . Forexample, as A . C. Hekker has commented(personal communication, 1981), in 1875there were about 15 `parts vaccinogenes" in acountry as small as the Netherlands, with atleast 1 in every province . By 1900 the numberhad been reduced to 3 in Amsterdam, Gro-ningen and Rotterdam respectively. Finally,in 1954, production was centralized in theNational Institute of Public Health, Bilt-hoven. The situation was similar in manyother countries-for example, in Great Bri-tain, where lymph maintained by arm-to-arminoculation was used until the 1890s .
Since different strains of vaccinia virusvary considerably in their biological proper-ties (see Chapter 2) and since the properties ofthe viral strain were probably important indetermining the differences found in the ratesof occurrence of postvaccinial encephalitis indifferent countries (see Table 7.8), this wasnot a trivial matter. However, no steps weretaken to recommend internationally whichvaccinia strain should be used for vaccineproduction until after 1967 (see Chapter 11),although some countries in which postvac-

282
The Stability of Vaccinia Virus
Stocks of all viruses, even after cloning (i.e., being grown from a single plaque or pockand thus a single viral particle), contain a small proportion of mutant virions (see Chapter2). Most attenuated live virus vaccines were developed by selecting for certain of thesemutants by continued serial passage of concentrated viral suspensions in a novel host. Withan agent that was suitable to start with, such as vaccinia virus, the reverse sometimesoccurred. The early vaccinators believed that serial passage in humans "weakened" thevaccine, and they resorted to periodic "retrovaccination" i .e ., passage of the virus incows-to enhance its potency (see Chapter 6). Subsequently, some manufacturers observedthat continued serial passage in calves led eventually to a fall in the take rates of the vaccinein man, although others (e .g ., W. A. Collier, 1953) found that potency was maintainedthroughout 35 serial passages in water-buffaloes .
Manufacturers sought to overcome the fluctuations in potency by periodic passage ofthe seed virus in other animals, usually the rabbit but sometimes monkeys, donkeys or evenhuman subjects. These manipulations were rendered unnecessary by the development ofthe "seed lot" system .
cinial encephalitis had been a serious problemhad changed their production to the lesspathogenic Lister strain before this .
Titre of inoculum. All authorities agreed thatit was desirable to use an inoculum with ashigh a titre as possible. Two methods formeasuring the titre had been used after theSecond World War : scarification of the skinof a rabbit and pock counts on the chorioal-lantoic membrane of the chick embryo . Therabbit-skin assay, which consisted of a seriesof scarifications of 10-fold or sometimes 3-fold dilutions of the material under test, wasnot very precise, hence many producers couldnot make accurate estimates of the titre ofeither their inoculum or their product. Pockcounting, although early shown to be verysuitable for the assay of vaccinia virus (Keogh,1936), did not come to be widely used byvaccine producers until the 1950s .
Maintenance of seed virus . As recently as 1966,many manufacturers still used some of thevaccine lymph prepared for distribution asthe inoculum for the next series of vaccinifers,a procedure that over the years involved alarge but unknown number of serial passagesof the virus in these animals . Other manu-facturers passed the virus in the skin of man orthe rabbit after a certain number of subcul-tures in calves, or alternately in vaccinifer andrabbit. Meeting in 1958, a WHO Study Groupon Requirements for Smallpox Vaccine(1959) recommended the use of the seed lotsystem . This involved, in principle, laboratorymaintenance at refrigerator temperature oflarge stocks of a primary seed lot of a suitable
SMALLPOX AND ITS ERADICATION
preparation of vaccinia virus . From thisprimary seed lot enough virus had to beprepared for the production run. Dependingon its titre, the extent to which it multipliedand the number of vaccinifers used, theprimary seed was passaged once or severaltimes by the scarification of single calves toobtain the seed lot for the production run .The number of such serial passages of thevirus in the vaccinifer was usually restrictedto 5. With this method, possible alteration ofthe strain could be limited, the chance ofextraneous contamination was reduced, andthe inoculum could be standardized in termsof viral concentration and freedom fromcontamination .
Preparation of Liquid Vaccine
Traditionally, the vaccine pulp was pro-cessed so as to remove some of the extraneousmaterial and reduce the bacterial count, and itwas then dispersed as a liquid suspensioncalled vaccine lymph .
Clarification of the vaccine pulp
The semisolid pulp was usually ground intolymph by comminuting it in a grinder, orlater by homogenization in a blending ma-chine. For this purpose it was usually mixedwith 40-60% glycerol. Storage of the glycer-olated homogenate at low temperature over aperiod of months led to a steady fall in thenumber of viable bacteria, but it was later

7. DEVELOPMENTS IN VACCINATION AND CONTROL, 1900-1966
283
found that the same result could be morerapidly achieved by the addition of phenol(see below) . Periodically bacteriological testswere made to determine when the lymph wassuitable for distribution .
Use of glycerol
The introduction of glycerol to "stabilize"the vaccine virus and at the same time preventbacterial multiplication was regarded as amajor step forward in lymph production . Thisprocedure made it feasible to change fromarm-to-arm vaccination or the use of anitinerant vaccinated cow (see Chapter 6, Plate6.12) to the distribution of liquid vaccine incapillary tubes .
Glycerol had three advantages : it acted asan antibacterial preservative, it helped tomake the vaccine stick to the skin, and itpermitted the maintenance of the vaccine inliquid form at -10 °C and thereby ensuredthe long survival of active vaccinia virus . Italso prevented ice formation, a process which,in the presence of phenol (contained in nearlyall smallpox vaccines), led to the reduction ofviral infectivity .
However, although Copeman (1892, 1899)had claimed that glycerol was bactericidal butnot virucidal, subsequent work showed thatat temperatures above 0 °C it inactivatedvaccinia virus rather rapidly . The deleteriouseffect of glycerol was of little importance incountries with temperate climates, especiallyif good refrigeration was available, but it wasan important cause of vaccine failure intropical areas .
Use of phenol
The bacterial count in glycerolated pulpstored in the refrigerator fell off very slowly .Several months were usually required beforeit was low enough to allow the vaccine to beissued for use, and repeated testing wasnecessary during this period . The procedurecould be greatly accelerated by adding phenolto a final concentration of 0.5%, a procedureoriginally recommended by Gins (1924)and Lehmann (1937) and popularized byMcClean (1949), whose protocol was as fol-lows : Material harvested from the sheep wasground with twice its weight of a 1 % solutionof phenol in distilled water . After this hadstood at 22 °C for 48 hours, glycerol, equal inamount to the phenol solution, was added, so
that the final concentration of phenol was0.4% .
Mode of distribution
Liquid vaccine was usually dispensed inglass or, later, plastic capillary tubes, in single-dose lots or in amounts sufficient for about 20vaccinations .
Preparation of Dried Vaccine
Liquid vaccine was satisfactory in temper-ate countries with well-developed healthservices, good transportation networks andreliable refrigerator capacity. Endemic small-pox was eliminated from Europe and NorthAmerica by vaccination with liquid glycero-lated vaccine, even though its potency wassometimes lower than desirable . At this timemany authorities favoured the use of multiplesites of insertion (usually 2 or 4), a procedurewhich continued up to the 1960s in India andwhich sometimes produced a satisfactory takeeven with a substandard vaccine. However,liquid vaccine was totally unsatisfactory fortropical countries, as reports from medicalofficers in those areas attested . In 1919, forexample, the complaint was made in Africathat even for primary vaccination "only 7-20% positive results were obtained with thebest vaccine" (Tanganyika Territory, 1920) .Likewise, in Madras, Hobday et al . (1961)obtained a 27% take rate in revaccinationswith fresh liquid vaccine compared with a63% take rate with freeze-dried vaccine .Because of its low heat stability, healthauthorities sometimes went to great troubleto try to maintain the potency of liquidvaccine . In Peru, for example, inthe period before freeze-dried preparationsbecame available, vaccine was carried in thefield in kerosene refrigerators mounted onthe backs of mules (C. Quiros, personalcommunication, 1984) .
Air-dried vaccines
It was recognized very early that driedvaccine often survived far longer than liquidvaccine when both were maintained at am-bient temperatures, and Jenner himself dis-tributed vaccine dried on threads or betweenglass slides. Over the years a variety ofmethods for drying liquid vaccine were em-ployed (L. H. Collier, 1954) . Among the more

284 SMALLPOX AND ITS ERADICATION

7. DEVELOPMENTS IN VACCINATION AND CONTROL, 1900-1966 285
Plate 7.2 (facing page) . A: Apparatus developedby Camus and Fasquelle and used for the preparationof freeze-dried vaccine from 1917 onwards . B: Ap-paratus developed by Hornibrook (1949) for prepar-ing freeze-dried vaccine . (From Hornibrook, 1949 .)
Plate 7.3 (above and right) . A : Apparatus used byOtten (1927) for evacuating ampoules containing air-dried vaccine before sealing . (From Olivier et al .,1932 .) B: Commercial development of Hornibrook'sapparatus used for making freeze-dried vaccine inPeru in the early 1950s .

286
effective were those devised by Camus (1909),working at the Vaccine Institute in Paris andconcerned to produce an effective vaccine foruse in French colonies in the tropics, and byOtten (1927), working in Batavia (Jakarta) .Camus placed vaccine pulp in a thin layerunder an evacuated bell jar, in the presence ofsulfuric acid. The pulp was cooled and shadedfrom light, and drying was complete within afew hours. In tests in western Africa, aftertransport at ambient temperatures, it gavetake rates in different trials of 66-100% .Otten used a similar procedure : buffalolymph was dried in vacuo over sulfuric acid, atroom temperature. Subsequently the am-poules were attached to a manifold and sealedunder vacuum (Plate 7 .3A). Although theresults were variable, the majority (80%) ofpreparations of such dried vaccine producedtakes in 75-100% of primary vaccinees, afterstorage at room temperature in Batavia for16-30 months or at 37 °C for 12 months(Otten, 1932 ; W. A. Collier, 1953) .
Otten's vaccine was an important factor inachieving the elimination of smallpox fromthe Netherlands East Indies (now Indonesia)in 1937 (see Chapters 8 and 13) . However,there was considerable batch-to-batch vari-ation, the vaccine was often heavily contami-nated with bacteria, and it was difficult toreconstitute. Further, the technique did notlend itself readily to large-scale production.
Freeze-dried vaccinesIn 1909 Shackell reported an improved
method of drying biological materials, basedon the fact that H 2O could pass directly froma solid to a gaseous state . He deep-froze thebiological material and sublimated it in vacuo.During the First World War, Wurtz & Camus(1919) produced a freeze-dried vaccine whichwas packed in tubes under vacuum. Samplesprepared by this method were active afterseveral weeks at 37 °C and, when transportedfrom France to Cote d'Ivoire, Guinea andFrench Guiana, gave take rates of 85-100%(Fasquelle & Fasquelle, 1949) (Plate 7 .2A) .
Approximately 10 million doses of thisdried vaccine were sent every year between1920 and 1940 to the French colonies inAfrica for the smallpox vaccination cam-paign, and the Vaccine Institute in Pariscontinued to supply it to the francophonecountries of Africa until 1966, in amountsranging from 4 to 12 million doses annually(J. Fasquelle, personal communication, 1983) .
SMALLPOX AND ITS ERADICATION
During the eradication programme in wes-tern Africa in 1967 (see Chapter 17), it wasfound that smallpox was less of a problem incountries that had been French colonies, inpart because of their previous use of freeze-dried vaccine.
Meanwhile, from the 1930s onwards var-ious laboratory workers in other countrieshad adopted freeze-drying for the preserva-tion of vaccinia virus (Rivers & Ward, 1933,1935 ; Lloyd & Mahaffy, 1935 ; Hahn, 1951 ;L. H. Collier, 1951). The technology wassubstantially improved by Flosdorf & Mudd(1938). A freeze-dried vaccine developed byKaiser (1937, 1942) was said to have beenused extensively by the German army duringthe Second World War (cited by L . H. Collier,1954) .
In 1948, the year in which the WorldHealth Organization was established, a WHOstudy group on smallpox vaccine met in Parisand reported to the First World HealthAssembly that freeze-dried vaccine such asthat prepared at the Paris Vaccine Institute(using the method developed by Wurtz &Camus) had proved to be an effective heat-stable vaccine in the French colonies for anumber of years . Stimulated by these reports,Dr Fred L. Soper, then Director of the PanAmerican Sanitary Bureau, encouraged theUnited States National Institutes of Health tocarry out studies on appropriate methods forthe production of freeze-dried smallpox vac-cine, in order to fulfil the proposal made bythe Executive Committee of the Pan Ameri-can Sanitary Organization in 1949 that allcountries in the Americas should cooperate innational programmes designed to eradicatesmallpox (Soper, 1966) . The technical investi-gations were undertaken by the Division ofLaboratories, Michigan Department ofHealth, then a leading producer of glycerol-ated liquid vaccines (Ducor, 1947) . Theyresulted in the development of a method forfreeze-drying vaccine that had been dispensedin 0.5-ml lots in Pyrex tubes (Hornibrook &Gebhard, 1951), using a sulfuric-acid drier(Plate 7 .2B) developed by Hornibrook (1949) .Peru was the first country in the Americas touse this process on a commercial scale, begin-ning in October 1953 .
In June 1952, WHO organized compara-tive studies on the heat stability of freeze-dried vaccine produced by the Vaccine Insti-tute, Paris, the State Serum Institute, Vienna,the Division of Laboratories, Michigan De-partment of Health, Lansing, USA, and the

7. DEVELOPMENTS IN VACCINATION AND CONTROL, 1900-1966
287
Plate 7 .4 . Leslie H . Collier (b . 1921) . As a graduatestudent at the Lister Institute of Preventive Medicine,Elstree, Herts ., England, in the early 1950s Dr Collierdeveloped the method of freeze-drying of vacciniavirus that was subsequently adapted to large-scalefreeze-dried vaccine production in many laboratoriesthroughout the world .
Pasteur Institute, Bandung, Indonesia . Thetests were carried out in the State SerumInstitute,
Copenhagen,
the
Divisionof Laboratories, Michigan Department ofHealth, the Vaccine Institute, Paris, the ListerInstitute of Preventive Medicine, Elstree, andthe New York City Department of Health.No laboratory performed the tests on vaccinethat it had itself produced . The results showedthat the heat stability of the vaccine providedby the Michigan Department of Health wasthe best of the 4 tested .
The large demand for human plasma pro-teins for use in the Second World War had ledto further advances in the technology offreeze-drying, notably the introduction of acentrifugal freeze-drying apparatus (Greaves,1946). L. H. Collier (1951), working at theLister Institute as a graduate student underthe direction of D . McClean, applied thistechnique, with the addition of peptone as astabilizing agent, to the preservation of vac-cinia virus and subsequently developed it forlarge-scale commercial production (L. H.Collier, 1955) . WHO decided to conduct anadditional test to compare the new ListerInstitute vaccine with the freeze-dried vac-cine from Michigan . Samples maintained at
0,
37 °C and 45 °C for various periods weretitrated by pock counting on the chorioallan-toic membrane and by scarification in rabbitsand tested by primary vaccination of RoyalAir Force personnel (Cockburn et al ., 1957) .The Lister freeze-dried vaccine was found togive 100% successful takes after storage for64 weeks at either 37 °C or 45 °C. TheMichigan vaccine was much less heat stable,the take rate falling to 72% after 16 weeksand 10% after 32 weeks at 37 °C (Table 7.1),and to 47 % after 4 weeks at 45 °C. The resultsof titration of the two vaccines by pockcounting on the chorioallantoic membrane,in an independent laboratory, were consistentwith these results, in that the Lister vaccinemaintained its titre whereas that of theMichigan vaccine fell off steadily afterstorage .
As further modified by C . Kaplan, by thesubstitution of fluorocarbon treatment fordifferential centrifugation as a method ofpartial purification, L . H. Collier's methodwas eventually adopted by WHO for theglobal smallpox eradication programme (seeChapter 11) .
Subsequently, freeze-drying technologywas greatly improved for the large-scalecommercial production of vaccine, particu-larly in the methods of filling and sealingampoules. The availability of a method for thelong-term preservation of vaccine in tropicalclimates was an important factor in encourag-ing countries to participate actively in theglobal smallpox eradication programme .
Vaccine pulp destined for freeze-dryingwas prepared as for liquid vaccine, except thatglycerol was not added . In some laboratories itwas diluted or concentrated according to itspotency on assay. In order to reduce bacterialcontamination to an acceptable level, phenolwas added to the bulk solution of the vaccineso that its final concentration did not exceed0.5 0//0 -
Before 1967, the bulk solution was put intospecial ampoules or vials containing 0.25, 1 .0and 5.0 ml, corresponding respectively to 25,100 and 500 doses . These were then placed in afreeze-drier, of which there were two typesthe centrifugal drier and the shelf drier (seeChapter 11, Plate 11 .7). The former requiredthe use of a secondary drier, which consistedof a number of manifolds mounted overphosphorus pentoxide as a desiccant, whilethe latter provided both primary and secon-dary drying and sealing of the containersunder vacuum inside the drier .

288
SMALLPOX AND ITS ERADICATION
Development of Freeze-dried Smallpox Vaccine
"In 1948, I was told by the then Director [of the Lister Institute], Dr (later Sir) AlanDrury, that there was a great need for a smallpox vaccine that would be stable at tropicaltemperatures. He asked if I would be interested in this problem, and suggested that freeze-drying in which he himself was concerned as a means of preserving blood plasmamight be a useful technique .
"At the outset I aimed for a method that would yield consistent heat stability results andset myself these additional criteria : the vaccine must still comply with the official standardof potency after at least one month at 37 °C (a requirement later adopted by the British andEuropean Pharmacopoeias and by WHO) ; if dried, it must be safe and easy to reconstitutein the field by vaccinators with little technical training ; and it must be possible to produceit economically on a large scale. In addition, it would of course have to comply with theofficial regulations on bacterial contamination .
"In my field experiments I compared the stabilities of the glycerinated and lanolinatedvaccines in current production ; although the latter was the more stable at 22 °C, itcompletely lost its potency within a month at 37 °C. I then tried Otten's method of dryingcrude vaccine from the liquid state over sulphuric acid ; vaccine made in this way waswidely used in Indonesia and some batches had survived at ambient temperatures forremarkably long periods. There was however considerable batch-to-batch variation, afinding that I confirmed ; furthermore, the bulk dried vaccine was cumbersome to handleand distribute into ampoules.
"Without further ado I then started to explore the possibilities of drying from the frozenstate, using a large centrifugal dryer of the type that had recently been invented by R .Greaves at Cambridge . This machine was made in the Institute's workshops and althoughprimitive in appearance, it worked very well ; the main difficulty was the making ofvacuum-tight seals, at that time rather more of an art than a science .
"The general plan was to prepare experimental vaccines in various ways, to freeze-drypart of the batch and then to compare the keeping properties of the dried andcorresponding liquid preparations at 4 °C, 22 °C and 37 °C. Each batch was tested monthly,sometimes for more than two years. It was soon clear that dried lots of routinely-producedanimal skin vaccine varied considerably in stability ; materials partly purified bydifferential centrifugation yielded much more uniform results .
"The next problem was rather more difficult . Phenol was added to destroycontaminating bacteria ; this had to be done before drying, otherwise the bacteria wouldhave been preserved along with the virus . Although phenol in low concentration does notharm vaccinia virus in liquid suspensions, vaccines containing it lost much of their potencyon freeze-drying ; this was eventually traced to the tendency of phenol to come out ofsolution during rapid cooling and become concentrated to a degree that killed the vacciniavirus. This effect could however be prevented by adding peptone to a concentration of 5before drying the vaccine . Fortunately, among the many additives tried, peptone alsoproved by far the best for preserving potency at all temperatures tested ; it had the furtheradvantages of being non-antigenic, cheap and easy to reconstitute .
"After much experimentation, a satisfactory method was devised for purifying animalvaccine and freeze-drying it after adding peptone to a concentration of 5 % . Vaccine thusprepared consistently maintained its original potency for at least three months at 37 'C ; inlater experiments, batches stored at the high temperature of 45 °C still gave 100%successful primary vaccination after four years . The criterion for the permissible minimumcontent of vaccinia virus was fixed by determining the amount of virus needed to achieve100% successful vaccinations ; the final step in the development stage was the devising of asimple and safe method for reconstituting the dried vaccine in the field . It then remainedonly to scale up all the processes to a point at which full production could begin ; this wasaccomplished by 1953." (L. H. Collier, personal communication, 1980 .)

7 . DEVELOPMENTS IN VACCINATION AND CONTROL, 1900-1966
289
Table 7 .1 . Relation between potency measurements of preparations of freeze-dried vaccine (Michigan)stored at 37 'C for various periods, by pock counting on the chorioallantoic (CA) membrane andby rabbit-skin scarificationa,b
a From Cockburn et al . (1957).b KEY:- = no test .c = confluent lesion, 100% of the area .sc* = semiconfluent lesion, 70-80% of the area .sc = semiconfluent lesion, 50-70% of the area .sc = semiconfluent lesion, less than 50% of the area .Figures shown under "Rabbit scarification titre" indicate number of discrete vesicles .A = Lister Institute of Preventive Medicine .B = Department of Bacteriology, University of Liverpool .
Quality Control
At the national level
Smallpox vaccine had been used for manyyears before the concept developed that itshould be subject to national quality control,in addition to whatever steps the manufac-turer might take to protect the reputation ofhis products. By the mid-1920s a few coun-tries had developed regulations governingbiological products destined for medical use,such as vaccines, toxoids and sera.
In January 1926 the Smallpox and Vaccina-tion Commission of the Health Organisationof the League of Nations decided to collectinformation from vaccine producers regard-ing the production, testing, standardization,storage and delivery of smallpox vaccine .France, Germany, the Netherlands, Switzer-land and the United Kingdom participated inthis survey, which was completed in 1927 . Onthe basis of the results, the United Kingdomincorporated standards into the Therapeutic
Substances Regulations 1927 (England andWales, Ministry of Health, 1928a) . A briefreview of these regulations provides someinformation on how the quality control ofsmallpox vaccine was then being conductedin the United Kingdom. The regulationsdefined certain conditions concerning thequalifications of staff, the animals to be used,the housing of such animals, precautions to beobserved during the production process,specifications for final containers for the useof the vaccine, and labelling . The provisionsrelating to the purity of the vaccine indicatedthat each batch should be tested to ensurethe absence of anaerobic organisms andstreptococci : bacterial counts should be lessthan 5000 per ml . Scarification of the corneaof guinea-pigs or the skin of rabbits withdiluted vaccine lymph was the principalmethod for potency testing, typical vaccinialesions being regarded as the criterion foradequate potency. It seems likely that thequality control of vaccine lymph was beingcarried out along these lines in many other
CA PrimaryStorage Testing membrane titre
Rabbit scarification titrevaccination
conditions laboratory (pock-forming1 :10 1 :100 0001 :1 0001 :3 0001 :9 0001 :27
success rateunits per ml) (%)
-10 °C A 1 .5 x 10' c c sc* 6 100B 2 .9 x 10 6 c c c 8
4 weeks at 37 C A 3 .4 x 10' c sc* sc 6 I 96c c 6 I 3
B 1 .5 x 10 6 6 0 0 04 0 0 0
8 weeks at 37 °C A 3 .6 x 10 6 c c c sc 5 0 96c sc* 5 0 0 0
B 8 .5 x 10 5 c 6 1 0sc 6 4 3
16 weeks at 37 °C A 4.8 x 10 5 c sc 6 0 0 72c sc* 2 2 0
B 10 .3 x 10 5 c c I 0sc sC I 0
32 weeks at 37 °C A 5 .1 x 10 4 3 0 0 0 10? 0 0 0
B 10 .2 x 10 4 4 1 05 0 0

290
SMALLPOX AND ITS ERADICATION
countries of Europe and perhaps in NorthAmerica at that time . During this period theapplication of the control system dependedon the interest and capabilities of the produc-tion laboratory, since there was no mechanismfor independent assessment .
At the international level
In 1946 the Interim Commission of theWorld Health Organization was set up, tak-ing over the functions of the Health Organ-isation of the League of Nations . The Com-mission established a section (unit) of Biolo-gical Standardization in the Secretariat . Theresponsibilities of this section included theestablishment of international standards forbiological assay, the formulation ofrequirements for biological products, thecoordination of research on biological stan-dardization and the encouragement of Mem-ber States to set up national control laborato-ries for biological substances (Outschoorn,1973) .
WHO standards for smallpox vaccine werefirst established in 1958, at a meeting inwhich 6 experts from Europe, 2 from NorthAmerica, 2 from Asia, and 1 from NorthAfrica participated (WHO Study Group onRequirements for Smallpox Vaccine, 1959) .This meeting suggested the criteria thatshould be established for smallpox vaccine, inrelation to the strain of vaccine, methods ofpreparation of the vaccine lymph, bacterialcounts, use of the seed lot system, methods ofpotency assay and standards for the heatstability of freeze-dried vaccine . In 1965 theserequirements were revised in the light ofexperience accumulated during the interven-ing period (WHO Expert Group on Require-ments for Biological Substances, 1966). Mean-while, after extensive collaborative studies,the first reference preparations of smallpoxvaccine were established in 1962 (ampoulescontaining 14 mg of freeze-dried smallpoxvaccine ; Krag & Bentzon, 1963) and of anti-smallpox serum in 1965 (ampoules con-taining 84.3 mg of freeze-dried pooled humanserum 1000 IU per ampoule ; WHO ExpertCommittee on Biological Standardization,1967). These reference preparations wereproduced with a view to facilitating thelaboratory investigations needed in order toimprove vaccine quality . The modificationsproposed in 1965 reflect the progressiveimprovement in vaccine production andassay .
Seed lot ystem. In the 1959 WHO require-ments, up to 10 serial passages of the seedvirus were permitted . Meanwhile, advances inviral genetics and practical experience withpoliovirus vaccine had drawn attention to theneed to minimize the serial passage of seedvirus if genetic stability was to be maintained .In response to this new knowledge, theacceptable maximum number of passages ofvaccinia virus secondary seed lots was reducedto 5 .
Bacterial count. In 1959 the acceptable countwas set at less than 1000 non-pathogenicbacteria per ml, whereas in 1965 this numberwas reduced to less than 500 per ml, becausemanufacturers had improved their techniquesfor the handling of animals and the collectionof the vaccine pulp .
Potency. Cockburn et al . (1957) found thatvaccine with a titre of 1 .5 x 10' pock-forming units per ml gave 100% successfultakes in groups of about 100 primary vaccin-ees, and in a more elaborate statistical analysisof their data (published as an annex to thearticle cited), C . C. Spicer showed that vac-cines with a potency of 108 pock-formingunits per ml should give less than 1 failure in1000 primary vaccinations . In 1959 a titre of 5X 10 7 pock-forming units had been recom-mended as the minimal acceptable potency,but in 1965 the level was doubled, to 108pock-forming units per ml . This change wasbased on observations made by the WHOExpert Committee on Smallpox (1964), to theeffect that :
. . vaccines of relatively poor potency areadequate for successful primary vaccination butinadequate for successful revaccination . Their usefor revaccination gives a false sense of security,since a negative response is often taken as evidenceof immunity. Failure in successful revaccinationexplains in part the continued presence of small-pox in some endemic countries where vaccinationis regularly practised ."
Changes were also made in the recom-mended method of titration . Following theobservations by Cockburn et al . (1957) thatpock counting was considerably more precisethan rabbit scarification (see Table 7 .1) andthat pock counts correlated well with takerates (Fig. 7 .1), the 1959 recommendationthat rabbit-skin scarification and pock count-ing were acceptable alternatives was changedso as to eliminate scarification .
Heat stability . The requirements for heatstability remained unchanged ; vaccine

should maintain the minimum acceptablepotency (now 10 8 pock-forming units per ml)after incubation at 37 °C for 4 weeks .
Implementation of the WHO recommendations .The WHO requirements for smallpox vaccineestablished in 1965 remained in effectthroughout the Intensified Smallpox Eradi-cation Programme. However, the promulga-tion of standards by WHO in 1959, and againin 1965, and their application in laboratoriesin diverse countries were very differentmatters, especially before the WHO SmallpoxEradication unit organized an internationalquality control system in 1968 . Before that,many laboratories lacked competent staff,adequate facilities and interest . Some pro-duction laboratories did no potency assays atall ; others relied on tests in unvaccinatedchildren, regarding 9 takes out of 10 assatisfactory (a result that could be obtainedwith a vaccine whose titre was as low as 10 6.5pock-forming units per ml ; see Fig. 7 .1) . Forproducers who did wish to titrate theirproduction lots, reference preparations ofknown titre were required . However, only 2or 3 ampoules of the international referencevaccine, prepared in 1962, were supplied toproduction laboratories, from which the lab-oratories were expected to produce their ownworking standards. In developed countriesthis was no problem, but it was beyond the
3
7. DEVELOPMENTS IN VACCINATION AND CONTROL, 1900-1966
4
5
6
7Log,o (mean pock count)
8
Fig: 7 .1 . Relationship between pock counts ofvaccinia virus and the percentage of successful takeson primary vaccination . The solid line represents atheoretical curve based on probit analysis assuming a50% probability of a take at a dose of 3 x 10' pock-forming units per ml . (From Cockburn et al ., 1957 .)
291
capacity of many laboratories in developingcountries. Further, some developed countriesdid not adopt the standards recommended byWHO. For instance, in the USA, the rabbit-skin scarification method was still used asthe method for estimating the potency ofsmallpox vaccine until 1971 . In Japan, a titreof 5 x 107 pock-forming units per mlremained the officially accepted minimumlevel of potency for several years after 1965 .National quality control of smallpox vaccineswas exercised in only a few countries .
From 1959 to 1966, WHO's participationin monitoring the quality of vaccine waslimited to material which had been donated tothe Organization for use in the global eradica-tion programme . This amounted to onlyabout 7 million doses a year (total over theperiod : some 46 million doses ; see Chapter 11,Table 11 .1). Material supplied through bi-lateral assistance or by local production wasnot tested by WHO. This often resulted inthe use of substandard vaccine . As A. S .Outschoorn, former Chief Medical Officer ofthe WHO Biological Standardization unit,said
"It has never been feasible for W .H.O. laborato-ries to be established which would undertakecontrol of biological products on behalf of Mem-ber States . There would perhaps be a place in thefuture for private enterprise to make availablesources of expertise or advisory services and eventesting facilities from which Member Govern-ments could call for assistance outside of the WorldHealth Organization." (Outschoorn, 1973 .)
The absence of effective quality control wasone of the first obstacles that had to beovercome when the Intensified SmallpoxEradication Programme was established in1967 (see Chapter 11) .
VACCINATION TECHNIQUESBEFORE 1967
During the long history of vaccination,practices and techniques were gradually de-veloped that differed from country tocountry. However, by the 1950s they sharedmany features, which are summarized below .
Vaccination Site
The most commonly used site for primaryvaccination and revaccination was on the

292
"Vaccination" and "Immunization"
The term "vaccination" sometimes causes confusion because it has both a specific and ageneral meaning . Vaccination against smallpox was the only form of preventive im-munization against an infectious disease until 1880, when Pasteur developed techniques ofattenuation of virulence and protective inoculation of animals against anthrax and chickencholera. In 1881, in order to recognize Jenner's contribution to the concept of inoculationwith attenuated microbes as a method of protection against infectious diseases, Pasteurproposed that this procedure should be called "vaccination" and the product used a"vaccine", whatever its nature . This terminology remains in use, though the generalprocedure is now usually called "immunization" ; the product is still called a vaccine-e.g.,poliovaccine, measles vaccine. In this book "vaccine" always means smallpox vaccineunless specified in some other way .
extensor surface of the upper arm, over thedeltoid muscle. In some parts of India, how-ever, revaccination was carried out on theflexor surface of the forearm .
The skin site was usually rubbed withalcohol or acetone . Although studies de-scribed in Chapter 11 showed that such skinpreparation was unnecessary and could, if thealcohol did not completely evaporate, partial-ly inactivate the vaccine, the practice contin-ued to prevail in many countries .
Methods of Vaccination
Several methods were used, all involvingthe introduction of the virus into the Mal-pighian layer of the epidermis, with a varietyof instruments (Plate 7.5) . In most countries,either the skin was scarified by a single linearincision or scratch, or vaccine was introducedinto the epidermis by the multiple pressuremethod, but in a few places a rotary lancet wasused .
Dermal scarication
A scratch about 5 mm long was made in theskin with a needle, a lancet or a small knifeand the vaccine suspension was rubbed intothe site . A single cut or cross cuts were made,in 1, 2 or 4 different sites . This was essentiallythe same method as had been used forvariolation in Europe during the latter part ofthe 18th century.
Multiple pressure method
From very early times attempts were madeto deposit virus between the skin layers by
SMALLPOX AND ITS ERADICATION
methods other than the scratch method orintradermal inoculation with a syringe andneedle. Leake (1927), in a pamphlet offeringofficial advice on vaccination to physiciansin the USA, recommended the "multiplepressure" method (Fig . 7 .2), which was subse-quently adopted in several other countries(Parish, 1944 ; England and Wales, Ministryof Health, 1956) . A small drop of vaccine wasplaced on the skin and the side of a straightsurgical needle, held tangentially to the skinsurface, was pressed firmly and rapidly intothe drop by an up-and-down motion, about10 times for primary vaccination and 30 timesfor revaccination . Excess vaccine was wipedoff. Only 1 insertion site was recommended,for both primary vaccination and revaccina-tion. This method was less traumatic thanscarification, while still producing an ade-quate take. However, it was difficult to trainvaccinators to exert sufficient pressure, andthis sometimes caused unsuccessful vac-cinations.
Rotary lancet
Vaccination using the rotary lancet (Plate7.5) was carried out in many parts of theIndian subcontinent . A rotary lancet designedfor vaccination was first described by Rose(1871) and was manufactured in the UnitedKingdom and later in India. The vaccine wasplaced on the skin with the small spoon onone end of the instrument. The disc, anchoredby the slightly longer central spike, wasrotated in such a way that the small lateralspikes abraded the epidermis . If potent vac-cine was used, the ensuing trauma produced alarge and severe vaccinial reaction, which wasa frequent cause of refusal to undergo vaccina-

a
A
rv
-
B
C
Plate 7.5 . Instruments used for vaccination (actual size) before the introduction of the bifurcated needle .A : Rotary lancet . B : Vaccinostyle, used for scratch vaccination . C : Straight surgical needle, used for vaccinationby scratch or multiple pressure method (See Fig . 7.2) .
tion. Further, the vaccines then in use wereoften heavily contaminated with bacteria andthe use of the rotary lancet could producescarring even when the infection had beendue to pyogenic bacteria rather than vacciniavirus. Failures sometimes occurred whenvaccinators did not allow the lancet to cooladequately after the flaming that was carriedout after each vaccination .
Although the WHO Expert Committee onSmallpox (1964) recommended that thismethod should not be used, it was stillroutinely employed in some parts of theIndian subcontinent long after this . Duringthe smallpox eradication programmes inPakistan and India (see Chapters 14 and 15),the programme staff hunted for rotary lancetsand confiscated a large number of them fromvaccinators who were reluctant to abandonthe method but were thus obliged to use thebifurcated needle . However, many remained
Ew0w
Stratum
_corneum==
StratumMalpighii
Papillarylayer
Reticular
. .layer -4. ti~~4;_e-
Vessel
7. DEVELOPMENTS IN VACCINATION AND CONTROL, 1900-1966
Fig . 7 .2 . The principle of the multiple pressuremethod of vaccination . Virus on the tip of the needleis deposited within the deeper layers of the epidermis .
in use, particularly in the municipal corpora-tions in India, as late as 1974 .
Age for Primary Vaccination
Throughout the 19th century, stress wasplaced on the primary vaccination of infantsas the optimum method of providing pro-tection against smallpox, and laws for com-pulsory vaccination during the first 3-6months of life were introduced in manycountries. However, in the St PetersburgFoundling Hospital, infants aged 7-8 dayswere vaccinated with lymph maintained byarm-to-arm vaccination from 1801, when theEmpress of Russia obtained lymph fromJenner, until 1867, when vaccine from cowsbegan to be used. There were no seriouscomplications, but a few infants requiredrepeated inoculation before a take was ob-tained. Compulsory registration made it pos-sible to keep track of foundlings until theywere 25 years old, so that observations onthe efficacy of vaccination were possible .There were 17 epidemics of smallpox in StPetersburg between 1826 and 1846 ; out ofabout 15 000 foundlings, only 34 had small-pox, with only 1 fatality (Frobelius, 1869 ;Donnally & Nicholson, 1934) . Elsewhere, thevaccination of newborn infants exposed tocases of smallpox was occasionally recom-mended, but routine vaccination of newbornchildren in a hospital appears to date from theearly 20th century, in some centres in Franceand Germany . The compulsory vaccination of
29 3

294
Plate 7 .6 . Lesions in a Pakistani child due to use ofthe rotary lancet, with insertions at 4 separate sites .
neonates was first practised in Detroit, USA,at the time of an epidemic of variola major in1925 (Lieberman 1927) .
Espmark & Rabo (1965a,b) examined theeffect of maternal antibody on the response ofinfants vaccinated under the age of 1 month .They found that more potent vaccines wereneeded for these younger infants than forinfants vaccinated at 5-12 months of age, butthat with potent vaccines (10 80TCID50 perml or higher) take rates and neutralizingantibody responses were equally good in bothgroups, and the local signs and constitutionalsymptoms were milder in the younger infants .
In most countries of Europe and NorthAmerica, infants were vaccinated during thesecond 6 months after birth . In the UnitedKingdom (Conybeare, 1964b) and in the USA(Neffet al., 1967 ; Lane et al., 1969), investiga-tions into the complications of vaccinationindicated that the risk of postvaccinial en-cephalitis in infants vaccinated before theage of 1 year was greater than that in those
SMALLPOX AND ITS ERADICATION
vaccinated later .'I'his led to recommendationsthat vaccination should be postponed untilthe 2nd year of life. However, in countries inwhich the maternal antibody level was rea-sonably high e.g., Sweden it was shownthat vaccination in the first 3 months of lifewas effective, and was usually attended by lesssevere signs than vaccination later in infancy(Espmark et al., 1973) .
Other considerations were important inendemic countries, in which the case-fatalityrate for smallpox was very high in younginfants. Noting that in Madras, India, mostinfants were born in hospitals and wereaccessible as neonates but often difficult totrace after they left hospital, Rao carried out apilot study in 1959-1960 in which 2500infants were vaccinated with liquid vaccineon the 3rd day of life, with a take rate of 82 ;o(Rao & Balakrishnan, 1963) . Subsequently,take rates of 100% were obtained withfreeze-dried vaccine, and the practice of neo-natal vaccination was extended to a num-ber of urban areas throughout India(WHO/SE/71 .30, Rao) .
Interpretation of the Results of Vaccination
In susceptible individuals, smallpox vacci-nation produced a typical Jennerian pustule atthe inoculation site and frequently swellingand tenderness of the draining lymph node .At the height of the reaction there was usuallyslight fever and the subject might feel indis-posed for a few days. A feature of smallpoxvaccine, which among the variety of agentsnow used for immunization against infectiousdiseases is shared only with BCG vaccine, isthat successful vaccination produced a charac-teristic skin reaction which could be readilyobserved and which usually left a permanentand characteristic scar . This had both immedi-ate and long-term consequences . Observationof the nature of the cutaneous lesion afterrecent vaccination or revaccination enabledthe vaccinator to decide whether the virushad replicated and the patient had thus beenrendered immune to smallpox. In the longerterm, the vaccination status of an individualor a population could be determined, withconsiderable accuracy, by visual examinationfor vaccination scars, thus obviating the needfor a serological survey . For these reasons,special attention was devoted to skin reac-tions after both primary vaccination andrevaccination .

7. DEVELOPMENTS IN VACCINATION AND CONTROL, 1900-1966
295
The clinical features of smallpox in unvac-cinated and vaccinated persons and the patho-genesis and immune responses in smallpoxand after vaccination are described in Chapter1 and Chapter 3 respectively. It may be usefulto recall here the salient features of immunityto smallpox (see box) .
Major reaction in primary vaccination
A typical Jennerian pustule was termed a"major reaction", and constituted evidencethat the vaccinee would be protected againstsmallpox. The course of the reaction isillustrated in Plate 7 .7A and C. A papuleappeared at the vaccination site on the 3rd dayafter vaccination, and within 2 or 3 days thisbecame vesicular, to constitute the umbilica-ted and loculated "Jennerian vesicle". As insmallpox (see Chapter 1), the vesicle soonbecame pustular, owing mainly to the entry ofpolymorphonuclear cells, the migration ofwhich was stimulated by the viral infectionitself, and the surrounding area became eryth-ematous and indurated to a much greaterextent than was found in the skin lesions of
smallpox . The area of erythema reached amaximum between the 8th and 12th days(usually on the 9th or 10th day), and at thistime the draining lymph nodes were enlargedand tender and the subject often sustained amild fever and may have felt unwell . Thepustule dried from the centre outwards tobecome a dry brown or black scab which felloff about 3 weeks after vaccination, to leave atypical pitted scar.
For routine inspection, observation of thepustule on the 7th day confirmed whethervaccination had been successful . The reactionto vaccinia virus could be readily dis-tinguished from reactions due to bacterialinfection, both by its time course and itscharacteristic appearance .
Revaccination
As described in Chapter 3, successful pri-mary vaccination elicited not only humoralimmunity, but also a longer-lasting cell-mediated immunity, which conditioned theresponse to revaccination . Interpretation ofthe results of revaccination was sometimes
How Vaccination Protected against Smallpox
A large part of the DNA of all orthopoxviruses is very similar and codes for polypeptidesthat have a close resemblance in all orthopoxviruses . Vaccination against smallpoxconsisted in the production of an infection of the skin with vaccinia virus, with extensionto the lymph nodes and spleen, organs concerned with the immune response . Becausevaccination involved infection of the skin with a relatively large dose of a virus thatreplicated rapidly, generalization of infection and therefore the immune response occurredmore quickly than they did in naturally acquired smallpox. This explains why vaccinationduring the incubation period of smallpox sometimes aborted or modified the clinicalcourse of the disease.
The immune response to vaccination results in the development of cell-mediatedimmunity, probably to antigens expressed on the surfaces of infected cells, and a number ofhumoral antibodies, some of which can neutralize infectivity and may persist for longperiods. There are also memory cells for both cell-mediated and humoral immuneresponses, which wane slowly .
For a few years after vaccination the level of immunity may have been sufficient toprevent completely the replication of variola virus . A somewhat lower level of immunitymay have allowed limited replication of variola virus, short of symptom production, butwith an anamnestic immune response (subclinical infection) . Still lower levels ofimmunity may have allowed the generalization of variola virus to occur, but stimulation ofthe memory cells would have produced an accelerated immune response which would havemodified the clinical manifestations of smallpox (modified-type smallpox) . After manyyears the immunity provided by vaccination might have waned to such an extent that theattack of smallpox might not have been modified in any way and might indeed have beenfatal .

296
SMALLPOX AND ITS ERADICATION
difficult, in terms of evaluating their sig-nificance in relation to protection againstsmallpox. Sometimes there was no reaction atall, a result which was usually due to the use ofvaccine of low potency, and which wasimpossible to interpret correctly (WHO Ex-pert Committee on Smallpox, 1964) . If it didoccur, the reaction to revaccination could bemaximal at any time between the 2nd and the8th day . During the period before the globalsmallpox eradication programme, 3 varietiesof response used to be distinguished (see, forexample, van Rooyen & Rhodes, 1948) :
(1) Immediate reaction . Although it used to bedescribed as an "immediate" reaction, dermalhypersensitivity to vaccinial protein pro-duced erythema during the first 24-48 hoursafter vaccination . It was a classical delayedhypersensitivity reaction, which could beelicited by non-infectious vaccine as well as byactive vaccinia virus . Such a response mightbe given by highly immune individuals evenwhen potent vaccine was used, but it couldalso occur in individuals with little or noresidual immunity who were given inactivevaccine .
(2) Accelerated reaction . Persons with someresidual cell-mediated immunity but notenough to inhibit viral replication exper-ienced erythema and the development of avesicle and sometimes a pustule, whichevolved in a sequence more rapid than thatseen in a primary vaccination reaction (Plate7.7B and D) . Those with substantial immun-ity experienced little more than an immediatereaction, whereas those with minimal residualimmunity experienced a reaction almost in-distinguishable from that seen after primaryvaccination. The result of revaccination wasdependent on the balance between the po-tency of the vaccine and residual immunity . Ahighly potent vaccine could provoke a majorreaction, perhaps slightly accelerated, in anindividual who had failed to respond to a lesspotent vaccine ; revaccination on the flexorsurface of the forearm was more often fol-lowed by a substantial reaction than revaccin-ation over the deltoid muscle .
(3) Major reaction in revaccination. If a longperiod had elapsed after a primary vaccina-tion, revaccination could produce a reactionsimilar to that described for a primary vacci-nation. This was called a major reaction .
The WHO Expert Committee on Smallpox(1964) considered that the traditional classifi-cation of the reaction to revaccination as
"immediate", "accelerated" or "major", as justdescribed, could be misleading, in terms ofjudging whether an individual might besusceptible to smallpox. The Expert Com-mittee therefore recommended that revac-cination should be recorded as successfulif, on examination 6-8 days later, therewas a pustular lesion or an area of definiteinduration or congestion surrounding a cen-tral lesion, which might be a scab or an ulcer .Such a response was termed a "major reac-tion". All others were termed "equivocalreactions"-i.e., the persons concerned couldnot be presumed to be immune to smallpoxand were revaccinated .
COMPLICATIONS OF VACCINATION
Smallpox was such a dire disease and theeffects of vaccination by comparison so trivialthat for a hundred years after vaccination wasintroduced little account was taken of itscomplications in places in which smallpoxwas still endemic. There was a strong anti-vaccinationist movement in several countries,but this was based less on concern about therisks of the procedure than on moral andphilosophical objections to compulsory vac-cination (see Chapter 6) . Among those whosupported vaccination there was a reluctanceto admit that there were any risks . Forexample, in the United Kingdom during thefirst quarter of this century, 103 deaths among4 275 109 primary vaccinations were record-ed as being "associated with vaccination", butthe official view was that these "may merelyindicate that the child has been vaccinatedbefore death and that death is really attribut-able to some current illness" (England andWales, Ministry of Health, 1924) . However,smallpox vaccination consisted in the infec-tion of the human host with a virus that mustreplicate and produce lesions if it was to evokeimmunity. Any such procedure that is used ona sufficiently large scale will be associatedwith occasional cases in which more severelesions result . The pustular skin lesion illus-trated in Plate 7.7 and the fever and lympha-denitis described earlier were the normalresults of infection with vaccinia virus . Vacci-nation was sometimes complicated by muchmore severe symptoms and was sometimesfatal . These severe complications became amatter of much concern in many industrial-ized countries, in which endemic smallpoxhad been eliminated but routine vaccination

C
DAY 0
7. DEVELOPMENTS IN VACCINATION AND CONTROL, 1900-1966
DAY 3 DAY 7 DAY 10
Primary vaccination : multiple pressure method
Late revaccination: multiple pressure method
Primary vaccination : jet injector
Late revaccination: jet injector
DAY 14
297
Plate 7.7 . Skin reactions after primary vaccination and late revaccination (several years afterprimary vaccination) by the multiple pressure method and jet injector .

298 SMALLPOX AND ITS ERADICATION
C .'
Plate 7 .8 . Severe complications of vaccination . A: Eczema vaccinatum in the unvaccinatedcontact of a vaccinated sibling . B: Progressive vaccinia, which was fatal, in a child with animmunodeficiency. C: Generalized vaccinia, 10 days after vaccination ; benign course, noscarring . D: Auto-inoculation with vaccinia virus .

7. DEVELOPMENTS IN VACCINATION AND CONTROL, 1900-1966
programmes were maintained in order toprotect the community in the event of the im-portation of smallpox from an endemic area .
Types of Complication
Three groups of complications occurredamong vaccinated subjects : abnormal skineruptions, disorders affecting the central ner-vous system, and a variety of other rarer or lesssevere complications.
Abnormal skin eruptions
Three kinds of abnormal skin eruptionwere recognized . Two of them, eczema vac-cinatum and progressive vaccinia, were asso-ciated with abnormal host reactions ; truegeneralized vaccinia occurred in otherwisehealthy persons.
Eczema vaccinatum . This complication oc-curred in vaccinated persons or unvaccinatedcontacts who were suffering from or had ahistory of eczema. Either concurrently withor shortly after the development of the localvaccinial lesion (or after an incubation periodof about 5 days in unvaccinated eczematouscontacts) a vaccinial eruption occurred atsites on the body that were at the timeeczematous or had previously been so . Theseareas became intensely inflamed, and some-times the eruption later spread to healthyskin. Constitutional symptoms were severe,with high temperature and generalized lym-phadenopathy, and the prognosis was grave ininfants in whom large areas of skin wereaffected (Plate 7 .8A) .
It was to allow the safe vaccination ofchildren with eczema that Kempe (1968)promoted the use of the CVI-78 attenuatedvaccine (see Chapter 11), and vaccinia-immune globulin was often used to treat thesecases, in both vaccinated persons and thoseaccidentally infected. The risk of this infec-tion remains, since military personnel con-tinue to be vaccinated in some countries .Several cases of vaccinial infection (and thuspotentially of eczema vaccinatum) in contactsof recently vaccinated military personnelwere reported in Canada and the UnitedKingdom, and in the USA as recently as 1985(Journal of the American Medical Association,1985) .
Progressive vaccinia (vaccinia necrosum) . Thiscomplication occurred only in persons whosuffered from a deficient immune mechanism,
299
Plate 7.9 . Abram S. Benenson (b . 1914) . UnitedStates expert in immunology and communicablediseases, who carried out studies on methods ofevaluating responses after vaccination and plannedtrials of attenuated vaccines . He was a consultant toseveral WHO committees on smallpox eradicationand was instrumental in developing the vaccine pro-duction laboratory in Dhaka, Bangladesh .
such as agammaglobulinaemia, defective cell-mediated immunity or immunodeficiencyassociated with tumours of the reticulo-endothelial system or the use of immuno-suppressive drugs (see Chapter 3, Fig . 3 .8) .In these cases the local lesion at the vac-cination site failed to heal (Plate 7 .8B),secondary lesions sometimes appeared else-where on the body and all lesions spreadprogressively until-as was likely-thepatient died, usually 2-5 months later .
Generalized vaccinia. As mentioned earlier,vaccinia virus produced a systemic infectionin man, with transient viraemia . Very rarely ageneralized vaccinial rash, sometimes cover-ing the whole body, occurred 6-9 days aftervaccination (Plate 7 .8C). The course of theindividual skin lesions resembled that of thelesion at the vaccination site, but if the rashwas profuse the lesions sometimes variedgreatly in size. The generalized eruptionusually did not have the "centrifugal" distri-bution which was characteristic of the rash ofsmallpox (see Chapter 1) . Generalized vac-cinia was not associated with severe immuno-deficiency, and the prognosis was good .
Accidental infection . This was the most com-mon complication of vaccination, but it wasusually not serious and was certainly greatly

300
SMALLPOX AND ITS ERADICATION
underreported. The commonest sites, in casesthat were seen by physicians, were the eye-lids (Plate 7 .8D), vulva and perineum. Twocategories were included in a national surveycarried out in the USA (see below and Table7.3) : accidental infection of secondary siteson vaccinees and accidental infection of nor-mal contacts of vaccinated persons .
Postvaccinial tonsillitis
Some Soviet authors (Braginskaya et al .,1971 ; Gurvich et al., 1974) regard post-vaccinial tonsillitis as a not uncommon com-plication of primary vaccination. Gurvichet al. (1979) reported the recovery of vac-cinia virus from pharyngeal swabs in 49%of children with postvaccinial tonsillitis,compared with 7% of those with nocomplications.
Postvaccinial encephalitis
This was the most serious complication ofvaccination in persons in whom there was nocontraindication for the procedure. There isan extensive literature on the subject, re-viewed by Wilson (1967) ; the histopathologyis described in Chapter 3 . One difficulty inassessing postvaccinial encephalitis is that theterm encompassed 3 conditions, only 2 ofwhich were due to vaccinial infection (seebox) .
Concomitant disease . A temporal associationdoes not prove causation, and some cases ofencephalitis after vaccination were undoubt-edly merely coincident disease due to other
causes. For example, Greenberg & Appel-baum (1948) noted that of 49 cases diagnosedante mortem as postvaccinial encephalitis, 4out of the 8 fatal cases proved on autopsy tohave been due to other causes (2 cases oftuberculous meningitis, 1 brain tumour and 1case of hypertensive vascular disease) . Some ofthe non-fatal cases may also have beencoincidental .
Cases of encephalitis may be expected tooccur in any large population of childrenwithin a defined period even if no vaccines ofany kind are administered . A survey in NewJersey, USA, in 1965 showed that in theabsence of vaccination 2.86 cases of en-cephalitis occurred per million children 1-9years old per 28-day period ; an investigationin Florida in 1968 reported a figure of 2 .28cases per million, in the same age group andduring the same time span (Landrigan &Witte, 1973). Figures of a like magnitudewere found in the National Childhood Ence-phalopathy Study in the United Kingdom,undertaken in 1976 because of widespreadpublic and professional concern over thesafety of pertussis immunization (Englandand Wales, Department of Health and SocialSecurity, 1981) . The results showed that themajority of the severe neurological disordersstudied were not associated with recent im-munization (within 28 days) and must beattributed to other causes . Nevertheless, ser-ious neurological complications were some-times caused by smallpox vaccination, 2 formsbeing recognized .
Encephalopathy and encephalitis. The patho-logical distinction made by Vries (1960)
Central Nervous System Disease after Vaccination
"Postvaccinial encephalitis" probably includes several different pathological con-ditions, of which 3 are specific . First, in any procedure practised as widely as wasvaccination against smallpox, there were inevitably some cases of the temporal coincidenceof vaccination and some other quite unrelated disease that produced signs of encephalitis .Very rarely, there could be infection of the meninges with vaccinia virus . In infants under2 years of age there was sometimes a general hyperaemia of the brain, mild lymphocyticinfiltration of the meninges, widespread degenerative changes in ganglion cells andoccasionally perivascular haemorrhages what Vries (1960) called postvaccinial encepha-lopathy . The commonest form, in individuals over 2 years of age, was characterized byperivenous demyelination and microglial proliferation in the demyelin-ated area, with some lymphocytic infiltration but very little oedema. The pathologicalfeatures of this form, for which the term "postvaccinial encephalitis" (or "encephalomyeli-tis") was usually reserved, were similar to those seen in other post-infection encephalitides .

7. DEVELOPMENTS IN VACCINATION AND CONTROL, 1900-1966
between encephalopathy, in infants under 2years of age, and postvaccinial encephalitisor encephalomyelitis, with characteristic peri-venous demyelination, in individuals over 2years of age, is important and can be tenta-tively recognized by consideration of the ageof the subject, the symptomatology and theincubation period . According to Spillane &Wells (1964) the onset in cases of encephalo-pathy was often violent, characterized byconvulsions ; hemiplegia and aphasia werecommon, the period of amnesia was short, andthe spinal fluid, though under increasedpressure, was often normal. Recovery wasfrequently incomplete, the patient being leftwith cerebral impairment and hemiplegia .
On the other hand, in the perivenousdemyelinating microglial encephalitis fol-lowing vaccination in subjects over 2 years ofage the onset was usually abrupt, with fever,vomiting, headache, malaise, and anorexia,succeeded by such symptoms as loss of con-sciousness, amnesia, confusion, disorienta-tion, restlessness and delirium, drowsiness,convulsions and coma, with incontinence orretention of urine, obstinate constipation, andsometimes meningismus . Paralysis, when itoccurred, tended to be of the upper ncurontype. The spinal fluid showed an increase inthe concentration of protein and the numberof lymphocytes. The case-fatality rate wasusually about 35% and in fatal cases deathusually occurred within a week . In patientswho survived, recovery often set in within afew days and was complete within 2 weeks .
Weber & Lange (1961) found that almostall cases of postvaccinial central nervoussystem disease in children less than 2 years oldand diagnosed as encephalopathy had incu-bation periods of 6-10 days (mean, 8 .6 ± 2 .3days) from the date of vaccination (Table 7.2) .By contrast, 96 % of 161 cases of postvaccinialencephalitis were in individuals over 2 yearsof age and most had incubation periods of 11-15 days (mean, 12 .3 ± 2.1 days), an intervalcompatible with an immunopathologicalbasis for the syndrome . In fatal cases, the dayof death in infantile encephalopathy was onaverage 10 .5 ± 3.0 days after vaccination ; thecorresponding figure for encephalitis was16.3 ± 3.9 days.
Postvaccinial encephalitis began to causeconcern in the 1920s and 1930s (Hurst, 1953),when it appeared to be especially frequent inseveral European countries. As smallpox be-came less common, the importance of thisserious complication of vaccination increased,
301
mainly because there was no way of assess-ing the risk of postvaccinial encephalitisbeforehand-unlike progressive vaccinia andeczema vaccinatum, for which there wereknown predisposing conditions . No meanswere known then, or in fact are known now,of predicting the occurrence of post-infectionencephalitis, whether attributable to measles,vaccination against rabies, or smallpox vac-cination (Johnson, 1982).
Other complications of vaccination
Very rarely, the fetus carried by a womanwho had been vaccinated was infected in utero .Although a possible example of this wasdescribed by Jenner (1809), up to 1978 only28 cases had been reported in the scientificliterature, almost all as single case reports (A .Gromyko, personal communication, 1978) .Of the 25 cases for which data are available, 21occurred in mothers who had been vaccinatedduring the first 6 months of pregnancy and 4occurred in mothers vaccinated later . In thefirst group, a fetus with generalized vacciniawas delivered on average 8 weeks after thevaccination, and in the second group about 4weeks after vaccination . Many cases werefatal, the fetus being stillborn or dying a fewdays after birth . There is no convincing
Table 7 .2. Length of the incubation period in 259cases of postvaccinial cerebral damageafter primary vaccinationa
a Based on Weber & Lange (1961) .
EncephalopathyPostvaccinialencephalitis
Incubationperiod (days) Number
of casesNumberof cases %
4 2 2.0 0 -5 3 3 .1 2 1 .26 12 12.2 0 -7 13 13 .3 I 0 .68 17 17.4 6 3 .79 24 24.5 8 5 .010 10 10.2 6 3 .7I
I 5 5 .1 21 13 .012 3 3 .1 37 23 .013 3 3 .1 31 19 .314 4 4.1 31 19 .315 I 1 .0 12 7 .56 0 - 3 1 .97 0 1 0 .618 1 1 .0 2 1 .2Total 98 161
Subjects aged2 years 96 98.0 7 4.3
Subjects aged> 2 years 2 2.0 154 95 .7

302
SMALLPOX AND ITS ERADICATION
evidence that congenital malformations everresulted from vaccination of the mother ; theinfected fetus usually died, but if it survived itrecovered completely (Tondury & Foukas,1964). The mother usually sustained anormal vaccination reaction ; the occurrenceof fetal vaccinia was additional evidence thatviraemia occurred during normal vac-cination .
Until smallpox was eradicated, smallpoxvaccination was the most widespread immu-nization procedure in the world. It was thusinevitable that there should sometimes be atemporal coincidence between vaccinationand the onset of certain other rare conditionsof unknown etiology, such as multiple sclero-sis . One rare association that probably hadsome etiological significance was the occur-rence of a malignant skin tumour, such asmelanoma, in the smallpox vaccination scar,usually many years after vaccination (Mar-melzat, 1968) . Vaccinial osteomyelitis wasoccasionally reported, the diagnosis of whichwas sometimes confirmed by the recovery ofvaccinia virus (Sewall, 1949) .
Sometimes vaccines were contaminatedwith pyogenic cocci, or the introduction ofstaphylococci into the skin during the vacci-nation led to localized bacterial infection .
Frequency of Complications
Apart from a multitude of case reports,estimates of the frequency of severecomplications-especially postvaccinial en-cephalitis, which was widely recognized inthe 1930s-were produced in many Europeancountries during the period 1940-1965 .These have been summarized by Wilson(1967). More useful, because they are morecomprehensive, are the two surveys carriedout in the USA (nation-wide and in 10 states)by the Communicable Disease Center(CDC-subsequently renamed the Centersfor Disease Control), Atlanta, Georgia. Usingdifferent methodologies, these surveys weredesigned to estimate the incidence of allcomplications of smallpox vaccination in theUSA for the year 1968. The methodologiesof these two surveys will be described beforethe frequency of various complications isdiscussed .
Methodology of the CDC surveys
Following a nation-wide retrospective sur-vey of complications occurring during the
year 1963 (Neff et al ., 1967), CDC undertooka comprehensive prospective national survey,and a confirmatory, less extensive, surveythrough physicians in 10 selected states, of thefrequency of complications of smallpox vac-cination in the USA in the year 1968 .
National survey (Lane et al., 1969). Effortswere made to identify all possible compli-cations, on a national scale, using 8 methodsto obtain information .
(1) The American Red Cross Vaccinia-Immune Globulin (VIG) distribution systemsupplied the names of physicians who hadbeen provided with VIG, which was in shortsupply, for patients . It was distributed fromsome 10 centres and released to the attendingphysician only after a telephone conversationwith the physician at the Red Cross centre anddue justification of its use had been made . Theattending physicians were asked for clinicaland epidemiological information on theirpatients shortly after receiving VIG .
(2) Consultants to the Red Cross VIGProgram supplied the names of patientssuspected of having complications of vaccina-tion who came to their attention but did notreceive VIG .
(3) The National Encephalitis Surveil-lance Program of CDC received reports fromeach state of all cases of encephalitis, nomatter what the cause .
(4) Death certificates citing complicationsof vaccination were scrutinized .
(5) Casual reports reaching state and terri-torial epidemiologists regarding vaccinationcomplications that had not been officiallyreported were transmitted to CDC .
(6) The Burroughs Wellcome Companysupplied information on patients who re-ceived the drug metisazone (Marboran) forthe treatment of complications of vac-cination .
(7) Reports were provided by smallpoxvaccine producers who had received com-plaints from patients with complicationsallegedly attributable to their products .(8) The Viral Exanthems Unit of CDC
reported on specimens submitted to its diag-nostic laboratory for the confirmation ofvaccinia virus.
The results obtained in this national sur-vey, expressed in absolute numbers and ascases per million vaccinations, are set out inTables 7 .3 and 7 .4 respectively .
Ten-state survey (Lane et al., 1970b). Tenstates, whose populations constituted 11 .6%

7. DEVELOPMENTS IN VACCINATION AND CONTROL, 1900-1966
of the total population of the USA, werechosen, and information was sought therethrough mail surveys directed to practisingphysicians . The states in question were select-ed partly because of their size (not too large)and partly because of the interest shown bytheir state epidemiologists and the presence ofepidemic intelligence service officers assignedby CDC. Some 84% of physicians respondedin 8 of the states and 44% and 49%respectively in the other 2. The questionnairessought information on any patients withcomplications of vaccination .
The physicians' diagnoses were acceptedfor minor complications, but clinical data formore severe complications were thoroughlyreviewed and accepted only if the informa-tion was considered adequate. The resultsof this survey are presented in Tables 7 .5 and7 .6 .
Comparisons of data from different sources
Lack of generally accepted diagnostic cri-teria, within countries and between countries,as well as variability in the completeness ofreporting, makes it difficult to arrive atcomparative judgements . Problems of variouskinds were associated with each of the impor-tant complications. For example, some physi-cians reported patients who had erythemamultiforme accompanying vaccination, oreven accidental infection of a site or siteselsewhere on the body, as "generalized vaccin-ia". Others restricted this term to cases with ageneralized rash (Plate 7 .8C) .
Most important, there were no gener-ally accepted criteria for the diagnosis ofpostvaccinial encephalitis . In some countriesall reports of postvaccinial encephalitis werereviewed by an experienced team ; in othersthe report was based on the views of theattending physician, who might report asencephalitis cases in which convulsions orsome other single symptom occurred, or caseswith high fever and drowsiness after vaccina-tion. In addition, there were always a fewcases of encephalitis due to other causes whichwere merely coincident with vaccination, aproblem that was dealt with in some countriesby national encephalitis surveys .
As regards the USA in 1968, significantlymore cases of all types of complication werefound in the 10-state survey than in thenational survey (compare Tables 7 .4 and 7.6) .This presumably resulted from the moreintensive effort to discover all cases of compli-
303
cations made possible by the methodology ofthe 10-state survey, the data from whichprovide the better basis for comparison ofcomplication rates in the USA with those inother countries .
Eczema vaccinatum . The CDC national sur-vey recorded 58 cases of eczema vaccinatumamong primary vaccinees, 8 among personswho had undergone revaccination and 60,with 1 death, among persons infected bycontact. The frequencies were over 3 timeshigher than this in the 10-state survey (38 .5compared with 10.4 per million after primaryvaccination and 3 .0 compared with 0 .9 permillion after revaccination).
Apart from the CDC survey, few data onthe frequency of this complication are avail-able. In the mass vaccination campaign thatfollowed the importation of smallpox intoNew York in 1947, during which 5-6 millionpeople were vaccinated (but childhood ecze-ma was accepted as a contraindication tovaccination), 10 cases of eczema vaccinatumoccurred among vaccinees and 28 casesamong persons who had not been vaccinatedbut had been in intimate contact with arecently vaccinated subject (Greenberg,1948). There was an outbreak of smallpox inSouth Wales in 1962-1963 and about 900 000persons were vaccinated . Waddington et al .(1964), who probably saw all patients withsevere skin eruptions, recorded 35 cases ofeczema vaccinatum (10 in vaccinees, 25 inunvaccinated contacts), with 2 deaths . Theauthors emphasized that the severity of ecze-ma vaccinatum was independent of the activ-ity of the underlying eczema, which in mostpatients was quiescent at the time of infection .This suggests that the virus often reached theskin by the haematogenous route, rather thanas a result of the direct infection of eczema-tous lesions .
Progressive vaccinia (vaccinia necrosum). Elevencases of progressive vaccinia were recorded inthe CDC national survey. Four of these-allof whom had received vaccinia-immune glo-bulinwere also identified in the 10-statestudy. In the national survey 6 cases were seenin revaccinated individuals, all of whomshowed evidence of serious pre-existing ill-ness, including leukaemia, Hodgkin's diseaseand lymphoma . Only 1 case occurred in achild, a 22-month-old infant with a congeni-tal immune disorderBruton's hypogamma-globulinaemia . There were 4 deaths, despitetreatment with vaccinia-immune globulinand metisazone .

304
SMALLPOX AND ITS ERADICATION
Table 7.3 . Complications of smallpox vaccination in the USA for the year 1968, as determined by the CDCnational survey . Numbers of different kinds of complication by vaccination status and agea
< I1-45-910-1415-1920
Age unknownTotal
Grand total
14 168 000
a From Lane et al . (1969) .b Figures in parentheses indicate numbers of deaths attributable to vaccination .C Includes 31 patients with unknown vaccination status .
Table 7.4 . Complications of smallpox vaccination in the USA for the year 1968, as determined by the CDCnational survey . Data of Table 7.3 expressed as cases per million vaccinationsa,b
a From Lane et al . (1969) .b omits 114 patients with contact-acquired vaccinia .C Rate computed on the basis of 3 cases or less .
Conybeare (1964a) reported 8 cases ofprogressive vaccinia (with 7 deaths) among 5million vaccinees in England and Wales overthe years 1951-1960. All occurred after the pri-mary vaccination of infants less than 6 months
Number of cases
old, most of whom were probably sufferingfrom congenital immunodeficiencies .
Generalized vaccinia . Being a relatively mildcondition, generalized vaccinia was recordedmuch more frequently in the 10-state than in
Vaccination statusand age (years)
Postvaccinialencephalitis
Progressivevaccinia
Eczemavaccinatum
Generalizedvaccinia
Accidentalinfection Other Total
Primary vaccination< I 6.5 - 8 .1 70.0 11 .4 16.3 1 12 .41-4 2.2 0 .4c 11 .3 17 .2 33 .3 14.6 79 .05-9 3 .2 0 .6c 7.1 12.9 20 .6 5 .2 49 .610-19 - 2 .5c 7.4 12.3 7 .4 2.5c 32 .0>_20 3 .5c 6 .9C 24.3 45 .1 13 .9 17.4 111 .1Total 2 .9 0 .9 10 .4 23 .4 25 .4 11 .8 74 .7
Revaccination<I - - -1-4 - 2 . IC - - 2.Ic 4 .2C5-9 0 .6C 2.4 0.6c 1 .8c 1 .2c 6 .710-19 0 .4C 1 .1 - - - 1 .520 I .I 2.4 0 .8C 1 .6 5 .8
Total 0 .7 0.9 1 .2 0 .8 1 .0 4 .7
Post-vaccinial
encephalitisb
Progressivevacciniab
Eczemavaccinatumb
Generalizedvaccinia
Accidentalinfection
Other Total
4 (3) 0 5 43 7 10 696 I 31 47 91 40 2165 (1) 1 (1) 1 1 20 32 8 770 0 I 2 1 1 50 1 (1) 2 3 2 0 8
1 2 7 13 4 5 320 0 I 3 5 2 1
116 (4) 5 (2) 58 131 142 66 418c
0 0 0 0 0 0 00 0 1 0 I 1 30 1 (1) 4 1 3 2 1 10 0 1 0 0 0 10 I 2 0 0 0 30 4 (1) 0 9 3 6 220 6 (2) 8 10 7 9 40
0 0 4 0 9 1 140 0 38 (I) I 16 6 610 0 8 0 7 0 150 0 0 0 2 0 20 0 I 0 1 0 20 0 9 I 9 0 190 0 0 0 0 I 10 0 60 (1) 2 44 8 114
16 (4) 1
1 (4) 126 (I) 143 193 83 572
Vaccination status
Estimatedand age (years)
number ofvaccinations
Primary vaccinations< I 614 0001-4
2 733 0005-9
1 553 00010-14 295 00015- 1 9 111 000>_20 288 000Age unknownTotal
5 594 000
Revaccination<I 01-4 478 0005-9
1 643 00010-14
1 440 00015-19
1 217 00020
3 796 000Total
8 574 000
Contacts

7. DEVELOPMENTS IN VACCINATION AND CONTROL, 1900-1966
305
Table 7.5 . Complications of smallpox vaccination in 10 states of the USA for the year 1968 . Numbers ofdifferent kinds of complications by age and vaccination statusa
a From Lane et al . (I970b) .b Includes 65 patients with unknown vaccination status .
Table 7.6 . Complications of smallpox vaccination in 10 states of the USA for the year 1968 . Data of Table 7.5expressed as cases per million vaccinationsa,b
a From Lane et al . (I 970b) .b Omits 45 patients with contact-acquired vaccinia .c Total includes 59 patients of unknown age .d Total includes 4 patients of unknown age .
the national survey in the USA (241 .5 permillion primary vaccinations compared with23.4 per million among the same group in thenational survey) . Generalized vaccinia wasrare in persons undergoing revaccination .
Conybeare (1964a) recorded 162 cases inabout 5 million vaccinations and revaccin-ations carried out in England and Wales in1951-1960. The lesion at the vaccination sitematured normally, but 9-14 days after vac-
cination papular lesions appeared elsewhereon the body ; these became vesicular and thenpustular before scabbing . On any individualpatient the lesions usually varied considerablyin size. One hundred and fifty cases occurredin primary vaccinees and 106 in infants lessthan 1 year old . The accompanying constitu-tional disturbance was mild .
Accidental infection . Not surprisingly, manycases of accidental infection were not re-
Vaccination statusand age (years)
Post-vaccinial
encephalitis
Progressivevaccinia
Eczemavaccinatum
Generalizedvaccinia
Accidentalinfection
Erythemamultiforme
Other Total
Primary vaccination< I 42 .3 - 14 .1 394.4 507 .0 436.6 154.9 1549 .31-4 9 .5 3 .2 44.2 233 .4 577 .3 157.7 236 .6 1 261 .85-19 8 .7 - 34.9 139 .7 371 .2 87.3 214.0 855 .9> 20 - 30.3 212.1 606 .1 30.3 636 .4 1 515 .2Totalc 12 .3 1 .5 38.5 241 .5 529 .2 164.6 266 .2 1253 .8
Revaccination<I1-4 - - 198 .1 72.7 18 .2 200 .05-19 - - 2.0 9 .9 47 .7 2.0 23 .9 85 .5> 20 4 .5 6 .8 4.5 9 .1 25 .0 9.1 54 .5 113 .6Totald 2 .0 3 .0 3 .0 9 .0 42 .1 10.0 39 .1 108 .2
Vaccination statusand age (years)
Estimatednumber of
vaccinations
Post-vaccinial
encephalitis
Progressivevaccinia
Eczemavaccinatum
Generalizedvaccinia
Accidentalinfection
Erythemamultiforme
Other Total
Primary vaccinationb< I 71 000 3 0 I 28 36 31 I I 1101-4 317 000 3 1 14 74 183 50 75 4005-19 229 000 2 0 8 32 85 20 49 196> 20 33 000 0 0 1 7 20 I 21 50Age unknown . . 0 0 I 16 20 5 17 59Total 650 000 8 1 25 157 344 107 173 815 6
Revaccination<I 0 0 0 0 0 0 0 0 01-4 55 000 0 0 0 0 6 4 I II5-19 503 000 0 0 1 5 24 I 12 43> 20 440 000 2 3 2 4 I I 4 24 50Age unknown . . 0 0 0 0 1 1 2 4Total 998 000 2 3 3 9 42 10 39 108
Contact<1 0 0 0 0 1 0 1 21-4 0 0 4 I 12 1 0 185-19 0 0 6 0 5 0 0 11>20 0 0 3 0 11 0 0 14Age unknown 0 0 0 0 0 0 0 0Total 0 0 13 I 29 1 I 45
Grand total 1 648 000 10 4 41 167 415 118 213 968

306
SMALLPOX AND ITS ERADICATION
ported and therefore did not figure in the
Table 7 .7 . Vaccination status of subjects with ocularCDC national survey. The rates in the 10-statesurvey were about 20 times higher (25 .4 permillion primary vaccinations in the nationalsurvey ; 529.2 per million in the 10-statesurvey). Very few cases occurred afterrevaccination .
A special kind of accidental infection onwhich some statistics were collected was thatassociated with ocular lesions (Plate 7 .8D) .Sedan et al . (1953) recorded 19 cases among850 000 vaccinees in Marseilles in 1952 (22 .3per million), and Waddington et al . (1964)noted 11 cases of vaccinia on the eyelid among900 000 vaccinees in South Wales in 1962 .The most comprehensive report (Ruben &Lane, 1970), derived from cases detected bythe perusal of requests for vaccinia-immuneglobulin addressed to the American RedCross, records 348 cases, most of which cameto light in the years 1963 and 1968, whenspecial national surveys had been conducted .There were also some cases that occurred in1964, 1965 and 1969 . Corneal involvementoccurred in 22 cases and produced a muchhigher rate of residual ocular defect (Table7.7) .
Postvaccinial encephalitis. Although compari-sons of data were difficult because of thevariability of the criteria for making thediagnosis and the extent of reporting, thefrequency of postvaccinial encephalitis variedgreatly in different countries. Table 7.8 pre-sents data from 5 countries (9 series of studies)which illustrate dramatically the large differ-ences reported, especially for postvaccinialencephalitis after the primary vaccination ofindividuals over 2 years of age. All thestatistics presented probably include a fewcases of encephalitis that were merely coinci-dent with, rather than caused by, vaccination,but the differences in frequencies are so greatthat they could not have been due solely todiagnostic or statistical eccentricities .
Postvaccinial encephalitis was much morecommon in European countries than in theUSA, and more common in the countries ofcontinental Europe than in the United King-dom. There were also differences in the ageincidence. In most countries postvaccinialencephalitis was considered mainly a risk ofprimary vaccination in adolescents or youngadults, but in the USA the higher inci-dence of encephalopathy in infants under theage of 1 year led to a recommendation thatcompulsory vaccination should be postponeduntil the 2nd year of life . More detailed
a Based on Ruben & Lane (1970) .b Figures In parentheses indicate numbers of cases showing
residual defects .
analysis of the data used in Table 7 .8 forvarious age groups showed that the frequencyof postvaccinial encephalitis was greatest inthe age group 6-12 years .
Wilson (1967) summarized data from manysources which demonstrate that the case-fatality rate for most series of cases ofpostvaccinial encephalitis was about 30%,with a reported low of 9% and a high of57%.
Although host factors were certainly in-volved in a disease believed to have animmunopathological basis (see Chapter 3),the strain of virus appears to have beenimportant in determining the frequency ofpostvaccinial encephalitis. The New YorkCity Board of Health strain, which was theprincipal strain used in the USA, appears tohave been the least likely of the widely usedstrains to cause it, closely followed by theLister strain. Indeed, the frequencies recordedby Neffet al . (1967) and Lane et al. (1969) forindividuals over 1 year of age were so low thatthey could almost be accounted for by thecoincident occurrence of encephalitis due toother causes. However, the rate was muchhigher in the 10-state survey reported by Laneet al. (1970b) .
Although there is no single laboratorytest that can satisfactorily determine the viru-lence of vaccinia virus for man or assess thelikelihood that vaccination will cause post-vaccinial encephalitis, investigations byMarennikova et al. (1969) in mice and rab-bits were consistent with the following classi-fication of several strains in terms oftheir pathogenicity : mildly pathogenic-New York City Board of Health and EM-63 ;moderately pathogenic-Lister, Bern andPatwadangar ; and highly pathogenic-Co-penhagen, Tashkent and Ikeda (see Chapter11, Table 11 .20) .
vacciniaa
Number of cases
Vaccination status Without cornealInvolvement
With cornealinvolvement
Primary vaccination 229 I sRevacclnatlon 14 IContact infection 60 6Unknown 23 0
Total 326 (7)b 22 (4)b

Table 7 .8 . Incidence of postvaccinial encephalopathy (in infants under 2 years of age) and postvaccinialencephalomyelitis (in individuals over 2 years of age) after primary vaccination, in various placesand at various timesa
7. DEVELOPMENTS IN VACCINATION AND CONTROL, 1900-1966
a Based on Wilson (1967) and Lane et al. (1969, 1970b) .b Age less than 4 years .c Age 4 years or more.d From Conybeare (I964b), 1951-1960 and J . Barnes (upublished observations), 1961-1970 .e Age less than I year .fAge I year or more.
Several different strains of vaccinia viruswere used in Belgium and the Netherlandsduring the 1950s ; the incidence of post-vaccinial encephalopathy in infants droppedsubstantially after the Lister strain was intro-duced in the Netherlands in 1963 (Table 7 .9) .In Switzerland and Austria the number ofreported cases of postvaccinial encephalitisfell dramatically after the Bern strain wasreplaced by the Lister strain in 1962 and 1967respectively (C . Fleury, personal communica-tion, 1967 ; Berger & Heinrich, 1973) .
Contraindications to Vaccination
During smallpox eradication programmesin areas in which smallpox was endemic,WHO recommended that no contraindica-tions to vaccination should be envisaged fortwo reasons. First, the risk of smallpoxinfection was considered to be significantlygreater than the risk of complications and,secondly, most vaccinations were carried outby personnel without medical training, whocould not be expected to diagnose correctlyconditions such as eczema. However, it was
307
recommended that very sick individualsshould not be vaccinated, because their subse-quent death might be attributed to vaccina-tion. On the other hand, in countries in whichsmallpox was not endemic, special attentionwas paid to contraindications to vaccination .Instructions as to what physical conditionsshould be regarded as constituting con-traindications varied according to nationalhealth legislation, but the following 4 condi-tions were generally accepted
(1) Immune disorders . These includedagammaglobulinaemia, hypogammaglobulin-aemia, neoplasms affecting the reticuloendo-thelial system and the use of immunosup-pressive drugs. Such conditions substantiallyenhanced the risk of the most serious com-plication of vaccination-namely, pro-gressive vaccinia .
(2) Eczema. Vaccination was contra-indicated in persons who were currentlysuffering from eczematous skin lesions orwhose family included an individual witheczema, because of the risk of eczema vaccina-turn in either the vaccinee or the familymember concerned. However, it was alwaysdifficult to exclude from vaccination persons
Netherlands, 1924-1928(van den Berg, 1946)
6/155 730 39 127/548 420 232
22/441 294Netherlands, 1940-1943(Stuart, 1947)
50 56/160 775 348
0/28 768DOsseldorf, 1948(Femmer, 1948; Stuart, 1947)
0 14/67 068 209
Bavaria, 1945-1953(Herrllch, 1954)
51/1 008 000 56 17/140 800 121
Austria, 1948-1953(Berger & Puntigam, 1954)
6/58 438 103 26/21 323
1 219
34/367 390 6Hamburg, 1939-1958(Seelemann, 1960)
93 12/26 713 0 449
England and Wales, 1951-1970(Dick, 1973)d
51/3 730 000 13 76/7 620 000 10
USA, 1968 : national survey(Lane et al ., 1969)
4/614 000e 7 12/4 980 000f 2
3/71 000eUSA, 1968 : 10-state survey(Lane et al ., 1970b)
42 5/579 000f 9
Encephalopathy Encephalomyelitis
Age less than 2 years Age more than 2 yearsPlace, date (Investigator) Number of Number of
Number of cases/ cases per Number of cases/ cases perNumber of vaccinations million Number of vaccinations million
vaccinations

308
SMALLPOX AND ITS ERADICATION
Table 7.9 . Cases of encephalopathy after the vaccination of infants less than I year of age in the Netherlands,1959-1970a
a Based on Polak (1973) .b Figures in parentheses indicate numbers of deaths .
who had suffered from eczema in the past butdid not have active skin lesions ; such personssometimes experienced eczema vaccinatum .
(3) Pregnancy. It is a general principle toavoid immunization in pregnancy . This poli-cy was followed with smallpox vaccination,because of the risk (admittedly rare) of fetalvaccinia, a usually fatal condition .
(4) Disorders of the central nervous )/stem. Inorder to minimize the risk of postvaccinialencephalitis, disorders of the central nervoussystem in the person to be vaccinated, or infamily contacts, were accepted as contra-indications in many countries . However,there is no evidence that the exclusion of suchsubjects affected the incidence of thatcomplication .
In addition to the above 4 generally ac-cepted contraindications, in some countriesvaccination was considered undesirable forpersons with an acute infectious disease(influenza, measles, etc .), a chronic infectiousdisease (e.g ., tuberculosis) or an allergic con-stitution, or for persons who had been immu-nized against other diseases such as yellowfever, cholera, or typhoid fever on the sameday as the scheduled smallpox vaccination .The justifications were, respectively, the hy-pothetical risk of complications arising frominfection with vaccinia virus in personswhose physical condition was not normal atthe time, and the belief that an interactionbetween the different immunizing agentsmight prevent the occurrence of a properimmunological response .
In most countries in which smallpoxwas endemic, leprosy was also present .Since primary smallpox vaccination oftenprecipitated reactions such as erythema nodo-sum leprosum or neuritis in leprosy patients(Webster, 1959), health officers in these areashad to determine whether patients withlepromatous symptoms should be vaccinated .The WHO recommendation was that leprosy,including lepromatous leprosy, should not bea contraindication in such circumstances,
since the risk of smallpox infection wassubstantially greater than that posed by thereactions concerned (Browne & Davis, 1962) .
Prevention and Treatment ofComplications
Immunoprophylaxis and immunotherapy
Human antivaccinia immunoglobulin(vaccinia-immune globulin), prepared fromthe plasma of recently vaccinated persons,became available in the early 1950s . Potencyrequirements were that it should contain atleast 500 IU of vaccinia antibody per ml, interms of the International Standard for Anti-Smallpox Serum (WHO Expert Committeeon Biological Standardization, 1967) .
It was thought that since some of the moresevere complications of vaccination werecaused by defects in antibody production, theadministration of vaccinia-immune globulinat the time of vaccination might prevent suchcomplications, without inhibiting an activeimmune response. Nanning (1962) reportedon a field experiment in the Netherlands inwhich about 100 000 army recruits werevaccinated, half of them given vaccinia-immune globulin and the other half a placebo .There were 3 cases of central nervous sys-tem complications in the vaccinia-immuneglobulin group and 13 in the placebo group .No study of similar magnitude was conductedelsewhere, but in the Netherlands vaccinia-immune globulin was subsequently used in allprimary vaccinations of adults (Polak, 1973) .Vaccinia-immune globulin was also recom-mended for the prevention of eczema vaccin-atum, being administered at the time ofvaccination, whenever an eczematous childhad to be vaccinated because of specialcircumstances, such as exposure to a case ofsmallpox (Sharp & Fletcher, 1973) .
Kempe (1960) analysed 300 cases of severecomplications of vaccination treated withvaccinia-immune globulin . There was noevidence that it influenced the course of
PeriodNumber ofvaccinations Vaccinia strain Number of casesb
Number of cases permillion vaccinations
1959-1962 821 000 Copenhagen 31 (16) 37 .71963-1970 1 708 000 Lister 19 (11) 11 .1

7. DEVELOPMENTS IN VACCINATION AND CONTROL, 1900-1966
postvaccinial encephalitis, but observationson 132 treated cases of eczema vaccinatumsuggested that it reduced the mortality fromthe usual level of 30-40% to 7% . It was alsouseful in treating 28 cases of accidental auto-inoculation with vaccinia virus, and led tothe prompt cessation of the development ofnew lesions in 62 patients with general-ized vaccinia. However, vaccinia-immuneglobulin was much less effective in treatingcases of progressive vaccinia, because themajor immunodeficiency in these cases was incell-mediated immunity. Vaccinia-immuneglobulin administration was associated withthe production of neutralizing antibody incases of eczema vaccinatum, generalized vac-cinia and progressive vaccinia . Kempe treatedall subjects who presented, holding that thecases were few in number and occurred onlysporadically and that the early indications ofthe value of the treatment made it ethicallydifficult to withhold its use . In another study,Sharp & Fletcher (1973) observed rapidimprovement within 48 hours of the admin-istration of vaccinia-immune globulin tocases of generalized vaccinia, eczema vaccina-turn and severe local vaccinial reactions .
ChemotherapyIn the 1950s and 1960s several chemicals
were found to inhibit vaccinia virus replica-tion in cell cultures and in laboratory animals .In addition to being investigated for thetreatment of smallpox (see Chapter 1), theywere tested for the treatment of com-plications of vaccination . The most effectivesubstances in experimental systems were de-rivatives of cytosine arabinoside, rifampicin, aurea derivative of diphenyl sulfone, and athiosemicarbazone derivative termed metisa-zone (N-methylisatin f3-thiosemicarbazone).There was no evidence that any of them waseffective, although Brainerd et al . (1967)reported that the use of metisazone had abeneficial effect in progressive vaccinia, acondition in which vaccinia-immune globu-lin was useless .
Reconsideration of Vaccination Policies inNon-endemic Countries
As smallpox transmission was interruptedin various countries, the occasional untowardresults of routine vaccination graduallyemerged as a public health problem, which
309
Plate 7.10 . C . Henry Kempe (1922-1984) . AsProfessor and Chairman of the Department of Pedi-atrics at the University of Colorado Medical Center,Denver, USA, Kempe was a major figure in theinvestigation of complications of vaccination inchildren in the USA during the 1950s and 1960s . Healso participated in the extensive investigations ofsmallpox carried out with Dr A .R. Rao in Madras,India, over the same period .
concerned both the general public and healthadministrators . In essence, in smallpox-freecountries routine vaccination was maintainedor mass vaccination campaigns were under-taken in order to maintain a protective barrieragainst the spread of smallpox in the popula-tion, but this community benefit was gainedat the expense of a few individuals whosuffered from the complications of vaccin-ation . For example, the last case of smallpox inthe USA was reported in 1949 but routinevaccination continued until 1972. The na-tional survey of vaccination in the USAduring 1963 carried out by CDC (Neff et al .,1967) showed that among the 14 millionpersons who were vaccinated against small-pox in that year (6 .2 million primary vac-cinations and 7 .8 million revaccinations),there were 132 cases of severe complicationsand 7 deaths . From the results of this survey, itcould be roughly estimated that between 1949and 1972 there may have been about 3000cases of severe vaccinial complications, withsome 150 deaths .
Lane & Millar (1969) compared the pro-jected number of deaths from routine vaccina-tion in the USA for the 30 years from 1970 to2000 with what might be expected if this

310
SMALLPOX AND ITS ERADICATION
procedure were replaced by vaccination ofonly high-risk groups (military draftees, hos-pital workers and international travellers), incombination with ring vaccination of con-tacts (at most 5000 per importation) andoccasional mass vaccination campaigns tocontrol smallpox outbreaks resulting fromimportations . They concluded that theremight be 210 vaccination deaths if routinevaccination were continued, compared with60 deaths from the vaccination of high-riskgroups. There would have to be 21 separateimportations of smallpox to make up thedifference of 150 deaths ; but no cases hadbeen imported into the USA during theprevious 20 years and the risk was constantlydiminishing. Dick (1973) carried out a similarkind of calculation for the United Kingdomand concluded that on the basis of themortality due to vaccination in that countrythere would be 150 such deaths if routinevaccination were continued-a figure thatwould be equalled by the number of smallpoxdeaths only if there were 50 importations ofvariola major over the 30 years between 1970and 2000, compared with the 13 which hadoccurred during the preceding 20 years. It isclear that routine vaccination in the UnitedKingdom and the USA, and by analogy inother countries which had long since elimin-ated smallpox, entailed a cost which had beenacceptable when there was a substantial risk ofsmallpox, either endemic or imported, butwhich was not justified when the risk hadbecome very slight .
Aside from the risks inherent in routinevaccination, complications posed a severeproblem when a country in which smallpoxwas not endemic conducted mass vaccinationfor the containment of an outbreak followingan importation. For example, in 1963 small-pox was imported into Sweden from anunidentified Asian country . Twenty-sevencases resulted . A voluntary mass vaccinationcampaign was performed in which about300 000 persons in central Stockholm werevaccinated in the course of a few weeks(Strom & Zetterberg, 1966) . As a result of thevaccination campaign, 77 persons sufferedvaccinial complications (neurological com-plications, 14 ; carditis, 7 ; eczema vaccinatum,7 ; and postvaccinial exanthema, 49) . Withoutvaccination, of course, there would have beenmany more than 27 cases of smallpox .
These experiences provoked substantialdebate among research workers and healthplanners during the 1960s as to whether it was
justified to continue routine smallpox vacci-nation in countries in which smallpox was nolonger endemic (Benenson, 1974 ; Dick, 1966,1971, 1973 ; Kempe & Benenson, 1965 ;Langmuir, 1974). This was not a new debate .In the geographically isolated country ofAustralia compulsory vaccination had beenadopted in only 2 of the 6 states, andCumpston (1914) calculated that only about30% of the children born in Australiabetween 1860 and 1910 had ever been vaccin-ated. "Conscience clauses" introduced intolegislation enacted in the states in whichcompulsory vaccination of infants was opera-tive reduced the proportion of newborninfants vaccinated each year to less than 10%by 1923 (Cumpston & MacCallum, 1925). Theresponsible state and Commonwealth healthofficers repeatedly inveighed against thislaxity in vaccination, but the state govern-ments took no action . The situation in NewZealand was similar . The threat of smallpoxwas never perceived as great enough to justifythe enforcement of an unpopular measure,and even the large outbreak of variola minorin New South Wales in 1913-1917 (seeChapter 8) was not enough to cause theparliament of that state to pass a compulsoryvaccination act .
By the late 1960s, several countries ofEurope and those of North America hadalready discontinued compulsory routinesmallpox vaccination programmes, but it wasstill common for paediatricians to recom-mend that children should be vaccinated,usually during the 2nd year of life . The reasonfor this recommendation was that it wasbelieved that complications were less com-mon when primary vaccination was carriedout in childhood ; moreover, the Inter-national Health Regulations, as applied inmany non-endemic countries, made thepossession of a valid smallpox vaccinationcertificate almost a sine qua non for interna-tional travel .
Complications: the Overall Picture
The complications arising from vaccin-ation against smallpox clearly posed a seriouspublic health problem in the non-endemiccountries. Several steps were taken to mitigateits effects, notably the substitution of "mil-der" strains of vaccinia virus, such as the NewYork City Board of Health and the Listerstrains, that caused fewer complications, the

7. DEVELOPMENTS IN VACCINATION AND CONTROL, 1900-1966
311
postponement of vaccination until the 2nd or3rd year of life (which greatly reduced the riskof postvaccinial encephalopathy), the use ofvaccinia-immune globulin for the treatmentof complications and the development ofmore attenuated strains of vaccinia virus (seeChapter 11) . Nevertheless, there was an irre-ducible minimum rate of complications, andeven normal primary vaccination was asso-ciated with unpleasant local and generalreactions. The ultimate solution was the dis-continuation of vaccination, which could bedone without argument only if smallpox wereeradicated globally. In addition, universaldiscontinuation of smallpox vaccinationwould result in a substantial saving in healthbudgets covering vaccination programmesand the medical care of patients sufferingfrom complications. These considerations hadbegun to preoccupy the world scientificcommunity during the 1950s and 1960s, andconstituted one of the reasons for promotingthe development of the global smallpoxeradication programme.
PROGRAMMES FOR VACCINATIONAND REVACCINATION
Vaccination and Revaccination of theGeneral Public
By the middle of the 20th century, small-pox vaccination had become part of theroutine immunization programme of mostcountries in the world . The recommended agefor vaccination varied from country tocountry, but it was common practice forprimary vaccination to be done during thefirst 2 years of life and revaccination per-formed when children entered and left pri-mary school. The first report of the WHOExpert Committee on Smallpox (1964) rec-ommended that in countries in which small-pox was endemic, primary vaccination shouldbe carried out as early as possible, preferably inthe neonatal period, and repeated about 12months later . For revaccination, a 5-10 yearinterval was recommended for the non-endemic countries and one of 3 years for theendemic countries. In North America andsome European countries, hospital staff were,in theory, obliged to be vaccinated every 3years, but as smallpox faded from memory thisrequirement was rarely enforced.
Because of the relatively high incidence ofpostvaccinial encephalopathy among infants
in the USA revealed by the CDC surveys, itwas recommended that primary vaccinationshould not ordinarily be carried out duringthe first 2 years of life . On the other hand,public health experts in many Europeancountries, noting that the highest incidenceof postvaccinial encephalitis was in adoles-cents undergoing primary vaccination, rec-ommended that this immunization should beperformed during the 2nd year of life.
Simultaneous Vaccination with SeveralAntigens
Smallpox vaccination was often carried outat approximately the same time as immuniza-tion with diphtheria and tetanus toxoidor with inactivated antigens of pertussis,typhoid and poliomyelitis, since it was con-sidered that such a practice was safe and didnot interfere with the immune responses toeach agent (Winter et al., 1963) . However, itwas important not to use the same arm for theinjection of bacterial antigens as had beenused for the inoculation of smallpox vaccine afew days earlier, in order to avoid the severefebrile reactions that occasionally resulted (A .S. Benenson, personal communication, 1982) .
Studies were carried out during the 1950sand 1960s to find out whether the combineduse of various live vaccines would affect theirsafety and efficacy. The simultaneous admin-istration of oral poliovaccine and smallpoxvaccine caused no particular problems eitherin terms of increased side-effects or reducedtake rates (Karchmer et al., 1971 ; Winter etal ., 1963). Other studies showed that combi-nations of smallpox vaccine, BCG vaccine(Lin, 1965), yellow fever vaccine (Meers,1960), and measles vaccine (Breman et al.,1975) were safe and produced good immuneresponses. In these studies, separate vaccineswere administered simultaneously at differentsites. However, when smallpox, measles andyellow fever vaccines were combined andinoculated by jet injection into the same site,there were no untoward effects but theimmune response for yellow fever virus wasreduced (Meyer et al ., 1964b) . When smallpox,yellow fever, measles and diphtheria-pertus-sis-tetanus (DPT) vaccines were administeredat separate sites by jet injection, the responseto smallpox vaccine was unaffected but themeasles seroconversion rate dropped from89% (if DPT was not given) to 70% (Rubenet al., 1973) . However, this apparent decrease

312
SMALLPOX AND ITS ERADICATION
was not observed in later studies, and simulta-neous administration of the antigens com-monly used in developing countries in the1970s was generally regarded as safe andefficacious (Foege & Foster, 1974). In prac-tice, the commonest combinations weresmallpox and yellow fever vaccines (in muchof francophone Africa) and simultaneousimmunization against smallpox and measles,in the CDC-assisted programme in westernand central Africa (see Chapter 17) . Small-pox and BCG vaccinations were given simul-taneously but in opposite arms in manycountries in central and eastern Africa .
Vaccination of International Travellers
The 1944 International Sanitary Conven-tion (United Nations Relief andRehabilitation Administration, HealthDivision, 1945) amended the previousConvention, formulated in 1926, and deviseda vaccination certificate (Plate 7 .11), whichrequired that the vaccinial reaction should beinspected 8-14 days after the primary vacci-nation and 48 hours after revaccination . Acertificate was not valid for more than 3 years .
On 9 April 1951, a special committee onthe drafting of the International SanitaryRegulations (the former International Sani-tary Conventions) met in Geneva (WorldHealth Organization, 1951a). During theCommittee's sessions, the original draft formof the vaccination certificate was extensivelyamended (World Health Organization,1951b ; Plate 7.12A). As revised (Plate 7 .12B),this form was adopted by the Fourth WorldHealth Assembly on 25 May 1951 . When, in1981, the vaccination of travellers againstsmallpox was no longer a requirement a stampwas used to cancel the smallpox vaccinationcertificate but the form was still in use forother vaccination requirements . In 1983 itwas replaced by a new form lacking anyprovision for smallpox vaccination (seeChapter 28, Plate 28 .1) .
As early as 1945, the authorities concernedwith the International Sanitary Conventionstipulated that, in relation to vaccinationcertificates, "recent vaccination shall be takenas meaning evidence of successful vaccinationnot more than 3 years or less than 14 dayspreviously, or evidence of an immune reac-tion" (United Nations Relief and Rehabilita-tion Administration, Health Division, 1945) .In 1956, the WHO Committee on Interna-
International Sanitary Convention, 1944.INTERNATIONAL CERTIFICATE OF VACCINATION
AGAINST SMALLPOXTHIS IS TO CERTIFY THAT --
_(Age
Sex) whose signature appears below hasthis day been vaccinated by me against smallpox .Origin and Batch No. of vaccine
Signature of Vaccinator.__Official Position _ ..--- ..PlaceDate
O®cialstamp
Signature of person vaccinatedHome Address._-.___-_
Imporh¢ml Note : In the use of primary vaccination the person vaccinatedshould be warned to report to a medical practitioner between the 8th and14th day, in order that the result of the vaccination may be recorded on thiscertificate. In the case of revaceination the person should report within 48hour@ for first inspection in order that any immune reaction which has de-veloped may be recorded.
THIS IS TO CERTIFY THAT the above vaccination was in-spected by me on the date(s) and with the result(s) shown here •under :Date of Inspection
Result .
----- --
---- -------
.. ._ .
OfilclalStamp
Signature of Doctor
--
-Official PositionPlace _
_- .Date..._.____. ..
Use one or other cf the following terms in stating the result, viz :"Reaction of immunity," "Accelerated reaction (vaccinoid),""Typical primary vaccinia ." A certificate of "No reaction" willnot be accepted .
Signature of person vaccinated --- .... .. . .. ..___(This certificate is not valid for more than 3 yews frown date of
issue) .
40
Plate 7.11 . The first International Certificate ofVaccination against Smallpox, developed by the Inter-national Sanitary Convention in 1944 .
tional Quarantine noted that although theserules "may lack a firm scientific basis, they arenevertheless administratively expedient inorder to avoid delay to persons on an interna-tional voyage" (World Health Organization,1956). The maximum interval of 3 years, inparticular, lacked a carefully documentedbasis, although Marsden (1936) had discov-ered no cases of variola minor in personsvaccinated less than 7 years earlier, and beforethat Hanna (1913) had found that variolamajor was rare and mild in children under 4years of age who had been vaccinated ininfancy, but severe (case-fatality rate, 45 %) inunvaccinated children in that age group (seeChapter 1, Table 1 .11). Subsequently, Rao(1972) reported that only 90 out of 2181 casesof variola major in children under 4 years ofage occurred in those with a vaccination scar .
Nyerges et al . (1972) reported that thelevels of neutralizing antibody 3 years afterthe last revaccination were as high as thosefound 3 weeks after primary vaccination .Taking the absence of rises in the level of

7. DEVELOPMENTS IN VACCINATION AND CONTROL, 1900-1966
72
WHO RIOULATIONS No . It INTERNATONAL -ANITARY REOULATONI
Appendix 4INTERNATIONAL CERTIFICATE OF VACCINATION OR REVACCINATIONAGAINST SMALLPOXCERTWICAT INTERNATIONAL DE VACCINATION OU DE REVACCINATIONCONFINE LA VARIOLE
:raed:nd(a) aSA. I... )tie } --
~ } ._. .wwM1r,e n,n.m. frllrw. Jdoor le vwmm ewt
_ . . . .
...~ a the f[e7 to tea muf(e7remo.tr
vmok 1 tam mdiit r
.llrue .
Amexe 4
The teeter of vewinetlon or revecdnaen to be reorded In the meowing tai..POSITIVE O,:OS. when an erlerated Inie . rr rodion (va¢inoid) sperms
Z- thfifth end eighth day inclusive, or if a typical puatuler --to..NEGATIVE or to .. at,NEG . when no reaction or early non-vesicular reaction appearsduring the four days following the
r lI . . .The term "Rrani .e of immunity" will n It a used .This urhficate is valid for Ihrm ywrs from the date of vauimtion rr . .it reu .tor
y soyother p
.I slam of the vaoina man a unified by the heahhb
authorityor y any other person qualified to do so . b y N Government of the m,,1 -,Ithe ots , me
issued or when the
tl health eerice or thhe e -Id place. If thp he Star,e.be er of a
n.l o m a le m
ed E
.f s setthe placing
the unifira0 of IbI Mtial stttmp If Fii servo . wit] aufio. In the eauof the Armed rm F ... the localioa of the issuing unit is not required .Any emend.. ., o
wII, Of Ibis certificate, or failure to omelets any part ofrL may render it invalid.Le rlmlut de la vaccination nu de la rcveuinedon dolt !lm indiqud de la POSITIVE ou POS
. lorsgv'une rru
rreiculeim a—lrde (veuinolde) ure II cinquidme el le huiiilme lour (indui), Ou en cas de rludirn-milentypique (pustule) .A
haemagglutinin-inhibiting antibodies afterrevaccination as evidence of resistance to viralinfection, these investigators found that suchresistance increased with each successive 3-year revaccination, and suggested that therevaccination interval of health personnelat high risk could be prolonged beyond 3years after 2 successful revaccinations. Thisresult suggests that for international travel-lers the 3-year interval was conservative, but,as the WHO Committee on InternationalQuarantine had concluded, it was administra-tively convenient, and continued to be ac-cepted as long as vaccination certificates wererequired .
The day on which the certificate becamevalid after primary vaccination or revac-cination was often debated at meetings of theWHO Committee on International Quaran-tine. The times agreed on in 1951-namely, 8days after primary vaccination and the dayafter revaccination were consistent with theearliest expected development of the immuneresponse . Modifications, such as 12 or 14 days
313
INTERNATIONAL SANITARY REGULATIONS
49Appendix 4 Amexe 4INTERNATIONAL CERTIFICATE OF VACCINATION OR REVACCINATIONAGAINST SMALLPOXCERTIFICAT INTERNATIONAL DE VACCINATION OU DE REVACCINATIONCONTRE LA VARIOLEThis ousaisnf(e)ifceettiifie woe l .
weft) le birth J
-- - sett 1whose
to,, follows ~-
._. .
._door la sienama suit
-aaetI v file He) ::d
.,itnA)e)vwait, ]a-H.I. °oriole & `Is d data
I.As .
The validity of this certificate shall emend for a period of three years . beginningeight days alter the date of a successful primary vaccinahon or. It the event of, rcvac-unalion, oo the date of that reThe approved stamp mentiouedcIII- e must be in a form prescribed by the healthadministration of the territory in which the vaccination is performed .Any amendment of this certificate . or erasure, or failure to complete any part ofit, may render it invalid .La validitl de ce certifical couvre tune plriode de role
ncant hoot jour.aproe la date do la primovaccination effectude acre autos (prim) oI, dues le cas dunenation, le jour de cello revacciouAon .rovaLE niche[ d'authenlificetion don We conforms au models prescrit par I'adminis-tration sanitaire du lerritoire vu 1, vaccnation est effectule .Touts correction ou rstate scar Ie certifictt ou ('omission dune q,,] . .. q- tiesmentions gv'il comporle peat affeder ea Yalidill .
B
Plate 7.12. A: The form proposed to the Fourth World Health Assembly in 1951, by the committee draftingthe International Sanitary Regulations . B: The revised form approved by the Health Assembly .
after the date of both primary vaccination andrevaccination, were suggested, and the obliga-tory inspection of the vaccinial reaction wasquestioned. In a sense, this debate is areflection on the ways in which internationalcommittees sometimes operate, especially inthe absence of a real problem.
It is clear from these discussions thatnational health administrations attached con-siderable importance to the use of vaccinationcertificates, regarding them as one of the mostimportant measures for preventing importa-tions of smallpox . However, although allagree that because possession of a vaccinationcertificate was mandatory more travellerswere vaccinated than would otherwise havebeen the case, the importance of this require-ment is challenged by some critics, who pointout that it was subject to abuse . For example,certificates were not always examined by theappropriate health officer at the point ofentry, and if a passenger had transferred at anintermediate port in a smallpox-free countryhis vaccination certificate might not have
DateSign-or a dp «°
. orSignature tastir!
fn-pron. It. as-i arcarCac et d authe~ficafion
State whether oiimary-i°` whethe :eea~fei ary.Indiaer ail e'ayl d'uneinr`mo-alion ou do rcvacT a iode siimoneelprier ,°'o°ieraieer rd r a ea moa
1 x2
I a4
Wet ufr.I ft, I.varumreur
sirnawre end na°n ti abre CNLa1ylimeu ntifie n
Rn .bRlel S'!^~ee-briar
Dam ofburnus. aucon e
I 1--x
44

314
SMALLPOX AND ITS ERADICATION
been examined at all. Worse, perhaps, wereinstances of deliberate falsification, or theprovision of certificates by travel agencies tounvaccinated customers. Persons who had anapparently valid certificate might neverthe-less contract smallpox if the vaccine ortechnique used had been faulty .
The situation was at its worst during the1960s and 1970s, a period of greatly increased
air travel, which reduced the travelling timebetween even the most distant endemic andnon-endemic countries to a matter of hours .In earlier times, the inspection of all crew andpassengers on ships from overseas ports todetect patients with smallpox had proved auseful method of limiting importations,especially into countries situated at some dis-tance from endemic areas .
![~ 5 ~ Smallpox and the First Vaccine...Dissolving Illusions – Disease, Vaccines, and a History You Don’t Know Smallpox and the First Vaccine [Draft 1.17] © Roman Bystrianyk &Suzanne](https://static.fdocuments.us/doc/165x107/6119f9729d77061d3e784b50/-5-smallpox-and-the-first-vaccine-dissolving-illusions-a-disease-vaccines.jpg)