Developmental Disabilities and Pervasive Developmental disorders Dr. Sophia Hrycko April 4, 2012.
76
Developmental Disabilities and Pervasive Developmental disorders Dr. Sophia Hrycko April 4, 2012
-
Upload
godfrey-porter -
Category
Documents
-
view
219 -
download
0
Transcript of Developmental Disabilities and Pervasive Developmental disorders Dr. Sophia Hrycko April 4, 2012.

Developmental Disabilities and Pervasive Developmental disorders
Dr. Sophia HryckoApril 4, 2012

Objectives
To review Developmental Disabilities
To review Pervasive Developmental Disorders (will only review questions, as topic was covered earlier today)
To discuss comorbidity and treatment options

Case
A 12 y old girl is brought to the Emergency by 2 police officers because of suicidal ideation.She is in handcuffs.
She is screaming, bit her mouth, blood is smeared all over her T-shirt, face and hands.
You are paged urgently. Think about what you want to ask, we will come
back to this……

Developmental Disability
Often diagnosed in infancy Mental retardation is the result of a
pathological process in the brain characterized by limitations in intellectual and adaptive function.
Areas of function affected: communication, self-care, independence, functional/academic skills, work, health, leisure, safety (helpful when you try to take a history, as it can guide some of your questions)

DSM-IV-TR
Mental retardation requires intellectual deficits (IQ measured by standardized test) and deficit in adaptive function (use of measure with deficits in at least two areas of deficits, Vineland Adaptive Behavior Scale: communications, daily living skills, socialization and motor skills)
Manifested before age of 18

TABLE 21–3. Clinical features of mental retardation
Source. Reprinted from American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision. Washington, DC, American Psychiatric Association, 2000. Used with permission.

#1
DSM-IV-TR lists the prevalence of mental retardation in the US as A. 1% B. 3% C. 5% D. 6% E. None of the above

#1A
DSM-IV-TR lists the prevalence of mental retardation in the US as A. 1% B. 3% C. 5% D. 6% E. None of the above

#2
When IQ is used as the sole criterion for mental retardation, the prevalence rate is estimated to be: A. 0.5% B. 1% C. 2% D. 3% E. 10%

#2A
When IQ is used as the sole criterion for mental retardation, the prevalence rate is estimated to be: A. 0.5% B. 1% C. 2% D. 3% E. 10%

#3
The DSM-IV-Tr criteria for mental retardation include ALL of the following essential features EXCEPT:
A. Subnormal intellectual functioning B. Commensurate deficits in adaptive
functioning C. Onset before 18 years of age D.IQ less than 75

#3A
The DSM-IV-Tr criteria for mental retardation include ALL of the following essential features EXCEPT:
A. Subnormal intellectual functioning B. Commensurate deficits in adaptive
functioning C. Onset before 18 years of age D.IQ less than 75 (less than 70)

Epidemiology
About 1% of the population. 1.5 time more common in men High mortality rates with severe or
profound MR because of complications associated with physical disorders.

Etiology
Genetic Down syndrome Fragile X Prader-Willi syndrome PKU Neurofibromatosis Tuberous sclerosis
Developmental/Acquired Environmental/social (organic cause about 50%, pre/peri/post
natal insult)

#4
Moderate Mental retardation A. Reflects an IQ range of 25 to 40 B. Is seen in approximately 3 to 4% of
persons with mental retardation
C. Has an identifiable organic etiology in the vast majority of cases
D. Usually is associated with the ability to achieve academic skills at the second to 3rd grade level
E. All of the above

#4A
Moderate Mental retardation A. Reflects an IQ range of 25 to 40 B. Is seen in approximately 3 to 4% of persons
with mental retardation C. Has an identifiable organic etiology in the
vast majority of cases D. Usually is associated with the
ability to achieve academic skills at the second to 3rd grade level
E. All of the above

Acquired/developmental
Prenatal: rubella, CMV, Syphilis, Toxoplasmosis, Herpes, AIDS, fetal alcohol syndrome
Complications of pregnancy Perinatal Infection, head trauma, etc.

Environmental/Social
Toxic exposure: lead Severe Psychosocial deprivation
Failure to thrive Abuse Neglect Attachment disorder

#5
A. Adrenoleukodystrophy B. Rett’s disorder C. Acquired immune
deficiency syndrome AIDS
D. Rubella E. Cytomegalic virus
CMV F. Toxoplasmosis
Mental retardation with periventricular intracerebral calcifications, jaundice, microcephaly and hepatosplenomegaly
Progressive encephalopathy and MR in 50% of children born to mother with this disorder
An X-linked MR syndrome that is degenerative and affects only females
Diffulse demyelination of cerebral cortex leading to visual and intellectual impairment, seizures, and spasticity, and adrenocortical insufficiency
MR, microcephay, microphthalmia, congenital heart disease, deafness, cataracts

#5A
A. Adrenoleukodystrophy B. Rett’s disorder C. Acquired immune
deficiency syndrome AIDS
D. Rubella E. Cytomegalic virus CMV F. Toxoplasmosis (MR,
diffuse intracerebral calcifications,
hydrocephalus, seizures and chorioretinitis
Mental retardation with periventricular intracerebral calcifications, jaundice, microcephaly and hepatosplenomegaly E
Progressive encephalopathy and MR in 50% of children born to mother with this disorder C
An X-linked MR syndrome that is degenerative and affects only females B
Diffulse demyelination of cerebral cortex leading to visual and intellectual impairment, seizures, and spasticity, and adrenocortical insufficiency A
MR, microcephaly, microphthalmia, congenital heart disease, deafness, cataracts D

Comorbidity
Up to 2/3 of individuals with MR have comorbid mental disorders.
The more severe the MR, the higher the risk for other mental disorders.
Disruptive and conduct-disorder behaviors are more frequent in Mild MR
Autistic disorder more common with severely retarded individuals.

#6
Common manifestations of anxiety in persons with mental retardation include A. Aggression B. Agitation C. Repetitive behaviors D. Self-injury E. All of the above

#6A
Common manifestations of anxiety in persons with mental retardation include A. Aggression B. Agitation C. Repetitive behaviors D. Self-injury E. All of the above

Evaluation
Complete history and physical exam Will need to evaluate Intellectual
function (WISC or WPPSI) and Adaptive function (Vineland Adaptive Behavior Scale)
Sensory screening ( speech, hearing) Laboratory studies:
Genetic testing, metabolic testing, thyroid/lead screening, imaging

Practice Parameters: Evaluation of child with Global Develop. Delay
Metabolic screening NOT indicated in initial evaluation (yield 1%)
Routine cytogenetic studies and molecular testing for FRA X mutation recommended (yield 3.5-10%)
Consider Rett syndrome in girls with unexplained moderate to severe delay
Serum lead when identifiable risk EEG NOT recommended initially unless features of
epilepsy Imaging with MRI > CT if physical findings Shevell et al Neurology 2003 60:367-380

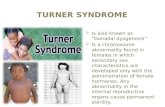
Down Syndrome
Trisomy 21, 95% nondisjunction 1 in 1000 live births 1 in 80 at 40 yrs Hypotonia, upward slanted
palpebral fissures, midface depression, flat wide nasal bridge, simian crease, short stature, increased incidence of thyroid anomaly and congenital heart disease.
Passive, affable 25% ADHD Verbal processing > auditory
processing Increased risk of depression and
dementia as adult

Fragile X
Mutation of the FMRI gene at Xq27.3. Full mutation: CGG trinucleotide repeat > 200 to 230 repeats
Prevalence 1/1000 male births and 1/3000 female birth
Second most known cause of MR of genetic origin (10-12% MR in men)
long face, large ears, midface hypoplasia, arched palate

Men and boys with fragile-X syndrome, showing classical facial features

Fragile X
Macroorchidism Short stature, strabismus, joint
laxity ADHD, anxiety, speech/language
delays, shyness, irritability, stereotypies. LD in some female
Male: moderate to severe MR Female: mild MR

#7
Fragile X syndrome A. Has a phenotype that includes
postpubertal microorchidism B. Affects only males C. Usually causes severe to profound
MR D. Has a phenotype that includes large
head and large ears E. All of the above

#7A
Fragile X syndrome A. Has a phenotype that includes
postpubertal microorchidism B. Affects only males C. Usually causes severe to profound
MR D. Has a phenotype that includes
large head and large ears E. All of the above

#8
Which of the following disorders is least often associated with Fragile X syndrome: A. Autistic disorder B. Schizotypal personality disorder C. Attention deficit/hyperactivity
disorder D. Bipolar disorder E. Social anxiety disorder

#8A
Which of the following disorders is least often associated with Fragile X syndrome: A. Autistic disorder B. Schizotypal personality disorder C. Attention deficit/hyperactivity
disorder D. Bipolar disorder E. Social anxiety disorder

Praeder-Willi Syndrome
Deletion on long arm of chr. 15q11-15q13 (70% paternal, rest maternal uniparental disomy)
1 in 15 000 birth Hyperphagia Obesity Small hands/feet Short stature Microorchidism Fair hair/light skin Almond shaped eyes

Praeder-Willi Syndrome
Obsessions and compulsions
High rates of behavior problems: aggression, temper tantrums, emotional lability, daytime sleepiness
Increased risk for OCD, affective and impulse control disorders.

Phenylketonuria
Autosomal Recessive defect in phenylalanine hydroxylase 12q.24.1 or cofactor 11q22.3-q23.3
Cause accumulation of phenylalanine if untreated and will result in MR (mild to profound), microcephaly, delayed speech, seizures and behavior problems (self-injury, hyperactivity)
Prevalence 1/12 000 Fair skin, blue eyes, blond hair

Tuberous Sclerosis
Autosomal Dominant Mutation in TSC1 gene (hamartin)
9q34 or the TSC2 tumor suppressor gene (tuberin) 16p13
Prevalence 1/6 000 Spectrum of MR, none (30%) to
profound Epilepsy, autism, hyperactivity,
impulsivity, aggression, self-injurious behaviors, sleep problems

Tuberous Sclerosis
Figure 589-2 Tuberous sclerosis. A, CT scan with subependymal calcifications characteristic of tuberous sclerosis. B, The MRI demonstrates multiple subependymal nodules in the same patient (black arrow). Parenchymal tubers are also visible on both the CT and the MRI scan as low-density areas in the brain parenchyma.

Neurofibromatosis type 1
Autosomal dominant 17q11.2 Prevalence 1/3 000 (NF2 1/33 000, 22q) Café au lait spots Neurofibromas Short stature and
macrocephaly in 30- 45%
10% with moderate to profound MR
ADHD, anxiety, mood problems

#9
True or False: Relative to the general population, people with MR are more likely to show autism, behavior disorders, substance abuse, and affective disorders.

#9A
True or False: Relative to the general population, people with MR are more likely to show autism, behavior disorders, substance abuse, and affective disorders.MR: more likely to show psychosis, autism, behavior disorders and less likely to be diagnosed with substance abuse and affective disorder.

Fetal Alcohol Syndrome

Fetal Alcohol Syndrome
Most common preventable cause of MR
1/3 000 live birth Microcephaly, short
stature, midface hypoplasia, short palpebral fissure
Thin upper lip, micrognatia, hypoplastic long/smooth philtrum
Mild to moderate MR, irritability, memory impairment, LD, behavior problems

#10
A. Prader-Willi syndrome
B. Down’s syndrome
C. Fragile X syndrome
D. Phenylketonuria
Attributed to a deletion in chromosome 15
Most commonly occurs via autosomal recessive transmission
Abnormalities involving chromosome 21
Occurs via a chromosomal mutation at Xq27.3
Example of a genomic imprinting

#10A
A. Prader-Willi syndrome
B. Down’s syndrome
C. Fragile X syndrome
D. Phenylketonuria
Attributed to a deletion in chromosome 15 A
Most commonly occurs via autosomal recessive transmission D
Abnormalities involving chromosome 21 B
Occurs via a chromosomal mutation at Xq27.3 C
Example of a genomic imprinting A

#11
Which of the following features does not distinguish autistic disorder from mixed receptive-expressive language disorder? A. Echolalia B. Stereotypies C. Imaginative play D. Associated deafness E. Family history of speech delay

#11A
Which of the following features does not distinguish autistic disorder from mixed receptive-expressive language disorder? A. Echolalia B. Stereotypies C. Imaginative play D. Associated deafness E. Family history of speech delay
(25% for both autistic and language disorders)

Autistic Disorder Associated Features
IQ below 70 for 75% of autistics Uneven cognitive skills Level of receptive language below
expressive language Behavioral symptoms: hyperactivity,
impulsivity, aggressiveness, self-injurious behavior (head banging, finger/hand/wrist biting), temper tantrums
Abnormal mood (giggling or weeping) Lack of fear

Evaluation ( PDD and MR)
History Pregnancy, neonatal and developmental hx,
medical hx, family and psychosocial factors, intervention hx.
Psychiatric examination of the child Medical evaluation
Physical exam, including neurological exam Audiological/visual exam
Psychological evaluation Speech/language/communication
assessment OT evaluation

Differential Diagnosis - PDD
Various PDDs MR not associated with PDD Specific developmental disorder,
e.g. language Early onset psychosis

Treatment Plan Multimodal Establish goals for educational interventions Establish target symptoms for intervention Prioritize target symptoms and/or co-morbid
conditions Monitor multiple domains of functioning
(behavioral adjustment, adaptive skills, academic skills, social/communicative skills, social interactions)
Monitor pharmacological interventions for efficacy and side-effects.

Issues for MD providing care for individuals with Developmental Disability
Overall live longer now: age related illnesses
Coexisting physical and mental health needs
Severity of functional limitation Quality of the environment Quality of the social support

Issues cont
Health problems often present differently (11 y old autistic with moderate-severe DD
presented with abscess secondary to perforated appendix)
Less resources for adults with DD Poorer health: î morbidity, earlier mortality Difficulty communicating pain/distress: non-
specific change in behavior may be the only indication of medical illness or injury

Issues cont
Multiple or long-term use of some medication can cause harm: do review Q3mo: indication, dose, effectiveness, S/E
At Î risk of abuse/neglect: could present with change in wt, non-compliance, aggression, withdrawal, depression, avoidance, poor self-esteem, etc.
Monitor activity level: obesity – Î risk of CV disease, DM, osteoporosis, constipation, early mortality

Issues cont
Vision/hearing problems: often missed Dental disease: most common health
problem with adults with DD– can present with change in behavior
Cardiac Disease: risk F: inactive, obesity, smoking, long term use of antipsychotics
Resp: aspiration pneumonia: most common cause of death (meds, neuromuscular dysf)
GI/feeding problems: Î risk of helicobacter pylori (GH, rumination, exposure to saliva/feces)

Issues cont
Sexuality MSK: scoliosis, contractures, spasticity,
decreased mobility/activity Behavior problems: aggression and self-
injury. It may be a symptom of a health related disorder or circumstance, such as lack of support. BEFORE considering a psychiatric diagnosis, R/O physical causes (infection, constipation, pain, environment: change in residence, support; emotional: stress, trauma, grief.. Dementia in older pt.

Behavior problems
Do a functional analysis of the problematic behavior
Consider decrease or removal of the medications
Before considering pharmacological treatment: address sensory issues, modify the environment, education and skill development, communication aids, psychological and behavior therapy, caregiver support

If you use medication to manage behavior:
Use judiciously Start slow, go slow Do NOT use antipsychotics as first
line of treatment for behavior problems without confirmed diagnosis of psychotic disorders

Potential Targets for Pharmacotherapy
Motor hyperactivity Inattention Repetitive behavior Motor and/or vocal tics Aggression Self-injury

Back to the Case
A 12 y old girl is brought to the Emergency by 2 police officers because of suicidal ideation.She is in handcuffs.
She is screaming, bit her mouth, blood is smeared all over her T-shirt, face and hands.
You are paged urgently. Think about what you want to ask, we will come
back to this……

You want to know
What happened: triggers Background: recent changes? PMHx Past psych hx Meds Allergy

What next?
Now that you know that she is deaf, likely has developmental delay, that she was abused, moved 3 months ago to this group home. Lost her hearing aids.
Is on Quetiapine 150 mg po QHS, 25 mg po QID PRN, clonidine 0.1 mg po QHS. That lorazepam made things worse.
She is still in handcuff, screaming but “medically cleared”…..

What are your options?
Behavior Mod? In ER? Meds? In ER?

#12
A. Autistic disorder B. Childhood
disintegrative disorder
C. Pervasive developmental disorder NOS
D. Asperger’s Disorder E. Rett’s disorder
Normal development for the 1st 6 mo, followed by a progressive encephalopathy:
A better prognosis than other PDD because of the lack of delay in language and cognitive development:
Some but not all the features of autistic disorder:
Occurrence at a rate of 2 to 10 per 10 000 and impairment in social interaction, communication (language or symbolic play) before age 3:

#12A
A. Autistic disorder B. Childhood
disintegrative disorder
C. Pervasive developmental disorder NOS
D. Asperger’s Disorder E. Rett’s disorder
Normal development for the 1st 6mo, followed by a progressive encephalopathy: E
A better prognosis than other PDD because of the lack of delay in language and cognitive development: D
Some but not all the features of autistic disorder: C
Occurrence at a rate of 2 to 10 per 10 000 and impairment in social interaction, communication (language or symbolic play) before age 3: A

#13
Which of the following chromosomal abnormalities is most likely to cause mental retardation? A. Extra chromosome 21 (trisomy 21) B. Fusion of chromosomes 21 and 15 C. XO Turner’s syndrome D. XXY Kinefelter’s syndrome E. XXYY and XXXY Klinefelter’s
syndrome variants

#13A
Which of the following chromosomal abnormalities is most likely to cause mental retardation? A. Extra chromosome 21 (trisomy
21) B. Fusion of chromosomes 21 and 15 C. XO Turner’s syndrome D. XXY Klinefelter’s syndrome E. XXYY and XXXY Klinefelter’s
syndrome variants

References
http://www.mic.ki.se/Diseases/C16.html http://medgen.genetics.utah.edu/thumbnail
s.htm Fra X: http://www.fraxa.org Handbook of Developmental Disabilities SL
Odom, RH Horner, ME Snell, J Blacher eds. 2007 The Guilford Press
Primary care of adults with developmental disabilities. Canadian consensus guidelines. Can. Fam. Physician. Vol 57 May 2011, 541-553

References
Child Adol Psych Clin NA 16 (2007) Fragile X syndrome 663-675 VCFS 677-693 Praeder-Willi 695-708
Fetal alcohol spectrum disorder: Canadian guidelines for diagnosis AE Chudley, J Conry, JL Cook, C Loock, T. Rosales, N LeBlanc CMAJ Mar 1, 2005 172 (5 suppl) S1-S21
www.naddontario.org

References
Volkmar F, Cook et al 1999. Practice parameters for the assessment and treatment of adolescents and adults with autism and other PDD. J. Am. Acad. Child & Adol. Psych. 38 (12 suppl): 32S-54S (erratum 2000 39 (7): 938 and 38:12: 1611-1615
Mental Retardation: A Review of the Past 10 Years. Part 1. B.H. King et al 1997. J. Am. Acad. Child Adole. Psych. 36:12, 1656- 1663 (1664–1671 for part II)

#14
A decline in IQ begins at approximately 10 to 15 years in which of the following disorders? A. Down’s syndrome B. Fragile X syndrome C. Cerebral palsy D. Nonspecific mental retardation E. Fetal alcohol syndrome

#14A
A decline in IQ begins at approximately 10 to 15 years in which of the following disorders? A. Down’s syndrome B. Fragile X syndrome C. Cerebral palsy D. Nonspecific mental retardation E. Fetal alcohol syndrome

#15
The most common inherited cause of mental retardation is A. Down’s syndrome B. Fragile X syndrome C. Fetal alcohol syndrome D. Prader-Willi syndrome E. None of the above

#15A
The most common inherited cause of mental retardation is A. Down’s syndrome (most common
chromosomal abnormality leading to MR)
B. Fragile X syndrome (most common inherited cause of MR)
C. Fetal alcohol syndrome D. Prader-Willi syndrome E. None of the above

#16
Mild mental retardation has been associated with A. Nonspecific causes B. Prader-Willi syndrome C. Females with fragile X syndrome D. Poor socioeconomic background E. All of the above

#16A
Mild mental retardation has been associated with A. Nonspecific causes B. Prader-Willi syndrome C. Females with fragile X syndrome D. Poor socioeconomic background E. All of the above