A Portable Measurement System for the Evaluation of Human Gait

Development and Sensibility Evaluation of the Gait Outcomes Assessment List (GOAL) Module for Children with Lower Limb
Anomalies
by
Jennifer Anne Dermott
A thesis submitted in conformity with the requirements for the degree of Master of Science
Rehabilitation Sciences Institute University of Toronto
© Copyright by Jennifer Anne Dermott, 2015

ii
Development and Sensibility Evaluation of the Gait Outcomes Assessment List (GOAL) Module for Children with Lower Limb
Anomalies
Jennifer Anne Dermott
Master of Science
Rehabilitation Sciences Institute
University of Toronto
2015
Abstract
Background: Functional evaluation of children with lower limb anomalies (LLAs) is limited
due to a lack of appropriate outcome measures for this population.
Objective: To develop a module of the Gait Outcomes Assessment List (GOAL) questionnaire
that is specific and sensible for use with children with LLAs.
Methods: An iterative adaptation and sensibility evaluation of the GOAL was informed by
field-testing this questionnaire with children and their parents, conducting cognitive interviews
with children, and administering an e-Survey to healthcare professionals.
Results: Twenty-five children, 20 parents, and 31 healthcare professionals evaluated the content
and sensibility of the GOAL that ultimately led to 22 of the original 50 items being retained, 16
modified, and six new items added in the final questionnaire iteration (GOAL-LLA 2.0).
Conclusion: This study supports the GOAL-LLA 2.0 as a promising new outcome measure for
comprehensively evaluating the function and priorities of children with LLAs, for both research
and clinical purposes.
iii
Acknowledgments
I would like to thank Unni Narayanan, who, when I first approached him with the idea of
pursuing a graduate degree, responded with enthusiasm, support, and a number of project ideas.
Unni was instrumental in setting me on my path. His commitment to providing children and
families with an opportunity to have a voice is inspiring.
I am grateful to Virginia Wright for agreeing to co-supervise my project. Virginia’s contribution
to my development as a researcher has been exceptional. Regardless of her own grant deadlines
and work demands, or where she was in the world, she could be relied upon for a quick reply.
She was generous with her time and her words of encouragement. I will endeavor to emulate her
attention to written detail.
Nancy Salbach was the ideal addition to my advisory committee, introducing an academic rigour
to my predominately clinical way of thinking. Nancy’s suggestions always improved the depth
and quality of my work. I greatly appreciate that, despite being on sabbatical, Nancy was always
invested in my work, providing timely and thoughtful feedback.
I am eternally grateful to my husband Dean, for without his unwavering support I would never
have been able to complete a thesis, work full-time, and raise a family. To my extended family,
who has always stood by with love and support, and provided an extra hand when needed. To my
sons, Jack and Sam, I hope I have been able to exemplify the merits of working hard to obtain
your goals. The past couple years has not been easy for any of us but the fact is, we survived and
I feel we are actually the better for it.
I would like to acknowledge support through Holland Bloorview Graduate Support program,
SickKids Continuing Professional Development Fund, and the University of Toronto Open
Fellowship. I would also like to acknowledge Unni’s research team (Shannon Weir, Clarissa
Encisa, and Rachel Moline) who always responded to my questions so promptly, and his past
students (Benjamin Davidson, Falisha Karpati, and Edwin Ho) for their foundational GOAL-CP
work.

iv
Table of Contents
Table of Contents ........................................................................................................................... iv
List of Tables ................................................................................................................................ vii
List of Figures .............................................................................................................................. viii
List of Appendices ......................................................................................................................... ix
List of Abbreviations ...................................................................................................................... x
Chapter 1 Introduction .................................................................................................................... 1
Chapter 2 Lower Limb Anomalies ................................................................................................. 3
2.1 Characterization and Epidemiology ..................................................................................... 3
2.2 Treatment ............................................................................................................................ 3
2.2.1 Rationale and Goals of Treatment .......................................................................... 4
2.2.2 Conservative (Non-surgical) Management Options ............................................... 5
2.2.3 Surgical Options ...................................................................................................... 5
Chapter 3 Outcome Measurement in Children with Lower Limb Anomalies ................................ 8
3.1 The International Classification of Functioning, Disability, and Health ............................ 8
3.1.1 Linking Health-related Measures to the International Classification of
Functioning, Disability, and Health ........................................................................ 9
3.2 Current Outcome Measurement in Children with Lower Limb Anomalies ..................... 10
3.2.1 Technical Outcomes .............................................................................................. 10
3.2.2 Functional Outcomes ............................................................................................ 11
Chapter 4 Gait Outcomes Assessment List (GOAL) .................................................................... 19
4.1 Background and Rationale ................................................................................................ 19
4.2 Application of the Gait Outcomes Assessment List to Children with Lower Limb
Anomalies- Sensibility ...................................................................................................... 22
Chapter 5 Rationale and Study Objectives ................................................................................... 25
5.1 Rationale ........................................................................................................................... 25

v
5.2 Purpose .............................................................................................................................. 26
5.2.1 Objectives ............................................................................................................. 26
Chapter 6 Methods ........................................................................................................................ 28
6.1 Study Design ..................................................................................................................... 28
6.2 Child and Parent Perspectives (Phase 1) ............................................................................ 29
6.1.1 Participants ............................................................................................................ 29
6.1.2 Recruitment ........................................................................................................... 29
6.1.3 Data Collection ..................................................................................................... 30
6.1.3.1 Questionnaire Administration (Objectives 1, 3, and 4) ........................................ 30
6.1.3.2 Cognitive Interviews (Objectives 1 and 2) ........................................................... 31
6.1.4 Analysis of Child and Parent Perspectives (Phase 1) ........................................... 32
6.1.5 Child and Parent Sample Size ............................................................................... 34
6.2 Health Care Professional Perspectives (Phase 2) .............................................................. 34
6.2.1 Participants ............................................................................................................ 34
6.2.2 Sampling Recruitment .......................................................................................... 34
6.2.3 Data Collection ..................................................................................................... 35
6.2.3.1 e-Survey Questionnaire (Objective 1 and 2) ......................................................... 35
6.2.4 Analysis of Healthcare Professional Perspectives ................................................ 35
6.2.5 Healthcare Professional Sample Size .................................................................... 36
Chapter 7 Results .......................................................................................................................... 37
7.1 Child and Parent Perspectives (Phase One) ...................................................................... 37
7.1.1 Participants ............................................................................................................ 37
7.1.2 Content Adaptation (Objective 1) ......................................................................... 39
7.1.3 Sensibility Evaluation (Objective 2) ..................................................................... 47
7.1.4 Children versus Parent Response (Objective 3) .................................................... 49
7.1.5 Item Scores versus Importance Ratings (Objective 4) .......................................... 50

vi
7.2 Healthcare Professional Perspectives (Phase Two) .......................................................... 51
7.2.1 Participants ............................................................................................................ 51
7.2.2 Content Adaptation (Objective 1) ......................................................................... 51
7.2.3 Sensibility (Objective 2) ....................................................................................... 55
7.3 GOAL-LLA 2.0 ................................................................................................................ 56
Chapter 8 Discussion .................................................................................................................... 57
8.1 Limitations ......................................................................................................................... 63
8.2 Future Directions .............................................................................................................. 66
8.3 Conclusions ....................................................................................................................... 67
References ..................................................................................................................................... 68
Appendices .................................................................................................................................... 77

vii
List of Tables
Table 1. Patient Reported Outcome (PRO) Measures Identified ................................................. 14
Table 2. Categorization of the Items in the GOAL and the Outcome Measures Identified in
Published Paediatric LLA-related Studies, using the ICF Framework ......................................... 22
Table 3. Phase 1 Participants by Questionnaire Version Administered ....................................... 37
Table 4. Child Participant Demographics .................................................................................... 38
Table 5. Summary of Content Adaptation from the Initial to Third Iteration of the GOAL ....... 39
Table 6. Results of the Initial Administration of the GOAL (GOAL-CP) in Phase 1 ................ 41
Table 7. Results of the Second Administration of the GOAL (GOAL-LLA 1.0) in Phase 1 ...... 44
Table 8. Demographics of Phase 2 Respondents ......................................................................... 51
Table 9. Summary of Content Adaptation from the Third to Final Iteration of the GOAL ........ 51
Table 10. Results of the Administration of the GOAL-LLA 1.1 in Phase Two .......................... 53

viii
List of Figures
Figure 1. International Classification of Functioning, Disability, and Health .............................. 9
Figure 2. Priority Framework for Outcomes Assessment ............................................................ 20
Figure 3. Example Scale Used in GOAL Domains Evaluating Self-perceived Ability............... 21
Figure 4. Example Scale Used in GOAL Domains Evaluating Emotions ................................... 21
Figure 5. Illustration of Study Events ......................................................................................... 28
Figure 6. Modified Scale used in GOAL Domains Pertaining to Self-perceived Ability ........... 49
Figure 7. Children's and Parents' Mean Item Scores for the GOAL-LLA 1.1 ............................. 49
Figure 8. Children’s and Parents’ Mean Importance Ratings for the GOAL-LLA 1.1 ............... 50

ix
List of Appendices
Appendix 1. Literature Search Strategy ....................................................................................... 77
Appendix 2. Development of the Gait Outcomes Assessment List (GOAL) ............................. 78
Appendix 3. GOAL-CP ............................................................................................................... 80
Appendix 4. Child Consent Form ................................................................................................ 89
Appendix 5. Determination of Child’s Capacity to Consent ....................................................... 93
Appendix 6. Research Ethics Board Approval ........................................................................... 94
Appendix 7. Research Ethics Board Approval- Holland Bloorview ........................................... 95
Appendix 8. University of Toronto Study Approval ................................................................... 96
Appendix 9. Information Sheet .................................................................................................... 97
Appendix 10. Cognitive Interview Guide .................................................................................... 98
Appendix 11. Cognitive Pretesting Model ................................................................................. 104
Appendix 12. Information Letter for Healthcare Professionals ................................................. 105
Appendix 13. GOAL-LLA 1.0 ................................................................................................... 107
Appendix 14. GOAL-LLA 1.1 ................................................................................................... 117
Appendix 15. Results of the Third Administration of the GOAL (GOAL-LLA 1.1) in Phase 1
..................................................................................................................................................... 127
Appendix 16. GOAL-LLA 2.0 ................................................................................................... 129

x
List of Abbreviations
AAOS: American Academy of Orthopedic Surgeons
ADL: Activities of Daily Living
AMP: Amputee Mobility Predictor
AOFAS: American Orthopedic Foot and Ankle Society
ASK: Activities Scale for Kids
BSCOS: British Society for Children’s Orthopaedic Surgery
CAPP-FSI: Child Amputee Prosthetics Project- Functional Status Inventory
CHQ: Child Health Questionnaire
CORA: Center of Rotation of Angulation
COSMIN: Consensus-based Standards for the selection of health status Measurement
Instruments
CP-QOL: Cerebral Palsy Quality of Life
CP: Cerebral Palsy
CPT: Congenital Pseudarthrosis of the Tibia
CT: Computed Tomography
EBM: Evidence-based Medicine
EFT: External Fixator Treatment
EPIC: Evidence-Based Practice Confidence Scale
FAQ: Gillette Functional Assessment Questionnaire
FMS: Functional Mobility Scale
GDI: Gait Deviation Index
GGI: Gillette Gait Index
GMFCS: Gross Motor Function Classification System
GMFM: Gross Motor Function Measures
GOAL-CP: Gait Outcomes Assessment List for Cerebral Palsy
GOAL-LLA: Gait Outcomes Assessment List for Lower Limb Anomalies
GPS: Gait Profile Score
GRF: Ground Reaction Force
HCP: Health Care Professional
HDQ: HIV Disability Questionnaire

xi
ICC: Intraclass Correlation Coefficient
ICF: International Classification of Function, Disability, and Health
LLA: Lower Limb Anomaly
LLD: Leg Length Discrepancy
LLRS: Limb Lengthening and Reconstruction Society
MAD: Mechanical Axis Deviation
MAP: Motion Analysis Profile
MDC: Minimal Detectable Change
mLDFA: Mechanical Lateral Distal Femoral Angle
MPTA: Medial Proximal Tibial Angle
MSTS: Musculoskeletal Tumour Society Rating Scale
PedsQL: Pediatric Quality of Life
PODCI: Pediatric Outcomes Data Collection Instrument
PRO: Patient-Reported Outcome
QAPAQ: Qualitative Assessment of Physical Activity Questionnaire
QOL: Quality of Life
ROM: Range of Motion
SAC: Scientific Advisory Committee
SD: Standard Deviation
SEM: Standard Error of Measurement
TESS: Toronto Extremity Salvage Scale
TSF: Taylor Spatial Frame

1
Chapter 1 Introduction
The purpose of this thesis is to address the need for a comprehensive outcome measure to
evaluate the function (physical and psychosocial) of children with lower limb anomalies (LLAs)
(i.e., orthopaedic impairments that are characterized by deformity, deficiency, and/or length
discrepancies).
The altered structure of the lower limb often presents physical challenges related to a
pathologically abnormal gait, but may also have a social and psychological impact. Outcomes
research related to children with LLAs tends to focus on correction of the impairment, namely
technical outcomes (at the level of body functions and structure) including limb alignment and
length discrepancy, measured radiographically, and post-operative complications and healing
index (1). Although functional (physical and/or psychosocial) improvement is often considered
an aim and important outcome of surgery, a comprehensive measurement of function (at the level
of activity and participation) is rarely reported (2). Indeed, when currently available functional
outcome measures have been used in this population they have proved problematic,
demonstrating limited discriminative ability and an inability to detect change (2-6). For this
reason, some investigators have opted to use non-validated functional status measures they have
created to fulfill their study’s measurement requirement (5, 7-9).
This imperative to develop a standardized functional outcome measure for use with this
population has been identified by a number of paediatric LLA research groups so as to improve
the uniformity and comprehensiveness of patient assessment, to ensure comparable
benchmarking across intervention studies, and ultimately to provide evidence that will give
insight into the assumed functional benefits of treatment (10-13). Moreover, an outcome measure
that identifies patient priorities would facilitate treatment planning that addresses the specific
goals and expectations of each family, as well as align with the philosophy of evidence-based
medicine (EBM), defined as “the integration of best research evidence with clinical expertise and
patient values” (14). If clinical decisions are to serve the patient, their unique preferences,
concerns, and expectations must be integrated (14). To date there are no studies that use
individualized measures to explore children’s or families priorities with regard to treatment of
LLAs.

2
The following sections provide background information about the conditions that result in LLAs,
the functional impact of these, and the treatment options that are available. A framework to
conceptualize function (ICF) will be described. Common outcome measures (technical and
functional) that have been used for children with LLAs, and how these measures fit within this
framework, will be presented. The literature will be reviewed to highlight the gap in functional
outcome measurement, based on the infrequent and problematic use of patient-reported outcome
(PRO) measures for this population. Finally the Gait Outcomes Assessment List (GOAL) will be
introduced and the plans to evaluate and adapt this questionnaire to create a module specific for
children with LLAs will be detailed.

3
Chapter 2 Lower Limb Anomalies
2.1 Characterization and Epidemiology
Lower limb anomaly (LLA) is a broad term that encompasses length discrepancy with or without
limb deficiency (missing or insufficiently developed parts), and/ or deformity (malalignment) of
the lower limb/s. LLAs often present as a structural impairment associated with deficits in
strength and range of motion, and consequently, altered gait mechanics. In terms of specific
types of LLA, lower limb length discrepancies are common, with 23% of the general population
having a discrepancy of 1 centimetre or greater (15), although as the magnitude of difference
increases, the prevalence decreases (3). Large magnitude discrepancies (greater than 1.5
centimetres) occur in about 5% of the population (1). Lower limb deficiencies have a reported
incidence of 2 to 7 in 10 000 births (16). There is a wide spectrum of lower limb deficiencies that
include small or deformed feet, absent or deficient bony segments in the feet, lower leg or thigh,
unstable joints due to absent or deficient ligaments, absent or weak muscles, and inequalities of
length and girth (1, 17). Congenital deficiencies account for approximately two thirds of lower
limb amputations (12). Fibular deficiency is the most common long bone deficiency with an
incidence of 7-20 per million births (18). LLAs might also be acquired as a result of bone loss,
malunion, or abnormal growth following trauma or post-traumatic sequelae, oncologic disease,
or infection (10, 19). A lower limb deformity is characterized by abnormal alignment of the
thigh (femur) and/or lower leg (tibia and fibula) and/or foot and ankle. These deformities might
occur in one or more of the coronal, sagittal, and/or axial (transverse) planes. It is important to
note that these different types of LLAs often coexist. For example, a length discrepancy might
be secondary to a limb deficiency; and may be associated with a deformity that could be in more
than one plane. More details about specific LLAs are provided below in the context of treatment
options (Section 2.2).
2.2 Treatment
The prevailing management philosophy is to correct the LLA, and to this end, children with
LLAs may undergo a multitude of orthopaedic surgeries throughout their childhood. The typical
model of care for the management of these children positions the orthopaedic surgeon as the key

4
healthcare professional (HCP) to inform treatment, with input from other members of the
healthcare team (i.e., nurse, physical therapist, orthotist/prosthetist). If the healthcare team feels
there is a need, the circle of care might be expanded to include a social worker, or a psychologist.
This is because there may be an additional effect of an LLA on an individual’s social and
psychological function. HCPs and families must collectively decide the most appropriate
treatment option (or combination of options) for the individual child. Families rely on HCPs to
provide information related to the rationale and the details of available treatment options
(detailed below).
2.2.1 Rationale and Goals of Treatment
LLAs often result in an abnormal gait pattern and increased mechanical effort (2, 20-22).
Treatment of LLAs aims to minimize these consequences through surgical and non-surgical
techniques (as described in 2.2.2) to level the pelvis, improve symmetry, and allow more even
distribution of joint loads in a bipedal standing position and during stance phase in gait (1). If
uncorrected, compensatory strategies are likely adopted by the child in an attempt to normalize
gait patterns, provide a more stable base of support, optimize energy expenditure, and reduce
joint load (22). The long-term sequelae of these compensatory strategies may include pain, joint
degeneration, and dynamic deformity of adjacent joints (22). Incremental increases in
discrepancy increase the stress across the sacroiliac joint (23). There is general consensus that
in the absence of a deformity, leg length discrepancies less than 2 cm do not require treatment as
these have negligible clinical impact (24, 25). Deformity can cause asymmetry of loading across
all lower extremity joints. Asymmetric loading across the knee joint is a well-recognized risk
factor for the development of osteoarthritis (26, 27).
These gait-related consequences of an LLA not only affect a child physically but may also have a
social and psychological impact. For example, fatigue related to increased mechanical effort,
functional impairments (e.g., limited range of motion), or dissatisfaction with appearance can
limit participation in social and physical activities and can lead to difficulties in social and
psychological adjustment (2, 3, 20).

5
2.2.2 Conservative (Non-surgical) Management Options
Modest leg length discrepancies of less than 6% inequality are amenable to non-operative
treatment (28). Shoe inserts (insoles) can be used to equalize discrepancies up to 1.5
centimetres, and if further correction is needed, the sole of the shoe can be built up externally
(29). It is recommended that external shoe lifts not exceed five centimetres, to minimize the risk
of an ankle sprain, although, if required, an ankle-foot orthosis can provide support to an
unstable joint (30). It is estimated that about 1 in 1000 individuals in the general population have
been prescribed a shoe lift (1). For discrepancies greater than two centimetres, these approaches
become less acceptable as a long-term solution because of the perceived aesthetics including
dissatisfaction with shoe choice, impaired biomechanics and barefoot function, and associated
costs of maintenance and replacement of devices and footwear (1). As a result, individuals are
more likely to either live with their asymmetry or opt for surgical intervention. For massive
length discrepancies, typically related to severe limb deficiencies for which surgical management
might not be feasible, prosthetics (e.g., extension prosthesis) can be used. There are no effective
non-surgical strategies to deal with clinically significant deformities (malalignment) of the lower
limbs. Deformities of the foot can be accommodated with custom orthotics or orthopaedic
footwear.
2.2.3 Surgical Options
2.2.3.1 Limb Reconstruction
There are a number of surgical options to manage limb length discrepancies, limb deformities,
and some limb deficiencies. Limb length discrepancies can be managed by complete
epiphysiodesis (growth plate arrest) or shortening procedures of the longer side, or lengthening
procedures by gradual distraction osteogenesis of the bone/s on the short side using lengthening
devices such as external fixators (EFT) or motorized intramedullary rods. Lower limb deformity
can be corrected using guided growth techniques by temporary or permanent hemiepiphysiodesis
(partial growth arrest), acute deformity correction by osteotomies, or gradual correction by
distraction osteogenesis using external fixators. Many LLAs are managed by various
combinations of the above.
Epiphysiodesis is arrest of the growth plate on the longer side, allowing for the shorter side to
catch up, and is considered an option for projected length discrepancies between two and five

6
centimetres at skeletal maturity (31) or in combination with lengthening techniques to reduce the
magnitude or number of lengthening procedures of the shorter side. Epiphysiodesis does limit a
child’s final standing height therefore it is less likely to be used in conditions associated with
short stature (e.g., Noonan’s syndrome, Turner’s syndrome) or in isolation for more significant
length discrepancies. This is considered a technically simple procedure to perform but must be
appropriately timed, to correlate with remaining growth if it is to be successful. Epiphysiodesis
is no longer an option if there is too little growth remaining (near skeletal maturity) or if the short
limb cannot grow due to growth arrest.
External fixator treatment is used for lengthening and gradual deformity correction using
distraction osteogenesis. Bone is lengthened and or alignment corrected through an osteotomy
that is gradually pulled apart using an external fixator that uses pins and wires to anchor the bone
segments above and below the osteotomy. The rate of distraction of the bone and soft tissues
(including muscles and neurovascular structures) is gradual enough to be tolerated by the patient
and to allow for new bone formation in the gap (regenerate) that is being created at the site of the
osteotomy. There are two categories of external fixators: a monolateral fixator that allows for
lengthening but is less versatile for deformity correction, and a circular or ring-type fixation that
allows for multiplanar correction in addition to lengthening (32).
The maximum amount of length that should be targeted in a single lengthening procedure has
traditionally been no more than 20% of the limb segment length (33). Lengthening beyond this
increases the likelihood of complications including functional deficits related to muscular and/or
neural tissue dysfunction and deformity at adjacent joints (34).
Lengthening may also be performed over an intramedullary nail in conjunction with an external
fixator. The benefit of this technique is that it decreases time in the external fixator by providing
increased stability to the consolidating bone, decreasing the risk of fracture post-frame removal
(9, 35). The possible drawback of this technique is increased risk of deep infection (35). The
possible functional benefit has not been investigated.
Recently lengthening through internal, intramedullary devices has been trialed. Lengthening is
actualized through a mechanical, motorized, or electro-magnetic system. This fully implantable
method of lengthening is becoming more widely available but has not been adequately studied to

7
compare the safety, efficacy, and cost with conventional methods (36). The functional impact of
internal versus external lengthening has not been explored.
2.2.3.2 Amputation
Amputation was once considered standard procedure for severe congenital limb deficiencies in
which the length discrepancy was more than 5 centimetres at birth or predicted to be greater than
15% at skeletal maturity, if there were less than three rays in the foot, and if the foot was unable
to achieve a plantigrade position (8, 28). The decision to amputate is commonly made in infancy
and performed at about the time a child begins to stand (28). Although surgical advances now
permit limb preservation to be considered in cases where amputation would have once been
routine, a non-functional foot continues to be an indication for a Boyd or Syme amputation (37).
Effort is made to achieve an optimal residual limb for prosthetic fitting, which in children may
necessitate additional surgical intervention to account for growth. In a study by Westberry et al.
(38), 117 Boyd procedures were performed on 109 children with approximately one quarter of
these requiring concomitant procedures such as a proximal tibial epiphysiodesis, and one third
requiring subsequent surgical procedures.
Van Nes rotationplasty is an alternative amputation technique that may be considered for femoral
deficiencies. This involves rotation of the lower limb, allowing the ankle to foot to act as a
functional knee joint within a prosthesis. This procedure offers a functional “knee” joint, less
energy consumption and potentially fewer future surgeries but is not always well accepted by
families, because of the cosmetically unusual appearance (39).
If limb preservation (i.e., reconstruction) can be done safely and reliably, many orthopaedic
surgeons consider amputation a last resort (40), even though, the long-term functional outcome
of limb preservation, relative to the previously routine amputation, is not as well documented
(41).

8
Chapter 3 Outcome Measurement in Children with Lower Limb Anomalies
Once the details of the treatment options are well understood by families, they must decide what
is “best” for their child. Families will look to the HCP for guidance related to the expected
outcomes and effectiveness of treatment in achieving these outcomes. As such, there is an
imperative to focus on the measurement of outcomes. As highlighted previously, LLAs are
likely to impact children’s lives on multiple levels (i.e., physical and psychosocial functioning)
so a measurement tool that is designed to capture these levels is necessary to evaluate the
outcomes of treatment.
3.1 The International Classification of Functioning, Disability, and Health
The ICF conceptualizes function as a “dynamic interaction between a person’s health condition,
environmental factors, and personal factors” (42). This framework provides a standard language
with which to communicate and describe the effects of a health condition on one’s functional
ability (43). It defines function as more than traditionally measured structural impairments, and
focuses on how individuals live with their condition (44).
The individual components of the ICF include: body structures (anatomical parts of the body),
body functions (body systems including psychological function), activities (the completion of a
specific task or action), and participation (activities that are performed for a specific purpose or
role), environment (attitudinal, physical, and social), and personal factors (45). Environmental
and personal factors are collectively referred to as contextual factors and can be either facilitators
or barriers to overall function. The ICF illustrates a dynamic and complex multidirectional
interaction between all of its components (Figure 1), suggesting a linear relationship may not
exist between a discrete area of the ICF and overall functional status (44) or between changes
among ICF areas (46). This suggests that outcomes such as range of motion (body function) or
limb alignment (body structure), that are traditional clinician measures of impairment associated
with LLA, may not be valid proxies for functional status. Moreover, one cannot assume that
changes in these outcomes as a result of intervention, will result in the desired changes in other
areas of the ICF.

9
Figure 1. International Classification of Functioning, Disability, and Health (WHO, 2001)
For patients, the most meaningful indicators of the effectiveness of interventions must be tied to
the desired goals of the patient (47). These are more likely to focus on improvements in
activities and participation affected by the condition rather than indicators that focus on
improvements in body structure and function (47), termed technical outcomes by Goldberg (48).
Narayanan suggests that the ultimate desired functional outcomes (focused on activities and
participation) might not require technical perfection (47). For example, maintaining a length
discrepancy up to one centimetre post-lengthening may be advantageous for individuals with an
equinus contracture of the ankle joint to minimize the risk of tripping.
3.1.1 Linking Health-related Measures to the International Classification of Functioning, Disability, and Health
Specific linking rules have been developed to connect health-related measures to the ICF (49,
50). Every item within a measure can be linked to the content coding that has been built into the
ICF classification, and thus also connected to a specific domain of the ICF model. Any item that
does not fit into a domain is classified as ‘not definable’. Personal factors are not coded in the
ICF classification, therefore, were not included in the original linkage rules published in 2002
(50). Three years after being introduced, the linkage rules were revised to increase specificity,
allowing differentiation from other ‘not covered’ concepts (49). This adjustment improves
consistency with the ICF model (49). Once completed, this linkage process illustrates how well
an outcome measure relates to the ICF and also highlights what concepts within the ICF a
specific measure is focused on. This allows for easier comparison among measures and should

10
facilitate researchers and clinicians in selecting the most appropriate measure to meet their needs.
The ICF linkage process is illustrated in section 4.2.
3.2 Current Outcome Measurement in Children with Lower Limb Anomalies
LLA-related literature consists primarily of case series and observational comparative studies of
surgical interventions, with a multitude of outcomes measured. Orthopaedic outcome
measurement has been categorized as either technical (at the level of body functions and
structures) or functional (at the level of activities and participation, environmental and personal
factors) (47).
3.2.1 Technical Outcomes
Traditionally, studies on LLAs provide thorough reports of radiographic outcomes (10). Indeed,
surgical success is often determined radiographically, with the objective being a +/- 5 millimetre
residual length difference and a mechanical axis deviation (MAD) through the centre of the knee
or comparable to the contralateral limb (1, 9, 51-56). Additional components of a deformity
analysis include: centre of rotation angulation (CORA), and standard measures of joint
orientation: mechanical lateral distal femoral angle (mLDFA), medial proximal tibial angle
(MPTA) (1). Femoral and tibial torsion may be assessed on computed tomography (CT) (57),
although more recently, EOS has been validated as a good alternative with equivalent reliability
and accuracy, and a comparatively reduced dose of radiation (58). As suggested previously,
success ascertained radiographically cannot be assumed to result in a successful outcome as
reflected across the other levels of the ICF encompassing physical and psychosocial function.
These “outcomes” reported are related to the efficiency or time needed for treatment rather than
true measures of treatment effectiveness. These are typically based on radiographic evaluation,
of which the most widely used is known as the healing index (1). In the context of limb
lengthening, the healing index is reported as the distraction-consolidation time (in days or
months) required per centimetre of length achieved. Other related numeric measurement
parameters include lengthening time, distraction index, mean time to consolidation, and
weightbearing index (59).

11
Complication rates, which are common, are routinely reported, often using Paley’s classification
of difficulties during limb reconstruction as problems, obstacles, or complications (60).
Clinical impairment measures include joint range of motion (ROM) or strength assessment (1, 9,
51, 52, 54, 61). Measuring ROM during EFT is important for a variety of reasons, as
maintaining adequate ROM throughout EFT prevents muscular atrophy, diminishes joint reaction
forces, avoids cartilage damage, decreases pain, prevents adhesions of muscles to bony
regenerate, and increases blood supply to the bone, inducing bone formation (1). However, as
described earlier, ROM is not a sufficient proxy for overall functional status.
3.2.2 Functional Outcomes
Activity-based clinical outcomes include timed walk tests [e.g., 6- minute walk test (62), Timed
Up and Go (63)] or gait assessment. Assessing gait might involve an observational evaluation
by the surgeon or physical therapist (PT), sometimes as basic as characterizing a limp on clinical
evaluation (9) or noting independent versus assisted gait (61). Conversely, this could involve an
instrumented approach in a motion laboratory to provide a more detailed analysis of gait and
running mechanics, standing balance and postural sway (29). There is little consistency across
studies in the methodology employed in gait analysis, making interpretation and comparison of
results difficult (29). Furthermore, regardless of the approach taken, these measures provide no
direct information on the impact that improving gait speed or symmetry has on the overall
functional status of the individual.
3.2.2.1 Patient Reported Outcome (PRO) Measures
PRO measures allow for direct subjective assessment by the patient on elements of their health
and related function (64) and are considered the best way to measure participation domains of the
ICF (47). It is the individual who has first-hand knowledge of their daily functioning in all
contexts (65), making them the most qualified to report. Narayanan (47) states: “to the extent
that the patient’s perspective is recognized to be pre-eminent in making judgments about
effectiveness, the use of patient-reported outcome (PRO) measures is now considered the
standard when evaluating effectiveness of interventions”.
Despite the widespread use of PRO measures in many areas of health research and clinical care,
the use of PRO measures in pediatric orthopaedics lags behind (66) and was essentially non-

12
existent in all orthopaedic research prior to the 1980’s (67). It is argued that PRO measures are
more difficult to measure and interpret than traditional clinician measured “objective” parameters
(67). However, a major disadvantage of relying solely on traditional clinical outcomes in
evaluative orthopaedic research is that these may not directly relate to patients’ reasons or goals
for undergoing surgery (68, 69). The measured variables may be of interest to the clinician but
not necessarily to the patient being evaluated in the study (67). Furthermore, traditional clinical
outcomes have not always been found to correlate well with PROs (70, 71).
PRO measures can be either generic or condition-specific. In general, condition-specific
measures, designed to focus on issues relevant to a particular condition, are more sensitive to
change than generic ones (72), although the applicability of these measures is limited to the
diagnostic group for which they were designed. There are condition-specific measures available
for use with children that use a prosthetic device [e.g., Child Amputee Prosthetics Project-
Functional Status Inventory (CAPP-FSI), Amputee Mobility Predictor Questionnaire (AMP)].
Similarly, there are condition-specific measures available for use with children that have an LLA
related to sarcoma [e.g., Toronto Extremity Salvage Scale (TESS), Musculoskeletal Tumour
Society Rating Scale (MSTS)]. Most of these condition-specific instruments were developed for
an adult population and there is not always an equivalent measure for pediatrics. A pediatric
version of the TESS (pTESS) has been developed and a multi-centre study is presently
evaluating its psychometric properties (J. Piscione and S. Hopyan, personal communication,
September 14, 2014).
Individualized measures are a distinct type of PRO measures. To date there are no studies that
use these measures to explore children’s or families’ priorities in regard to treatment of LLAs.
There is increasing recognition that children should be consulted on their treatment goals and this
information incorporated into treatment plans (45, 73). Individualized measures allow for these
goals to be captured and measured (74). The initial administration of an individualized measure
requires the child or parent (or clinician) to identify intervention goals with subsequent
administration measuring change that is unique to the individual. Patients find outcomes are
most meaningful when they are aligned with their priorities (47) and attention to patient needs
and circumstances when planning care is associated with improved health care outcomes (75).

13
Examples of individualized measures include the Canadian Occupational Performance Measure
(COPM), the most frequently used individualized measure in paediatric rehabilitation (76), and
the Goal Attainment Scale (GAS). Both these measures were designed for an adult population
but have been used in paediatric studies with success (77). Tam et al (77) found that when these
individualized measures were used in pediatric research, most authors (19 out of 28 studies in
which COPM was used, 22 out of 34 GAS use studies) also employed a standardized fixed item
functional measure to evaluate the effectiveness of intervention.
In general, there are very few studies pertaining to children with LLAs that actually employ a
PRO measure. A literature search was conducted prior to commencement of this project with the
sole purpose of identifying validated PRO measures that have been used in these children.
Medline (1995 to 2013) was used as the source database. The index terms “leg length
inequality”, “limb deformity”, “osteogenesis distraction”, “bone lengthening”, “external fixator”,
“Ilizarov technique”, “femur”, “tibia”, “genu varum” or “genu valgum”, “amputation”, and
“artificial limb” were used in combination with “questionnaire” or the keyword “function”.
Inclusion criteria for detailed review of a publication included: the mean age of participants was
less than 18 years and no participants had upper extremity involvement. See Appendix 1 for the
full search strategy.
The search returned 435 papers, of which six were relevant. It is important to stress that
amputee-, sarcoma-, or joint-specific outcome measures (e.g., CAPP-FSI, MSTS or American
Orthopedic Society Foot and Ankle Society Score (AOFAS)) that were revealed in the search
were not included as the aim was to identify measures that would be applicable across the
spectrum of conditions that result in LLAs. Table 1 lists the six PRO measures identified within
these papers. There were no individualized measures used in any of the identified studies.

14
Table 1. Patient Reported Outcome (PRO) Measures Identified
in LLA-related Literature (1995-2013)
Name Construct Target
Population
Studies Cited
Child Health
Questionnaire (CHQ)
Physical and
psychosocial well-
being of children
(Generic)
Child report for ages
11-17 years; parent
report for ages 2
months up to 5 years
and 5-17 years
The effect of leg
length difference on
health related quality
of life: is the '2cm
rule' appropriate? (3)
Gillette Functional
Assessment
Questionnaire (FAQ)
Functional walking
ability and mobility
skills
(Originally
developed for CP)
Parent report for ages
2+ years
Measurement of
health-related quality
of life in children
undergoing external
fixator treatment for
lower limb
deformities (2)
Activity Scale for Kids
(ASK)
Measure of
children’s physical
ability (capacity
and performance)
(Generic)
Ages 5 to 15 years old Physical activity
assessment in
adolescents with
limb salvage (6)
Pediatric Outcomes Data
Collection Instrument
(PODCI)
Functional and
health outcomes
associated with
paediatric
orthopaedic
conditions
(Generic)
Child and parent
report for ages 11-18
years; parent proxy
report for children
ages 10 years and
under
The correlation of
specific orthopaedic
features of
polyostotic fibrous
dysplasia with
functional outcome
scores in children (4)
Parental perspectives
on leg length
discrepancy (5)
PedsQL Measure of health
related quality of
life
(Generic)
Child report for ages
5-7 years, 8-12 years,
13-18 years; parent
report for ages 2-4
years, 5-7 years, 8-12
years
Measurement of
health-related quality
of life in children
undergoing external
fixator treatment for
lower limb
deformities (2)
The following section summarizes the sample population in each study and what each study
revealed with respect to the PRO measure it utilized. The level of detail in this summary is
considered important to justify the need for this thesis study.
When the Child Health Questionnaire (CHQ) was administered by parent-proxy, in a sample of
children undergoing femoral lengthening, widespread ceiling effects were noted with many of

15
the domain scores close to the maximum scores. Accordingly, it was speculated this measure
may not be adequately sensitive to change or discriminative for the study population (3).
The administration of the Gillette Functional Assessment Questionnaire (FAQ) in children
undergoing EFT showed limited discriminative ability and inability to detect change following
EFT (2). The FAQ was originally developed for children with CP and the reliability and validity
of this assessment has not been established in children with LLAs, putting in question its use as
an outcome tool for this population (78).
Monpetit and colleagues (2) used the PedsQL and showed that it was able to discriminate
between children with leg length discrepancies (LLD) from normative data (derived from healthy
children), and was responsive to change over time as a result of EFT. On the other hand, the
PedsQL effect size related to the impact of EFT was small (total score and physical health
domain) to small-medium (psychosocial health and emotional functioning domain) for child
report, and small (total score and all domains) for parent report, as measured between baseline to
3 months post frame removal. It is possible that this might be an accurate reflection of EFT
impact, however, given the magnitude of clinical change seen with EFT (e.g., up to 20% increase
in limb length) this might also suggest the PedsQL is too generic and therefore underestimates
potentially important clinical change. Further, it remains unclear if the PedsQL can discriminate
among different severities of LLD or if severity impacts responsiveness.
Sheiko et al. (6) used the ASKp-38 for 20 children (mean age 15.8 years) who had undergone
limb salvage to treat bone sarcomas (mean time since initial procedure or major revision = 2.46
years) versus a matched cohort of typically developing youth. Their results show that the
summary score differentiated between groups (p=0.001), however this was related only to
differences in the locomotion subscale scores. The mean score of the other three domains
(personal care, standing, and transfers) was 100, the maximum score of the scale. This
corroborates a previously reported concern about the ceiling effects due to a lack of higher-level
items in the ASK (e.g., competitive sports, climbing activities) (41).
Children with LLA were included in the development of the Pediatric Outcomes Data Collection
Instrument (PODCI) (79), although when Leet et al. (4) looked at the relationship between

16
PODCI scores with specific orthopaedic features, they found no correlation between PODCI
score and deformity of the limbs. In general, the PODCI is considered difficult to score and does
not offer a ‘not applicable’ option for items that are not relevant to a respondent (41).
Lee et al. used the PODCI (5) to investigate the perspectives of parents of children, ages 6-20
years, with an LLD. They found that pain and global function subscale scores were significantly
lower (p<0.05) for children that have a LLD secondary to trauma versus idiopathic etiology.
However, they did not find a correlation between the magnitude of LLD and any of the PODCI
subscale scores, and thus concluded the PODCI may not be useful in evaluations of children with
LLDs.
Within the context of the same study, Lee et al. (5) devised a new outcome measure, the LLD
Questionnaire, with an increased focus on psychological aspects. They administered the LLD
Questionnaire to the same parent group. This outcome measure consists of 34 items generated
through literature review, a semi-structured interview with parents of children with LLDs (no
indication of sample size is provided) who were asked “What are your concerns regarding LLD
of your child?” Item consensus was achieved through a panel discussion involving three
paediatric orthopaedic surgeons, 1 orthopaedic resident, 1 nurse, and 2 research assistants. Items
are organized into six domains: parent’s satisfaction, effect of LLD, preferred treatment, parent’s
mood, concern, and expectation with regard to the treatment, and are answered using a 5-point
Likert scale. Retrospectively Lee noted, “some issues could have been addressed more
accurately by putting them directly to the patients.” The study publication indicated that the
questionnaire was available as supplementary digital content however the provided link is not
currently accessible. No further psychometric testing of this questionnaire has been published.
There are many instances in which researchers have used a non-validated outcome measure or
questionnaire they created specifically for their study with children with LLAs. Ramaker (7)
developed a study-specific questionnaire to look at the social function of children after Ilizarov
leg lengthening. This questionnaire, a separate child and parent report, contained items
regarding current function at school, activities of daily living, physical and social activities, and
treatment related experiences, rated using a 5-point Likert scale. The number of items and the
item details were not described, nor are they available. Similarly, no psychometric evaluation of

17
this questionnaire has been reported.
McCarthy (8) compared function after amputation and lengthening in children with fibular
hemimelia in a 3-item measure that evaluated activity using a 4-point Likert scale (0=no
restrictions, 1-mild restrictions with strenuous activity, 2=limitation of activity, 3= severe
limitation of activity), pain using a 5-point scale (0=no pain, 1= any pain, even after strenuous
activity, 2= mild pain, 3= moderate pain, 4= severe pain), and satisfaction on a 2-point scale
(yes/no). Das (80) later used the activity item in this measure to evaluate “total lower limb
function” in children with bilateral fibular hemimelia that had undergone angular correction. No
psychometric testing of this questionnaire has been published.
Paley et al (9) devised a functional outcome scoring system to evaluate the outcome of femoral
lengthening. The scoring details were published in the original article and are easily
reproducible. Referred to as the Paley functional criteria, clinical and radiographic criteria
(clinician measures) are used (i.e., ROM of the knee, gait, mLDFA, and amount of lengthening)
in combination with patient report (i.e., pain and ability to perform activities of daily living
(ADLs) or work). Gait was evaluated on clinical examination and rated as no limp, slight limp,
or moderate limp. Patients rated their pain as none, slight, moderate, or severe and their
participation in activities/work as full, reduced, or none. There is no published evaluation of the
psychometric properties of this scoring system. Despite this, several other researchers have used
the measure (81, 82). There is concern that using unpublished measures creates bias, illustrated
by Marshall (83) who showed in schizophrenia randomized control trials, authors were more
likely to report superior treatment results versus control when using an unpublished versus
published measure, a finding most pronounced in non-pharmacological studies.
In summary, existing PRO measures of function are limited in their discriminative ability and
ability to detect change with intervention when used with children having LLAs. Consequently,
these measures are infrequently used in LLA-related outcomes research, thus our knowledge of
outcomes at the level of activities and participation is limited in this population. The Gait
Outcomes Assessment List (GOAL) (described in 4.1) is a recently developed outcome measure
with the potential to overcome the limitations of existing PRO measures of function. The need
for a new standardized functional outcome measure for use with children with LLAs has been
identified by several researchers to improve the uniformity and comprehensiveness of patient

18
assessment, to ensure fair comparisons across intervention studies, and ultimately to provide
evidence for the assumed functional benefit of surgery (10-13). Moreover, an outcome measure
that identifies patient priorities and goals would facilitate treatment planning that addresses the
specific goals and expectations of each family. According to Varni (73) the hallmark of pediatric
comprehensive care is “multidimensional assessment leading to targeted interventions based on
patient perceived needs”.
19
Chapter 4 Gait Outcomes Assessment List (GOAL)
The GOAL is a child and parent report questionnaire that evaluates the functional aspects of gait
and mobility related activities and symptoms. The overall purpose of the original GOAL was to
evaluate the physical, psychological, and social gait-related function of ambulant children with
cerebral palsy (CP). It was designed for use with children aged 9 to 18 years and their parents.
The GOAL is a hybrid measure, combining the specificity of an individualized measure (to allow
identification of patient priorities for treatment) with the standardization of a fixed item
questionnaire. It is intended to be self-administered. The GOAL is grounded within the ICF
framework (84, 85), and was developed with a view to ultimately broadening its application to
any childhood condition that is associated with gait related problems.
4.1 Background and Rationale
The GOAL was first conceptualized as an outcome measure within the context of a randomized
control trial involving children with ambulatory CP, and was created because no existing
outcome measure fulfilled the study’s objective of evaluating function and children’s and
parents’ priorities for orthopaedic surgical intervention (84, 85).
As such, GOAL development proceeded from Narayanan’s (47) Priority Framework for
Outcome Assessment (Figure 2). At the centre of this framework is the health condition of
interest. Priorities are influenced by an individual’s concerns, desires, and expectations, as they
relate to this health condition. Goals are a reflection of one’s priorities and guide the decision-
making process related to interventions. The effectiveness of these interventions is evaluated by
outcome measures. For these outcome measures to be meaningful they must, in turn, reflect the
original goals. Moreover, the framework recognizes that multiple stakeholders are involved in
health care decision-making, and although their perspectives might overlap, they may not be
concordant.

20
Figure 2. Priority Framework for Outcomes Assessment (adapted from Narayanan, 2015)
The current version of the GOAL (3.1) consists of 50 items that assess seven domains: (A)
activities of daily living & independence, (B) gait function & mobility, (C)
pain/discomfort/fatigue, (D) physical activities/games & recreation, (E) gait appearance, (F) use
of braces and assistive devices, and (G) body image & self-esteem. Domains that examine self-
perceived ability (A, B, D, E) use a 7-point ordinal scale anchored from 0 = “extremely
difficult/impossible” to 6 = “no problem at all”. Domains that examine an individual’s feelings
(F, G) use a 5-point ordinal scale from 0 = “very unhappy” to 4 = “very happy”. Symptoms of
pain/discomfort or fatigue are rated for their frequency (C) from 0 to 5, with 0 = “every day” to 5
= “none of the time”. The questionnaire also collects information on the level of assistance
required (A), walking aid used (B), and pain intensity (C). The GOAL asks children to reflect on
their abilities and experiences in the past 4 weeks. Furthermore, the GOAL captures the
perceived importance (the priority) of improving the outcome of each of its 50 items as rated on
a 5-point ordinal scale from 0 = “not a goal” to 4 = “extremely important”. Figure 3 illustrates
the 7-point ordinal scale used in four GOAL domains that evaluate self-perceived ability.

21
Figure 3. Example Scale Used in GOAL Domains Evaluating Self-perceived Ability
Studies have shown that respondents have difficulty using scales with greater than seven
response options although the optimal number of response options is unclear (86). A greater
number of options may increase ability to measure change however if there is not a meaningful
difference between response options, the reliability of the questionnaire may be negatively
impacted. For example, while it may be ideal for the GOAL to use a consistent 7- point scale
throughout, it became problematic in its creation because of the diversity of the domains. Figure
4 illustrates the 5- point ordinal scale used in GOAL domains that examines an individual’s
feelings or emotions. The GOAL development team felt it would be difficult to convert this to a
7- point ordinal scale and maintain a meaningful difference between each option.
Figure 4. Example Scale Used in GOAL Domains Evaluating Emotions
Table 2 illustrates the categorization of items in the GOAL (84) compared to previously
identified standardized outcome measures used in pediatric LLA research (Table 1) applying the
ICF linkage rules. This shows that items in the GOAL cover the domains of the ICF framework
more broadly than any other functional outcome measure evaluated, and representation of
personal factors exceeds all other measures where most have no items pertaining to personal
factors. These same results were seen when items of the GOAL were compared to standardized
outcome measures frequently used with children with CP (84).

22
Table 2. Categorization of the Items in the GOAL and the Outcome Measures Identified in
Published Paediatric LLA-related Studies, using the ICF Framework
Measure Percentage of Concepts in Each Category
Body
Structures
Body
Functions
Activities and
Participation
Environmental
Factors
Personal
Factors
Not
Definable
GOAL1
5% 25% 43% 11% 16% 0%
CHQ2 0% 27% 55% 5% 0% 12%
FAQ1 0% 9% 91% 0% 0% 0%
ASK1
0% 5% 93% 2% 0% 0%
PODCI1
0% 15% 52% 22% 6% 5%
PedsQL 4.02
0% 33% 52% 11% 0% 4% Table 2 Legend:
1adapted from (84).
2(45)
As development of the GOAL is in progress at the time of writing this thesis, there are currently
no publications specific to it. However, elements of the developmental process, related to
children with CP, have been exhibited as poster presentations at various conferences (84, 85, 87),
and the developer (UN) and his research team have been a ready resource during completion of
this thesis. A detailed description of the development of the GOAL from inception to present
state is provided in Appendix 2. This process informed the methods and decisions taken in the
current thesis project that evaluates and progressively adapts the GOAL for use with children
with LLAs.
4.2 Application of the Gait Outcomes Assessment List to Children with Lower Limb Anomalies- Sensibility
The GOAL appears to have good potential as a comprehensive outcome measure for evaluating
physical and psychosocial gait-related function in children with LLAs, given the breadth of its
content, however, to date it has only been used for ambulant children with CP, and not all aspects
of its sensibility have been explored.
Sensibility refers to “an aggregate of properties that make up the common sense aspect of an
instrument, including face and content validity” (88). A framework for evaluating sensibility
was proposed by Feinstein (89), consisting of 21 principles grouped into seven domains: purpose

23
and framework, comprehensibility, replicability (clarity of instruction), suitability of the output
scale, face validity, content validity, and ease of usage. Sensibility assessments are increasingly
being applied in studies that evaluate the quality of a questionnaire. One of the first examples of
this evaluation is by Rowe and Oxman (88) who created a sensibility questionnaire based on the
tenets of Feinstein’s framework to assess an asthma quality of life measure. This has since been
adapted by others to assess, for example, the HIV Disability Questionnaire (HDQ) (90), and the
Evidence-Based Practice Confidence (EPIC) Scale (91). Moreover, the concept of sensibility is
embedded within several of the available frameworks that are available to guide the development
and subsequent evaluation of the methodological quality of standardized outcome measures such
as the Qualitative Assessment of Physical Activity Questionnaire (QAPAQ) checklist (88, 92),
the Consensus-based Standards for the selection of health status Measurement Instruments
(COSMIN), and the Scientific Review Criteria presented by the Medical Outcomes Trust and its
Scientific Advisory Committee (SAC) (93, 94).
Not all aspects of sensibility have been explored for the original GOAL for children with CP.
Face and content validity has been established using direct input from children with CP, their
parents, and HCPs from different disciplines who care for these children (Appendix 2).
However, aspects of comprehensibility, clarity of instructions, suitability of the output scale and
ease of usage have only been assessed by HCPs (87) but have not yet been formally assessed by
children or parents. Further, the results cannot be assumed to apply to populations other than
children with CP. Therefore, an assessment of the overall sensibility of the GOAL that is
modified for children with LLA (to be known as the GOAL-LLA) is essential prior to in-depth
psychometric evaluation. Feinstein considered this of fundamental importance, stating, “if it is
not sensible, it does not warrant all the subsequent effort used to demonstrate its [internal]
consistency, criterion, and construct validity”. Since the purpose and framework of the GOAL
has already been well established (described in 4.1), this thesis study focuses on the other six
domains of sensibility evaluation (i.e., face and content validity, comprehensibility and ease of
usage, clarity of instructions and suitability of the scale) from the perspective of key stakeholders
(i.e., children with LLAs, their parents, and HCPs who care for children with LLAs). Moreover,
the study design of this thesis project provides an ideal opportunity for the results of the
sensibility assessment to inform progressive content adaptation of the GOAL-LLA.

24
Directly capturing not only an adult (parent and HCP) perspective via GOAL-LLA feedback, but
the perspectives of these children, ages 9 years and up, is of particular interest for several
reasons. Children are beginning to participate in clinical and surgical decision-making at this
point in their development, so it is valuable to gain insight into the issues they feel are important
during this stage in their life (45, 73). Studies support this age group being capable of accurate
self-report (95). Additionally, this age range aligns well with the timing of several of the
surgical options available. Although EFT may be used at any age, it is often used in combination
with growth dependent interventions (i.e., epiphyseodesis and guided growth techniques) to
achieve lower limb symmetry by the onset of skeletal maturity. Although the exact timing of
these interventions is determined by the magnitude of discrepancy or malalignment, they are
most often performed within the last few years of a child’s predicted growth period, consistent
with the age range used in this study.

25
Chapter 5 Rationale and Study Objectives
5.1 Rationale
Given the need for a comprehensive functional outcome measure specifically for children with
LLA, the starting point for this study was the consideration of the use of the GOAL for these
children. Despite some commonality in the physical impairments that characterize CP and LLAs,
such as range of motion limitations, strength deficits, and altered gait biomechanics, the
experiences of these populations may be quite different with respect to physical function. This is
because individuals with CP may also have spasticity, upper extremity involvement, and
involuntary movements of the extremities that might further hinder function or affect it in
different ways. We also anticipated that if the GOAL was used among children with LLAs,
some of the original item content that made sense for use with children with CP might be too
easy (e.g., getting in and out of bed, standing at a sink or counter) (face and content validity
issues). Consequently, we did not expect every item of the GOAL would be considered an
important goal of treatment, meaning that some items might need to be eliminated or modified to
ensure that the questionnaire content is relevant and meaningful for outcome measurement with
children having LLAs.
Moreover, not all aspects of sensibility of the GOAL have been comprehensively explored
during its development for children with CP. We believed there was a possibility that the
language could be too advanced (comprehensibility), and the questionnaire length (ease of usage)
might be a deterrent to its adoption. Additionally, we felt it was important to ask children
themselves about the clarity of instruction and suitability of the GOAL items and response
options.
The use of cognitive interviews (96) in this evaluation process allows information to be collected
from children pertaining to each of the six domains of sensibility on which this study is focused
(i.e., face and content validity, comprehensibility, ease of usage, clarity of instruction, and
suitability of scale). Cognitive interviewing is considered a critical component of paediatric
outcome measure development (13, 96, 97). This approach evaluates children’s comprehension
of questionnaire items and instructions, and ensures that a questionnaire meets its intended
26
purpose (13). Cognitive interview methods, also referred to as cognitive pretesting (96),
cognitive testing (97), and cognitive debrief (98), evolved from social and cognitive psychology
(13) and are believed to compliment field-testing of questionnaires (96).
5.2 Purpose
Given the above considerations, the purpose of this study was to develop a GOAL module
suitable for children with a lower limb anomaly (GOAL-LLA) that could serve as an evaluative
measure of physical and psychosocial gait-related function. Development of the GOAL-LLA
would be accomplished through an iterative adaptation of the current GOAL 3.1, hereafter
referred to as the GOAL-CP (Appendix 3) given its original focus for use with children with CP.
5.2.1 Objectives
To create this new evaluative measure, the GOAL-LLA, the perspectives of children and their
parents, and healthcare professionals were considered in the research process that addressed the
primary objectives of this study:
Objective 1. Evaluate the suitability of the items of the GOAL-CP for use with children with
LLA (face and content validity), to inform the elimination, modification, or retention of each
item and addition of new items (content adaptations) for the GOAL-LLA.
Objective 2. Assess the sensibility of the GOAL-LLA, namely its comprehensibility, clarity of
instruction, suitability of the response scale, and ease of usage.
The secondary objectives of this study (using child and parent data) were to:
Objective 3. Compare the responses of children with LLAs with those of their parents, for the
GOAL-LLA item scores and importance ratings, to inform the future need for separate child- and
parent-report versions. It was hypothesized that while children’s responses would be positively
correlated with their parents’, children’s item scores would be higher than parents’ scores. This
is consistent with a previous study that compared PODCI and PedsQL scores between children
with congenital upper extremity deficiency and their parents, and showed parents tended to
underestimate their children’s physical and social function (99). Conversely, it was hypothesized
that children’s item importance ratings would be lower than their parents’ ratings, based on a
study by Narayanan that showed, in regard to adolescent idiopathic scoliosis, parents’ level of

27
concern and their number of serious concerns exceeded their children’s (100). A similar trend is
expected as both scoliosis and LLAs are childhood orthopaedic conditions that may be associated
with physical and psychosocial sequelae.
Objective 4. Assess the relationship between an individual’s item scores and their importance
ratings, for children with LLAs and parents separately, to assess the respondent’s interpretation
of the questionnaire’s instructions and rating system. It was hypothesized that high scoring items
would not be considered important to improve upon, hence there would be a negative correlation
between item scores and importance ratings for both children’s and parents’ scores.

28
Chapter 6 Methods
6.1 Study Design
The four objectives of this study were addressed over two phases, with the perspectives and
feedback of children with LLAs and their parents sought in Phase 1 (addressing objectives 1 to
4), while HCPs provided input in Phase 2 (addressing objectives 1 and 2).
Administering the questionnaire to children and parents and conducting cognitive interviews
with children informed the iterative adaptation of the GOAL module (initial version= GOAL-CP,
second version= GOAL-LLA 1.0, third version = GOAL-LLA 1.1) (Phase 1). The final iteration
of the questionnaire (GOAL-LLA 2.0) was guided by the analysis of the third administration of
the GOAL in Phase 1 (GOAL-LLA 1.1) in combination with data from an e-survey administered
to HCPs (Phase 2). The sequence of study events is illustrated in Figure 5.
Cognitive Interview
Children and Parents
Objectives 1,3,4
--------------------------------
Children
Objectives 1 & 2
GOAL-LLA 1.0
Questionnaire Administration
Cognitive Interview
Children and Parents
Objectives 1,3,4
--------------------------------
Children
Objectives 1 & 2
Questionnaire Administration
Questionnaire AdministrationChildren and Parents
Objectives 3 & 4
--------------------------------
Objectives 1 & 2
Healthcare Professionals
Objectives 1 & 2
GOAL-CP
GOAL-LLA 1.1
e-Survey
GOAL-LLA 2.0
PHASE 2
PHASE 1
Content Adaptation
Content Adaptation
Content Adaptation Content Adaptation
Figure 5. Illustration of Study Events
29
6.2 Child and Parent Perspectives (Phase 1)
6.1.1 Participants
Children from 9 to 18 years with a congenital, acquired, or developmental LLA (inclusive of
lower limb deformity, deficiency, and/or length discrepancy) were eligible to be in this study,
including children who had previous surgical intervention, as we believed they would provide a
unique perspective on the functional priorities that guide surgical decision-making. The lower
age for eligibility was established based on evidence that reading proficiency and cognitive
development affects the ability of those less than 8 years to accurately self-report (95).
Children were not eligible if they had cognitive impairments preventing comprehension of test
instructions or accurate self-report, an inability to read or write English, concurrent upper
extremity involvement, or neuromuscular co-morbidities or acute or systemic illness that may
influence physical function or day-to-day performance (e.g., CP, sarcoma, or juvenile arthritis).
Parents of eligible children were invited to participate in addition to, or independent of, their
child as their views are unique and should not be considered interchangeable (101). This reflects
a family-centred care view in which family members each have opportunity if they desire to
collectively guide healthcare decision-making.
6.1.2 Recruitment
Consecutive sampling over a period of seven months was used to recruit participants from the
Limb Reconstruction Program at a pediatric tertiary care hospital and the Prosthetic Clinic at a
pediatric rehabilitation hospital in the same city. The orthopaedic surgeon or physical therapy
(PT) practitioner in clinic informed prospective participants (child and parent) of their eligibility
for this study and, if they expressed interest to participate, they met with the study investigator
(JD) who described the study in detail, answered questions, and obtained written consent to
complete the GOAL questionnaire (Appendix 4). Additionally, children had the option to
consent to participate in a cognitive interview. A child’s capacity to consent was determined by
the investigator using parental input, in combination with guidelines developed for this study
(Appendix 5). This was in accordance with the study’s Research Ethics Board-approved
protocol (Appendices 6-8) for both this Phase and Phase 2 (below).

30
6.1.3 Data Collection
Demographic information pertaining to the child was collected from the child and their parent
using an Information Sheet (Appendix 9) created for this study. Specifically, the child’s gender,
age, diagnosis, and any previous surgery were recorded. The magnitude of their total lower limb
length discrepancy and the severity of deformity, based on the position of the mechanical axis
(55), were measured from their most recent full-length lower limb alignment radiograph. For
children currently undergoing EFT, values were obtained from the most recent radiograph prior
to the initiation of EFT. The investigator (JD) also tracked the gender of parents that
participated.
6.1.3.1 Questionnaire Administration (Objectives 1, 3, and 4)
The GOAL questionnaire was administered at the point of care. The consenting child and/or
parent completed the questionnaire simultaneously but independently in the same clinic room, in
the presence of the study investigator (JD) who was available to respond to, and keep detailed
notes of any questions that arose. The questionnaire instructed respondents to score each of its
items using 5-, 6-, and 7- point domain-specific ordinal scales (as described in 4.1), and rate its
importance using a 5- point ordinal scale (also described in 4.1). Our protocol varied slightly
from that of Narayanan et al. in that we did not use general importance ratings (Appendix 2) but
rather, respondents were instructed to consider how important a goal it was to improve for each
item. This is consistent with the GOAL-CP’s current use of itemized importance ratings. In the
event the child had an external fixator in situ, the child/parent was instructed to consider the
child’s pre-fixator status rather than use the time frame indicated in the questionnaire. Based on
our clinical experience, we believed that children undergoing EFT, particularly those in the
active lengthening phase, might have temporarily lower item scores consistent with their
impairments at the time. We wanted to capture feedback on which items are impacted by an
LLA, irrespective of EFT, and felt that inclusion of this specific cohort (who had recently made a
decision to undergo lengthy and intensive treatment) would provide valuable input as to what
items were most influential in their treatment decision-making process. The last page of the
questionnaire asked respondents to list items they felt were missing and should be added.

31
6.1.3.2 Cognitive Interviews (Objectives 1 and 2)
Children who also consented to participate in the cognitive interview did this with the same
researcher (JD) immediately after completing the questionnaire. A cognitive interview guide
(Appendix 10) was developed specifically based on the Cognitive Pretesting Model for Children
(96) (Appendix 11).
The child was asked to refer to their completed copy of the GOAL as they answered the
questions and probes outlined in the cognitive interview guide that were read to them by the
researcher. ‘Think aloud interviewing’ and ‘probing’ are the two main techniques employed in
cognitive interviewing (13). Think aloud interviewing is performed concurrent to questionnaire
completion with the respondent being encouraged to talk through their thought process as they
answer each question. The probing technique can be performed concurrently or retrospectively
with the interviewer asking questions to retrieve specific information from the respondent. Our
decision to use a probing technique immediately after the child had completed the questionnaire
was related to lower respondent burden and ease, as well as fear that using the alternative think
aloud method might affect the way children answered the questions (102).
Open-ended probes were used to test the child’s understanding of words, phrases, and concepts
in the GOAL that were deemed potentially problematic a priori by the development team (e.g.,
what do you think “symmetry” means?). Children were instructed to read the GOAL section
instructions and specific items aloud (e.g., can you read [item] #7 aloud?) and were then
prompted to rephrase in their own words (in your own words can you explain what is being asked
of you?). This method of probing helped to evaluate a child’s understanding of
instructions/questions and ensured that there was consistent interpretation among participants.
Children were also asked questions regarding: the scale format and response options, (did you
feel you were able to find your answer in the list of possible answers listed?), items that they felt
should be added (is there anything you would add to this section?) or eliminated (are there any
questions that you would get rid of completely from this questionnaire?), and their overall
impressions of the questionnaire (How do you feel about the amount of time it took you to
complete the GOAL?). Detailed notes were kept by JD from each child’s cognitive interview.

32
6.1.4 Analysis of Child and Parent Perspectives (Phase 1)
Preliminary analysis of the completed questionnaires in combination with the cognitive interview
responses and investigator notes was conducted during the recruitment phase on three occasions
approximately 8 weeks apart, a schedule that accommodated at least six clinic dates for the
study’s overall recruitment activities. The results of each analysis informed the iterative
refinement of the questionnaire that was subsequently piloted on the next group of respondents
(initial version= GOAL-CP, second version= GOAL-LLA 1.0, third version = GOAL-LLA 1.1).
The final iteration of the questionnaire (GOAL-LLA 2.0) was informed by the analysis of the
completed GOAL-LLA 1.1 questionnaires in combination with Phase 2 responses. All statistical
analyses for this Phase and Phase 2 objectives, were performed using R for Mac OS X (103).
6.1.4.1 Content Adaptation Analysis (Objective 1)
Descriptive statistics (mean, median, standard deviation [SD], range) were calculated separately
for children’s and parents’ item scores and importance ratings.
Mean item scores and importance ratings from children and parents were used to inform item
elimination and to highlight items that might need to be modified. Items were judged to perform
poorly, and would be considered for elimination, if both the child and parent mean item score
was within 0.5 of the maximum score (e.g., 5.5 to 6.0 out of 6.0) indicating these items would
have poor discriminate ability and be unresponsive to change, and if both the child and parent
mean importance rating was less than 0.5 out of 4.0 indicating these items were not a priority for
improvement in this population. We were cautious in the elimination of items, particularly with
the initial questionnaire administration so poorly performing items were examined in
combination with cognitive interview results to assess for opportunities to modify, rather than
eliminate. If the research team felt an item might perform better if it were modified, the item
would be altered and incorporated into the next iteration of the questionnaire for subsequent
piloting.
New items suggested by children and parents on the last page of the questionnaire or ideas
generated from cognitive interviews were considered by the research team (JD and UN) in terms
of redundancy and fit within the measurement concept. If deemed appropriate, these items were
incorporated as described above.

33
The results of the third administration of the GOAL (GOAL-LLA 1.1) were considered in Phase
2 in combination with HCP feedback, to inform the final iteration of the questionnaire (GOAL-
LLA 2.0).
6.1.4.2 Sensibility Evaluation (Objective 2)
Children’s detailed responses from the cognitive interviews were collated into a single document,
allowing general themes to be easily identified. The format of the cognitive interview guide
allowed issues to be easily categorized by four aspects of sensibility: comprehensibility (of
words and/or concepts), clarity of instructions, suitability of the response scale, and ease of
usage. The results of the sensibility assessment were used to further inform content adaptation in
each of these areas. All ideas and related changes to the GOAL-LLA were tracked to provide a
clear audit trail.
6.1.4.3 Child versus Parent Responses Analysis (Objective 3)
We aimed to compare and describe the relationship of the total item scores and importance rating
scores, between children with LLAs and their parents, using paired sample t-tests and Pearson’s
correlation coefficient respectively. The total score was calculated as a percentage of the total
possible score, taking into account missing items. These analyses were performed on data
obtained across all versions of the questionnaire (initial version= GOAL-CP, second version=
GOAL-LLA 1.0, third version = GOAL-LLA 1.1) as, despite iterative adaptation of the
questionnaire, we expected the underlying constructs to remain stable. Moreover, this
maximized the sample size. Statistical significance was determined by an alpha-level greater
than 0.05.
6.1.4.4 Item Scores versus Importance Ratings Analysis (Objective 4)
The relationship between an individual’s total item score and importance rating score, for
children and parents, was assessed using Pearson’s correlation coefficient. For the same reason
as stated above, analysis was performed on data obtained across all versions of the questionnaire
(initial version= GOAL-CP, second version= GOAL-LLA 1.0, third version = GOAL-LLA 1.1).
Likewise, statistical significance was determined by an alpha-level greater than 0.05.

34
6.1.5 Child and Parent Sample Size
The sample size target was set at 25 children and 25 parents (could be a child-parent dyad, or a
single child or parent). This was based on the number of participants in the initial development
of the GOAL-CP (n= 22 children) (85). However, the extended plan was that recruitment could
continue until informational saturation was achieved, (i.e., the point that the development team
[JD and UN] felt no new suggestions related to content adaptation, or novel input pertaining to
sensibility), were forthcoming. The required number of subjects estimated for the cognitive
debrief was 10 children based on similar studies that have used this process during the
development phase of a pediatric self-report measure (41, 104).
To broaden the sample of questionnaire respondents, a surgical caseload review was conducted
(by JD and UN) five months into the recruitment period. Children identified as eligible but not
having a scheduled clinic appointment within the remaining recruitment period, were mailed an
information letter, child and parent consent forms, and the questionnaire (child and parent
version), with a self-addressed return envelope. Families choosing to participate completed the
questionnaire at home and mailed it back. Children in this sample were not eligible for the
cognitive interview as this needed to be conducted in-person.
6.2 Health Care Professional Perspectives (Phase 2)
6.2.1 Participants
Orthopaedic surgeons, PTs, Nurse Practitioners, and PT Practitioners that have experience
working with children with LLAs were eligible for inclusion in this study. It was thought that
the inclusion of HCPs would enhance face and content validity by providing a cross-check, as
their broad clinical experience and knowledge of natural history might help to identify issues not
considered by families (105). Finally, HCP participation in the development stage might
increase the likelihood of their future utilization of this measurement outcome.
6.2.2 Sampling Recruitment
The international multi-disciplinary group of content expert HCPs was identified through their
local affiliation with our institutions or the membership lists of the Limb Lengthening and
Reconstruction Society (LLRS) and the British Limb Reconstruction Society (BLRS). Identified

35
HCPs received an electronic copy of the GOAL-LLA 1.1 (the resulting questionnaire from Phase
1), and an introductory letter (Appendix 12) including a link to an online survey. The letter
clearly stated that completing the survey implied consent to participate.
6.2.3 Data Collection
Prior to completing the e-survey, HCPs provided demographic information concerning their
occupation (orthopaedic surgeon, physical therapist, orthotist/prosthetist, or other) and years of
experience working with children with LLAs (< 5years, 5-<10 years, 10-<15 years, > 15 years).
6.2.3.1 e-Survey Questionnaire (Objective 1 and 2)
Consistent with the methodology employed in the development of the GOAL-CP, HCPs were
invited to review the GOAL-LLA 1.1 and complete the study e-survey that asked them, for each
item in the questionnaire: to accept; accept with modification and state the modification, or reject
and provide rationale for rejection. Additionally, HCPs were invited to list any other items they
felt should be included in the GOAL-LLA. Four questions were added at the end of the survey
to obtain further feedback on the GOAL-LLA 1.1 (i.e., what do you consider to be the strengths
of the GOAL-LLA, what do you consider to be the weaknesses of the GOAL-LLA, would you
consider use of the GOAL-LLA in your clinical practice, yes/no (please explain), would you
consider using the GOAL-LLA for research purposes, yes/no (please explain)). Their responses
provided additional insight into the sensibility of the questionnaire.
6.2.4 Analysis of Healthcare Professional Perspectives
6.2.4.1 Content Adaptation Analysis (Objective 1)
The frequency of HCP responses (Accept, Accept with Modification, and Reject) for the items in
GOAL-LLA 1.1 were collated for each item and percentages calculated. Items that received
greater than 3 out of 31 reject responses (> 10%) were considered for elimination. Conversely,
items that received at least 28 out of 31 accept responses (90%) were retained in the final version
of the GOAL (GOAL-LLA 2.0). Similar to the process in Phase 1, modification and new item
suggestions put forth in the HCP survey were considered by the development team (JD and UN)
in terms of redundancy and fit within the measurement concept and, if deemed acceptable, were
incorporated. If the development team felt uncertain about the fate of an item, they consulted the

36
results of the third administration of the GOAL (GOAL-LLA 1.1) to children and parents, to
obtain further feedback on the item’s performance.
6.2.4.2 Sensibility Evaluation (Objective 2)
HCP e-survey responses provided input on two domains of sensibility, specifically
comprehensibility and ease of usage.
6.2.4.2.1 Comprehensibility
The development team reviewed each of the suggested modifications and rejection rationales and
identified any comments that related to the comprehension of the GOAL. If the development
team believed that a suggestion would add clarity to the instructions or an item concept, improve
understanding of a word, increase its international applicability, and was consistent with the
original intent of the item, the modification was incorporated into the final version of the GOAL
(GOAL-LLA 2.0). In this way, the sensibility assessment informed content adaptation.
6.2.4.2.2 Ease of Usage
Responses to the open-ended questions regarding the strengths and weakness of the
questionnaire were collated and reviewed for common themes, including themes related to ease
of usage. The number of similar responses were summed and calculated as a percentage. The
frequency of HCP responses related to the amount of time it took to administer the GOAL
(appropriate/too long) and to their considered use of the GOAL in the future (yes/no) were
collated by question and percentages calculated.
6.2.5 Healthcare Professional Sample Size
A response rate of 30-35%, although low, was considered realistic based on the response
achieved by Narayanan and colleagues when they employed a similar protocol with CP-related
HCPs in the development of the original GOAL-CP (E. Ho, personal communication, June 26,
2013). We aimed to have at least 30-35 HCPs in our sample (of varying levels of experience,
different professional backgrounds, and with international representation), so we ensured that at
least 100 HCPs received an invitation to participate.

37
Chapter 7 Results
7.1 Child and Parent Perspectives (Phase One)
7.1.1 Participants
Forty-five participants were enrolled in Phase 1. These included 25 children (14 girls) with a
mean age of 13.7 years (range, 9.0 to 17.9), and 20 parents (16 mothers). There were 20 child-
parent pairs. Sixteen children had a congenital LLA, 5 acquired, and 4 developmental. Total
lower limb length discrepancies ranged from zero to 100 mm, and deformity ranged from none to
greater than 15 degrees malalignment. Table 3 summarizes all Phase 1 participants by the
questionnaire version they were administered (initial version= GOAL-CP, second version=
GOAL-LLA 1.0, third version = GOAL-LLA 1.1). Two child-parent dyads completed the
questionnaire (GOAL-LLA 1.1) at home, with all other questionnaires completed at the point of
care. Table 4 catalogues the demographics of the child participants. Thirteen children
participated in the cognitive interviews (8 with the GOAL-CP and 5 with the GOAL-LLA 1.0).
The development team judged informational saturation had been achieved related to new item
suggestions from questionnaire administration and cognitive interviews.
Table 3. Phase 1 Participants by Questionnaire Version Administered
Children
Parents
Questionnaire
Administered
GOAL
Completion
(n)
Mean age (SD)
Range
Cognitive
Debrief*
(n)
Mean age (SD)
Range
GOAL
Completion
(n)***
GOAL-CP 12
(7 girls/5 boys)
14.8 (2.3)
12-17
8
(5 girls/3 boys)
15.7 (2.6)
13-17
11
(9 mothers)
GOAL-LLA 1.0 5
(3 girls/2 boys)
11.8 (2.6)
9-16
5
(2 girls/3 boys)
13.2 (2.7)
10-16
3
(2 mothers)
GOAL-LLA 1.1 7
(4 girls/3 boys)
13.4 (2.4)
9-17
n/a n/a 6
(5 mothers)
Total 24**
(14 girls/10 boys)
13.7 (2.6)
9-17
13
(7 girls/6 boys)
14.6 (2.5)
10-17
20
(16 mothers) Table 3 Legend:
*Cognitive debrief sample is a subsample of the children who did the questionnaire
**Total study enrollment was 25 children. One child opted not to complete the questionnaire (GOAL-LLA 1.0) but
did participate in a cognitive debrief interview ***
Each parent completed a child-parent dyad
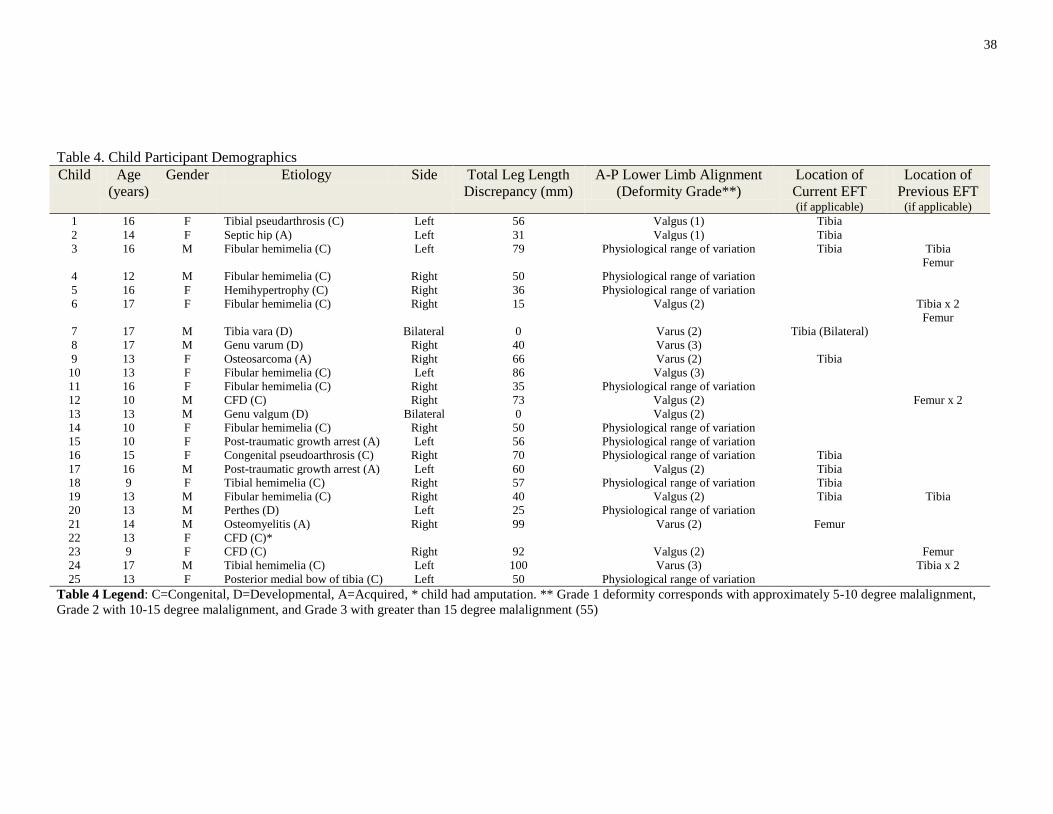
38
Table 4. Child Participant Demographics
Child Age
(years)
Gender Etiology Side Total Leg Length
Discrepancy (mm)
A-P Lower Limb Alignment
(Deformity Grade**)
Location of
Current EFT (if applicable)
Location of
Previous EFT (if applicable)
1 16 F Tibial pseudarthrosis (C) Left 56 Valgus (1) Tibia
2 14 F Septic hip (A) Left 31 Valgus (1) Tibia
3
16
M
Fibular hemimelia (C)
Left 79
Physiological range of variation
Tibia
Tibia
Femur
4 12 M Fibular hemimelia (C) Right 50 Physiological range of variation
5 16 F Hemihypertrophy (C) Right 36 Physiological range of variation
6
17
F
Fibular hemimelia (C)
Right 15
Valgus (2)
Tibia x 2
Femur
7 17 M Tibia vara (D) Bilateral 0 Varus (2) Tibia (Bilateral)
8 17 M Genu varum (D) Right 40 Varus (3)
9 13 F Osteosarcoma (A) Right 66 Varus (2) Tibia
10 13 F Fibular hemimelia (C) Left 86 Valgus (3)
11 16 F Fibular hemimelia (C) Right 35 Physiological range of variation
12 10 M CFD (C) Right 73 Valgus (2) Femur x 2
13 13 M Genu valgum (D) Bilateral 0 Valgus (2)
14 10 F Fibular hemimelia (C) Right 50 Physiological range of variation
15 10 F Post-traumatic growth arrest (A) Left 56 Physiological range of variation
16 15 F Congenital pseudoarthrosis (C) Right 70 Physiological range of variation Tibia
17 16 M Post-traumatic growth arrest (A) Left 60 Valgus (2) Tibia
18 9 F Tibial hemimelia (C) Right 57 Physiological range of variation Tibia
19 13 M Fibular hemimelia (C) Right 40 Valgus (2) Tibia Tibia
20 13 M Perthes (D) Left 25 Physiological range of variation
21 14 M Osteomyelitis (A) Right 99 Varus (2) Femur
22 13 F CFD (C)*
23 9 F CFD (C) Right 92 Valgus (2) Femur
24 17 M Tibial hemimelia (C) Left 100 Varus (3) Tibia x 2
25 13 F Posterior medial bow of tibia (C) Left 50 Physiological range of variation
Table 4 Legend: C=Congenital, D=Developmental, A=Acquired, * child had amputation. ** Grade 1 deformity corresponds with approximately 5-10 degree malalignment,
Grade 2 with 10-15 degree malalignment, and Grade 3 with greater than 15 degree malalignment (55)

39
7.1.2 Content Adaptation (Objective 1)
The first objective of this project was to evaluate the suitability of the items of the GOAL-CP for
use with children with LLA. The results of the questionnaire administration to children and their
parents were combined with findings and recommendations arising from the cognitive interviews
of children. These informed the iterative adaptation of the questionnaire [initial version= GOAL-
CP, second version= GOAL-LLA 1.0 (Appendix 13), third version= GOAL-LLA 1.1 (Appendix
14)], summarized in Table 5.
Table 5. Summary of Content Adaptation from the Initial to Third Iteration of the GOAL
GOAL-CP GOAL-LLA 1.0 GOAL-LLA 1.1 A) Activities of Daily Living &
Independence
Getting in and out of bed Retained Eliminated
Getting in and out of a chair or wheelchair Retained Eliminated
Standing at a sink or counter Retained Eliminated
Showering or bathing Retained Eliminated
Using the toilet Eliminated
Getting dressed Modified: Putting your pants on one leg
at a time
Eliminated
Carrying an object while walking (e.g.,
toy, doll, book, cell-phone
Modified: Carrying heavy objects while
walking (e.g., grocery bags, several
school books)
Retained
Modified: Balancing objects while
walking (e.g., a cup of hot chocolate, a
tray of food)
Retained
Opening a door manually Modified: Opening a door Retained
Picking up an object off the floor Retained Retained
Getting in and out of a vehicle (e.g.,
unmodified car, van, or bus)
Modified: Getting in and out of a vehicle
(e.g., car, van or bus) Retained
B) Gait Function & Mobility
Walking for more than 250 m (around 2
blocks or 2 football fields) Retained Retained
Getting around at school (indoors) Retained Retained
Added: Getting around in crowded
spaces (concert, special event, mall) Retained
Getting around at home Eliminated
Added: Standing in long lineups Retained
Walking for more than 15 minutes Retained Eliminated
Walking faster than usual to keep up with
others
Modified: Moving quickly if I am in a
hurry (e.g., to catch a bus, late for school)
Modified: Moving quickly when
in a hurry (e.g., to catch a bus,
late for an event)
Modified: Keeping up with my friends
while walking outdoors
Modified: Keeping up with my
friends
Stepping around or avoiding obstacles Retained Retained
Going up and down stairs Retained Retained
Going up and down slopes Retained Retained
Walking on uneven ground (rough, rocky,
sandy) Retained Retained
Walking on slippery or icy surfaces
Retained Retained
C) Pain/Discomfort/Fatigue
Pain or discomfort in the feet or ankles Retained Retained

40
Pain or discomfort in the lower legs Eliminated
Pain or discomfort in the knees Retained Retained
Pain or discomfort in the thighs or hips Retained Retained
Pain or discomfort in the back Retained Retained
Feeling tired while walking Retained Retained
Feeling tired during any other physical
activities that I usually enjoy (e.g.,
swimming, running, horseback riding, or
other)
Retained Retained
D) Physical Activities, Games, &
Recreation
Using playground equipment (ladders,
monkey bars, slides, etc.)
Modified: Climbing (e.g., ladder or
stepstool) Retained
Running Retained Modified: Running fast
Participating in gliding sports (e.g.,
skating, rollerblading, skiing,
skate/snowboarding)
Retained Retained
Riding a bike or tricycle (with or without
training wheels)
Retained Retained
Swimming Retained Retained
Participating in sports that require running
(e.g., soccer, baseball, football, track) Retained Retained
Participating in sports that require jumping
(e.g., basketball, volleyball) Retained Retained
Participating in dance or martial arts (e.g.,
karate, judo, taekwondo) Retained Modified: Participating in
gymnastics, dance or martial arts
(e.g., karate, judo, taekwondo)
E) Gait Appearance
Walking with my feet flat on the ground Retained Retained
Walking taller or more upright (less
crouched or bent at the knees) Retained Retained
Walking with my feet pointing straight
ahead Retained Retained
Added: Walking without a limp
Walking without dragging my feet Retained Eliminated
Walking without tripping and falling Retained Retained
Wearing my choice of footwear (e.g.,
shoes, boots, sandals)
Modified: Moved from E) to G) Retained
F) Use of Braces and Assistive Devices
Wearing braces or orthotics (e.g., AFO) Modified: Wearing braces or orthotics
(e.g., AFO, shoe lift)
Modified: A shoe lift
Modified: A brace (e.g., AFO)
Using a walking aide (e.g., walker, stick,
cane, crutches) Retained Retained
Using a wheelchair Eliminated Re-added
Added: Other assistive devices
(e.g., built-up bicycle pedal
or________)
G) Body Image & Self-Esteem
The shape and position of my legs Retained Retained
The shape and position of my feet Retained Retained
The symmetry of my legs (in length and
size) Retained Retained
Added: Wearing my choice of clothing
(e.g., shorts, skirts, bathing suits) Retained
The appearance of how I get around
compared with others Retained Retained
The way others feel about how I get
around Retained Retained
How I am treated by others Retained Retained
The descriptive statistics (mean, SD, range) for children’s and parents’ item scores and
importance ratings for the initial and second administration of the questionnaire are presented in
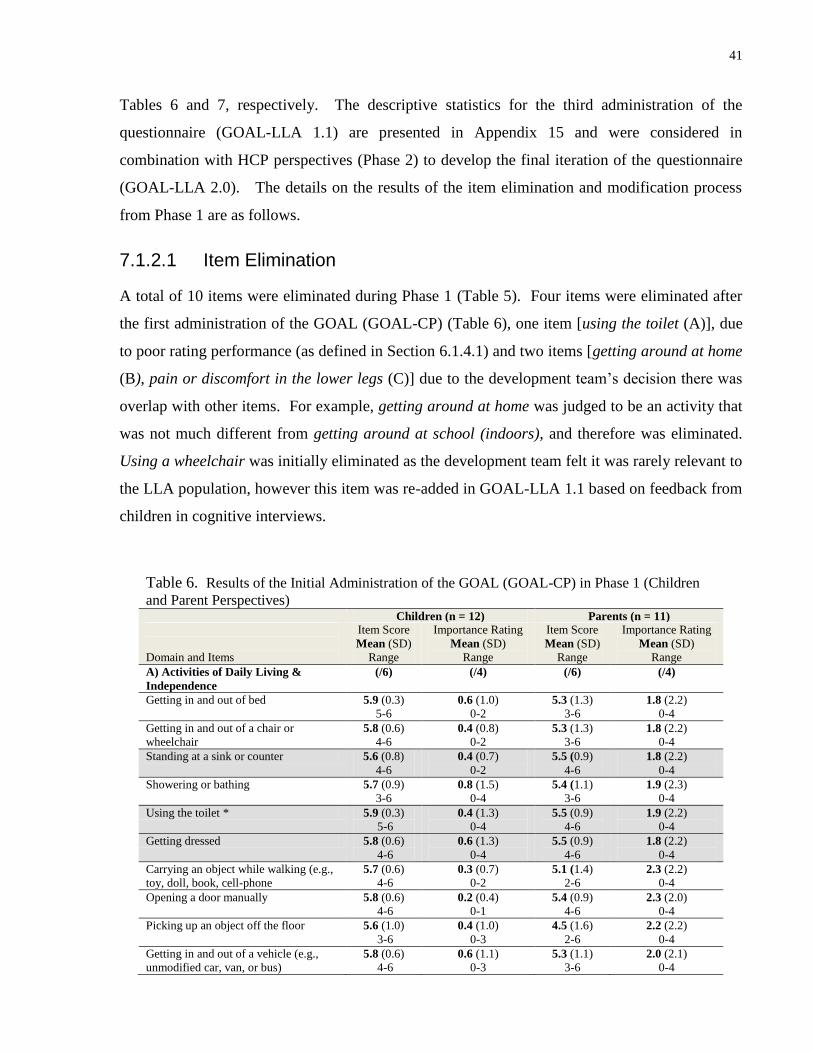
41
Tables 6 and 7, respectively. The descriptive statistics for the third administration of the
questionnaire (GOAL-LLA 1.1) are presented in Appendix 15 and were considered in
combination with HCP perspectives (Phase 2) to develop the final iteration of the questionnaire
(GOAL-LLA 2.0). The details on the results of the item elimination and modification process
from Phase 1 are as follows.
7.1.2.1 Item Elimination
A total of 10 items were eliminated during Phase 1 (Table 5). Four items were eliminated after
the first administration of the GOAL (GOAL-CP) (Table 6), one item [using the toilet (A)], due
to poor rating performance (as defined in Section 6.1.4.1) and two items [getting around at home
(B), pain or discomfort in the lower legs (C)] due to the development team’s decision there was
overlap with other items. For example, getting around at home was judged to be an activity that
was not much different from getting around at school (indoors), and therefore was eliminated.
Using a wheelchair was initially eliminated as the development team felt it was rarely relevant to
the LLA population, however this item was re-added in GOAL-LLA 1.1 based on feedback from
children in cognitive interviews.
Table 6. Results of the Initial Administration of the GOAL (GOAL-CP) in Phase 1 (Children
and Parent Perspectives)
Children (n = 12) Parents (n = 11)
Domain and Items
Item Score
Mean (SD)
Range
Importance Rating
Mean (SD)
Range
Item Score
Mean (SD)
Range
Importance Rating
Mean (SD)
Range
A) Activities of Daily Living &
Independence
(/6) (/4) (/6) (/4)
Getting in and out of bed 5.9 (0.3)
5-6
0.6 (1.0)
0-2
5.3 (1.3)
3-6
1.8 (2.2)
0-4
Getting in and out of a chair or
wheelchair
5.8 (0.6)
4-6
0.4 (0.8)
0-2
5.3 (1.3)
3-6
1.8 (2.2)
0-4
Standing at a sink or counter 5.6 (0.8)
4-6
0.4 (0.7)
0-2
5.5 (0.9)
4-6
1.8 (2.2)
0-4
Showering or bathing 5.7 (0.9)
3-6
0.8 (1.5)
0-4
5.4 (1.1)
3-6
1.9 (2.3)
0-4
Using the toilet * 5.9 (0.3)
5-6
0.4 (1.3)
0-4
5.5 (0.9)
4-6
1.9 (2.2)
0-4
Getting dressed 5.8 (0.6)
4-6
0.6 (1.3)
0-4
5.5 (0.9)
4-6
1.8 (2.2)
0-4
Carrying an object while walking (e.g.,
toy, doll, book, cell-phone
5.7 (0.6)
4-6
0.3 (0.7)
0-2
5.1 (1.4)
2-6
2.3 (2.2)
0-4
Opening a door manually 5.8 (0.6)
4-6
0.2 (0.4)
0-1
5.4 (0.9)
4-6
2.3 (2.0)
0-4
Picking up an object off the floor 5.6 (1.0)
3-6
0.4 (1.0)
0-3
4.5 (1.6)
2-6
2.2 (2.2)
0-4
Getting in and out of a vehicle (e.g.,
unmodified car, van, or bus)
5.8 (0.6)
4-6
0.6 (1.1)
0-3
5.3 (1.1)
3-6
2.0 (2.1)
0-4

42
B) Gait Function & Mobility (/6) (/4) (/6) (/4)
Walking for more than 250 m (around 2
blocks or 2 football fields)
4.6 (1.7)
1-6
0.7 (1.3)
0-3
3.5 (1.8)
1-6
2.7 (1.8)
0-4
Getting around at school (indoors) 5.5 (1.0)
3-6
0.2 (0.6)
0-2
5.0 (1.1)
3-6
1.7 (2.1)
0-4
Getting around at home * 5.7 (0.8)
4-6
0.2 (0.6)
0-2
5.3 (0.9)
4-6
1.7 (2.1)
0-4
Walking for more than 15 minutes 4.7 (1.5)
1-6
0.7 (1.1)
0-3
3.7 (2.2)
1-6
2.7 (1.8)
0-4
Walking faster than usual to keep up
with others
4.5 (1.5)
2-6
1.1 (1.3)
0-3
3.4 (1.7)
0-6
2.4 (1.8)
0-4
Stepping around or avoiding obstacles 5.4 (1.0)
3-6
0.2 (0.6)
0-2
4.7 (1.1)
3-6
2.2 (1.9)
0-4
Going up and down stairs 5.4 (1.2)
2-6
0.3 (0.9)
0-3
4.6 (1.4)
3-6
2.1 (2.0)
0-4
Going up and down slopes 4.3 (1.4)
2-6
0.7 (1.1)
0-3
3.4 (1.5)
1-6
2.0 (1.9)
0-4
Walking on uneven ground (rough,
rocky, sandy)
4.0 (1.8)
2-6
1.1 (1.6)
0-4
3.7 (1.4)
2-6
2.4 (1.7)
0-4
Walking on slippery or icy surfaces
4.0 (2.0)
0-6
1.0 (1.6)
0-4
3.4 (1.6)
1-6
2.9 (2.0)
0-4
C) Pain/Discomfort/Fatigue (/5) (/4) (/5) (/4)
Pain or discomfort in the feet or ankles 3.9 (1.1)
2-5
1.8 (1.3)
0-4
4.1 (0.9)
2-5
1.7 (1.7)
0-4
Pain or discomfort in the lower legs * 4.1 (0.9)
2-5
1.7 (1.6)
0-4
3.7 (0.8)
2-5
2.9 (0.9)
2-4
Pain or discomfort in the knees 3.9 (1.2)
2-5
1.8 (1.6)
0-4
4.0 (0.8)
3-5
1.7 (1.5)
0-4
Pain or discomfort in the thighs or hips 4.2 (1.3)
1-5
1.3 (1.8)
0-4
4.1 (1.2)
2-5
2.0 (1.8)
0-4
Pain or discomfort in the back 4.4 (0.9)
2-5
0.9 (1.5)
0-4
4.3 (1.2)
1-5
2.2 (1.5)
0-4
Feeling tired while walking 4.2 (0.9)
2-5
0.9 (1.4)
0-4
3.5 (1.0)
2-5
2.7 (1.2)
0-4
Feeling tired during any other physical
activities that I usually enjoy (e.g.,
swimming, running, horseback riding,
or other)
3.8 (0.7)
2-5
1.8 (1.6)
0-4
3.2 (1.7)
0-5
2.7 (1.5)
0-4
D) Physical Activities, Games, &
Recreation
(/6) (/4) (/6) (/4)
Using playground equipment (ladders,
monkey bars, slides, etc.)
5.5 (0.9)
4-6
0.6 (1.1)
0-3
4.0 (1.3)
3-6
2.0 (0.9)
1-3
Running 3.8 (1.2)
2-6
2.0 (1.4)
0-4
3.2 (1.5)
1-6
2.5 (1.3)
0-4
Participating in gliding sports (e.g.,
skating, rollerblading, skiing,
skate/snowboarding)
3.4 (1.6)
0-5
1.4 (1.1)
0-3
2.7 (1.9)
0-6
1.4 (1.4)
0-4
Riding a bike or tricycle (with or
without training wheels)
5.5 (0.9)
4-6
0.6 (1.1)
0-3
4.9 (1.5)
2-6
2.1 (1.5)
0-4
Swimming 4.8 (1.5)
3-6
0.8 (1.2)
0-3
5.1 (1.6)
2-6
1.7 (1.4)
0-4
Participating in sports that require
running (e.g., soccer, baseball, football,
track)
4.2 (1.2)
3-6
1.4 (1.6)
0-4
3.7 (1.4)
2-6
2.0 (1.2)
0-4
Participating in sports that require
jumping (e.g., basketball, volleyball)
4.7 (1.1)
3-6
1.6 (1.7)
0-4
3.7 (1.5)
2-6
1.9 (1.3)
0-4
Participating in dance or martial arts
(e.g., karate, judo, taekwondo)
4.6 (1.1)
3-6
1.1 (1.7)
0-4
3.0 (1.5)
1-6
2.3 (1.1)
1-4
E) Gait Appearance (/6) (/4) (/6) (/4)
Walking with my feet flat on the
ground
4.2 (1.7)
2-6
0.6 (0.9)
0-2
3.2 (1.8)
0-5
2.2 (1.4)
0-4
Walking taller or more upright (less 3.8 (1.6) 1.3 (1.5) 3.7 (1.6) 2.7 (1.4)

43
crouched or bent at the knees) 1-6 0-4 1-6 0-4
Walking with my feet pointing straight
ahead
3.9 (1.8)
1-6
0.7 (1.3)
0-4
2.7 (1.7)
0-5
2.9 (1.5)
0-4
Walking without dragging my feet 4.8 (1.3)
3-6
0.6 (1.1)
0-3
3.8 (2.0)
0-6
1.8 (1.6)
0-4
Walking without tripping and falling 5.3 (0.9)
4-6
0.4 (0.9)
0-2
4.7 (1.3)
3-6
2.0 (1.7)
0-4
Wearing my choice of footwear (e.g.,
shoes, boots, sandals)
4.5 (2.2)
0-6
1.1 (1.8)
0-4
3.0 (1.9)
0-6
2.2 (1.8)
0-4
F) Use of Braces and Assistive
Devices
(/4) (/4) (/4) (/4)
Wearing braces or orthotics (e.g., AFO) 1.5 (1.6)
0-4
0.8 (1.3)
0-3
1.9 (1.4)
0-4
2.5 (1.8)
0-4
Using a walking aide (e.g., walker,
stick, cane, crutches)
1.8 (0.8)
1-3
0.8 (1.0)
0-2
1.8 (0.8)
1-2
2.3 (1.5)
1-4
Using a wheelchair * 2 (0.8)
1-3
1.0 (1.1)
0-2
2.0 (0.8)
1-3
1.5 (0.7)
1-2
G) Body Image & Self-Esteem (/4) (/4) (/4) (/4)
The shape and position of my legs 1.7 (1.3)
0-4
2.1 (1.4)
0-4
1.7 (1.1)
0-3
2.9 (1.5)
0-4
The shape and position of my feet 2.1 (1.3)
0-4
1.6 (1.6)
0-4
2.1 (1.0)
1-4
2.1 (1.6)
0-4
The symmetry of my legs (in length and
size)
1.7 (1.2)
0-4
2.1 (1.7)
0-4
1.7 (1.0)
0-3
2.9 (1.8)
0-4
The appearance of how I get around
compared with others
1.8 (1.1)
0-4
1.7 (1.5)
0-4
2.2 (1.5)
0-4
1.9 (1.8)
0-4
The way others feel about how I get
around
2.3 (1.3)
0-4
0.9 (1.5)
0-4
2.6 (1.0)
1-4
1.2 (1.7)
0-4
How I am treated by others 3.3 (0.9)
2-4
1.8 (1.8)
0-4
3.1 (0.9)
1-4
1.8 (2.1)
0-4
Table 6 Legend: The four items eliminated after the first administration of the questionnaire (GOAL-CP) are
marked with an asterisk. The three shaded items had poor rating performance (both the child and parent mean item
score was within 0.5 of the maximum score or both the child and parent mean importance rating was less than 0.5
out of 4.0). Despite poor rating performance, standing at a sink or counter was retained (as standing had been
highlighted in cognitive interviews as a problematic activity) and getting dressed was modified for the GOAL-LLA
1.0 to make the task more difficult (putting your pants on one leg at a time). Both were ultimately eliminated due to
continued poor rating performance.
A further seven items were eliminated after the second administration of the GOAL (GOAL-
LLA 1.0) (Table 5), of which six were due to poor item performance [getting in and out of bed
(A), getting in and out of a chair (or wheelchair) (A), standing at a sink or counter (A),
washing/bathing (A), putting your pants on one leg at a time while standing (A) and walking
without dragging my feet (E)] (Table 7). Walking for more than 15 minutes was eliminated
based on children having difficulty in the cognitive debrief distinguishing this item from walking
for more than 250 meters (around 2 blocks or 2 football fields). The latter was retained because
children were able conceptualize this item in the cognitive debrief (“from swimming”, “from
track and field”, “the example is good, it makes it clear”) and also reported lower mean item
scores (i.e., more difficult) for this activity.

44
Table 7. Results of the Second Administration of the GOAL (GOAL-LLA 1.0) in Phase 1 (Child and
Parent Perspectives) Children (n = 5) Parents (n=3)
Domain and Items
Item Score
Mean (SD)
Range
Importance Rating
Mean (SD)
Range
Item Score
Mean (SD)
range
Importance Rating
Mean (SD)
Range
A) Activities of Daily Living & Independence (/6) (/4) (/6) (/4)
Getting in and out of bed * 5.8 (0.5)
5-6 0
All 0 6.0
All 6 0
All 0
Getting in and out of a chair (or wheelchair) * 5.4 (0.9)
4-6 0
All 0 6.0
All 6 0
All 0
Standing at a sink or counter * 5.6 (0.9)
4-6 0
All 0 6.0
All 6 0
All 0
Washing/bathing myself (e.g., shower or tub) * 5.8 (1.1)
5-6 0
All 0 6.0
All 6 0
All 0
Putting your pants on one leg at a time while
standing *
5.6 (0.5)
5-6 0
All 0
5.7 (0.6)
5-6 0
All 0
Carrying heavy objects while walking (e.g.,
grocery bags, school books)
5.0 (1.1)
3-6
0.5 (1.0)
0-2 6.0
All 6
0 All 0
Balancing objects while walking (e.g. a cup of
hot chocolate, a tray of food)
5.2 (1.0)
4-6
0.8 (1.0)
0-2 6.0
All 6 0
All 0
Opening a door 5.8 (0.7)
5-6 0
All 0 6.0
All 6 0
All 0
Picking up an object off the floor 5.8 (1.1)
5-6 0
All 0 6.0
All 6 0
All 0
Getting in and out of a vehicle (e.g., car, van or
bus)
5.4 (0.9)
4-6 0
All 0 6.0
All 6 0
All 0
B) Gait Function & Mobility (/6) (/4) (/6) (/4)
Walking for more than 250 meters (around 2
blocks or 2 football fields)
4.6 (1.8)
3-6
1.0 (1.4)
0-3
5.3 (1.2)
4-6
1.5 (2.1)
0-3
Getting around at school (indoors) 5.8 (1.1)
5-6 0
All 0 6.0
All 6 0
All 0
Getting around in crowded spaces (e.g. a
concert or special event, the mall)
5.4 (0.9)
5-6 0
All 0 6.0
All 6 0
All 0
Standing in long lineups 4.8 (1.6)
3-6
0.3 (0.5)
0-1
5.7 (0.6)
5-6 0
All 0
Walking for more than 15 minutes 5.0 (1.6)
3-6
0.5 (1.0)
0-2
4.3 (1.5)
3-6
3.5 (0.7)
3-4
Keeping up with my friends while walking
outdoors
4.8 (1.6)
3-6
0.5 (1.0)
0-2
4.3 (2.1)
2-6
2.0 (2.8)
0-4
Moving quickly if I am in a hurry (e.g., to catch
a bus, late for school)
5.0 (1.6)
3-6
0.5 (1.0)
0-2
5.7 (0.6)
5-6 0
All 0
Stepping around or avoiding obstacles 5.2 (1.5)
4-6
0.3 (0.5)
0-1
5.7 (0.6)
5-6 0
All 0
Going up and down stairs 5.6 (1.4)
5-6 0
All 0
5.7 (0.6)
5-6 0
All 0
Going up and down slopes 5.0 (2.0)
4-6
0.3 (0.5)
0-1
5.7 (0.6)
5-6 0
All 0
Walking on uneven ground (rough, rocky,
sandy)
5.2 (1.5)
3-6 0
All 0
5.3 (0.6)
5-6
1.5 (2.1)
0-3
Walking on slippery surfaces (wet or icy) 4.6 (1.5)
3-6
0.3 (0.5)
0-1
5.3 (0.6)
5-6
1.5 (2.1)
0-3
C) Pain/Discomfort/Fatigue (/5) (/4) (/5) (/4)
Pain or discomfort in my feet or ankles 3.8 (1.3)
2-5
1.3 (1.3)
0-3
3.7 (1.2)
3-5
2.0 (2.8)
0-4
Pain or discomfort in my knees 4.4 (1.5)
3-5
0.6 (0.6)
0-1
4.3 (0.6)
4-5
3.5 (0.7)
3-4
Pain or discomfort in my thighs or hips 4.6 (1.1)
4-5
0.5 (0.5)
0-1
4.0 (1.0)
3-5
3.5 (0.7)
3-4
Pain or discomfort in my back 5.0 (1.1)
All 5 0
All 0
4.7 (0.6)
4-5
3.5 (0.7)
3-4
Feeling tired while walking 3.0 (2.0)
0-5
1.5 (1.9)
0-4
4.0 (1.7)
2-5
2.0 (2.8)
0-4

45
Feeling tired during any other physical
activities that I usually enjoy (e.g., swimming,
running, horseback riding or other sport)
3.4 (1.8)
1-5
1.8 (1.5)
0-3
4.0 (1.0)
3-5
3.5 (0.7)
3-4
D) Physical Activities, Games, & Recreation (/6) (/4) (/6) (/4)
Running 3.4 (1.8)
1-6
1.8 (1.3)
0-3
4.0 (1.7)
3-6
3.5 (0.7)
3-4
Participating in gliding sports (e.g., skating,
rollerblading, skiing, skate/snowboarding)
3.0 (1.7)
2-4
0.7 (0.6)
0-1
3.3 (2.3)
2-6
2.5 (0.7)
2-3
Riding a bicycle 4.5 (1.2)
3-6
0.7 (0.6)
0-1
4.0 (1.7)
3-6
3.5 (0.7)
3-4
Swimming 5.4 (1.2)
4-6
0.5 (1.0)
0-2
5.7 (0.6)
5-6
1.0 (1.4)
0-2
Participating in sports that require running (e.g.,
soccer, baseball, football, track)
4.5 (1.0)
4-5
0.3 (0.5)
0-1
3.3 (2.5)
1-6
2.5 (0.7)
2-3
Participating in sports that require jumping
(e.g., basketball, volleyball)
4.8 (1.5)
2-6
0.3 (0.5)
0-2
3.7 (2.1)
2-6
2.5 (0.7)
2-3
Participating in dance or martial arts (e.g.,
karate, judo, taekwondo)
4.8 (1.3)
3-6
1.3 (1.5)
0-3
4.0 (2.8)
2-6
2.0 (1.4)
1-3
Climbing (e.g., ladder or stepstool) 5.3 (1.7)
3-6 0
All 0
5.7 (0.6)
5-6 0
All 0
E) Gait Appearance (/6) (/4) (/6) (/4)
Walking with my feet flat on the ground 4.6 (2.2)
1-6
1.0 (2.0)
0-4
4.7 (1.2)
4-6
1.5 (2.1)
0-3
Walking taller or more upright (less crouched
or bent at the knees)
5.0 (2.3)
1-6
1.0 (2.0)
0-4
5.7 (0.6)
5-6 0
All 0
Walking with my feet pointing straight ahead 4.4 (1.8)
1-6
1.0 (2.0)
0-4
5.3 (1.2)
4-6
1.0 (1.4)
0-2
Walking without dragging my feet * 5.6 (1.8)
1-6
1.0 (2.0)
0-4 6.0
All 6 0
All 0
Walking without tripping and falling 5.0 (2.2)
3-6
0.5 (1.0)
0-2
5.7 (0.5)
5-6
2.0 (2.8)
0-4
Walking straight and level (less leaning to the
side)
4.2 (2.7)
0-6
1.0 (2.0)
0-4
5.0 (1.7)
3-6
1.5 (2.1)
0-3
F) Use of Braces and Assistive Devices (/4) (/4) (/4) (/4)
Wearing braces or orthotics (e.g., shoelift,
AFO)
2.5 (1.5)
0-4
1.7 (2.1)
0-4
3.3 (1.2)
2-4
1.5 (2.1)
0-3
Using a walking aide (e.g., walker, stick, cane,
crutches)
4.0 (1.3)
1-4
1.0 (0)
All 1.0
n/a n/a
G) Body Image & Self-Esteem (/4) (/4) (/4) (/4)
The shape and position of my legs 2.4 (1.6)
1-4
2.0 (2.3)
0-4
2.3 (2.1)
2-4 0
All 0
The shape and position of my feet 2.6 (1.7)
0-4
1.5 (1.9)
0-4
3.0 (1.0)
1-4
1.0 (1.4)
0-2
The symmetry of my legs (in length and size) 2.6 (1.4)
1-4
2.0 (1.6)
2-5
3.0 (1.0)
2-4
2.5 (0.7)
2-3
Wearing my choice of footwear (e.g., shoes,
boots, sandals)
3.2 (1.5)
2-4
0.8 (1.0)
0-2
3.3 (1.2)
2-4
1.0 (1.4)
0-2
Wearing my choice of clothing (e.g., shorts,
skirts, bathing suits)
2.2 (1.6)
0-4
2.0 (1.8)
0-4
3.0 (1.0)
2-4
1.0 (1.4)
0-2
The appearance of how I get around compared
with others
2.6 (1.6)
0-4
1.5 (1.9)
0-4
3.0 (1.0)
1-4
1.0 (1.4)
0-2
The way others feel about how I get around 2.8 (1.6)
0-4
1.3 (1.9)
0-4
3.3 (1.2)
2-4
1.0 (1.4)
0-2
How I am treated by others 3.0 (1.7)
0-4
1.3 (1.9)
0-4
3.3 (1.2)
2-4
1.0 (1.4)
0-2
Table 7 Legend: The five items eliminated after the second administration of the questionnaire (GOAL-LLA 1.0)
are marked with an asterisk. Shaded items had poor performance (both the child and parent mean item score was
within 0.5 of the maximum score or both the child and parent mean importance rating was less than 0.5 out of 4.0).
Of those items shaded but not eliminated, opening a door, picking up an object off the floor, and getting in and out
of a vehicle continued to perform poorly and were eliminated after the third administration of the questionnaire
(GOAL-LLA 1.1). Conversely, stepping around or avoiding obstacles, going up and down stairs, and pain or
discomfort in my back were retained in Phase 2 as there was no issue with their subsequent performance (Appendix

46
15). Getting around at school (indoors), getting around in crowded spaces, standing in long lineups, going up and
down slopes, and climbing were modified in Phase 2 (Table 9).
7.1.2.2 Item Modification and Retention
After the initial administration of the GOAL (GOAL-CP) all 10 items in domain A) Activities of
Daily Living & Independence, had very high mean item scores for children (greater than 5.5 out
of 6) (Table 6). In other words, children felt they could complete these activities with great ease.
However, the development team felt several of these items were of potential content value if they
were modified to increase their level of difficulty. For example, based on feedback from
children’s cognitive interviews, the item carrying objects while walking (e.g., toy, doll, book,
cellphone) (A) was adapted and made into two items, carrying heavy objects while walking (e.g.,
grocery bags, school books) and balancing objects while walking (e.g., a cup of hot chocolate, a
tray of food). Each of these items was retained through all subsequent iterations of the GOAL-
LLA.
Wearing my choice of footwear was initially in E) Gait Appearance which instructs the child to
“rate how much of a problem you experienced with… ”. The development team believed it was
more important to capture children’s feelings about their ability/inability to wear their preferred
footwear than about the perceived difficulty of using footwear itself. Thus, the item was moved
to domain G) Body Image & Self Esteem, piloted in the GOAL-LLA 1.0, and subsequently
retained in G) which instructs the child to “rate how you felt about… ”.
At the end of Phase 1, thirty of the 50 items in the GOAL-CP (60%) were retained within their
original domain and without modification (Table 5).
7.1.2.3 Item Addition
There were 5 new items added in Phase 1 based on children’s and parents’ suggestions [getting
around in crowded spaces (B), standing in long lineups (B), walking without a limp (E), use of
other assistive devices (e.g., built up bicycle pedal) (F), and wearing my choice of clothing (e.g.,
shorts, skirts, bathing, suits (G)] (Table 5). All of these were retained into Phase 2.

47
7.1.3 Sensibility Evaluation (Objective 2)
7.1.3.1 Comprehension
No participant asked for assistance or clarification in regard to language during questionnaire
administration. Overall, during cognitive interviews children demonstrated that they were able
to read and understand the words, phrases, and concepts in the questionnaire that the
development team had considered potentially problematic a priori. For example, during cognitive
interviews children were asked, “what does symmetry mean to you?” Their responses, (e.g.,
“comparable on both sides”, “split and have two equal parts”, “line down the middle”, “same
on both sides), assured us that symmetry is a word they know and a concept they understand.
Children did however, experience difficulty defining the word gait. Five of 13 children admitted
in cognitive interviews that they were not familiar with the word or were uncertain of its
meaning. Four other children thought they understood the word but provided a definition for
gate. The word has been retained as it is part of the formal title of the original questionnaire, but
the development team ensured that gait did not appear in any of the instructions or item content
of the GOAL.
7.1.3.2 Clarity of Instruction
Instructions with regard to importance ratings proved problematic in the initial administration of
the GOAL. The intended purpose of the importance ratings was to capture how important a goal
it was to improve each specific item, allowing us to identify the items that contribute most to
treatment priorities and related decision-making. Contrary to our intent, many respondents had a
more generalized interpretation of importance, as observed by the investigator (JD) during
questionnaire administration and then confirmed during cognitive interviews. For example, most
individuals believed that the ability to get out of bed independently was very important, therefore
would rate it high. However, if that individual had no difficulty with this task then it would not
be expected to be important to improve, and ought to be rated as a low importance goal within
the questionnaire. In an attempt to improve the clarity of the instructions, they were modified in
GOAL-LLA 1.1 from select how important a goal it is for you to improve each of the following
to select how important a goal it is for you to improve each of the following activities. Despite
this effort to clarify these instructions, inconsistent interpretation continued to be observed by the
investigator, specifically for parents (JD).

48
Finally, five of the 13 cognitive interview participants admitted they had not actually read the
instructions when initially completing the questionnaire.
7.1.3.3 Suitability of the Response Scale
It was evident during the first round of GOAL administration that the recall period in the GOAL-
CP (in the past 4 weeks) was problematic in D) Physical Activities, Games & Recreation, as
some of these items were seasonal [e.g., riding a bicycle (D), swimming (D)]. Given that our
questionnaire administration was primarily over the winter, several items had respondents
checking the option I did not do this in the past 4 weeks. One child commented “I’ve been living
with this a long time, I know how these activities affect me even if I haven’t done them in the past
4 weeks”. To facilitate data collection for item analysis, respondents to the GOAL-CP were
instructed to consider the past year for the activities in D). This change was then formalized in
the next iteration of the questionnaire (GOAL-LLA 1.0).
Eleven of 13 children indicated during the cognitive debrief that they were able to find their
answer in the response options provided. One child believed their difficulty identifying an
appropriate response option was item specific, reporting that he had the greatest difficulty
categorizing his pain/discomfort. There was no consensus on the number of response options
that should be used. Seven children indicated the current number of options was adequate (“it’s
great, people need options”), four felt there were too many options (in the domains that used the
7- point ordinal scale) (“there’s a LOT of options”), and two believed that there should be more
options (“like a scale of 1 to 10”). No child reported concern using a scale that varied by
domain in wording or response option numbers.
When probed, some children had difficulty distinguishing between the qualifiers (extremely
difficult versus very difficult) used with the 7- point ordinal scale (“same as very difficult”,
“there’s not much difference between very difficult and extremely difficult”). Moreover,
although the scale used an odd number of response options, the midpoint was identified as
“slightly difficult”, negating the neutrality of a natural midpoint. Based on this and the
children’s cognitive interview comments, the development team (JD and UN) decided to modify
the scale of the GOAL-LLA 1.1 by using qualifiers only as anchors for the highest and lowest
score, Figure 6. No direct feedback was obtained from children or parents on this revised scale.

49
Figure 6. Modified Scale used in GOAL Domains Pertaining to Self-perceived Ability
(implemented in the GOAL-LLA 1.1)
7.1.3.4 Ease of usage
When asked in cognitive interviews “How do you feel about the amount of time it took to
complete the GOAL” three of 13 children (23%) indicated they felt it was too long. Time
required for children to complete the questionnaire varied from 12 to 19 minutes. When asked
“How easy or difficult did you find the GOAL to answer?” nine children (69%) reported that it
was easy. Two of these children indicated that they found importance ratings more difficult than
item scores to complete, and one child stated that they had difficulty providing responses for the
items in G) Body Image & Self-Esteem.
7.1.4 Children versus Parent Response (Objective 3)
Twenty pairs of children and their parents completed the GOAL questionnaires. Children’s item
scores were moderately correlated (r=0.42) with their parents’, although this did not reach
statistical significance (p=0.07, 95%CI=-0.03 to 0.73). As hypothesized, children’s item scores
were significantly higher (p<0.05) than their parents’. Figure 7 illustrates the relationship
between children’s and parents’ item scores across each item of the GOAL-LLA 1.1.
Figure 7. Children's and Parents' Mean Item Scores for the GOAL-LLA 1.1

50
Children’s importance ratings were strongly correlated (r=0.61, p<0.05, 95%CI=0.16 to 0.85)
with their parents’ ratings. However, as hypothesized, parents’ importance ratings were
significantly higher (p<0.001) than their children’s. Figure 8 illustrates the relationship between
children’s and parents’ importance rating scores across each item of the GOAL-LLA 1.1.
Figure 8. Children’s and Parents’ Mean Importance Ratings for the GOAL-LLA 1.1
FIGURE 7 and 8 Legend: Results from the third administration of the questionnaire (GOAL-LLA 1.1) (n=6 child-
parent dyads). Items 1-6 = A) Activities of Daily Living & Independence, Items 7-17 = B) Gait Function &
Mobility, Items 18-23 = C) Pain/Discomfort/Fatigue, Items 24-31 = D) Physical Activities, Games & Recreation,
Items 32-36= E) Gait Appearance, Items 37-41 = F) Use of Braces and Assistive Devices, Items 42-49 = G) Body
Image & Self-Esteem
7.1.5 Item Scores versus Importance Ratings (Objective 4)
There was a strong inverse association between children’s (n=24) total item score and
importance rating score (r=-0.69, p<0.001, 95% CI=-0.87 to -0.37). This relationship, presented
as mean scores for the GOAL-LLA 1.1, is illustrated by comparing Figures 7 and 8.
The association between parent’s (n= 19) item scores and importance ratings (r=-0.07, p=0.81,
95% CI=-0.54 to 0.44) was insubstantial (106) and did not reach significance.
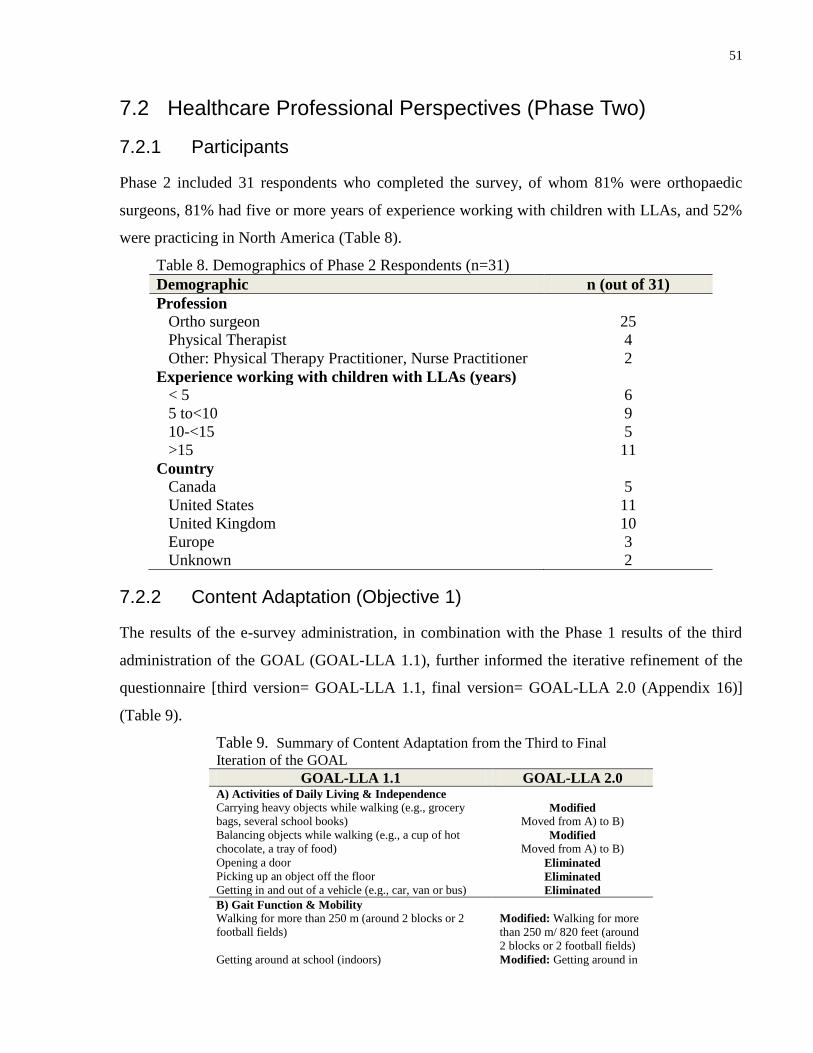
51
7.2 Healthcare Professional Perspectives (Phase Two)
7.2.1 Participants
Phase 2 included 31 respondents who completed the survey, of whom 81% were orthopaedic
surgeons, 81% had five or more years of experience working with children with LLAs, and 52%
were practicing in North America (Table 8).
Table 8. Demographics of Phase 2 Respondents (n=31)
Demographic n (out of 31)
Profession
Ortho surgeon 25
Physical Therapist 4
Other: Physical Therapy Practitioner, Nurse Practitioner 2
Experience working with children with LLAs (years)
< 5 6
5 to<10 9
10-<15 5
>15 11
Country
Canada 5
United States 11
United Kingdom 10
Europe 3
Unknown 2
7.2.2 Content Adaptation (Objective 1)
The results of the e-survey administration, in combination with the Phase 1 results of the third
administration of the GOAL (GOAL-LLA 1.1), further informed the iterative refinement of the
questionnaire [third version= GOAL-LLA 1.1, final version= GOAL-LLA 2.0 (Appendix 16)]
(Table 9).
Table 9. Summary of Content Adaptation from the Third to Final
Iteration of the GOAL
GOAL-LLA 1.1 GOAL-LLA 2.0 A) Activities of Daily Living & Independence
Carrying heavy objects while walking (e.g., grocery
bags, several school books) Modified
Moved from A) to B)
Balancing objects while walking (e.g., a cup of hot
chocolate, a tray of food) Modified
Moved from A) to B)
Opening a door Eliminated
Picking up an object off the floor Eliminated
Getting in and out of a vehicle (e.g., car, van or bus) Eliminated
B) Gait Function & Mobility
Walking for more than 250 m (around 2 blocks or 2
football fields)
Modified: Walking for more
than 250 m/ 820 feet (around
2 blocks or 2 football fields)
Getting around at school (indoors) Modified: Getting around in

52
crowded spaces (school,
concert, shopping centre)
Getting around in crowded spaces (concert, special
event, mall)
See above
Standing in long lineups Modified: Standing for a long
time (lineups/ queues, parade,
concert)
Moving quickly when in a hurry (e.g. to catch a bus,
late for an event) Eliminated
Keeping up with my friends Modified: Keeping up with
my friends while walking
outdoors
Stepping around or avoiding obstacles Retained
Going up and down stairs Retained
Going up and down slopes Modified: Going up and
down ramps/ hills
Walking on uneven ground (rough, rocky, sandy) Retained
Walking on slippery or icy surfaces Modified: Walking on wet,
slippery or icy surfaces
C) Pain/Discomfort/Fatigue
Pain or discomfort in the feet or ankles Retained
Added: Pain or discomfort in
the lower legs (shin or calf)
Pain or discomfort in the knees Retained
Pain or discomfort in the thighs or hips Retained
Pain or discomfort in the back Retained
Feeling tired while walking Retained
Feeling tired during any other physical activities that I
usually enjoy (e.g., swimming, running, horseback
riding, or other)
Modified: Feeling easily tired
during physical activities that
I enjoy (swimming, running,
or other sports)
D) Physical Activities, Games, & Recreation
Climbing (e.g., ladder or stepstool) Modified: Climbing (e.g.,
ladder, playground
equipment, climbing wall)
Running fast Retained
Participating in gliding sports (e.g., skating,
rollerblading, skiing, skate/snowboarding) Retained
Riding a bike or tricycle (with or without training
wheels) Retained
Swimming Retained Participating in sports that require running (e.g., soccer,
baseball, football, track) Retained
Participating in sports that require jumping (e.g.,
basketball, volleyball) Retained
Participating in gymnastics, dance or martial arts (e.g.,
karate, judo, taekwondo)
Modified: Participating in
sports that require balance
(e.g., gymnastics, dance,
martial arts)
E) Gait Appearance
Walking with my feet flat on the ground Retained
Walking taller or more upright (less crouched or bent at
the knees) Retained
Walking with my feet pointing straight ahead Retained
Walking without a limp Retained
Walking without tripping and falling Retained
F) Use of Braces and Assistive Devices
A shoelift Retained
A brace (e.g., AFO) Retained
Added: A prosthesis
Using a walking aide (e.g., walker, stick, cane,
crutches) Retained
Using a wheelchair Retained

53
Other assistive devices (e.g., built-up bicycle pedal
or________) Retained
G) Body Image & Self-Esteem
The shape and position of my legs Retained
The shape and position of my feet Retained
The symmetry of my legs (in length and size) Retained
Wearing my choice of footwear (e.g., shoes, boots,
sandals) Retained
Wearing my choice of clothing (e.g., shorts, skirts,
bathing suits) Retained
The appearance of how I get around compared with
others Retained
The way others feel about how I get around Retained How I am treated by others Retained
The frequency of HCP responses (Accept, Accept with Modification, and Reject), by item, is
illustrated in Table 10.
7.2.2.1 Item Elimination
Four items that were in GOAL-LLA 1.1 were eliminated in the final iteration of the GOAL
(GOAL-LLA 2.0) (Table 9). One item [opening a door (A)] received four HCP reject responses
(Table 10) too many to be retained (as previously described in 6.2.4.1). Based on concerns put
forth by HCPs related to perceived redundancy in the GOAL (described in 7.2.3.2), the
development team (JD and UN) judged that moving quickly when in a hurry (B) overlapped with
running fast (D) since both items were speed related. The latter was retained based on children
and parent’s having an overall lower item score and a wider range of item scores noted for
GOAL-LLA 1.1 (Appendix 15). The other two items eliminated were informed by Phase 1
results and were discussed in 7.1.2.1.
Table 10. Results of the Administration of the GOAL-LLA 1.1 in Phase Two (Health Care
Professional Perspectives) (n=31)
‘Accept’
(%)
‘Accept with
Modification’
(%)
‘Reject’
(%) A) Activities of Daily Living & Independence
Carrying heavy objects while walking (e.g. grocery
bags, several school books)
24 (77) 5 (16) 2 (6)
Balancing objects while walking (e.g., a cup of hot
chocolate, a tray of food)
28 (90) 1 (3) 2 (6)
Opening a door 22 (71) 5 (16) 4 (13)
Picking up an object off the floor 26 (84) 2 (6) 3 (10)
Getting in and out of a vehicle (e.g., car, van, or bus) 27 (87) 3 (10) 0
B) Gait Function & Mobility
Walking for more than 250 m (around 2 blocks or 2
football fields)
22 (71) 9 (29) 0
Getting around at school (indoors) 27 (87) 3 (10) 1 (3)
Getting around in crowded spaces (concert, special 24 (77) 6 (19) 1 (3)

54
event, mall)
Standing in long lineups 22 (71) 6 (19) 3 (10)
Keeping up with friends 24 (77) 7 (23) 0
Moving quickly when in a hurry (catch a bus, late for
event)
27 (87) 3 (10) 1 (3)
Stepping around or avoiding obstacles 29 (94) 0 2 (6)
Going up and down stairs 25 (81) 6 (19) 0
Going up and down slopes 24 (77) 6 (19) 1 (3)
Walking on uneven ground (rough, rocky, sandy) 29 (93) 2 (6) 0
Walking on slippery or icy surfaces 27 (87) 2 (6) 2 (6)
C) Pain/Discomfort/Fatigue
Pain or discomfort in the feet or ankles 28 (90) 2 (6) 1 (3)
Pain or discomfort in the knees 27 (87) 3 (10) 1 (3)
Pain or discomfort in the thighs or hips 26 (84) 4 (13) 1 (3)
Pain or discomfort in the back 29 (94) 1 (3) 1 (3)
Feeling tired while walking 19 (61) 12 (39) 0
Feeling tired during any other physical activities that
I usually enjoy (e.g., swimming, running, horseback
riding, or other)
22 (71) 8 (26) 1 (3)
D) Physical Activities, Games, & Recreation
Running fast 25 (81) 6 (19) 0
Participating in gliding sports (e.g., skating,
rollerblading, skiing, skate/snowboarding)
25 (80) 3 (10) 3 (10)
Riding a bicycle 29 (94) 2 (6) 0
Swimming 28 (90) 2 (6) 1 (3)
Participating in sports that require running (e.g.,
soccer, baseball, football, track)
27 (87) 4 (13) 0
Participating in sports that require jumping (e.g.,
basketball, volleyball)
29 (94) 2 (6) 0
Participating in gymnastics, dance or martial arts
(e.g., karate, judo, taekwondo)
28 (90) 2 (6) 1 (3)
Climbing (e.g., ladder or stepstool) 23 (77) 6 (19) 1 (3)
E) Gait Appearance
Walking with my feet flat on the ground 29 (94) 2 (6) 0
Walking taller or more upright (less crouched or bent
at the knees)
27 (87) 4 (13) 0
Walking with my feet pointing straight ahead 27 (87) 2 (6) 2 (6)
Walking without a limp 29 (94) 2 (6) 0
Walking without tripping and falling 31 (100) 0 0
F) Use of Braces and Assistive Devices
A shoe lift 25 (81) 6 (19) 0
A brace (e.g., AFO) 25 (81) 6 (19) 0
A walking aide (e.g., walker, stick, cane, crutches) 25 (81) 6 (19) 0
A wheelchair 25 (87) 6 (19) 0
Other assistive devices (e.g., built-up bicycle pedal
or________)
27 (87) 4 (13) 0
G) Body Image & Self-Esteem
The shape and position of my legs 30 (97) 1 (3) 0
The shape and position of my feet 30 (97) 1 (3) 0
The symmetry of my legs (in length and size) 25 (81) 5 (16) 1 (3)
Wearing my choice of footwear (e.g., shoes, boots,
sandals)
30 (97) 1 (3) 0
Wearing my choice of clothing (e.g., shorts, skirts,
bathing suits)
29 (94) 2 (6) 0
The appearance of how I get around compared with
others
30 (97) 1 (3) 0
The way others feel about how I get around 29 (94) 1 (3) 1 (3)
How I am treated by others 29 (94) 0 2 (6)
Table 10 Legend: Shaded items were automatically retained based on receiving at least 28 out of 31 Accept
responses. The other items required further critical appraisal to determine their appropriateness for retention or the
need to modify or eliminate.

55
7.2.2.2 Item Modification
Eleven items were modified in Phase 2 (Table 9), including two items that were moved to a
different domain (discussed in 7.2.2.4). Five of these modifications were based on HCP
suggestions and related directly to comprehension (7.2.3.1). Other changes were made to make
items more explicit (e.g., keeping up with my friends was modified to keeping up with my friends
while walking outdoors), and were based on suggestions of HCPs in their completed surveys.
7.2.2.3 Item Addition
There were two items added in Phase 2. Pain or discomfort in the lower legs (C) had been
eliminated in Phase 1, however, based on the comment of a HCP [“add shin, (sometimes kids get
bone pain, not just joint pain”)], the development team (JD and UN) felt that this item should be
included. The other addition was to include prosthetic as a separate item in F) (Table 9).
7.2.2.4 Item Retention
Two items that were retained in the GOAL-LLA 2.0 [carrying heavy objects while walking (A)
and balancing objects while walking (A)] were relocated to domain B) Gait Function and
Mobility, where the development team believed they were better aligned in concept (Table 9).
Seventeen of the 48 items were retained based on receiving at least 28 out of 31 “accept”
responses (previously discussed in 6.3.4.1). In total, 32 of the 48 items in the GOAL-1.1 (67%)
were retained (without being moved or modified) at the end of Phase 2 (GOAL-LLA 2.0).
7.2.3 Sensibility (Objective 2)
7.2.3.1 Comprehensibility
Comments from several HCPs reflected the development team’s initial concerns related to the
language used in the GOAL (e.g., “language too technical”, “symmetry probably not
understood…”, “vocab too advanced”), however, the definitions provided by the children during
cognitive interviews, described above (7.1.3.1), assured the development team the language was
appropriate.
To improve the generalizability of the questionnaire for use outside Canada the following
modifications were suggested by HCPs and implemented by the development team: distance

56
described in metres and feet, use of the term shopping centre as opposed to mall, add queue to
the list of examples provided for the item standing for a long time.
7.2.3.2 Ease of Usage
All 25 HCPs who identified strengths of the GOAL focused on its content, with 13 (52%)
commenting specifically that the questionnaire’s level of detail (comprehensiveness) was an
asset. The majority of responses (18 of 20 HCPs) identified weaknesses of the GOAL that could
be categorized as either its length or its complexity. 12 respondents (60%) indicated the length
was a weakness, of whom 4 specifically reported that there was redundancy of items.
Fifteen of 31 HCPs (48%) responded that the amount of time it would take for the GOAL-LLA
to be administered, was “too long”. Moreover, 5 HCPs indicated they would not consider the
GOAL-LLA for clinical use related to time constraints and lack of support staff to assist with
administration. Overall, after reviewing the GOAL-LLA 1.1, 23 of 30 (77%) would consider
using it in their clinical practice and twenty-seven of 30 HCPs (90%) reported they would
consider using this questionnaire for research purposes.
7.3 GOAL-LLA 2.0
The final iteration of the GOAL questionnaire, reflecting the cumulative results of Phase 1 and 2
of this study, is the GOAL-LLA 2.0 (Appendix 16). This questionnaire has 44 items organized
into six domains. Twenty-two items from the original 50 items (GOAL-CP) (44%) were retained
through each iteration of the questionnaire (with no modifications). Six items were new and 16
original items were modified. Domain A) Activities of Daily Living & Independence was
eliminated as a result of these adaptations.

57
Chapter 8 Discussion
This study aimed to develop an evaluative measure of physical and psychosocial gait-related
function suitable for children with a lower limb anomaly (GOAL-LLA), through iterative content
adaptation and questionnaire refinement of the GOAL-CP that was developed for a different
population. This process involved field-testing and sensibility evaluation of the GOAL-CP and
the subsequent two interim versions of the GOAL-LLA (GOAL-LLA 1.0 and GOAL-LLA 1.1).
LLAs encompass a wide spectrum of disorders and clinical presentations and the research team
wanted to create a questionnaire that was relevant (specific) to the issues of this diverse
population.
The decision to adapt the GOAL-CP for children with LLAs, as opposed to creating an entirely
new measure, was made for several reasons. The GOAL-CP already appeared to be a
comprehensive functional outcome measure for gait related problems that broadly covered all
domains of the ICF framework and was focused on patient priorities (84). Moreover, the content
of the GOAL-CP was generated, in part, from review of existing outcome measures that included
three measures previously used for children with LLAs (i.e., PODCI, ASK, FAQ) (84). Further,
working from the GOAL-CP as a template, required a shorter time frame than creating a new
measure. Although creating a new measure may appear to be a more comprehensive process, the
use of cognitive interviews in our study, and the opportunity for children, their parents, and
HCPs to provide suggestions for modifications and new items, ensured the adaptations through
the various iterations of the GOAL-LLA were well informed.
The inclusion of children, parents, and HCPs in the development of the GOAL-LLA module
contributes to its face and content validity, and ensures that the measured outcomes are
meaningful to all of the key stakeholders. Administration of the original GOAL-CP to children
with LLAs and their parents revealed that some of the item content was too easy, and
consequently, not considered important to change with treatment. This was true, particularly for
items in domain A) Activities of Daily Living & Independence. We found that children with
LLAs do not generally have functional issues with basic activities of daily living and
independence in contrast to children with CP, for whom these items pose a wide range of
difficulty. Domain A) was therefore eliminated from the questionnaire because its items

58
demonstrated a ceiling effect despite modifications to make them more challenging. Retaining
such items in the GOAL-LLA would impede the GOAL’s ability to discriminate between
children or its sensitivity to demonstrate change following interventions. This was one of the
limitations of generic functional outcome measures such as the ASK (6) and PODCI (5) when
applied to this population.
Conversely, domains that performed well and required minimal content adaptation were C)
Pain/Discomfort/Fatigue and G) Body Image and Self-Esteem. It appears that the original items
in these domains are generic enough to be applicable across the spectrum of LLAs as no items
were eliminated in either domain. In general, the items in these domains were the highest
priority items as indicated by their having the highest mean importance rating scores across all
versions of the questionnaire (Tables 6 and 7). For some children, cosmetic gains may be the
primary underlying motivation for surgical intervention such as EFT (2, 107, 108). Of note,
Varni and Setoguchi (109) found that the perceived physical appearance of children having a
congenital or acquired limb deficiency was significantly influenced by social environment and
perceived competence/adequacy (peer acceptance, scholastic competence, athletic competence),
and was positively correlated with self-esteem (p<0.001).
Of the six new items added, three are not typically used for children with CP (i.e., use of a
shoelift, use of a prosthesis, use of other assistive devices [e.g., built-up bicycle pedal]). Their
addition to the GOAL-LLA increased the specificity of this questionnaire module for use with
children with LLAs. Many of the modifications made based on child and parent feedback (Phase
1) were to increase the difficulty of the item content in keeping with the higher functional
abilities of this population (e.g., carrying an object while walking [e.g., toy, doll, book, cell-
phone] was modified to carrying heavy objects while walking [e.g., grocery bags, several school
books]). Subsequent modifications, informed primarily by HCPs (Phase 2) helped to refine the
language to improve specificity of the items (keeping up with friends while walking was
modified to keeping up with friends while walking outdoors); and to better reflect variations in
English language use internationally. For example ramp replaced slope as this could be
misconstrued as ski slope, and shopping centre replaced shopping mall, as this term is not
commonly known in the UK.

59
The inclusion of a multi-national group of HCPs in Phase 2 (16/28 from North America, 12/28
from the UK and Europe) was a first step in advancing the international transferability of the
questionnaire, however the results of this study may not be entirely generalizable beyond Canada
given the sample of children and parents used in Phase 1. Further cognitive interviews
conducted on small groups of children in other countries would either confirm the
generalizability of the questionnaire internationally or identify content or language that was
problematic. The results of these cognitive interviews would inform further questionnaire
modifications, or possibly, the need for a separate country/language-specific version (or module)
of the GOAL-LLA.
The use of cognitive interviews provides insight into children’s thought process and their level of
understanding while completing the GOLA-LLA. The greatest advantage of this process is the
opportunity to dialogue with the children and ensure that the questionnaire truly resonates with
them, which is difficult to ascertain through field-testing alone. The children in this study were
willing to talk about their personal experiences related to their LLA and several new item
suggestions were generated in this manner (e.g., wearing my choice of clothing, standing for a
long time).
The length of the GOAL might present a challenge for HCPs as far as administrative burden
(ease of use). The majority of children felt the length of the questionnaire was appropriate,
indicating that there is limited burden on the respondent. Often, too high a value is placed on
brevity, with many short scales having less than adequate reliability (110). Moreover, we believe
that the comprehensiveness of this questionnaire might be jeopardized if the number of items
was further reduced. Three HCPs suggested that some of the items in D) Physical Activities,
Games, & Recreation could be combined into team versus independent sports. However, each
group of activities measure a different component of gross motor function (e.g., running,
jumping, coordination) and should be evaluated separately for purposes of meaningful and
specific goal setting, intervention, and outcome evaluation.
The language of the questionnaire (comprehensibility) was appropriate for the children
participating in our study (i.e., Canadian children from 9 to 18 years of age). Fears of language
being too advanced were reflected in HCP comments (and had been a concern of the
investigators at the outset of the study), but these were not substantiated by children’s responses

60
in cognitive interviews or their performance during questionnaire administration. However, the
clarity of the instructions was problematic with regard to importance ratings of the items.
Despite modifications to the wording of these instructions, importance ratings were not always
interpreted as importance to improve with intervention, as intended by the development team.
Some parents continued to rate all items with high importance, presumably to demonstrate that
they felt the item was important to perform, indicated by their mean importance ratings being
significantly higher than children’s responses (mean difference of total importance rating scores
between children and their parents = 28.0, p<0.001). Items that received high scores would not
ordinarily be considered important to improve upon and it was judged that at least a moderate
negative correlation between item scores and their respective importance rating indicated that
respondents were properly interpreting the questionnaire’s instructions and rating system. This
pattern was observed between children’s item and importance rating scores (r=-0.69, p<0.05) but
not parents’ scores (r=-0.07, p=0.81). This is most likely attributable to misinterpretation of the
importance scoring or because the instructions were not read. Thirty-eight percent of children
participating in cognitive interviews reported they had not read the instructions. Additionally,
the investigator administering the questionnaire might have provided more detailed instruction to
the child respondent assuming they would require more direction than their parents. As such,
standardized verbal instructions may be required to ensure interpretation of importance ratings
that is consistent with the intended meaning. Inconsistent interpretation of items or instructions
among respondents invalidates the results of a questionnaire for comparative studies.
Children had significantly higher item scores and lower importance ratings than their parents.
However, there was a moderate association between both groups’ importance rating scores (r=
0.61), indicating both children and their parents had similar ideas related to what their priorities
were, despite attributing different number values to the score. This is consistent with the Priority
Framework for Outcomes Assessment (47) that indicates the perspectives of stakeholders might
overlap but might not be concordant. This affirms that child- and parent- report versions of the
GOAL-LLA should be administered to ensure that both perspectives are captured and taken into
consideration when making health-care decisions.
Scoring of the GOAL provides a total GOAL score and six separate domain scores. Importance
ratings do not contribute to the score. They are only intended to identify those items to focus on
when goal setting for intervention. Unlike other outcome measures that have previously been

61
used in this population (e.g., ASK, FAQ), the GOAL-LLA is intended, through its design, to
capture the priorities of families related to intervention (e.g., surgical, rehabilitative) goals. The
example below illustrates how the inclusion of importance ratings, results in different items
being highlighted as a consideration for intervention goals. Very importantly, this shows that the
items that are rated highest in importance are not consistent across all respondents. Individual
children and/or their parents have individual priorities that cannot be assumed to be similar even
for children with similar diagnoses and severity of involvement. The GOAL allows for easy
identification of items that are particularly problematic to the individual and that they consider
very important to improve. Therefore the GOAL allows clinicians to identify an individual’s
treatment priorities, not all of which might be feasible, that would provide an opportunity to
guide further discussion, define/refine expectations and goals, assist with informed consent, and
facilitate appropriate clinical decision-making with regard to choice of intervention.
Furthermore, effectiveness of an intervention can be judged based on positive changes
particularly in items and domains that were identified to be most important. This aligns well with
the individualized goal approach taken with measures like the COPM and GAS in which priority
goals are identified. This is illustrated in the two following examples. In the future validation of
the GOAL-LLA, it would be helpful to consider whether the GOAL scores modified by the
importance ratings might provide a more meaningful or responsive outcome measure to evaluate
effectiveness of an intervention.
a) 11-year-old girl with a congenital femoral deficiency on the right side with nearly a nine-
centimeter length discrepancy.
Child’s Total Score: 221/246 = 89.8%
Item
Domain Item Score
Importance Rating
Wearing a brace (AFO) F) Use of Braces & Assistive Devices
1/4 4/4
Wearing my choice of footwear (e.g., shoes, boots, sandals)
G) Body Image & Self-Esteem
1/4 4/4
Wearing my choice of clothing (e.g., shorts, skirts, bathing suits)
G) Body Image & Self-Esteem
2/4 4/4
The shape and position of my feet G) Body Image & Self-Esteem
2/4 3/4
Walking taller or more upright (less crouched or bent at the knees)
E) Gait Appearance 2/6 2/4

62
b) 13-year-old boy with fibular hemimelia on the right side with nearly a five-centimeter
length discrepancy.
Child’s Total Score: 220/276 = 79.7%
Item
Domain Item Score
Importance Rating
Feeling tired during any other physical activities that I usually enjoy (e.g., swimming, running, horseback riding, or other sport)
C) Pain/Discomfort/Fatigue 2/5 3/4
Running D) Physical Activities, Games & Recreation
3/6 3/4
Feeling tired while walking C) Pain/Discomfort/Fatigue 1/5 2/4 Swimming D) Physical Activities, Games
& Recreation 4/6 2/4
The way I get around compared with others
G) Body Image & Self-Esteem 1/4 2/4
There is some potential for application of the GOAL-LLA 2.0 to individuals outside of the age
range used in our study sample (9 to 18 years). The content of the questionnaire content may be
applicable to children as young as five or six years of age, who spend all day at school and share
some physical and social experiences that overlap with those of older children. The suitability of
the GOAL-LLA 2.0 for younger children would however have to be confirmed, as there may be
age related developmental considerations for some of the item responses (e.g., riding a bicycle,
swimming, walking for more than 250 meters, standing for a long time) which may be
challenging for some five to eight year-olds (regardless of the presence of an LLA). Given that
the reliability of self-report decreases for children younger than nine years (95), the use of
parent-proxy may be most appropriate for this age group.
For children less than 5 years of age the GOAL-LLA 2.0 may serve as a template from which to
create a more developmentally appropriate evaluative outcome measure. Daltroy et al. (79)
found that while developing the PODCI, the questionnaires completed for children aged two to
five years, had more missing data for items pertaining to physical function and sports, than those
for older age groups, a likely indication these type of items are less relevant to young children.
Similarly, it is likely that the GOAL-LLA 2.0 would require revision to be suitable for an adult
population. Although several domains do appear relevant to individuals over 18 years of age
(Pain/Discomfort/Fatigue, Gait Appearance, Use of Braces/Assistive Devices, and Body Image
and Self-esteem) the items in domains specific to physical function (Gait Function and Mobility,
Physical Activities/Games/Recreation) may not all be applicable. For instance, some items are

63
activities specific to a school environment or emphasize sporting activities, which adults may
find less relevant or have less time or interest to perform. Additionally, it is possible that the
negative correlation between item scores and importance ratings is weaker than that seen with
children. For example, an adult may have great difficulty running fast (i.e., low item score) but
at this stage of their life they may place less value on this as an item to improve upon with
intervention (i.e., low importance rating). Adults with LLAs may feel there are many pertinent
items missing from the questionnaire (e.g., regarding employment opportunities, adult
relationships, parenting). The suitability of the GOAL-LLA 2.0 content to children and adults
outside of the age range used in our study sample could be further explored through cognitive
interviews or focus groups and field-testing of the questionnaire.
The development of age-appropriate modules of the GOAL-LLA 2.0 would allow the
questionnaire to be administered at different stages in an individual’s life. This may provide
clinicians and researchers with a better understanding of how individuals’ priorities might
change over time. The emergence of certain trends (i.e., domains that generally become more or
less important over time) could provide children with LLAs and/or their parents with meaningful
insight into possible future issues.
8.1 Limitations
The population of children with LLAs is very diverse with a range of clinical presentations and
severity. Our sample of only 25 children included a wide range of ages (the full range of targeted
ages was sampled), both genders (56% were female), and a broad range of diagnoses, but only
one participant was an amputee and a prosthetic user. A systematic review of lower limb
prosthetic outcome measures, by Condie (111) concluded that generic function and quality of life
measures are not appropriate for lower limb amputees. Future studies are needed to more closely
evaluate the suitability of the GOAL for this LLA sub-group and compare its performance with
them to other amputee-specific outcome measures such as AMP. Amputee-specific measures
tend to include items that pertain specifically to the fit and use of a prosthetic device and may
compare performance with and without prosthetic wear. Although such measures specifically
target issues that are unique to these children, there is value in using a more generic measure
such as the GOAL, as it increases the opportunity for comparison of results across the LLA
spectrum. In addition, children with acute illness related to sarcoma were excluded from our

64
study because it was anticipated the comorbidities of their condition (e.g., fatigue) might
influence their day-to-day performance, making the suitability of the GOAL-LLA to this LLA
sub-group uncertain. In the future the suitability of the GOAL-LLA will also need to be
evaluated with these children.
Although all of the key HCPs that work with children with LLAs were represented in our study
(i.e., orthopaedic surgeons, PTs, and nurses), our sample comprised primarily orthopaedic
surgeons (81%). It is not surprising that surgeons are over-represented in this sample, since they
are the key HCP in the current model of care to inform treatment, and most often serve as
primary investigators in research initiatives involving this population. More feedback however,
from physical therapists and nurses, may be warranted. In addition, orthotists/prosthetists,
psychologists, and social workers were not represented in this study sample. Further consultation
with these professionals could possibly generate new item suggestions.
The response scale was adjusted after the second administration of the questionnaire (GOAL-
LLA 1.0). Using word descriptors as anchors for only the end values (highest and lowest), the
development team felt that, given the odd number of response options, a neutral midpoint had
been created where it did not previously exist. Specific feedback on this new scale design still
needs to be sought to ensure it is actually an improvement compared to the original version.
Asking respondents to put words to the response options that are unlabeled will reveal their
comprehension of the scale and its intervals, and their perception of midpoint neutrality.
In an effort to optimize recruitment there were two different methods used for the administration
of the GOAL. The questionnaire was completed either in clinic in the presence of an investigator
available to provide support and ensure that parents and children worked independently, or at
home. There is no way of knowing if the children and parents completed the GOAL
independently in the home environment even though we asked them to do so on their own.
However, in total, only two families (less than 9% of the sample size) completed the
questionnaire at home and mailed in their responses so the effect of inconsistent administration
was considered negligible.
The GOAL is intended to be self-administered. However, for this study the questionnaire was
administered at the point of care by the investigator to ensure that the child and parent worked
independently, and to be available to respond to (and keep detailed notes on) any questions that
65
arose. The opportunity for respondents to ask questions and seek clarification when needed
might decrease the likelihood of missing item responses. Additionally, having the investigator in
the same room might increase a child and/or parent’s sense of accountability, making them more
likely to respond to each item but might decrease the respondent’s sense of anonymity making
them more likely to respond in a way they perceive as socially desirable. Additionally, this
increased sense of accountability may have minimized the time required to complete the
questionnaire (between 12 to 19 minutes) compared to self-administration.
The guiding principle used to eliminate items (i.e., “items were considered for elimination if both
the child and parent mean item score was within 0.5 of the maximum score (e.g., 5.5 to 6.0 out of
6.0) or if both the child and parent mean importance rating was from 0 to 0.5 out of 6.0”) led to
some inconsistencies in the decision-making process in regard to which items were retained or
eliminated. The research team (JD and UN) was cautious in their elimination of items,
recognizing that each administration of the questionnaire was to a relatively small sample [n= 12
children and 11 parents (GOAL-CP), n= 5 children and 5 parents (GOAL-LLA 1.0), and n= 7
children and 6 parents (GOAL-LLA 1.1)]. Additionally, the elimination process was
complicated by the misinterpretation of importance ratings by some respondents, as previously
discussed, casting some doubt on the validity of these scores to inform item elimination in the
manner that the research team intended. To overcome these limitations, the team often opted to
retain an item until it had performed poorly in two subsequent administrations (versions) of the
questionnaire, allowing for input from a larger sample. As a result, some items that performed
poorly on one administration were ultimately retained (e.g., going up and down stairs).
The study methodology provided families the opportunity to guide the preliminary adaptations of
the questionnaire (GOAL-CP was modified to GOAL-LLA 1.0, that was then modified to
GOAL-LLA 1.1) and HCPs the opportunity to guide the final adaptations (GOAL-LLA 1.1 was
modified to GOAL-LLA 2.0). Unlike the first two adaptations of the questionnaire, the
performance of the final HCP-guided adaptation (GOAL-LLA 2.0) was not evaluated with
children and parents. However, it is reassuring that that the content between the third and final
iteration was quite stable, and any concerns will be picked up during the future formal validation
of the GOAL-LLA 2.0. The item focus was retained in 44 of 48 items from the GOAL-LLA 1.1
to GOAL-LLA 2.0, albeit with slight modifications to 12 of these items (e.g., standing in long
lineups was modified to standing for a long time (lineups/ queues, parade, concert) (Table 9).

66
Until the performance of the GOAL-LLA 2.0 is evaluated, we cannot know for certain if the
final adaptations will fully resonate with children having LLAs and their parents, and if not, what
final revisions might further improve this questionnaire for future use in this population.
8.2 Future Directions
Firstly, it would be beneficial to pilot the GOAL-LLA 2.0 on a sample of children and parents
across Canada to ensure there are no unanticipated issues considering, as noted above, that the
final questionnaire revision (GOAL-LLA 1.1 modified to GOAL-LLA 2.0) was guided primarily
by HCP feedback. This would provide an opportunity for the research team to make final
revisions to the questionnaire in preparation for formal psychometric testing.
Appreciating the time constraints and the limited support staff that HCPs might have to assist
with administration of questionnaires, our development team is committed to creating an
electronic (tablet or web-based) version of the GOAL to facilitate future clinical and research
use. This is considered a priority and should also precede formal psychometric testing so that the
electronic and paper versions of this questionnaire can be validated concurrently.
Formal psychometric testing of the GOAL-LLA is required prior to its utilization as an outcome
measure in research or clinical practice. These studies should evaluate reliability (internal
consistency and test-retest), validity (construct), and responsiveness (sensitivity to change).
Additionally, a larger sample of amputees and inclusion of children with sarcoma is required to
ensure the GOAL-LLA 2.0 is suitable for these LLA sub-groups. High internal consistency
(Cronbach’s alpha >90%) (112) within a specific domain may be suggestive of item redundancy,
indicating that further item elimination should be considered.
A confirmatory factor analysis is recommended to evaluate the development team’s decision to
group certain items together by domain based on subjective judgments. Factor analysis may
further highlight items that should be considered for elimination (e.g., items that do not load on
to any factor [i.e., domain]).
Given that the paediatric LLA population that requires treatment is small, and that the final
results of some surgical interventions (e.g., EFT, epiphyseodesis) may not be fully appreciated
for several months to years, the most practical study design would be to combine several

67
elements of psychometric testing together (i.e., reliability, validity, and responsiveness) and use a
large, international cohort, that can be studied both cross-sectionally and longitudinally.
8.3 Conclusions
This study supports the introduction of the GOAL-LLA 2.0 as a promising new outcome
measure for comprehensively evaluating the physical and psychosocial gait-related function and
priorities of children with LLAs, across all domains of the ICF, for both research and clinical
purposes. The methodology employed ensures this questionnaire is sensible for this population
and in particular carries excellent face and content validity. Following successful psychometric
testing, the GOAL-LLA has the potential to fill an identified gap in outcome measurement for
this population. Furthermore, it should fit well with family centered, team based care, providing
an opportunity for family priorities to be formally identified and inform individualized goal-
setting, intervention strategies, and outcome evaluation.

68
References
1. Hasler C, Krieg A. Current concepts of leg lengthening. Journal of Children's
Orthopaedics. 2012;6:89-104.
2. Montpetit K, Hamdy R, Dahan-Oliel N, Zhang X, Narayanan U. Measurement of health-
related quality of life in children undergoing external fixator treatment for lower limb
deformities. Journal of Pediatric Orthopedics. 2009;29:920-6.
3. Vitale M. The effect of leg length difference on health related quality of life: is the '2cm
rule' appropriate? J Ped Ortho. 2006;15:1-5.
4. Leet A, Wientroub S, Kushner H, Brillante B, Kelly M, Robey P, et al. The correlation of
specific orthopaedic features of polyostotic fibrous dysplasia with functional outcome scores in
children. Journal of Bone & Joint Surgery. 2006;88:818-23.
5. Lee K, Chung C, Gwon D, Sung K, Cho J, Kim T, et al. Parental perspectives on leg
length discrepancy. Journal of Pediatric Orthopedics, Part B. 2012;21:146-9.
6. Sheiko M, Bjornson K, Lisle J, Song K, Eary J, Conrad Er. Physical activity assessment
in adolescents with limb salvage. Journal of Pediatric Orthopedics. 2012;161:1138-41.
7. Ramaker R, Lagro S, van Roermund P, Sinnema G. The Psychological and Social
Functioning of 14 children and 12 adolescents after Ilizarov Leg Lengthening. Acta Orthop
Scand. 2000;71:55-9.
8. McCarthy J, Glancy G, Chang F, Eilert R. Fibular hemimelia: comparison of outcome
measurements after amputation and lengthening. Journal of Bone and Joint Surgery. 2000;82-
A(12):1732-5.
9. Paley D, Herzenberg J, Paremain G, Bhave A. Femoral lengthening over an
intramedullary nail: a matched-case comparison with Ilizarov femoral lengthening. The Journal
of bone and joint surgery American volume. 1997;79:1464-80.
10. Paloski M, Taylor B, Iobst C, Pugh K. Pediatric and Adolescent Applications of the
Taylor Spatial Frame. Orthopaedics 2012;35:518-27.
11. Hudak P, Amadio P, Bombardier C, Group UEC. Development of an Upper Extremity
Outcome Measure: The DASH (Disabilities of the Arm, Shoulder, and Head). American Journal
of Industrial Medicine. 1996;29:602-8.
12. Pruitt S, Varni J, Setoguchi Y. Functional Status in Children with Limb Deficiency:
Development and Initial Validation of an Outcome Measure. Archives of Physical Medicine and
Rehabilitation. 1996;77:1233-38.
13. Collins D. Pretesting survey instruments: An overview of cognitive methods. Quality of
Life Research. 2003;12:229-38.

69
14. Sackett R, Straus S, Richardson W, Rosenberg W, Haynes R. Evidence Based Medicine:
How to practice and teach EBM. 2nd ed. Toronto: Churchill Livingstone; 2000.
15. Gross R. Leg Length Discrepancy: How much is too much? Orthopedics. 1978;1:307-10.
16. Michielsen A, Van Wijk I, Ketelaar M. Participation and quality of life in children and
adolescents with congenital limb deficiencies: a narrative review. Prosthetics and Orthotics
International. 2010;34:351-61.
17. Walker J, Knapp D, Minter C, Boakes J, Salazar J, Sanders J, et al. Adult outcomes
following amputation or lengthening for fibular deficiency. The Journal of bone and joint surgery
American volume. 2009;91:797-804.
18. Froster U, Baird P. Congenital defects of lower limbs and associated malformations: a
population based study. Am J Med Genet. 1993;45:60-4.
19. Saran N. Prevelance, significance, and etiology of limb-length discrepancies. . In: Hamdy
R, McCarthy J, editors. Management of Limb Length Discrepancies. Rosemont, IL: American
Academy of Orthopaedic Surgeons; 2011. p. 1-6.
20. Ghoneem HF WJ, Cole WG, Rang M,. The Ilizarov method for correction of Complex
Deformities. The Journal of Bone & Joint Surgery. 1996;78-A(10):6.
21. Kaufman K, Miller L, Sutherland D. Gait asymmetry in patients with limb-length
inequality. J Ped Ortho. 1996;16:144-50.
22. Paley D. Principles of Deformity Correction. JE H, editor. New York: Springer; 2005.
23. Kiapour A, Abdelgawad A, Goel V, Souccar A, Terai T, Ebraheim N. Relationship
between limb length discrepancy and load distribution across the sacroiliac joint- a finite element
stidy. J Orthop Res. 2012;30:1577-80.
24. McCarthy J, MacEwen G. Management of leg length inequality. J South Orthop Assoc.
2001;10:73-85.
25. Murrell P, Cornwall M, Doucet S. Leg-length discrepancy: its effect on mean center-of-
pressure position and postural sway. Arch Phys Med Rehabil. 1991;72:646-48.
26. Harvey W, Yang M, Cooke T, al. e. Association of leg-length inequality with knee
osteoarthritis: a cohort study. Ann Intern Med. 2010;152:287-95.
27. Golightly Y, Allen K, Helmick C, Schwartz T, Renner J, Jordan J. Hazard of incident and
progressive knee and hip radiographic osteoarthritis and chronic joint symptoms in individuals
with and without leg length inequality. Journal of Rheumatology. 2010;37:2133-40.
28. Birch J, Guidera K, Heinrich S. Knee and Leg: Pediatric Aspects. In: Beatty J, editor.
Orthopedic Knowledge Update 6: American Academy of Orthopedic Surgeons; 1999. p. 505-20.
29. Gurney B. Leg length discrepancy. Gait & Posture. 2002;15:195-206.
70
30. Scaduto A, Otsuka N. Amputation and Prosthetic Fitting. In: Hamdy R, McCarthy J,
editors. Managament of Limb-Length Discrepancies. Rosemont, IL: American Academy of
Orthopaedic Surgeons; 2011.
31. Saran N, Rathjen K. Treatment of Limb-Length Discrepancy with Epiphysiodesis. In:
Hamdy R, McCarthy J, editors. Management of Limb-Length Discrepancies. Rosemont, IL:
American Academy of Orthopaedic Surgeons; 2011.
32. Behrens F. General theory and principles of external fixation. Clinical Orthopaedics and
Related Research. 1989:15-23.
33. Birch J. Lengthening for congenital lower limb deficiencies. In: Hamdy R, McCarthy J,
editors. Management of Limb-Length Discrepancies. Rosemont, IL: American Academy of
Orthopaedic Surgeons; 2011.
34. Emara k, Diab R, El Ghazali S, Farouk A, El Kersh M. Foot and ankle function after
tibial overlengthening. Journal of Foot and Ankle Surgery. 2014;53:12-5.
35. Gordon J, Manske M, Lewis T, O'Donnell J, Schoenecker P, Keeler K. Femoral
Lengthening over a Pediatric Femoral Nail: Results and Complications. J Ped Ortho.
2013;33:730-6.
36. Sabharwal S, Louie K, Reid J. What's new in limb-lengthening and deformity correction.
The Journal of bone and joint surgery American volume. 2014;96:1399-1406.
37. Hamdy R, Makhdom A, Saran N, Birch J. Congenital fibular deficiency. J Am Acad
Orthop Surg. 2014;22:246-55.
38. Westberry D, Davids J, Pugh L. The Boyd amputation in children: indications and
outcomes. J Ped Ortho. 2014;34:86-91.
39. Nagarajan R, Neglia J, Clohisy D, Robison L. Limb salvage and amputation in survivors
of pediatric lower-extremity bone tumours: What are the long term implications? Journal of
Clinical Oncology. 2002;Electronic Edition:4493-507.
40. Patel S, Paley D, Herzenberg JE. Limb-lengthening versus amputation for fibular
hemimelia. The Journal of bone and joint surgery American volume. 2002;84-A(2):317-9.
41. Pakulis J, Young N, Davis A. Evaluating physical function in an adolescent bone tumour
population. Pediatric Blood & Cancer. 2005;45:635-43.
42. World Health Organization. How to use the ICF: A practical manual for using the
International Classification of Functioning, Disability and Health (ICF). Exposure draft for
comment. Geneva: WHO; 2013.
43. Stucki G. Cieza A. The International Classification of Functioning, Disability and Health
(ICF) in physical and rehabilitation medicine. European journal of physical and rehabilitation
medicine. 2008;44:4.

71
44. Jette A. Towards a common language for function, disability, and health. Physical
Therapy. 2006;86:726-34.
45. Petersson C, Simeonsson RJ, Enskar K, Huus K. Comparing children's self-report
instruments for health-related quality of life using the International Classification of Functioning,
Disability and Health for Children and Youth (ICF-CY). Health & Quality of Life Outcomes.
2013;11:75.
46. Wright V, Rosenbaum P, Goldsmith C, Law M, Fehlings D. How do changes in body
functions and structures, and activity, and participation relate in children with cerebral palsy.
Developmental Medicine and Child Neurology. 2008;50:283-9.
47. Narayanan U. Outcomes Assessment of Fractures in Children. In: Mencio G,
Swiontkowski M, editors. Green's Skeletal Trauma in Children. 5th ed. Philadelphia: Elsevier
Saunders; 2015.
48. Goldberg M. Measuring outcomes in cerebral palsy. Journal of Pediatric Orthopedics.
1991;11:682-5.
49. Cieza A, Geyh S, Chatterji S, Kostanjsek N, Ustun B, Stucki G. ICF linking rules: an
update based on lessons learned. Journal of Rehabilitation Medicine. 2005;37:212-8.
50. Cieza A, Brockow T, Ewert T, Amman E, al. e. Linking health-status measurements to
the international classification of function, disability, and health. Journal of Rehabilitation
Medicine. 2002;34:205-20.
51. Krieg A, Lenze U, Speth B, Hasler C. Intramedullary leg lengthening with a motorized
nail. Acta Orthop. 2011;82:344-50.
52. Ganger R, Radler C, Speigner B, Grill F. Correction of post-traumatic lower limb
deformities using the Taylor spatial frame. Int Orthop. 2010;34:723-30.
53. Birch J, Walsh M, Morton A, Koch K, Smith C, Cummings D, et al. Syme amputation for
the treatment of fibular deficiency: an evaluation of long-term physical and psychological
functional status. Journal of Bone & Joint Surgery- American Volume. 1999;81:1511-8.
54. Mahboubian S, Seah M, Fragomen A, Rozbruch S. Femoral lengthening with lengthening
over a nail has fewer complications than intramedullary skeletal kinetic distraction. Clin Orthop
Relat Res. 2012;470:1221-31.
55. Muller K, Muller-Farber J. Indications, localization and planning osteotomies about the
knee. In: Hierholzer G, Muller K, editors. Corrective osteotomies of the lower extremity after
trauma. Berline: Spinger-Verlag; 1984. p. 195-223.
56. Al-Sayyad M. Lower limb lengthening and deformity correction using the Fitbone
motorized nail system in the adolescent patient. Journal of Pediatric Orthopedics. 2012;21:131-6.

72
57. Radler C, Kranzl A, Manner H, Hoglinger M, Ganger R, Grill F. Torsional profile versus
gait analysis: consistency between the anatomic torsion and the resulting gait pattern in patients
with rotational malalignment of the lower extremity. Gait & Posture. 2010;32:405-10.
58. Escott B, Ravi B, Weathermon A. EOS low-dose radiography: a reliable and accurate
upright assessment of lower limb lengths. Journal of Bone & Joint Surgery. 2013;95(e):1831-7.
59. Thaller P, Furmetz J, Wolf F, Eilers T, Mutschier W. Limb lengthening with fully
implantavle magnetically actuated mechanical nails (PHENIX)- preliminary results. Injury.
2014;45(Supplement 1):S60-5.
60. Paley, D. Problems, obstacles, and complications of limb lengthening by the Ilizarov
technique [review]. Clin Orthop Relat Res. 1990;250:81-104.
61. Courvoisier A, Sailhan F, Thevenin-Lemoine C, Vialle R, Damsin J. Congenital tibial
deficiencies: treatment using the Ilizarov's external fixator. Orthopaedics & Traumatology:
Surgery & Research. 2009;95:431-6.
62. Geiger R, Strasak A, Treml B, Gasser K, Kleinsasser A, Fischer V, et al. Six-minute walk
test in children and adolescents. Journal of Pediatrics. 2007;150:395-9.
63. Schoppen T, Boonstra A, deVries J, Goeken L, Eisma W. The TImed "Up & Go" Test:
reliability and validity in persons with unilateral lower limb amputation. Archives of Physical
Medicine and Rehabiliitation. 1999;80:825-8.
64. Rothman M, Beltran P, Cappelleri J, Lipscomb J, Teschendorf B, group MFP-rOCm.
Patient-reported outcomes: Conceptual Issues. ISPOR. 2007;10:S66-75.
65. Young N, Wright J. Measuring pediatric physical function. J Ped Ortho. 1995;15:244-53.
66. Furlong W, Barr R, Feeny D, Yandow S. Patient-focused measures of functional health
status and health-related quality of life in pediatric orthopedics: a case study in measurement
selection. Health & Quality of Life Outcomes. 2005;3(3).
67. Roye B, Matsumoto M, Vitale M. Selection of Appropriate Outcomes Instruments. J Ped
Ortho. 2012;32:S104-10.
68. Wright J, Feinstein A. A comparative contrast of clinimetric and psychometric methods
for consructing indexes and rating scales. Journal of clinical epidemiology. 1992;11:1201-18.
69. Wright J, McLeod R, Lossing A, Walters B. Measurement in surgical clinical research.
Surgery. 1996;119:241-44.
70. Vitale M, Choe J, Vitale M, al. e. Patient-based outcomes following clubfoot surgery: a
16-year follow-upu study. J Ped Ortho. 2005;25:533-8.
71. Bohtz C, Meyer-Heim A, Min K. Changes in health-related quality of life after spinal
fusion and scoliosis correction in patients with cerebral palsy. Journal of Pediatric Orthopedics.
2011;31:668-73.
73
72. Finch E, Brooks D, Stratford P, Mayo N. Physical rehabilitation outcome measures: A
guide to enhanced clinical decision making. Toronto: Canadian Physiotherapy Association;
2002.
73. Varni J, Burwinkle T, Lane M. Health-related quality of life measurement in pediatric
clinical practice: An appraisal and precept for future research and application. Health & Quality
of Life Outcomes. 2005;3:34.
74. Donnelly C, Carswell A. Individualized outcome measures: a review of the literature.
Canadian Journal of Occupational Therapy - Revue Canadienne d Ergotherapie. 2002;69:84-94.
75. Weiner S, Schwartz A, Sharma G, Binns-Calvey A, Ashley N, Kelly B, et al. Patient-
centered descision making and health care outcomes: an observational study. Annals of Internal
Medicine. 2013;158:573-9.
76. Wallen M, Ziviani J. Canadian Occupational Performance Measure: Impact of Blinded
parent-proxy ratings on outcome. The Canadian Journal of Occupational Therapy. 2012;79:7-14.
77. Tam C, Teachman G, Wright V. Paediatric application of individualised client-centred
outcome measures: a literature review. British Journal of Occupational Therapy. 2008;71:286-96.
78. Novacheck T, Stout J, Tervo R. Reliability and validity of the Gillette Functional
Assessment Questionnaire as an outcome measure in children with walking disabilities. Journal
of Pediatric Orthopedics. 2000;20.
79. Daltroy L, Liang MH, Fossel A, Goldberg M. The POSNA Pediatric Musculoskeletal
Functional Health Questionnaire: Report on Reliability, Validity, and Sensitivity to Change.
Journal of Pediatric Orthopedics. 1998;18:561-71.
80. Das S, Ganesh G, S P, Mohanty R. Outcome of eight-plate hemiepiphysiodesis on genu
valgum and height correction in bilateral fibular hemimelia. Journal of Pediatric Orthopedics.
2014;23:67-72.
81. Eralp L, Kocaoglu M, Toker B, Balci H, Awad A. Comparison of fixator-assisted aniling
versus circular external fixator for bone realignment of lower extremity anular deformities in
rickets disease. Archives of Orthopaedic & Trauma Surgery. 2011;131:581-9.
82. Liu T, Zhang X, Li Z, Peng D. Management of combined bone defect and limb-length
discrepancy after tibial chronic osteomyelitis. Orthopedics. 2011;34:e363-7.
83. Marshall M, Lockwood A, Bradley C, Adams C, Joy C, Fenton M. Unpublished rating
scales: a major source of bias in randomized controlled trials of treatments for schizophrenia.
British Journal of Psychiatry. 2000;176:249-52.
84. Karpati F, Narayanan U, Weir S. Gait Outcomes Assessment List (GOAL): Further
development of a meaningful outcome measure for children with ambulatory Cerebral Palsy. 6th
Annual Bloorview Research Symposium; Holland Bloorview Kids Rehabilitation Hospital2011.

74
85. Narayanan U, Weir S, Davidson B, editors. Gait Outcomes Assessment List (GOAL):
Developing a meaningful outcome measure for children with ambulatory cerebral palsy. 65th
Annual Meeting of American Academy for Cerebral Palsy and Developmental Medicine
(AACPDM); 2011; Las Vegas, Nevada.
86. Guyatt G, Bombardier C, Tugwell P. Measuring disease-specific quality life in clinical
trials. Canadian Medical Association Journal. 1986;134:889-95.
87. Ho E, Narayanan U, editors. Further development of the Gait Outcomes Assessment List
(GOAL): A patient priority-based outcome measure for ambulatory children with cerebral palsy.
Hospital for Sick Children Reasearch Day; June 26, 2013; Toronto, ON.
88. Rowe B, Oxman A. An assessment of the sensibility of a quality-of-life instrument. Am J
Emerg Med. 1993;11:374-80.
89. Feinstein A. Clinimetrics. New Haven, CT: Yale University Press; 1987.
90. O'Brien KK, Bayoumi AM, Bereket T, Swinton M, Alexander R, King K, et al.
Sensibility assessment of the HIV Disability Questionnaire. Disability and rehabilitation.
2013;35:566-77.
91. Salbach N, Jaglal S, Williams J. Reliability and validity of the Evidence-Based Practice
Confidence (EPIC) Scale. Continuing Education in the Health Professions. 2013;33:33-40.
92. Terwee CB, Mokkink LB, van Poppel M, Chinapaw M, van Mechelen W, de Vet H.
Qualitative attributes and measurement properties of physical activity questionnaires: A
checklist. Sports Med. 2010;40:525-37.
93. Lohr K, Aaronson N, Alonso J, Burman M, Patrick D, Perrin E, et al. Evaluating quality-
of-life and health status instruments: development of scientific review criteria. Clinical
Therapeutics. 1996;18:979-92.
94. Scientific Advisory Committee of the Medical Outcomes Trust. Assessing health status
and quality of life instruments: Attributes and review criteria. Quality of life research : an
international journal of quality of life aspects of treatment, care and rehabilitation. 2002;11:193-
205.
95. Raven-Sieberer U, Erhart M, Wille N, Wetzel R, Nikel J, Bullinger M. Generic health-
related quality-of-life assessment in children and adolescents. Pharmoeconomics. 2006;24:1199-
220.
96. Wooley M, Bowen G, Bowen N. Cognitive pretesting and the developmental validity of
child self-report instruments: theory and application. Res Soc Work Pract. 2004;14:191-200.
97. Mulcahey M, Chafetz R, Santangelo A, Costello K, Merenda L, Calhoun C, et al.
Cognitive Testing of the Spinal Appearance Questionnaire with Typically Developing Youth and
Youth with Idiopathic Scoliosis. J Ped Ortho. 2011;31:661-7.

75
98. Kelly L, Jenkinson C, Ziebland S. Measuring the effects of online health information for
patients: Item generation for an e-health impact questionnaire Patient Education and Couseling.
2013;93:433-8.
99. Sheffler L, Hanley C, Bagley A, Molitor F, James M. Comparison of self-reports and
parent proxy-reports of function and quality of life of children with below-the-elbow deficiency.
Journal of Bone & Joint Surgery. 2009;91:2852-9.
100. Narayanan U. Concerns, Desires, and Expectations of for Adolescent Idiopathic
Scoliosis: A Comparison of Patients', Parents', and Surgeons' Perspectives. Toronto: University
of Toronto; 2008.
101. Forrest C, Riley A, Vivier P. Predictors of children's healthcare use: the value of child
versus parental perspectives on healthcare needs. Medical Care. 2004;42:232-8.
102. Jobe J, Mingay D. Cognition and survey measurement: History and overview. Appl Cogn
Pyschol. 1991;5:175-92.
103. R Core Team. R: A language and environment for statistical computing Vienna, Austria:
R Foundation for Statistical Computing; 2014. Available from: http://www.R-project.org.
104. Young N, Bradley C, Blanchette V, Wakefield C, Barnard D, Wu J, et al. Development
of a health-related quality of life measure for boys with haemophilia: the Canadian Haemophilia
Outcomes- Kids Life Assessment Tool (CHO-KLAT). Haemophilia. 2004;10(Supplement 1):34-
43.
105. Turner R, Quittner A, Parasuraman B, Kallich J, Cleeland C, Group MFP-ROCM.
Patient-reported outcomes: Instrument development and selection issues. Internation Society for
Pharmoeconomics and outcomes research (ISPOR). 2007;10(Suppl 2):S86-93.
106. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. New Jersey:
Lawrence Erlbaum; 1988.
107. Bond J, Kent G, Binney V, Saleh M. Psychological adjustment of children awaiting limb
reconstruction. Child: Care, Health, and Development. 1999;25:313-21.
108. Moseley C. Leg-Length discrepancy. In: Weinstein S, editor. Lovell and Winter's
Pediatric Orthopaedics, 6th Edition. Philadelphia, PA: Lippincott Williams & Wilkins; 2006. p.
1214-51.
109. Varni J, Setoguchi Y. Correlates of perceived physical appearance in children with
congenital/acquired limb deficiencies. Developmental and Behavioral Pediatrics. 1991;12:171-6.
110. DeVellis R. A consumer's guide to finding, evaluating, and reporting on measurement
instruments. Arthritis Care & Research. 1996;9:239-45.
111. Stucki G, Kostanjsek N, Ustun B, Cieza A. ICF-based classification and measurement of
functioning. European journal of physical and rehabilitation medicine. 2008;44:14.

76
112. DeVellis R. Scale development: Theory and applications. Newbury Park, CA: Sage;
1991.
113. Matza L, Swensen A, Flood E, Secnik K, Leidy N. Assessment of health-related quality
of life in children: a review of conceptual, methodological, and regulatory issues. ISPOR.
2004;7:79-92.
114. Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL, et al. The
COSMIN checklist for assessing the methodological quality of studies on measurement
properties of health status measurement instruments: an international Delphi study. Quality of
life research : an international journal of quality of life aspects of treatment, care and
rehabilitation. 2010;19:539-49.

77
Appendices
Appendix 1. Literature Search Strategy
Searches Results exp Leg Length Inequality/ae, cn, px, rh, su, th [Adverse Effects, Congenital, Psychology, Rehabilitation, Surgery, Therapy]
1399
exp Limb Deformities, Congenital/cl, px, rh, su, th [Classification, Psychology, Rehabilitation, Surgery, Therapy]
4982
exp Osteogenesis, Distraction/ae, cl, px, rh [Adverse Effects, Classification, Psychology, Rehabilitation]
326
exp Bone Lengthening/ae, px, rh [Adverse Effects, Psychology, Rehabilitation]
715
exp External Fixators/ae, sn [Adverse Effects, Statistics & Numerical Data]
312
exp Ilizarov Technique/ae, px, rh, sn [Adverse Effects, Psychology, Rehabilitation, Statistics & Numerical Data]
143
exp Femur/ab [Abnormalities] 1273
exp Tibia/ab [Abnormalities] 1105
exp Genu Varum/cn, rh, su, th [Congenital, Rehabilitation, Surgery, Therapy]
48
exp Genu Valgum/rh, su, th [Rehabilitation, Surgery, Therapy]
43
exp Amputation/ae, cn, px, rh, sn, su, th [Adverse Effects, Congenital, Psychology, Rehabilitation, Statistics & Numerical Data, Surgery, Therapy]
3530
exp Artificial Limbs/ae, px, rh, sn [Adverse Effects, Psychology, Rehabilitation, Statistics & Numerical Data]
465
1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12
12866
exp Questionnaires/cl, ec, mt, st, td, ut [Classification, Economics, Methods, Standards, Trends, Utilization]
10370
mobility.mp. 110706
function.mp. 1526202
14 or 15 or 16 1631879
13 and 17 1280
limit 18 to (yr="2000 - 2014" and "all child (0 to 18 years)")
435

78
Appendix 2. Development of the Gait Outcomes Assessment List (GOAL)
Item Generation
The GOAL’s initial bank of 60 potential items for children with CP, was generated through a
purposeful method of item generation from: 1) a literature review 2) appraisal of existing
questionnaires including the Gillette Gait Index (GGI), Gait Deviation Index (GDI), Movement
Analysis Profile (MAP), Gait Profile Score (GPS), Gross Motor Function Measure (GMFM-66),
Activity Scale for Kids (ASK), Pediatric Outcomes Data Collection Instrument (PODCI),
Gillette Functional Assessment Questionnaire (FAQ), Functional Mobility Scale (FMS), and the
Cerebral Palsy Quality of Life (CP-QOL), and 3) open-ended interviews with children having CP
(n=22, 15 boys, 7 girls) and their parents recruited from a paediatric rehabilitation hospital.
Appraisal of existing instruments, as was done with the GOAL, is considered a core component
of item generation as it serves two purposes: first, to ensure an appropriate measure does not
already exist, and two, to identify common themes or domains in similar or related measures
(86). Not all of the questionnaires appraised for item generation where CP-specific (e.g., the
PODCI is a generic measure for musculoskeletal and health function), increasing the likelihood
that items might be generalizable to the LLA population.
Inclusion of the target population during item generation provides valuable insight into
stakeholders’ perspectives, ensuring items correspond directly to their experiences and activities
(64, 113) and is considered a quality measure when reviewing the psychometric properties of an
outcome measure (94, 114). However, when a questionnaire is to be used in a population other
than the one for which it is developed, all items must be assessed for relevance with the new
population (114). As such, this thesis study includes children with LLAs and parents to provide
feedback on item content.
Item Elimination
The preliminary a pool of 60 items was subsequently reduced to 48 through the use of item
importance ratings. Children with CP (n=9) and their parents (n=10), recruited from a large
urban paediatric rehabilitation hospital completed the GOAL and rated the perceived importance
of each item using a 5-point scale (0=not a goal, 4=important goal). Items with average

79
importance ratings less than 1.5 were considered for elimination (84, 85). This thesis study
employed a similar methodology to evaluate the importance of the items in the GOAL to
children with LLAs and their parents, for the purpose of informing item elimination.
Item Consensus
GOAL content was further informed by a formal consensus method in which feedback was
obtained on the GOAL 2.0 from an international multi-disciplinary group of content-related
health care professionals (HCP), including developmental paediatricians, orthopaedic surgeons,
engineers, physical therapists, occupational therapists, kinesiologists, physiatrists, and orthotists.
An e-survey was sent to 187 HCPs (response rate 32%, n=60) whom were asked, for each item
of the questionnaire, to accept, accept with modification and state the modification, or reject and
provide rationale for rejection. Consultation with HCPs or an expert panel is a basic expectation
of measure development (86, 105) to ensure comprehensive coverage of all possible, relevant
signs/symptoms most often reported by patients and items that may not be considered/reported
by children (105).

80
Appendix 3- GOAL-CP
1. We are trying to learn more about how you walk and what is important to you and your mobility. 2. Please read the instructions on each page carefully. 3. Please answer all questions by circling the number and checking the box that fits best.
4. You may choose to add more items that are important to you at the end of the questionnaire.
For example:
A) Activities of Daily Living & Independence LEVEL of ASSISTANCE IMPORTANCE of GOAL
Consider how you usually perform each of the following activities. 1) Rate how easy or difficult it was for you to perform each of these activities in the past 4 weeks; AND 2) Choose how much assistance you required to help you perform these activities; AND 3) Select how important a goal it is for you to improve in each of the following activities.
TOTA
L
MO
DER
ATE
MIN
IMA
L O
R
SUP
ERV
ISED
IND
EPEN
DEN
T
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
During the past 4 weeks:
Extremely Difficult /
Impossible Very
Difficult Difficult Slightly Difficult Easy Very Easy
No problem
at all
1. Getting in and out of bed
0 1 2 3 4
6 0
2 3
In the above example, getting in and out of bed was rated as very easy; required a moderate level of assistance; & improving this is a very important goal.
Your Name: _______________________________________________________________
Date of Completion (dd/mm/yy): _____________________________________________
5 1
GOAL Gait Outcomes Assessment List
Child Version
Page 1

81
A) Activities of Daily Living & Independence LEVEL of ASSISTANCE IMPORTANCE of GOAL
Consider how you usually perform each of the following activities. 1) Rate how easy or difficult it was for you to perform each of these activities in the past 4 weeks; AND 2) Choose how much assistance you required to help you perform these activities; AND 3) Select how important a goal it is for you to improve in each of the following activities.
TOTA
L
MO
DER
ATE
MIN
IMA
L O
R
SUP
ERV
ISED
IND
EPEN
DEN
T
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
During the past 4 weeks:
Extremely Difficult /
Impossible Very
Difficult Difficult Slightly Difficult Easy
Very Easy
No problem at
all
1. Getting in and out of bed
0 1 2 3 4 5 6 0 1 2 3
2. Getting in and out of a chair or wheelchair
0 1 2 3 4 5 6 0 1 2 3
3. Standing at a sink or counter
0 1 2 3 4 5 6 0 1 2 3
4. Showering or bathing
0 1 2 3 4 5 6 0 1 2 3
5. Using the toilet
0 1 2 3 4 5 6 0 1 2 3
6. Getting dressed
0 1 2 3 4 5 6 0 1 2 3
7. Carrying an object while walking (eg. toy, doll, book, cell-phone)
0 1 2 3 4 5 6 0 1 2 3
8. Opening a door manually
0 1 2 3 4 5 6 0 1 2 3
9. Picking up an object off the floor
0 1 2 3 4 5 6 0 1 2 3
10. Getting in and out of a vehicle (eg. unmodified car, van or bus)
0 1 2 3 4 5 6 0 1 2 3

82
B) Gait Function & Mobility WALKING AID REQUIRED IMPORTANCE of GOAL
Consider how you usually perform each of the following activities. 1) Rate how easy or difficult it was for you to perform each of these activities in the past 4 weeks; AND 2) Choose what walking aid you required to help you perform these activities; AND 3) Select how important a goal it is for you to improve in each of the following activities.
WH
EELC
HA
IR
WA
LKER
TWO
CA
NES
OR
CR
UTC
HES
ON
E C
AN
E /C
RU
TCH
/HA
ND
SU
PP
OR
T/ R
AIL
ING
OR
WA
LL
IND
EPEN
DEN
T
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
eme
ly im
po
rtan
t
During the past 4 weeks: Extremely
Difficult / Impossible
Very Difficult Difficult
Slightly Difficult Easy Very Easy
No problem at
all
11. Walking for more than 250 meters (around 2 blocks or 2 football fields)
0 1 2 3 4 5 6 0 1 2 3 4
12. Getting around at school (indoors) 0 1 2 3 4 5 6 0 1 2 3 4
13. Getting around at home
0 1 2 3 4 5 6 0 1 2 3 4
14. Walking for more than 15 minutes
0 1 2 3 4 5 6 0 1 2 3 4
15. Walking faster than usual to keep up with others
0 1 2 3 4 5 6 0 1 2 3 4
16. Stepping around or avoiding obstacles
0 1 2 3 4 5 6 0 1 2 3 4
17. Going up and down stairs
0 1 2 3 4 5 6 0 1 2 3 4
18. Going up and down slopes
0 1 2 3 4 5 6 0 1 2 3 4
19. Walking on uneven ground (rough, rocky, sandy)
0 1 2 3 4 5 6 0 1 2 3 4
20. Walking on slippery or icy surfaces
0 1 2 3 4 5 6 0 1 2 3 4

83
C) Pain / Discomfort / Fatigue INTENSITY IMPORTANCE of GOAL
Consider each of the following items. 1) Rate how often you experienced pain or discomfort or tiredness in the past 4 weeks; AND 2) Choose how severe the pain or discomfort was; AND 3) Select how important a goal it is for you to reduce pain or discomfort or tiredness in each of the following.
SEV
ERE
MO
DER
ATE
MIL
D
NO
NE
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
im
po
rtan
t
During the past 4 weeks:
Every Day
Very Often (nearly every
day)
Fairly Often (2 to 3 times
a week)
A Few Times
(once a week)
Once or Twice
None of the Time
21. Pain or discomfort in my feet or ankles
0 1 2 3 4 5 0 1 2 3
22. Pain or discomfort in my lower legs
0 1 2 3 4 5 0 1 2 3
23. Pain or discomfort in my knees
0 1 2 3 4 5 0 1 2 3
24. Pain or discomfort in my thighs or hips
0 1 2 3 4 5 0 1 2 3
25. Pain or discomfort in my back
0 1 2 3 4 5 0 1 2 3
26. Feeling tired while walking
0 1 2 3 4 5 0 1 2 3
27. Feeling tired during any other physical activities that I usually enjoy (eg. swimming, running, horseback riding or other sport)
0 1 2 3 4 5 0 1 2 3
Other pain: _________________
0 1 2 3 4 5 0 1 2 3

84
D) Physical Activities, Games & Recreation IMPORTANCE of GOAL
Consider how you usually perform each of the following activities. 1) Rate how easy or difficult it was for you to perform each of these activities in the past 4 weeks; AND 2) Select how important a goal it is for you to improve in each of the following activities.
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
im
po
rtan
t
During the past 4 weeks:
Extremely Difficult /
Impossible Very
Difficult Difficult Slightly Difficult Easy Very Easy
No problem at all
I did not do this activity in the past 4
weeks
28. Using playground equipment (ladders, monkey bars, slides, etc.) 0 1 2 3 4 5 6
29. Running
0 1 2 3 4 5 6
30. Participating in gliding sports (eg. skating, rollerblading, skiing, skate/snowboarding)
0 1 2 3 4 5 6
31. Riding a bike or tricycle (with or without training wheels)
0 1 2 3 4 5 6
32. Swimming
0 1 2 3 4 5 6
33. Participating in sports that require running (eg. soccer, baseball, football, track)
0 1 2 3 4 5 6
34. Participating in sports that require jumping (eg. basketball, volleyball)
0 1 2 3 4 5 6
35. Participating in dance or martial arts (eg. karate, judo, taekwondo)
0 1 2 3 4 5 6
Other recreational or sporting activity: _________________
0 1 2 3 4 5 6

85
E) Gait Appearance IMPORTANCE of GOAL
Consider each of the following items. 1) Rate how much of a problem you experienced with each of the following in the past 4 weeks; AND 2) Select how important a goal it is for you to improve in each of the following.
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rta
nt
Extr
em
ely
im
po
rtan
t
During the past 4 weeks:
Extremely Difficult /
Impossible Very
Difficult Difficult Slightly Difficult Easy
Very Easy
No problem
at all 36. Walking with my feet flat on the ground
0 1 2 3 4 5 6
37. Walking taller or more upright (less crouched or bent at the knees)
0 1 2 3 4 5 6
38. Walking with my feet pointing straight ahead
0 1 2 3 4 5 6
39. Walking without dragging my feet
0 1 2 3 4 5 6
40. Walking without tripping and falling
0 1 2 3 4 5 6
41. Wearing my choice of footwear (eg. shoes, boots, sandals)
0 1 2 3 4 5 6
Other aspect of my walking: _________________
0 1 2 3 4 5 6
Page 6 Version 3.1

86
F) Use of Braces and Assistive Devices IMPORTANCE of GOAL
Consider each of the following items. 1) Rate how you felt about using each of the following in the past 4 weeks; AND 2) Select how important a goal it is for you to reduce or eliminate your use of these devices.
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
During the past 4 weeks: Very
Unhappy Unhappy
Neither Happy
nor Unhappy Happy
Very Happy
42. Wearing braces or orthotics (eg. AFO)
0 1 2 3 4 I do not wear braces or
orthotics.
43. Using a walking aide (eg. walker, stick, cane, crutches)
0 1 2 3 4
I do not use any walking aides.
44. Using a wheelchair
0 1 2 3 4 I do not use a wheelchair.

87
G) Body Image & Self-Esteem IMPORTANCE of GOAL
Consider each of the following items. 1) Rate how you felt about each of the following in the past 4 weeks; AND 2) Select how important a goal it is for you to improve in each of the following.
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
im
po
rtan
t
During the past 4 weeks:
Very Unhappy Unhappy
Neither Happy nor Unhappy Happy Very Happy
45. The shape and position of my legs
0 1 2 3 4 46. The shape and position of my feet
0 1 2 3 4 47. The symmetry of my legs (in length and size)
0 1 2 3 4
48. The appearance of how I get around compared with others
0 1 2 3 4
49. The way others feel about how I get around
0 1 2 3 4 50. How I am treated by others
0 1 2 3 4
Page 7

88
Other Goals IMPORTANCE of GOAL
If there are any other goals (long or short term) that we have missed, please list them below AND Select how important a goal it is for you to improve in each.
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
Other Goals:
1.
2.
3.
4.
5.
Comments & Suggestions
Thank You Page 8 Version 3.1
89
Appendix 4. Child Consent Form
Title of Research Project: Priorities of Patients with Musculoskeletal Conditions and Related Gait Disorders
Investigator(s):
Dr. Unni Narayanan Co-Principal Investigator
Division of Orthopaedic Surgery, The Hospital for Sick Children
416-813-6432
Dr. Virginia Wright Co-Principal Investigator
Holland Bloorview Kids Rehabilitation Hospital
416-424-3824
Jennifer Dermott Investigator
Division of Physiotherapy, The Hospital for Sick Children
416-813-6755 x48
MSc candidate (Supervisor: Dr. Unni Narayanan)
University of Toronto, Graduate Department of Rehabilitation Science
Dr. Simon Kelley Investigator
Division of Orthopaedic Surgery, The Hospital for Sick Children
416-813-6435
Catharine Bradley Investigator
Division of Physiotherapy, The Hospital for Sick Children
416-813-8414
Dr. Nancy Salbach Investigator
Graduate Department of Rehabilitation Science
The University of Toronto
416-946-8558
Purpose of the Research: The purpose of this study is to help us understand how your orthopaedic condition affects your
daily life. We want to know what aspects of your condition concern or bother you, if at all, and
what goals you might wish from the treatments that you have received, or might receive in the
future. This will help guide treatments (including surgery) by identifying the goals that are most
important to you, and also help us measure whether our treatments actually achieve those goals.
Description of the Research: This study involves one meeting with a researcher that may take place the same day as a regular
clinic visit. If this is not convenient, you can still participate in the study. A researcher will work
with you to find a good time to follow-up by telephone or have you return to the hospital,
whichever you prefer.
For part 1 of this study, you will be asked to complete a questionnaire called the Gait Outcomes
Assessment List (GOAL). You will be asked how important each question is to you as a goal,
90
and if there is anything important that you feel is missing. This will take about 30 minutes of
your time.
If you choose to participate in part 2 of this study, you will be interviewed by a researcher who
will ask you questions about what you did and did not like or understand about the GOAL and
how we could make it a better questionnaire. This interview will be recorded, if you agree to this
(separate consent form required). Part 2 of this study will take approximately 30 minutes to
complete.
A review of your medical chart will be conducted to confirm your exact leg condition and
medical history.
Potential Harms: This study will not help or harm you in anyway. We know of no harm that taking part in this
study could cause you, other than the inconvenience of the time you spend completing it.
Potential Discomforts or Inconvenience:
Participation in the study will require between 30-60 minutes of your time.
Potential Benefits:
To individual subjects:
There will be no direct benefit for taking part in this study. However, your participation would be
most valuable and much appreciated. We might learn something new about how your condition
concerns you that your doctor might not know. If so, we will ask you whether we can share that
information with your doctor to help you with that problem.
To society:
We hope that this study will help other children in the future who have leg conditions that change
how they walk. The results may lead to a better way to measure the impact of these conditions on
their daily lives and help us to make decisions about which treatments to choose to address their
goals, by better understanding of which treatments are most likely to achieve these goals.
Confidentiality: We will respect your privacy. No information about who you are will be given to anyone or be
published without your permission, unless the law makes us do this.
For example, the law could make us give information about you
If a child has been abused
If you have an illness that could spread to others
If you or someone else talks about suicide (killing themselves), or
If the court orders us to give them the study papers
Sick Kids Clinical Research Office Monitor or the regulator of the study may see your health
record to check on the study. By signing this consent form, you agree to let these people look at
your records. We will put a copy of the signed research consent form in your health record and
provide you with a copy for your own records.

91
The data produced from this study will be stored in a secure, locked location. Only members
of the research team (and maybe those individuals described above) will have access to the data.
Following publication of the results of this study, data will be kept for 7 years then destroyed as
required by Sick Kids policy. Published study results will not reveal your identity.
Reimbursement: If your participation in this study requires any additional visits to the hospital, we will reimburse
your family for parking costs.
In recognition of your time and effort you will receive a $20 gift card to either Chapters/Indigo or
iTunes.
Participation: It is your choice to take part in this study. You may choose to complete Part 1 or Part 1 and 2 of
this study. You can stop at any time. The care you get at Sick Kids will not be affected in any
way by whether you take part in this study.
Sponsorship:
This research is funded through a University of Toronto Fellowship.
Conflict of Interest:
I, and the other research team members have no conflict of interest to declare.
Consent :
By signing this form, I agree that:
1) You have explained this study to me. You have answered all my questions.
2) You have explained the possible harms and benefits (if any) of this study.
3) I understand that I have the right not to take part in the study and the right to stop at any
time. My decision about taking part in the study will not affect my health care at Sick Kids.
4) I am free now, and in the future, to ask questions about the study.
5) I have been told that my medical records will be kept private except as described to me.
6) I understand that no information about who I am will be given to anyone outside of this
study or be published without first asking my permission.
7) I agree, or consent, to take part in this study.
I would like to be in Part 1 of this study. _______________________
Yes No Signature/ Date
I would like to be in Part 2 of this study. _____________________
Yes No Signature/Date
Printed Name of Subject & Age

92
_
______________________________
Printed Name of person who explained consent Signature of Person who explained
consent & date
_____________________________________________ _____________________________
Printed Witness’ name (if the subject/legal guardian Witness’ signature & date
does not read English)
If you have questions about your

93
Appendix 5. Determination of Child’s Capacity to Consent
Prior to seeking consent the researcher will determine if the child is capable of providing consent.
The researcher is an experienced paediatric clinician with experience determining capacity for
consent to treatment.
Assent will be sought for incapable children. Consent for these children will be sought from their
accompanying parent/guardian.
Process
Review the information letter and study details in conversation with both the child and parent
Encourage and answer all questions and re -explain any information that is not clear.
Through this conversation determine the child’s capacity. Questions to help assess capacity may
include:
o Who can be a part of this study?
o What will you do in the study? What else? Do you want to do all these things?
o What if you start and decide you don’t want to do it anymore?
o Who will know what you say?
o Why do you think we are doing this study?
o Will I use your name when I write a report?
o Do you have to do this?
o Will taking part hurt you in any way?
o Who can tell you more if you have questions?
Note , an ‘incorrect’ answer will not necessarily be construed as incapacity but will cue the
researcher to re-explain and reassess.

94
Appendix 6- Research Ethics Board Approval

95
Appendix 7. Research Ethics Board Approval- Holland Bloorview

96
Appendix 8. University of Toronto Study Approval

97
Appendix 9. Information Sheet
If you need help, your parents can help you complete this form.
Date: ______________________
Male: ☐ Female: ☐
Age: ____________
Diagnosis: __________________
Which side? Left: ☐
Right: ☐ Both:☐
Have you previously had surgery
related to your legs? Yes: ☐
No: ☐
If yes, please describe____________________
__________________________________________
Do you currently:
Use an ankle foot orthosis (AFO)? Yes: ☐ No: ☐
Wear a shoe lift? Yes: ☐ No: ☐
Use any walking aid (i.e. cane) Yes: ☐ No: ☐

98
Appendix 10. Cognitive Interview Guide
Thank you for agreeing to complete the GOAL and to give me feedback on what you think of this
questionnaire and how we can make it better. Your feedback will help make sure the GOAL asks
questions that are meaningful and important to you and that the wording of the instructions, the
questions, and the answer scale are very clear and easy to understand.
Task 1: Questionnaire completion
Please use the black pen to complete every item of the questionnaire. As you read each question,
if there are any words or sentences that you do not completely understand, please highlight these
words or sentences with the provided highlighter. If there is anything you would like me to
explain, please ask. If there is anything you would like to share your thoughts on, for example
something you really like or don’t like, let me know, either right away as you think of it, or circle
it and we can talk about it at the end, when you are finished the questionnaire. If you have any
other ideas that you think should be included in this questionnaire, please write these on the last
page of the questionnaire.
Notes: Task 2: Instructions
Let’s look at the 4 instructions at the top of page 1.
Are these easy to understand? Notes: What does the word ‘mobility’ mean to you? Notes: Let’s look at the instructions at the top of page 2.
In your own words can you explain what is being asked of you? Notes: What does the phrase “usually” mean to you?
Task 3: Scale
Let’s take a look at the possible answers listed across the top of page 3.
There are 7 choices ranging from extremely difficult/impossible (0) to no problem at all (6).
Did you feel you were able to find your answer in the list of possible answers listed?
Do you think there are too many options, not enough options, or is it just right? (if they answer
too many or not enough, how would you change it?)

99 Notes: How would you describe the difference between’ very difficult’ and ‘extremely difficult’? Notes: Now let’s look at the importance rating scale on this page. There are 5 choices ranging from ‘not
a goal’ to ‘extremely important’.
Are there too many options, not enough options, or is it just right? (if too many or not enough,
how would they change it) Notes: Let’s look at the scale on page 5. Notice that this now includes a new column, “I did not do this
activity in the past 4 weeks”.
Do you think this is a good or bad option to include in the scale? Why? Notes: Now let’s look at page 7. This scale is asking about your feelings. You have 5 choices from
very (0) unhappy to (4) very happy.
Are there too many options, not enough options, or is it just right? (if too many or not enough,
how would you change it?) Notes: In your own words what does “neither happy nor unhappy” mean to you? Notes: Task 4: Items
Section A: Let’s take a look at page 2.
Can you read #7 aloud? (note words of
difficulty)_____________________________________________________________________________ Can you ask the same question in your own words? Notes: The question lists “toy, doll, book, cellphone” as examples. Can you think of other examples that
you might use? Notes: Look at the next question (#8).
What does the word “manually” mean to you? Notes: Take another look at all the questions in section A.
Are there any questions that you don’t think belong in this section? Notes: Are there any questions that you would get rid of completely from this questionnaire? Notes: Is there anything you would add to this section? Notes:

100
Section B: Let’s look at page 3.
Can you read #11 aloud? (note words of
difficulty)_________________________________________________________________________
Do you feel you understand a distance of 250 m? Notes: Now Compare #11 to #14.
Explain to me the difference between these questions. Notes: Read the next question (#15).
Is there a different way to say this? Notes: Which way do you prefer?
__________________________________________________________________
Take another look at all the questions in section B.
Are there any questions that you don’t think belong in this section? Notes: Are there any questions that you would get rid of completely from this questionnaire? Notes: Is there anything you would add to this section? Notes: Section C: Let’s look at page 4.
Explain to me the difference between pain and discomfort. Notes: Can you read #27 aloud? (note words of
difficulty)___________________________________________________________________________ Is there a different way to say this? Notes: Which way do you prefer?
__________________________________________________________________
This section asks about pain/discomfort in 5 different parts of your body.
Is it easy for you to think about each of these body parts separately? Notes: Would organize or ask this group of questions any other way? Notes: Take another look at all the questions in section C.

101
Are there any questions that you don’t think belong in this section? Notes: Are there any questions that you would get rid of completely from this questionnaire? Notes: Is there anything you would add to this section? Notes: Section D: Let’s look at page 5.
Can you read #30 aloud for me? (note words of
difficulty)______________________________________________________________
What does the word ‘participating’ mean to you? Notes: What does the word ‘gliding’ mean to you? Notes: Is there another way to ask this question? Notes: Look at #33.
Is there another way to ask this question? Notes: Take another look at all the questions in section D
Are there any questions that you don’t think belong in this section? Notes: Are there any questions that you would get rid of completely from this questionnaire? Notes: Is there anything you would add to this section? Notes: Section E: Let’s look at page 6.
Look at #41.
How else could you ask this question? Notes: Look at the last line at the bottom of the page.
What does the word “aspect” mean? Notes: Is there a different word that you would use? Notes: Take another look at all the questions in section E.
Are there any questions that you don’t think belong in this section?

102 Notes: Are there any questions that you would get rid of completely from this questionnaire? Notes: Is there anything you would add to this section? Notes: Section F: Let’s look at the top of page 7.
Are there any questions that you don’t think belong in this section? Notes: Are there any questions that you would get rid of completely from this questionnaire? Notes: Is there anything you would add to this section? Notes: Section G: Let’s look at the bottom of page 7.
Can you read #47 aloud for me? (note words of
difficulty)__________________________________________
What do you think “symmetry” means? Notes: Would you ask this question(#47) any differently? Notes: Can you read #48 aloud for me?
How would you ask this question in your own words? Notes: Take another look at all the questions in section G.
Are there any questions that you don’t think belong in this section? Notes: Are there any questions that you would get rid of completely? Notes: Is there anything you would add to this section? Notes: Task 5: General How do you feel about the amount of time it took you to complete the GOAL? Notes: How easy or difficult did you find the GOAL to answer? Notes:

103
There are two purposes of the GOAL. One is to measure the impact of your leg condition on
your daily life…how well do you think the GOAL does this? Notes: And two is to highlight the areas you think are most important and would like to change…how
well do you think the GOAL does this? Notes: Do you think if your leg condition was corrected your answers would look very different? Notes: Is there anything else you can think of that would make this questionnaire better? Notes:

104
Appendix 11. Cognitive Pretesting Model
From Woolley, Bowen, Bowen, 2004, informed by DeMaio & Rothgeb (1996), Jobe & Mingay (1989), and Tourangeau, Rips, &
Rasinski, (2000).
For response options:
1. “Tell me what this means to you”
2. “Is there a different way to word this?”
3. “Do you feel there are enough/not enough options?”
For items:
1. “Will you please read the question aloud?” *
2. “Is there a different way to word this?”
3. “Do you feel you can give a good answer to that question?”
4. “Why did you pick your answer?” **
Upon completion of the questionnaire:
1. “How can we make this questionnaire better?”
2. “Do you feel there are questions too much the same?”
3. “What do you think of the length of this questionnaire?”
4. “How do you feel about the response options? Clear? Enough/not enough options?”
5. “Are the instructions clear?”
6. “Is there anything else you’d like to share?”
* Make special note of any words that children may have difficulty with.
**Any time that ‘not applicable’ is chosen, ask and record the reason for this (i.e.,
developmentally inappropriate? are they not allowed?)

105
Appendix 12. Information Letter for Healthcare Professionals
Date
Dear name of health care professional
We are writing to ask for your help in a study being conducted at SickKids and Holland
Bloorview that looks at the impact of certain orthopaedic conditions on children’s everyday life.
We want to better understand the concerns and experiences of children who have an orthopaedic
condition that affects how they walk. This will help guide treatments by identifying the goals
that are most important to them, and also help us measure whether our treatments actually
achieve those goals.
For this study you will be asked to review a questionnaire called the Gait Outcomes Assessment
List (GOAL). The Gait Outcomes Assessment List (GOAL©) has been identified as a candidate
measure to evaluate the impact of lower limb anomalies on the daily life of these children and the
effectiveness of interventions in eliciting functional change. The GOAL© was initially
developed for a pediatric ambulatory cerebral palsy population (GMFCS level I-III), to evaluate
children’s and parents’ priorities for gait interventions, as no existing outcome measure was
found appropriate for this purpose. The GOAL was developed within the context of a randomized
trial evaluating the impact of gait analysis for surgical decision making on functional outcomes
following multi-level orthopaedic surgery for children with ambulatory cerebral palsy. The
instrument was developed with a view to broadening its application to any childhood condition
associated with gait differences.
Phase one of this study consists of a content evaluation in the context of pediatric lower limb
deformities, deficiencies, and/or length discrepancies. Based on feedback from children with
lower limb anomalies and their parent(s), and cognitive debrief interviews with children a new
module of the GOAL has been created specific to orthopaedic lower limb anomalies. At this
point we are requesting input from health care professionals from different disciplines
(orthopaedic surgeons, physiotherapists, orthotists, prosthetists, etc.) who have experience in the
care of these children. For each item you will be asked to ‘Accept’, ‘Accept with modification’,
or ‘Reject’. Additionally, we would like to know if there is anything important that you feel is
missing. Participation is expected to take about 30 minutes. The survey will be conducted

106
electronically via FluidSurveys. Consent to participate will be implied by completion of the
survey.
Participation in this research is voluntary but your participation would be most valuable and
much appreciated. Even if you choose to participate in this study, you can withdraw from the
study at any time. Your privacy will be respected and all information about you will remain
confidential. You will not be identified in any presentations or publications without your
permission.
You may also contact us anytime at (416) 813-6755, x48 or by e-mail at
[email protected] to let us know if you have any questions or concerns.
Thank you for taking the time to read this information. This study is an important one and your
contributions are extremely valuable.
Sincerely,
Unni G. Narayanan, MBBS, Msc, FRCS(C)
Pediatric Orthopaedic Surgeon
The Hospital for Sick Children
Simon Kelley, MBChB, FRCS
Pediatric Orthopaedic Surgeon
The Hospital for Sick Children
Virginia Wright PhD
Co-Principal Investigator
Holland Bloorview Kids Rehabilitation Hospital
Phone: 416-425-6220 ext. 35xx
Jennifer Dermott BSc(Kin), BSc(PT), MSc(c)
Physiotherapist
The Hospital for Sick Children
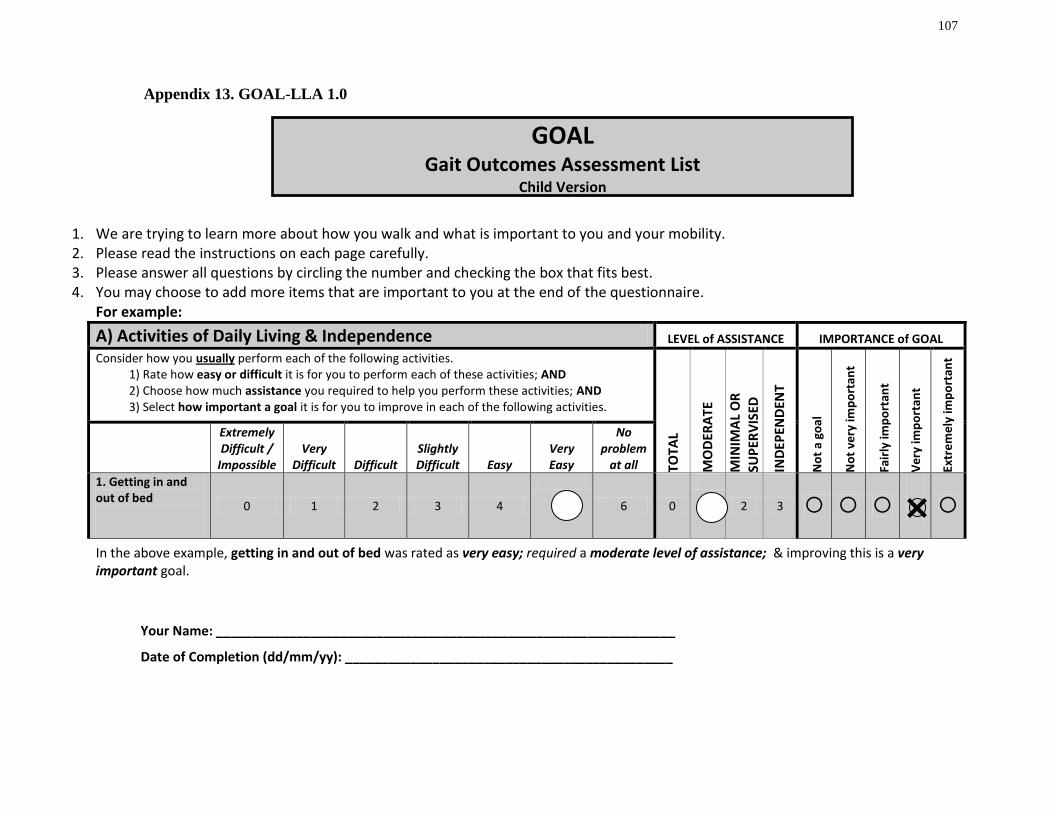
107
Appendix 13. GOAL-LLA 1.0
1. We are trying to learn more about how you walk and what is important to you and your mobility. 2. Please read the instructions on each page carefully. 3. Please answer all questions by circling the number and checking the box that fits best. 4. You may choose to add more items that are important to you at the end of the questionnaire.
For example:
A) Activities of Daily Living & Independence LEVEL of ASSISTANCE IMPORTANCE of GOAL
Consider how you usually perform each of the following activities. 1) Rate how easy or difficult it is for you to perform each of these activities; AND 2) Choose how much assistance you required to help you perform these activities; AND 3) Select how important a goal it is for you to improve in each of the following activities.
TOTA
L
MO
DER
ATE
MIN
IMA
L O
R
SUP
ERV
ISED
IND
EPEN
DEN
T
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
Extremely Difficult /
Impossible Very
Difficult Difficult Slightly Difficult Easy
Very Easy
No problem
at all
1. Getting in and out of bed
0 1 2 3 4
6 0
2 3
In the above example, getting in and out of bed was rated as very easy; required a moderate level of assistance; & improving this is a very important goal.
Your Name: _______________________________________________________________
Date of Completion (dd/mm/yy): _____________________________________________
5 1
GOAL Gait Outcomes Assessment List
Child Version

108
A) Activities of Daily Living & Independence LEVEL of ASSISTANCE IMPORTANCE of GOAL
Consider how you usually perform each of the following activities. 1) Rate how easy or difficult it is for you to perform each of these activities; AND 2) Choose how much assistance you required to help you perform these activities; AND 3) Select how important a goal it is for you to improve in each of the following activities.
TOTA
L
MO
DER
ATE
MIN
IMA
L O
R
SUP
ERV
ISED
IND
EPEN
DEN
T
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
Extremely Difficult /
Impossible Very
Difficult Difficult Slightly Difficult Easy Very Easy
No problem
at all
1. Getting in and out of bed
0 1 2 3 4 5 6 0 1 2 3
2. Getting in and out of a chair (or wheelchair)
0 1 2 3 4 5 6 0 1 2 3
3. Standing at a sink or counter
0 1 2 3 4 5 6 0 1 2 3
4. Washing/bathing myself (eg. shower or tub)
0 1 2 3 4 5 6 0 1 2 3
5. Putting your pants on one leg at a time while standing
0 1 2 3 4 5 6 0 1 2 3
6. Carrying heavy objects while walking (eg. grocery bags, school books)
0 1 2 3 4 5 6 0 1 2 3
7. Balancing objects while walking (e.g. a cup of hot chocolate, a tray of food)
0 1 2 3 4 5 6 0 1 2 3
8. Opening a door
0 1 2 3 4 5 6 0 1 2 3
9. Picking up an object off the floor
0 1 2 3 4 5 6 0 1 2 3
10. Getting in and out of a vehicle (eg. car, van or bus)
0 1 2 3 4 5 6 0 1 2 3

109
B) Function & Mobility WALKING AID REQUIRED IMPORTANCE of GOAL
Consider how you usually perform each of the following activities. 1) Rate how easy or difficult it is for you to perform each of these activities; AND 2) Choose what walking aid you required to help you perform these activities; AND 3) Select how important a goal it is for you to improve in each of the following activities.
WH
EELC
HA
IR
WA
LKER
TWO
CA
NES
OR
CR
UTC
HES
O
NE
CA
NE
/CR
UTC
H/H
AN
D
SUP
PO
RT/
RA
ILIN
G
OR
WA
LL
IND
EPEN
DEN
T
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
Extremely Difficult /
Impossible Very
Difficult Difficult Slightly Difficult Easy
Very Easy
No problem
at all 11. Walking for more than 250 meters (around 2 blocks or 2 football fields)
0 1 2 3 4 5 6 0 1 2 3 4
12. Getting around at school (indoors)
0 1 2 3 4 5 6 0 1 2 3 4
13. Getting around in crowded spaces (e.g. a concert or special event, the mall)
0 1 2 3 4 5 6 0 1 2 3 4
14. Standing in long lineups
0 1 2 3 4 5 6 0 1 2 3 4 15. Walking for more than 15 minutes
0 1 2 3 4 5 6 0 1 2 3 4
16. Keeping up with my friends while walking outdoors
0 1 2 3 4 5 6 0 1 2 3 4

110
17.Moving quickly if I am in a hurry (eg. to catch a bus, late for school)
0 1 2 3 4 5 6 0 1 2 3 4
18. Stepping around or avoiding obstacles
0 1 2 3 4 5 6 0 1 2 3 4
19. Going up and down stairs
0 1 2 3 4 5 6 0 1 2 3 4
20. Going up and down slopes
0 1 2 3 4 5 6 0 1 2 3 4 21. Walking on uneven ground (rough, rocky, sandy)
0 1 2 3 4 5 6 0 1 2 3 4
22. Walking on slippery surfaces (wet or icy)
0 1 2 3 4 5 6 0 1 2 3 4

111
C) Pain / Discomfort / Fatigue INTENSITY IMPORTANCE of GOAL
Consider each of the following items. 1) Rate how often you experienced pain or discomfort or tiredness in the past 4 weeks; AND 2) Choose how severe the pain or discomfort was; AND 3) Select how important a goal it is for you to reduce pain or discomfort or tiredness in each of the following.
SEV
ERE
MO
DER
ATE
MIL
D
NO
NE
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
im
po
rtan
t
During the past 4 weeks:
Every Day
Very Often
(nearly every day)
Fairly Often (2 to 3 times a week)
A Few Times
(once a week)
Once or Twice
None of the Time
23. Pain or discomfort in my feet or ankles
0 1 2 3 4 5 0 1 2 3
24. Pain or discomfort in my knees
0 1 2 3 4 5 0 1 2 3
25. Pain or discomfort in my thighs or hips
0 1 2 3 4 5 0 1 2 3
26. Pain or discomfort in my back
0 1 2 3 4 5 0 1 2 3
27. Feeling tired while walking
0 1 2 3 4 5 0 1 2 3
28. Feeling tired during any other physical activities that I usually enjoy (eg. swimming, running, horseback riding or other sport)
0 1 2 3 4 5 0 1 2 3
Other pain:
(please specify)
0 1 2 3 4 5 0 1 2 3

112
D) Physical Activities, Games & Recreation IMPORTANCE of GOAL
Consider how you usually perform each of the following activities. 1) Rate how easy or difficult it is for you to perform each of these activities; AND 2) Select how important a goal it is for you to improve in each of the following activities.
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
Extremely Difficult /
Impossible
Very Difficult Difficult
Slightly Difficult Easy
Very Easy
No problem
at all
I have never tried this activity
29. Running
0 1 2 3 4 5 6
30. Participating in gliding sports (eg. skating, rollerblading, skiing, skate/snowboarding)
0 1 2 3 4 5 6
31. Riding a bicycle
0 1 2 3 4 5 6
32. Swimming
0 1 2 3 4 5 6
33. Participating in sports that require running (eg. soccer, baseball, football, track)
0 1 2 3 4 5 6
34. Participating in sports that require jumping (eg. basketball, volleyball)
0 1 2 3 4 5 6
35. Participating in dance or martial arts (eg. karate, judo, taekwondo)
0 1 2 3 4 5 6
36. Climbing (eg. ladder or stepstool) 0 1 2 3 4 5 6
Other recreational or sporting activity:
(please specify)
0 1 2 3 4 5 6

113
E) Appearance IMPORTANCE of GOAL
Consider each of the following items. 1) Rate how much of a problem you experience with each of the following in the past 4 weeks; AND 2) Select how important a goal it is for you to improve in each of the following.
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
im
po
rtan
t
During the past 4 weeks:
Extremely Difficult /
Impossible Very
Difficult Difficult Slightly Difficult Easy
Very Easy
No problem
at all 37. Walking with my feet flat on the ground
0 1 2 3 4 5 6
38. Walking taller or more upright (less crouched or bent at the knees)
0 1 2 3 4 5 6
39. Walking with my feet pointing straight ahead
0 1 2 3 4 5 6
40. Walking without dragging my feet
0 1 2 3 4 5 6
41. Walking without tripping and falling
0 1 2 3 4 5 6
42. Walking straight and level (less leaning to the side)
0 1 2 3 4 5 6
Other aspect of my walking:
(please specify)
0 1 2 3 4 5 6

114
F) Use of Braces and Assistive Devices IMPORTANCE of GOAL
Consider each of the following items. 1) Rate how you felt about using each of the following in the past 4 weeks; AND 2) Select how important a goal it is for you to reduce or eliminate your use of these devices.
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
During the past 4 weeks: Very
Unhappy Unhappy
Neither Happy
nor Unhappy Happy
Very Happy
43. Wearing braces or orthotics (eg. shoelift, AFO)
0 1 2 3 4
I have not been given a lift or brace
44. Using a walking aide (eg. walker, stick, cane, crutches)
0 1 2 3 4
I have not been given a walking aid

115
G) Body Image & Self-Esteem IMPORTANCE of GOAL
Consider each of the following items. 1) Rate how you felt about each of the following in the past 4 weeks; AND 2) Select how important a goal it is for you to improve in each of the following.
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
im
po
rtan
t
During the past 4 weeks:
Very Unhappy Unhappy
Neither Happy nor Unhappy Happy Very Happy
45. The shape and position of my legs
0 1 2 3 4 ☐ ☐ ☐ ☐ ☐ 46. The shape and position of my feet
0 1 2 3 4 ☐ ☐ ☐ ☐ ☐ 47. The symmetry of my legs (in length and size)
0 1 2 3 4 ☐ ☐ ☐ ☐ ☐ 48,Wearing my choice of clothing (eg. shorts, skirts, bathing suits)
0 1 2 3 4 ☐ ☐ ☐ ☐ ☐
49.Wearing my choice of footwear (sandals, heeled boots/shoes)
0 1 2 3 4 ☐ ☐ ☐ ☐ ☐
50. The way I get around compared with others 0 1 2 3 4 ☐ ☐ ☐ ☐ ☐ 51. The way others feel about how I get around
0 1 2 3 4 ☐ ☐ ☐ ☐ ☐ 52. How I am treated by others
0 1 2 3 4 ☐ ☐ ☐ ☐ ☐

116
Other Goals IMPORTANCE of GOAL
If there are any other goals (long or short term) that we have missed, please list them below AND Select how important a goal it is for you to improve in each.
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
Other Goals:
1.
2.
3.
4.
5.
Comments & Suggestions
Thank You

117
Appendix 14. GOAL-LLA 1.1
1) We are trying to learn more about you and any goals you may have for treatment of your leg condition 2) Please read the instructions on each page carefully 3) Please answer all questions by circling the number and checking the box that fits best 4) You may choose to add more items that are important to you at the end of the questionnaire
For example:
A) Activities of Daily Living & Independence LEVEL of ASSISTANCE IMPORTANCE of GOAL
Consider how you usually perform each of the following activities. 1) Rate how easy or difficult it was for you to perform each of these activities over the past 4 weeks; AND 2) Choose how much assistance you required to help you perform these activities; AND 3) Select how important a goal it is for you to improve in each of the following activities.
TOTA
L
MO
DER
ATE
MIN
IMA
L O
R
SUP
ERV
ISED
IND
EPEN
DEN
T
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
Impossible l l l l l l
No problem
at all l
3. Balancing objects while walking (e.g., a cup of hot chocolate, a tray of food)
0 1 2 3
5 6 0 1 2
In the above example, usual performance for ‘balancing objects while walking ‘ is rated 4 out of 6; requires no assistance; and improving this is a fairly important goal.
Your Name: _______________________________________________________________
Date of Completion (dd/mm/yy): _____________________________________________
GOAL-LLA Gait Outcomes Assessment List (for Children with Lower Limb Anomalies)
Child Version
4 3

118
A) Activities of Daily Living & Independence LEVEL of ASSISTANCE IMPORTANCE of GOAL
Consider how you usually perform each of the following activities. 1) Rate how easy or difficult it was for you to perform each of these activities in the past 4 weeks; AND 2) Choose how much assistance you required to help you perform these activities; AND 3) Select how important a goal it is for you to improve in each of the following activities.
TOTA
L
MO
DER
ATE
MIN
IMA
L O
R
SUP
ERV
ISED
IND
EPEN
DEN
T
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
During the past 4 weeks:
Impossible l l l l l l
No Problem
At All l
1. Carrying heavy objects while walking (e.g., grocery bags, several school books)
0 1 2 3 4 5 6 0 1 2 3
2. Balancing objects while walking (e.g., a cup of hot chocolate, a tray of food)
0 1 2 3 4 5 6 0 1 2 3
3. Opening a door 0 1 2 3 4 5 6 0 1 2 3 4. Picking up an object off the floor
0 1 2 3 4 5 6 0 1 2 3 5. Getting in and out of a vehicle (e.g., car, van or bus)
0 1 2 3 4 5 6 0 1 2 3

119
B) Gait Function & Mobility WALKING AID REQUIRED IMPORTANCE of GOAL
Consider how you usually perform each of the following activities. 1) Rate how easy or difficult it was for you to perform each of these activities in the past 4 weeks; AND 2) Choose how much assistance you required to help you perform these activities; AND 3) Select how important a goal it is for you to improve in each of the following activities.
WH
EELC
HA
IR
WA
LKER
TWO
CA
NES
OR
CR
UTC
HES
ON
E C
AN
E /C
RU
TCH
/HA
ND
SUP
PO
RT/
RA
ILIN
G O
R W
ALL
IND
EPEN
DEN
T
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
During the past 4 weeks:
Impossible l l l l l l
No problem
at all l
6. Walking for more than 250 meters (around 2 blocks or 2 football fields)
0 1 2 3 4 5 6 0 1 2 3 4
7. Getting around at school (indoors) 0 1 2 3 4 5 6 0 1 2 3 4
8. Getting around in crowded spaces (e.g., a concert or special event, the mall)
0 1 2 3 4 5 6 0 1 2 3 4
9. Standing in long lineups
0 1 2 3 4 5 6 0 1 2 3 4 10. Keeping up with friends
0 1 2 3 4 5 6 0 1 2 3 4 11. Moving quickly when in a hurry (e.g., to catch a bus, late for an important event)
0 1 2 3 4 5 6 0 1 2 3 4

120
B) Gait Function & Mobility- continued WALKING AID REQUIRED IMPORTANCE of GOAL
Consider how you usually perform each of the following activities. 1) Rate how easy or difficult it was for you to perform each of these activities in the past 4 weeks; AND 2) Choose how much assistance you required to help you perform these activities; AND 3) Select how important a goal it is for you to improve in each of the following activities
WH
EELC
HA
IR
WA
LKER
TWO
CA
NES
OR
CR
UTC
HES
ON
E C
AN
E /C
RU
TCH
/HA
ND
SUP
PO
RT/
RA
ILIN
G O
R W
ALL
IND
EPEN
DEN
T
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
During the past 4 weeks:
Impossible l l l l l l
No problem
at all l
12. Stepping around or avoiding obstacles
0 1 2 3 4 5 6 0 1 2 3 4
13. Going up and down stairs 0 1 2 3 4 5 6 0 1 2 3 4
14. Going up and down slopes
0 1 2 3 4 5 6 0 1 2 3 4 15. Walking on uneven ground (rough, rocky, sandy)
0 1 2 3 4 5 6 0 1 2 3 4
16. Walking on slippery or icy surfaces
0 1 2 3 4 5 6 0 1 2 3 4
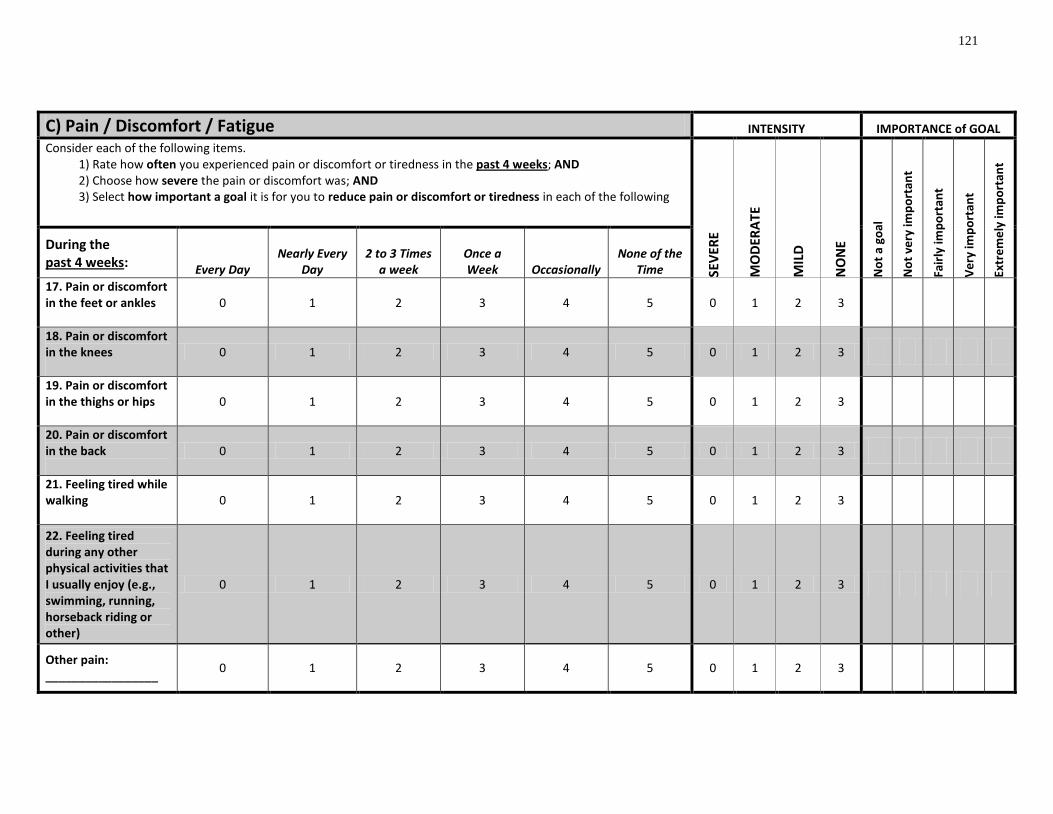
121
C) Pain / Discomfort / Fatigue INTENSITY IMPORTANCE of GOAL
Consider each of the following items. 1) Rate how often you experienced pain or discomfort or tiredness in the past 4 weeks; AND 2) Choose how severe the pain or discomfort was; AND 3) Select how important a goal it is for you to reduce pain or discomfort or tiredness in each of the following
SEV
ERE
MO
DER
ATE
MIL
D
NO
NE
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
During the past 4 weeks:
Every Day Nearly Every
Day 2 to 3 Times
a week Once a Week Occasionally
None of the Time
17. Pain or discomfort in the feet or ankles
0 1 2 3 4 5 0 1 2 3
18. Pain or discomfort in the knees
0 1 2 3 4 5 0 1 2 3
19. Pain or discomfort in the thighs or hips
0 1 2 3 4 5 0 1 2 3
20. Pain or discomfort in the back
0 1 2 3 4 5 0 1 2 3
21. Feeling tired while walking
0 1 2 3 4 5 0 1 2 3
22. Feeling tired during any other physical activities that I usually enjoy (e.g., swimming, running, horseback riding or other)
0 1 2 3 4 5 0 1 2 3
Other pain: _________________
0 1 2 3 4 5 0 1 2 3

122
D) Physical Activities, Games & Recreation IMPORTANCE of GOAL
Consider how you usually perform each of the following activities. 1) Rate how easy or difficult it was for you to perform each of these activities in the past year; AND 2) Select how important a goal it is for you to improve in each of the following activities
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
During the past year:
Impossible l l l l l l
No problem at
all l
I have never tried this activity
23. Running fast
0 1 2 3 4 5 6
24. Participating in gliding sports (e.g., skating, rollerblading, skiing, skate/snowboarding)
0 1 2 3 4 5 6
25. Riding a bicycle
0 1 2 3 4 5 6
26. Swimming
0 1 2 3 4 5 6
27. Participating in sports that require running (e.g., soccer, baseball, football, track)
0 1 2 3 4 5 6
28. Participating in sports that require jumping (e.g., basketball, volleyball)
0 1 2 3 4 5 6
29. Participating in gymnastics, dance or martial arts (eg. karate, judo, taekwondo)
0 1 2 3 4 5 6
30. Climbing (e.g., ladder or stepstool) 0 1 2 3 4 5 6
Other recreational or sporting activity: _________________
0 1 2 3 4 5 6

123
E) Gait Appearance IMPORTANCE of GOAL
Consider each of the following items. 1) Rate how much of a problem you experienced with each of the following in the past 4 weeks; AND 2) Select how important a goal it is for you to improve in each
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
im
po
rtan
t
During the past 4 weeks:
Impossible l l l l l l
No problem
at all l
31. Walking with my feet flat on the ground
0 1 2 3 4 5 6 32. Walking taller or more upright (less crouched or bent at the knees)
0 1 2 3 4 5 6 33. Walking with my feet pointing straight ahead
0 1 2 3 4 5 6 34. Walking without a limp
0 1 2 3 4 5 6 35. Walking without tripping and falling
0 1 2 3 4 5 6 Other aspect of my walking: _________________
0 1 2 3 4 5 6

124
F) Use of Braces and Assistive Devices IMPORTANCE of GOAL
Consider each of the following items. 1) Rate how you felt about using each of the following in the past 4 weeks; AND 2) Select how important a goal it is for you to reduce or eliminate use of these devices
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
During the past 4 weeks:
Very Unhappy
l l l l
Very Happy
l
36. A shoe lift
0 1 2 3 4
☐ I have not been prescribed a
shoe lift
☐ I choose not to wear my shoe
lift
37. A brace (e.g., AFO)
0 1 2 3 4 ☐ I have not been prescribed any
type of brace
☐ I choose not to wear my brace
38. A walking aide (e.g., walker, stick, cane, crutches)
0 1 2 3 4 ☐
I do not use any walking aides
39. A wheelchair
0 1 2 3 4 ☐ I do not use a wheelchair
40. Other assistive devices (e.g., built-up bicycle pedal or _________________)
0 1 2 3 4 ☐
I do not use any other assistive
devices

125
G) Body Image & Self-Esteem IMPORTANCE of GOAL
Consider each of the following items. 1) Rate how you felt about each of the following in the past 4 weeks; AND 2) Select how important a goal it is for you to improve in each of the following
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
During the past 4 weeks:
Very Unhappy
l l l l Very Happy
l 41. The shape and position of my legs
0 1 2 3 4 42. The shape and position of my feet
0 1 2 3 4 43. The symmetry of my legs (in length and size)
0 1 2 3 4 44. Wearing my choice of footwear (e.g., shoes, boots, sandals)
0 1 2 3 4
45. Wearing my choice of clothing (e.g., shorts, skirts, bathing suits)
0 1 2 3 4
46. The appearance of how I get around compared with others
0 1 2 3 4
47. The way others feel about how I get around
0 1 2 3 4 48. How I am treated by others
0 1 2 3 4

126
Other Goals IMPORTANCE of GOAL
If there are any other goals (long or short term) that we have missed, please list them below AND select how important a goal it is for you to improve in each.
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
Other Goals:
1.
2.
3.
4.
5.
Comments & Suggestions
Thank You

127
Appendix 15. Results of the Third Administration of the GOAL (GOAL-LLA 1.1) in Phase 1 (Child
and Parent Perspectives) Children (n = 5) Parents (n=3)
Ability
Score Mean
(range)
Importance
Rating Mean
(range)
Ability
Score Mean
(range)
Importance
Rating Mean
(range)
A) (/6) (/4) (/6) (/4)
Putting your pants on one leg at a time while
standing
5.7 (4-6) 1 (0-4) 5.3 (3-6) 2.1 (0-4)
Carrying heavy objects while walking (e.g.,
grocery bags, school books)
5.4 (2-6) 1 (0-3) 4.7 (3-6) 2.3 (0-4)
Balancing objects while walking (e.g. a cup
of hot chocolate, a tray of food)
5.0 (4-6) 1.0 (0-3) 4.7 (3-6) 2.4 (0-4)
Opening a door 6.0 (6) 0.5 (0-3) 6.0 (6) 1.7 (0-4)
Picking up an object off the floor 6.0 (6) 0.5 (0-3) 5.7 (5-6) 2.0 (0-4)
Getting in and out of a vehicle (e.g., car, van
or bus)
5.9 (5-6) 0.5 (0-3) 5.4 (4-6) 2.0 (0-4)
B) (/6) (/4) (/6) (/4)
Walking for more than 250 meters (around 2
blocks or 2 football fields)
4.0 (2-6) 2.3 (0-4) 4.4 (2-6) 2.9 (0-4)
Getting around at school (indoors) 5.9 (5-6) 1.3 (0-4) 5.1 (3-6) 2.3 (0-4)
Getting around in crowded spaces (e.g. a
concert or special event, the mall)
4.9 (2-6) 1.3 (0-4) 4.6 (2-6) 2.3 (0-4)
Standing in long lineups 4.4 (2-6) 1.8 (0-4) 4.1 (2-6) 2.7 (0-4)
Keeping up with my friends 5.1 (3-6) 1.7 (0-4) 4.1 (2-6) 3.4 (2-4)
Moving quickly if I am in a hurry (e.g., to
catch a bus, late for event)
5.3 (4-6) 1.3 (0-4) 4.1 (3-6) 2.7 (0-4)
Stepping around or avoiding obstacles 5.6 (5-6) 1.2 (0-4) 5.4 (4-6) 1.8 (0-4)
Going up and down stairs 5.9 (5-6) 1.3 (0-4) 5.0 (3-6) 2.3 (0-4)
Going up and down slopes 5.3 (5-6) 1.4 (0-4) 4.7 (3-6) 2.8 (0-4)
Walking on uneven ground (rough, rocky,
sandy)
5.0 (4-6) 1.7 (0-4) 4.1 (3-5) 2.7 (0-4)
Walking on slippery surfaces (wet or icy) 4.9 (3-6) 1.7 (0-4) 3.7 (1-5) 2.7 (0-4)
C) (/5) (/4) (/5) (/4)
Pain or discomfort in my feet or ankles 3.3 (0-5) 1.2 (0-4) 3.1 (0-5) 3.0 (0-4)
Pain or discomfort in my knees 2.3 (0-5) 2.3 (0-4) 2.6 (0-5) 3.2 (0-4)
Pain or discomfort in my thighs or hips 3.4 (0-5) 1.7 (0-4) 3.7 (0-5) 1.3 (0-4)
Pain or discomfort in my back 2.9 (0-5) 2.3 (0-4) 3.7 (0-5) 2.5 (0-4)
Feeling tired while walking 1.9 (0-4) 1.9 (0-4) 2.4 (0-5) 2.8 (0-4)
Feeling tired during any other physical
activities that I usually enjoy (e.g.,
swimming, running, horseback riding or other
sport)
3.4 (0-5) 1.2 (0-4) 3.4 (0-5) 2.6 (0-4)
D) (/6) (/4) (/6) (/4)
Running fast 3.9 (1-6) 1.2 (0-4) 3.0 (0-6) 2.3 (0-3)
Participating in gliding sports (e.g., skating,
rollerblading, skiing, skate/snowboarding)
4.6 (1-6) 1.25 (0-4) 3.8 (1-5) 2.5 (2-3)
Riding a bicycle 5.7 (5-6) 0.2 (0-1) 4.7 (0-6) 2.6 (0-4)
Swimming 5.4 (2-6) 0.3 (0-2) 5.4 (3-6) 2.6 (0-4)
Participating in sports that require running
(e.g., soccer, baseball, football, track)
3.8 (1-5) 1.8 (0-4) 2.6 (1-6) 2.3 (1-4)
Participating in sports that require jumping
(e.g., basketball, volleyball)
4.7 (2-6) 1.5 (0-4) 3.3 (1-6) 2.3 (1-4)
Participating in gymnastics, dance or martial
arts (e.g., karate, judo, taekwondo)
4.0 (1-5) 2.0 (1-4) 3.3 (0-6) 1.6 (0-2)
Climbing (e.g., ladder or stepstool) 5.6 (5-6) 0.8 (0-4) 4.3 (2-6) 2.3 (0-4)
E) (/6) (/4) (/6) (/4)
Walking with my feet flat on the ground 2.1 (0-6) 3.2 (0-4) 1.9 (0-6) 2.7 (0-4)
Walking taller or more upright (less crouched
or bent at the knees)
4.3 (2-6) 1.8 (0-4) 3.7 (1-6) 3.1 (2-4)
Walking with my feet pointing straight ahead 5.1 (3-6) 1.2 (0-4) 4.7 (3-6) 2.4 (0-4)

128
Walking without a limp 5.6 (5-6) 1.0 (0-4) 4.7 (3-6) 2.4 (0-4)
Walking without tripping and falling 5.0 (1-6) 1.0 (0-4) 5.0 (2-6) 2.3 (0-4)
F) (/4) (/4) (/4) (/4)
A shoe lift 1.4 (0-4) 3.5 (3-4)
1.8 (0-4) 3.6 (3-4)
A brace (e.g., AFO) 2.0 (0-4) 4.0 (4) 3.0 (2-4) 2.0 (0-4)
A walking aide (e.g., walker, stick, cane,
crutches)
2.5 (2-3) 4.0 (4) 3.0 (2-4) 3.0 (2-4)
A wheelchair 1.0 (0-2) 4.0 (4) 4.0 (4) 0
Other assistive devices (e.g., built-up bicycle
pedal or ____________)
G) (/4) (/4) (/4) (/4)
The shape and position of my legs 3.0 (0-4) 1.3 (0-4) 2.1 (0-4) 3.0 (0-4)
The shape and position of my feet 3.3 (0-4) 0.8 (0-4) 2.3 (1-4) 2.3 (0-4)
The symmetry of my legs (in length and size) 1.7 (0-4) 2.5 (0-4) 1.1 (0-3) 3.5 (2-4)
Wearing my choice of footwear (e.g., shoes,
boots, sandals)
1.6 (0-4) 3.0 (2-4) 1.6 (0-4) 3.1 (0-4)
Wearing my choice of clothing (e.g., shorts,
skirts, bathing suits)
3.6 (1-4) 0.8 (0-4) 3.1 (2-4) 2.4 (0-4)
The appearance of how I get around
compared with others
3.1 (1-4) 1.0 (0-4) 2.0 (0-4) 3.3 (1-4)
The way others feel about how I get around 3.0 (2-4) 1.3 (0-4) 2.9 (1-4) 2.4 (0-4)
How I am treated by others 3.7 (3-4) 1.0 (0-4) 3.4 (2-4) 2.3 (0-4)

129
Appendix 16. GOAL-LLA 2.0
1) We are trying to learn more about you and any goals you may have for treatment of your leg condition 2) Please read the instructions on each page carefully 3) Please answer all questions by circling the number and checking the box that fits best 4) You may choose to add more items that are important to you at the end of the questionnaire
For example:
A) Gait Function & Mobility WALKING AID REQUIRED IMPORTANCE of GOAL
Consider how you usually perform each of the following activities. 1) Rate how easy or difficult it was for you to perform each of these activities in the past 4 weeks; AND 2) Choose how much assistance you required to help you perform these activities; AND 3) Select how important a goal it is for you to improve in each of the following activities.
WH
EELC
HA
IR
WA
LKER
TWO
CA
NES
OR
CR
UTC
HES
ON
E C
AN
E /C
RU
TCH
/HA
ND
SUP
PO
RT/
RA
ILIN
G O
R W
ALL
IND
EPEN
DEN
T
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
During the past 4 weeks:
Impossible
l l l l l l
No problem at all
l
1. Carrying heavy objects (e.g., grocery bags, several school books) while walking
0 1 2 3 X 5 6 0 1 2 3 X X
In the above example, usual performance for ‘carrying heavy objects ‘ is rated 4 out of 6; requires no walking aid; and improving this is a fairly important goal.
Your Name: _______________________________________________________________
Date of Completion (dd/mm/yy): _____________________________________________
GOAL-LLA Gait Outcomes Assessment List (for Children with Lower Limb Anomalies)
Child Version

130
A) Gait Function & Mobility WALKING AID REQUIRED IMPORTANCE of GOAL
Consider how you usually perform each of the following activities. 1) Rate how easy or difficult it was for you to perform each of these activities in the past 4 weeks; AND 2) Choose how much assistance you required to help you perform these activities; AND 3) Select how important a goal it is for you to improve in each of the following activities.
WH
EELC
HA
IR
WA
LKER
TWO
CA
NES
OR
CR
UTC
HES
ON
E C
AN
E /C
RU
TCH
/HA
ND
SUP
PO
RT/
RA
ILIN
G O
R W
ALL
IND
EPEN
DEN
T
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
During the past 4 weeks:
Impossible
l l l l l l
No problem at all
l
1. Carrying heavy objects (e.g., grocery bags, several school books) while walking
0 1 2 3 4 5 6 0 1 2 3 4
2. Balancing objects (e.g., a cup of hot chocolate, a tray of food) while walking
0 1 2 3 4 5 6 0 1 2 3 4
3. Walking for more than 250 meters/820 feet (around 2 blocks or 2 football fields)
0 1 2 3 4 5 6 0 1 2 3 4
4. Getting around in crowded spaces (e.g., school, a concert or the shopping mall)
0 1 2 3 4 5 6 0 1 2 3 4
5. Standing for a long time (e.g., lineups, queues, parade)
0 1 2 3 4 5 6 0 1 2 3 4

131
A) Gait Function & Mobility- continued WALKING AID REQUIRED IMPORTANCE of GOAL
Consider how you usually perform each of the following activities. 1) Rate how easy or difficult it was for you to perform each of these activities in the past 4 weeks; AND 2) Choose how much assistance you required to help you perform these activities; AND 3) Select how important a goal it is for you to improve in each of the following activities
WH
EELC
HA
IR
WA
LKER
TWO
CA
NES
OR
CR
UTC
HES
ON
E C
AN
E /C
RU
TCH
/HA
ND
SUP
PO
RT/
RA
ILIN
G O
R W
ALL
IND
EPEN
DEN
T
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
During the past 4 weeks:
Impossible l l l l l l
No problem
at all l
6. Keeping up with friends while walking outdoors
0 1 2 3 4 5 6 0 1 2 3 4
7. Stepping around or avoiding obstacles
0 1 2 3 4 5 6 0 1 2 3 4
8. Going up and down stairs 0 1 2 3 4 5 6 0 1 2 3 4
9. Going up and down ramps
0 1 2 3 4 5 6 0 1 2 3 4 10. Walking on uneven ground (rough, rocky, sandy)
0 1 2 3 4 5 6 0 1 2 3 4
11. Walking on wet, slippery or icy surfaces
0 1 2 3 4 5 6 0 1 2 3 4

132
B) Pain / Discomfort / Fatigue INTENSITY IMPORTANCE of GOAL
Consider each of the following items. 1) Rate how often you experienced pain or discomfort or tiredness in the past 4 weeks; AND 2) Choose how severe the pain or discomfort was; AND 3) Select how important a goal it is for you to reduce pain or discomfort or tiredness in each of the following
SEV
ERE
MO
DER
ATE
MIL
D
NO
NE
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
During the past 4 weeks:
Every Day Nearly Every
Day 2 to 3 Times
a week Once a Week Occasionally
None of the Time
12. Pain or discomfort in the feet or ankles
0 1 2 3 4 5 0 1 2 3
13. Pain or discomfort in the lower legs (shin, calf)
0 1 2 3 4 5 0 1 2 3
14. Pain or discomfort in the knees
0 1 2 3 4 5 0 1 2 3
15. Pain or discomfort in the thighs or hips
0 1 2 3 4 5 0 1 2 3
16. Pain or discomfort in the back
0 1 2 3 4 5 0 1 2 3
17. Feeling easily tired during physical activities that I enjoy (e.g., swimming, running, or other sports)
0 1 2 3 4 5 0 1 2 3
Other pain: _________________
0 1 2 3 4 5 0 1 2 3

133
C) Physical Activities, Games & Recreation IMPORTANCE of GOAL
Consider how you usually perform each of the following activities. 1) Rate how easy or difficult it was for you to perform each of these activities in the past year; AND 2) Select how important a goal it is for you to improve in each of the following activities
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
During the past year:
Impossible l l l l l l
No problem at
all l
I have never tried this activity
18. Running fast
0 1 2 3 4 5 6
19. Participating in gliding sports (e.g., skating, rollerblading, skiing, skate/snowboarding)
0 1 2 3 4 5 6
20. Riding a bicycle
0 1 2 3 4 5 6
21. Swimming
0 1 2 3 4 5 6
22. Participating in sports that require running (e.g., soccer, baseball, football, track)
0 1 2 3 4 5 6
23. Participating in sports that require jumping (e.g., basketball, volleyball, trampoline)
0 1 2 3 4 5 6
24. Participating in sports that require balance (gymnastics, dance or martial arts)
0 1 2 3 4 5 6
25. Climbing (ladder, playground equipment, wall climbing)
0 1 2 3 4 5 6
Other recreational or sporting activity: _________________
0 1 2 3 4 5 6

134
D) Gait Appearance IMPORTANCE of GOAL
Consider each of the following items. 1) Rate how much of a problem you experienced with each of the following in the past 4 weeks; AND 2) Select how important a goal it is for you to improve in each
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
im
po
rtan
t
During the past 4 weeks:
Impossible l l l l l l
No problem
at all l
26. Walking with my feet flat on the ground
0 1 2 3 4 5 6 27. Walking taller or more upright (less crouched or bent at the knees)
0 1 2 3 4 5 6 28. Walking with my feet pointing straight ahead
0 1 2 3 4 5 6 29. Walking without a limp
0 1 2 3 4 5 6 30. Walking without tripping and falling
0 1 2 3 4 5 6 Other aspect of my walking: _________________
0 1 2 3 4 5 6

135
E) Use of Braces and Assistive Devices IMPORTANCE of GOAL
Consider each of the following items. 1) Rate how you felt about using each of the following in the past 4 weeks; AND 2) Select how important a goal it is for you to reduce or eliminate use of these devices
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
During the past 4 weeks:
Very Unhappy
l l l l
Very Happy
l
31. A shoe lift
0 1 2 3 4
☐ I have not been prescribed a
shoe lift
☐ I choose not to wear my shoe
lift
32. A brace (e.g., AFO)
0 1 2 3 4 ☐ I have not been prescribed any
type of brace
☐ I choose not to wear my brace
33. A prosthesis (artificial leg) 0 1 2 3 4
☐ I have not been prescribed a
prosthesis
☐ I choose not to wear my
prosthesis
34. A walking aide (e.g., walker, stick, cane, crutches)
0 1 2 3 4 ☐
I do not use any walking aides
35. A wheelchair
0 1 2 3 4 ☐ I do not use a wheelchair
36. Other assistive devices (e.g., built-up bicycle pedal or _________________)
0 1 2 3 4 ☐
I do not use any other assistive
devices

136
F) Body Image & Self-Esteem IMPORTANCE of GOAL
Consider each of the following items. 1) Rate how you felt about each of the following in the past 4 weeks; AND 2) Select how important a goal it is for you to improve in each of the following
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
During the past 4 weeks:
Very Unhappy
l l l l Very Happy
l 37. The shape and position of my legs
0 1 2 3 4 38. The shape and position of my feet
0 1 2 3 4 39. The symmetry of my legs (in length and size)
0 1 2 3 4 40. Wearing my choice of footwear (e.g., shoes, boots, sandals)
0 1 2 3 4
41. Wearing my choice of clothing (e.g., shorts, skirts, bathing suits)
0 1 2 3 4
42. The appearance of how I get around compared with others
0 1 2 3 4
43. The way others feel about how I get around
0 1 2 3 4 44. How I am treated by others
0 1 2 3 4

137
Other Goals IMPORTANCE of GOAL
If there are any other goals (long or short term) that we have missed, please list them below AND select how important a goal it is for you to improve in each.
No
t a
goal
No
t ve
ry im
po
rtan
t
Fair
ly im
po
rtan
t
Ve
ry im
po
rtan
t
Extr
em
ely
imp
ort
ant
Other Goals:
1.
2.
3.
4.
5.
Comments & Suggestions
Thank You

138