
DEVELOPING CHILDREN’S PALLIATIVE CARE IN TWO … · Developing Children’s Palliative Care in...
36
DEVELOPING CHILDREN’S PALLIATIVE CARE IN TWO COUNTRIES - MAHARASHTRA, INDIA AND MALAWI - THOUGH AN INTERNATIONAL NETWORK Mid-Term Review
Transcript of DEVELOPING CHILDREN’S PALLIATIVE CARE IN TWO … · Developing Children’s Palliative Care in...
DEVELOPING CHILDREN’S PALLIATIVE CARE IN TWO COUNTRIES - MAHARASHTRA, INDIA AND MALAWI - THOUGH AN INTERNATIONAL NETWORK Mid-Term Review

Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
1
Contents General Overview of the project ............................................................................................................. 2
Supporting the Development of Children’s Palliative Care in the Maharashtra State in India through an International Network (2010-2015) .................................................................. 5
Executive summary ................................................................................................................................. 5
Background ................................................................................................................................................. 5
Midterm Review Report ........................................................................................................................ 7
Methodology .............................................................................................................................................. 7
Evaluation Findings ................................................................................................................................. 8
Project Design ............................................................................................................................................ 8
Effectiveness of the model of partnership with National association and children’s palliative care expert site .................................................................................................................... 10
Effectiveness of the model of training followed by periodic mentorship ........................ 11
Collaboration between multiple partners and involvement of stakeholders in decision making and planning .......................................................................................................... 11
Effectiveness of Project Expenditure and Sustainability ........................................................ 12
Palliative Care Impact ........................................................................................................................... 13
Monitoring and Evaluation ................................................................................................................. 14
Lessons Learnt ........................................................................................................................................ 14
Feedback for the Future ...................................................................................................................... 15
Supporting the Development of Children’s Palliative Care in Malawi through an International Network (2010-2015) ................................................................................................... 16
1.0 Background .................................................................................................................................. 17
2.0 Overview of method/approach ............................................................................................ 18
3.0 Key findings................................................................................................................................. 18
3.1 General ...................................................................................................................................... 18
3.2 Project Design ......................................................................................................................... 22
3.3 Differences across the sites .............................................................................................. 25
3.4 Quality ....................................................................................................................................... 26
3.5 Training of care providers and skill mix ...................................................................... 27
3.6 Clinical outcomes .................................................................................................................. 29
4.0 Conclusions .................................................................................................................................. 31
5.0 Key Recommendations ............................................................................................................ 31
Appendix 1 – Questions used in semi-structured interviews across all three sites ..... 33
Appendix 2: Breakdown of beneficiaries and guardians that took part in semi structured interviews ........................................................................................................................... 35

Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
2
General Overview of the project In 2010 an advocacy project over five years was approved by the UK Department for International Development (DFID) to develop three new children’s palliative care programmes in hospitals in Malawi and in the Maharashtra region of India, based on model programmes in each country. The overarching objective of the project is to improve the quality of life of children facing HIV and other life-limiting conditions and life-threatening illnesses. The project partners are:
The International Children’s Palliative Care Network (ICPCN), which has
its head office in South Africa. The Palliative Care Association of Malawi (PACAM) and the Indian
Association of Palliative Care (IAPC). The Umodzi Children’s Palliative Care Team at Queen Elizabeth Central
Hospital (Malawi) and the Department of Palliative Care at Tata Memorial Hospital (India).
Help the Hospices UK (HTH). The International children’s Palliative Care Network (ICPCN) designed the project working together with Help the Hospices UK. The funding and overall oversight of the project lies with Help the Hospices and the technical oversight with the ICPCN. In both countries the national hospice and palliative care association, Indian Association of Palliative Care (IAPC) and Palliative Care Association of Malawi (PACAM) were responsible for employing the staff, managing the finances and in-country responsibility for the project. In Malawi the development was based on the Umodzi model developed by the Department of Paediatrics at Queen Elizabeth ll Central Hospital, and now part of the Palliative Care Support Trust. The three development sites selected were the three other Central Hospitals in Malawi- Kamuzu in Lilongwe, Mazuzu in the northern region, and Zomba in the southern region. In Maharashtra the model selected was the Tata Memorial Hospital’s Palliative Medicine Department‘s children’s palliative care programme. India selected three very different hospital programmes. In Lokmanya Tilak Municipal General Hospital at Sion in Mumbai, the project was integrated into the Paediatric HIV Clinic which is a recognized national Centre of Excellence. The second site is at a rural hospital in Jawhar, Thane, linked to four primary health care centres and a community programme. The final site is the Mahatma Ghandi Hospital, a public-private partnership hospital in Navi Mumbai with outreach into the villages.

Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
3
This project brings together partners from South Africa, the UK, Malawi and India to expand children’s palliative care services in Maharashtra state in India and in Malawi. The project results have prompted commitment to children’s palliative care service development above and beyond the original project scope. It demonstrates how international partnerships can inspire and promote others to take on palliative care to meet the huge need for palliative care around the world. Methods The project uses international donor funds to integrate children’s palliative care into existing services in urban and rural settings in both project countries. Each partner brings to the project distinct skills and experience:
As a worldwide network, ICPCN has extensive experience and expertise to draw on in relation to children’s palliative care. ICPCN’s role in the project has been to provide technical expertise and to strengthen and support the two national palliative care associations and local services involved in implementation and care delivery.
The national associations, PACAM and IAPC, have expertise in advocacy and awareness raising at national level in relation to children’s right to palliative care and relief from pain. They also play a key role in identifying opportunities to increase access to children’s palliative care training for health and social professionals.
The palliative care teams at TATA and Queen Elizabeth Hospital are pioneering the development of children’s palliative care in their health settings. The services they provide are models for other centres to follow and they have played a key role in the capacity building of health professionals from other health centres.
Help the Hospices UK has been supporting the development of hospice and palliative care internationally since 2001 through provision of grants and by working with international partners to access funding for palliative care projects. HTH supported partners in this project in the development of a proposal and provides on-going support in project management and reporting.
Results The mix of these skills has seen the following key results:
The development of children’s palliative care services in 6 new settings, 3 in each country, reaching over 1,900 children. These services are integrated into existing services in order to contribute to their sustainability.
The integration of children’s palliative care into health service curricula. In Malawi a training module on children’s palliative care, developed by PACAM, is part of the training programme at the College of Medicine. Palliative care for children is included in the training of nurses. The Maharashtra University of
Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
4
Health Sciences advertises a certificate course on its website and has included a 3-hour session in post graduate programmes.
The inclusion of children’s palliative care in draft palliative care policy. As a result of project activities, children’s palliative care has been included in in a draft Palliative Care Policy for Maharashtra State while in Malawi a section on children’s palliative care has been included in the draft national Palliative Care Policy.
The opportunity for children to have their wishes and feelings listened to. Through structured focus group meetings of children, they have been encouraged to speak openly about their personal experiences. In Malawi the children had the opportunity to meet with the Minister of Health and were promised her support.
The project has also prompted extended impact:
The National Rural Health Mission (in Maharashtra State, India) has committed to a wider programme of palliative care service delivery for both children and adults and is already funding training, staff and services.
District hospitals in Malawi are showing strong interest in developing palliative care services.
Project stakeholders are increasingly seeking extra funding and gifts in kind to support and develop children’s palliative care services.
The collaborative implementation of this project has proved to be a catalyst for further development of palliative care than originally anticipated.

Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
5
Supporting the Development of Children’s Palliative Care in the Maharashtra State in India through an International Network (2010-2015) A Midterm Review
Executive summary ‘Supporting the development of children’s palliative care in the state of Maharashtra, India’, is an initiative which aims to improve the quality of life for children living with life-limiting illness and their families in Maharashtra State in India. Multiple partners like the Indian Association of Palliative Care, Tata Memorial Hospital, the International Children’s Palliative Care Network and the Help the Hospices in the UK are involved and is funded by DFID CSCF. A midterm evaluation of the project was sought to look at both the approach and the impact of the project. Project exhibited a variety of clearly specified aims and objectives like increasing advocacy, increasing skill and knowledge in paediatric palliative care among health care workers, improving access to opioid medications and empowerment of children and their families. The project is operating in 2 sites in Maharastra (Sion Hospital, Jawhar Rural Health Service) and a new site at Mahatma Gandhi Mission Hospital at Navi Mumbai is proposed. The review found that the project is making a significant contribution to palliative care for children in the state of Maharashtra. The project is very well planned and it is being delivered with the help of a very dedicated and trained group of people. The project is well on the track and most milestones in relation to project targets are already achieved for the year 2013. A few recommendations based on feedback given by different stakeholders are a better medical management and end- of- life- care policy and training in the project planning, better coordination and support from the national organization and plan for a long term mentoring and support of the partners. The report is a summary of the findings of midterm review based on combination of questionnaires, interviews, visits and desk research to gather quantitative and qualitative data about various activities of the project.
Background Globally, children account for 6 per cent of all HIV infections, 17 per cent of new infections and 14 per cent of all HIV-related mortality (UNICEF). According to World Child Cancer each year more than 160,000 children die of cancer and in low-income countries typically more than 80% of young cancer victims die from their illness. “Palliative care for children is the active, total care of the child’s body, mind and spirit, and also involves giving care to the family. It begins when the illness is diagnosed and continues regardless of whether a child receives treatment directed at the disease… Effective palliative care requires a broad multidisciplinary approach that includes the family and makes use of available community resources.”- World Health Organization 2002. There are several barriers to the effective provision of CPC (children palliative care):

Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
6
In India at health policy and practice level there is a lack of knowledge and understanding of the real need for palliative care. But with Maharashtra state holding the fourth highest incidence of HIV in India, palliative care needs are extensive. CPC is not written into health, child rights legislation or HIV plans. Furthermore, it is not possible to effectively control and manage pain in children without access to essential pain relieving drugs, including opioids. In Maharashtra, strict licensing rules limit the use of morphine in children. Health and social care training colleges do not include CPC in training curricula and health care professionals are not receiving training in the relief of chronic and acute pain in children, or the effective use of the WHO’s pain ladder. At the national level, palliative care associations in India are already advocating strongly for a change to support palliative care. However, palliative care for children is not currently included in advocacy plans as a specific area for targeting. The centre in Mumbai are pioneering the development of CPC in their settings, yet they remain critically under-resourced in comparison with need, and do not have the capacity to use their knowledge to advocate for change. Focus of the Project ‘Supporting the development of children’s palliative care in the state of Maharashtra, India’, is an initiative which aims to improve the quality of life for children living with life-limiting illness and their families and carers in Maharashtra State in India. Scope of the Project The Indian Association of Palliative Care and Tata Memorial Hospital are the implementing partners for the project. The International Children’s Palliative Care Network provides leadership and guidance on technical aspects of children’s palliative care development and Help the Hospices in the UK maintains project oversight as the lead applicant partner. The project is funded by DFID CSCF. Project term The project started in October 2010 and will conclude in March 2015. Location The project is operating in 2 sites in Maharastra (Sion Hospital, Jawhar Rural Health Service) and a new site at Mahatma Gandhi Mission Hospital at Navi Mumbai is proposed to start by the year 2013. Partner organizations IAPC – Calicut Tata memorial Hospital – Mumbai ICPCN – South Africa Help the Hospices – London, UK. Output 1. National associations in India have increased ability to advocate for CPC (at
state level)
Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
7
2. Health care workers equipped with skills and knowledge to deliver CPC in Maharashtra State, India
3. Greater access to pain relieving medicines for children living with HIV and other life limiting conditions in Maharashtra state
4. Children with life-limiting illness and their families empowered to inform service delivery around the provision of CPC in Maharashtra state
Activities The project is implemented through the following broad activities:
1) Building capacity of the National Association, the Indian association of Palliative Care (IAPC) to advocate for children’s palliative care. The ICPCN and local expert partners Tata Memorial Hospital (TMH) equip the national association with knowledge and understanding of children’s palliative care.
2) The national association and expert partner identify and work with 3 sites to conduct training in children’s palliative care. The sites integrate children’s palliative care into their services, mentored by the project partners.
3) The project partners work with relevant educational bodies to integrate children’s palliative care into health professional training curricula.
4) Awareness activities are conducted to raise profile of children’s palliative care and increase demand for services.
5) Project partners actively working with policy makers and legislators to improve the relevant policy environment for children’s palliative care
6) Support and encouragement in the use of opioids for children 7) Workshops and focus groups held with children attending the services help to
empower and inform them in their health care choices, and also provide valuable feedback to the project.
Midterm Review Report The midterm review of the project was done by a visit to Tata Memorial hospital, Sion Hospital, Jawhar Rural Health Service on 19th to 21st March 2013. The review process involved both the process and impact and outcome evaluation. The specific objectives of the review were:
To assess the extent to which the project objectives are being met
To identify areas for program adjustment or strengthening to ensure objectives can be met by the end of the project.
To ensure mechanisms for sustainability are in place and effective by the end of the project.
To record and share lessons learned
To ensure effectiveness and efficiency in the program design.
Methodology The review plan was developed by the evaluator in collaboration with the project staff and with inputs from Help the Hospice by communication through emails, teleconferencing and phone calls
Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
8
Proper ethical guidelines were followed when conducting the evaluation like informing participants about the purpose of data gathering and how it will be analysed and how the results will be used, ensuring data privacy and confidentiality, obtaining informed consent wherever necessary, when analysing or reporting the qualitative data, being
careful about sensitive comments or those that may reveal personal
identities, obtaining necessary permission when approaching children and institutions (e.g., hospitals), being sensitive to cultural norms and beliefs etc. The following evaluation methods were incorporated in the review process:
Meetings and discussions with project staff
Participant Observation
Desk review and analysis of key documents above
Structured and semi-structured interviews
Focus groups / interviews with beneficiaries
Focus groups / interviews with key stakeholders to provide views and opinions
Review of project progress against objectives
Photographic record Main reference documents were project proposal, log- frame, and annual project reports, including financial information, original baseline study and project quarterly reports
Evaluation Findings General / overall The evaluation found that the project is making a significant contribution to palliative care for children in the state of Maharashtra. The project is very well planned and it is being delivered with the help of a very dedicated and trained group of people. The project is well on the track and most milestones in relation to project targets are already achieved for the year 2013 (LOGFRAME CSCF 521 October 2012). A noteworthy positive impact of the project is evolution of palliative care awareness in general and a possible development of state level palliative care health policy for people living with life-limiting illnesses. “The biggest change which I have noticed is a perceptible change in attitude seen among staff and parents of Sion hospital.”- A social worker of CPC Project ‘Today around 50 children with developmental disorders/ CPs have come for the camp. They won’t have come if it was not felt effective. They feel cared for and they think we care for them. Project may or may not remain but patients and families will always remember us’- A social worker with the out-reach program.
Project Design Lokmanya Tilak Municipal General Hospital, Sion, Mumbai, one of the sites selected for the project is one of the Centers of Excellence in the country for HIV and AIDS in children. The CPC project focuses on a selected group of high-risk children with the eligibility criteria as the following:
Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
9
Orphans
Children developing opportunistic infection
Children receiving 2nd line ART
Children with HIV and TB
Chronically sick
Difficult in schools
Adolescent
Non-adherence The team in ART center consisting of doctors, a nurse, care coordinator, nutritionist, Redressel cell Volunteers and councillors is well sensitized to needs of children and their caregivers and palliative care. The two social workers are trained in palliative care. They are empowered to do focus group meetings of children and their caregivers, identify their problems and discuss with the rest of the team to address the issues. The focus group discussion of children (< 12years and 2-18 years group) and their caregivers are mostly oriented towards
Need assessment
Difficulties faced
Expectations from the services provided
Special needs of Orphans They are also trying to assess the impact of palliative care intervention by administering a QOL questionnaire to the patients. The work is supervised and mentored by regular visits from CPC project team members. A separate case record for palliative care is maintained by the social workers in the centre. Regular orientation of outreach workers and redressal cell workers is also provided during their visits. The team in general is highly motivated. So far, 87 children are enrolled in the CPC project. The vulnerable group who are probably missed out in this project is children who need end of life care for situations like advanced AIDS and other advanced life-limiting illnesses. They are either dying in the homes in the community or are admitted in other parts of the hospitals. As quoted by one of the physicians working in the ART centre, ‘Sometimes we follow up on children when they become very sick and get admitted. Otherwise, doctors in the hospital give the end of life care. We don’t see much pain in the ART centre but not sure what happens to those with advanced diseases. There is no protocol in place as to when to stop ART/ antibiotics or other active treatment.’ A lot of migrant children population are also not getting the continuity of care. In the proposed new site, it is expected that there will be wider coverage of many other life- limiting illnesses in the program. A lot of cultural beliefs and superstition is expressed as a barrier to effective palliative care for children. In Jawhar Cottage Hospital (JCH), children with range of life-limiting illnesses like CP, Developmental disorders, HIV and AIDS, Sickle Cell, Thalassemia and Malnutrition are seen in the community. Many get admitted in the hospital but otherwise they are followed up in their homes in the community until their death. The

Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
10
program in JCH is supported by the government agency called the National Rural Health mission (NRHM). The NRHM is providing the staff support to JCH by hiring a social worker and a doctor. The essential drugs like oral morphine are also bought by the NRHM. There are two trained nurses in JCH who are helping with regular data entering. The ASHA (Accredited Social Health Activist) workers are trained to identify the patients in the villages and to bring them to PHC. ASHA workers are given basic training in palliative care (one day training with a refresher course for a few). They also visit patients in homes. They are provided a basic medicine kit to provide basic nursing care. They are paid by the NRHM based on number of patients identified and brought and number of patients brought for follow up to PHC. ‘The bedridden patients are admitted in JCH. They are treated with drugs like pain- killers and other drugs and are provided health education and nursing care like care of the wound. The families are empowered to take care of the patients. The choice is given to them whether to remain in the hospital or to be cared in the homes.’- A Nurse, trained in palliative care. A regular focus group meetings are held where the stakeholders and beneficiaries come together and discuss and share. In these meetings, the patients and their families are encouraged to express their needs and concerns. ‘I need rest. If someone like a teacher can keep them engaged for a few hours, it will be so good. I feel sorry when see other children going to school and my child cant’ ‘Why don’t you find us a teacher who can spend time with our children’? Last year one teacher used to visit our Anganvadi and used to teach them for 2-3 hours. Children used to enjoy leaning and playing with them. Now that has stopped. We miss their visits’ – Grandmother of a 4 years old child with developmental disorder from Sakershety PHC, enrolled 3 years ago. It is difficult for patients and their families to come for regular follow up to both JCH and to the Sion ART centre as expressed by a couple of caregivers, ‘For each visit we lose our wages. If only the long hours of wait in the centre can be avoided’. ‘Travel to PHCs often require long distance and so much is money spent on the travel’
Effectiveness of the model of partnership with National association and children’s palliative care expert site The model of partnership between the National association and the expert site is found to be quite effective as is evident from frequent visits by the representative from the Indian association of Palliative Care (IAPC) to the project site and efforts taken by both in advocacy and education. The program is widely published in the e-hospice and the official website, http://palliativecare.in/cpc. Enough importance and coverage were given in the last few national and international conferences on paediatric palliative care in the form of workshops and seminars. There is still a potential for the IAPC to play a bigger role in national level advocacy and policy related to paediatric palliative care. The local expert group has expressed the need for more support and involvement of IAPC in their effort to bring the change both at state and in the country.
Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
11
Effectiveness of the model of training followed by periodic mentorship Volunteers and social workers are encouraged to undergo 8-days training in palliative care at TMH where the curriculum has a special emphasis on paediatric palliative care. The training is followed by 1-2 weeks of clinical placement. The staff of CPC provides the continuing mentorship by hands-on training and skill building by regular visits to both the site. Initially, it used to be 3-visits / week but now reduced to weekly visits. The general feeling among the health care providers in both the sites was that more on going and hands on training were needed. In the community outreach program at JCH, the ASHA workers expect regular refresher training 1-2 times a year and more widespread training to all the ASHA workers. ‘More training is required. We are unable to handle when family ask difficult questions. We are very uncomfortable dealing with death happening in the homes even though we are often called to attend’, says an ASHA worker. ‘More hands- on training is required for our new initiative in non-cancer palliative care’, says the Head of the Department, Paediatrics. For the effectiveness of the program at ART centre in Sion Hospital, the staffs expect more audio video aids like puppetry, demonstration, storytelling and posters for the children and the families and more networking and meetings with NGOs. However, there was a concern expressed by one of the paediatrician in Sion hospital about ensuring the quality and standards in the services provided by the health professionals. ‘There should be a restriction on who qualifies as a counsellor specially when dealing with children with disability. There should be a proper licensing system and quality assurance on the service provided’, says Dr Dalawai, Department of Paediatrics, Sion Hospital The positive impact is possible commencement of new courses in paediatric palliative care in near future like the one year Fellowship in Palliative care by the Department of Social and Preventive Medicine (Distance Education), Sion Hospital, which is expected to start in June 2013 and the Six Months Certificate course in Paediatric Palliative Care by the TMH
Collaboration between multiple partners and involvement of stakeholders in decision making and planning Even though multiple partners are involved in the project, efforts are made to involve all the partners in decision making and planning, as is evident from number of meetings held for different stakeholders. ‘There is a nicely created chain and no interference in reporting and finances’, says Dr Pradnya. ‘The program initially had a teething problem and there was a lag in the first year. The last one-year had been really fruitful. All the partners are involved in planning. Meetings are frequently held involving partners like NRHM, HODs, Government, MHSAC etc. thanks to efforts taken by Dr Pradnya’- Dr Mamta V Manglani, HOD, Department of Pediatrics.

Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
12
There are yearly and biannual visits by representatives from Help the hospice and ICPCN to provide the necessary mentorship, training and evaluation.
Many stakeholders mentioned Dr Pradnya Talawadekar, the Country Co-ordinator-
CPC as the main key person who is holding all the stakeholders together. The leadership role of TMH and the support of Dr Maryann Muckaden are also playing a crucial role in bringing different stakeholders together. Priorities of different stakeholders, including IAPC, are seen as one of the challenges in meeting the goals in expected timeline of the project. Constant involvement of different changing government officials is also perceived as a challenge especially when it is expected that the Government of Maharashtra adopts a stand on state level health care policy on paediatric palliative care. The communication between staff of local CPC project and IAPC office is found to be sometimes challenging because of reasons like language problem and different people involved in both places answering to different heads.
Effectiveness of Project Expenditure and Sustainability It is unlikely that the results could have been achieved at a lower cost or with fewer inputs. The success of the project so far has been supported through the buy-in and engagement of key stakeholders (as reported in the CSCF ANNUAL NARRATIVE REPORT, 2011-2012). The program has utilised the existing systems and infrastructures to implement the CPC project. At both the sites, the existing staff is trained and empowered to provide palliative care. The most significant area of community level empowerment has been among ASHA workers within Jawhar rural area. In addition, the NRHM has supported project scale up in JCH through training of existing HCWs and recruitment of dedicated palliative care health care providers, responsibility of salaries and drug provision. This approach has ensured sustainability in both the sites. “This is a model which can be replicated in any resource poor country with a shoe-string budget. The beauty is that it utilises the existing resources” – Dr Maryann Muckaden. The stakeholders have however expressed some concerns. Frequent staff attrition and change has posed a big concern for the program. The existing staff in Sion are overworked with the many responsibilities undertaken on behalf of MHSAC like doing HIV and ART testing, counselling, documentation, implementation, follow up etc. No extra remuneration is paid for the extra time spent on doing palliative care activities. Most of them are doing it out of their interest and dedication. The CPC member mentions that documentation needs repeated reminder and motivation. ‘If the CPC project stops, there will not be any motivation for the existing staff at ART centre in Sion to go on. Similarly, if the current head of the Department of Pediatrics at Sion retires/ changes, the project may not get the necessary support’, a concern expressed by the project coordinator. ‘The target is to enrol 200 children by next year but that also means more manpower is needed’ – Professor Dr Mamta V Manglani.

Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
13
The Nurses, MHWs and ASHA workers in the community are involved in many projects and overworked. The team in JCH suggests a dedicated team for palliative care just like many other successful focused government -led program like Leprosy and Tuberculosis control program. Dr Ramdas M Marad, Pediatrician and Chief Medical Officer of JCH also echoes similar concerns. He wishes a dedicated ambulance for the home-based care of the patients in the community. The only social worker employed by the NRHM project feels that he is unable to focus on his work because of multiple responsibilities like documentation, data entry, camp arrangement, medicine stocking, reporting, home visits and visits to PHC/ RC, motivation of staff etc. ASHA workers are not on full time payroll and if for some reason they can’t work, no wages are paid. Also, if patients identified by them are not eligible for PC, there is no remuneration. There is undue delay in in getting the payment. No payment is given for providing home visits. Dr Mrinal Marathe (Paediatric Counsellor) mentions development of a state level policy as the main priority to ensure sustainability and while planning allocation of resources, more funding should be earmarked for advocacy and media related activities. High risk of staff burnt among members of CPC project and partner organizations is another of concerns expressed by the country coordinator. The local CPC players consider leaving of Dr Manjeri who is responsible for many of the initial initiatives as a big setback. The staff of the CPC project is also worried about their own future and job security.
Palliative Care Impact The immediate impact is a significant increase in number of children receiving palliative care in Maharastra state. The target of is 250 (Sion, Jawhar) achieved in the year 2013 in which 40 % are girl children. 80% children in targeted areas of Maharastra state report improved quality of life. (Measured by reduced pain and improved ability to interact and play.) No of centres within Maharastra with an oral opioids licence has gone up to two since the inception of the project and the number of children prescribed strong opioids in two centres is 50(new). There are dedicated team members in CPC project who are regularly communicating with professional bodies like Indian association of Pediatrics and visiting pediatricians across the state imparting awareness and sensitization on pediatric palliative care. The number of Health care workers trained in children’s’ palliative care and opioid use (introductory and intensive courses) are 270 (new overall) with a training records from the project (with pre and post-test questionnaire analysis). Efforts are being made to develop a group of trainers by doing TOT courses.

Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
14
Intensive Sensitisation
Medical 54 81
Para-medical
54 81
In terms of advocacy and policy change, the draft document for change in legislation is in the process of translation to Marathi Language before the final submission to the Government of Maharshatra. A two volumes of Training Manuals on Pediatric Palliative Care, a joint initiatives by the IAPC and TMH, Information leaflets and booklets ,a 15 min short film on paediatric palliative care, rallies and cultural events, several media articles in local and national dailies are some examples of efforts at training, dissemination of information and advocacy. The Tata Memorial Hospital has adopted a ‘Child Protection Policy’ as a result of constant advocacy. The Indian Journal of Practical Pediatrics is planning to bring out a dedicated supplement on ‘Supportive and Palliative care’. Several meetings are held with bodies like AIDS control society, Ministry of Health in Government of Maharshtra, Municipal Corporation, Department of Food and Drug Administration, Central Ministry for woman and child welfare, IAP, several NGOs, disability and training institutes. As a result of positive outcome of CPC project with HIV and AIDS, an out-patient service, twice a week, has been initiated by the Department of Pediatrics for other life limiting illnesses. Departments like Nephrology and Neurology are actively linked with this service.
Monitoring and Evaluation The CPC project team has developed an adequate record keeping and data collection system. Efforts are being made to ensure adherence to time scale by the partners and adequate monitoring system. There seems to be an adequate clarity of arrangements for meetings and deadlines
Lessons Learnt This is a useful learning experience, which can be replicated in other places. The goals and objectives are very clearly defined and the team is very well trained in executing it with focus and clarity. They have acknowledged Kate’s and ICPCN contribution in getting this kind of mentorship and training. They also mentioned how they themselves evolved as a leader and learnt the skill of project/ proposal and report writing, executing it in a focused manner and the skill of advocacy. “Tremendous management and advocacy skills are required to carry out a project like this. But the lesson is persistence and tenacity.” – Dr Maryann Muckaden. The project is clearly helping to develop a palliative care health policy for children with life limiting illnesses in the state of Maharashtra as compared to other states in India where it is virtually non-existent.

Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
15
“If it were to be replicated in any other place, there should be a top down approach to make it effective. Currently, when we approach the government or the management, it is almost like it is our need. Legislation of palliative care is mandatory in all hospitals and clinics, both government and private’- Dr Mamta V Mangalani. Dr Mrinal Marathe (Paediatric Counsellor) also emphasise the main priority as the policy development if it were to be replicated in other places and separate funding should be committed to advocacy and media. The local partners have found the mentoring by HTH and ICPCN very useful.
Feedback for the Future A better medical management and end- of- life- care policy in the project
planning.
Better coordination and support from the National organization
A system for self-care among CPC staff and members of partner organisation
A plan for a long term mentoring and support to partners

Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
16
Supporting the Development of Children’s Palliative Care in Malawi through an International Network (2010-2015)
Executive Summary
Help the Hospices together with funding from the Department of International
Development have been working together with international partners to establish
and implement a four year programme to improve access, quality and awareness of
children’s palliative care in Malawi. The project is implemented by the Palliative Care
Association of Malawi (PACAM) with technical input from Umodzi Children’s
Palliative Care Service. The project is operational across three central hospitals
(tertiary providers) in the large towns of Zomba, Mzuzu and the capital city Lilongwe.
The project is at half way point and has commissioned an independent review
focusing on evaluating the impact and approach of the project, areas for
improvement and mechanisms for sustainability and lessons learned.
The review was delivered in March 2013, through a mixture of semi structured
interviews with coordinators’, staff, guardians and beneficiaries from all three
sites. The review also included discussions with PACAM staff and desktop
analysis of documentation and reports.
The review concludes that the project is delivering well and is online to reach the
targets set for 2015 ahead of schedule in most areas. The changes introduced
are integrated within the Ministry of Health provision and therefore likely to be
sustainable post project.
The collaboration between the partners works well, however the mentorship
provided by Umodzi clinic is weak and could be strengthened which could positively
impact on the variation in implementation across the three sites.
The development of advocacy and awareness of children’s palliative care has
increased demonstrably across all sites and within government, with PACAM
greatly enhanced and a strengthened profile.
Palliative care being offered currently is limited to central hospitals and a few
proportions of referred patients are able to access the care, expansion of such care
to district care facilities will improve access and quality and reduce the burden of
patients travelling. The current trend is that palliative care is available for those that
have knowledge about it, can access it with their own initiative. The service is not
yet demand driven.
The review identified a range of recommendations that could provide focus for the
final two years of the project; these include expansion of the model into district
hospitals, greater collaboration with Umodzi and standardisation of data collection
tools and sharing best practice across sites.
Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
17
1.0 Background
The purpose of the project is to gain government commitment to providing
appropriate and effective palliative care for children living with HIV and other life
limiting illnesses in Malawi and India. This will contribute towards the goal of
improving the quality of life of children with HIV and other life limiting conditions in
Malawi and India. In Malawi the project is implemented through the following broad activities:
- Building capacity of the national association to advocate for children’s palliative care.
- The national association to identify and work with three sites to conduct
training in children’s palliative care. The sites integrate children’s palliative care into their services, mentored by the project partners.
- The project partners work with relevant educational bodies to integrate
children’s palliative care into health professional training curricula.
- Awareness activities are conducted to raise profile of children’s palliative care and increase demand for services.
- Project partners actively working with policy makers and legislators to
improve the relevant policy environment for children’s palliative care
- Support and encouragement in the use of opiates for children
- Workshops and focus groups held with children attending the services help to empower and inform them in their health care choices, and also provide valuable feedback to the project.
In Malawi the project is implemented by the Palliative Care Association of Malawi
(PACAM) with technical input from Umodzi Children’s Palliative Care Service. The
project is operational across three central hospitals (tertiary providers) in the large
towns of Zomba, Mzuzu and the capital city Lilongwe.
This review focuses on evaluating the impact and approach of the project in Malawi only. The specific objectives of the review are:
To assess the extent to which the project objectives are being met
To identify areas for programme adjustment or strengthening to ensure objectives can be met by the end of the project.
To ensure mechanisms for sustainability are in place and effective by the
end of the project
To record and share lessons learned and to ensure effectiveness and efficiency in the programme design.
Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
18
2.0 Overview of method/approach The review was conducted by independent consultants to provide objective
analysis. Health Management Consultant Gemma Dawson together with Public
Health and Palliative care specialist Norton Gondwe from Malawi College of
Medicine worked together combining management and clinical perspectives to
deliver the review. The review was conducted using a variety of different methods;
Reviewing current project documentation (including finance information, annual reports, Log frame and proposal documents)
Interview and discussion with PACAM senior staff about the project
Interview and discussion with Umodzi senior staff about the project
Structured interviews were conducted with the identified co-coordinators at
each of the central hospitals, with questions based around the reviewing criteria.
Structured interviews were held with two members of clinical staff at each
central hospital that has received the palliative care training as part of the
programme, these individuals were identified by the co-coordinator.
Structured interviews were held with three sets of children in receipt of the
services and their guardian at each of the central hospital sites. Some were
conducted in a group setting whilst others in privacy, dependent upon the
beneficiaries preferences.
Visit to the clinic room dedicated for children’s palliative care to observe
and look through the data monitoring and collection services at each
hospital.
Observation of patients assessment and care planning
A single day was spent at each hospital at the end of March 2013.
3.0 Key findings
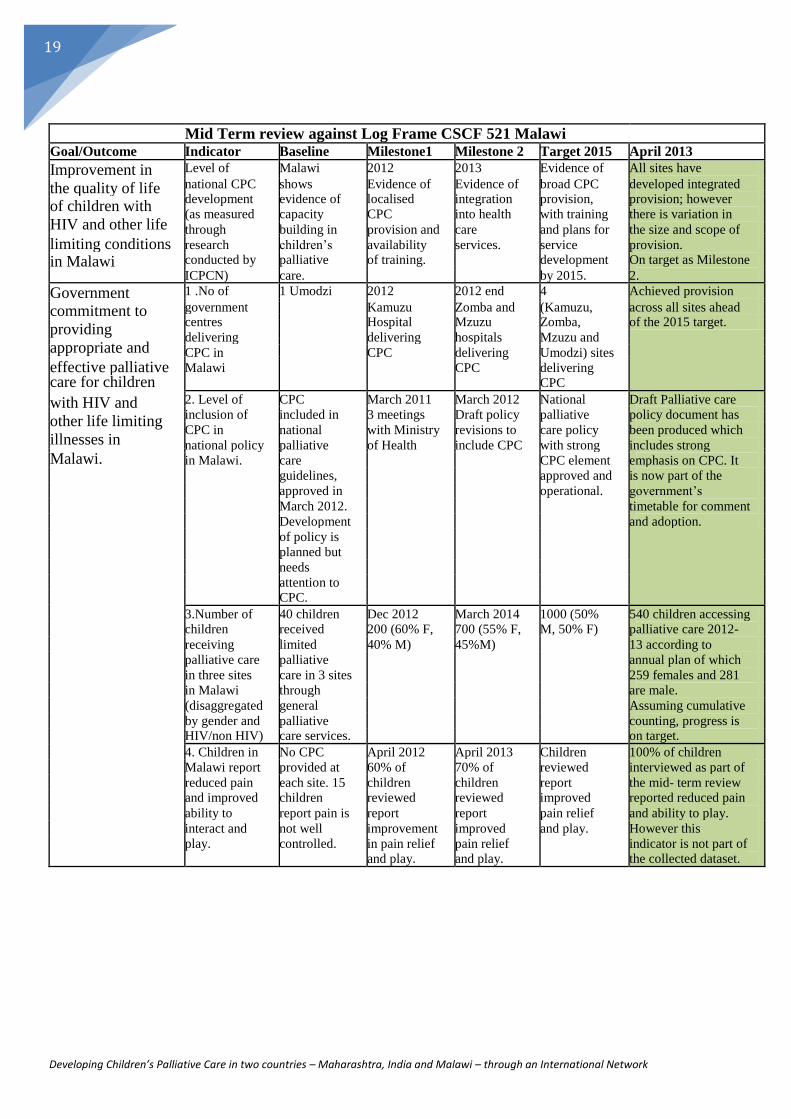
3.1 General The following table is based on the agreed Log frame for the project. It includes just the
indicators relevant to Malawi together with an additional column providing progress as of
April 2013, mid-way through the project. It is colour coded using traffic light system to
provide at a glance reference on progress against agreed timeframes. Green represents
on track, amber working towards and red issues with progress.
Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
19
Mid Term review against Log Frame CSCF 521 Malawi
Goal/Outcome Indicator Baseline Milestone1 Milestone 2 Target 2015 April 2013
Improvement in Level of Malawi 2012 2013 Evidence of All sites have
the quality of life national CPC shows Evidence of Evidence of broad CPC developed integrated
development evidence of localised integration provision, provision; however
of children with
(as measured capacity CPC into health with training there is variation in
HIV and other life
through building in provision and care and plans for the size and scope of
limiting conditions research children’s availability services. service provision.
in Malawi conducted by palliative of training. development On target as Milestone
ICPCN) care. by 2015. 2.
Government 1 .No of 1 Umodzi 2012 2012 end 4 Achieved provision
commitment to government Kamuzu Zomba and (Kamuzu, across all sites ahead
centres
Hospital Mzuzu Zomba, of the 2015 target.
providing
delivering delivering hospitals Mzuzu and
appropriate and
CPC in CPC delivering Umodzi) sites
effective palliative Malawi CPC delivering
care for children CPC
with HIV and 2. Level of CPC March 2011 March 2012 National Draft Palliative care
inclusion of included in 3 meetings Draft policy palliative policy document has
other life limiting
CPC in national with Ministry revisions to care policy been produced which
illnesses in
national policy palliative of Health include CPC with strong includes strong
Malawi.
in Malawi. care CPC element emphasis on CPC. It
guidelines, approved and is now part of the
approved in operational. government’s
March 2012. timetable for comment
Development and adoption.
of policy is
planned but
needs
attention to
CPC.
3.Number of 40 children Dec 2012 March 2014 1000 (50% 540 children accessing
children received 200 (60% F, 700 (55% F, M, 50% F) palliative care 2012-
receiving limited 40% M) 45%M) 13 according to
palliative care palliative annual plan of which
in three sites care in 3 sites 259 females and 281
in Malawi through are male.
(disaggregated general Assuming cumulative
by gender and palliative counting, progress is
HIV/non HIV) care services. on target.
4. Children in No CPC April 2012 April 2013 Children 100% of children
Malawi report provided at 60% of 70% of reviewed interviewed as part of
reduced pain each site. 15 children children report the mid- term review
and improved children reviewed reviewed improved reported reduced pain
ability to report pain is report report pain relief and ability to play.
interact and not well improvement improved and play. However this
play. controlled. in pain relief pain relief indicator is not part of
and play. and play. the collected dataset.

Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
20
Output Indicator Baseline Milestone1 Milestone 2 Target 2015 April 2013
National 1.1 Level of No inclusion 2011 2012 Implement- Clear strategy in place
associations inclusion of of CPC in Inclusion of Clear ation of the for CPC delivered by
CPC within advocacy CPC in advocacy strategy. PACAM, as
(IAPC & IAP) in
advocacy strategy of PACAM strategies for evidenced by
Malawi have
strategies of PACAM strategic CPC for advocacy activities
increased ability to PACAM plan. PACAM. carried out by
advocate for CPC PACAM.
1.2 Number No materials. 2011 2012 Advocacy PACAM have held
and type of Fact sheet on Journal materials events to co-
advocacy CPC need articles available in productively produce
material drafted in World Day print and web advocacy material
produced. Malawi. materials widely (e.g. Development of
and calendar distributed in educational material
published. three on Feb 6th
) and
languages. various awareness
sessions, this is on
target.
1.3 Number of 1 2011 2014 12 meetings Difficulties in gaining
CPC advocacy 3 meetings 8 Meetings with MOH minister commitment
and with MOH with MOH Task force and diary time,
sensitisation Task force Task force meetings (2 however one key
meetings with meetings (2 meetings (2 per year) event has been held in
government per year) per year) National Aids March with children,
policy makers National National Aid Association guardians and
and Aids Association (4 per year) ministers together
stakeholders. Association (4 per year) with PACAM.
(4 per year)
3. Healthcare workers 3.1 Number of 3 people 2011 2012 600 54 people trained, of
equipped with skills healthcare trained in 35 Clinical 30 Clinical sensitisation which 12 are Clinical
and knowledge to workers CPC in officers, officers and 30 CPC intro Officers and
deliver CPC in trained in CPC Malawi (1 nurses nurses 5 day course, Sensitisation occurs
Malawi doctor, 2 received 15 pain informally so no
clinical sensitisation management records of numbers.
officer) and morphine
3.2 Number of 2 in Malawi 2011 2012 19 (3 From the 54 people
health care (1 doctor, 1 Kamuzu +7 (Mzuzu) hospitals) trained, 33 are
workers clinical Hospital 5 Mzuzu Kamuzu: practicing palliative
providing CPC officer) nurses and 1 hospital 5 5nurses, 1 care giving a 63%
clinical nurses, 2 CO average training to
officer clinical Mzuzu: 5 practicing rate.
officers nurses, 2 CO However low rate of
Zomba: 3 CO practicing despite
nurses, 3 CO receiving training.
3.3 Level of Malawi 2012 2014 CPC being PACAM updated
recognition of College of Curriculum Sensitisation taught. palliative care training
and Medicine includes CPC of lecturers. module with inclusion
engagement in recognises of CPC that is now
CPC among CPC – included in the
professional proximity to training programme at
training Umodzi. College of Medicine
bodies. 2013 academic year.

Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
21
Mid Term review against Log Frame CSCF 521 Malawi
Goal/Outcome Indicator Baseline Milestone1 Milestone 2 Target 2015 April 2013
Greater access to 5.1 Number of Limited 2012 2013 At least 30 33 practicing
pain relieving professionals prescribers – +15 +15 professional’s professionals
prescribing in part due to
now following training all
medicines for
morphine for fear around prescribing confident in
children living
children at the opiate use in morphine to prescribing, exceeding
with HIV and target sites children. children. the 2015 target
other life limiting already.
conditions in 5.2 Number of Stock outs Improved Reduction of No stock out Stock outs common
opiate stock are believed perception stock out days at any of and occurred during
Malawi.
out days at to be severe among key days by half. the three the review. Data is not
each hospital. as is a lack of stakeholders hospitals collected by the
data on the about the (Kamuzu, project therefore
full nature of seriousness Mzuzu, unable to measure
the problem. of morphine Zomba) affect of the project on
stock outs – stock out reductions.
resulting in
clear data on
stock outs.
5.3 No of 40 from 3 2012 2013 200 Due to data collection
children sites 100 150 variations no
prescribed 314 Umodzi prescribed prescribed confirmed but assured
opiates in the Use of liquid morphine in morphine in over 150 are
three sites plus morphine the 3 sites. the 3 sites. prescribed morphine.
Umodzi Averages from
quarterly data show
83% of those seen
were reported as
prescribed morphine.
7. Children with life 7.1 Number of 0 2012 2013 30 per year Quarterly meetings
limiting illness and children 30 per year 30 per year (50% female, held in every location
their families involved in (50% female, (50% 50% male) with over 30
empowered to inform focus groups 50% male) female, 50% beneficiaries and
service delivery meetings/semi male) guardians’ attending,
around the provision structured well above the
of CPC in Malawi interviews targeted levels.
7.2 Level of 0 2012 2012 2013 Evident that the
incorporation Messages Draft articles All published activities of PACAM
of children’s gathered materials are co-produced and
opinions into from focus include have strong roots with
advocacy groups children’s lived experience of
articles voices. beneficiaries and
guardians.
7.3 Voices of No such 2012 Children’s White paper Large event held in
children engagement Focus groups voices on children’s with policy makers
presented to in Malawi discussions recorded and experiences and ministers and
government in with children shared at of CPC children from all the
policy and MOH meetings presented to project held in March
discussions officials local and government 2013.children
(50% f 50% international presented various
M) issues to the minister
including the
availability of
morphine

Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
22
Generally the project is progressing well against the targets in the log frame. However some
targets are already achieved with still two years of the project left, leaving room for further
development. There is potential opportunity to enhance the targets to achieve greater
impact within the final two years of the programme.
The project is on track to achieving the targets well before March 2015 with three exceptions:
The levels of Clinical Officers trained are much lower, although the total number of
trained staff members is more than exceeding targets outlined in 3.2. This is
explored in further detail in the training section of this report.
The target of 5.2 around stock outs is potentially unrealistic as the stock outs issues
are a national problem and the project has limited influence, or any activities
delivered or planned to affect the availability or potential priority of morphine stock.
Sensitisation within the hospitals has been varied and limited. Staff have cited lack of
time and resources to do any formal sensitisation wider than interested parties.
Therefore it is proving difficult to gain reliable figures on those sensitised and the
target of 600 sensitised could prove challenging or unrealistic.
3.2 Project Design 3.2.1 Access to Palliative care service
All services report good access routes and referral networks across the hospital, including
ward rounds either daily or weekly to ensure all children who could benefit from palliative care
within the hospital are identified and treated in the service. All services also report a growing
positive profile of children's palliative care evidenced by wards/departments referring to the
service. Patients with HIV and other conditions requiring palliative care are able to access
care through the service, however it is clear that the majority of patients requiring palliative
care, not already referred or inpatient at the hospital are not able to access care from these
sites due to project based in tertiary referral hospital only. Palliative Care co-ordinator, Kamuzu Central Hospital Lilongwe: "Yes there are still vulnerable people not reached, it is hard to estimate the proportion of children that come to palliative care as a ratio to the total number who need."
It was universally mentioned by all staff and guardians interviewed, including
representatives from PACAM that there remains significant unmet need and the feeling that
the majority of vulnerable children who could benefit from palliative care were not being met
through the project. The most common barrier cited for unmet children and those who are
accessing the project was travel. Central hospitals are located in large urban towns/cities,
majority of people accessing are referred from rural district health centres and therefore
have travelled great distances to receive care. This poses financial and time issues for the
family and children and issues in continuity of care as when faced with drug stock outs, or
follow up consultations, regular travelling is not possible or reliably made.

Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
23
Guardian, Mzuzu:
“It is ok for me as I live in Mzuzu but others that live far away it is difficult. It should
be available in the districts and local clinics so that they can get access. Should be
all over , I am speaking for others that come from afar, if we could go out to the
districts to let people know about palliative care could save lots of children. Children
are dying, people don't know about palliative care so go to witch doctors as they are
ignorant. We should go out to the districts."
Establishing the project within central hospitals which require a referral from district or other localised institutions creates a barrier to access adequate palliative care services. Particularly when staff within district hospitals are not aware or skilled in palliative care in order to recognise and make a referral onto the central hospitals. Therefore it can be concluded that the design of the project within central hospitals creates a barrier to accessing palliative care.
Palliative care co-ordinator Zomba Central Hospital: “There are lots of people that have not been reached. More people need to be
sensitised to palliative care, to avoid long distance travel. They should get palliative
care in the district to avoid coming here to the central hospital." 3.2.2 Collaboration between partners There is evidence that collaboration with other partners outside PACAM is limited. This
limited collaboration could be attributed to low advocacy and poor attitude on palliative care
among individuals. Zomba service, based within the Physiotherapy department has
therefore developed relationship with disabled peoples organizations; 'Malawi against
physical disability’ and Digintas International.
The relationship with PACAM is strong and well developed across all sites, particularly with
the onsite co-coordinators and the Project Co-coordinator at PACAM. There is regular
communication and events and groups held are highly regarded, particularly the quarterly
advocacy and sensitization meetings with guardians and beneficiaries.
However apart from the initial training and clinical placement option all interviewed reported
no further support or mentoring from Umodzi service. The most valuable support received
from Umodzi was unanimously reported as the initial training. There appears to be no
ongoing communication between Umodzi on implementation since training or regular
supervision, which could explain the variations that have appeared in delivery.
The collaboration between partners (Ministry of Health and PACAM) appears to be working, where the partners are actively engaged, or have the capacity and resources to engage (such as PACAM). 3.2.3 Beneficiary and guardian empowerment/involvement There is maximum involvement of patients and guardians in the care planning, decision making
and all other issues surrounding care in all three sites. Guardians felt that they have gained
more knowledge on palliative care and are able to perceive the benefits. One challenge that
limits the involvement of guardians is distance to the facility as they have to travel long
distance to access care this has implications in reducing their involvement.
Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
24
Guardian, Mzuzu: "I also know what to do when something happens and now he is always in school and not missing classes. I am involved in administering of the drugs, following instructions and ensure they have been taken. I enforce adherence according to the instructions that is why he is getting well now." We asked every guardian the question: “How empowered and involved are you in decisions
making about your child’s care?” to which 100% commented on feeling more aware, greater
understanding and therefore more involved as a partner in the medical care of their child.
Guardians frequently reported appreciation in the time taken to explain their child’s
condition, the treatment plan and how to administer drugs and how this reassured them and
made them feel confident ahead to deal with future exacerbations of their child’s condition. Guardian, Zomba: "We are given a chance to explain the problems and challenges; I take part in the care." Beneficiaries reported within the group sessions that they had good awareness of their
condition and were active members of the quarterly meetings held by PACAM. Guardians
and beneficiaries reported that they enjoyed the opportunity these meetings presented to
meet others in similar situations and discuss the issues pertinent to delivering children’s
palliative care, expressing only that they wished they were more frequent.
The interaction, time and empowerment have had a positive effect on guardians in
particular and have helped develop their general understanding and knowledge about
disease and chronic illness management. This is evidenced in the following quote from a
guardian in Mzuzu and is typical of responses found across all sites. This empowerment
particularly through knowledge is crucial in overcoming cultural barriers to accessing health
care (such as witchcraft, herbal remedies) resulting in children presenting at health centres
earlier. Guardian, Mzuzu: "We are empowered as we have knowledge about some other conditions and palliative care, we didn't know what to do previously now we do. The sessions at palliative care clinic is helped. At home people don't know. We should have more education, request a session on cancer so you can tell us about that."
Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
25
3.2.4 Sustainability As the project is delivered by staff employed and embedded within the Ministry of Health,
the practicing staff members will continue to practice palliative care expertise once the
additional support and infrastructure of the project has finished. In that regard, a level of
sustainability is achieved, particularly across department s and divisions, ensuring good
penetration of expertise across the workforce.
However, although perceptions within the hospitals have been reported to have changed
positively since the existence of the project it is doubtful whether the continuing practice
will grow and any further service expansion independently of additional resources or
external support.
The achievements of embedding children’s palliative care training within the national nursing
curriculum will ensure that expertise is continued through the incoming workforce, but
implementation in practice across all healthcare settings could be slow without dedicated
support. It is too early to ascertain any evidence to demonstrate this new cohort practicing
palliative care from their initial training, not part of a dedicated project. Staff Nurse, Kamuzu Central Hospital Lilongwe: "There was real need in the wards and we kept having to fetch the palliative care nurses from the department so I asked if it was possible for me to be trained so that we didn't have to refer and we could support them on our wards, right there. Palliative care training helped me address the need in the ward that I was working"
3.3 Differences across the sites All sites are striving towards the same model of delivery: establishing or developing a
dedicated children's palliative care clinic that can take referrals from across the hospital and
support palliative care practice across the hospital. Variation in implementation occurs in
their various maturities towards this model. Kamuzu Hospital in Lilongwe is the most
established, with adequate space and resources dedicated to a permanent clinic. They
have established their own medicines cabinet to avoid referral to pharmacy and long waits
for patients. Mzuzu and Zomba share space with other clinics or departments, and suffer
from limited full time staff dedicated to the clinic. All locations use a roster to deploy the
trained staff from across the hospital to staff the dedicated children’s palliative care clinic.
However in Mzuzu where the dedicated clinic only runs one day a week there are
unintended positives as the lack of fully established clinic has resulted in wider integration
of trained staff and practicing palliative care professionals, with more palliative care being
delivered holistically on the wards as there is no ‘other’ clinic to refer too. The variation
highlights how important the design of the service and the impact of integration into hospital
services, Mzuzu although feels behind the others in delivery is ahead in wider integration
into mainstream hospital services.
A second major variation across sites is around data collection. The programme has not
identified single set of information requirements; therefore different information is collected
at different sites using a variety of different methods.

Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
26
The sites mainly collect data manually in registers and then enter into the computer
retrospectively to compile reports for PACAM. Agreement around the requirement to
standardise data collection was recognised by all partners across the project and PACAM
taking responsibility to co-ordinate and take this work forward. Key alignment together
with the Log Frame data requirements is key to ensure the project can accurately
evidence the progress made.
All sites had the computer up and running, however there is clear training requirements
to ensure that the co-ordinators and all palliative care staff make the best from this
valuable resource. Again this issue was recognised by PACAM.
3.4 Quality Clinical observation was carried at Kamuzu Central Hospital on an assessment of a child
in the palliative care clinic. This observation demonstrated a high quality and a well
organised palliative care service that is able to address most of the patients and guardian
needs.
Thorough assessment of the patient’s physical, social and spiritual needs of the patients
and guardians is conducted in order to gain an insight of the problem and provide
appropriate care. The holistic needs of the patient, their caregiver/s and family, are
acknowledged in the assessment and care planning processes, and strategies are
developed to address those needs, in line with their wishes.
Treatment is provided according to standard treatment guidelines for Malawi. Patients
requiring morphine are able to access it with the relevant teaching on administration and
side effects and home management. Staff referenced the WHO best practice guidelines
for assessing pain and administering morphine.
Care is coordinated to minimise the burden on patient, their caregiver/s and family. Visits
are scheduling to provides opportunities for rest among patient and guardians
Through structured interviews with staff report that 100% were confident assessing and
managing pain, confident in palliative care to practice in other settings outside of the
clinic and 100% were confident with prescribing morphine.
Satisfaction as an indicator of the quality of palliative care services. It also aimed to
provide a solid basis upon which further work could be built. In this evaluation Patients and
guardians as well as care providers clearly indicated that they were satisfied with the
Palliative care service on offer
There were some differences in the perception of satisfaction between
patients/guardians and nurses. Nurses felt that they had partial satisfaction due to limited
resources while patients and guardians felt maximum satisfaction due to the fact that
their problems have resolved and are pain free.
Staff members expressed frustration, particularly around the unavailability of necessary
drugs to treat patients and the inequity of drug costs on the open market, where
patients were forced to purchase in the event of stock outs.

Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
27
3.5 Training of care providers and skill mix Most of the care provider’s currently providing palliative care have undergone the five day
CPC training from the project to equip them with knowledge and skill relevant for the
delivery of palliative care. This has an impact in improving the quality of care at the facilities.
Team meetings help to strengthen the palliative care team in the delivery of palliative care
service. Availability of providers from different wards/departments help to ensure that most
patients access care from where they are and there is a wide variety of skill mix relevant for
the delivery of Palliative care. It is clear that incorporating palliative care in the existing
hospital teams is the best way to go in this era of shortage of health care workers.
Provider training and mentorship followed by clinical placement is an ideal approach in
increasing altitude of providers, exposing them to various clinical skills and knowledge
about palliative care, Majority of providers who have undergone placement recommended
clinical placement in palliative care as a model of teaching and learning.
Each site has delivered successfully the five day training targets as laid out in the log-frame.
However, there was interesting discrepancy between the trained and practicing staff levels.
From staff trained (54) only 33 are recognised by the project co-coordinators to be still
practicing palliative care in the hospitals. This varies across sites, with Mzuzu Central
Hospital reporting 100% practicing from trained staff to just 44% in Kamuzu Central Hospital
Lilongwe and 45% at Zomba Central Hospital. Produces a 63% success of trained staff
practicing average for the project, which is an area for improvement to ensure maximum
impact and value for money from training resources.
Table 1: Training by designation of Children’s Palliative Care 5 day course
Designation Mzuzu Lilongwe Zomba Total
Nurse 3 14 9 26
Nurse/Midwife 3 0 0 3
Pharmacist 1 0 1 2
Clinical Officer 4 1 6 11
Medical Doctor 3 0 2 5
Dermatology Officer 1 0 1 2
Dental Officer 1 0 1 2
Physiotherapist 0 0 2 2
Total 16 15 22 53

Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
28
Figure 1: Malawi staff trained in CPC by designation
4% 4%
4% Nurse
Nurse/Midwife
9% Pharmacist
49% Clinical Officer
21% Medical Doctor
Dermotology Officer
5%
Dental Officer
4% Physiotherapist
Variation occurs in how staff are selected to take part in the training and therefore the
designation of staff partaking. Feedback through the interviews from questions around
training and improving the perception of palliative care, demonstrated that Clinical Officers
have limited capacity to deliver palliative care and that the majority of delivery is by Nurses.
This provides some explanative narrative; perhaps the Clinical Officers represent the trained
staff not practicing deficit? This not only presents a barrier to gaining maximum impact from
trained staff, achieving the target volumes of trained Clinical Officers but also outlines
further work to demonstrate the added value and potential time saving from delivering
palliative care instead of other more conventional interventions.
Palliative care co-ordinator, Zomba Central "We selected people for training from across all the departments to get coverage across the hospital."
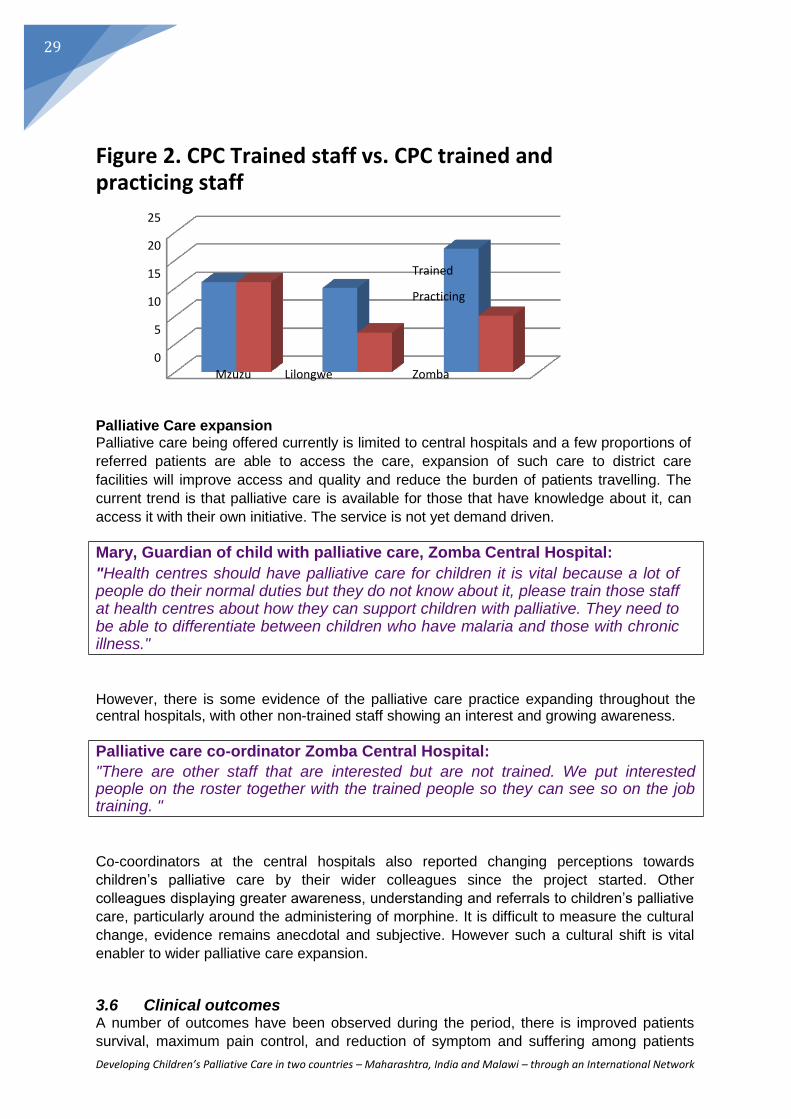
Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
29
Figure 2. CPC Trained staff vs. CPC trained and practicing staff
25
20
15 Trained
10 Practicing
5
0
Mzuzu Lilongwe Zomba
Palliative Care expansion Palliative care being offered currently is limited to central hospitals and a few proportions of
referred patients are able to access the care, expansion of such care to district care
facilities will improve access and quality and reduce the burden of patients travelling. The
current trend is that palliative care is available for those that have knowledge about it, can
access it with their own initiative. The service is not yet demand driven. Mary, Guardian of child with palliative care, Zomba Central Hospital: "Health centres should have palliative care for children it is vital because a lot of people do their normal duties but they do not know about it, please train those staff at health centres about how they can support children with palliative. They need to be able to differentiate between children who have malaria and those with chronic illness."
However, there is some evidence of the palliative care practice expanding throughout the central hospitals, with other non-trained staff showing an interest and growing awareness.
Palliative care co-ordinator Zomba Central Hospital: "There are other staff that are interested but are not trained. We put interested people on the roster together with the trained people so they can see so on the job training. "
Co-coordinators at the central hospitals also reported changing perceptions towards
children’s palliative care by their wider colleagues since the project started. Other
colleagues displaying greater awareness, understanding and referrals to children’s palliative
care, particularly around the administering of morphine. It is difficult to measure the cultural
change, evidence remains anecdotal and subjective. However such a cultural shift is vital
enabler to wider palliative care expansion.
3.6 Clinical outcomes A number of outcomes have been observed during the period, there is improved patients
survival, maximum pain control, and reduction of symptom and suffering among patients

Developing Children’s Palliative Care in two countries – Maharashtra, India and Malawi – through an International Network
30
and guardians (Key aspects include symptom control, recognition and management of
psychological problems, good communication skills, and helping patients and carers with
financial and practical issues).
All of the children clearly pointed out that they are pain free and able to live normally, this is an indication of improved quality of life though living with a life limiting illness.
Guardian, Mzuzu: "I am very thankful for the services as my daughter’s life has improved. She used to
come to the hospital twice a month and would get admitted but since she has being
coming here she has not been in hospital."
Knowledge of disease conditions among patients and guardians has improved greatly. We observed children who are no longer afraid and have hope for life.
Currently patients with malignancy have access not only to oncological expertise to
maximise survival but also to a multidisciplinary palliative approach which focuses on how
best to support patients and their families through the illness while maintaining reasonably
good quality of life.
Single area that was identified across all sites, universally by staff and guardians was
around providing adequate nutrition as part of an effective palliative care programme. The
inability due to scarce resources and rising prices of food in Malawi compromises the clinical
outcomes for the children being treated. Nurse, Zomba Central Hospital: "Malnutrition is vital. We wish we could prescribe nutrition supplements."
Guardian, Kamuzu Central Hospital, Lilongwe: "It would be better if this is a disease for rich people, as condition affects diet and she can't afford the foods that the hospital recommends for example fruit. She wishes there was nutrition supplements."
31
Developing CPC in two countries - Maharashtra, India, and Malawi through an International network Midterm review
31
4.0 Conclusions In conclusion the programme is delivering good quality services but to low numbers compared to
the total need or demand for palliative care. The design of the project; based at tertiary tier
hospital, requiring referral from district hospitals restricts the service to top tier of most critical
patients restricts access to the service and therefore the impact. There us opportunity to impact a
greater number of people requiring palliative care if available at district level. Excellent palliative
care is best given closer to the community, with greater awareness of other environmental and
social factors. Furthermore:
The programme has performed well against the targets set, achieving the four year target
early in some areas, and is set to deliver sustainable improvements across the three
dedicated sites.
The collaborative approach of the project is working effectively between the Ministry of
Health Hospitals and PACAM; however more resource and support from Umodzi could
have positive impact on the project and support expertise sharing.
The project sites are achieving similar outcomes although through slightly different
implementation models, particular regard should be paid to the models that promote
further integration of children’s palliative care within the hospitals rather than creating
‘separate stand-alone’ clinics.
It is unclear the affect, if any, the programme has had on the stock outs of morphine and
other drugs and the ability the programme has to influence and affect this area. No
clear activities were identified that would tackle this issue.
5.0 Key Recommendations
The following recommendations are put forward:
1) Some targets identified in the Log frame are already achieved or close to being
achieved suggesting that there is scope to stretch some of the targets for 2015 delivery
to encourage growth of the project, or development of new targets for the final two
years of the project building on the achievements already made.
2) Further exploration and rationale developed to identify people eligible for training to
ensure they have a passion for palliative care to increase value for money and impact
and the ratio between trained and practicing staff.

32
Developing CPC in two countries - Maharashtra, India, and Malawi through an International network Midterm review
32
3) Further work to engage Clinical Officers, to encourage and show benefit in terms of
saving time by delivering Palliative Care as opposed to other more conventional
interventions
4) Further explanatory work to understand why those who have completed the training are
not continuing to practice, is there an additional training need or is there more work to
ensure the most appropriate people are selected for training.
5) Greater support towards sensitisation could yield greater impact – area of minimal
activities so far. Case studies, people changed their perceptions once they had a positive
experience, perhaps some case studies could be written up together with a photo to
encourage families and staff about the value of palliative care Resources to support wider
clinicians; guidance about morphine use to combat misconceptions perhaps fact sheets
could be produced and circulated or presentations made. Could this be a role for one of
the partners? Perhaps PACAM or Umodzi?
6) Augmenting patients home visit to the model will help to increase access improve care
continuity and lessen the burden of travelling by patients.
7) Review the periodic mentorship delivered by Umodzi, exploring more proactive regular
ways Umodzi can support the service development in other areas and the resources
that it may require to do this in a meaningful way.
8) Potential to look into providing subsidised transport for follow up consultations and
nutrition supplements as part of prescription to increase clinical outcomes of treatment.
9) Development of standardised data collection agreements that are realistic and
deliverable across the project to increase transparency.
10) Potential to duplicate the service model within district hospitals, perhaps in a certain area
(to form a pilot) or with a few in each area, joining up Central and district practice.

33
Developing CPC in two countries - Maharashtra, India, and Malawi through an International network Midterm review
33
Appendix 1 – Questions used in semi-structured interviews across all three sites
Mid-term review: Guardian/Parent and Child interview questions - Welcome and introductions - Interviewee name and village/town Guardian/Parent:
1. How is your child's life different since receiving palliative care?
2. How empowered and involved are you in decision making about your child's care?
3. What do you think could be improved?
4. What are the main challenges?
Child:
1. Since being in the service do you feel reduced pain?
2. Are you able to play more?
3. What do you think of your treatment?
Thank you Co-ordinator interview Questions: - Welcome and introductions - Interviewee name and profession
1. When did you complete Palliative care training?
2. When did you start in the role of co-ordinator?
3. How long have you been practicing palliative care?
4. How many staff in your hospital have completed palliative care training?
5. How many of the trained staff are practicing palliative care in your hospital?
6. Are all the trained staff in the same department?
7. What activities have you conducted to sensitise other staff in the hospital about
children's palliative care?
8. Do you hold frequent meetings where you discuss issues around children's
palliative care?
9. Do you carryout daily ward rounds of admitted/newly admitted patients to check
for palliative care eligibility?
10. What are the perceptions of other staff in the hospital about children's palliative
care?
11. Do you feel staff perception has changed during the project?
12. Do you feel the majority of children you treat for palliative care are living with HIV?

34
Developing CPC in two countries - Maharashtra, India, and Malawi through an International network Midterm review
34
13. Have you received mentor support from Umodzi?
14. What was the most valuable support you received from Umodzi?
15. Apart from PACAM and Umodzi who are the other partners you are working with?
16. Do you feel there are still vulnerable children not being reached by the project?
17. What could be done to reach more children with palliative care needs?
18. What challenges are you encountering?
19. Any other questions/comments?
Thank you Trained staff interview questions: - Welcome and introductions - Interviewee name and profession
1. When did you complete palliative care training?
2. Which department do you practice palliative care?
3. How did you find the palliative care training?
4. How confident do you feel assessing and managing pain?
5. Apart from practicing palliative care in this clinic, do you practice palliative care in
other settings or wards?
6. How confident do you feel prescribing morphine?
7. What are the main barriers to prescribing morphine?
8. What strategies could we use to combat these barriers?
9. Do you think the barriers are increasing or decreasing since the project started?
10. Have you received mentor support from Umodzi?
11. What was the most valuable support from Umodzi?
12. How empowered and involved are children and guardians in their palliative care
treatment/decisions?
13. Do you record details about children who receive palliative care?
14. What and where do you record information/data?
15. What strategies could we use to combat these barriers?
16. What could be done to reach more children with palliative care needs?
17. What challenges are you encountering?
18. What strategies could we use to combat these challenges?
19. Any other comments / questions?
Thank you
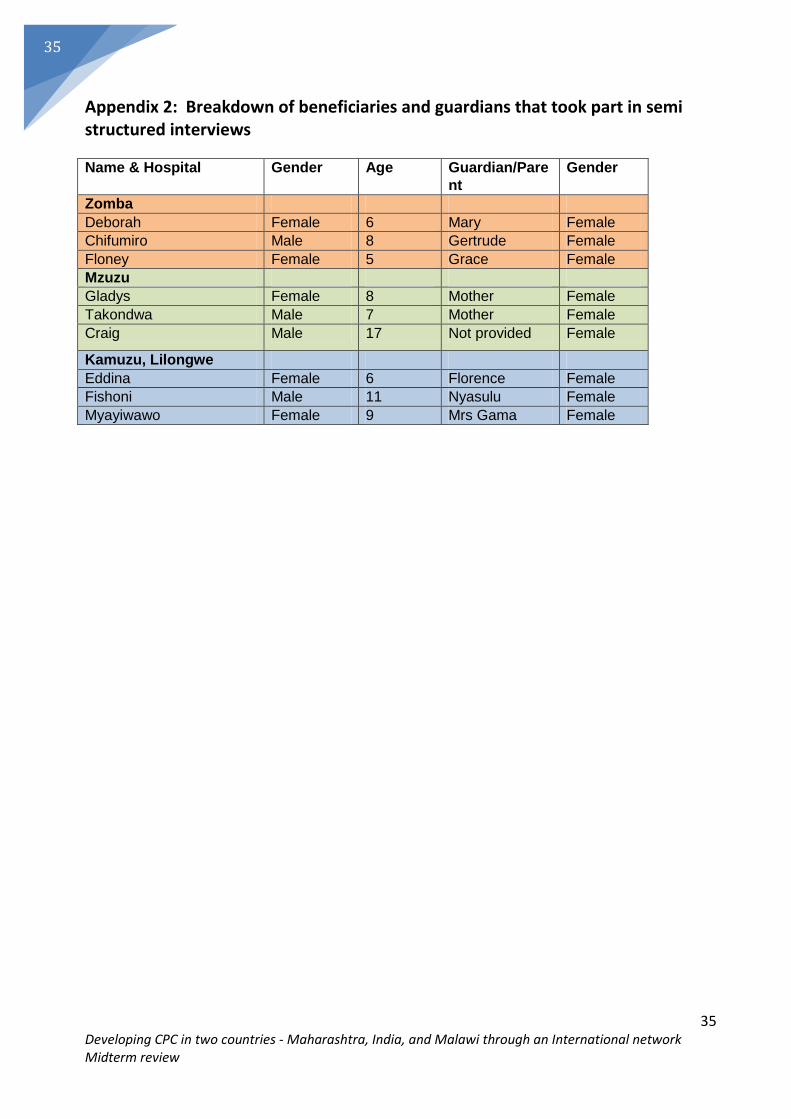
35
Developing CPC in two countries - Maharashtra, India, and Malawi through an International network Midterm review
35
Appendix 2: Breakdown of beneficiaries and guardians that took part in semi structured interviews
Name & Hospital Gender Age Guardian/Pare
nt
Gender
Zomba
Deborah Female 6 Mary Female
Chifumiro Male 8 Gertrude Female
Floney Female 5 Grace Female
Mzuzu
Gladys Female 8 Mother Female
Takondwa Male 7 Mother Female
Craig Male 17 Not provided Female
Kamuzu, Lilongwe
Eddina Female 6 Florence Female
Fishoni Male 11 Nyasulu Female
Myayiwawo Female 9 Mrs Gama Female


















