Developing a Secure Base: Application of Attachment Theory to Clinical Practice Douglas Goldsmith,...
82
Developing a Secure Base: Application of Attachment Theory to Clinical Practice Douglas Goldsmith, Ph.D. Executive Director The Children’s Center
-
Upload
daniel-marsh -
Category
Documents
-
view
214 -
download
0
Transcript of Developing a Secure Base: Application of Attachment Theory to Clinical Practice Douglas Goldsmith,...

Developing a Secure Base:Application of Attachment Theory to
Clinical Practice
Douglas Goldsmith, Ph.D.
Executive Director
The Children’s Center
Overview Foundations of Clinical Practice Attachment theory
– Strange Situation Internal Working Models Reflective Functioning Maternal Representations
– Adult Attachment Interview Insightfulness Treatment implications
Clinical Practice
Referral
Intake
Assessment
Treatment
Discharge

Good Progress!

Poor Progress
Child
Parents
System
Med Management
Alternative Hypotheses
Inadequate assessment Failure to accurately diagnose the child Failure to accurately assess family
dynamics Failure to formulate the case Failure to address the relationship
issues

Added value of attachment theory and developmental concepts:
Provides foundation for conceptualization of the parent-child relationship
Able to focus interventions on repair of relationship-based issues even when a diagnosable condition exists
Attachment
Emotional bond with another person Behaviors promote proximity with one
perceived as older, stronger, and wiser Motivational system to seek proximity Enhances feelings of security Motivates baby to take action when
frightened
Attachment Theory
When I am close to my loved one I feel good, when I am far away I am anxious, sad or lonely
Attachment is mediated by looking, hearing, and holding
When I’m held I feel warm, safe, and comforted
Results in a relaxed state so that one can, again, begin to explore Holmes (1993)
Attachment in Action
Behaviors shown by careseeker and caregiver
Aware of and seek each other out if careseeker is in danger due to physical separation, illness, or fright
Attachment Classifications
The strange situation– Secure 65%– Avoidant 20%– Ambivalent 10%– Disorganized 5-10% (80% maltreated)

Secure (B)
Uses mother as secure base Signs of missing mother Actively greets with smile or gesture Signals or seeks contact if upset Once comforted resumes exploration
Solomon & George (1999) p.291

Secure Attachment
Child feels safe and secure
Avoidant (A)
Explores readily Little visible distress when left alone Upon reunion, looks away or actively
avoids May stiffen or lean away if picked up
Solomon & George (1999) p. 291
Ambivalent (C)
Distressed, fretful, passive Fails to explore Unsettled, distressed by separation Alternates bids for contact with signs of
angry rejection Fails to find comfort from the parent
Solomon & George (1999) p.291

Insecure Attachment
Intense love and dependency Fear of rejection Irritability Vigilance Punish their attachment figure for any
sign of abandonment
Insecure Attachment
The insecurely attached person is saying:“Cling as hard as you can to people –they are likely to abandon you: hangon to them and hurt them if they showsigns of going away, then they may be less likely to do so.”
Holmes (1993)
Disorganized (D)
Behavior lacks an observable goal Look fearful Behavior is bizarre May try to leave after the reunion or
freeze
Attachment Relationship
Proximity Seeking Secure base effect Separation protest

Attachment Behavioral System
Attachment figure:Near, responsive,
attunedFelt security, love,
self-confidence
Playful, smiling,Exploratory, sociable
Holmes (1993)

Attachment Behavioral SystemAttachment
Figure:Distant,
UnresponsivePoor attunement
FearAnxiety Defensive
AvoidantWatchful
Wary
AmbivalentClingingAngry
Holmes (1993)
Visual checkingPleadingClinging

Attachment ProblemsBowlby
A severely hurt child fails to seek comfort
Signals that ordinarily activate attachment behavior fail to do so
System controlling attachment, and the feelings and desires associated, is rendered incapable of being aroused
Classification vs. Disorder
Secure infants are at a decreased risk for psychopathology but not immune
There is no clear link between insecure infants and psychopathology
Links to Other Disorders
An avoidant child may develop a hostile, aggressive, antisocial pattern in response to experience with a rejecting and emotionally unavailable caregiver
An ambivalent child may be easily overstimulated, showing impulsivity, restlessness, short attention span, and low frustration tolerance
(Greenberg, 1999 p.481)
Video

Internal Working Model
Based on the child’s real-life experience of day to day interactions with his parents
Reflects the images the parents have of the child
Images communicated by how each parent treats the child and what each parent says to the child

Impact of the Internal Working Model
The model governs how children feel toward each parent and about themselves, how they expect to be treated and how they plan their own behavior toward their parent
Securely Attached Child
Internal Working Model– Responsive, loving, reliable caregiver– Self is worthy of love and attention
Holmes (1993)
Insecurely Attached Child
The world is dangerous Treat others with great caution Self is ineffective and unworthy of love These assumptions are stable and
enduring and terribly difficult to modify Holmes (1993)
Video

Development of Relationships
“For a relationship between any two individuals to proceed harmoniously each must be aware of the other’s point-of-view, his goals, feelings, and intentions, and each must so adjust his own behavior that some alignment of goals is negotiated.

Development of Relationships
This requires that each should have reasonably accurate models of self and other which are regularly updated by free communication between them. It is here that the mothers of securely attached children excel, and those of the insecure are markedly deficient.”
Bowlby (1988) p. 131

Mothers of Secure Infants
Continuously monitor the infant’s state Accurately interpret the signal for
attention Act accordingly to meet the infant’s
needs

Mother’s of Anxious Infants
Monitor the infant’s state only sporadically
Inconsistently notice the infant’s signals May interpret the signal inappropriately Respond to the signal inappropriately,
or tardily
Impact of Anxious Attachment
“By the age of 12 months, there are children who no longer express to their mothers one of their deepest emotions or the equally deep-seated desire for comfort and reassurance.”
Bowlby (1988)

Ambivalently Attached Child
Shows overt aggression toward the inconsistent mother
“Don’t you dare do that again!” but has to cling because he knows from experience that she will.
Holmes (1993)
Avoidant Child
Outbursts of unprovoked aggression Needs to appease to the mother
because the child wants so badly to feel close
Fears she’ll rebuff him if needs are revealed too openly; or if anger about abandonment is shown too openly
Holmes (1993)

Impact of Empathic Failure
“Whatever she fails to recognize in him he is likely to fail to recognize in himself. In this way, it is postulated, major parts of a child’s developing personality can become split off from, that is, out of communication with, those parts of his personality that his mother recognizes and responds to, which in some cases include features of personality that she is attributing to him wrongly.” Bowlby (1988) p.132
Reflective Function
“The reflective function refers to the psychological processes underlying the capacity to mentalize. . . mentalizing refers to the capacity to perceive and understand oneself and others’ behavior in terms of mental states, i.e., reflection.”
Fonagy, Steele, Steele & Target (1997)
Reflective Function
Allows the individual to make sense of his or her own and others’ psychological experience, to enter into another’s experience, to “read” another’s mind
Allows the child to make others’ behavior meaningful and predictable, and permits him to respond adaptively
Slade (1999)
Reflective Function
The mother’s capacity to understand the child’s mental states create the context for a secure attachment relationship
The mother is able to view the infant as intentional
Reflective functioning provides protection against damaging effects of abuse and trauma
Slade (1999)
Reflective Function
The capacity to tell a story that is affectively believable
The capacity to understand emotional processes
The ability to accurately understand ones own and others behavior
Slade (2002)

Adult Attachment Interview
Secure-Autonomous– Coherent– Not overwhelmed by emotion– Show compassion, humor, forgiveness,
awareness of unconscious, awareness of lack of perfection

AAI
Preoccupied– No overview– Ramble, get lost in memories– Talk about irrelevant issues– “We did this, that, and the other thing”– Seems angry, passive, or fearful

AAI
Dismissing– Push aside experiences– May idealize parents– Avoid emotional aspects– “Nothing negative in my childhood”
AAI Unresolved
– Lapses in monitoring– Indicate belief that a dead person is still
alive or the person was killed by a childhood thought
– Long silences
Dyadic Patterns Marvin et al (2002)
Secure child – Autonomous Parent– Easily approach and interact when distressed– The reunion calms the child and facilitates
exploration– Child can shift between exploration and using the
parent as a safe harbor with little anxiety– Close attunement – disruptions easily repaired
Dyadic Patterns Marvin et al (2002)
Insecure child – Dismissing Parent– Both partners minimize intimate
attachment-caregiving interactions– Miscue – I’m really more interested in
playing– “Independence” is highly valued– Overregulated affect, little emotional self-
knowledge

Dyadic Patterns Marvin et al (2002)
Insecure Child –
Ambivalent/Preoccupied Parent– Both partners minimize independent
exploration– Child is overly dependent on the parent– Miscue – don’t explore, there really is
something to be anxious about– Under-regulated affect

Dyadic Patterns Marvin et al (2002)
Insecure, Disordered Child
Disorganized/ Insecure Parent– Parent fears or becomes angry in response
to child’s attachment behavior and abdicates caregiving
– Caregiver has unresolved trauma– Role reversed relationship

Maternal Attributions
Fixed beliefs that the mother has about the child – “beliefs that she perceives as objective, accurate perceptions of the child’s essence.”
Lieberman (2000)
Positive Maternal Attributions
“When a mother sees her child as the cutest, most intelligent, most endearing being ever created, she is summoning from the depths of herself the capacity for ecstasy that allows her to put up with the inevitably annoying, exasperating, or simply tedious aspects of raising a child.”
Lieberman (2000)

Maternal Attributions:Protective Function
Child feels adored Allow child to cope with self-doubts and
feelings of despair Allow parent to better tolerate self-
sacrifices that are integral to the parenting process
Lieberman (2000)
Affect Regulation
We must develop in the mother flexible, affectively balanced and coherent representations of the child and the self as a parent.
Slade (2002)
Parental Insightfulness
“Parental empathic understanding involves the capacity to see things from the child’s point of view within a balanced, accepting, and coherent frame.”
Oppenheim (2000)

Balanced
Able to see experiences through their child’s eyes and make attempts to understand the underlying motives
Talk openly about positive and negative aspects
Oppenheim (1999)

One-sided
Preset conception of their child Difficulty staying focused on their child
and their relationship with the child Talk about their own feelings/issues
Oppenheim (1999)
Disengaged
Lack emotional involvement Minimally attempt to understand what’s
on their child’s mind
Oppenheim (1999)Video

Goal of Treatment
Therapy must help the parents place the child’s behavior in the appropriate context in order to facilitate a response to the behavior that will nurture trust and security.
Ports of Entry
Developmental Information Parent-child relationship Projections onto the child
Lieberman (1999)

Treatment Considerations
Secure-Autonomous– Cooperative with treatment– Appreciate attachment issues
Dismissing– Dismiss importance of attachment issues– Uncomfortable, resistant, hostile
Preoccupied– Want help but struggle to focus on task– Enmeshed in their own issues Dozier (2003)

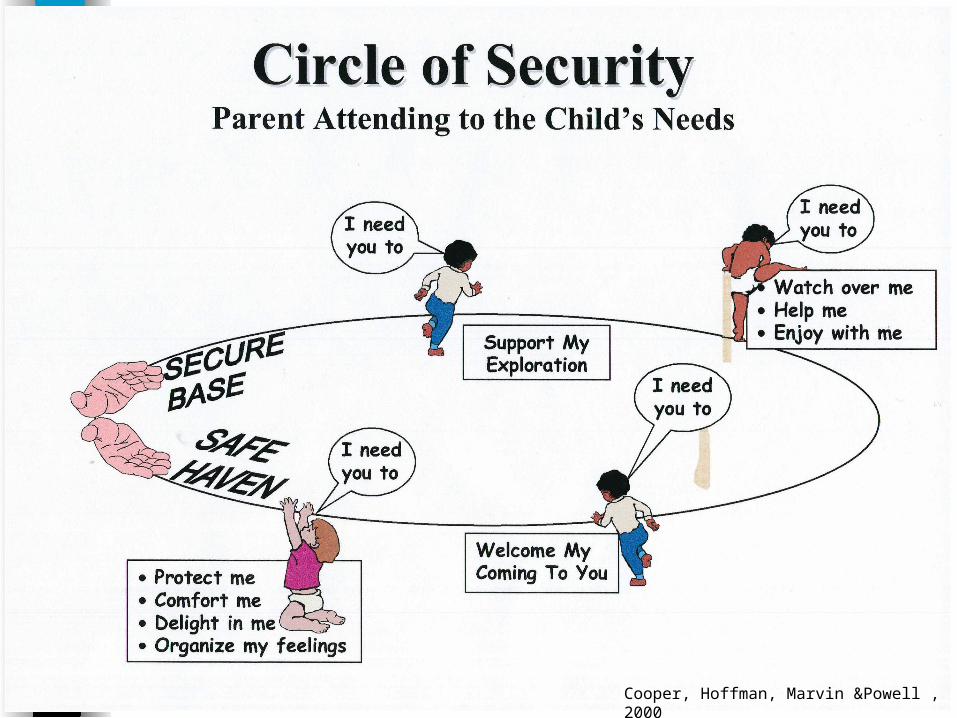
Circle of SecurityMarvin, Cooper, Hoffman & Powell (2002)
Child’s Exploratory System and Needs– The child can move off and explore, if he
believes and expects that the attachment figure will be available if, or when, needed
Attachment System– The child needs the attachment figure to
be available to protect, comfort, delight, and organize his feelings when he becomes overwhelmed
Secure Attachment Formula
Always be bigger, wiser, and kindWhenever possible, follow the
child’s leadWhenever necessary, take charge
Marvin, et al (2002)
Cooper, Hoffman, Marvin &Powell , 2000
Cooper, Hoffman, Marvin &Powell , 2000
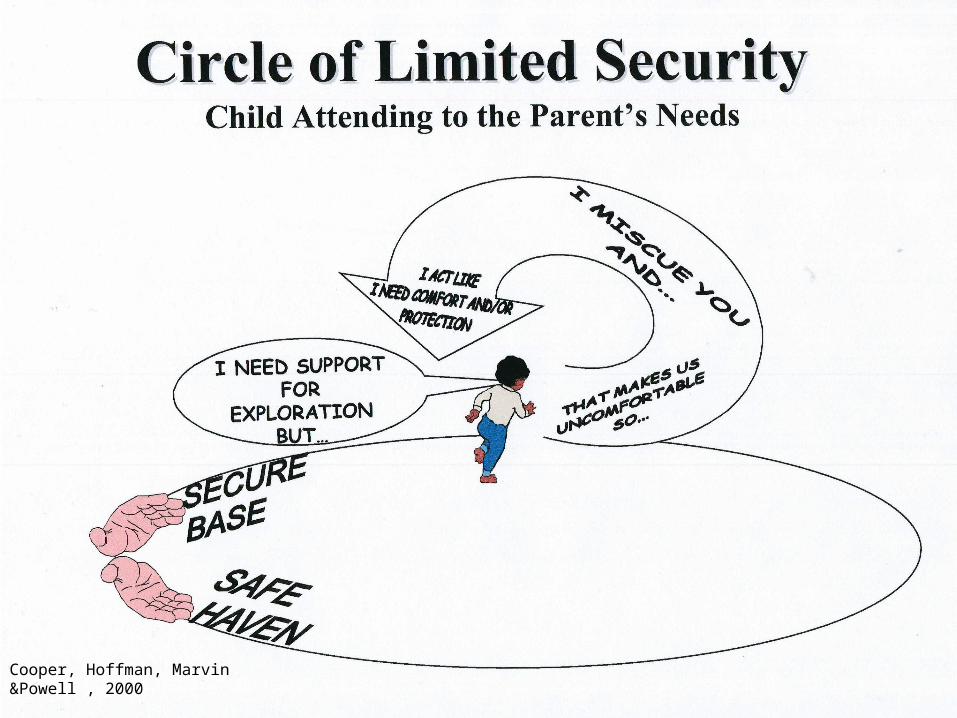
Cooper, Hoffman, Marvin &Powell , 2000

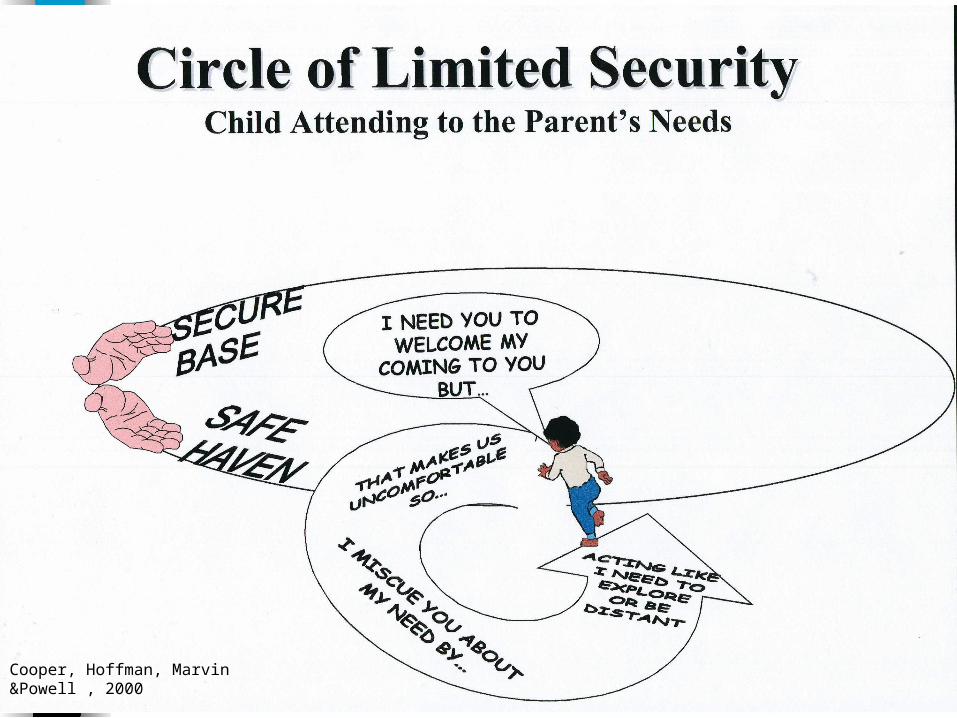
Cooper, Hoffman, Marvin &Powell , 2000

Cooper, Hoffman, Marvin &Powell, 2000
Negative Maternal Attributions
Determine whether and how mother will respond to, misinterpret, or ignore certain behaviors
Lieberman (2000)

Observation of Parent-Child Relationship
Observe proximity seeking behaviors Observe parental sensitivity and
insightfulness Who does child seek out when
frustrated or frightened Use doll play to assess attachment
hierarchy

Assessment – Secure Base
Over the past two weeks can you think of a time when your child was:– Hurt?– Frightened?– Separated from you?
What did your child do? How did you respond?
Assessment of Parent’s Point of View Interview questions:
– Could you give me a thumbnail sketch of your child?
– Tell me about a time in the past two weeks when you and your child really clicked.
– Tell me about a time when you didn’t.– What gives you the most joy in your relationship?– What gives you the most pain?– Where do you turn for emotional support?
Steele (2003)
Treatment ConsiderationsExample of Typical Process
Parent complains about the child’s destructive behavior
The therapist understands how upsetting the behavior must be to the parents
The therapist responds by discussing ways to control the destructive behavior

Empathic Therapeutic Failures
It is critical for the clinician to avoid making the faulty assumption that it is obvious why the referral behavior was so offensive to the parent. We must, instead, “get into the parent’s head.”
Treatment ConsiderationsAvoiding Empathic Failures
Avoid being an “expert” Be careful not to intellectualize Avoid being in a hurry to solve the
problem The goal of the process is to
thoughtfully explore with the parent the impact of the child’s behavior

Thoughtful Exploration
Don’t jump to your own conclusion, let the parent’s responses guide you.
Wonder aloud why the behavior of this child is so distressing for this parent.
Listen for emotionally laden words,
e.g. “Control”, “manipulate”.

Parental Empathic Understanding
“Parental empathic understanding involves the capacity to see things from the child’s point of view within a balanced, accepting, and coherent frame.”
Oppenheim (2000)

Goal of Treatment
Therapy must help the parents place the child’s behavior in the appropriate context in order to facilitate a response to the behavior that will nurture trust and security.
Circle of Security
Understanding Secure Base– Did/Does parent have a secure base?
Negative Projections– He doesn’t care if I’m there for him– He doesn’t need me– She gets so frantic it’s like she’s crazy!

Safe Haven
Comfort level with nurturing Emotional/Physical availability Negative projections
Treatment Approaches
Bridging affect Present the child’s point of view “Challenge” the parent’s interpretation
of the child’s behavior

Secure Base Interventions
Nurturing Anticipating needs Helping child regulate emotions Parental emotional availability Structure and consistency Experience of being in one’s mind

Time In
Stay close by to help the child calm down
Avoid processing until the child is calm If child becomes aggressive distance
yourself while reassuring the child that you’ll be available once the child is calm
Secure Base
“When a child is held in mind, the child feels it, and knows it. There is a sense of safety, of containment, and, most important, existence in that other, which has always seemed to me vital. . . It seems to me that one of life’s greatest privileges is just that – the experience of being held in someone’s mind.”
Pawl (1995)