
Detection of survivin and p53 in human oral cancer: Correlation with clinicopathologic findings
10
ORIGINAL ARTICLE DETECTION OF SURVIVIN AND p53 IN HUMAN ORAL CANCER: CORRELATION WITH CLINICOPATHOLOGIC FINDINGS Zakir Khan, PhD, 1 * Ram P. Tiwari, PhD, 2† Rita Mulherkar, PhD, 3 Nand K. Sah, PhD, 1 Godavarthi BKS Prasad, PhD, 4 Braj R. Shrivastava, PhD, 5 Prakash S. Bisen, DSc 1 1 Department of Biotechnology, Madhav Institute of Technology and Science, Race Course Road, Gwalior 474005, India. E-mail: [email protected] 2 Diagnostic Division, Nicholas Piramal India Limited, Pawane, Navi Mumbai 400705, India 3 Advance Centre for Treatment, Research and Education in Cancer (ACTREC), Tata Memorial Centre, Kharghar, Navi Mumbai 410 210, India 4 School of Studies in Biotechnology, Jiwaji University, Gwalior 474011, India 5 College of Life Sciences, Cancer Hospital and Research Institute, Gwalior 474001, India Accepted 29 October 2008 Published online 1 April 2009 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/hed.21071 Abstract: Background. Survivin, an inhibitor of apoptosis, is overexpressed in cancer. It has been implicated in both preven- tion of apoptosis and cell cycle regulation. We investigated the distribution of antiapoptotic protein survivin in 29 oral squamous cell carcinoma (OSCC) and 16 oral premalignant lesions. It has been suggested that wild-type p53 represses survivin expression. Therefore, we investigated the status of p53 in relation to survivin to determine the potential involvement in oral tumorigenesis. Methods. Oral cancer tissues were freshly obtained at the time of surgery and classified as per general rules of head and neck cancer (TNM classification). Immunohistochemistry and reverse transcriptase-polymerase chain reaction were con- ducted to study the expression of survivin and p53. The Fish- er’s exact test was employed to determine the association of survivin and p53 with clinicopathologic parameters of the sub- jects being studied. Results. Positive staining for survivin was found in 72% OSCC and 44% oral premalignant lesions with no immunoreac- tions in the corresponding normal tissues. For p53, 59% OSCC, 38% premalignant lesions, and 14% normal tissues were positive. Importantly, about half of the p53-positive OSCC and premalignant tissues also showed survivin positiv- ity (28% OSCC and 18% premalignant lesions). Further, it is observed that the number of survivin positive cells was signif- icantly higher in the p53-positive group. Survivin is expressed in a varying proportion of cells, and in majority of patients it was localized in cytoplasm, whereas p53 is strictly restricted to the nucleus. The survivin expression levels in both primary OSCC and premalignant lesions were significantly higher than in normal oral tissues (OSCC, p < .0008; premalignant lesions, p < .04). No significant correlations between survivin and p53 expression with clinicopathologic parameters were found. Conclusions. Frequent overexpression of apoptosis regula- tors, survivin and p53, in OSCC as well as in oral premalignant lesions were found. Overexpression of these 2 markers in pre- malignant lesions suggest a role in early stages of oral carcinogenesis. V V C 2009 Wiley Periodicals, Inc. Head Neck 31: 1039–1048, 2009 Keywords: oral squamous cell carcinoma (OSCC); survivin; p53; apoptosis; immunohistochemistry Correspondence to: P. S. Bisen *Current address: INSERM U841, IMRB-Faculty of Medicine, Department of Neurosciences, Paris University, F-94010 Cre ´ teil, Paris, France. . † Current address: Production and Development Division, Trinity Biotech (Nigeria) Ltd., Shestco Complex, Sheda, Abuja, Nigeria. V V C 2009 Wiley Periodicals, Inc. Detection of Survivin and p53 in Human Oral Cancer HEAD & NECK—DOI 10.1002/hed August 2009 1039
-
Upload
zakir-khan -
Category
Documents
-
view
215 -
download
1
Transcript of Detection of survivin and p53 in human oral cancer: Correlation with clinicopathologic findings
ORIGINAL ARTICLE
DETECTION OF SURVIVIN AND p53 IN HUMAN ORAL CANCER:CORRELATION WITH CLINICOPATHOLOGIC FINDINGS
Zakir Khan, PhD,1* Ram P. Tiwari, PhD,2† Rita Mulherkar, PhD,3 Nand K. Sah, PhD,1
Godavarthi BKS Prasad, PhD,4 Braj R. Shrivastava, PhD,5 Prakash S. Bisen, DSc1
1Department of Biotechnology, Madhav Institute of Technology and Science, Race Course Road, Gwalior474005, India. E-mail: [email protected] Division, Nicholas Piramal India Limited, Pawane, Navi Mumbai 400705, India3Advance Centre for Treatment, Research and Education in Cancer (ACTREC), Tata Memorial Centre,Kharghar, Navi Mumbai 410 210, India4 School of Studies in Biotechnology, Jiwaji University, Gwalior 474011, India5College of Life Sciences, Cancer Hospital and Research Institute, Gwalior 474001, India
Accepted 29 October 2008Published online 1 April 2009 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/hed.21071
Abstract: Background. Survivin, an inhibitor of apoptosis, is
overexpressed in cancer. It has been implicated in both preven-
tion of apoptosis and cell cycle regulation. We investigated the
distribution of antiapoptotic protein survivin in 29 oral squamous
cell carcinoma (OSCC) and 16 oral premalignant lesions. It has
been suggested that wild-type p53 represses survivin expression.
Therefore, we investigated the status of p53 in relation to survivin
to determine the potential involvement in oral tumorigenesis.
Methods. Oral cancer tissues were freshly obtained at the
time of surgery and classified as per general rules of head
and neck cancer (TNM classification). Immunohistochemistry
and reverse transcriptase-polymerase chain reaction were con-
ducted to study the expression of survivin and p53. The Fish-
er’s exact test was employed to determine the association of
survivin and p53 with clinicopathologic parameters of the sub-
jects being studied.
Results. Positive staining for survivin was found in 72%
OSCC and 44% oral premalignant lesions with no immunoreac-
tions in the corresponding normal tissues. For p53, 59%
OSCC, 38% premalignant lesions, and 14% normal tissues
were positive. Importantly, about half of the p53-positive
OSCC and premalignant tissues also showed survivin positiv-
ity (28% OSCC and 18% premalignant lesions). Further, it is
observed that the number of survivin positive cells was signif-
icantly higher in the p53-positive group. Survivin is expressed
in a varying proportion of cells, and in majority of patients it
was localized in cytoplasm, whereas p53 is strictly restricted
to the nucleus. The survivin expression levels in both primary
OSCC and premalignant lesions were significantly higher than
in normal oral tissues (OSCC, p < .0008; premalignant
lesions, p < .04). No significant correlations between survivin
and p53 expression with clinicopathologic parameters were
found.
Conclusions. Frequent overexpression of apoptosis regula-
tors, survivin and p53, in OSCC as well as in oral premalignant
lesions were found. Overexpression of these 2 markers in pre-
malignant lesions suggest a role in early stages of oral
carcinogenesis. VVC 2009 Wiley Periodicals, Inc. Head Neck
31: 1039–1048, 2009
Keywords: oral squamous cell carcinoma (OSCC); survivin;
p53; apoptosis; immunohistochemistry
Correspondence to: P. S. Bisen
*Current address: INSERM U841, IMRB-Faculty of Medicine,Department of Neurosciences, Paris University, F-94010 Creteil, Paris,France..†Current address: Production and Development Division, Trinity Biotech(Nigeria) Ltd., Shestco Complex, Sheda, Abuja, Nigeria.
VVC 2009 Wiley Periodicals, Inc.
Detection of Survivin and p53 in Human Oral Cancer HEAD & NECK—DOI 10.1002/hed August 2009 1039

Development of oral cancer is a multistepprocess associated with increasing genetic in-stability involving activation of oncogenes andinactivation of tumor suppressor.1–3 Mostpatients of human carcinogenesis seem to becharacterized, in the early stages, by loss ofmechanisms regulating cell cycle progression,cell death/viability balance, and apoptosis. Apo-ptosis preserves normal homeostasis and organmorphogenesis.4–6 An aberration of this processmay contribute to carcinogenesis by prolongingthe cell, viability resulting in the accumulationof transformation mutations.7 It has nowbecome evident that apart from uncontrolledproliferation, many genetic alterations occurwithin tumor cells, which actively suppress apo-ptosis.8,9 The molecular pathways in the execu-tion of apoptotic cell death are highly conservedevolutionarily, as are their regulators.8–10
Recently, a novel gene encoding a structur-ally unique IAP apoptosis inhibitor, designatedas survivin, has been identified. Survivin is a16.5 kDa protein with a single BIR (baculovirusIAP repeat) and no RING finger.11,12 It is unde-tectable in terminally differentiated adult tis-sues but becomes notably expressed in the mostcommon human cancers, including stomach,12
colorectal,13 lung, breast, pancreatic, and pros-tate cancers and high-grade non-Hodgkin’s lym-phomas in vivo.14,15 In malignant cells, survivinexpression is upregulated during the G2/Mphase of the cell cycle and peaks during mito-sis.12–16 Overexpression of survivin in cancermay overcome cell-cycle checkpoints, to facilitateaberrant progression of transformed cellsthrough mitosis.11,16–18 Survivin expression issignificantly associated with poor clinical out-come in cancers such as neuroblastoma, colorec-tal cancer, breast cancer, lung cancer, andesophageal cancer.15,19–23 In gastric and esopha-geal cancer, expression of survivin was studiedwith respect to p53 protein, which frequentlyshares the early steps of carcinogenesis.12,24
Survivin expression and its relation with p53 inoral carcinogenesis has not been widely studied.
In the present study, we investigated survivinexpression with respect to p53 protein and itsassociation with clinical outcome in oral cancer.
PATIENTS AND METHODS
Specimens. Oral cancer tissues including 29oral squamous cell carcinoma (OSCC) and 16
oral premalignant lesions were freshly obtainedat the time of surgery from Cancer Hospital andResearch Institute (CHRI) and Jayarogya Groupof Hospitals, Gwalior (Madhya Pradesh) India,after obtaining due consent from the patientsunder a protocol reviewed and approved by acommittee constituted for the purpose by theBoard of Management of the Hospital. Normalspecimen was obtained from area far from thepremalignant lesions. Biopsy or resected speci-mens were immediately frozen and stored in liq-uid nitrogen as well as bit parts of the allspecimens were formalin-fixed and paraffin-em-bedded. Tumor size and clinicopathologic stage ofOSCC and other samples were classified accord-ing to the general rules of head and neck cancer(TNM classification). Tumor samples werechecked to ensure that tumor tissue was present.
Immunohistochemistry. Expression of p53 andsurvivin in tumor samples of different develop-mental stages was examined by immunohisto-chemistry. Samples were fixed in neutral 10%formalin and embedded in paraffin after resec-tion. Five-micrometer-thick sections were cutand transferred on to the slide, deparaffinizedin xylene, and dehydrated in graded ethanol.Endogenous peroxidase activity was blocked byimmersing the slides in 1% hydrogen peroxidein phosphate saline buffer (PBS, 137 mM NaCl,10 mM phosphate, 2.7 mM KCl, pH 7.4) for 1hour at room temperature and rinsed with dis-tilled water. Microwave antigen retrieval wascarried out by placing the slides in 10 mM so-dium citrate buffer (pH 6) in a microwave ovenat 800 W for 10 minutes and then allowed tocool. Nonspecific binding of the antibody wasblocked by 20% fetal calf serum in phosphate-buffered saline (PBS). Immunostaining wasperformed by using avidin-biotin peroxidaseenzyme complex (ABC kit, vector laboratory,Denmark). The sections were incubated withpolyclonal anti-survivin antibody (Santa Cruz,sc-10811, 1 : 500) or monoclonal anti-p53 anti-body (Sigma, P 5813, 1 : 500) and subsequentlyplaced in secondary anti-rabbit antibody for sur-vivin or anti-mouse antibody for p53 (SantaCruz) followed by avidin-biotin complex (DakoA/S, Denmark) reagent. The sections werefinally incubated in the substrate 3,30
diaminobenzidine (0.05%) and 0.1% hydrogenperoxide for 10 minutes. The intensity of immu-nohistochemical staining was graded as nega-tive and positive. The grade of staining was
1040 Detection of Survivin and p53 in Human Oral Cancer HEAD & NECK—DOI 10.1002/hed August 2009

converted into numerical scores. Overexpressionwas considered if the index was higher than10%. The area with the maximum number ofpositive cells was considered in each section,and the slides were coded and examined blindly.
RT-PCR. Extraction of RNA and reverse tran-scriptase-polymerase chain reaction (RT-PCR)was performed according to the manufacturer’sinstructions. Briefly, total RNA was extractedfrom tumoral and nonneoplastic tissue sampleswith Trizol reagent (Invitrogen) following themanufacturer’s protocol. RNA purity was con-firmed by spectrophotometry (260/280 nm ratio),and its integrity was established by agarosegels. Total RNA (2 lg) was reverse-transcribedin a final 20 lL reaction volume using 15 UThermoScript reverse transcriptase, 2.5� RTbuffer, and random hexamers (Thermo-ScriptRT-PCR, Invitrogen). PCR reactions contained0.25 lL amplitaq gold polymerase (Applied Bio-systems, ROCHE), 2.5 lL 10� reaction buffer, 0.5lL dNTP mixture (10 mM), 1 lL sense primer(10 lM), 1 lL anti-sense primer (10 lM), and 1lL cDNA in a 25 lL final volume. The followingprimers were used: (A) survivin gene, forwardprimer 50-CCCTGCCTGGCAGCCCT TTC-30, andreverse primer 50-CTGGCTCCC AGCCTTCCA-30
(PCR product, 188 bp); (B) p53 gene, forwardprimer, 50-TAC ATG TGT TAA CAG TTC CTGCA-30; reverse primer, 50-TTC TGA CAA CGATCG GAG GA-30 (PCR product, 282-bp); (C) glyc-eraldehyde-3-phosphate dehydrogenase, forwardprimer 50-AGGGGTCTA CATGGCAACTG-30, andreverse primer 50-CGACCACTTTGTCAAGCTCA-30 (PCR product, 227 bp).
Statistical Analysis. The correlation betweenthe expression of survivin/p53 and the clinico-pathologic features was analyzed by using theFisher’s exact test. A probability value of <.05was considered significant.
RESULTS
Patients and Samples Characteristics. The cohortconsisted of 45 patients with oral cancer andoral lesions. The study included 39 specimensfrom men and 6 from women, with a medianage of 42.5 years (range, 20–65 years). Tumorsize varied from 1.1 to 6 cm, with a mean of 3.7cm. Primary sites of cancer in different subjectswere as follows: buccal mucosa, 19 patients
(40.4%); tongue, 11 (23.4%); lip, 5 (10.6%); alveo-lus, 5 (10.6%); floor of mouth, 5 (10.6%). Grada-tion of tumors was performed according to thegeneral rules of head and neck cancer (TNMclassification). Six patients (20.6%) had stage I,7 had stage II (24.1%), 10 had stage III (34.4%),and 4 had stage IV (3.7%), and 2 were unidenti-fied. The histologic grades of 29 carcinoma wereas follows: 9 well differentiated, 12 moderately,and 8 poorly differentiated. Sixteen putativepremalignant lesions constituting 9 leukoplakia,2 submucous fibrosis, and 2 erythroplakia, and3 others were identified. Seven normal tissuesfrom areas away from premalignant lesion siteof the same tissues were collected and used ascontrol (Table 1).
Survivin Analysis. In imunohistochemical analy-sis, all 7 normal oral mucosa patients showed
Table 1. Patient characteristics and tumor features.
Patient and sample characteristics No.
Total patients 45
Median age, y 42.5
Sex
Male 39
Female 6
Tumor site
Buccal mucosa 19
Tongue 11
Lip 5
Others 10
Tumor size
<2 cm 9
>2 cm 20
T-Primary tumor
T1 þ T2 24
T3 þ T4 5
N-Nodal status
N (þ) 14
N (�) 15
Stage
I þ II 15
III þ IV 14
Histopathology
OSCC 29
Well-differentiated 9
Moderately differentiated 12
Poorly differentiated 8
Premalignant lesion 16
Leukoplakia 9
Submucous fibrosis 2
Erythoplakia 2
Other 3
Normal* 7
Abbreviation: OSCC, oral squamous cell carcinoma.*Normal samples were collected from the area away from the premalig-nant lesion site.
Detection of Survivin and p53 in Human Oral Cancer HEAD & NECK—DOI 10.1002/hed August 2009 1041

survivin phenotype. Among the carcinomas, 21of 29 (72%) revealed survivin expression in tu-mor tissues. More interestingly, 7 of 16 (44%)subjects with premalignant lesions were consid-ered survivin positive. A significant difference in
survivin immunoexpression was observed withrespect to the histologic grade. The survivinexpression levels in both primary OSCCand premalignant lesions were significantlyhigher than that in normal oral tissues (OSCC,
FIGURE 1. Representative results of immunohistochemical staining for survivin. (A) Normal tissue, (B) leukoplakia, (C) submucous fi-
brosis, (D) erythroplakia, (E) OSCC. Immunohistochemical analysis was used to analyze distribution of survivin in all cases in which
paraffin-embedded tissue sections (5 lm) were stained with anti-human survivin antibodies. Normal tissues from area far from prema-
lignant lesions site of the same tissues were used as control. Brown color showing immunoreactions for survivin. [Color figure can be
viewed in the online issue, which is available at www.interscience.wiley.com.]
1042 Detection of Survivin and p53 in Human Oral Cancer HEAD & NECK—DOI 10.1002/hed August 2009
p < .0008; premalignant lesions, p < .04) Incontrast, we found no significant difference insurvivin-IHC scores between OSCC and prema-lignant (p ¼ .057). Survivin immunoexpressionindex was not significantly associated with theother clinical variables analyzed (Figures 1–3,Table 2). The expression pattern of survivin was
further evaluated with respect to intracellularlocalization between OSCC and premalignantlesions. Nuclear expression was found to be pos-itive in 14 of 21 (66%) survivin-positive OSCCtissues, whereas cytoplasmic expression wasfound in all of 21 (100%). In case of premalig-nant lesions, there is no major difference
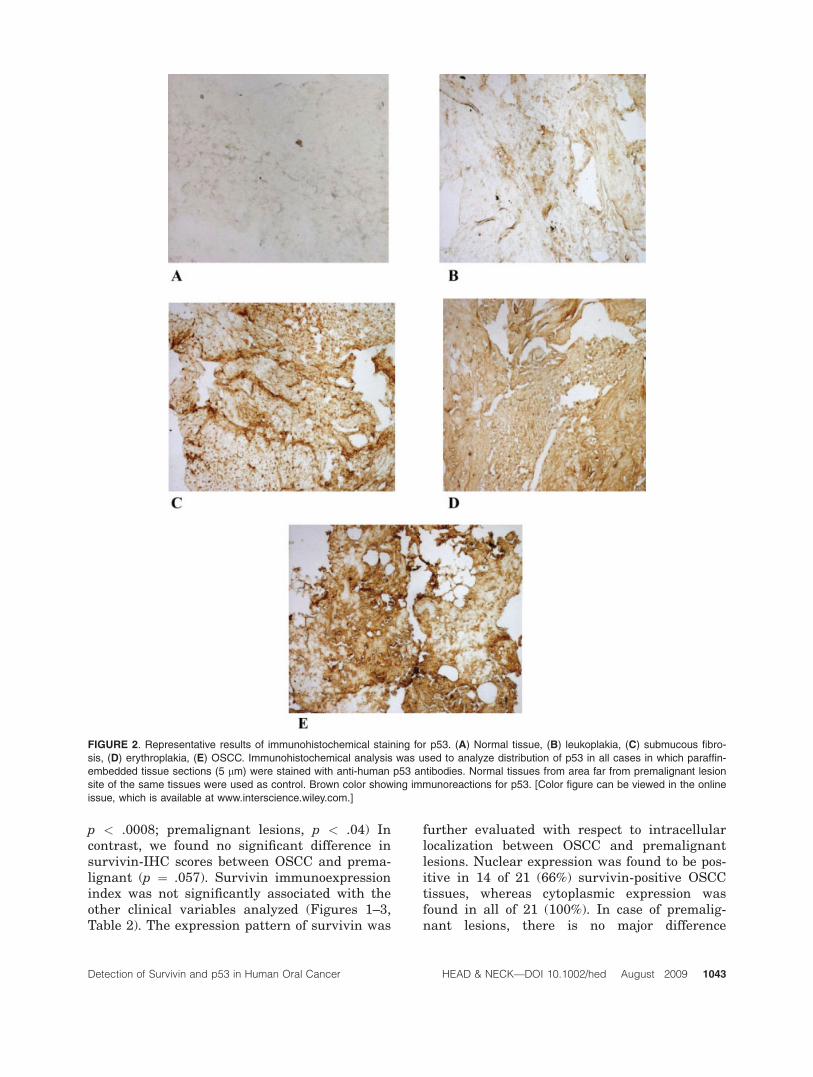
FIGURE 2. Representative results of immunohistochemical staining for p53. (A) Normal tissue, (B) leukoplakia, (C) submucous fibro-
sis, (D) erythroplakia, (E) OSCC. Immunohistochemical analysis was used to analyze distribution of p53 in all cases in which paraffin-
embedded tissue sections (5 lm) were stained with anti-human p53 antibodies. Normal tissues from area far from premalignant lesion
site of the same tissues were used as control. Brown color showing immunoreactions for p53. [Color figure can be viewed in the online
issue, which is available at www.interscience.wiley.com.]
Detection of Survivin and p53 in Human Oral Cancer HEAD & NECK—DOI 10.1002/hed August 2009 1043

between cytoplasmic versus nuclear localizationof survivin expression. All 7 survivin-positivepremalignant tissues were showing cytoplasmicexpression of survivin, whereas 6 of 7 showednuclear localization as well (Table 3).
p53 Analysis. The expression pattern of p53 inthe same tumor tissues was determined byimmunohistochemistry (see Figure 2). All 7 nor-mal oral mucosa cases were negative for p53,except 1 case which showed slight immunoreac-tivity for p53. Furthermore, 17 of 29 OSCC(59%), 2 of 9 leukoplakia (22%), 2 of 4 submu-cous fibrosis (50%), erythroplakia, and 1 of 3(34%) other premalignant lesions were p53 pos-itive. Mean percentage for p53 positivity intissues of premalignant lesions was (6 of 16)38%. Slightly more prominent alteration wasobserved in p53 immunoexpression in lymphnode–positive carcinoma (73%) when comparedwith lymph node–negative cases (47%). Therewas no correlation between p53 expression andclinicopathologic parameters (Figures 2 and 3,Table 2). The p53 immunoreativity was re-stricted to the nuclei, generally with high inten-sity, and a few cases showed both nuclear andcytoplasmic positive phenotype (Table 3).
Relationship between Survivin and p53. The com-bined expression patterns of survivin and p53 inOSCC and oral premalignant lesions were ana-lyzed in relation to clinicopathologic features.The percentage of survivin and p53 positivity in
various histologic groups and tumor stages ispresented graphically in Figure 4. It is notewor-thy that 28% OSCC and 18% oral premalignantlesions demonstrated expression of both survivinand p53. The coexpression of survivinþ/p53þwas seen in about 20% of patients irrespectiveof tumor size (T1 or T2 or T3 or T4). Of 8 poorlydifferentiated patients, 3 patients (37.5%) weresurvivinþ/p53þ; of 12 moderately differentiatedpatients 2 (16.6%) were survivinþ/p53þ, andonly 1 of 9 well differentiated patients (11.1)showed survivinþ/p53þ phenotype. In 14patients with lymph node metastasis, 4 patients(28.5%) were survivinþ/p53þ and 10 patients(71.5%) showed lack of coexpression. Withrespect to tumor stage, 4 patients of I–II group(26.6%) and 2 patients of III–IV group (14.2)were survivinþ/p53þ, whereas 11 patients(73.4%) of I–II and 12 patients (85.8%) of III–IVshowed lack of coexpression (Table 4). Consider-ing premalignant lesions, leukoplakia was foundmore positive for survivin (44%) in comparisonto p53 (22%). In total 9 patients of leukoplakia,2 patients were survivinþp53þ and 1 patient oferythroplakia showed survivinþp53þ pheno-type. Statistical analysis revealed that coexpres-sion of survivin, and p53 is not significantlyassociated with clinicopathologic parameterssuch as tumor size (p ¼ 1.000), stages (p ¼.6513), lymph node metastasis (p ¼ .3898), andtumor differentiation (p ¼ .386) (Table 4).
RT-PCR. Using RT-PCR analysis, we examinedthe expression levels of survivin and p53 mRNAin 29 OSCC, 16 premalignant lesions and 7 nor-mal tissues from whom RNA was available fromprimary tumors. No normal tissue, with theexception of 1 case, had p53 expression, whereasthe expression of survivin and p53 weredetected, respectively, in 22 (79%) and 15 (59%)OSCC tissues tested (see Figure 5). Theseresults are entirely consistent with the detectionof survivin protein in 72% and p53 in 59% ofOSCC from the same cohort of patients. In total16 premalignant lesions 8 (50%) were survivinþ,whereas 6 (38%) showed p53 expression. No sta-tistical significance was observed between thepresence of the gene expression and clinicopath-ologic features studied (data not shown).
DISCUSSION
The present study demonstrates frequent over-expression of apoptosis-regulating proteins
FIGURE 3. Relationship of survivin and p53 expression with dif-
ferent major histological groups. Survivin expressions in OSCC
and premalignant lesions (PL) were significantly higher than in
normal oral tissues (OSCC, p < 0.0008; PL < 0.04).
1044 Detection of Survivin and p53 in Human Oral Cancer HEAD & NECK—DOI 10.1002/hed August 2009

survivin and p53 in oral cancers. The expressionof survivin was detected in more than half ofthe specimens obtained from OSCC (72%),whereas absence of survivin was observed innormal tissues. The accumulation of mutatedp53 protein was detected in 59% of OSCC sub-
jects and 1 of 7 normal subjects also showedslight positivity for p53. In addition, aberrantsurvivin and p53 expression were observed inpremalignant lesions. Forty-four percent prema-lignant patients were survivin-positive whereas38% showed p53 positivity.
Table 3. Subcellular localization of survivin and p53 in positive samples.
Proteins
Subcellular localization
Histology Total positiveNucleus, % Cytoplasm, % NucleusþCytoplasm, %
Survivin 14 (66) 21 (100) 14 (66) OSCC 21
p53 15 (89) 2 (11) 6 (35) OSCC 17
Survivin 6 (85) 7 (100) 6 (85) PL 7
p53 6 (100) 1 (16) 1 (16) PL 6
Abbreviations: OSCC, oral squamous cell carcinoma; PL, premalignant lesion.
Table 2. Statistical correlation of survivin and p53 expression with clinicopathological features.
Characteristics Total
Results of immunohistochemistry
Survivin (�), % Survivin (þ), % p value p53 (�), % p53 (þ), % p value
Total patients 45
Age, y
<60 39 14 (36) 27 (69) .6529 20 (51) 21 (53) 1.0000
>60 6 3 (50) 3 (50) 3 (50) 3 (50)
Sex
Male 39 16 (39) 25 (61) .3958 20 (51) 21 (54) 1.0000
Female 6 1 (17) 5 (83) 3 (50) 3 (50)
T-primary tumor
T1þT2 24 7 (29) 17 (71) 1.0000 9 (37) 15 (63) .6221
T3þT4 5 1 (20) 4 (80) 3 (60) 2 (40)
Stage
IþII 15 4 (26) 11 (74) 1.0000 7 (47) 8 (53) .7104
IIIþIV 14 4 (29) 10 (71) 5 (36) 9 (64)
Tumor size
<2cm 9 2 (22) 7 (78) 1.0000 4 (44) 5 (56) 1.0000
>2cm 20 6 (30) 14 (70) 8 (40) 12 (60)
N-Nodal status
N (þ) 14 4 (28) 10 (72) 1.0000 4 (28) 10 (72) .2635
N (�) 15 4 (27) 11 (73) 8 (53) 7 (47)
Histological type
OSCC
Well differentiated 9 3 (33) 6 (67) .06749 4 (44) 5 (56) 1.0000
Moderately differentiated þ 20 5 (25) 15 (75) 8 (40) 12 (60)
Poorly differentiated
Premalignant lesions
Leukoplakia 9 5 (56) 4 (44) 1.0000 6 (67) 3 (33) .5961
Others 7 4 (57) 3 (43) 4 (57) 3 (43)
OSCC 29 8 (28) 21 (72) .0007 12 (41) 17 (59) .08
Normal tissue 7 7 (100) 0 (0) 6 (66) 1 (14)
Premalignant lesions 16 9 (56) 7 (44) .0466 10 (62) 6 (38) .2753
Normal 7 7 (100) 0 (0) 6 (66) 1 (14)
OSCC 29 8 (28) 21 (72) .0579 12 (41) 17 (59) .1480
Premalignant lesion 16 9 (56) 7 (44) 10 (62) 6 (38)
Tumor site
Buccal mucosa 19 7 (37) 12 (63) 1.0000 10 (53) 9 (47) .7701
Others 26 10 (38) 18 (69) 13 (50) 15 (57)
Abbreviation: OSCC, oral squamous cell carcinoma.
Detection of Survivin and p53 in Human Oral Cancer HEAD & NECK—DOI 10.1002/hed August 2009 1045
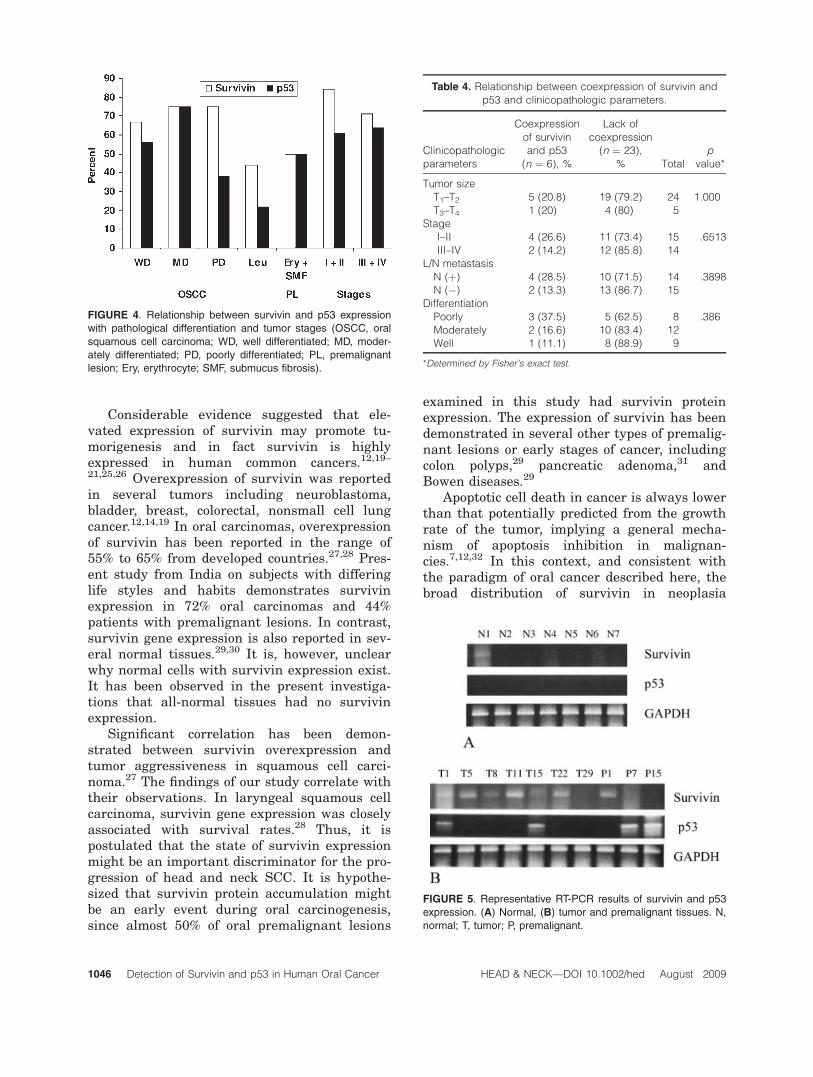
Considerable evidence suggested that ele-vated expression of survivin may promote tu-morigenesis and in fact survivin is highlyexpressed in human common cancers.12,19–21,25,26 Overexpression of survivin was reportedin several tumors including neuroblastoma,bladder, breast, colorectal, nonsmall cell lungcancer.12,14,19 In oral carcinomas, overexpressionof survivin has been reported in the range of55% to 65% from developed countries.27,28 Pres-ent study from India on subjects with differinglife styles and habits demonstrates survivinexpression in 72% oral carcinomas and 44%patients with premalignant lesions. In contrast,survivin gene expression is also reported in sev-eral normal tissues.29,30 It is, however, unclearwhy normal cells with survivin expression exist.It has been observed in the present investiga-tions that all-normal tissues had no survivinexpression.
Significant correlation has been demon-strated between survivin overexpression andtumor aggressiveness in squamous cell carci-noma.27 The findings of our study correlate withtheir observations. In laryngeal squamous cellcarcinoma, survivin gene expression was closelyassociated with survival rates.28 Thus, it ispostulated that the state of survivin expressionmight be an important discriminator for the pro-gression of head and neck SCC. It is hypothe-sized that survivin protein accumulation mightbe an early event during oral carcinogenesis,since almost 50% of oral premalignant lesions
examined in this study had survivin proteinexpression. The expression of survivin has beendemonstrated in several other types of premalig-nant lesions or early stages of cancer, includingcolon polyps,29 pancreatic adenoma,31 andBowen diseases.29
Apoptotic cell death in cancer is always lowerthan that potentially predicted from the growthrate of the tumor, implying a general mecha-nism of apoptosis inhibition in malignan-cies.7,12,32 In this context, and consistent withthe paradigm of oral cancer described here, thebroad distribution of survivin in neoplasia
FIGURE 4. Relationship between survivin and p53 expression
with pathological differentiation and tumor stages (OSCC, oral
squamous cell carcinoma; WD, well differentiated; MD, moder-
ately differentiated; PD, poorly differentiated; PL, premalignant
lesion; Ery, erythrocyte; SMF, submucus fibrosis).
Table 4. Relationship between coexpression of survivin and
p53 and clinicopathologic parameters.
Clinicopathologic
parameters
Coexpression
of survivin
and p53
(n ¼ 6), %
Lack of
coexpression
(n ¼ 23),
% Total
p
value*
Tumor size
T1–T2 5 (20.8) 19 (79.2) 24 1.000
T3–T4 1 (20) 4 (80) 5
Stage
I–II 4 (26.6) 11 (73.4) 15 .6513
III–IV 2 (14.2) 12 (85.8) 14
L/N metastasis
N (þ) 4 (28.5) 10 (71.5) 14 .3898
N (�) 2 (13.3) 13 (86.7) 15
Differentiation
Poorly 3 (37.5) 5 (62.5) 8 .386
Moderately 2 (16.6) 10 (83.4) 12
Well 1 (11.1) 8 (88.9) 9
*Determined by Fisher’s exact test.
FIGURE 5. Representative RT-PCR results of survivin and p53
expression. (A) Normal, (B) tumor and premalignant tissues. N,
normal; T, tumor; P, premalignant.
1046 Detection of Survivin and p53 in Human Oral Cancer HEAD & NECK—DOI 10.1002/hed August 2009

seems ideally positioned to mediate a general-ized apoptosis inhibition, potentially contri-buting to tumor progression and multidrugresistance.14
There is an emerging body of evidence thatpersons who develop squamous carcinoma of thehead and neck may have undergone alterationsin p53 genes.33,34 In addition, there is evidencethat altered p53 genes may cooperate with otheroncogenes, to generate cells with a growthadvantage for tumor progression. For its role intranscriptional repression,35 potentially involv-ing apoptosis inhibitors like bcl-2, it is possiblethat p53 may negatively regulate survivin geneexpression in a mechanism potentially disruptedby cancer-associated mutations of p53. Giventhe high frequency of p53 mutations in allhuman cancers, this may explain the dramaticderegulated expression of survivin in diversetypes of tumors14 and its absence in neighboringnormal tissues. In vitro studies have shown thatsurvivin expression is regulated in transcrip-tional response by wt-p53,36,37 or by wt-adeno-matous polyposis coli protein.38 In gastriccancer, a significant correlation was foundbetween survivin expression and accumulationof mutant p53.12 It would therefore be interest-ing to determine the survivin expression in rela-tion to tumor suppressor in OSCC.
We detected p53 alteration in 59% of tumorsfrom patients with OSCC and 38% premalignantlesions. These results support prior data, sug-gesting that p53 mutation is an early event inoral cancer pathogenesis often detected in pre-malignant lesions.39,40. We found that approxi-mately 50% p53þ tissues were also survivinþ,although the coassociation of survivin with p53is not statistically significant.12 The lack of coex-pression of p53 and survivin (Figure 5 and Table4) suggests that p53 is not perhaps a major con-tributor to survivin deregulation in oral cancer,although it is possible that p53 contributes tosurvivin deregulation in a subset of oral cancer.These studies thus indicate alterations in survi-vin and p53 expression may play an importantrole in oral tumorigenesis probably by inhibitingapoptosis. In addition, high percentage of survi-vin and p53 overexpression in premalignantlesions suggested early involvement in oral can-cer development.
Acknowledgments. We thank Dr. IK Patro(School of Studies in Neuroscience, Jiwaji Uni-
versity, Gwalior) for his excellent assistance inthe entire course of study and Ms. SadhanaKannan (Biostatistician, ACRTEC, Tata Memo-rial Centre, Navi Mumbai) for her help in statis-tical analysis.
REFERENCES
1. Scully C, Porter S. ABC of oral health: oral cancer. BMJ2000;321:97–100.
2. Neville BW, Day TA. Oral cancer and precancerouslesions. CA Cancer J Clin 2002;52:195–215.
3. Hardisson D. Molecular pathogenesis of head and necksquamous cell carcinoma. Eur Arch Otorhinolaryngol2003;260:502–508.
4. Vaux DL, Haecker G, Strasser A. An evolutionary per-spective on apoptosis. Cell 1994;76:777–779.
5. Nagata S. Apoptosis by death factor. Cell 1997;88:355–365.
6. Nagata S. Apoptosis and autoimmune diseases. IUBMBLife 2006;58:358–362.
7. Thompson CB. Apoptosis in the pathogenesis and treat-ment of disease. Science 1995;267:1456–1462.
8. Aravind L, Dixit V, Mand Koonin EV. The domains ofdeath: evolution of the apoptosis machinery. Trends Bio-chem Sci 1999;24:47–53.
9. Mawji IA, Simpson CD, Hurren R, et al. Critical role forFas-associated death domain-like interleukin-1-convert-ing enzyme-like inhibitory protein in anoikis resistanceand distant tumor formation. J Natl Cancer Inst2007;99:811–822.
10. Reed JC. Dysregulation of apoptosis in cancer. J ClinOncol 1999;17:2941–2953.
11. Li F, Ackermann EJ, Bennett CF, et al. Pleiotropic cell-division defects and apoptosis induced by interferencewith survivin function. Nat Cell Biol 1999;1:461–466.
12. Lu C-D, Altieri DC, Tanigawa N. Expression of a novelantiapoptosis gene, survivin, correlated with tumor cellapoptosis and p53 accumulation in gastric carcinomas.Cancer Res 1998;58:1808–1812.
13. Yang E, Korsmeyer SJ. Molecular thanatopsis: a dis-course on the bcl-2 family and cell death. Blood1996;88:1456–1462.
14. Ambrosini G, Adida C, Altieri DC. A novel anti-apoptoticgene, survivin, expressed in cancer and lymphoma. NatMed 1997;3:917–921.
15. Adida C, Crotty PL, McGrath J, Berrebi D, Diebold J,Altieri DC. Developmentally regulated expression of thenovel cancer anti-apoptosis gene survivin in human andmouse differentiation. Am J Pathol 1998;152:43–49.
16. Li F, Ambrosini G, Chu EY, et al. Control of apoptosisand mitotic spindle checkpoint by survivin. Nature1998;396:580–584
17. Khan Z, Bhadouria P, Gupta R, Bisen PS. Tumor controlby manipulation of the human anti-apoptotic survivingene. Curr Cancer Ther Rev 2006;2:73–79.
18. Deveraux QL, Reed JC. IAP family proteins-suppressorsof apoptosis. Genes Dev 1999;13:239–252.
19. Kawasaki H, Altieri DC, Lu CD, Toyoda M, Tenjo T,Tanigawa N. Inhibition of apoptosis by survivin predictsshorter survival rates in colorectal cancer. Cancer Res1998;58:5071–5074.
20. Monzo M, Rosell R, Felip E, et al. A novel anti-apoptosisgene: re-expression of survivin messenger RNA as aprognostic marker in non-small-cell lung cancers. J ClinOncol 1999;17:2100–2104.
21. Tanaka K, Iwamoto S, Gon G, Nohara T, Iwamoto M,Tanigawa N. Expression of survivin and its relationship
Detection of Survivin and p53 in Human Oral Cancer HEAD & NECK—DOI 10.1002/hed August 2009 1047

to loss of apoptosis in breast carcinomas. Clin CancerRes 2000;6:127–134.
22. Islam A, Kageyama H, Takada N, et al. High expressionof survivin, mapped to 17q25, is significantly associatedwith poor prognostic factors and promotes cell survivalin human neuroblastoma. Oncogene 2000;19:617–623.
23. Kato J, Kuwabara Y, Mitani M, et al. Expression of sur-vivin in esophageal cancer: correlation with the progno-sis and response to chemotherapy. Int J Cancer 2001;95:92–95.
24. Parenti AR, Rugge M, Frizzera E, et al. p53 overexpres-sion in the multistep process of oesophageal carcinogene-sis. Am J Surg Pathol 1995;19:1418–1422.
25. Jane C, Nerurkar AV, Shirsat NV, Deshpande RB, Amra-purkar AD, Karjodkar FR. Increased survivin expressionin high-grade oral squamous cell carcinoma: a study inIndian tobacco chewers. J Oral Pathol Med 2006;35:595–601.
26. Freier K, Pungs S, Sticht C, et al. High survivin expres-sion is associated with favorable outcome in advancedprimary oral squamous cell carcinoma after radiationtherapy. Int J Cancer 2007;120:942–946.
27. Lo Muzio L, Staibano S, Pannone G, et al. Expression ofthe apoptosis inhibitor survivin in aggressive squamouscell carcinoma. Exp Mol Pathol 2001;70:249–254.
28. Dong Y, Sui L, Watanabe Y, Sugimoto K, Tokuda M. Sur-vivin expression in laryngeal squamous cell carcinomasand its prognostic implications. Anticancer Res 2002;22:2377–2383.
29. Gianani R, Jarboe E, Orlicky D, et al. Expression of sur-vivin in normal, hyperplastic, and neoplastic colonic mu-cosa. Hum Pathol 2001;32:119–125.
30. Grossman D, McNiff JM, Li F, Altieri DC. Expressionand targeting of the apoptosis inhibitor, survivin, inhuman melanoma. J Invest Dermatol 1999;113:1076–1081.
31. Satoh K, Kaneko K, Hirota M, Masamune A, Satoh A,Shimosegawa T. Expression of survivin is correlatedwith cancer cell apoptosis and is involved in the develop-ment of human pancreatic duct cell tumors. Cancer 2001;92:271–278.
32. Graeber TG, Osmanian C, Jacks T, et al. Hypoxia-medi-ated selection of cells with diminished apoptotic poten-tial in solid tumours. Nature 1996;379:88–91.
33. Brachman DG, Graves D, Vokes E, et al. Occurrence ofp53 gene deletions and human papillomavirus infectionin human head and neck cancer. Cancer Res 1992;62:4832–4836.
34. Shin DM, Lee JS, Choi LG. Prognostic significance ofp53 expression in head and neck squamous cell carci-noma. Proc Am Soc Clin Oncol 1994;13:283–289.
35. Levine AL. p53, the cellular gatekeeper for growth anddivision. Cell 1997;88:323–331.
36. Hoffman WH, Biade S, Zilfou JT, Chen J, Murphy M.Transcriptional repression of the anti-apoptotic survivingene by wild type p53. J Biol Chem 2000;277:3247–3257.
37. Mirza A, McGuirk M, Hockenberry TN, et al. Humansurvivin is negatively regulated by wild-type p53 andparticipates in p53-dependent apoptotic pathway. Onco-gene 2002;21:2613–2622.
38. Zhang T, Otevrel T, Gao Z, Ehrich SM, Fields JZ. Evi-dence that APC regulates survivin expression: a possiblemechanism contributing to the stem cell origin of coloncancer. Cancer Res 2001;61:8664–8667.
39. Greenblat MS, Bennett WP, Hollstein M, Harris C.Mutations in the p53 tumor suppressor genes: clues tocancer etiology and molecular pathogenesis. Cancer Res1994;54:4855–4878.
40. Chiang CP, Lang MJ, Liu BY, et al. Expression of p53protein in oral submucous fibrosis, oral epithelial hyper-kerotosis and oral epithelial dysplasis. J Formos MedAssoc 2000;99:229–234.
1048 Detection of Survivin and p53 in Human Oral Cancer HEAD & NECK—DOI 10.1002/hed August 2009


















