
Detection of New Delhi Metallo-²-Lactamase (blaNDM-1) in
14
1 Detection of New Delhi Metallo-β-Lactamase (bla NDM-1 ) in Acinetobacter schindleri during 1 routine surveillance 2 Patrick McGann 1* , Michael Milillo 1 , Robert J. Clifford 1 , Erik Snesrud 1 , Lindsay Stevenson 2 , 3 Michael G. Backlund 2 , Helen B. Viscount 2 , Reyes Quintero 1 , Yoon I Kwak 1 , Michael J. Zapor 3 , 4 Paige E Waterman 1 , Emil P Lesho 1 5 1 Multidrug-resistant Organism Repository and Surveillance Network, Walter Reed Army 6 Institute of Research, Silver Spring, Maryland 7 2 Department of Pathology, Walter Reed National Military Medical Center, Bethesda 8 Maryland 9 3 Infectious Diseases Service, Walter Reed National Military Medical Center, Bethesda, 10 Maryland 11 12 Running Title: bla NDM1 in Acinetobacter schindleri 13 Keywords: Acinetobacter schindleri, bla NDM-1 , surveillance network 14 15 * Corresponding author 16 Patrick McGann, PhD 17 Multidrug-resistant Organism Repository and Surveillance Network 18 Walter Reed Army Institute of Research, Building 503, 2S35 19 Silver Spring, Maryland 20910, USA 20 Ph: (301) 319 9912 21 Fax (301) 319 9548 22 Email: [email protected] 23 Copyright © 2013, American Society for Microbiology. All Rights Reserved. J. Clin. Microbiol. doi:10.1128/JCM.00281-13 JCM Accepts, published online ahead of print on 3 April 2013 on January 14, 2019 by guest http://jcm.asm.org/ Downloaded from
Transcript of Detection of New Delhi Metallo-²-Lactamase (blaNDM-1) in

1
Detection of New Delhi Metallo-β-Lactamase (blaNDM-1) in Acinetobacter schindleri during 1
routine surveillance 2
Patrick McGann1*, Michael Milillo1, Robert J. Clifford1, Erik Snesrud1, Lindsay Stevenson2, 3
Michael G. Backlund2, Helen B. Viscount2, Reyes Quintero1, Yoon I Kwak1, Michael J. Zapor3, 4
Paige E Waterman1, Emil P Lesho1 5
1 Multidrug-resistant Organism Repository and Surveillance Network, Walter Reed Army 6
Institute of Research, Silver Spring, Maryland 7
2 Department of Pathology, Walter Reed National Military Medical Center, Bethesda 8
Maryland 9
3 Infectious Diseases Service, Walter Reed National Military Medical Center, Bethesda, 10
Maryland 11
12
Running Title: blaNDM1 in Acinetobacter schindleri 13
Keywords: Acinetobacter schindleri, blaNDM-1, surveillance network 14
15
* Corresponding author 16
Patrick McGann, PhD 17
Multidrug-resistant Organism Repository and Surveillance Network 18
Walter Reed Army Institute of Research, Building 503, 2S35 19
Silver Spring, Maryland 20910, USA 20
Ph: (301) 319 9912 21
Fax (301) 319 9548 22
Email: [email protected] 23
Copyright © 2013, American Society for Microbiology. All Rights Reserved.J. Clin. Microbiol. doi:10.1128/JCM.00281-13 JCM Accepts, published online ahead of print on 3 April 2013
on January 14, 2019 by guesthttp://jcm
.asm.org/
Dow
nloaded from
2
Abstract. A carbapenem-resistant Alcaligenes faecalis was isolated from a surveillance swab of 24
a service member injured in Afghanistan. The isolate was positive for blaNDM by real-time PCR. 25
Species identification was re-evaluated on three identification systems, but was inconclusive. 26
Genome sequencing indicated the closest relative was Acinetobacter schindleri and blaNDM-1 was 27
carried on a plasmid that shared >99% identity with one identified in an Acinetobacter lwoffi. 28
The isolate also carried a novel chromosomally-encoded class D oxacillinase. 29
on January 14, 2019 by guesthttp://jcm
.asm.org/
Dow
nloaded from
3
In response to global concerns over the spread of blaNDM (1-3), the Multidrug-resistant Organism 30
Repository and Surveillance Network (MRSN) implemented routine monthly screening for this 31
gene in all carbapenem-resistant Gram-negative organisms in 2010 (4). From this surveillance 32
initiative, we previously described the first incidence of blaNDM-1 in the US military healthcare 33
system from a strain of Providencia stuartii, isolated from a local Afghan national treated at a 34
military facility in Afghanistan (5). Timely feedback was provided to the submitting facility, 35
which resulted in increased surveillance and enhanced infection control policies. 36
In June 2012, following a blast injury involving shrapnel in Afghanistan, a 22 year-old male 37
received cefazolin for routine prophylaxis and was evacuated to the U.S. via Germany. During 38
that escalation of care, a routine groin surveillance swab revealed mixed microbial flora. An 39
isolate identified as Alcaligenes faecalis using the BD Phoenix Automated Microbiology System 40
(BD Diagnostics Systems, Sparks, MD) displayed resistance to all tested B-lactam antibiotics 41
(Intermediate to Ceftriaxone), including the carbapenems and the monobactam aztreonam (Table 42
1). A Modified Hodge Test (MHT) was negative for meropenem. For ertapenem, the MHT was 43
positive but the clover leaf-like growth indentation of E.coli ATCC 25922 was significantly 44
reduced when grown with the test isolate, designated MRSN 10319, compared to growth 45
alongside the blaKPC-positive control strain Klebsiella pneumoniae ATCC BAA-1705. The 46
isolate was forwarded to the MRSN, a College of American Pathologists (CAP) certified 47
laboratory, for further evaluation. Identification was re-evaluated on three automated 48
identification systems: the VITEK 2 (bioMerieux, Durham, NC), the BD Phoenix, and the 49
Microscan Walkway (Siemens Healthcare Diagnostics Inc, Deerfield, IL). The MRSN employs 50
the three most common automated instruments as these instruments are used throughout the 51
Military Healthcare System (MHS) and discrepancies between their results have been noted (for 52
on January 14, 2019 by guesthttp://jcm
.asm.org/
Dow
nloaded from
4
a comprehensive review see (6)). Both VITEK 2 and Microscan identified the organism as 53
Acinetobacter lwoffi, whereas the Phoenix was in agreement with the initial identification of 54
Alcaligenes faecalis. 16S rRNA sequencing was performed (7) and indicated the isolate shared 55
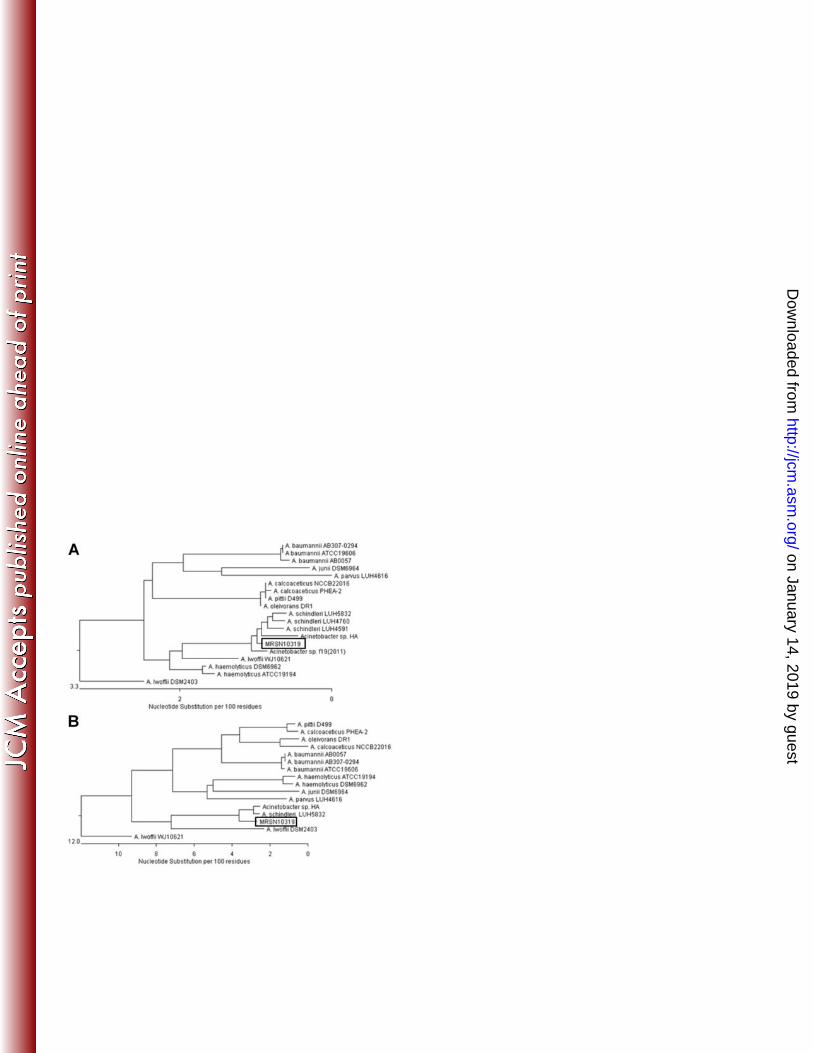
99% identity with Acinetobacter schindleri/Acinetobacter johnsonii. Whole genome sequencing 56
(WGS) using an Ion Torrent PGM (Ion Torrent Systems, Inc., Guilford, CT), which provided 57
87X coverage of the 16S rRNA gene, demonstrated 99.5% identity to Acinetobacter schindleri 58
16S rRNA sequences deposited at GenBank (Figure 1A) (8). Phylogenetic analysis using the 59
rpoB gene sequence confirmed this identification (Figure 1B). 60
MRSN 10319 was tested by real-time PCR for carbapenemase genes (9), and was positive for 61
blaNDM. The gene was found to contain a single nucleotide polymorphism (guanine to adenine) at 62
position 468 compared to blaNDM-1, resulting in a synonymous mutation. The gene was located 63
on a 47.3 kB plasmid that shared >99% identity with pNDM-BJ02, a plasmid identified in an 64
isolate of Acinetobacter lwoffi cultured from the urine of a 62-year-old female patient in Beijing 65
in November 2010 (10). Hu and colleagues identified A. lwoffi by VITEK 2, but make no 66
mention of the 16S rRNA sequence to verify this result. In accordance with the discrepancies 67
noted in this report, Dortet and colleagues have noted that the VITEK 2 identifies rare species of 68
Acinetobacter, including A. schindleri, as A. lwoffi (11). 69
Plasmid pNDM-BJ02 has 46 open reading frames and there is no plasmid sequence in 70
Genbank that shares more than 15% homology with it. Furthermore, the plasmid cannot be 71
assigned to any of the described incompatibility groups using the PCR replicon typing method 72
developed by Carattolli and colleagues (12). The plasmid harbors a type IV secretion system 73
(T4SS) gene cluster and a single copy of aphA6, which encodes resistance to some 74
aminoglycosides. However, MRSN 10319 was susceptible to all aminoglycosides tested (Table 75
on January 14, 2019 by guesthttp://jcm
.asm.org/
Dow
nloaded from
5
1). Sequence comparison to pNDM-BJ02 suggests that the original promoter sequence for this 76
gene has been disrupted by an upstream transposition event as previously noted (10). Hu and 77
colleagues demonstrated that the plasmid had a relatively high transfer frequency (9.1 x 10-3 to 78
1.3 x 10-2 per donor cell) to E. coli J53 AziR, suggesting that this plasmid has a high propensity 79
for horizontal transmission (10). 80
Analysis of the chromosomal sequence revealed just a single locus with homology to 81
known antibiotic resistance genes. This locus encoded a class D oxacillinase that shares closest 82
homology to the recently described blaOXA-237 gene (13), but has 18 amino acid differences and 83
represents a novel blaOXA allele. The final nomenclature for this gene is currently being assigned 84
by the Lahey group (www.lahey.org; last accessed March 2013) and the complete gene sequence 85
has been deposited at GenBak (Accession number KC771279). There is no evidence (i.e. no 86
transposons or Insertion Sequences) in the surrounding genetic environment to suggest 87
horizontal acquisition of this gene. Based on the antibiotic profile of blaOXA-237 (13) and the lack 88
of any other antibiotic resistance genes, including other β-lactams, aztreonam resistance in this 89
strain is most likely due to this class D oxacillinase,. A complete analysis of the MRSN 10319 90
genome is ongoing and will provide further information. 91
This report highlights the limitations of automated identification systems when working 92
with unusual species. Commonly used clinical laboratory identification systems do not include A. 93
schindleri or A. johnsonii on identification panels (manufacturer literature), which can lead to 94
erroneous identification. Due to the high correlation between blaNDM carriage and the 95
Enterobacteriaceae, surveillance strategies for this gene have primarily focused on this group of 96
bacteria. However, given the association of this gene with highly promiscuous plasmids, as well 97
as documented horizontal dissemination of this gene, it is critical that surveillance efforts 98
on January 14, 2019 by guesthttp://jcm
.asm.org/
Dow
nloaded from
6
continue to test all carbapenem-resistant Gram-negative organisms for blaNDM. A number of good 99
techniques exist for detecting NDM-producing Enterobacteriaceae (14), but false-negative and 100
weakly-positive results have been observed in this Family with the popular MHT (15, 16). 101
Detection in Acinetobacter species remains a challenge due to the potential failure of many 102
techniques, including the MHT and Etest MBL strip (17). Bonnin and colleagues have suggested 103
that for carbapenem-resistant A. baumannii, isolates should first be screened using EDTA 104
inhibition-based techniques, followed by further PCR-based techniques in a reference laboratory 105
(17). We suggest that the same method be applied to all other carbapenem-resistant 106
Acinetobacter species isolated from clinical specimens. 107
on January 14, 2019 by guesthttp://jcm
.asm.org/
Dow
nloaded from
7
Acknowledgements 108
Major funding for this project was provided by the Global Emerging Infections Surveillance and 109
Response System (GEIS; Grant #C070912WR) and Defense Medical Research and Development 110
Program (DMRDP; Grant #D61I10J258). 111
Material has been reviewed by the Walter Reed Army Institute of Research. There is no 112
objection to its presentation. The opinions or assertions contained herein are the private views of 113
the authors and are not to be construed as official, or reflecting the views of the Department of 114
Defense. 115
on January 14, 2019 by guesthttp://jcm
.asm.org/
Dow
nloaded from
8
References 116
1. Bonomo, R. A. 2011. New Delhi metallo-beta-lactamase and multidrug resistance: a 117
global SOS? Clinical infectious diseases : an official publication of the Infectious 118
Diseases Society of America 52:485-487. 119
2. Hammerum, A. M., M. A. Toleman, F. Hansen, B. Kristensen, C. H. Lester, T. R. 120
Walsh, and K. Fuursted. 2010. Global spread of New Delhi metallo-beta-lactamase 1. 121
The Lancet infectious diseases 10:829-830. 122
3. Walsh, T. R. 2010. Emerging carbapenemases: a global perspective. International 123
journal of antimicrobial agents 36 Suppl 3:S8-14. 124
4. Waterman, P., Y. Kwak, R. Clifford, M. Julius, F. Onmus-Leone, C. Tsurgeon, M. 125
Riley, C. Black, P. McGann, and E. Lesho. 2012. A multidrug-resistance surveillance 126
network: 1 year on. The Lancet infectious diseases 12:587-588. 127
5. McGann, P., J. Hang, R. J. Clifford, Y. Yang, Y. I. Kwak, R. A. Kuschner, E. P. 128
Lesho, and P. E. Waterman. 2012. Complete sequence of a novel 178-kilobase plasmid 129
carrying bla(NDM-1) in a Providencia stuartii strain isolated in Afghanistan. 130
Antimicrobial agents and chemotherapy 56:1673-1679. 131
6. Winstanley, T., and P. Courvalin. 2011. Expert systems in clinical microbiology. 132
Clinical microbiology reviews 24:515-556. 133
7. Weisburg, W. G., S. M. Barns, D. A. Pelletier, and D. J. Lane. 1991. 16S ribosomal 134
DNA amplification for phylogenetic study. Journal of bacteriology 173:697-703. 135
8. Nemec, A., T. De Baere, I. Tjernberg, M. Vaneechoutte, T. J. van der Reijden, and 136
L. Dijkshoorn. 2001. Acinetobacter ursingii sp. nov. and Acinetobacter schindleri sp. 137
on January 14, 2019 by guesthttp://jcm
.asm.org/
Dow
nloaded from
9
nov., isolated from human clinical specimens. International journal of systematic and 138
evolutionary microbiology 51:1891-1899. 139
9. Milillo, M., Y. I. Kwak, E. Snesrud, P. E. Waterman, E. Lesho, and P. McGann. 140
2013. Rapid and Simultaneous Detection of blaKPC and blaNDM using Multiplex Real-141
Time PCR. Journal of clinical microbiology. 142
10. Hu, H., Y. Hu, Y. Pan, H. Liang, H. Wang, X. Wang, Q. Hao, X. Yang, X. Yang, X. 143
Xiao, C. Luan, Y. Yang, Y. Cui, R. Yang, G. F. Gao, Y. Song, and B. Zhu. 2012. 144
Novel plasmid and its variant harboring both a bla(NDM-1) gene and type IV secretion 145
system in clinical isolates of Acinetobacter lwoffii. Antimicrobial agents and 146
chemotherapy 56:1698-1702. 147
11. Dortet, L., P. Legrand, C. J. Soussy, and V. Cattoir. 2006. Bacterial identification, 148
clinical significance, and antimicrobial susceptibilities of Acinetobacter ursingii and 149
Acinetobacter schindleri, two frequently misidentified opportunistic pathogens. Journal 150
of clinical microbiology 44:4471-4478. 151
12. Carattoli, A., A. Bertini, L. Villa, V. Falbo, K. L. Hopkins, and E. J. Threlfall. 2005. 152
Identification of plasmids by PCR-based replicon typing. Journal of microbiological 153
methods 63:219-228. 154
13. Higgins, P. G., F. J. Perez-Llarena, E. Zander, A. Fernandez, G. Bou, and H. Seifert. 155
2013. OXA-235, a novel Class D Beta-Lactamase Involved in Resistance to 156
Carbapenems in Acinetobacter baumannii. Antimicrobial agents and chemotherapy. 157
14. Nordmann, P., L. Poirel, A. Carrer, M. A. Toleman, and T. R. Walsh. 2011. How to 158
detect NDM-1 producers. Journal of clinical microbiology 49:718-721. 159
on January 14, 2019 by guesthttp://jcm
.asm.org/
Dow
nloaded from
10
15. Castanheira, M., L. M. Deshpande, D. Mathai, J. M. Bell, R. N. Jones, and R. E. 160
Mendes. 2011. Early dissemination of NDM-1- and OXA-181-producing 161
Enterobacteriaceae in Indian hospitals: report from the SENTRY Antimicrobial 162
Surveillance Program, 2006-2007. Antimicrobial agents and chemotherapy 55:1274-163
1278. 164
16. Girlich, D., L. Poirel, and P. Nordmann. 2012. Value of the modified Hodge test for 165
detection of emerging carbapenemases in Enterobacteriaceae. Journal of clinical 166
microbiology 50:477-479. 167
17. Bonnin, R. A., T. Naas, L. Poirel, and P. Nordmann. 2012. Phenotypic, biochemical, 168
and molecular techniques for detection of metallo-beta-lactamase NDM in Acinetobacter 169
baumannii. Journal of clinical microbiology 50:1419-1421. 170
18. Clinical and Laboratory Standards Institute. 2012. Performance standards for 171
antimicrobial susceptibility testing. M100–S22. Wayne (PA). 172
19. Zapor, M. J., M. Barber, A. Summers, G. H. Miller, L. A. Feeney, L. E. Eberly, and 173
G. Wortmann. 2010. In vitro activity of the aminoglycoside antibiotic arbekacin against 174
Acinetobacter baumannii-calcoaceticus isolated from war-wounded patients at Walter 175
Reed Army Medical Center. Antimicrobial agents and chemotherapy 54:3015-3017.176
on January 14, 2019 by guesthttp://jcm
.asm.org/
Dow
nloaded from
11
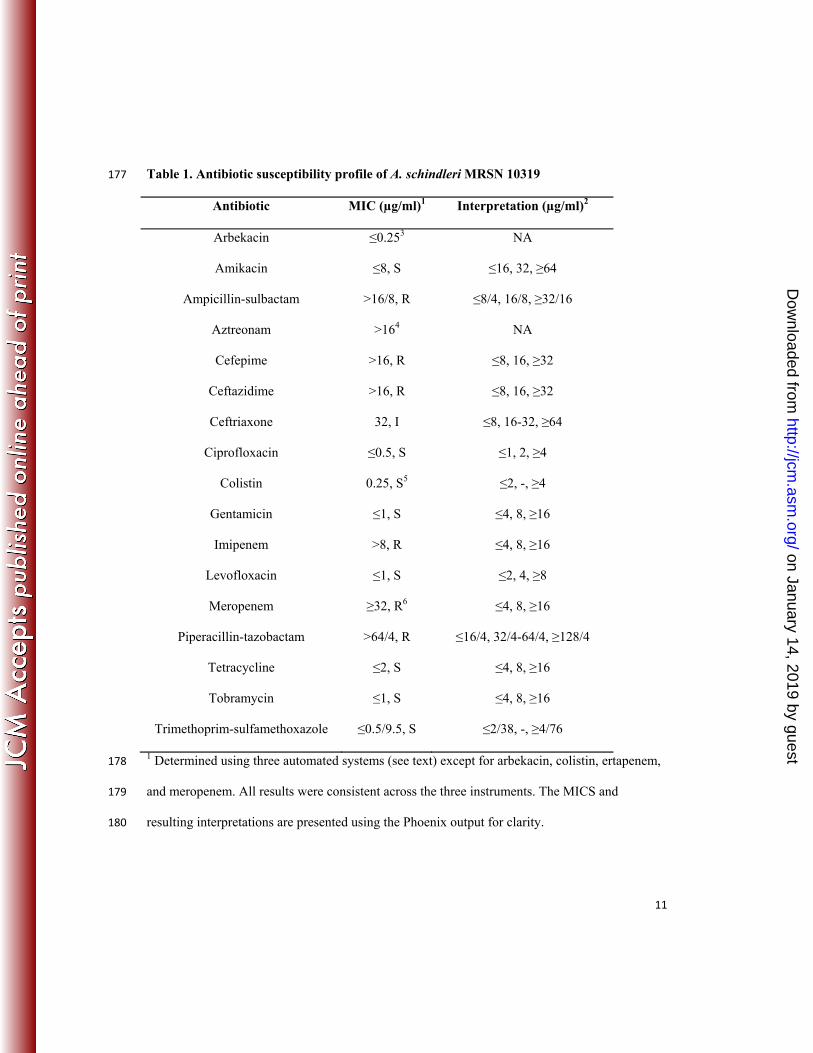
Table 1. Antibiotic susceptibility profile of A. schindleri MRSN 10319 177
Antibiotic MIC (µg/ml)1 Interpretation (µg/ml)2
Arbekacin ≤0.253 NA
Amikacin ≤8, S ≤16, 32, ≥64
Ampicillin-sulbactam >16/8, R ≤8/4, 16/8, ≥32/16
Aztreonam >164 NA
Cefepime >16, R ≤8, 16, ≥32
Ceftazidime >16, R ≤8, 16, ≥32
Ceftriaxone 32, I ≤8, 16-32, ≥64
Ciprofloxacin ≤0.5, S ≤1, 2, ≥4
Colistin 0.25, S5 ≤2, -, ≥4
Gentamicin ≤1, S ≤4, 8, ≥16
Imipenem >8, R ≤4, 8, ≥16
Levofloxacin ≤1, S ≤2, 4, ≥8
Meropenem ≥32, R6 ≤4, 8, ≥16
Piperacillin-tazobactam >64/4, R ≤16/4, 32/4-64/4, ≥128/4
Tetracycline ≤2, S ≤4, 8, ≥16
Tobramycin ≤1, S ≤4, 8, ≥16
Trimethoprim-sulfamethoxazole ≤0.5/9.5, S ≤2/38, -, ≥4/76
1 Determined using three automated systems (see text) except for arbekacin, colistin, ertapenem, 178
and meropenem. All results were consistent across the three instruments. The MICS and 179
resulting interpretations are presented using the Phoenix output for clarity. 180
on January 14, 2019 by guesthttp://jcm
.asm.org/
Dow
nloaded from
12
2 As recommended by the Clinical and Laboratory Standards Institute (CLSI) (18). No CLSI 181
interpretative guidelines are indicated by “NA”. 182
3 MICs for arbekacin represent the average of three independent microbroth dilution assays as 183
described (19). 184
4 No CLSI interpretive guidelines of aztreonam are available for Acinetobacter species. 185
5 Average of three independent Etest assay performed as described by the manufacturer 186
(bioMérieux). Etest results were consistent across replicates. 187
6 Ertapenem is not usually reported for Acinetobacter species due to intrinsic resistance but is 188
included due to the rarity of susceptibility data from A. schindleri. As meropenem is not reported 189
by the BD Phoenix Automated Microbiology System, MICs were performed in triplicate by Etest 190
as described by the manufacturer (bioMérieux). Meropenem MICs represents the average of 191
three independent Etests performed as described by the manufacturer (bioMérieux). No 192
variation in Etest results was evidenced. 193 on January 14, 2019 by guesthttp://jcm
.asm.org/
Dow
nloaded from
13
Figure 1. Dendrogram showing the relationship between A. schindleri MRSN 10319 and other 194
Acinetobacter species based on (A) 16S rRNA and (B) rpoB gene sequences. Acinetobacter 195
species 16S rRNA and rpoB gene sequences were retrieved from GenBank 196
(http://www.ncbi.nlm.nih.gov/pubmed: last accessed August 23rd 2012) and aligned using 197
MegAlign (DNASTAR, Madison, MI). Dendrograms, based on the number of nucleotide 198
changes were generated using the MegAlign program (DNASTAR). 199
200
on January 14, 2019 by guesthttp://jcm
.asm.org/
Dow
nloaded from