Design of Eyedropper Tips for Topical Beta-Blocking Agents
2
Vol. 102, No.1 Letters to The Journal 123 Retinal sensitivity to damage from short wave- lengths of light. Nature 260:153, 1976. 4. Boettner, E. A., and Wolter, J. R.: Transmission of the ocular media. Invest. Ophthalmol. 1:776, 1962. 5. Boldrey, E. E., Ho, B. T., and Griffith, R. D.: Retinal burns occurring at cataract extraction. Oph- thalmology 91:1297, 1984. Design of Eyedropper Tips for Topical Beta-Blocking Agents Reay H. Brown, M.D., and Mary G. Lynch, M.D. Department of Ophthalmology, University of Texas, Dallas. Inquiries to Reay H. Brown, M.D., Department of Oph- thalmology, University of Texas Health Science Center at Dallas, 5323 Harry Hines Blvd., Dallas, TX 75235. The design of an eyedropper tip influences both the drop size and the number of drops delivered per application.' Eyedropper tips that deliver large or multiple drops may in- crease the risk of systemic toxicity since the excess drop volume drains into the nasolacri- mal system where it may be systemically ab- sorbed." Drop size and method of delivery are also important from an economic standpoint since tips that deliver large or multiple drops increase costs. Eyedropper tips for many ophthalmic medi- cations are constructed with an inner aperture that is much smaller than the inner diameter of the aperture at the tip surface (Fig. 1). This design increases the resistance to fluid flow so that squeezing the bottle results in a single drop rather than multiple drops or a stream. By instilling a single drop, a patient receives a known quantity of medication and avoids the problem of administering multiple drops with the increased chance for systemic absorption. The outer surface dimensions of an eyedropper tip affect drop size. By varying the size of the outer diameter and platform width, drops of different volumes can be produced.' We have examined the eyedropper tip design of the three currently available topical beta- blocking agents: timolol, betaxolol, and levo- bunolol. The outer diameter of each tip was measured with a micrometer (Fig. 1, Table). The inner diameters were measured with standardized gauging pins. The mean drop size for each tip was measured by a standard tech- nique in which the eyedropper bottles were Inner chamber Inner aperture Outer chamber I Platform --: width : I.D. .. Outer diameter Fig. 1 (Brown and Lynch). A cross section through an eyedropper tip. The inner aperture is substantial- ly smaller than the inner diameter (I.D.) at the outer surface of the tip. squeezed by hand. A consistent pressure was applied so that a maximally large drop of the beta-blocker accumulated on the tip surface before it fell. Ten successive drops were collect- ed on a small plastic dish and weighed on a balance to give an average drop volume. Three or more ten-drop averages were calculated for each tip. Five different tips were tested for each beta-blocker. An average drop volume was determined for each of the five tips. The TABLE EYEDROPPER TIP DIMENSIONS AND DROP SIZE BETA-BLOCKERS MEASUREMENTS TIMOLOL BETAXOLOL LEVOBUNOLOL Eyedropper Inner diameter (inches) 0.135 0.120 0.185 Outer diameter (inches) 0.063 0.074 0.067 Drop volume Mean (,.d) 30.7 25.7 42.0 Range (111) 28.2 24.0 40.0 to to to 32.5 27.2 44.2
Transcript of Design of Eyedropper Tips for Topical Beta-Blocking Agents

Vol. 102, No.1 Letters to The Journal 123
Retinal sensitivity to damage from short wavelengths of light. Nature 260:153, 1976.
4. Boettner, E. A., and Wolter, J. R.: Transmissionof the ocular media. Invest. Ophthalmol. 1:776, 1962.
5. Boldrey, E. E., Ho, B. T., and Griffith, R. D.:Retinal burns occurring at cataract extraction. Ophthalmology 91:1297, 1984.
Design of Eyedropper Tips forTopical Beta-Blocking Agents
Reay H. Brown, M.D.,and Mary G. Lynch, M.D.Department of Ophthalmology, University of Texas,Dallas.Inquiries to Reay H. Brown, M.D., Department of Ophthalmology, University of Texas Health Science Center atDallas, 5323 Harry Hines Blvd., Dallas, TX 75235.
The design of an eyedropper tip influencesboth the drop size and the number of dropsdelivered per application.' Eyedropper tipsthat deliver large or multiple drops may increase the risk of systemic toxicity since theexcess drop volume drains into the nasolacrimal system where it may be systemically absorbed." Drop size and method of delivery arealso important from an economic standpointsince tips that deliver large or multiple dropsincrease costs.
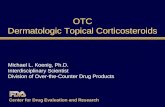
Eyedropper tips for many ophthalmic medications are constructed with an inner aperturethat is much smaller than the inner diameter ofthe aperture at the tip surface (Fig. 1). Thisdesign increases the resistance to fluid flow sothat squeezing the bottle results in a singledrop rather than multiple drops or a stream. Byinstilling a single drop, a patient receives aknown quantity of medication and avoids theproblem of administering multiple drops withthe increased chance for systemic absorption.The outer surface dimensions of an eyedroppertip affect drop size. By varying the size of theouter diameter and platform width, drops ofdifferent volumes can be produced.'
We have examined the eyedropper tip designof the three currently available topical betablocking agents: timolol, betaxolol, and levobunolol. The outer diameter of each tip wasmeasured with a micrometer (Fig. 1, Table).The inner diameters were measured withstandardized gauging pins. The mean drop sizefor each tip was measured by a standard technique in which the eyedropper bottles were
Inner chamber
Inner aperture
Outer chamber
I
Platform ~--:width : I.D...
Outerdiameter
Fig. 1 (Brown and Lynch). A cross section throughan eyedropper tip. The inner aperture is substantially smaller than the inner diameter (I.D.) at the outersurface of the tip.
squeezed by hand. A consistent pressure wasapplied so that a maximally large drop of thebeta-blocker accumulated on the tip surfacebefore it fell. Ten successive drops were collected on a small plastic dish and weighed on abalance to give an average drop volume. Threeor more ten-drop averages were calculated foreach tip. Five different tips were tested for eachbeta-blocker. An average drop volume wasdetermined for each of the five tips. The
TABLEEYEDROPPER TIP DIMENSIONS AND DROP SIZE
BETA-BLOCKERS
MEASUREMENTS TIMOLOL BETAXOLOL LEVOBUNOLOL
Eyedropper
Inner diameter (inches) 0.135 0.120 0.185Outer diameter (inches) 0.063 0.074 0.067
Drop volume
Mean (,.d) 30.7 25.7 42.0Range (111) 28.2 24.0 40.0
to to to
32.5 27.2 44.2

124 AMERICAN JOURNAL OF OPHTHALMOLOGY July, 1986
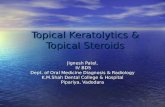
Fig. 2 (Brown and Lynch). A cross section throughthe redesigned betaxolol eyedropper tip (left) containing a resistance aperture and the original tipwithout one (right).
average of these five drop volumes yieldedthe mean drop volume for each beta-blocker(Table).
The drop volume was increased for the betablockers with eyedropper tips that had largerouter diameters (Table), supporting the conclusion of a previous study that drop size increased linearly with outer diameter. I
We cut each tip in cross section to examinethe internal structure. The eyedropper tips fortimolol and levobunolol contained an internalresistance aperture. Betaxolol was originallyreleased with a tip that did not contain a resistance aperture. This increased the potential fordelivering multiple drops or a stream. We demonstrated this in our laboratory and the tip wasredesigned to incorporate a resistance aperture(Fig. 2).
The availability of several topical betablockers is an important addition to glaucomatherapy. The potential for systemic toxicityfrom topical beta-blockers has been documented extensively. 3 The drop size and number ofdrops delivered per administration become increasingly important as medications capable ofcausing adverse systemic effects are applied tothe eye. The safety and economy of any topicalmedication should be enhanced with eyedropper tips designed to deliver small, single dropsconsistently.
References
1. Brown, R. H., Hotchkiss, M. L., and Davis,E. B.: Creating smaller eyedrops by reducing eyedropper tip dimensions. Am. J. Ophthalmol. 99:460,1985.
2. Shell, J. W.: Pharmacokinetics of topically applied ophthalmic drugs. Surv. Ophthalmol. 26:207,1982.
3. Van Buskirk, E. M., and Fraunfelder, F. T.: Ocular beta-blockers and systemic effects. Am. J. Ophthalmol. 98:623, 1984.
Paralysis of Convergence Causedby Mushroom Poisoning
Emil Giladand Yoram BigerDepartment of Ophthalmology, Rebecca Sieff Government Hospital.
Inquiries to Dr. Emil Gilad, Department of Ophthalmology, Rebecca Sieff Government Hospital, Sated, Israel.
Amanita pantherina, a poisonous mushroomthat contains ibotenic acid and muscimol isknown to cause anticholinergic symptoms suchas mydriasis and cycloplegia."! We treated apatient in whom diplopia resulting from paralysis of convergence was the initial symptom ofintoxication by that mushroom.
A l O-year-old boy was sent to the emergencyroom because of the sudden onset of diplopiasix hours after he ate raw mushrooms. He hadtachycardia, red dry skin, confusion, mild ataxia, and a heart rate of 120 beats/minute. Thepupils were fully dilated and nonreactive tolight and nearness. Paralysis of convergencewas seen with the near point of fusion at 1meter. There were no gastrointestinal symptoms. The poisonous mushrooms were identified as Amanita pantherina. Supportive therapyconsisted of bedrest and mild sedation. Reexamination after 24 hours showed the near pointof fusion to be at 35 em. Full recovery wasachieved within five days.
The pathway for convergence by which impulses pass from the cortex to the oculomotornuclei is poorly understood." Amanita pantherina contains ibolenic acid and muscimol whichhave caused anticholinergic reaction. Furtherstudy is needed to explain the effects of ibotenic acid on the mechanisms of convergence.