Derma to Fibroma
8
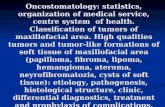
Dermatofibroma Erythematous, slightly hyperpigmented nodule on the leg. Courtesy of David Barnette, MD. Background Dermatofibroma (superficial benign fibrous histiocytoma) is a common cutaneous nodule of unknown etiology that occurs more often in women. Dermatofibroma frequently develops on the extremities (mostly the lower legs) and is usually asymptomatic, although pruritus and tenderness can be present. It is actually the most common painful skin tumor. [1] A number of well-described, histologic subtypes of dermatofibroma have been reported. Removal of the tumor is usually not required unless diagnostic uncertainty exists or particularly troubling symptoms are present. This article discusses primarily cutaneous (superficial) dermatofibroma. Subcutaneous (deep) benign fibrous histiocytomas are also well documented. In addition, benign fibrous histiocytomas are reported in bone, orbital, airway, gastrointestinal, genitourinary, and intracranial locations. Pathophysiology The precise mechanism for the development of dermatofibroma is unknown. Rather than a reactive tissue change, evidence that dermatofibroma may be a neoplastic process is demonstrated by its clonal proliferative growth. [2] Clonality, by itself, is not necessarily synonymous with a neoplastic process; it has been demonstrated in inflammatory conditions, including atopic dermatitis, lichen sclerosis, and psoriasis. Results from immunohistochemical testing with antibodies to factor XIIIa, which label dermal dendritic cells, are frequently positive in dermatofibroma, while antibodies to MAC 387, which label monocyte-derived macrophages (histiocytes), show less consistent results. One study evaluated the expression in dermatofibroma of HSP47, a recently used marker for skin fibroblasts; CD68, a marker for histiocytes; and factor XIIIa. Most of the spindle-shaped cells in all 28 cases of dermatofibroma, irrespective of histologic variant, stained positively with HSP47, indicating that skin fibroblasts are a major constituent of dermatofibroma. Factor XIIIa–positive dendritic cells also are present, but the presence of CD68-positive histiocytes was inconsistent, especially between histologic variants. [3] The cell surface proteoglycan, syndecan-1, [4] and fibroblast growth factor receptor 2, involved in epithelial-mesenchymal cross-talk, [5] may play a role in the growth of dermatofibromas. Transforming growth factor-beta (TGF- beta) signaling might be a trigger of the fibrosis seen in dermatofibromas.
description
dermatofibroma
Transcript of Derma to Fibroma
Dermatofibroma
Erythematous, slightly hyperpigmented nodule on the leg. Courtesy of David Barnette, MD.BackgroundDermatofibroma (superficial benign fibrous histiocytoma) is a common cutaneous nodule of unknown etiology that occurs more often in women. Dermatofibroma frequently develops on the extremities (mostly the lower legs) and is usually asymptomatic, although pruritus and tenderness can be present. It is actually the most common painful skin tumor.[1]A number of well-described, histologic subtypes of dermatofibroma have been reported. Removal of the tumor is usually not required unless diagnostic uncertainty exists or particularly troubling symptoms are present.This article discusses primarily cutaneous (superficial) dermatofibroma. Subcutaneous (deep) benign fibrous histiocytomas are also well documented.In addition, benign fibrous histiocytomas are reported in bone, orbital, airway, gastrointestinal, genitourinary, and intracranial locations.PathophysiologyThe precise mechanism for the development of dermatofibroma is unknown. Rather than a reactive tissue change, evidence that dermatofibroma may be a neoplastic process is demonstrated by its clonal proliferative growth.[2]Clonality, by itself, is not necessarily synonymous with a neoplastic process; it has been demonstrated in inflammatory conditions, including atopic dermatitis, lichen sclerosis, and psoriasis.Results from immunohistochemical testing with antibodies to factor XIIIa, which label dermal dendritic cells, are frequently positive in dermatofibroma, while antibodies to MAC 387, which label monocyte-derived macrophages (histiocytes), show less consistent results. One study evaluated the expression in dermatofibroma of HSP47, a recently used marker for skin fibroblasts; CD68, a marker for histiocytes; and factor XIIIa. Most of the spindle-shaped cells in all 28 cases of dermatofibroma, irrespective of histologic variant, stained positively with HSP47, indicating that skin fibroblasts are a major constituent of dermatofibroma. Factor XIIIapositive dendritic cells also are present, but the presence of CD68-positive histiocytes was inconsistent, especially between histologic variants.[3]The cell surface proteoglycan, syndecan-1,[4]and fibroblast growth factor receptor 2, involved in epithelial-mesenchymal cross-talk,[5]may play a role in the growth of dermatofibromas. Transforming growth factor-beta (TGF-beta) signaling might be a trigger of the fibrosis seen in dermatofibromas.[6]TGF-beta, along with other fibrinogenic factors, may be produced by mast cells, which have been reported to occur in abnormally high numbers in dermatofibromas.[7]EpidemiologyFrequencyUnited StatesDermatofibromas are relatively common.InternationalIncidence of dermatofibroma is probably similar to that in the United States.Mortality/MorbiditySimple dermatofibromas are regarded as benign lesions; however, discomfort from pain or itching may be significant.Some early reported cases of metastatic dermatofibroma may be disputable from the standpoint of histologic diagnosis. However, cellular, aneurysmal, and atypical variants, which are notoriously more locally recurrent, can rarely metastasize.[8]Such variants, and indeterminant dermatofibromas, might be regarded as potentially malignant lesions.[9]In these exceptional cases, indolent nodal and pulmonary metastases were typically seen.[10]Fatal metastases of large (>5 cm), deep, fibrous histiocytomas (a subset of dermatofibroma that arises in the subcutaneous or deep soft tissue, the classification of which may undergo further evolution) has been reported. Like the more aggressive cellular, aneurysmal, and atypical variants, local recurrence rates can approach 20%.[11]RaceFrequency of dermatofibroma appears to be similar in all races.SexFemales are affected by dermatofibroma more commonly than males, with a male-to-female ratio of 1:4.AgeDermatofibroma can occur in patients of any age, but it usually develops in young adulthood. Approximately 20% of the lesions occur before age 17 years.HistoryDermatofibromas typically arise slowly and most often occur as a solitary nodule on an extremity, particularly the lower leg, but any cutaneous site is possible. Dermatofibromas are usually asymptomatic, but itching and pain often are noted. They are the most common of all painful skin tumors.[1]Women who shave their legs may be bothered by the razor traumatizing the lesion in that region, causing pain, bleeding, erosive changes, and ulceration. Although cases of unusually rapid growth exist, most dermatofibromas remain static for decades or persist indefinitely. Patients may describe a hard mole or unusual scar and are often concerned about the possibility of skin cancer.Several lesions may be present, but rarely are numerous (ie, 15 or more) tumors found. A multiple eruptive variant occurs in only 0.3% of patients, many of whom have an alteration in their immune status, classically, HIV infection and systemic lupus erythematosus.[12, 13]However, dermatomyositis,[14]Graves disease,[15]Hashimoto thyroiditis,[16]myasthenia gravis,[16]Down syndrome,[17]leukemia,[18]myelodysplastic syndrome,[19]cutaneous T-cell lymphoma,[20]multiple myeloma,[20]and atopic dermatitis[21]have all been reported in association with the phenomenon. In addition, antiretroviral agents[22]and the biologic agent efalizumab[23]have been linked to their appearance.Both congenital[24]and acquired[25]cases of multiple clustered dermatofibromas have been reported.A case of haloasteatotic eczemadeveloping around a dermatofibroma on an edematous lower extremity has been described.[26]Spontaneous regression has been reported[27]and this may yield postinflammatory hypopigmentation.PhysicalTypically, the clinical appearance of dermatofibroma is a solitary, 0.5- to 1-cm nodule. A sizable minority of patients may have several lesions, but rarely (0.3% of cases) are more than 15 lesions present. (See History) The overlying skin can range from flesh to gray, yellow, orange, pink, red, purple, blue, brown, or black, or a combination of hues (see the image below). On palpation, the hard nodule may feel like a small pebble fixed to the skin surface and is freely movable over the subcutis. Tenderness may be elicited with manipulation of the lesion.The characteristic tethering of the overlying epidermis to the underlying lesion with lateral compression (pinching), called the dimple sign, may be a useful clinical sign for diagnosis.[28]However, presence of the dimple sign does not always assure the lesion is dermatofibroma,[29]and dermatoscopy may be useful in supporting the clinical impression.[30]The extremities are the most common sites of involvement, particularly the lower legs. Although any cutaneous site can be seen, palm, sole, digital, oral, and genital involvement is relatively rare. Giant (>5 cm in diameter),[31]atrophic,[32]polypoid,[33]and dermatofibroma with spreading satellitosis[34]variants have been reported.Multiple clustered dermatofibromas[25]are rare but can mimic dermatofibrosarcoma protuberans.A halo of asteatotic eczema surrounding a dermatofibroma occurred in one patient.[26]CausesHistorically attributed to be a reactive process to some traumatic insult to the skin (eg, arthropod bite),[35]the cause of dermatofibroma is unknown. Clonal analysis suggest it may represent a true neoplasm.[2]Altered immunity likely plays a role in many cases of multiple eruptive dermatofibromas (see History).A study of eruptive dermatofibromas in a kindred suggests that a genetic component may exist.[36]Differential Diagnoses Atypical Fibroxanthoma Atypical Mole (Dysplastic Nevus) Basal Cell Carcinoma Blue Nevi Cutaneous Manifestations of HIV Cutaneous T-Cell Lymphoma Dermatofibrosarcoma Protuberans Dermatologic Manifestations of Lipomas Dermatologic Manifestations of Merkel Cell Carcinoma Dermatologic Manifestations of Multicentric Reticulohistiocytosis Erythema Elevatum Diutinum Infantile Digital Fibromatosis Juvenile Xanthogranuloma (Nevoxanthoendothelioma) Keloid and Hypertrophic Scar Keratoacanthoma Leiomyoma Malignant Melanoma Mastocytosis Metastatic Carcinoma of the Skin Multinucleate Cell Angiohistiocytoma Neurilemoma Nevi, Melanocytic Pilomatrixoma Prurigo Nodularis Spiradenoma Spitz Nevus Squamous Cell Carcinoma Supernumerary Nipple Targetoid Hemosiderotic HemangiomaImaging StudiesA study of localized lesions of the skin imaged via variable-frequency ultrasound included the image of a hypoechoic solid nodule created by a dermatofibroma.[37]Dermatofibroma can mimic a malignant lesion on fluorodeoxyglucose positron-emission tomography (FDG-PET) scans.[38]ProceduresFor those trained indermoscopy, this may be a useful adjunctive diagnostic technique for dermatofibromas. The most common pattern seen is a peripheral pigment network with a central white area.[39]Dermoscopy of a xanthomatous dermatofibroma shows a homogeneous pattern with shades of yellow and a peripheral pigment network.[40]If a suggestive melanocytic pattern is noted with dermoscopy, a diagnostic biopsy is warranted.Confocal laser scanning microscopy findings have been described.[41]If any diagnostic uncertainty exists, excisional biopsy into the subcutaneous fat is advised.Histologic FindingsThe overlying epidermis is usually acanthotic. Pseudoepitheliomatous hyperplasia and a basaloid proliferation may be noted. The hyperplasia may be caused by the action of fibroblasts on epidermal keratinocytes.[42]Basaloid changes occurring upon a dermatofibroma have been frequently reported. Increased pigment may be seen, which may be iron or melanin. Most lesions display a grenz zone of normal papillary dermis overlying the tumor.The bulk of the tumor is within the mid dermis where no capsule is present and the periphery of the lesion blends with the surrounding tissue. Whorling fascicles of a spindle cell proliferation with excessive collagen deposition are characteristic. At the periphery, the spindle cells characteristically wrap around normal collagen bundles (see the images below). Occasionally, melanocytes have been reported to be interspersed amongst the spindle cells.[43]
Acanthotic epithelium with basilar hyperpigmentation (dirty feet) over a dermal spindle cell proliferation (X10). Courtesy of David Barnette, MD.
Collagen trapping by the dermal fibrohistiocytic infiltrate (X40). Courtesy of David Barnette, MD.The subcutis typically is preserved, but if involved (especially when a storiform [cartwheel] pattern is observed), be alert to the possibility of the lesion being adermatofibrosarcoma protuberans (DFSP).[44] Antibodies toward factor XIIIa and CD34 are useful in distinguishing the 2 tumors, with the former suggesting dermatofibroma and the latter suggesting DFSP.[45] Stromelysin-3 (ST-3) expression of dermatofibroma by immunohistochemical staining may also be useful in differentiation from DFSP.[46] Transforming growth factor-beta type I and type II receptor expression patterns may also help distinguish between dermatofibroma and DFSP.[6]Thrombospondin-1 (TSP-1) mediates TGF-beta I activation, and its elevated expression in DFSP may aid in the differential diagnosis.[47] Immunostaining with insulinlike growth factorbinding protein 7 (IGFBP7) is positive more frequently in dermatofibroma and aids in the differentiation from DFSP.[48] Nestin, expressed in only 13% of dermatofibroma, but 94% of DFSP, could be a useful marker to distinguish between these 2 tumors.[49] Collagen triple helix repeat containing-1 (Cthrc1) staining is positive much more frequently in DFSP and is another potential discriminating test.[50] D2-40 immunostain appears to be a sensitive marker for dermatofibromas, including the cellular variant, which can also aid in differentiation from DFSP.[51] Cathepsin K expression[52]and immunohistochemical analysis of chemokine receptor CXCR4[53]are other possible tools in delineating the 2 tumors. Indeterminate tumors that share histologic and immunohistochemical features of dermatofibroma and DFSP have been described[54]; however, those studied do not harbor the COL1A1-PDGFB chimeric transcripts of DFSP.[55]One clinicopathologic classification scheme[56]describes the following 4 categories of dermatofibroma: Those with architectural peculiarities, such as deep penetrating, atrophic, giant, aneurysmal (angiomatoid), hemangiopericytomalike, palisading, or ossifying variants Cellular/stromal dermatofibromas, such as clear cell, granular cell, myofibroblastic, sclerotic, monster cell, atypical (pseudosarcomatous), elusive (hemosiderotic), cholesterotic (lipidized), and myxoid variants Dermatofibromas with architectural and cellular/stromal changes in homogeneous arrangement, including epithelioid cell, cellular benign, smooth muscle proliferative, basal cell carcinomalike, pseudolymphomatous,Multinucleate Cell Angiohistiocytoma(perhaps not a subtype of dermatofibroma), cellular neurothekeoma, plexiform fibrohistiocytic tumor, plexiform xanthoma, and plexiform xanthomatous tumor subtypes A complex, composite, or combined dermatofibroma[57]category with 2 or more architectural and cellular/stromal patterns in a single lesionOf the variants listed above, keep in mind that the uncommon sclerotic fibromalike dermatofibroma should be differentiated from sclerotic fibroma. One study[58]showed 7 of 7 of the former lesions to be negative for CD34 and CD99, while 3 of 3 solitary fibromas were positive for CD34 and CD99. For comparison, 14 of 14 "common-type" dermatofibromas in this study were negative for CD34, while 4 demonstrated positivity with CD99.In another study, CD10 was positive in 11 of 11 dermatofibromas and only positive in 1 of 7 epithelioid dermatofibromas, so it was postulated that epithelioid dermatofibroma may be a distinct entity.[59]Lichenoid dermatofibroma,[60]ulcerated dermatofibroma,[60]erosive dermatofibroma,[60]dermatofibroma with diffuse eosinophilic infiltrate,[61]and dermatofibroma accompanied by perforating dermatosis[62]have been described. Dermatofibromas with overlying sebaceous hyperplasia,[63]with intracytoplasmic eosinophilic globules,[64]signet-ring cells,[65]amyloid light chain deposition,[66]and incidental acantholysis[67]have also been reported. A case of an apocrine gland cyst with a hemosiderotic dermatofibroma was termed an apocrine hemosiderotic dermatofibroma.[68]Induction of adnexal structures by dermatofibroma is quite common and may mimic overlying basal cell carcinoma.[69]Two variants have been reported relatively frequently on the hands and feet. One shows schwannomalike features with lamellar and storiform fibrosis and a palisading of fibroblasts. The other is a myxoid variant, which appears to localize to the fingers and toes and is thought to share an association with mucous cyst of the finger.A case series[70]reported the uncommon occurrence of dermatofibroma and melanocytic lesions in the same biopsy specimen. Four of 14 specimens showed the 2 processes to seemingly merge imperceptibly. The lesions included junctional, dermal, and compound nevi as well as a single case of melanoma in situ. Knowledge of this relationship can help prevent rendering the wrong diagnosis and is facilitated by the use of immunohistochemistry, with the melanocytic lesions showing S-100 and Mart-1 positivity with FXIIIa negativity and the dermatofibroma showing S-100 and Mart-1 negativity and FXIIIa positivity. A subsequent case report[71]documenting an invasive melanoma occurring in association with a dermatofibroma underscores the role of these immunohistochemical stains.INI-1, present in 100% of dermatofibromas, but decreased or absent in the vast majority of epithelioid sarcomas in one study, can help distinguish between the 2 lesions.[72]Medical CareNo treatment is usually necessary for dermatofibromas. Simple reassurance that the lesion is benign may be indicated, unless one of the aggressive subtypes is suspected or diagnosed.Intralesional steroid injections have been attempted with variable results.Surgical CareFor cosmetically unacceptable lesions, those that are particularly symptomatic, if there is any diagnostic uncertainty, or when one of the aggressive subtypes is suspected, complete excision, including the subcutaneous fat, is the ideal procedure.An inverted pyramidal biopsy technique may allow for an aesthetically pleasing result, while still providing adequate tissue for histologic findings.[73]Superficially shaving the lesion or cryosurgery can be attempted for cosmesis or to decrease the symptoms; however, recurrences are more likely.Carbon dioxide laser treatment of multiple facial dermatofibroma has been reported.[74]More recently, pulsed-dye laser has been used with success.[75]Further Outpatient CareIf the dermatofibroma is not removed and significant change occurs in the color, size, border, or symptoms, the patient should seek follow-up evaluation.If complete removal has been previously attempted, patients with lesions that recur should seek follow-up evaluation. An aggressive subtype or another diagnosis should be ruled out.If multiple eruptive lesions develop, screening for autoimmune disease or altered immunity is warranted.PrognosisSimple dermatofibromas are considered a benign lesion, and the prognosis for patients with this condition is excellent.Aggressive subtypes (cellular, aneurysmal, atypical, and deep/subcutaneous) locally recur in up to 20% of cases and can rarely metastasize.In a study of common dermatofibromas with an increased mitotic rate but no other worrisome features, none recurred or metastasized.[76]Spontaneous regression has been reported,[27]and this may yield postinflammatory hypopigmentation, although this appears to be quite rare.Patient EducationFor patient education resources, see theProcedures Center, as well asMole Removal.