Department of Oncology - University of Oxford · In 2010, the Department of Oncology was formed...
37
Department of Oncology
Transcript of Department of Oncology - University of Oxford · In 2010, the Department of Oncology was formed...
Department of Oncology

Message from Professor Gillies McKenna, 2 Head of Department
Introduction 3
DNA Damage and Repair 4
Tumour Microenvironment 16
Clinical and Translational Research 28
Scientific Cores and Specialist Facilities 50
Training 60
Communicating the Impact of Research 62
Working in Partnership 64
Running the Department 66
Contents
With thanks to:
Photography by KJG Photography and Andrew Ogilvy Design by The Image Works (UK) Ltd Project managers: Claire Shingler and Peter O’Neill Writers/editors: Claire Shingler, Peter O’Neill, Martin Christlieb, Sarah Norman, Pam Nieto Other images supplied by research Group Leaders and Scientific Core Leaders
Acknowledgements
1For more information about our research and details of publications, please go to www.oncology.ox.ac.uk

2 3For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
In 2010, the Department of Oncology was formed with the vision of enhancing basic and clinical cancer research in Oxford. This was to be underpinned by maximising opportunities for multidisciplinary collaboration and scientific interaction with the ultimate goal of increasing cancer cure rates.
As Head of the Department of Oncology, it is with great pleasure that I can report that we are achieving this vision and fulfilling our aim to facilitate rapid translation from scientific discovery to patient benefit.
Together with the Cancer Research UK and Medical Research Council Oxford Institute for Radiation Oncology, we have focused our efforts on better understanding DNA damage and repair processes, defining the tumour microenvironment and enhancing radiotherapy treatments.
To realise success, it is vital that our research comes from a range of disciplines – some at the heart of traditional cancer research and others not historically linked with cancer. With this at the forefront of our minds, we have invested heavily in key
areas, such as medical physics, imaging, bioinformatics, pathology and clinical trials, to expand our capabilities in those areas where multidisciplinary collaboration is the only way to excel and lead the field. In Oxford, we are in a unique and privileged position to have a great wealth of broad-ranging expertise and a powerful network of cancer researchers.
We have worked hard to form close and lasting partnerships across Oxford. Thanks to a series of major initiatives managed through the Department, such as the CRUK Oxford Centre, the CRUK & EPSRC Oxford Imaging Centre, the Biomedical Research Centre Cancer Theme and the Experimental Cancer Medicine Centre, we have seen major developments in our understanding of cancer. There have been huge advances, to name but a few, in determining potential molecular agents to improve efficacy of treatment, in applying imaging methods for earlier detection of metastases and identifying biomarkers to aid in defining the most appropriate treatment for each patient. By coupling these partnerships to effective collaboration with colleagues in the Oxford University Hospitals NHS Trust, we strive to become the leading centre for translational early phase oncology trials in the UK and to lead national networks in our areas of expertise such as radiotherapy and precision medicine.
We pride ourselves on supporting and training the next generation of world leaders in cancer research to ensure our research and clinical excellence continues over the long term. Our multidisciplinary graduate and postdoctoral training programmes for both scientists and clinicians are internationally recognised and attract the most promising and able scientists from around the world.
We see the next decade as one where this integration and collaboration will enable huge strides in our understanding of cancer and how best to treat it.
I hope you enjoy reading more about the Department of Oncology, our people, and the depth and breadth of the activities we support.
Professor Gillies McKenna
Head of Department of Oncology
Message from Professor Gillies McKenna, Head of Department
Welcome to the Department of Oncology brochure. It has been an exciting time since the Department came into being in 2010; one in which we have seen collaboration, expansion and important scientific discoveries.
The formation of the Department brought together the CRUK/MRC Oxford Institute for Radiation Oncology (formerly the Gray Institute for Radiation Oncology and Biology) and the pre-existing departments of Medical Oncology and Clinical Pharmacology. It was born out of a collective desire amongst senior leaders in Oxford and major funders to create a structure for cancer research in Oxford that would maximise opportunities for future improvements in the treatment and detection of cancer.
The Department now houses over 400 staff and postgraduate students - both clinical and non-clinical - and is one of the largest departments in the University of Oxford’s Medical Sciences Division. It brings together research and clinical groups from across Oxford who are based in the Old Road Campus Research Building, the Radiobiology Research Institute, the Weatherall Institute for Molecular Medicine and the NHS Cancer and Haematology Centre.
Our research and clinical activities contribute to an annual Department turnover of £26M. Much of this is external research funding, including over £10M per year provided by CRUK and the MRC as funding to the CRUK/MRC Oxford Institute for Radiation Oncology; a specialist radiation biology centre of excellence which sits within the Department. Other funding comes from a variety of sources, including charities, industry, government (NIHR, Department of Health and Research Councils) and the European Commission (EC). The department is involved in numerous clinical trials to take our research to patients.
Supporting researchOur main research themes of DNA damage and repair, tumour microenvironment and clinical and translational research are strongly supported by an expanding group of core specialist facilities equipped with state-of-the-art equipment and staffed by highly qualified individuals with knowledge and expertise in a number of areas. We have strong links with other parts of the University and also benefit from local expertise in neighbouring University facilities such as the Target Discovery Institute.
All research and clinical activities are underpinned by a multi-faceted administration team who provide financial and HR management, graduate studies support and facilities and Health and Safety provision.
Working and studying with usWe are committed to maintaining organisational and cultural practices that promote gender equality, and to improving the working environment for all. The personal and career development of our students and staff is very important to us and we are working hard to ensure that our most talented researchers, both men and women, are supported to become the future leaders in their fields.
We have embedded into our culture an annual personal development review process for all staff and we provide a mentoring programme for our postdoctoral researchers and group leaders. We also have a postdoctoral network and run a busy programme of seminars with speakers invited from around the world. Our postgraduate students are provided with a world-class academic environment and the best support services, including a comprehensive portfolio of personal and professional skills development.
In recognition of our efforts, we were awarded a departmental Athena SWAN Bronze award in July 2014 and are working towards gaining a Silver award.
The Department of Oncology’s Main Funders
52%
18%
9%
8%
6%4% 3%
CRUK
MRC
Other Charity
Industry
Government
ECOther Research Council (3%)
Introduction

4 5For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
DNA Damage and Repair
DNA contains the critical genetic information in all living cells. When cells grow and divide they need to correctly replicate their DNA and repair any mistakes or damage to their DNA. Unrepaired damage can lead to accumulation of mutations, in turn producing genome instability which can ultimately drive the uncontrolled proliferation of cells that is one of the hallmarks of cancer.
DNA damage responses
We are particularly interested in characterising the mechanisms of induction of damage to DNA and understanding how the damage is repaired. The research focuses on identifying biomarkers in DNA damage and repair pathways for clinical application; identifying targets in these repair pathways that could be exploited for therapeutic gain; and taking compounds active on these targets to clinical trial.
Genomic stability is essential for cells to survive and to prevent the onset of tumourigenesis. DNA damage responses, mediated by signalling networks, play a key role in maintaining genomic stability and are affected by several cellular processes such as cell cycle progression
and replication, and by chromosome structure, chromatin and telomeres. Failure of these responses causes genomic instability and cancer.
Research at Oxford brings together scientists working on different but complementary elements that impact on DNA damage responses; these range from studies on telomeres and maintenance of telomere integrity, to chromosome structure and the mechanisms of DNA damage repair. A diversity of approaches and expertise is harnessed using simple organisms such as yeast, through to human cell culture and mouse models to provide new insights into the maintenance of genomic stability and its role in preventing cancer development and progression.
DNA damage and repair as a therapeutic target
DNA damage and repair plays a dual role in cancer: aberrant repair drives genomic instability and tumourigenesis. However, many therapeutic agents and radiation exert their anticancer effects by generating DNA damage. For example, radiotherapy and some
chemotherapies cause single- and double-strand breaks, DNA interstrand cross links (ICLs–a particularly toxic form of DNA damage), replication lesions and base damage. These all prevent cancer cell replication and drive cancer cell death. Thus, repair of this ‘therapeutic’ damage can make cancer cells insensitive to these agents.
Researchers in Oxford are identifying and characterising key molecules and mediators in DNA damage and repair pathways that play a pivotal role in determining cancer cell sensitivity to DNA damage-inducing agents. The aim is to develop novel techniques for sensitising (or re-sensitising) cancer cells to DNA-damaging radiotherapy or chemotherapy in order to enhance tumour cell eradication while reducing damage to non-cancerous tissue.
DNA damage in early detection of cancer
Oxford researchers are using several biomarkers, which are proving to be a valuable research tool, to identify cells with DNA damage accumulation and detect cells which ‘poorly’ repair DNA damage. Identification of cells with DNA damage accumulation would also be a valuable clinical tool for early detection of potentially cancerous cells. These approaches are also being used for early detection of DNA damage in model systems.
The research in Oxford on DNA damage and repair mechanisms is providing new insight into the aberrant processes and key mediators that drive cancer development and progression. This insight will facilitate the identification of novel targets for therapeutic intervention. It will also contribute to improvements in the effectiveness of therapies that work by introducing DNA damage in cancer cells.
DN
A D
amag
e and
Rep
air
DNA Damage and Repair

6 7For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
We aim to identify novel cell proliferation pathways to investigate drug resistance and predict response to chemotherapy and ionising radiation. Our work focuses, in particular, on two processes relevant to cancer cell survival: (1) the role of ubiquitin–mediated proteolysis and (2) metabolism of deoxyribonucleotides (dNTPs). Further investigation into these processes will prove to be a powerful tool for the design and implementation of novel therapies.
Alteration of mechanisms monitoring cell cycle progression leads to cancer whereby cell proliferation is not integrated with checkpoint control signals. Instead cancer cells tend to proliferate in an uncontrolled fashion and become insensitive to external stimuli and checkpoint signals that ensure correct execution of the cell cycle. The ubiquitin proteasome system (UPS) lies at the heart of checkpoint mechanisms and dictates the fate of cellular proteins by tagging specific proteins with the small molecule ubiquitin. Single ubiquitin molecules are added via an enzymatic cascade, in which ubiquitin is activated by a covalent linkage to an activating enzyme (E1 ubiquitin) and transferred to a conjugating enzyme (E2 ubiquitin). The E3 ubiquitin ligases mediate the transfer to a lysine residue in the substrate from E2 ubiquitin to form polyubiquitin chains. Polyubiquitinated proteins are recognised for degradation by the proteasome (Figure 1).
Human cancers contain altered UPS components and E3 ubiquitin ligases, which highlights the relevance of these proteins in regulation of cell survival and proliferation. Furthermore, the blockage of the UPS is currently exploited for the treatment of cancer through the use of bortezomib, a general inhibitor of the proteasome. Therefore, we are investigating the role of E3 ubiquitin ligases in cancer cell proliferation. Our studies will prove useful in developing effective therapies that specifically target the mechanism of action of E3 ubiquitin ligases and improve the efficacy of current approaches targeting the UPS.
Substrate
Nedd8NAE
+ ATP
AMP + PPi
E1
E2
Ub
Ub
E2
Rbx1/2
(Bortezomib)
Adaptor
Substraterecognition
Cullin
Ub
Proteasome inhibitor
NAE inhibitor(MLN4924)
Activator/inhibitor of substrate recognition
Multi-subunit Cullin-Ring ubiquitin Ligase E3
Degron
Chemical approaches to modulate the UPS
Substrate
E1
Tom Brown
Tom Brown came from Southampton to Oxford University in 2013 to take up a joint Chemistry/Oncology position as Professor of Nucleic Acid Chemistry. He has published over 300 scientific papers and patents and has received several awards including the Royal Society of Chemistry awards for nucleic acid chemistry and for interdisciplinary research. He is President of the Chemistry Biology Interface Division of the Royal Society of Chemistry, co-founder of several biotech companies and is Chemistry World Entrepreneur of the Year for 2014. Tom is a Fellow of the Royal Society of Edinburgh and a Fellow of the Royal Society of Chemistry.
DNA Damage Signalling Group
Figure 1: Cullin-Ring ubiquitin Ligases (CRLs) are multisubunit E3 enzymes: This figure presents the assembly of a prototypical multi-subunit E3 through adaptors. Substrates contain a degron that serves as a signalling platform for the recruitment by the E3. Rbx1/2 are recruited by cullins to bridge the substrate selected by the substrate recognition protein to the E2. E2 and E1 provide activated ubiquitin molecules that are coupled with target lysine residues within the substrates. Poly-ubiquitinated substrates are degraded by the proteasome. NAE (Nedd8-activating enzyme) catalyses the transfer of Nedd8 to cullins. Chemical approaches to target the UPS are outlined. Figure published in British Journal of Cancer 9 December 2014 doi:10.1038/bjc.2014.594
DN
A D
amag
e and
Rep
air
DN
A D
amag
e and
Rep
air
Our group designs and synthesises chemically modified DNA for diagnostic and therapeutic applications. My research is in nucleic acid chemistry and structure, and the application of nucleic acids and analogues to diagnostics and therapeutics. Using various biophysical techniques including X-ray crystallography we study the nature of base mispairing in DNA, the
structure of DNA duplexes containing mutagenic lesions and the interaction of DNA with specific repair enzymes.
We have also developed rapid methods for the identification of mutations in the human genome without the need for DNA sequencing. The best example is Scorpion primers which are used in fluorogenic real-time PCR to analyse genomic DNA sequences at specific loci. Scorpions were developed in collaboration with AstraZeneca (subsequently an AZ spin-out DxS), and have been used in companion diagnostics.
By determining the genotype of a cancer, this technology allows the clinical use of cancer drugs which were previously rejected on the basis of limited efficacy.
For example, a Scorpion kit is used to group patients on the basis of their KRAS mutation status; and as a result of this the drug Vectibix® was approved for the KRAS wild-type population for which it is particularly effective. Similarly an EGFR kit is being used to establish the mutation status of non-small cell lung cancer tumours to determine likely response to the drugs Iressa® and Tarceva®. The Scorpion technology has been acquired by Qiagen who recently obtained FDA approval of the KRAS kit in the US for use with the colorectal cancer drug Erbitux®.
We are also working on the synthesis of analogues of DNA for therapeutic applications and we have recently started a project on the synthesis of next generation aptamers with the aim of specifically targeting cancer cells with drugs. In this project we aim to develop DNA and RNA aptamers with additional chemical functionality (such as hydrophobic - water-repelling - groups and hydrogen bonding residues) to increase target binding and selectivity beyond that which is achieved by the use of traditional aptamers.
Nucleic Acids Research Group
We synthesise cyclic mini-DNA duplexes to facilitate the study of base pairing in DNA (including mutagenic lesions) at high resolution
Vincenzo D’Angiolella
Vincenzo D’Angiolella is an MRC Group Leader at the CRUK/MRC Oxford Institute for Radiation Oncology. He has a Medical Degree (MD) from the University of Naples “Federico II” and completed his PhD at the same University in the field of General Pathology. Following the completion of his studies, he worked as a postdoctoral fellow at the New York University School of Medicine in the USA in the laboratory of Dr Michele Pagano. He has been awarded fellowships from AIRC (Associazione Italiana per la Ricerca sul Cancro) and AICF (American Italian Cancer Foundation) and was a Scholar of the Leukemia & Lymphoma Society from 2008 to 2011.

8 9For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
The long-term goal of our work is to study the proteins and mechanisms involved in the coordination and regulation of Base Excision Repair. Our research focuses on the study of the proteins and mechanisms involved in the coordination and regulation of Base Excision Repair (BER, Figure 1), to unravel their role in the repair of radiation-induced DNA damage and to examine the relationship to human diseases, such as cancer.
BER is a frontline DNA repair system that is responsible for maintaining genome integrity, thus preventing many human diseases, including premature ageing, cancer, and neurodegenerative diseases. It is estimated that through BER pathway a human cell repairs 10,000-20,000 DNA lesions every day. The majority of these lesions arise from the intrinsic chemical instability of DNA, resulting in DNA single-strand breaks, hydrolytic loss of DNA bases, base oxidations, non-enzymatic methylations and other chemical alterations. BER is also the principal DNA repair system in cancer cells that counteracts the killing effect of the major cancer treatments, i.e. chemotherapy and ionising radiation (approximately 80% of DNA damage induced by ionising radiation are DNA base lesions).
Changes in BER capacity most probably are responsible for many cases of cancer treatment efficiency, since many cancers have altered expression of BER proteins. Although BER enzymes have been studied in detail, the mechanisms involved in BER coordination and regulation are unclear.
The Biochemistry Laboratory has identified a novel molecular mechanism that regulates expression of BER proteins and coordinates DNA repair with the cell cycle progression (Figure 2). These studies are providing new insight into the biochemistry and regulation of DNA repair and how they impact cancer development and progression.
The aim of our research is to understand how genome stability is maintained in response to DNA double-strand breaks. Exposure to ionising radiation (IR) can cause chromosome breaks, in which both DNA strands are broken. In addition to causing cell death (the desired outcome during radiation therapy) such lesions can also cause chromosomal rearrangements, a hallmark of cancer cells, which can lead to oncogene activation or tumour suppressor loss. We are examining the mechanisms and determinants of DNA double-strand break (DSB) repair in normal cells, and how misrepair can lead to chromosomal rearrangements, genome instability and cancer.
DNA is tightly wrapped up around proteins called histones to form chromatin. We have studied a chromatin mark, (histone H3 methylated on lysine 36), which is frequently lost in human cancers, most notably in more than 50% of high grade paediatric gliomas (childhood brain tumours). From our studies using fission yeast (Schizosaccharomyces pombe) we have found this mark to have an important role in DSB repair. Further, we identified a role for this chromatin mark in human cells in facilitating DSB repair within active genes across the genome and its loss leads to aberrant DSB repair associated with loss of genetic material. These findings are helping us understand how DNA damage can lead to chromosomal rearrangements, thus promoting tumourigenesis.
Further, we have exploited powerful genetic approaches (synthetic lethality) in yeast and human cells to identify drugs, which specifically kill cancer cells that are deficient in this chromatin mark. Using this novel combination of approaches we are now translating our findings into the clinic.
Chromosome Integrity GroupBiochemistry and Regulation of DNA Repair Group
Grigory Dianov
Grigory Dianov is Professor of Molecular Biology and MRC Group Leader at the CRUK/MRC Oxford Institute for Radiation Oncology. He came to the UK in 1990 and spent three years as a Senior Research Fellow at the Imperial Cancer Research Fund, Clare Hall Laboratories. From 1993 to 1995 he was a Visiting Associate Professor within the Department of Pathology at the University of Texas, USA and then joined the National Institute on Aging in Baltimore, USA. He returned to the UK in 2000 as a Senior Group Leader within the Radiation and Genome Stability Unit of the Medical Research Council, before coming to Oxford to lead the Biochemistry Laboratory within the CRUK/MRC Oxford Institute for Radiation Oncology in 2007.
Figure 1: BER pathway
DN
A D
amag
e and
Rep
air
DN
A D
amag
e and
Rep
air
Lig3
Pol b
AP site
DNA glycosylase
APE1
Damaged base
DNA strand breaks containing blocked DNA ends
SSB end processors: Pol β, APE1, Tdp1/2,
PNKP, Aprataxin
P 5' 3'
Nicked DNA
One nucleotide gap
5' 3'
Repaired DNA
OH
BER pathway
CHIP
Cytoplasm
Nucleus
Proteasome
Lig 3
XRCC1
DNA damage
DNA repair
Pol b
Pol b
Pol b Pol b
Pol b
Mule
Pol b
ATM
PPM1G
USP7S
Mdm2 p53
Cell cycle delay
CK2
BER regulation Figure 2: BER regulation
Tim Humphrey
Tim Humphrey is an Associate Professor and MRC Group Leader at the CRUK/MRC Oxford Institute for Radiation Oncology. Tim performed his doctoral studies at the University of Oxford and was an EMBO and HFSP postdoctoral research fellow at Harvard Medical School before returning to the UK to become a group leader at the MRC Radiation and Genome Stability Unit, Oxfordshire. He was awarded tenure in 2003, and in 2008 he moved to the CRUK/MRC Oxford Institute for Radiation Oncology in Oxford and heads the Chromosome Integrity Group. As Director of Studies, he oversaw the development of the Institute’s graduate studies research programme.
Modulating chromatin through histone methylation orchestrates repair of DNA double-strand breaks. SETD2-dependent trimethylation of histone H3 lysine 36 (H3K36me3) is associated with active genes. Following a DNA double-strand break (zigag), this chromatin mark promotes accurate repair by homologous recombination (HR) through recruitment of repair factors to the break site. In the absence of this chromatin mark these factors are not recruited efficiently and instead the break is repaired by error-prone microhomology-mediated end joining (MMEJ) leading to mutations in active genes.

10 11For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
We are investigating DNA damage signalling and repair factors in bladder cancer to develop new radiotherapy-based treatments and to identify markers for personalised treatments. Patients with muscle-invasive bladder cancer (MIBC) can be treated by surgical removal of their bladder or radiotherapy-based treatments. Radiotherapy has the advantage of bladder preservation. Adding chemotherapy to radiotherapy makes the tumour more sensitive to radiation and improves outcomes but adds to the side effects of treatment. We have found that muscle-invasive tumours repair their DNA less efficiently than normal tissues and we are trying to exploit this difference by using radiosensitising drugs which target the remaining DNA repair pathways, thus damaging the tumour more than the surrounding normal tissues. Such drugs include gemcitabine, which is already in clinical use as a radiosensitiser and the histone deacetylase inhibitors. Further understanding of the mechanisms of action of these drugs will allow the development of more specific agents, which should result in reduced side effects.
We are also looking for markers in patients’ tumours which could help us predict which patients would benefit most from a particular treatment, and this could help patients make their choice between surgery and radiotherapy-based treatments. One such marker is the DNA damage signalling protein MRE11, which we found predicted patient survival after radiotherapy but not surgery, in two groups of patients. We are testing this marker further in tissue from patients treated in two large randomised clinical trials. Muscle-
invasive bladder tumours seem to have a shortened version of MRE11 and this could be important in terms of our clinical findings, so we are studying this in more detail. We have also found that a genetic variant of the MRE11 gene found in patients’ blood also predicted for radiotherapy outcomes and we are investigating the underlying mechanisms further. We are also exploring other predictive markers in tissue microarray samples from our patients, in an exciting
Citizen Science project, where members of the public score our tumour samples, based on pattern recognition. 'Reverse the Odds' is an award winning mobile game developed by the Citizen Science team at CRUK in collaboration with Channel 4, Maverick TV and Chunk.
DNA Repair in Cancer Treatment Group
Anne Kiltie
Anne Kiltie is an Associate Professor and CRUK Clinical Group Leader at the CRUK/MRC Oxford Institute for Radiation Oncology. She is also an Honorary Consultant Clinical Oncologist at Oxford University Hospitals NHS Trust. Between 2001 and 2009 she was a Senior Lecturer/Honorary Consultant Clinical Oncologist at Leeds Institute of Molecular Medicine and St James’ University Hospital, Leeds. She was previously a Clinical Research Fellow at the Imperial Cancer Research Fund (ICRF) Clare Hall Laboratories in Hertfordshire. Her clinical training was undertaken at the Christie Hospital, Manchester, and Cookridge Hospital, Leeds. Anne is the winner of the 2015 Research Engagement Award in the Flame of Hope Awards from CRUK.
Figure 1: Bladder cancer cells stained for two molecular markers following irradiation.
DN
A D
amag
e and
Rep
air
DN
A D
amag
e and
Rep
air
Figure 2: Consistency of IHC staining for MRE11 across three clinical trial sites.
Nicholas La Thangue
Nicholas La Thangue is Professor of Cancer Biology in the Department of Oncology, and was previously Cathcart Professor of Biochemistry at the University of Glasgow, and before that a scientist at the Medical Research Council. He is a Fellow of the Royal Society of Edinburgh, a Member of the European Molecular Biology Organisation (EMBO), a Fellow of the Academy of Medical Sciences, a Fellow of the European Academy of Cancer Sciences, a Fellow of the Lister Institute and Professorial Fellow at Linacre College Oxford. He has founded several biotech companies, most recently Oxford Cancer Biomarkers.
Research in our group focuses on the mechanisms that give rise to the abnormal proliferation characteristic of tumour cells. An underpinning theme of our studies is that we believe, in order to design better therapies that effectively treat cancer, it is essential to decipher the molecular and biological details of pathways that control proliferation in normal cells and thereafter understand how they become aberrant in cancer.
A hallmark of tumour cells is evident in the control of the G1 to S phase transition; in normal cells this transition is tightly regulated whereas tumour cells progress liberally into S phase in an unrestrained fashion.
There are two key pathways of pivotal importance that govern progress through G1 into S phase, controlled by the retinoblastoma tumour suppressor protein pRb and the p53 tumour suppressor protein. pRb principally acts as a transcriptional regulator of the E2F family of cell cycle regulating transcription factors. In contrast, p53 is a stress-responsive transcription factor that activates genes involved with cell cycle arrest and apoptosis. Most tumour cells harbour mutations that alter pRb and p53 activity. Loss of pRb results in deregulated proliferation as a consequence of liberating E2F activity, whereas loss of p53 causes an insensitivity to checkpoint control.
The primary objective of our work is to explore the regulation of and control by pRb and p53 activity. Specifically, we have defined new levels of control in regulating pRb tumour suppressor activity, particularly novel post-translational signals. We have elucidated new members of the E2F family, and identified the key pathways through which they act. Functional characterisation of E2F in cell cycle control and apoptosis has identified a remarkable level of complexity that governs the switch to apoptosis. Our p53 research is principally focused on uncovering the diverse modifications that dictate the outcomes of the p53 response to stress.
We believe that biological knowledge on the mechanisms which drive cancer cell proliferation can be harnessed in designing new therapeutic modalities to treat cancer. Consequently, we work closely with the bio-technology and pharmaceutical sectors, together with clinical colleagues in translating our academic discoveries into an applied clinical setting. Drugs emanating from our earlier studies have been approved for haematological malignancy.
A major focus of our current work is to develop technologies that enable predictive biomarkers to be identified for cancer therapies. We have devised a genome-wide loss-of-function screen that identifies predictive biomarkers and deployed the platform to develop companion diagnostic tests for diverse cancer drugs.
Cancer Cell Cycle Group

12 13For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
We are investigating how cells resolve replicative stress arising from endogenous and exogenous sources and how failure to do so impacts on genome stability, cancer development and ageing. Our research in genomic instability syndromes and development of cancer focuses on understanding the mechanisms disrupted in a childhood cancer predisposing syndrome named Fanconi Anaemia (FA). Children afflicted with FA show developmental defects, progressive bone marrow failure and have up to 1000 fold increased cancer risk. This underscores the essential role of this pathway in suppressing tumour formation.
The genes mutated in this syndrome encode a network of ‘caretaker’ proteins, which not only ensure that DNA is accurately copied but also prevent replication failure and associated genomic instability. Consequently, a properly functioning FA pathway is important for normal development, haematopoiesis and suppression of solid tumours in everyone, and as such underscores the importance of research in this area.
We are particularly interested in how the repair of damaged DNA is executed in the context of the replication fork, and how fork stability is achieved under stressful conditions. To address these questions we are employing state-of-the art techniques that allow monitoring of DNA replication at the single molecule level in vivo (Figure 1). Using these approaches we aim to explain how the FA proteins function to promote DNA replication, and whether dysfunctional replication-mediated DNA repair is a common signal that drives FA disease progression to leukaemia.
A long-term goal of our research is to elucidate the FA-dependent mechanism required to suppress devastating haematological and malignant conditions and translate our basic laboratory findings into the development of novel therapies for cancer.
DNA Repair and Replication Group
Peter McHugh
Peter McHugh is an Associate Professor and Group Leader in the Department of Oncology. Following a period of postdoctoral research at University College London, he was awarded a Royal Society University Research Fellowship in 2001. In 2002 he joined the Oncology Laboratories at the MRC Weatherall Institute of Molecular Medicine, where he heads the DNA Damage and Repair research group. He is a co-organiser of the UK Genome Stability Network Annual meeting and of the FEBS Nucleotide Excision Repair and Interstrand Crosslink repair meeting.
DN
A D
amag
e and
Rep
air
Figure 1: (A) DNA labelling procedure. (B) Newly replicated DNA. (C) Examples of replication structures that can be visualised with this technique. Representative images showing (D) co-localisation of γH2AX (red) and CldU (green) foci in WT DT40 and ΔFANCM cells treated with CPT and (E) increased Rad51 foci formation in FANCM-depleted cells treated with HU.
DN
A D
amag
e and
Rep
air
Wojciech Niedzwiedz
Wojciech Niedzwiedz is a Group Leader in the Department of Oncology, based at the Weatherall Institute of Molecular Medicine. He came to Oxford in 2007 after receiving a Senior International Research Fellowship from the Association for International Cancer Research to set up his own laboratory. In 2012 he was awarded a MRC Senior Non Clinical Fellowship to continue his work on dissecting the FA tumour suppressor pathway. He is a member of the Polish Radiation Research Society and the European Environmental Mutagen Society.
We aim to understand how repair of damaged DNA is controlled during chromosome duplication, and why potentially dangerous changes in cell behaviour can occur when this process goes wrong. The DNA contained in our chromosomes holds our genetic blueprint (genome). Before dividing, cells must copy their DNA accurately to prevent changes being introduced into our genome. DNA damage can lead to errors being created during chromosome replication, including mutations that lead to cancer. Cells have evolved elaborate repair mechanisms to fix this damage and ensure that the genetic information is faithfully duplicated. Understanding these mechanisms has important implications for efforts to prevent cancer, while also helping to identify individuals who might be at increased risk of developing cancer.
A related aspect of our work focuses on improving cancer treatment. Many chemotherapy drugs and radiotherapy kill tumour cells by damaging their chromosomal DNA. For many cancer patients, such treatment improves their chances of survival, but sometimes these approaches fail. There is evidence that an increased capacity to repair the DNA damage induced by cancer therapies is an important factor in treatment failure.
One area of particular interest is the repair of DNA interstrand crosslinks (ICLs), which are formed when the two strands of the DNA double-helix become covalently linked together. ICLs are an extremely toxic form of DNA damage that prevent fundamental processes including DNA replication. Defects in ICL repair result in cancer predisposition syndromes, such as Fanconi anemia, underlining the importance of ICL repair in human development and cancer avoidance. Conversely, many important cancer chemotherapeutics work through ICL formation. Together, these facts emphasise the importance of understanding ICL repair for improving cancer prevention and treatment strategies (Figure 1).
Related to these ICL repair studies, we have a major interest in a family of DNA repair factors that contain a metallo-β-lactamase fold. These factors, the human SNM1 (DCLRE1)-family nucleases, play a key role in processing of ICLs and other forms of DNA damage (Figure 2). Here, our basic research programme is coupled to collaborations with chemists and structural biologists with the aim of developing inhibitors of repair factors, to help overcome tumour resistance to DNA damaging chemotherapy and radiotherapy.
DNA Damage and Repair Group
Figure 2: The domain organisation of the three metallo-β-lactamase fold DNA repair enzymes found in humans. The MBL fold is shown in blue and the distal β-CASP (CPSF-Artemis-SNM1-Pso2) domain is shown in green. Highly conserved motifs within these are highlighted.
Figure 1: How does SNM1A initiate interstrand crosslink repair? Our work suggests that the SNM1A nuclease (in green) can bind DNA at a single nick and digest past the ICL, removing one of the damaged strands. This will permit downstream processes such as homologous recombination and damage tolerance mechanisms to effect complete repair of the ICL.

14 15For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
Our research is focused on how homologous recombination regulates telomeres and acts to prevent genomic instability. The ability of cancers to tolerate DNA damage and grow, despite the accumulation of genetic errors, is a hallmark of human tumours. Our group is using genetic tools to determine how normal and tumour cells differ in their responses to DNA damage induced by ionising radiation (Figure 1).
Our focus is to define the cellular roles of homologous recombination genes, which protect us against cancer and are involved in repair of DNA lesions. Cells lacking these genes accumulate chromosome breaks (Figure 2). The breast cancer-associated gene BRCA2 is one such example. Mutations in BRCA2 gene in cancer cells promote breast tumours, whilst paradoxically the same mutations cause normal cells to stop dividing. We have been screening human genes to identify those which, when mutated, prevent cells from dying and cause cancer. If some of these genes are mutated in human tumours and if mouse models implicate them in tumour cell survival and proliferation, then this work
could be a source of novel therapeutic targets that may prove more tractable, from a pharmaceutical point of view, than currently known tumour suppressors.
Another major line of investigation in Dr Tarsounas' laboratory is the action of homologous recombination proteins at telomeres. Telomeres are key structures at chromosome ends in all eukaryotes, consisting
of repetitive DNA sequences and associated proteins. They are biologically fascinating because they protect chromosome ends from degradation and fusion, both leading to chromosome mis-segregation, genome instability and onset of tumourigenesis. In addition, due to their repetitive and G-rich DNA sequence, telomeres pose an intrinsic barrier to genome replication. We are investigating how factors involved in homologous recombination facilitate successful completion of telomere replication, thus protecting genomic integrity. These studies are extended to analyse how telomere dysfunction (Figure 3), generated in genetically defined models for cancer development, can make cancer cells more vulnerable to killing by radiation therapies.
Kristijan Ramadan
Kristijan Ramadan is an MRC Group Leader and Associate Professor at the CRUK/MRC Oxford Institute for Radiation Oncology. He holds degrees in Veterinary Medicine (DVM) and Pathology (MSc), and a PhD in Biochemistry and Molecular Biology. Between 2009 and 2013 he was a Junior Group Leader and Lecturer at the Institute of Pharmacology and Toxicology-Vetsuisse, University of Zurich. He received a Proud of Croatia Award (Croatian Hero for 2014) for his scientific contribution in saving the life of a young boy who suffered from liver cancer due to mutations in SPRTN gene.
DN
A D
amag
e and
Rep
air
Figure 1: Accumulation of homologous recombination proteins RAD51 ad RAD51C into sub-nuclear foci in response to ionising radiation.
Figure 2: Chromosome breakage in human cancer cells lacking Brca2 gene (arrows indicate breaks).
Figure 3: Dysfunctional telomeres (green) are recognised as damaged DNA (red) and can initiate cancer.
Genome Stability and Tumourigenesis Group
DN
A D
amag
e and
Rep
air
Madalena Tarsounas
Madalena Tarsounas is a CRUK Group Leader and Associate Professor within the CRUK/MRC Oxford Institute for Radiation Oncology. After obtaining her PhD at York University in Toronto, Canada, she undertook postdoctoral training at the CRUK Clare Hall Laboratories, London Research Institute, where she held fellowships from the European Molecular Biology Organization (EMBO) and The Breast Cancer Campaign. In 2011, she was elected EMBO Young Investigator. Dr Tarsounas has co-organised several international meetings, including the EMBO Workshop on Chromosome Structure, Damage and Repair (2011) and the Ramon Areces Symposium on Telomeres and Telomerase (2011). Dr Tarsounas has established the EMBO conference on DNA damage responses in cell physioogy and disease, which has now become a biennial international event.
We are interested in the role of the ubiquitin-proteasome system in DNA repair, ageing, cancer and radiotherapy. The research focus of the group is to understand the role of the ubiquitin-proteasome system (UPS) and its central component p97/VCP in genome stability. We aim to understand how can we use this knowledge to improve current cancer therapy, especially after ionising radiation. p97/VCP is a evolutionarily conserved segregase that with the help of specific cofactors binds and remodels (segregates) diverse and mostly ubiquitinated proteins (substrates) in a variety of cellular processes and compartments. In this way p97/VCP and its cofactors play an essential role in the maintenance of protein balance (homeostasis) in the cell. We are especially interested in chromatin-related p97/VCP functions and consequently in chromatin-related protein homeostasis (Figure 1; p97/VCP-dependent chromatin-associated protein homeostasis) after DNA damage. Chromatin is the substance of a cell nucleus consisting of DNA, RNA and proteins, and the basic source of genetic information.
Using biochemical and cell biological approaches we are investigating fundamental molecular aspects of protein homeostasis in DNA replication, DNA repair and DNA damage response. Mechanistic insights of basic cellular processes related to DNA metabolism and related protein homeostasis can improve our knowledge of ageing and ageing-related diseases as well as current diagnosis, prognosis and treatment of cancer.
We have identified the essential role of p97/VCP in chromatin and in DNA damage response, after ionising and ultraviolet radiation. We have discovered a new human syndrome characterised by premature ageing and early onset hepatocellular carcinoma (Figure 2; green arrow indicates tumour mass) that is caused by mutations in p97-cofactor SPRTN (Figure 3; genomic localisation and protein structure of SPRTN with patient mutations).
Our results strongly suggest that protein-induced chromatin stress (PICROS; pathological accumulation of proteins on chromatin) plays an essential role in cancer and ageing. The group is currently trying to understand how chromatin-associated protein homeostasis regulates PICROS and thus prevents accelerated ageing and cancer. We believe that understanding of PICROS might open new avenues in cancer diagnosis, prognosis and therapy, but also answer fundamental questions about ageing.
DNA Damage Response Group
Figure 1.
Figure 2.
Figure 3.

16 17For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
Like any other cells in the body, tumour cells are influenced by blood vessels and the normal cells and molecules that surround and feed the tumour cells – the tumour microenvironment.
Of all the cells found in solid tumours, tumour cells usually only account for 30-60%. The remainder are non-transformed (normal) cells such as fibroblasts, endothelial cells and immune cells. These normal cells are thought to have been commandeered by the tumour into playing a supporting role to help tumour growth, in many cases resembling a wound healing pathology with tumours referred to as ‘wounds that do not heal’.
Endothelial cells (which allow the formation of new vasculature) are essential for the provision of oxygen and nutrients to the growing tumour, while fibroblasts (which are usually activated as ‘myofibroblasts’) are an essential source of extracellular matrix and growth factors that assist tumour growth. The immune cells that are present within solid tumours are usually inactivated by immune-suppressive mechanisms associated with other tumour cells and this provides an opportunity for immune ‘reawakening’ to create an anticancer immune response. This complex mixture of cells comprises what we call the tumour ‘microenvironment’, and the interplay of cells within
the tumour microenvironment provides a range of new opportunities for therapeutic intervention.
Using the tumour microenvironment to identify novel therapeutic targets
Researchers in Oxford are investigating the tumour microenvironment in a number of ways. The ability of tumours to recruit a new blood supply provides an important point of therapeutic intervention that can severely restrict tumour growth and development. Innovative cancer killing viruses and oncolytic vaccines are being designed and developed to utilise the immune system to target tumour cells, leaving normal cells unharmed. This approach can be used in targeted cancer therapy in combination with biological agents.
Work is also underway to better understand signalling pathways within the cell and how alteration of these pathways can influence cancer onset and therapy. Gene mutations specific to lung cancer and changes in the microenvironment of pancreatic cancer are being exploited to identify novel therapies and optimise combination treatments including radiation therapy. The microenvironment is also thought to be crucial to allowing spread of cancer around the body (the process of ‘metastasis’), and the interaction of tumour cells with
normal cells at sites of potential metastasis is a central research focus.
Earlier detection of metastases
Specialised imaging technologies are being used to identify and better understand microenvironmental processes that are involved in, for example, loss of local control, invasiveness and metastasis. Work is ongoing to advance and apply imaging methods for earlier detection of metastases. Furthermore, novel methods using radionuclides are being developed to enable imaging of proteins inside cancer cells, such as those involved in DNA damage repair signalling. It is hoped that advances in this area will enable both earlier detection and improved treatment of cancers.
Targeting hypoxia
A key focus of researchers in the CRUK/MRC Oxford Institute for Radiation Oncology is overcoming resistance to radiotherapy. Programmes are underway to investigate
the molecular mechanisms that contribute to radiation survival and to target these mechanisms to sensitise tumour cells to radiotherapy.
An example is the study of hypoxia (areas of low oxygen), which is common in tumours and often associated with poor treatment outcome, both with chemo and radiotherapy. As such, hypoxia provides a target for cancer therapy. This is the subject of investigation, both by finding ways of making tumours less hypoxic during radiation therapy and by identifying drugs that target specifically hypoxic regions. These approaches may be highly effective in combination with chemotherapy or radiotherapy.
Hypoxia is also being targeted by developing novel therapeutic agents that only work in the absence of oxygen. Technologies are being advanced for visualisation of changes in tumour microenvironment which will allow response to therapy to be monitored. Tumour angiogenesis and metabolic changes that have come about as a result of hypoxia are being assessed in preclinical studies to provide new therapeutic avenues that will be evaluated in Phase 1 and Phase 2 clinical trials.
Tumour Microenvironment
Tum
ou
r Micro
enviro
nm
ent
Tumour Microenvironment

18 19For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
We aim to develop new radioisotope-labelled compounds for the imaging of tumour biology using nuclear medicine imaging techniques.
Molecular imaging using the nuclear medicine imaging techniques of single photon emission computed tomography (SPECT) and positron emission tomography (PET) allows the visualisation and quantification of biological processes in tumour tissue in living organisms. The main advantage of these non-invasive techniques is that they can be performed repeatedly in the same subject, and that the same imaging methods are used in the clinic, which makes them easier to translate from the laboratory to patients in the clinic. Because of their exceptional selectivity and sensitivity, we are mostly interested in the use of antibodies, proteins and peptides, labelled with radionuclides, to target very specific aspects of tumour biology.
Usually, molecular imaging targets are extracellular epitopes: cytokines, growth factors, or extracellular receptors. However, there is a mismatch between molecular imaging methods, which mostly target proteins or receptors on the outside of cancer cells, and cancer biology, where mostly intracellular events are studied. Therefore, one aim of the group is to develop novel methods to enable imaging of intracellular proteins, such as those involved in DNA damage repair signalling.
Furthermore, increased awareness and the rolling out of screening programmes have had a significant impact on cancer survival, especially breast cancer. The earlier a cancer is detected, the better the chances for survival are. Another aim of the group is therefore to develop methods that would allow early detection of tumour tissue.
We are evaluating the novel imaging agent developed in the group in models of breast and pancreatic cancer.
Ester Hammond
Ester Hammond is a CRUK Group Leader and Associate Professor at the CRUK/MRC Oxford Institute for Radiation Oncology. She completed her PhD at the School for Cancer Sciences, University of Birmingham then accepted a post as a postdoctoral fellow within the Molecular Oncology Group at the University of Cambridge School of Clinical Medicine. Subsequently, she moved to the USA to join the Department of Radiation Oncology at Stanford University, first as a postdoctoral fellow then a research associate. She joined the Oxford Institute in 2007 as a CRUK group leader. Ester was awarded the 2015 Michael Fry Research Award from the North American Radiation Research Society.
Radiopharmaceuticals and Molecular Imaging Group
Bart Cornelissen
Bart Cornelissen is a CRUK Career Development Fellow based at the CRUK/MRC Oxford Institute for Radiation Oncology and has headed the Radiopharmaceuticals and Molecular Imaging group since early 2013. He trained in analytical chemistry and radiochemistry at the Universities of Hasselt and Ghent, Belgium. He obtained his PhD in radiopharmaceutical sciences from the University of Ghent and spent several years at the University of Toronto as a postdoctoral fellow before joining the University of Oxford in 2007.
Tum
ou
r Micro
enviro
nm
ent
Tum
ou
r Micro
enviro
nm
ent
We are investigating how tumours survive in conditions which include hypoxia. Our goal is to target the hypoxic parts of tumours to improve cancer therapy. In order to progress beyond a certain size, tumours need to develop their own blood supply for nutrients and oxygen.
Although tumours are able to create their own blood supply this process is not perfect and so tumours have regions which do not receive enough oxygen. Hypoxia is the term used to describe any situation where there is insufficient oxygen. Most solid tumours have regions of hypoxia (Figure 1), which is significant because many studies have shown that the more hypoxic a tumour is, the worse the patient does. Importantly, this is independent of the therapy type the patient receives. Hypoxic tumours are resistant to both chemotherapy and radiotherapy as well as being more likely to spread and are therefore the most aggressive and hardest to treat. To improve the effectiveness of cancer therapy it is vital that we target the hypoxic part of tumours. Our group has three approaches to this problem:
1. We are investigating the biological response to hypoxia and in particular a pathway known as the DNA damage response. This pathway is active in hypoxic conditions despite a lack of detectable hypoxia-induced DNA damage. There are many drugs to target this pathway and it is possible that they will prove particularly useful in killing hypoxic cells when combined with standard therapies such as radiation.
2. We are developing novel drugs which only work in the absence of oxygen and so can be used to target the hypoxic areas of tumours. This approach allows us to use potentially toxic drugs as the normal cells in the body are unaffected.
3. Finally, it is vital that novel inhibitors/drugs are tested in conditions which mimic those found in tumours. Therefore, we test drugs in conditions which more closely resemble those found in tumours, including low oxygen, to determine if they are likely to be effective.
Tumour Hypoxia Group
Organic fluorescent dyes can be used as markers of hypoxia. These dyes can be synthesised to emit at various wavelengths of light, which is useful for obtaining greater levels of resolution when using multiple dyes in microscopy.
Figure 1: SPECT image of a very early breast cancer tumour (white circle), with changes in tight junction biology that can be imaged using 111In-labelled clostridium perfringens endotoxin fragments.
Genomic instabilities in the same tumour can be imaged using 89Zr-labelled antibodies, modified to enable nuclear localisation.
Figure 2: SPECT image highlighting halotag® expression using a radiolabelled halotag ligand in a tumour (white circle) tag ligand. This could be used as the basis of pretargeted imaging techniques.
Figure 1: Hypoxic regions occur in most of not all solid tumours. (A) HCT116 cells (human, colorectal) were grown as a tumour xenograft to an approximate diameter of 800 mm3. Prior to sacrifice animals were injected with 60 mg/kg pimonidazole. The hypoxic regions were then visualised by immunohistochemical staining of pimonidazole (brown). Nuclei were counterstained with hematoxylin. (B) An enlarged tumour region from (A) showing a hypoxic area and blood vessels (~ 70-200 μm). Necrotic regions were also identified beyond the hypoxic regions.

20 21For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
The focus of the group is on tumour angiogenesis and the role of notch signalling, and hypoxia biology and its regulation. The aim of our research is to develop ways to improve the treatment of breast cancer and other tumour types, by blocking the blood supply to tumours. Our special interest is in breast cancer and mechanisms of resistance to therapy, regulated by hypoxic metabolism and tumour angiogenesis, when tumours cannot grow without a new blood supply developing from pre-existing blood vessels.
Our research focuses on tumour angiogenesis and the role of notch signalling, and hypoxia biology and its regulation. New angiogenesis pathways involving notch signalling and G-coupled receptors have been discovered and therapeutic antibodies have been developed against them. We want to translate these basic discoveries into clinical relevance.
Hypoxia regulates many oncogenic pathways, as well as tumour angiogenesis, and it produces major metabolic changes. The latter may be responsible for resistance to endocrine therapy, chemotherapy and radiotherapy through different pathways. Our preclinical programme investigates several of these, and particularly those involved in lipid and glycogen metabolism. These provide new therapeutic avenues that will be assessed in Phase 1 and Phase 2 studies.
A major interest is in new angiogenic therapies, and developing ways to determine who will most benefit from these targeted therapies. Our work assesses the short-term effects on imaging with novel scanning agents, and biopsies for gene expression, then relates tumour response to longer term outcomes. In addition, metabolic profiling will be undertaken in patients to correlate the responses to new therapies with imaging changes and for individualisation of therapy.
Preclinical work has indicated combination therapy is significantly better and that the induction of hypoxia may induce a synthetic lethality approach, targeting the hypoxic pathways induced by antiangiogenic therapy. Many of these are also involved in the induction of tumour angiogenesis. The metformin study started because metabolic changes induced by Avastin® could be antagonised by metformin and combination therapy may therefore be a useful new modality. However, patients will respond differently to metformin based on the cancer cell biology and we want to try to identify those who show the clearest benefits and elucidate the pathways responsible.
Growth Factor Group
Gillies McKenna
Gillies McKenna, Professor of Radiation Oncology and Biology, has been Director of the CRUK/MRC Oxford Institute for Radiation Oncology since 2005 and Head of the Department of Oncology at the University of Oxford since 2010. Prior to that, he was Chairman and Henry K. Pancoast Associate Professor of Radiation Oncology at the University of Pennsylvania School of Medicine, rising to Professor in 1995. He has received several awards and honours including the Weiss Medal from the Association for Radiation Research, the Frank Ellis Medal from the Royal College of Radiologists, the Roentgen Medal from the Deutches Roentgen Museum and the Gold Medal from the Royal College of Radiologists.
Adrian Harris
Adrian Harris is the Cancer Research UK Professor of Medical Oncology in the Department of Oncology since 1988 and Professorial Fellow of St Hugh’s College, University of Oxford. He is a Consultant Medical Oncologist at the Oxford University Hospitals NHS Trust. He trained in Medicine and Biochemistry at Liverpool University and subsequently received his DPhil from the University of Oxford. He then trained at the Royal Marsden Hospital in Medical Oncology.
Tum
ou
r Micro
enviro
nm
ent
Tum
ou
r Micro
enviro
nm
ent
Spectrum of DCE-MRI response to Bevacizumab: We investigated 40 patients with breast cancer due to undergo neoadjuvant chemotherapy. They received 15mg/kg I.V. Bevacizumab (Avastin), 2 weeks before chemotherapy. This showed a spectrum of response on DCE-MRI within the 2 weeks. There were tumours where the ‘vascular rim’ markedly decreased without evidence of tumour cell death; those rarely with central necrosis and markedly decreased vessels; and finally those which grew straight through the therapy with an increase in rim perfusion.
Our research links basic science with clinical applications and focuses on understanding the mechanisms behind tumour resistance to radiation. The main goal of our research is sensitising cells to radiation by blocking mechanisms that control cell survival. Specifically we are interested in oncogenically activated signal transduction pathways that exert a radioprotective effect on tumour cells. The effectiveness of radiotherapy treatment could be significantly improved if tumour cells could be rendered more sensitive to ionising radiation without altering the sensitivity of normal tissues.
In the past, our research has shown that the EGFR-Ras-PI3K-PTEN-Akt pathway appears to be the major radioprotective pathway active in most solid tumours, and therefore this pathway presents targets that could be manipulated in a clinical setting to modify the radiation response. We have shown that a specialised DNA repair enzyme, DNA polymerase theta (POLQ), is overexpressed by tumour cells and that depletion of this enzyme makes cells more sensitive to radiation. Importantly, normal healthy cells do not appear to express POLQ and are therefore not affected by its inhibition. We also found that patients with high levels of POLQ expression have a worse prognosis. This would make POLQ an ideal therapeutic target for improving the effectiveness of radiotherapy without increasing normal tissue toxicity.
We are also interested in improving radiotherapy by reducing tumour hypoxia (low levels of oxygen in the tissue). One of the main reasons for the resistance of tumours to radiotherapy is the presence of large hypoxic regions that are significantly more resistant to radiation. One way of alleviating tumour hypoxia is to reduce the oxygen consumption of the fast growing cells at the tumour periphery so that more oxygen becomes available to the hypoxic regions. A high throughput screen conducted by our laboratory identified drugs that reduce oxygen consumption in tumour cells that could be used clinically to reduce tumour hypoxia.
Molecular Resistance to Treatments Group
Figure 1: High POLQ expression correlates with a poor prognosis. Univariate analysis of relapse-free survival in 152 breast cancer patients with POLQ expression divided in high and low expression groups by median value. From Higgins et al., 2010.
Figure 2: A drug identified by our laboratory that reduces hypoxia. The graph on the left shows the reduction in oxygen consumption following treatment with the drug in tumour cells grown as a monolayer. The panel on the right shows the reduction in the hypoxic core of tumour cells grown in spheroids, which mimic solid tumours. After 24 hours of treatment with this drug, the hypoxia in the centre of the spheroid is completely abolished.

22 23For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
Eric O’Neill
Eric O’Neill is a CRUK Group Leader and Associate Professor at the CRUK/MRC Oxford Institute for Radiation Oncology. After completing a PhD at the University of Umeå, Sweden he was a post-doc at the University of Oxford. Subsequently, he was awarded a Marie Curie research fellowship and completed a 5-year postdoctoral position investigating oncogenic and tumour suppressor signalling at the CRUK Beatson Institute for Cancer Research in Glasgow. He is a member of the Association for Radiation Research and an examiner for the Royal College of Radiologists. He has also been on the organising committee for several international conferences.
Ruth Muschel
Ruth Muschel has been Deputy Director of the CRUK/MRC Oxford Institute for Radiation Oncology and Professor of Molecular Pathology at the University of Oxford since 2005. She obtained MD and PhD degrees at Albert Einstein College of Medicine, New York City and completed her specialty training in anatomic pathology at Columbia University and the National Cancer Institute in Bethesda. She continued on staff at the NCI before taking an academic position at the University of Pennsylvania, where she advanced to the rank of Professor.
Tum
ou
r Micro
enviro
nm
ent
Tum
ou
r Micro
enviro
nm
ent
We are interested in the mechanisms underlying the development of metastasis, the spread of cancer from one part of the body to another. Our research focuses on the interaction of cancer cells with the host vasculature and the circulating blood cells. The interactions between tumour cells and the host vasculature are important in the initiation of metastases (secondary cancer) as well as allowing metastatic colony growth later in metastatic progression. Our work has indicated the importance of coagulation and platelets in recruiting myeloid cells to allow the earliest formation of metastatic colonies. Later in metastasis, recruitment of myeloid cells is also essential for colony growth and the formation of blood vessels in the colonies. We are asking how these myeloid cells enable metastatic progression. This work is beginning to identify targets both for detection and for treatment of metastatic lesions.
Tumour vascularity is essential for the response of cancers to radiation therapy. During therapy, hypoxia (low oxygen) is highly detrimental to effective radiation therapy. Hypoxia is of course determined by tumour vascularity and oxygen consumption. We have begun to develop strategies to reduce hypoxia during radiation by identifying agents that lead to better blood vessel formation, also called vascular normalisation, and strategies to reduce tumoural oxygen consumption. These strategies would be expected to generate tumours that are less hypoxic and more responsive to radiation therapy. Clinical trials are underway based on this work.
The final outcome of radiation therapy is also affected by tumour regrowth at the end of therapy. We have shown that inhibition of vascular regrowth leads to enhanced efficacy of radiation therapy. We are currently exploring the mechanisms that tumours treated with radiation use to stimulate vascular growth and the means to interfere with this growth.
Mechanisms of Metastasis Group
Figure 1: Tumour cell (green) metastatic to the lung endothelium (red) surrounded by platelets (blue).
Figure 2: Tumour cell (blue) clot (red) formation, triggered by expression of Tissue Factor, promotes the recruitment of a population of monocytes/macrophages (green) that enhance tumour cell survival. This is a phenomenon that occurs at the very early stages of metastasis and it is also observed during the formation of premetastatic niches.
We aim to understand the cell and molecular biology behind frequent tumour mutations and how they influence cancer onset and therapy. For cancers to develop, cells must acquire mutations and epigenetic alterations that prevent the normal control of proliferation and survival. While there are multiple signalling pathways that could be targeted for mutation, there are key genes that are recurrently altered in tumours. Our research focuses on the most frequent and clinically relevant events to understand how alteration of signalling pathways contributes to disease onset and affects treatment outcomes.
RAS is a family of proteins expressed in all cells. Our work focuses on how oncogenic RAS activation combines with tumour suppressor events such as loss of p53 function to allow tumour growth and invasion. By understanding these common events we aim to better define patients' cohorts and provide a scientific rationale for personalised medicine approaches. In particular, we have been exploring this within a multidisciplinary team tackling pancreatic cancer.
Our lab has focused on the RAS effector RASSF1, which is significantly inactivated by CpG island methylation in all major solid tumours. Epigenetic silencing of the RASSF1 promoter not only associates with tumour onset but also affects prognosis and is being adopted as a potential predictive biomarker for treatment in certain cancers.
We have concentrated on uncovering the role for RASSFs in normal biology to understand exactly why loss of expression has such widespread association with cancer initiation. Through this approach we have found that RASSF1A plays a key role in governing control of the hippo stem cell pathway and is important for genomic protection via the familial breast cancer tumour suppressor gene, BRCA2.
We are continuing to look at both these aspects with the intention of highlighting intervention strategies that are biologically relevant to patients with RASSF1 methylation, alongside developing plasma-based detection methods for this epigenetic event. We are collaborating with projects in lung, breast and colorectal susceptibility where RASSF1A methylation has a poor prognosis and are working together with clinicians and developmental biologists on the role of defective stem cell regulation in the onset of gliomas.
Cell Signalling Group
Figure 1: A. Oligomeric NPM and AKT phosphorylation site pS48. B. Blocking AKT phosphorylation of NPM promotes p14ARF localisation at the nucleolus and reduced p53 levels.
Figure 2: Loss of RASSF1 expression correlates with loss of the YAP partner and differentiation factor, RUNX2 in colorectal adenocarincomas. Normalised expression levels with red = upregulation and blue = downregulation.
p14ARFDAPI
DMSO
AKTi
A. B.

24 25For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
Len Seymour
Leonard Seymour is Professor of Gene Therapies in the Department of Oncology. He was the Founding President of the British Society for Gene and Cell Therapy, is the Secretary and Trustee of the European Society of Gene and Cell Therapy and an Executive Council Member of the International Society for Cell and Gene Therapy of Cancer. He is Chair of the Scientific Advisory Board of the Chronic Granulomatous Disorder Research Trust, and also chairs the Scientific Advisory Board of the Muscular Dystrophy Consortium. Len is Course Director of the part-time MSc in Experimental Therapeutics offered by the Department of Oncology in conjunction with the Department for Continuing Education.
Anderson Ryan
Anderson Ryan is an MRC Group Leader at the CRUK/MRC Oxford Institute for Radiation Oncology. Prior to coming to Oxford in 2010, he was a Principal Scientist in the Cancer Discovery Department at AstraZeneca based at Alderley Park in Cheshire and before that a University Lecturer at the University of Manchester based at the CRUK Paterson Institute for Cancer Research. He undertook postdoctoral research first at the University of Durham and then at the University of Cambridge. He is a member of several professional organisations including the American Association for Cancer Research and the American Association for the Advancement of Science and the Genetics Society.
Tum
ou
r Micro
enviro
nm
ent
Tum
ou
r Micro
enviro
nm
ent
A.
Our group aims to identify novel therapies that target subgroups of lung cancer patients harbouring specific genetic changes. Our research focuses on lung cancer where our primary aim is to identify new drug targets and to determine how best to integrate novel therapies with current standards of care in lung cancer, and to optimise combination treatments including radiation therapy.
During its development, lung cancer acquires activating mutations that are critical for continued tumour growth. For example, recurrent mutations have been described in several key oncogenes (including EGFR, KRAS, ALK, BRAF, PIK3CA and ERBB2). Since these activating mutations are not found in normal tissues, we are currently screening for combinations of novel compounds that can selectively kill these cells while leaving normal
cells unaffected. Importantly, lung cancer can also acquire loss of function mutations in tumour suppressor genes. As a consequence, tumour cells can become highly dependent on compensatory signalling pathways, which might then be targeted in order to kill the tumour cells. In contrast, non-tumour cells without the tumour suppressor gene mutation, are less dependent on these compensatory pathways and therefore are relatively unaffected by pathway inhibition. We are currently screening for targets and compounds that can lead to selective killing of cells with tumour suppressor gene mutations that are common in lung cancer (e.g. TP53, LKB1, ATM).
To study drug effects we also need to be aware of potential effects on normal tissues. In the case of radiotherapy for lung cancer, debilitating scarring known as fibrosis can occur throughout the lung several months after treatment. So in addition to seeking therapies to improve the effectiveness of radiation, we are also examining the impact on lung function using advanced imaging and histological techniques.
Translating findings from the laboratory to the clinic is an ongoing challenge in cancer research. So, in addition to standard cell lines, we are also working with samples derived directly from lung cancer patients so that we may be able to better predict responses in the clinic.
Lung Cancer Research Group
A. Chemically-induced lung adenoma. B. Lung cancer cell proliferation (mitosis) measured by phospho-histone H3 immuno-histochemical staining (DAB, brown). C. Radiation-induced lung fibrosis (Masson’s trichrome, blue=collagen). D. Radiation-induced DNA damage in epithelial cell of lung measured by γ-histone H2AX staining (DAB, brown foci).
Immunofluorescence images of lung cancer cell lines treated with an inhibitor of ATR kinase and showing signs of DNA replication stress (γH2AX) and DNA double strand breaks (53BP1).
Our research aims to design and develop innovative cancer-killing viruses and oncolytic vaccines. Our research develops anticancer ‘oncolytic’ viruses that are able to infect and kill cancer cells, while leaving normal cells unharmed. This approach exploits the natural life cycle of the virus, which lyses infected cells and releases progeny virus particles, allowing the infection to spread from cell to cell through the tumour. In this way the virus amplifies itself locally, reaching higher concentrations within the tumour than in the bloodstream during delivery – a very unusual feat for an anticancer drug.
Virus replication maximises therapeutic anticancer activity and simultaneously minimises unwanted systemic side effects. This represents the ultimate ‘magic bullet’, combining selectivity of action with a big amplification of activity at the tumour site.
The life cycle of some viruses, such as adenoviruses, is intimately dependent on the activities of the cells they infect, and this provides a range of opportunities to engineer oncolytic viruses that are only active when they encounter the specific cellular environment of a tumour cell. For example, adenoviruses can be designed that are dependent on deregulated cell cycle, dysfunctional apoptosis pathways, enhanced glycolytic metabolism and many others. In addition, this 'oncolytic' type of cell killing is very inflammatory, providing the possibility to create an anticancer immune response. These agents are often known as ‘oncolytic vaccines’.
To allow therapeutic use in treating advanced (metastatic) cancer, we give special attention to developing viruses that can be administered intravenously to patients. To achieve this it is important that the virus can survive the challenging environment of the human blood circulation, and also that virus particles are not cleared too quickly from the circulation, before they have a chance to access tumour deposits.
Finally, our viruses can be 'armed' to encode additional therapeutic agents, to be expressed only within the tumour and secreted from infected tumour cells into the microenvironment. In this way we can achieve targeted expression of therapeutic biologics such as cytokines, antibodies and enzymes, to augment the activity of the virus itself. This provides a simple and versatile approach to targeted cancer therapy, allowing the power of biological agents to be applied locally within tumours and avoiding unwanted toxicities.
Anticancer Viruses and Cancer Vaccines Group

26 27For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
Nicola Sibson
Nicola Sibson is Professor of Imaging Neuroscience, CRUK Group Leader and Director of Graduate Studies at the CRUK/MRC Oxford Institute for Radiation Oncology. On completion of her PhD at the University of Cambridge, Nicola spent four years at Yale University, before joining the MRC Biochemical and Clinical Magnetic Resonance Unit in Oxford. Subsequently, she moved to the Department of Physiology, Anatomy and Genetics as a University Research Lecturer, and was recruited to the Institute in 2007. Nicola has given numerous plenary lectures at national and international meetings, including the prestigious British Neuropathological Society Lecture, at the Neuro-Oncology Society Annual Conference, and serves on many funding panels and advisory boards. Nicola was recently made a Special Supernumerary Fellow of University College Oxford.
Tum
ou
r Micro
enviro
nm
ent
Our goals are to identify the role of the inflammatory and metabolic microenvironment in brain metastasis, and to develop imaging biomarkers for tumour detection and monitoring. Metastasis (secondary cancer) to the brain is a significant clinical problem and prognosis is extremely poor. The incidence of brain metastasis is increasing as patients survive longer, and even radiosurgery/radiotherapy has limited impact on prognosis.
We have identified three critical hurdles to effective treatment of brain metastases: (1) late stage of diagnosis; (2) poor access to the brain (bioavailability) of therapies that are successful in peripheral tumours; and (3) impact of microenvironmental factors on the effectiveness of treatment. By improving our understanding of the microenvironment of brain metastases, we believe that we will not only identify new therapeutic targets, but also drive the development of diagnostic imaging tools for use in patients.
Earlier detection of brain metastases is likely to yield substantial gains both for current therapies and the development of new metastasis-inhibiting agents. To this end, we have demonstrated that it is possible to detect brain metastases at a much earlier stage than current clinical methods allow, through the use of new molecularly-targeted imaging agents (Fig. 1).
In collaboration with others in the University, we developed and patented biodegradable microparticles of iron oxide (MPIO) as a platform for translating this technology to man. Together, this work has formed the basis of two successful applications to the MRC Developmental Pathways Funding Scheme to progress this agent to a Phase I/IIa clinical trial.
With regards to bioavailability, a significant hurdle is the presence of the blood-brain barrier (BBB). We have recently shown that it is possible to make the BBB selectively leaky at sites of brain metastasis, and that this approach enables metastasis-targeted delivery of both diagnostic agents and relevant therapies (Fig. 2).
The above ongoing studies feed into our overall research programme, in which our primary aims are to (1) determine the role of inflammatory processes in brain metastasis development and response to radiotherapy, and (2) develop novel approaches to imaging the tumour microenvironment for early diagnosis and treatment monitoring.
Experimental Neuroimaging Group
Figure 1(A): Confocal microscopy images showing co-localisation of the cellular adhesion molecule VCAM-1 (red) on vessels associated with a micrometastasis (green) in mouse brain. Cell nuclei stained blue. (B): MRI detection of VCAM-1 expression on brain blood vessels using VCAM-1-targeted MPIO in a mouse model of brain metastasis; 3D reconstruction showing spatial distribution of VCAM-MPIO binding (in red) indicating sites of metastases throughout the brain.
A B
Figure 2: SPECT image showing accumulation of radiolabelled Trastuzumab at the site of a micrometastatic colony in mouse brain
following selective permeabilisation of the metastasis-associated vasculature.

28 29For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
A key aim of the Department of Oncology is the optimal translation of fundamental research into patient benefit. Precision cancer medicine brings together the concepts of biological selection of therapy with targeting of treatment to deliver the best possible outcomes for a patient with cancer. Clinical research builds on the themes of DNA damage and repair and the tumour microenvironment and encompasses genomics, biomarkers, imaging and clinical trials. Computational biology, which sits at the interface of all these, generates essential knowledge in the pathway to providing cutting-edge clinical treatment for cancer patients.
Biomarkers and personalised medicine
Patients are individuals – made unique by their signature genes and proteins. In the same way, cancers have specific characteristics. Even within one type of cancer, not all patients will respond to the same treatment in the same way and response to therapy is influenced both by the individual patient and the cancer’s characteristics. In order
to select the right treatment for the right patient at the right time, we need to identify biological factors or biomarkers that can predict how an individual patient will respond to a particular drug or radiotherapy regime. The treatment can then be tailored to achieve the best outcome for each patient.
Researchers in Oxford are using existing, and developing new, biomarkers to select patients for therapy in both early and late phase clinical trials. Specific biomarkers are used to group patients into subtypes of a cancer, which can be used to guide participation in appropriate clinical trials. This may be with a new agent that promises benefit for the patient’s particular subtype of cancer.
Advancing imaging technologies in patient treatment
Imaging techniques play a central role in cancer research and treatment. Imaging is often the first means of detecting a tumour and is used to provide accurate information about the location and extent of the tumour (anatomical imaging) and the cancer’s behaviour (functional imaging). Imaging is used, therefore, to guide treatment decisions, to drive the anatomical precision of treatment for surgery and radiotherapy, and to monitor response to treatment – detecting tumour shrinkage or growth (progression).
A variety of sophisticated imaging and imaging analysis techniques, including MRI, PET and SPECT-based methods, are being developed, refined and enhanced through Oxford research programmes. Huge advances in fluorescence optical image guidance for use during human surgery have been made by researchers in the CRUK/MRC Oxford Institute for Radiation Oncology.
Researchers are also developing advances in techniques of radiotherapy planning coupled with advanced tumour imaging to deliver the radiation more precisely to predetermined volumes within the tumour. This reduces side effects and improves the outcome for the patient.
The Department is fortunate to be home to the CRUK & EPSRC Cancer Imaging Centre in Oxford. Since 2008, this highly successful initiative has nurtured multidisciplinary collaborations with the common goal of improving imaging and image analysis and has provided a focus for translational work.
Clinical trials
The Department’s clinical research programmes initiate and develop high quality clinical trials to test hypotheses emerging from the basic science research groups. The aim is to improve the effectiveness of radiotherapy and chemotherapy in the treatment of cancer.
Clinical activities are underpinned by the Department’s Oncology Clinical Trials Office (OCTO) and the Early Phase Clinical Trials Unit (EPCTU), which together, provide the necessary infrastructure and expertise to set up and run studies in Oxford and throughout Europe.
Clinical and Translational Research
Clinical and Translational Research
Clin
ical and
Translatio
nal R
esearch

30 31For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
We focus on the fundamental genetics and biology of colorectal cancer and the characterisation and distribution of genetic diversity in human populations. The fundamental genetics and biology of colorectal cancer (CRC) and their potential applications
We use a panel of over 100 colorectal cancer (CRC) cell lines to study the basic biology of colorectal cancer as well as the effects that new treatments have on the cancer cells. The cell lines have been extensively characterised for genetic mutations, expression profiles and growth characteristics. The use of this number of cell lines allows the identification of subsets of cancers that behave similarly with respect to their biology, drug responses and growth characteristics. This, in turn, allows us to identify the molecularly-defined profiles that correlate with, and can ultimately be used to predict for, those responses. Cancer stem cells can be isolated from within individual cell lines and we are also trying to identify the genes that control stemness and cellular differentiation in CRCs.
Recently, we have developed a protocol that allows efficient establishment of medium to long-term primary cultures from fresh CRC tumour material. These are now being compared with the cell lines, both with respect to their biological properties and their drug responses.
The characterisation and population distribution of genetic diversity in human populations, especially of the British Isles
We have collected DNA samples from people in rural areas of the UK whose grandparents all come from within a small geographic radius. This is to reduce the effects of
interbreeding between diverse populations, which has the effect of removing ancient regional differences. This serves as a very effective set of healthy controls for genetic studies into the causes of common diseases such as diabetes, psoriasis and schizophrenia. We have analysed Single Nucleotide Polymorphism data from our samples and shown a strong connection between geography and genetic variation. The genetics of normal differences, particularly facial features, are also being investigated; to this end, we are assembling a database of 3D photographs from volunteers whose genotype data we also have.
Cancer and Immunogenetics Laboratory
Walter Bodmer
In 1996, Sir Walter Bodmer assumed his current position at the Weatherall Institute of Molecular Medicine as Head of the Cancer and Immunogenetics Laboratory and more recently within the Department of Oncology. After obtaining a PhD in Genetics from Cambridge University, he moved to Stanford University in California where he rose to the position of Professor. In 1970, he returned to the UK as the first Professor of Genetics at Oxford University. He subsequently became the Director of Research, and finally the Director General, of the Imperial Cancer Research Fund in London. He is a Fellow of the Royal Society and was knighted in 1986.
Clin
ical and
Translatio
nal R
esearch
Clin
ical and
Translatio
nal R
esearch
A genetic map of the UK. Each symbol is the place where a sample comes from. Individuals who belong to a genetically similar group are distinguished by colour.
Cancer cells grown in 3D can sometimes still form highly organised structures. The central yellow ring of staining identifies the inner luminal surface of this polarised colony of colorectal cancer cells.
We investigate post-transcriptional mechanisms that drive cancer behaviour and research novel cancer therapeutics for patients with advanced malignancies.
mRNA Dysregulation in Cancer Gene expression describes the conversion of genetic message to protein. This depends on messenger RNA (mRNA) which copies the gene sequence, shuttles into the cytoplasm, binds ribosomes and generates protein. Numerous RNA binding proteins (RBPs) attach to these mRNA transcripts and regulate their splicing, stability, subcellular localisation and rate of translation.
In cancer cells, expression of RBPs is disrupted, driving the malignant state by preserving the stability of proto-oncogenic mRNAs while destabilising those with tumour suppressor functions. One such RBP is La-related protein 1 (LARP1). We have shown that LARP1 is capable of selectively binding transcripts involved in cancer processes and is present at high levels in some epithelial cancers. The net effect of LARP1 upregulation is to drive cancer progression.
The purpose of our research is to discover more about cancer RBPs and develop therapeutics against them that can be used as anticancer treatments.
Cancer TherapeuticsA crucial part of cancer drug discovery is finding the best cancer treatments for the future. In leading the Early Phase Clinical Trials Unit, Sarah's team investigates new treatments for
patients with cancer. Potential treatments are carefully chosen on their scientific rationale, their likelihood of being effective and, most importantly, their safety profile.
The Oxford Early Phase Clinical Trials Unit has a long established track record of drug discovery and delivering novel therapies safely and effectively. Sarah has a strong science and medical background which enables her to design clinical trials, investigate treatments (developed by academia or industry) and deliver them to cancer patients.
Cancer Therapeutics and mRNA Dysregulation
Sarah Blagden
Sarah Blagden has been Associate Professor of Experimental Cancer Therapeutics in the Department of Oncology since 2015. Following medical training and subsequent specialist training in Medical Oncology at Addenbrooke’s Hospital in Cambridge and the Royal Marsden Hospital, she was awarded a CRUK Junior Clinician Scientist PhD fellowship in 1999 at Cambridge University and held a Clinical Fellowship at the Institute of Cancer Research’s Drug Development Unit. She was appointed as Senior Lecturer and Honorary Consultant at Imperial College in 2006 and became Director of Imperial’s Early Cancer Trials Unit and established her laboratory studying the dysregulation of mRNA translation in cancer. She has been chief or principal investigator for a number of national and international clinical studies.
LARP1 (green) highly expressed in the cytoplasm of a cancer cell. LARP1 is associated with almost 3000 mRNAs predominantly those encoding cancer signalling proteins
LARP1 (stained green here) relocates to cytoplasmic stress granules following exposure to cell stress in ovarian cancer cells

32 33For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
We search for integrated genomic blueprints that enable us to predict how cancer will evolve and respond to treatment. High throughput technology has supported a scientific revolution both in molecular biology and clinical research. In molecular biology, and more specifically in both cancer and radiation biology, it is now possible to acquire data at the whole genome level, and to characterise a genomic blueprint for different cancer types. This has allowed us to ask questions on how the cancer genome is regulated. Most importantly, we are beginning to understand how and where the blueprint of the genome is functional and what the biological and clinical implications of this function are.
In translational and clinical research it is becoming increasingly possible to acquire both genomic and disease imaging data, and this combination can provide further understanding of the molecular and clinical cancer phenotype. This revolution has enabled the accumulation of cancer genomic big data and related knowledge at a speed never experienced before in science. The knowledge generated with this big data is being increasingly organised in both specialist and general knowledge databases which can be interrogated by computational tools.
We are investigating integrative approaches to combine results from functional assays, systems level approaches and clinical knowledge with genomics (DNA) and transcriptomic (RNA) data. To achieve this we apply a wide range of sophisticated computational and statistical techniques to analyse large clinical cohorts. Our research sits at the interface between genomics, imaging and biomarkers and it is applied to molecular and radiation oncology.
Our more recent work focuses on next generation sequencing techniques and high content screening, and the development of tools to aid the translation of this big data generated knowledge into beneficial use in the clinic for treatment of patients.
Computational Biology and Integrative Genomics
Francesca Buffa
Francesca Buffa is an Associate Professor and has been a Career Development Fellow, University of Oxford Research Lecturer and the head of the Computational Biology and Integrative Genomics Group at the CRUK/MRC Oxford Institute for Radiation Oncology since 2013. After postdoctoral research in statistical methods for predictive biomarkers at the Gray Cancer Institute (London), she joined the Weatherall institute of Molecular Medicine, University of Oxford, as a Senior Bioinformatics/Biostatistics Fellow, developing machine learning approaches for systems biology and biomarker discovery. She also provides biostatistics and bioinformatics expertise for genomics and clinical research.
Clin
ical and
Translatio
nal R
esearch
Clin
ical and
Translatio
nal R
esearch
We develop image analysis methods for quantitative analysis of medical images, specifically for a range of applications in cancer. Image analysis based on MRI, CT, PET, SPECT, ultrasound, and various forms of microscopy, is firmly established as a basis for detection and diagnosis of disease and for illustrating aspects of the fundamental science basis of cancer. In practice, much of image analysis is qualitative in that it relies upon the judgement of experts to interpret the images.
We aim to develop precise measurements from images, enabling us to: monitor the progression of disease; measure the response to therapy; and to estimate physical aspects of tumours, such as their size and density. Some of many examples of our work include: measuring from a mammogram the amount and distribution of dense tissue in the breasts of post-menopausal women (currently regarded as one of the main risk factors for breast cancer); identifying complete responders to neoadjuvant chemo/radiotherapy in colorectal cancer (potentially avoiding major surgery); and classifying liver textures, such as those characteristic of a range of liver diseases.
Figure 1 illustrates some of our quantitative analysis of breast density estimated from a single mammogram. Note that the volumes of fibroglandular tissue is expressed in cm3 while the x-ray dose estimated as a result of this particular mammogram is 2.8 mGy. Our work forms the basis of the products of VolparaSolutions, a company we founded in 2008 based on science we did in Oxford starting in 1993.
These applications rely upon, and motivate the development of, advances in image analysis techniques: image segmentation; feature extraction; deformable image registration; atlas development; and tumour modelling. Figure 2 shows the vasculature computed automatically for one slice of an MRI volume of the liver. This is used subsequently to detect and stage liver disease.
Oncological Image Analysis
Michael Brady
Sir Michael Brady was appointed as Professor of Oncological Imaging in the Department of Oncology, having retired from his 25-year Professorship in Information Engineering in 2010. After obtaining degrees in mathematics, he worked in computing science, artificial intelligence, and engineering. He founded the Oxford University Robotics Group, but switched his interests to cancer image analysis in the early 1990s. Apart from his Oxford research, Mike has founded a number of companies, including Matakina and ScreenPoint (mammographic image analysis), Mirada Medical (medical image fusion), and Perspectum Diagnostics (liver MRI). He is a member of CRUK’s Science Committee and chairs the Multidisciplinary Expert Review Panel and the Royal Society Publications Board. He is a Fellow of the Royal Society.
Figure 1: (Left) A mammogram; at point a, we estimate 3.6cm fat, 2.4cm of dense tissue; at point b, 5.8cm of fat; 0.2cm of dense tissue. (Right) quantitative measurement of the amount of dense tissue in the breast.
Figure 2.
The graph shows the interplay between genes regulated by hypoxia in a cancer cell. Genes are shown as circles, while their relationship with co-partners genes which help fuel progression of cancer is shown by green edges. The network demonstrates complex interplay which emerges when the cancer cell undergoes hypoxia following poor blood supply, and patients with such deregulation are shown to have a poorer outcome. A computational algorithm previously developed by us (Buffa et al.) was used, which aims at unravelling such interplays by starting with known key player genes in cancer (seeds). It extends the network by finding other genes in human genome (>25,000) exhibiting similar patterns of expression, and further limiting to those genes having the highest number of associates/co-partners. This way, a highly active network is identified which is shown to contain primary culprits of driving aggressive cancers.
SDC1
HIG2
LOC402538
PSRC1
FAS
SLC35E2
CNIH4
SLC6A8
FLJ43855
CDCA4
VEGF
HK2
EGLN3HPRT1
PPKFB4KIF4A
SIVA
P4HA1
MIF
MRPS17PLCL2
ARHGEF6
KOTD12
VDAC1
CUGBP2
IPPK
FBLN5
LOC91316
ANXA2P3
FAHD1
RCOR1
EXOC5
STAMBPL1
LOC81558
NDRG1
TACC1
PGAM1
BNC1
ICAM2
GYPC
PHLDB2
CSNK1E
ADM
GPI
PPM1J
RPL39L
TBRG1
ZDHHC9
PPARD
PGRALK3 C18orf1
PGK1
ALDOASLC2A1PPP4R1
CA12 LOCCAV2
FER BICD2RAE1 MTP18C6orf143GNAI1
KCTD11
BNIP3C20orf20ENO1
POLE2LDHA
TPI1
CDC20
TPBGPLEK2
UEV3
TGFA
CINP
RHOD
PTGFRN
SLC16A1
MRPL28
CA9
P18SRP
NIFUNCTSL2TNS4PYGL
ELP2
CDH3DCBLD1S100A3
ANKRD9
RRAS2
GPR109B
MAD2L2
WDHD1
CDKN3
DLG7
PEX14
UBE2C
AURKA
C1orf144
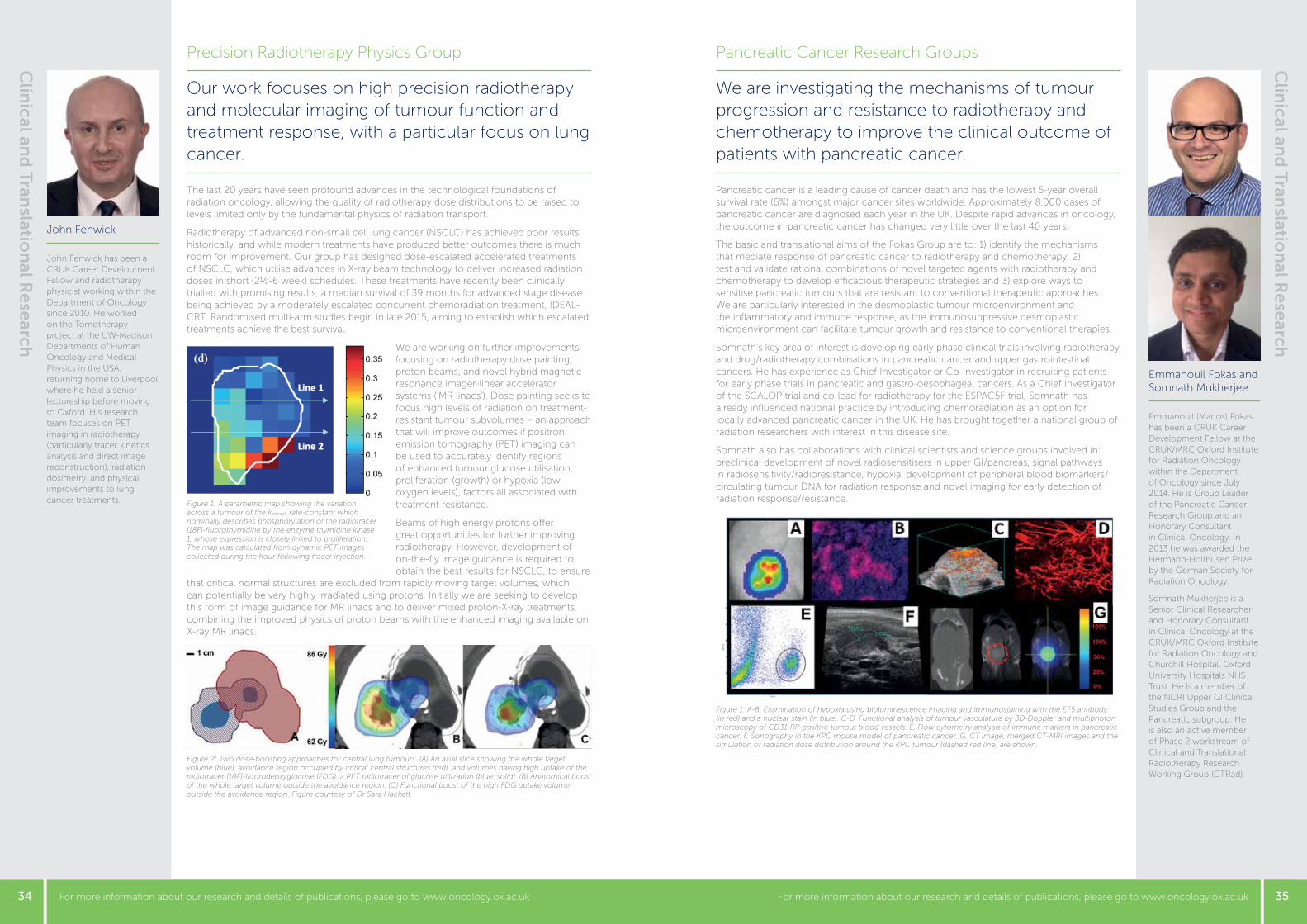
34 35For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
Our work focuses on high precision radiotherapy and molecular imaging of tumour function and treatment response, with a particular focus on lung cancer. The last 20 years have seen profound advances in the technological foundations of radiation oncology, allowing the quality of radiotherapy dose distributions to be raised to levels limited only by the fundamental physics of radiation transport.
Radiotherapy of advanced non-small cell lung cancer (NSCLC) has achieved poor results historically, and while modern treatments have produced better outcomes there is much room for improvement. Our group has designed dose-escalated accelerated treatments of NSCLC, which utilise advances in X-ray beam technology to deliver increased radiation doses in short (2½-6 week) schedules. These treatments have recently been clinically trialled with promising results, a median survival of 39 months for advanced stage disease being achieved by a moderately escalated concurrent chemoradiation treatment, IDEAL-CRT. Randomised multi-arm studies begin in late 2015, aiming to establish which escalated treatments achieve the best survival.
We are working on further improvements, focusing on radiotherapy dose painting, proton beams, and novel hybrid magnetic resonance imager-linear accelerator systems (‘MR linacs’). Dose painting seeks to focus high levels of radiation on treatment-resistant tumour subvolumes – an approach that will improve outcomes if positron emission tomography (PET) imaging can be used to accurately identify regions of enhanced tumour glucose utilisation, proliferation (growth) or hypoxia (low oxygen levels), factors all associated with treatment resistance.
Beams of high energy protons offer great opportunities for further improving radiotherapy. However, development of on-the-fly image guidance is required to obtain the best results for NSCLC, to ensure
that critical normal structures are excluded from rapidly moving target volumes, which can potentially be very highly irradiated using protons. Initially we are seeking to develop this form of image guidance for MR linacs and to deliver mixed proton-X-ray treatments, combining the improved physics of proton beams with the enhanced imaging available on X-ray MR linacs.
Emmanouil Fokas and Somnath Mukherjee
Emmanouil (Manos) Fokas has been a CRUK Career Development Fellow at the CRUK/MRC Oxford Institute for Radiation Oncology within the Department of Oncology since July 2014. He is Group Leader of the Pancreatic Cancer Research Group and an Honorary Consultant in Clinical Oncology. In 2013 he was awarded the Hermann-Holthusen Prize by the German Society for Radiation Oncology.
Somnath Mukherjee is a Senior Clinical Researcher and Honorary Consultant in Clinical Oncology at the CRUK/MRC Oxford Institute for Radiation Oncology and Churchill Hospital, Oxford University Hospitals NHS Trust. He is a member of the NCRI Upper GI Clinical Studies Group and the Pancreatic subgroup. He is also an active member of Phase 2 workstream of Clinical and Translational Radiotherapy Research Working Group (CTRad).
Precision Radiotherapy Physics Group
John Fenwick
John Fenwick has been a CRUK Career Development Fellow and radiotherapy physicist working within the Department of Oncology since 2010. He worked on the Tomotherapy project at the UW-Madison Departments of Human Oncology and Medical Physics in the USA, returning home to Liverpool where he held a senior lectureship before moving to Oxford. His research team focuses on PET imaging in radiotherapy (particularly tracer kinetics analysis and direct image reconstruction), radiation dosimetry, and physical improvements to lung cancer treatments.
Clin
ical and
Translatio
nal R
esearch
Clin
ical and
Translatio
nal R
esearch
Figure 1: A parametric map showing the variation across a tumour of the kphosph rate-constant which nominally describes phosphorylation of the radiotracer [18F]-fluorothymidine by the enzyme thymidine kinase 1, whose expression is closely linked to proliferation. The map was calculated from dynamic PET images collected during the hour following tracer injection.
Figure 2: Two dose-boosting approaches for central lung tumours. (A) An axial slice showing the whole target volume (blue), avoidance region occupied by critical central structures (red), and volumes having high uptake of the radiotracer [18F]-fluorodeoxyglucose (FDG), a PET radiotracer of glucose utilization (blue, solid). (B) Anatomical boost of the whole target volume outside the avoidance region. (C) Functional boost of the high FDG uptake volume outside the avoidance region. Figure courtesy of Dr Sara Hackett.
We are investigating the mechanisms of tumour progression and resistance to radiotherapy and chemotherapy to improve the clinical outcome of patients with pancreatic cancer. Pancreatic cancer is a leading cause of cancer death and has the lowest 5-year overall survival rate (6%) amongst major cancer sites worldwide. Approximately 8,000 cases of pancreatic cancer are diagnosed each year in the UK. Despite rapid advances in oncology, the outcome in pancreatic cancer has changed very little over the last 40 years.
The basic and translational aims of the Fokas Group are to: 1) identify the mechanisms that mediate response of pancreatic cancer to radiotherapy and chemotherapy; 2) test and validate rational combinations of novel targeted agents with radiotherapy and chemotherapy to develop efficacious therapeutic strategies and 3) explore ways to sensitise pancreatic tumours that are resistant to conventional therapeutic approaches. We are particularly interested in the desmoplastic tumour microenvironment and the inflammatory and immune response, as the immunosuppressive desmoplastic microenvironment can facilitate tumour growth and resistance to conventional therapies.
Somnath’s key area of interest is developing early phase clinical trials involving radiotherapy and drug/radiotherapy combinations in pancreatic cancer and upper gastrointestinal cancers. He has experience as Chief Investigator or Co-Investigator in recruiting patients for early phase trials in pancreatic and gastro-oesophageal cancers. As a Chief Investigator of the SCALOP trial and co-lead for radiotherapy for the ESPAC5F trial, Somnath has already influenced national practice by introducing chemoradiation as an option for locally advanced pancreatic cancer in the UK. He has brought together a national group of radiation researchers with interest in this disease site.
Somnath also has collaborations with clinical scientists and science groups involved in: preclinical development of novel radiosensitisers in upper GI/pancreas, signal pathways in radiosensitivity/radioresistance, hypoxia, development of peripheral blood biomarkers/circulating tumour DNA for radiation response and novel imaging for early detection of radiation response/resistance.
Pancreatic Cancer Research Groups
Figure 1: A-B, Examination of hypoxia using bioluminescence imaging and immunostaining with the EF5 antibody (in red) and a nuclear stain (in blue). C-D, Functional analysis of tumour vasculature by 3D-Doppler and multiphoton microscopy of CD31-RP-positive tumour blood vessels. E, Flow cytometry analysis of immune markers in pancreatic cancer. F, Sonography in the KPC mouse model of pancreatic cancer. G, CT image, merged CT-MRI images and the simulation of radiation dose distribution around the KPC tumour (dashed red line) are shown.

36 37For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
Personalising gastrointestinal cancers radiotherapy: the ultimate aim of the research of my group is to maximise clinical benefit in terms of better tumour control and reduction in toxicity after radiotherapy to enhance life expectancy of the patient. Despite several advances in techniques of radiotherapy planning (intensity modulated radiotherapy), tumour imaging (PET, MRI); radiation delivery (rotational arc therapy) the techniques and doses used for radiotherapy treatments of gastrointestinal malignancies cancers have remained unchanged. Chemoradiation remains the main treatment for inoperable patients and the outcomes in tumours such as oesophagus or pancreas have not improved over the last decades. The causes of local failure are due to several aspects: inadequate radiation dose, low oxygen levels (hypoxia), failure to target areas that have an unfavourable microenvironment. The advances in technology, imaging and understanding of biological processes offer an opportunity to explore novel approaches.
The aim of my research has three main themes with the ultimate aim of maximising clinical benefit in terms of better tumour control and reduction in toxicity.
1. Strategies of modulating radiotherapy (SMART). Radiotherapy dose escalation techniques using Simultaneous Integrated Boost permits intensification of radiotherapy dose to predetermined volumes within the tumour, derived from biological imaging such as PET or functional MRI. Tumour control probability/ normal tissue control probability models can be then used to refine the dose escalation within the tumour further and spare normal tissue exposure. The dose escalation is being tested in the Phase 3 clinical trial SCOPE2 for oesophageal cancer in collaboration with Dr. Crosby in Cardiff.
2. Margin targeted radiotherapy concept. The use of stereotactic ablative radiotherapy to areas at risk of not being completely cleared with surgery; with the aim of achieving complete tumour resection. This is tested in a Phase 1 trial in the preoperative setting for tumours that are difficult to clear due to proximity to critical organs.
3. Refining normal tissue toxicity modelling in thoracic malignancies. The objective of this work is to characterise and corroborate lung, heart and oesophagus radiotherapy toxicity parameters and develop individualised radiotherapy delivery techniques to minimise dose to susceptible heart, oesophagus and lung substructures. This would allow selecting the best radiotherapy dose delivery technique in patients receiving combined chemoradiation and surgery.
Maria Hawkins
Maria Hawkins is an Associate Professor and MRC Clinical Group Leader in Advanced Radiation Technology at the CRUK/MRC Oxford Institute for Radiation Oncology at the University of Oxford since 2013 and an Honorary Consultant Clinical Oncologist at the Oxford University Hospitals NHS Trust. Following a research Fellowship at Princess Margaret Hospital in Toronto Canada, she was a consultant in Clinical Oncology at the Royal Marsden Hospital and The Institute of Cancer Research, researching on integrating new technological developments in radiotherapy for gastrointestinal cancers. She was awarded the 2008 Dr Karol Sicher Fellowship by The Royal College of Radiologists and the 2009 Sylvia Lawler Prize by the Oncology Section of the Royal Society of Medicine.
Technical Radiotherapy/Advanced Radiation Oncology
Fergus Gleeson
Fergus Gleeson is a Consultant Radiologist and Professor of Radiology in Oxford. He trained in Cambridge, Papworth and London, and was a Fellow in Radiology at UCLA in Los Angeles. He was appointed to Oxford in 1992, and is head of academic radiology, the director of the Oxford Imaging Trials Unit, and a Divisional Director for the Oxford University Hospitals NHS Trust. His specialist interests are in PET and hyperpolarised xenon MRI.
Clin
ical and
Translatio
nal R
esearch
Clin
ical and
Translatio
nal R
esearch
Figure 1a: Standard dose radiotherapy treatment plan for a mid-oesophagus cancer patient. The dose scale is from 6 Gy (blue) to 50 Gy (orange) to 65 Gy (red).
Figure 1b: Increased radiotherapy dose may be delivered using SMART techniques to the central high risk volume with no increase in dose to the surrounding tissues. The dose scale is from 6 Gy (blue) to 50 Gy (orange) to 65 Gy (red).
Our group focuses on using imaging techniques in small-scale trials with the particular ambitions of improving the mechanisms of data analysis and correlating the imaging data provided with histology and treatment outcomes. There are now an unprecedented number of imaging techniques being developed that are potentially available for clinical practice, for instance, dynamic contrast enhanced MRI, perfusion CT, novel PET tracers, and hyperpolarised xenon. These techniques have yet to be shown to impact on clinical practice and often require modification of either scanning technique or methods for data analysis. There is also a significant amount of data available from current imaging techniques already in use that may potentially be used as a prognostic biomarker, predict treatment response, and modify treatment.
We have focused on a small number of different areas: angiogenesis imaging using dynamic contrast enhanced MRI and perfusion CT, dynamic FDG PET imaging, and the novel 18F PET integrin imaging agent fluciclatide (Figure 1).
We have also developed novel data analysis techniques for use in hyperpolarised xenon MRI (Figure 2). Trials in normal healthy volunteers, patients with COPD and lung cancer are currently underway, and have enabled us to develop methods of lobar analysis of ventilation and emphysema correlated with CT and pulmonary function. The aim is to develop an imaging tool that would, for instance, predict the change in lung function following lobar resection or following radiotherapy.
Novel Clinical Imaging Research Group
Figure 1: 18F fluciclatide PET-CT images of a patient with bilateral scapula bone metastases from renal cancer. Image A is pre-antiangiogenic therapy demonstrating active angiogenesis at the edge of the metastases. Image B confirms the anti-angiogenic effect of treatment with decreased integrin activity at the sites of pre-treatment avidity.
Figure 2: 3-D hyperpolarised xenon ventilation MRI image
A B
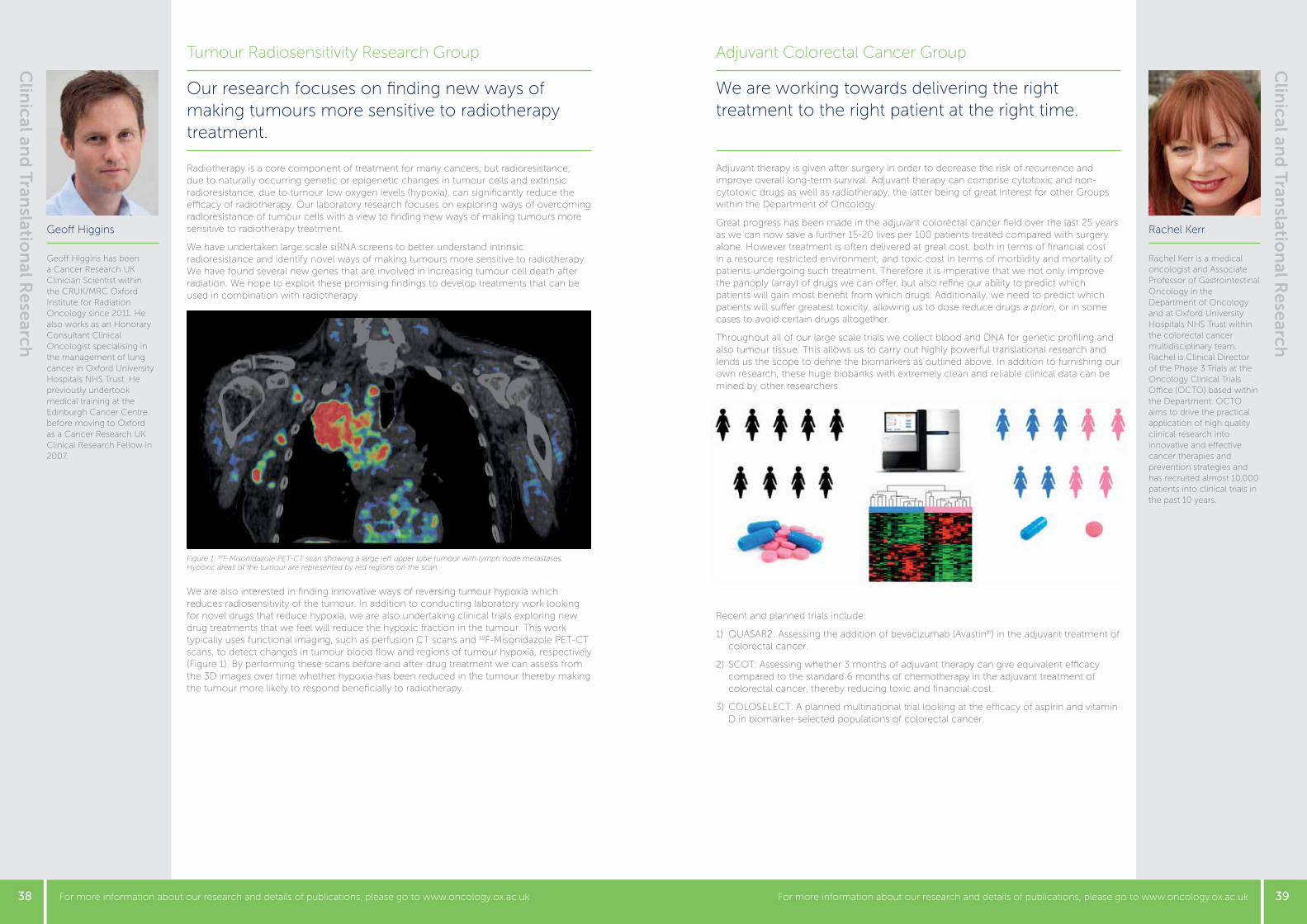
38 39For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
We are working towards delivering the right treatment to the right patient at the right time.
Adjuvant therapy is given after surgery in order to decrease the risk of recurrence and improve overall long-term survival. Adjuvant therapy can comprise cytotoxic and non-cytotoxic drugs as well as radiotherapy, the latter being of great interest for other Groups within the Department of Oncology.
Great progress has been made in the adjuvant colorectal cancer field over the last 25 years as we can now save a further 15-20 lives per 100 patients treated compared with surgery alone. However treatment is often delivered at great cost, both in terms of financial cost in a resource restricted environment, and toxic cost in terms of morbidity and mortality of patients undergoing such treatment. Therefore it is imperative that we not only improve the panoply (array) of drugs we can offer, but also refine our ability to predict which patients will gain most benefit from which drugs. Additionally, we need to predict which patients will suffer greatest toxicity, allowing us to dose reduce drugs a priori, or in some cases to avoid certain drugs altogether.
Throughout all of our large scale trials we collect blood and DNA for genetic profiling and also tumour tissue. This allows us to carry out highly powerful translational research and lends us the scope to define the biomarkers as outlined above. In addition to furnishing our own research, these huge biobanks with extremely clean and reliable clinical data can be mined by other researchers.
Recent and planned trials include:
1) QUASAR2: Assessing the addition of bevacizumab (Avastin®) in the adjuvant treatment of colorectal cancer.
2) SCOT: Assessing whether 3 months of adjuvant therapy can give equivalent efficacy compared to the standard 6 months of chemotherapy in the adjuvant treatment of colorectal cancer, thereby reducing toxic and financial cost.
3) COLOSELECT: A planned multinational trial looking at the efficacy of aspirin and vitamin D in biomarker-selected populations of colorectal cancer.
Rachel Kerr
Rachel Kerr is a medical oncologist and Associate Professor of Gastrointestinal Oncology in the Department of Oncology and at Oxford University Hospitals NHS Trust within the colorectal cancer multidisciplinary team. Rachel is Clinical Director of the Phase 3 Trials at the Oncology Clinical Trials Office (OCTO) based within the Department. OCTO aims to drive the practical application of high quality clinical research into innovative and effective cancer therapies and prevention strategies and has recruited almost 10,000 patients into clinical trials in the past 10 years.
Adjuvant Colorectal Cancer Group
Geoff Higgins
Geoff Higgins has been a Cancer Research UK Clinician Scientist within the CRUK/MRC Oxford Institute for Radiation Oncology since 2011. He also works as an Honorary Consultant Clinical Oncologist specialising in the management of lung cancer in Oxford University Hospitals NHS Trust. He previously undertook medical training at the Edinburgh Cancer Centre before moving to Oxford as a Cancer Research UK Clinical Research Fellow in 2007.
Clin
ical and
Translatio
nal R
esearch
Clin
ical and
Translatio
nal R
esearch
Our research focuses on finding new ways of making tumours more sensitive to radiotherapy treatment. Radiotherapy is a core component of treatment for many cancers, but radioresistance, due to naturally occurring genetic or epigenetic changes in tumour cells and extrinsic radioresistance, due to tumour low oxygen levels (hypoxia), can significantly reduce the efficacy of radiotherapy. Our laboratory research focuses on exploring ways of overcoming radioresistance of tumour cells with a view to finding new ways of making tumours more sensitive to radiotherapy treatment.
We have undertaken large scale siRNA screens to better understand intrinsic radioresistance and identify novel ways of making tumours more sensitive to radiotherapy. We have found several new genes that are involved in increasing tumour cell death after radiation. We hope to exploit these promising findings to develop treatments that can be used in combination with radiotherapy.
We are also interested in finding innovative ways of reversing tumour hypoxia which reduces radiosensitivity of the tumour. In addition to conducting laboratory work looking for novel drugs that reduce hypoxia, we are also undertaking clinical trials exploring new drug treatments that we feel will reduce the hypoxic fraction in the tumour. This work typically uses functional imaging, such as perfusion CT scans and 18F-Misonidazole PET-CT scans, to detect changes in tumour blood flow and regions of tumour hypoxia, respectively (Figure 1). By performing these scans before and after drug treatment we can assess from the 3D images over time whether hypoxia has been reduced in the tumour thereby making the tumour more likely to respond beneficially to radiotherapy.
Tumour Radiosensitivity Research Group
Figure 1: 18F-Misonidazole PET-CT scan showing a large left upper lobe tumour with lymph node metastases. Hypoxic areas of the tumour are represented by red regions on the scan.
40 41For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
We aim to deliver a step change in the effectiveness of radiotherapy through the evaluation of novel scientific approaches derived from the Institute’s scientists in hypothesis-driven clinical trials. The CRUK/MRC Oxford Institute for Radiation Oncology’s vision is to improve the chances of cure for patients with cancer through scientifically valid and novel ways of improving the effectiveness of radiotherapy. We are concentrating on some of the hardest to treat cancers, particularly those arising in the lung, gastrointestinal tract and bladder where radiotherapy makes an important contribution to treatment.
Improving effectiveness: We are pursuing three main ways to improve outcome from radiotherapy:• The major advances in radiotherapy in the past 30 years have been through improved
technical accuracy leading to reduced side effects. We are testing higher dose treatment using intensity modulated and stereotactic radiotherapy treatment and proton beam therapy. We have completed a clinical trial (‘Foxfire’) of targeted radiotherapy to the liver using yttrium-90 labelled microbeads.
• Low levels of oxygen (hypoxia) in the cancer make it resistant to radiotherapy and more likely to spread. We have shown in lung and pancreas cancer that use of novel targeted drugs which inhibit the PI3kinase-AKT pathway can improve oxygen delivery and reduce hypoxia.
• Radiotherapy causes DNA damage in the cancer and normal tissues. Cancer cells are often less effective at repairing damage. As novel drugs that target DNA damage repair show a marked improved response to radiotherapy in laboratory tests, we are planning to test these in patients with oesophageal cancer.
Precision Cancer Medicine: We are working on selecting approaches which can predict a person’s response to treatment based on functional imaging and biomarkers to help provide the right treatment for the right person at the right time.• Imaging hypoxia using PET scans has enabled us to prove that hypoxia is altered
through both drug and radiotherapy treatment. The degree of hypoxia and how it changes early in a treatment will help us select patients for hypoxia-modifying therapy.
• Biomarkers, which can be measured from tumour tissue or the circulation, may guide selection of the appropriate patients for specific therapies.
Colorectal cancer: Tim leads two national research studies in colorectal cancer. The MRC FOCUS4 trial started to recruit patients in 2014. It uses a novel trial design to evaluate treatments suitable for patients with molecularly-defined subgroups of colorectal cancer. The MRC funded stratified medicine consortium will be investigating biomarkers to identify those patients likely to benefit from either chemotherapy (oxaliplatin), radiotherapy, minimal surgery or novel drugs in the treatment of colorectal cancer.
Tim Maughan
Tim Maughan was appointed Professor of Clinical Oncology and Clinical Director of the CRUK/MRC Oxford Institute for Radiation Oncology in the Department of Oncology in 2011. Previously, Tim worked as an NHS consultant Clinical Oncologist in Cardiff, becoming Professor of Cancer Studies in 2007. During that time, he established the first clinical research network, the Wales Cancer Trials Network, and subsequently the development of the clinical research networks across the UK. He was the founding chair of the NCRI Clinical and Translational Radiotherapy Research Working Group (CTRad), which has a broad remit to enhance radiotherapy research in the UK.
Clinical Research Programmes
Valentine Macaulay
Valentine Macaulay is Associate Professor and Honorary Consultant in Medical Oncology in the Department of Oncology. Her clinical interests are in melanoma, and in exploring the potential of novel signalling inhibitors to enhance sensitivity to conventional anticancer treatments. She qualified as a doctor at Charing Cross Hospital Medical School and trained in Medical Oncology at the Royal Marsden Hospital, London and the Churchill Hospital, Oxford. Following a PhD with Alan Ashworth at Chester Beatty Laboratories in London, her postdoctoral training was supported by MRC Clinician Scientist and Cancer Research UK Senior Clinical Fellowships.
Clin
ical and
Translatio
nal R
esearch
Clin
ical and
Translatio
nal R
esearch
We are studying the role of insulin-like growth factor (IGF) signalling in tumour biology, aiming to exploit this information in the management of patients with cancer. The main aim of our research is to understand the contribution of insulin-like growth factor (IGF) signalling to cancer biology. Production of IGF-1 from the liver is regulated by growth hormone, and people with congenital deficiencies of growth hormone or IGF-1 are strongly protected from developing cancer. IGF-1 binds to type 1 IGF receptors that are expressed on the surface of cancer cells, activating intracellular signalling pathways that promote cell growth, invasion and resistance to killing by cancer treatments.
We have shown that IGF receptors are upregulated in prostate and renal cancers, and detectable in advanced primary tumours and metastatic disease. We also demonstrated that IGF receptors undergo ligand-dependent import into the nucleus of human tumour cells, and nuclear IGF receptor is associated with adverse prognosis in renal cancer. These findings suggest a link with aggressive tumour behaviour, and we are currently investigating the role of IGF receptor in the nucleus.
Our other major interest is to develop approaches to exploit IGF receptor and related signalling molecules as targets for cancer treatment. Our research aims to identify factors that influence sensitivity to drugs that block IGF receptor, and test IGF receptor inhibition as a route to chemo/radiosensitisation. We recently showed that IGF receptor inhibition delays the repair of DNA double-strand breaks, apparently independent of its well-known ability to regulate apoptosis induction. Understanding the basis of this effect may enable effective exploitation of this approach in the clinic.
We are also contributing to the establishment of a Preclinical Validation Core in the Department of Oncology. The aim is to provide preclinical support and optimisation for clinical trial proposals, such as the evaluation of targeted agents in new indications and/or novel combinations.
Insulin-like Growth Factor Group
Figure 1: IGF-1R undergoes nuclear translocation. Left: prostate cancer cells show IGF-induced change in IGF-1R localisation from membrane-associated to punctate nuclear signal upon IGF treatment. Centre: three clear cell renal cancers showing different patterns of IGF-1R staining: upper, predominantly membrane; centre, cytoplasmic; lower, nuclear. Right: nuclear IGF-1R is associated with adverse survival in patients.
Figure 2: IGF-1R inhibition delays repair of DNA double strand breaks. Irradiated prostate cancer cells stained for g-H2AX as a DSB marker. DNA damage is repaired within 24 hr in control cells but not in IGF-1R inhibited
cells, indicating persistence of toxic damage.

42 43For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
We apply functional and molecular imaging techniques to developing radiotherapy personalised to each patient's individual tumour biology. Medical imaging has for a long time played an absolutely central role in radiotherapy. Radiation treatments are carefully planned using patient-specific information from x-ray computed tomography (CT). An accurate 3D computer model of each patient’s anatomy is made using the CT data, with the tumour and surrounding normal organs carefully identified. Radiation treatments are then designed and simulated by computer before being delivered in the clinic. Advances in magnetic resonance imaging (MRI) and positron emission tomography (PET) now enable us to map not just patient anatomy but also physiological function, giving important information about the biochemistry of tumours as well as their physical characteristics (size and location).
For example, we know that regions of tumours that have low oxygen levels (hypoxic) are often resistant to both radiotherapy and chemotherapy. By imaging hypoxic tumour regions we can monitor response to therapy and, for patients who do not appear to be responding to treatment, either escalate radiation dose or add a hypoxia-modifying drug (or both). Dynamic contrast-enhanced (DCE) and diffusion-weighted MRI can be used to map blood flow and perfusion and/or diffusion properties in tissue, telling us about oxygen supply. PET can be used to map glucose metabolism using positron emitting radionuclides such as fluorine-18 labelled fluorodeoxyglucose (18F-FDG) and hypoxia using fluoromisonidazole (18F-FMISO).
In close collaboration with radiation oncologists within the Department of Oncology and the Churchill Hospital, we are planning, conducting and analysing a range of clinical trials acquiring a range of functional imaging (18F-FMISO and 18F-FDG PET, DCE MRI and perfusion CT) for a number of diseases including rectal, anal, pancreatic and oesophageal cancer. Data from these trials is being used to learn which imaging modality (or combination) gives the most useful information for either guiding individual patient treatments or for monitoring biological response during therapy, allowing treatments to be adapted to optimise response based on the biological profile of individual patients.
Radiotherapy Physics Research Group
Mike Partridge
Mike Partridge is an Associate Professor and has been a CRUK Group Leader of the Radiotherapy Physics Research Group at the CRUK/MRC Oxford Institute for Radiation Oncology within the Department of Oncology since 2012. He is a Fellow of the Institute of Physics. He has been working in medical imaging and radiotherapy research since 1999. He studied Natural Sciences at Cambridge University and obtained a PhD in imaging at Cranfield University before working as a postdoctoral scientist at the Institute of Cancer Research and The Royal Marsden Hospital in London, and at the German Cancer Research Centre in Heidelberg.
Mark Middleton
Mark Middleton is Professor of Experimental Cancer Medicine in the Department of Oncology and consultant Medical Oncologist at the Oxford Cancer and Haematology Centre. Mark is the Lead Cancer Clinician for the Oxford University Hospitals NHS Trust and Deputy Director of the Cancer Research UK Oxford Centre. He directs the EPCTU and the Cancer Theme of the NIHR Biomedical Research Centre. He studied medicine at Cambridge and Oxford and trained in medical oncology at the Christie Hospital. Mark is a member of the International Melanoma Working Group and of the NCRI Melanoma Clinical Studies Group. He leads several clinical trials in the national portfolio.
Clin
ical and
Translatio
nal R
esearch
Clin
ical and
Translatio
nal R
esearch
Radiotherapy treatment plan for an oesophageal cancer patient, showing the potential for dose escalation to the tumour.
Entire volume treated to 50 Gy. (outer red contour)
Tumour boosted to 62.5 Gy. (inner red contour)
Our Group's research concentrates on development of new cancer drugs and on the treatment of melanoma.
Early phase clinical trialsOur aim is to bring the excellent science in Oxford to cancer patients. Our strategy is to develop new treatments or combinations of treatments through the concepts of ‘synthetic lethality’ and oncogenic vulnerability.
To deliver this we have established the infrastructure to perform detailed analyses of tumours before, during and after intervention to select patients; to test our a priori hypotheses; and to better understand the biological effects of treatment.
We look to deliver smaller trials involving subsets of patients. These have the ability to change patient care, by focusing our efforts on tightly defined clinical populations to maximise differences in outcome, moving away from one-size-fits-all Phase 3 trials with purely correlative translational studies.
Through the Oncology Clinical Trials Office (OCTO; setting up studies to run in centres all around Europe) and the Early Phase Clinical Trials Unit (EPCTU; running trials
in the Oxford Cancer and Haematology Centre) we have established one of the largest academic early phase trials portfolios in Europe.
Melanoma trialsRecently we have seen incredible advances in the treatment of advanced melanoma. The challenges now are to understand why not all patients benefit from the new drugs at our disposal.
Genetic characteristics or signatures are being explored to identify patients who are likely to benefit from particular treatments and to make informed treatment decisions on the best combinations of drugs to use in the clinic. For example, we have defined new combinations of radiotherapy with vandetanib and of paclitaxel with trametinib, and
are active in the development of new drugs such as IMCgp100, MLN2480, T-Vec and IMM47. We are looking into biological markers to identify patients most likely to benefit from bevacizumab therapy in the national AVAST-M study, starting with those whose melanoma has a mutation in the BRAF gene.
Early Phase Clinical Trials & Melanoma Therapy
Figure produced in collaboration with Dr Samantha Warren and Dr Maria Hawkins.

44 45For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
The aim of my research group is to identify molecular-based disease classifiers using clinical omics to direct treatment of patients and precision medicine. As the Director of the Oxford NHS/BRC Molecular Diagnostics Centre (MDC), Anna Schuh leads on a translational research programme for the development, validation, standardisation and evaluation of clinical utility of next generation technologies and clinical omics. Her laboratory has developed the first fully certified next generation sequencing multigene panels for use in NHS diagnostics of cancer and a number of haematological malignancies.
The MDC has been designated an NHS England Genomic Medicine Centre and partners with Genomics England in the implementation of whole genome sequencing technology to provide NHS diagnostics. A particular focus of the laboratory is to define molecular-based disease classifiers for cancers and haematological malignancies that underpin precision medicine approaches including risk stratification and rational treatment design.
Using samples from National Cancer Research Network (NCRN) clinical trials, her group is also interested in the evaluation of the clinical utility of whole genome sequencing and was first to publish longitudinal studies of whole genome sequencing (WGS) from chronic lymphocytic leukaemia (CLL) patients undergoing treatment. A current focus of the laboratory is to further characterise hyper-mutated non-coding region in the CLL genome and to examine total RNA expression in CLL.
In her role as the clinical lead for CLL and other lymphoproliferative disorders for the Academic Health Science Network, Anna is a Chief or Principal Investigator on a number of early and late phase clinical trials that are currently undergoing review by the National Institute for Health and Care Excellence (NICE), which are likely to change clinical practice for treatment of relapsed CLL patients worldwide. She also has a particular clinical focus on Richter’s Syndrome (high grade transformation of CLL) and is the Chief Investigator on the first ever Phase 2 clinical trials for this rare patient group.
We are developing and validating novel diagnostic tests and new imaging techniques to select patients likely to benefit from certain cancer therapies and radiotherapy. Our research group’s focus is on the translation of biochemical knowledge of DNA damage repair to the selection of patients for certain cancer treatments. The group has developed several tissue biomarkers for the personalisation of chemotherapy and radiotherapy which are being tested in clinical trials.
Laboratory studies are ongoing in parallel with clinical studies of radiosensitisers to be used in the treatment of colorectal cancer, liver metastases and oesophageal cancer. New functional and dynamic imaging techniques are being tested in clinical trials led by Professor Sharma. These include:
FOXFIRE, a phase 3 trial comparing chemotherapy alone (5-fluorouracil, oxaliplatin and folinic acid) with chemotherapy plus radioembolisation for colorectal cancer that has spread to the liver. Radioembolisation (also called selective internal radiotherapy or SIRT) delivers radiation directly to the cancer cells in the liver. This novel approach minimises radiation dose to normal liver tissue;
PERFORM, a pilot study exploring the feasibility, safety and effectiveness of a novel computed tomography (CT) scanning technique called perfusion CT in patients having SIRT treatment. This approach aims to evaluate if the tumour perfusion pattern at baseline or shortly after the start of therapy can predict response to radioembolisation or chemotherapy;
SONATINA, a phase 1-2 clinical trial which aims to investigate the safety and the activity of the radiosensitising drug, nelfinavir, administered before and during radiotherapy in patients with rectal cancer. As well as establishing the safety of this novel treatment combination for patients with rectal cancer, an additional aim of the study is testing the feasibility of a new biomarker measured in tumour tissue, Tumour Cell Density (TCD).
Translational Biomarker Development Group
Ricky Sharma
Ricky Sharma has been an Associate Professor and Group Leader of the Translational Biomarker Development Group at the CRUK/MRC Oxford Institute for Radiation Oncology in the Department of Oncology since 2007. He is also an Honorary Consultant in Clinical Oncology at the Oxford University Hospitals NHS Trust and a Senior Research Fellow at Harris Manchester College, University of Oxford. He is a Fellow of both the Royal College of Physicians and the Royal College of Radiologists. He co-chairs the Early Phase Trials Workstream of the NCRI Clinical Translational Radiotherapy (CTRad) Group and is the founding chair of the Cancer Teaching Committee, University of Oxford.
Oxford Molecular Diagnostics Centre
Anna Schuh
Anna Schuh is an Associate Professor and the Director of Molecular Diagnostics in the Department of Oncology. She is also an Honorary Consultant Haematologist at Oxford University Hospitals NHS Trust. Her main research interests are with chronic lymphocytic leukaemia (CLL) and molecular diagnostics. She is a Principal Investigator on a number of early and late phase clinical trials in CLL and the Director of the Oxford NHS/BRC Molecular Diagnostics Centre (MDC). She receives grants from NIHR, Wellcome Trust and the Technology Strategy Board. She is an active member of the NCRN CLL subgroup she leads in the Genomics England 1000 CLL Genome programme.
Clin
ical and
Translatio
nal R
esearch
Clin
ical and
Translatio
nal R
esearch
Genome-wide clustering reveals changes in mutation profiles. (A-C) Grouping of somatic mutation profiles for all single nucleotide variants (SNVs). Absolute white blood cell (WBC) and lymphocyte (LY) counts are shown at the top of each figure. The bottom panels show genome-wide SNV frequencies plotted against the 5 time points. Mutation profiles for coding genes are shown as black lines.
RADIOTHERAPY
DRUG
GENE EXPRESSIONSYNERGY

46 47For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
We apply functional and molecular imaging techniques to developing radiotherapy personalised to each patient's individual tumour biology. Our primary goal is to develop radiopharmaceuticals to image and treat cancer. We have designed and synthesised investigational imaging probes that are directed against a range of cancer targets including DNA damage signalling proteins such as nucleolin, the ErbB family of receptors, angiogenesis (development of new blood vessels) and telomerase (involved in cell ageing and cancer) among others.
We have a particular interest in developing antibody-based imaging probes through our participation in the CRUK & EPSRC Cancer Imaging Centre in Oxford. Another focus is the development of techniques for targeting intracellular and, in some cases, intranuclear molecular targets for imaging through the use of cell-penetrating peptides, among other strategies.
Some tumour-seeking probes that we develop may be used for the treatment of cancer as well as imaging. We have worked with therapeutic radionuclides which emit radiation such as Auger electron-, β electron- or alpha-particles. To be effective as therapeutic agents, radionuclides must accumulate in a cancer in sufficient quantity to deliver a tumouricidal dose of radiation.
Through our work within the EPSRC Oxford Centre for Drug Delivery Devices (OxCD3), we are investigating radiolabelled nanoparticles, in combination with physical stimuli such as ultrasound, to enhance intratumoural drug release and delivery.
A major interest of the group is in the development of clinically applicable dosimetry systems for molecularly targeted theranostic agents. We are investigating novel methods for the detection of radionuclides at the subcellular, cellular and whole tissue levels. An understanding of the dose distribution at the nanometre to micrometre scale is particularly important for those therapeutic radionuclides that emit alpha particles or low energy particles, such as Auger electrons.
We use a combination of novel autoradiography approaches and Monte Carlo modelling to understand how the distribution of radionuclide in a single cell or multicellular situations determines their radiobiological effect. Our work in this area is also currently directed to understanding how to combine radionuclide therapy with external beam irradiation.
Our research group specialises in bringing fundamental physical concepts to enhance everyday clinical practice. The main concept we take is a physics approach. The model is used to provide predictions outside of the current measurement set and thereby test the model, which has the minimum number of parameters needed to describe the experimental data. While this is the standard practice of scientific methodology, we keep the ultimate clinical applicability of the concept in mind.
Fundamental concepts: One area of research is a first principle approach to quantifying DNA damage induction by irradiation with different types of ionising radiation (photon, protons, alpha particles), in such a way that it can be used in clinically relevant environments. In addition, confounding factors like the level of oxygen (as low oxygen levels confirm radio-resistance) and repair altering chemicals. The models can take these confounding factors into account. Another area of research is the use of the notion of alpha-stable distributions which are used to parametrise treatments and provide mathematical models for the robustness of external beam treatments.
Applied Work: The fundamental work is developed in a number of applied projects using dose calculations (Monte Carlo simulation and biological effects through DNA damage estimates), imaging using new equipment to allow visualisation of tumour and tumour changes during treatment, and proton therapy. Our group is strongly involved in the building of the proton therapy arm of the Precision Cancer Medicine Institute (PCMI), mainly concentrating on the possibility of low impact treatments of breast and haematological cancers (Hodgkin’s Lymphoma + Non-Hodgkin’s Lymphoma).
Clinical Implementation: Implementing concepts directly in the clinic where we introduce imaging during treatment to allow physicians to use models based on the change in texture to adapt the treatment using biological quantities (treatment response) rather than only physical ones (patient position, geometry changes). Also the robustness of models allows the planning process to be adapted to provide patient-individualised treatment margins.
Radiation Therapy Medical Physics Group
Frank Van den Heuvel
Frank Van den Heuvel has been an Associate Professor and Senior Research Scientist at the University of Oxford since 2014. He also holds an honorary appointment at the Oxford University Hospitals NHS Trust where he is Clinical Head of Section for Research and Development in Radiotherapy Physics. He was awarded a doctorate in Physics from the University of Brussels in 1994 where he also took the directorship of the radiotherapy physics department. In 1996 he moved to Wayne State University in Detroit Michigan to become an Associate Professor. In 2005 he moved back to Europe to join the University of Leuven as a Director and Professor of Medical Physics. In 2012 he was elected fellow of the American Association of Physicists in Medicine.
Experimental Radiation Therapeutics Group
Katherine Vallis
Katherine Vallis, Professor of Experimental Radiotherapeutics, is a CRUK Group Leader at the CRUK/MRC Oxford Institute for Radiation Oncology within the Department of Oncology and Honorary Consultant in Clinical Oncology within Oxford University Hospitals NHS Trust. She undertook specialist training in Clinical Oncology at the Hammersmith Hospital and doctoral research at Edinburgh University. In 1995 she was appointed as Staff Radiation Oncologist at the Princess Margaret Hospital and Scientist at the Ontario Cancer Institute, Toronto. She returned to the UK in 2006 to join the Oxford Institute and establish the Experimental Radiation Therapeutics Group.
Clin
ical and
Translatio
nal R
esearch
Clin
ical and
Translatio
nal R
esearch
Figure 1: A single-photon emission computed tomography (SPECT) image from a patient with metastatic breast cancer showing tumour accumulation of 111In-DTPA-hEGF, and a correlative CT image (Am J Nucl Med Mol Imaging 2014, 4:181-92)
Figure 2: Co-localisation of fluorophore-labelled imaging probe, anti-γH2AX-Tat (green) with γH2AX foci (red) in the nuclei (blue) of an X-irradiated MDA-MB-468 human breast cancer cell (Cancer Res. 2011, 71:4539-49)
Applied
Imaging
CBCT imaging - texture analysisTomosynthesis + Tumor Trak imaging
Dose Calculations
Monte Carlo simulations
Incorporation Radiobiology
Phenomenologic (TCP - NTCP - EUD)First principles DNA damage, repair
Robust trreatment planning
alpha stable distributions
Proton therapy
Beam parametrisationSmall fieldsBreast Treatment
Clinical
Radiosurgery
SRS small field Gaf Chromic film as detector
Adaptive treatment
IN treatment imagingAdaptive treatment - real timeAdaptive treatment - Biology
Automated QA
EPID analysistransmission dosimetryCentralized assesment
Fundamental
DNA damage
theoretical model (published)inclusion oxygen effects (write up)Validation using Au nano-particles (write up)Damage repair + in vitro validation
Mathematical modelling
Alpha -stable distributionsDynamic modeling (time dependent)Wavelet decomposition

48 49For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
Our work focuses on the application of novel imaging modalities and on the development of radiation delivery methods. Both of these are dependent on a range of interrelated technologies. Preclinical image-guided ionising radiation delivery systems are being developed, mimicking increasingly accurate patient radiotherapy. Numerous associated technical problems relate to dose delivery to small tissue volumes that ‘move’ due to breathing. We have developed sensors of this motion, coupled to very fast radiation beam gating. The accuracy of the radiation delivery critically depends on the quality of target imaging; conventional methods of cone beam CT are being complemented by optical fluorescence, ultrasound and other imaging techniques.
Fluorescence optical image guidance has also been developed for use during human surgery (Figure 1). Here we exploit the near infrared region of the optical spectrum (650-950 nm) to allow real-time imaging at tissue depths of <20 mm. This has been applied to lymph node imaging. An exciting new development is molecular optical imaging of prostate tumours to ensure that the surgeon is able to perform correct excision of extra-prostatic tumour tissue.
Time-resolved fluorescence microscopy techniques have been developed and enhanced over many years. Once excited by a light pulse, a fluorophore carries on emitting fluorescence light for a few nanoseconds. The kinetics of this process inform on resonance energy transfer between suitably chosen fluorophores tagged to proteins of interest (Főrster Resonance Energy
Transfer, FRET). This is strongly dependent on the inter-fluorophore distance and the method can be used as a molecular ruler, capable of measuring distances of 1-10 nm, way below any competing methods. We have developed medium throughput, high content automated microscopy platforms to allow protein interaction screening of patient biopsies (Figure 2). The aim here is to determine which drugs are likely to be effective at treating the cancer.
We have also developed a unique system, based around an in-house 6 MeV electron linear accelerator coupled to a robot and fluorescence microscopy, to study radiation-induced cell DNA repair kinetics using high resolution time-lapse imaging (Figure 3). We can resolve double strand breaks formed within seconds and are able to follow the temporal evolution of the repair of individual breaks.
Advanced Technology Development Group
Boris Vojnovic
Boris Vojnovic is Professor of Biophysics and has been the head of the Advanced Technology Development Group at the CRUK/MRC Oxford Institute for Radiation Oncology within the Department of Oncology since 2007. He held a similar position at the Gray Institute at Mount Vernon Hospital and has over 30 years’ experience in developing fast kinetic spectrophotometry techniques, fluorescence–based oxygen sensors, a range of accelerators and radiation sources applicable to radiobiology studies and numerous other biomedical instrumentation systems. His current interests include the application of fluorescence image-guidance techniques used during human surgery, in optimising preclinical radiation delivery systems and on the application of advanced fluorescence microscopy techniques in biomedicine.
Clin
ical and
Translatio
nal R
esearch
Figure 2: Typical images of fluorescence intensity (left) and pseudo-coloured image (right) of interacting fractions between specific proteins in a patient breast tumour tissue slice (collaboration T Ng and T Coolen, King’s College, London.
Figure 1: Right: Near infrared fluorescence image guidance system developed by the group used during surgery at the Churchill Hospital. Left: Sentinel node removal during endometrial cancer laparoscopic surgery using our guidance system.
Figure 3: the 6 MeV accelerator.

50 51For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
The Department’s world-leading scientific cores and specialist facilities provide essential support, expertise and knowledge to our research programmes. They afford the added value of in-house partnership and expert advice on developing experiments, designing equipment, maintaining cutting-edge technology and providing clinical support.
The strength of our facilities comes from a combination of outstanding staff and state-of-the-art equipment, which together enable support for basic science through to studies focused on patient benefit and clinical trials.
Our expertise is broad-ranging and multidisciplinary. It spans diverse activities, including analysis of biological samples with complex techniques such as HPLC and flow cytometry, establishment of validated assays for use in clinical studies, and modelling of cancer systems biology using computational genomics. We provide imaging at the cellular and whole body level using advanced microscopy techniques and multiple imaging platforms, including MRI, and we also have unique skills in developing radiation resources and techniques for both imaging and radiotherapy.
In addition to these physical activities, which are supported by a fully equipped mechanical engineering workshop, we have expertise in clinical trial design, optimisation and management as well as a busy, experienced early phase
clinical trials unit that provides patient care and plays an important role in the development of innovative cancer treatments.
We have invested heavily in these facilities to underpin the expanding department and provide comprehensive support
for our key areas of focus in cancer research: DNA damage and repair, tumour microenvironment, and clinical and translational research. Through a combination of funding sources, a number of new facilities have been created across the Department since 2014.
The Microscopy Core has been successful in consolidating state-of-the-art equipment and providing dedicated, skilled microscopists to optimise studies and capitalise on the available technology.
The challenges associated with the half-life of some radiolabelled agents have signalled the need for an in-house radiopharmacy unit. Once open, the PET Radiochemistry and Radiopharmacy Core will enable on-site production of radiolabelled pharmaceuticals and tracers for use in biological evaluation and clinical trials.
The Preclinical Validation Core has been established to optimise the design of both preclinical studies and clinical trials, using a combination of in vitro and in vivo methods. Additionally, support for our translational activities has been
provided through the formation of the Clinical Radiotherapy and Clinical Imaging Cores. Their focus is on improving clinical delivery through trials and the development of novel radiotherapy techniques, such as proton beam therapy, and advanced imaging techniques, including MRI, CT and PET.
Scientific Cores and Specialist Facilities
Scientific Cores and Specialist Facilities
DNA Damage & Repair Tumour Microenvironment
PET RadiochemistryOncology Clinical Trials Office
Preclinical ValidationEarly Phase Clinical Trials Unit
CLINICAL IMAGING
Microscopy
Clinical Radiotherapy
GCP LABSMechanical WorkshopClinical &Translational
Radiation Physics
Biomedical BIOINFORMATICS
Preclinical ImagingBioanalysis
Scientifi
c Co
res and
Specialist Facilities

52 53For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
We provide support in flow cytometry and in high performance liquid chromatography-mass spectrometry (HPLC-MS). The Bioanalysis Core works with research groups across the Department and also supports a number of clinical studies.
Flow cytometry can determine how actively the cell is growing, how intimate processes are proceeding, whether any abnormalities are occurring, and if necessary isolate a population of interest for further study. The flow cytometry laboratory consists of three flow cytometers and a cell sorter.
The HPLC laboratory operates as a controlled access facility in order to allow the maintenance of GCLP standards required for clinical studies. It is used for determination of cellular metabolites, and to measure the distribution of drugs in blood and tissues (pharmacokinetics) in clinical trials. New analytical methods are developed as required, and we also offer expertise in drug formulation and stability studies, and to confirm compound identity. There are three HPLC systems with coupled mass spectrometry, and a fourth HPLC offers alternative detection techniques.
Frank Van den Heuvel Academic Lead of the Clinical Radiotherapy Core
Frank Van den Heuvel is an Associate Professor, specialised in medical physics, with specific interests in in-treatment imaging and dose assessment.
Bioanalysis Core
Mike Stratford Bioanalysis Core Leader
Mike Stratford is the Bioanalysis Core Leader. He has 35 years’ experience in providing small-molecule bioanalytical support, focused on high performance liquid chromatography (hplc), for both preclinical and clinical studies. He previously worked at the Gray Cancer Institute in London before coming to Oxford in 2008.
Scientifi
c Co
res and
Specialist Facilities
Scientifi
c Co
res and
Specialist Facilities
We provide expertise in computational biology ranging from applied statistics to computational and functional genomics. The Bioinformatics Core supports investigators in the Department of Oncology in all aspects of bioinformatics through development of collaborative and independent research projects. We maintain state-of-the-art computational approaches to cancer systems biology and clinical trials to ensure coordination of experimental and analytics approaches through different phases of a research project. Increasingly, much of our research is related to individualised medicine such as an *omics assessment of cancer patients.
We focus on development of strategies for genomics data analytics, statistical algorithms for primary data analysis and interpretation, as well as on biological and clinical data integration to provide a richer and more comprehensive understanding of cancer aetiology and progression.
Bioinformatics Core
MDM2 (chr12:69,201,971–69,239,320) region amplification in bladder cancer (Cazier et al. 2014). Estimated copy number is indicated on the right hand y axis; Single nucleotide variation allele frequencies are presented on the left hand y axis.
Anastasia Samsonova Bioinformatics Core Leader
Anastasia Samsonova received her PhD from Cambridge and the EMBL-EBI. In 2007, she became a postdoctoral fellow in the laboratory of Professor Norbert Perrimon, Department of Genetics, Harvard University, where she designed innovative computational strategies for *omics data analytics.
We support the implementation of clinical trials involving novel applications of radiotherapy or novel radiotherapy techniques including proton beam. The Clinical Radiotherapy Core sits at the interface of the CRUK/MRC Oxford Institute for Radiation Oncology and the NHS radiotherapy department under the leadership of Dr Frank van den Heuvel, the Head of the NHS Radiotherapy Physics department.
The team works closely with the Radiation Oncology Group and associated staff funded by both University and NHS to support the development and implementation of the Institute’s clinical trials and those of the national trial portfolio (NIHR Clinical Research Network).
The core is increasingly focusing on proton beam therapy, undertaking comparative planning studies of photons and protons to identify subsets of patients where proton therapy has clear cut advantages as a basis for clinical trials in these areas.
Clinical Radiotherapy Core
Mike Partridge Academic Lead of the Clinical Imaging Core
Mike Partridge has 20 years’ experience in medical imaging and radiotherapy physics. He has worked at the Institute of Cancer Research, the Royal Marsden Hospital and the German Cancer Research Institute (DKFZ). He gained a PhD from Cranfield University and an MA in Natural Sciences from Cambridge.
DNA content
DNA content
We support the development and implementation of advanced imaging techniques in clinical trials. A new clinical imaging core is currently being established and will sit at the interface of the CRUK/MRC Oxford Institute for Radiation Oncology and the NHS Radiology department. The team will be led by Dr Mike Partridge (physics), Dr Ricky Sharma (oncology) and Professor Fergus Gleeson (radiology).
The team will support the development, implementation and analysis of advanced imaging techniques in magnetic resonance imaging (MRI) (spectroscopy, hyperpolarised xenon, dceMRI, shMOLLI); computerised tomography (CT) (perfusion); and positron emission tomography (PET) imaging (dynamic FDG, FMISO) in clinic trials supported by multiple funders.
Close collaboration with the Institute of Biomedical Engineering (Professor Julia Schnabel), The Oxford Centre for Functional Magnetic Resonance Imaging of the Brain (FMRIB) and commercial sources enables state-of-the-art techniques and analysis to be introduced into our studies.
Clinical Imaging Core

54 55For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
We aim to support the translation of research findings in to clinical practice. The Early Phase Clinical Trials Unit (EPCTU) supports academic and commercial research predominantly in patients with oncological and haematological cancers. The unit provides expertise in regulatory submission with most trials now being set up in under 12 weeks. The clinical space comprising of 10 beds is highly rated by patients as delivering quality care in a comfortable environment.
There is a sample handling facility co-located on the ward which enables a high sample throughput with record keeping, to demonstrate custodianship of the samples, allowing for quality analysis.
A team of research nurses and clinical fellows work across the broad portfolio of studies, providing expertise in patient management and protocol compliance. By taking a systematic approach to data capture, data entry is highly compliant and the team is trialling real-time data entry.
Early Phase Clinical Trials Unit
Kevin Myers GCP Laboratories Leader
Kevin Myers joined the Oxford ECMC in 2009 as the Senior Scientist to lead the development of GCP quality cancer biomarkers for a growing clinical trials portfolio. He previously worked for Oxford BioMedica developing novel immune cancer therapeutics, building on his postdoctoral research at the Cancer Research UK Manchester Institute.
Scientifi
c Co
res and
Specialist Facilities
Scientifi
c Co
res and
Specialist Facilities
Our goal is to accelerate the development of new cancer treatments by establishing validated assays for cancer biomarkers that can be used to evaluate clinical utility. The aim of the Oxford Experimental Cancer Medicine Centre (ECMC) GCP Laboratories is to describe the distribution and prognostic impact of markers in patient sample collections and evaluate their predictive potential in clinical trials. In order to deliver GCP compliance over the whole translational research process we collaborate with research groups to develop protocols that will produce samples of optimum quality for analysis in validated assays.
Our main areas of biomarker development and validation include tumour marker analysis by automated immunohistochemical staining, and analysis of circulating biomarkers using ELISA. Other studies include western blot analysis of cell signalling proteins and fluorometric detection of drug analytes.
We work with small phase 1/2 clinical trials and larger phase 3 studies and collaborate with groups to either carry out the whole study from development through to analysis of the trial samples, or to provide training on the use of the facilities for translational work.
GCP Laboratories
Sandie Wellman Early Phase Clinical Trials Unit Leader
Sandie Wellman has worked in the early phase team since 1999 and as the consultant nurse since 2008. She has worked in surgery, oncology and mental health.
We provide routine technical support services and operate a programme of advanced method development in order to optimise the use of the imaging facility. The Imaging Core is equipped with three Magnetic Resonance Imaging (MRI) systems, Positron Emission Tomography-CT, Single-Photon Emission Computed Tomography-CT, optical and ultrasound imaging, conventional and focused radiotherapy instruments, and a fully automated 100 Tb data storage and distribution system. We are staffed with specific expertise in in vivo biology, MR physics and engineering, and image analysis physics.
To maximise the utility of imaging in preclinical research, we develop new and better scanning techniques that reduce the impact of body motion and provide improved quantitative measurements of disease progression and the response to treatment. We are currently deploying these advances to enable multimodal image-guided radiotherapy of preclinical models of cancer, and to improve the clinical relevance and translational capabilities of the Department’s research.
Imaging Core
Sean Smart Imaging Core Leader
Sean Smart joined the CRUK/MRC Oxford Institute for Radiation Oncology in 2007 to establish the Preclinical Imaging Core. He attained degrees in Chemistry from Manchester, East Anglia and London and has worked in MRI applications and methods for over 25 years.
CAIX staining in whole TMA (a), Renal (b), Lung (c), Pancreatic (d) tumours
CT angiogram showing blood vessels on the surface of a tumour.
We provide support ranging from design to manufacture and assembly. The Mechanical Workshop assists numerous scientific groups, supporting experimental, preclinical and clinical studies. It offers a ‘total package’ from design consultation, computer modelling, computer-generated drawings, material sourcing, manufacture and assembly. Its facilities include state-of the-art machinery and innovative 3-D Computer Aided Design (CAD) packages and Computer Aided Manufacturing (CAM) software tools.
Work with ionising radiation, specialised preclinical imaging and indeed specialised clinical activities all require the development of highly specific assemblies and components. Work carried out within the Mechanical Workshop is diverse and can range from production of a peculiar optical adaptor or sample jig to manufacture of a complete radiation delivery machine.
In addition to item manufacture, the workshop offers design using CAD software tools, allowing the end user to have a complete perspective of their item prior to manufacture.
Mechanical Workshop
John Prentice Workshop Manager
John Prentice heads the Mechanical Workshop and is ably assisted by Gerald Shortland. Together, they have over 65 years of experience in tackling an extensive range of design, machining, cutting, and assembly of mechanical items.
An automated fluorescence lifetime microscope designed by Boris Vojnovic's group and manufactured in the Mechanical Workshop.

56 57For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
We provide clinical trial management support to investigators from concept to completion. OCTO was established in 2002 to run trials concerned with the practical application of high quality research into innovative and effective cancer therapies.
We work with investigators to deliver trials in medical oncology, radiotherapy and imaging from first-in-human drug trials to large phase 3 clinical studies across a range of tumour types. We have particular expertise in delivering early phase multi-centre trials for biologically distinct populations. By working with over 250 hospitals and collaborating academic groups in the UK, Europe, USA and Australia we have recruited over 10,000 patients into trials.
We work with academic research communities, industry and patients to support the work of the CRUK Oxford Centre, CRUK/MRC Oxford Institute for Radiation Oncology and the Oxford Biomedical Research Centre. OCTO is the oncology division of the UKCRC registered Oxford Clinical Trials Research Unit (OCTRU) and a member of the NCRI Cancer CTUs Working Group.
Oncology Clinical Trials Office (OCTO)
Sarah Pearson Trial Management Director of OCTO
Sarah Pearson joined OCTO in 2004 and took on the role of Trial Management Director for the unit in 2008. Before this she worked for Cancer Research UK on cancer genetics and epidemiology.
Scientifi
c Co
res and
Specialist Facilities
Scientifi
c Co
res and
Specialist Facilities
We aim to provide research groups with imaging technologies to investigate cellular processes both in vitro and in vivo. The Core is a facility established in 2014 which provides light based multidimensional imaging for researchers investigating processes at the cellular level. Fluorescently-labelled proteins can be visualised to provide an insight into their location and function in both fixed and living cells. We provide advice on sample preparation, labelling, imaging techniques and image processing.
We have a variety of systems including wide-field microscopes for time-lapse imaging of processes such as cell division, highly sensitive optical sectioning laser scanning confocal microscopes and a multi-photon microscope for deep tissue in vivo tumour imaging. We also provide commercial image processing software for data analysis.
We are developing the facility to include new technologies such as super–resolution microscopy and have strong links within the Oxford imaging community to share our resources and expertise.
Microscopy Core
Images courtesy L.Bradley, N.Vlahov and B.Markelc.
Graham Brown Microscopy Core Leader
Graham Brown established the Microscopy Core in 2014. He has a background in cell biology and has worked with Bio-Rad, Leica and Zeiss in their advanced microscopy groups.
We support radiochemistry-dependent research programmes and provide GMP-grade PET radiopharmaceuticals for clinical trials.
Currently under construction, the Positron Emission Tomography (PET) Radiochemistry and Radiopharmacy Core will be located at the Churchill Hospital alongside the PET-CT centre to enable translational research of radiotracers between the Department of Oncology and the Oxford University Hospitals NHS Trust.
The research and development labs will offer specialist radiosynthesis equipment, allowing the development of radiotracers and their production for in vitro and
preclinical research. We will transfer innovative radiochemistry protocols developed by our
collaborators in chemistry to widen the portfolio of radiotracers available for biological evaluation.
Radiotracers for human administration will be produced in the Good Manufacturing Practice (GMP)
labs since they must fulfil strict criteria for patient use. The facility and its team will provide proven PET imaging agents for trials and develop, validate and manufacture new tracer candidates.
PET Radiochemistry and Radiopharmacy Core
Rebekka Hueting PET Radiochemistry and Radiopharmacy Core Leader
Rebekka Hueting joined the Department of Oncology in 2014 to establish the PET Radiochemistry and Radiopharmacy Core. She obtained her DPhil on the synthesis of radiotracers for oncology and held a postdoctoral research fellowship at King's College London and Oxford.
Frances Willenbrock Lead Scientist
Frances Willenbrock joined the Department of Oncology in 2014 and previously held a Wellcome Trust Career Re-entry Fellowship at the CRUK London Research Institute.
Our aim is to meet the need for rapid translation of key aspects of basic science to the clinic. We work with clinicians and scientists to generate in vitro and in vivo data necessary to validate concepts emerging from basic research, and to optimise the design of in-house clinical trials. We assist in planning appropriate project proposals for further preclinical and clinical studies.
In vitro work: We have access to large panels of cell lines and are committed to a comprehensive range of techniques including primary and 3D cell culture, which may more accurately predict clinical outcome.
In vivo work: This builds upon in vitro results, focusing on new approaches for treating cancers using novel drug therapies as well as combinations with previously established drugs or radiotherapy.
The Core is embedded within the laboratories of Valentine Macaulay and Anderson Ryan.
Preclinical Validation Core
Examples of in vitro and in vivo models. Upper: human tumour cells were allowed to form spheroids, treated with drug, and spheroid size was monitored for 12 days. Graph: effect of drug on spheroid size. Lower: left, H&E staining of oesophageal cancer xenograft, and right, colorectal cancer xenograft stained for CAIX to show hypoxic areas of tumour.
Dispensing hotcell for the preparation of radiopharmaceutical doses for clinical research.

58 59For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
Scientifi
c Co
res and
Specialist Facilities
We facilitate radiation research within the department and investigate the health implications of human exposure. The Radiation Biophysics Core develops and supports a unique range of radiation resources and techniques along with providing associated expertise. These facilities range from those used for basic cell irradiations (including techniques capable of manipulating radiation fields on the sub-cellular micron scale), through to supporting and developing a SARRP image-guided preclinical x-ray irradiator and also includes developing techniques for dosimetry on clinical machines.
One of the main research interests includes investigating how and why ionising radiation initiates a diverse range of biological responses. We are also interested in how this correlates to differences in the temporal and spatial pattern of energy deposition events on the scale of DNA, cells and tissues associated with different radiation qualities of ionising radiation. Mechanisms are thus formulated which are interpreted in the context of risk associated with exposure or which can potentially be exploited in radiotherapy.
Radiation Biophysics Core
Mark Hill Radiation Biophysics Core Leader
Mark Hill is the Radiation Biophysics Core Leader, the chief examiner for the MSc in Radiation Biology and has been involved with a number of national and international committees on radiation.
Localisation of DNA repair proteins (RAD51) to damage in a cell nucleus following alpha-particle traversal; with insert showing a schematic of the alpha-particle track interacting with DNA, producing clustered damage.

60 61For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
Peter O'Neill
Professor Peter O’Neill has been the Course Director of the MSc in Radiation Biology and Deputy Director of the CRUK/MRC Oxford Institute for Radiation Oncology within the Department of Oncology since 2005. He is a Fellow of the Royal Society of Chemistry. He was awarded the Failla medal and the Weiss medal as an outstanding member of the scientific community in recognition of a history of significant contributions to radiation research.
Bleddyn Jones
Professor Bleddyn Jones is the Deputy Course Director of the MSc in Radiation Biology and researches on photon therapy at the CRUK/MRC Oxford Institute for Radiation Oncology within the Department of Oncology. He is clinically trained at the Guy’s Group of Hospitals and presently provides an advisory role in the clinic. His work in Medical Physics and Clinical Radiobiology has been recognised by the award of Honorary Fellowship of the Institute for Physics and Engineering in Medicine and the award of Honorary Fellowship of the British Institute of Radiology.
Training the next generation of scientists and clinicians to become leaders in cancer research is central to the Department of Oncology’s mission.
The Department of Oncology, which includes the CRUK/MRC Oxford Institute for Radiation Oncology, has an established, world-leading graduate training programme for science graduates and clinical research fellows. This programme is a critical element in the drive to revolutionise radiation oncology and cancer research in the UK, to make advances in radiation biology, and to translate these into improved clinical outcomes for cancer patients. The training programmes are recognised internationally and attract the highest quality students and postdoctoral researchers. As such, they play a key role in training future leaders in oncology and radiobiology research, and contribute substantially to the UK requirements for important disciplines of cancer research.
Graduate StudentsOur four year DPhil in Oncology programme has an annual intake of approximately 24 students. We have
studentships funded by Cancer Research UK, the MRC, Oxford’s prestigious Clarendon Fund, and a number of joint scholarships with Oxford colleges. We also attract a large number of externally-funded students with Commonwealth or Government funding, or with Rhodes, National Institutes of Health (NIH) or Marshall Scholarships. We hope to increase these studentships as the Department continues to expand.
We offer our promising graduates a broad range of multidisciplinary and translational cancer research projects. As a result, our graduates come from a wide range of scientific backgrounds including biology, medicine, engineering, mathematics, chemistry and physics. By coming to the Department of Oncology they work alongside and learn from leaders in their field, and we provide them with a world-class academic environment and the best support services, including a comprehensive portfolio of personal and professional skills development.
Destination of DPhil Students
Our established and successful MSc in Radiation Biology provides a core theoretical programme and also engages students in high quality basic and clinically applied research. The MSc can be a stand-alone degree, although many of our MSc scholars are medical students intercalating the MSc before returning to their medical studies in the UK or overseas. Furthermore, the MSc can form the first year of graduate research training for both science and medical students, most of whom go on to complete the DPhil in Radiation Biology or a PhD elsewhere.
Our students are equipped with the scientific knowledge and cutting-edge technical skills to become the scholars, teachers and researchers for the next generation both in the UK and globally.
Postdoctoral ResearchersOur training programme continues at the postdoctoral level to help build capacity for cancer research both in Oxford and elsewhere, through training and retention of outstanding young scientists.
Group Leaders are responsible for the scientific training of postdoctoral researchers in their groups, including the identification of appropriate external courses. Postdoctoral researchers are encouraged to develop their supervisory skills by taking leading roles in the supervision of undergraduate or MSc student research projects. The senior postdoctoral researchers are also named DPhil student co-supervisors. In addition, we have established a formalised postdoctoral programme of mentoring and scientific and generic skills development training to enhance career opportunities for our postdoctoral staff.
Destination of Postdoctoral Researchers
Clinical Research Training FellowsAlongside our DPhil programme, we run an active and expanding Clinical Research Training Fellowship programme. It provides structured research training for medical graduates to obtain a DPhil degree in radiobiology-related research and also aids them in becoming successful clinician scientists.
Case StudyMonica Olcina del Molino. Originally from Spain, Monica joined the CRUK/MRC Oxford Institute for Radiation
Oncology in 2009 from the University of Manchester with a first class degree in Pharmacy. She was in the first cohort of the MSc in Radiation Biology as part of an MRC-funded 4-year programme in Radiobiology. Monica obtained a distinction in her MSc in 2010 and then started her DPhil project in the laboratory of Ester Hammond. Monica’s
research generated 5 publications on the effects of hypoxia and DNA damage in cancer research in high profile journals such as Cell Cycle, Molecular Cell and Clinical Cancer Research. During her DPhil, Monica’s research excellence was recognised through the successful attainment of an MRC Centenary Early Career Award, numerous travel awards and poster presentation prizes. Monica is now working as a postdoctoral researcher with Professor Amato Giaccia, Department of Radiation Oncology, Stanford University.
■ Research Post, Oxford
■ Research Post, Overseas■ NHS
■ Management Industry
■ Research Post, Industry
8%17%
33%
17%
25%
■ Research Post, UK
■ Research Post, Overseas
■ Private industry
■ Healthcare
■ Teaching
■ Other
13%
12%
27%
36%8%
4%
Training

62 63For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
The Department of Oncology is committed to discovering new ways to reach the public and to support a culture of public engagement amongst its scientists.
Our public engagement strategy rests on three pillars: our choice of audiences; collaboration with stakeholders; and highly interactive delivery.
The aims of our strategy are:
• To raise aspirations amongst future scientists and encourage post-16 study of science and maths.
• To raise awareness of our work and the impact of our work amongst the general public and patient groups.
• To inform decision makers and opinion formers of the impact of our work, and to help them see the Department as a major asset to the Oxfordshire community.
Our target audiences are broad: students in secondary education and their teachers; patients, carers and allied health professionals; the general public; and high impact individuals.
Engaging with the Public
As you might expect we are a firm feature of the local science festivals. During March each year we bring our
science to the town centre events in Oxford and Abingdon and to 'Wow!How?' the University event in Oxford’s Museum of Natural History. We also supported a festival to celebrate the Centenary of the Medical Research Council. These events help us reach large numbers of people and give scientists an
opportunity to engage in short conversations with the public using existing engagement tools. The emphasis is very much on hands-on experience with table-top activities providing an interactive experience to support understanding amongst the visitors.
In addition, we have supported events further afield, including Brighton Science Festival, Big Bang in Birmingham and London, and the Northeast Science Festival in Newcastle.
Our senior researchers regularly act as the keynote speakers for major fundraising events such as the Cancer Research UK Race for Life and Relay for Life.
We ask our scientists to engage others with their science. To support them we have developed a training course which helps them develop interactive tools for engagement and then provides an audience of school students and patients; interacting with this audience allows the scientist to gain confidence through a positive experience. Feedback from the scientists has been very positive.
“It helps to make researchers enthusiastic about public engagement” Scientist participant on public engagement course
The resources developed during the course have been used at science festivals, and shared with other Cancer Research Centres across the country. Resources developed by our Public Engagement Manager have been deposited with the Times Education Supplement for use by teachers.
Enhancing Education We have responded to numerous school requests for curriculum enrichment, reaching out across Thames Valley and further to Sussex, Durham, and Denmark. We never just give talks, but have developed interactive workshops. Our latest initiative is to work with students to develop public communications tools, an approach which culminated with our annual Video Competition, which began in 2013 in support of the MRC Centenary; winning videos are published on YouTube as the Oxford Cancer Clips series.
“I really enjoyed making [the video], and I learnt a lot while researching it. Thank you for the opportunity to enter.” Year 12 student
Our collaboration with the University of Oxford’s outreach team has seen us deliver week-long oncology summer schools as part of the flagship UNIQ program. We also deliver evening classes through collaboration with The University of Oxford’s Department for Continuing Education. These classes attract audiences as diverse as students, retired teachers, biotech employees and NHS Trust workers.
Forging Partnerships
Local patient support groups are an important target audience and our update sessions focused on current research have been well received, providing hope and information to those who attend.
“My wife and I found [the evening] informative and encouraging. Keep up the good work to conquer cancer!” Member of patient group
We reach out to local VIPs especially those who can act as ambassadors for our work or who have influence or make decisions. Our guests have included the local MP, Andrew Smith, members of the county council, and the Lord Lieutenant of Oxfordshire.
Collaboration is key to good science and also good engagement. We joined hands with the British science
association to deliver SciBar evenings at a local pub; with the University Alumni Relations Office to reach the network of former students; and with the National Cancer Research Institute (NCRI) to develop their Annual Conference schools programme.
Our collaborations gained us access to audiences that would have been hard to reach in any other way. We also collaborated with school students to produce new engagement resources. By working with our audience to produce something together, we have forged partnerships based on high levels of engagement, ingenuity and energy both in the creation of resources and in the presentation of science. One senior academic at Newcastle reported shock
at finding out that the students she had been interacting with were still at school - she thought they were graduate students. This is testament to the confidence and familiarity they displayed with the material that they had presented.
Communicating the Impact of Research
Members of the public learn about cancer research at Wow!How? Family Science Fair
Professor Tim Maughan addressing CRUK Race for Life participants in Oxford
MP Andrew Smith hears about our work during a visit to the Department
Raising aspirations to study science

64 65For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
Providing a collaborative and nurturing environment for translational multidisciplinary cancer research is at the heart of the Department of Oncology. It is through these partnerships that we can attract long-term funding to remain at the forefront of oncology research. Furthermore, we work proactively within these partnerships on outreach and engagement with local schools, patient groups and the public to inform, educate and inspire.
Cancer Research UK and Medical Research Council Oxford Institute for Radiation OncologyDirector: Professor Gillies McKenna Deputy Directors: Professors Tim Maughan, Ruth Muschel and Peter O’Neill
The joint CRUK and MRC funded Oxford Institute for Radiation Oncology is an integral part of the Department of Oncology and is dedicated to exploring aspects of radiation biology research that could yield new advances in the treatment of cancer. These include understanding how
cells respond to and repair radiation-induced DNA damage, defining the microenvironmental factors that affect these responses and identifying targets to alter tumour or normal tissue responses to radiation. The Institute aims to integrate basic research with imaging science to advance radiation treatments. Incorporating these developments with radiotherapy in clinical trials allows identification of opportunities which have the potential to improve patient care and allow earlier detection of primary and metastatic cancers.
Working in Partnership
Cancer Research UK Oxford CentreDirector: Professor Gillies McKenna Deputy Director: Professor Mark Middleton
The CRUK/MRC Oxford Institute for Radiation Oncology took a leading role in establishing the CRUK Oxford Centre in 2010 as a partnership between the University of Oxford, Oxford University Hospitals NHS Trust and Cancer Research UK. The Centre aims to draw on the breadth and depth of fundamental research being undertaken at the University of Oxford and translate it into novel therapeutic strategies which increase cancer cure rates to save and improve people’s lives. The Centre currently comprises over 500 members from more than 25 Departments, Units and Institutes of the University, including the Department of Oncology (from where it is managed), as well as from the NHS Trust. Members work across a range of disciplines and collaborate on a local, national and international scale. The Centre supports the translation of novel ideas and hypotheses into early phase clinical trials to speed up the transition from scientific discovery to treatments in patients.
Cancer Research UK and Engineering and Physical Sciences Research Council Cancer Imaging Centre in OxfordLead: Professors Ruth Muschel, Mike Brady and Gillies McKenna
The Cancer Imaging Centre in Oxford is one of four national Centres funded by a strategic initiative between CRUK and the EPSRC. Its establishment was headed by the CRUK/MRC Oxford Institute for Radiation Oncology to develop advanced image-based methods for use in cancer therapy, diagnosis and prognosis.
Managed from within the Department of Oncology, it is built upon a University-wide and industrial consortium of imaging researchers and brings together multidisciplinary teams including radiologists, surgeons, radiation oncologists, medical oncologists, biologists, chemists, engineers and mathematicians. Together, through basic science, preclinical and clinical studies, they explore how imaging and image-analysis can be used to help select the most appropriate patients for treatment as well as how image-derived information can be used to guide treatment choices and direct assessment of response to therapy.
National Institute for Health Research Oxford Biomedical Research CentreDirector: Professor Keith Channon
The NIHR Oxford Biomedical Research Centre (BRC) brings together the research expertise of the University of Oxford and the clinical skills of the Oxford University Hospitals NHS Trust to support translational research and innovation to improve healthcare for patients. It is made up of 14 research themes covering all areas of therapy.
The Cancer Theme, led by Department of Oncology Professors Mark Middleton and Adrian Harris, aims to develop new treatments or combinations of treatments through the concepts of synthetic lethality and oncogenic vulnerability. It has established the infrastructure to deliver a wide portfolio of academic multi-centre early phase studies involving subsets of patients, and to perform detailed analyses of tumours before, during and after intervention to select patients.
Oxford Experimental Cancer Medicine CentreLead: Professor Mark Middleton
The Oxford Experimental Cancer Medicine Centre (ECMC) is jointly supported by CRUK and the UK Department of Health. The goal of the ECMC initiative is to develop new therapies to bring benefits to patients faster. In Oxford the focus has been on the application of basic scientific discoveries in cancer biology to the development of novel therapies and prognostic/diagnostic biomarkers to help personalised patient care. Through a team of scientists based in the Department of Oncology, the Oxford ECMC has expertise in immunology, DNA repair, angiogenesis and molecular pathology and has facilities for conducting imaging, proteomics, microarray and radioisotope studies.
Oxford University Hospitals NHS TrustThe Churchill Hospital, part of the Oxford University Hospitals NHS Trust, is a world-renowned centre of excellence for cancer services and a major centre for healthcare research. The Cancer and Haematology Centre was opened in the Churchill Hospital in 2009, and brought together a wide range of medical and surgical services including cancer medicine, surgery, and diagnostic services. It serves as a base for University research teams, working in partnership with NHS colleagues.
The Department of Oncology works closely with the Radiotherapy Department to ensure that research is rapidly and efficiently translated into cutting-edge clinical treatment for cancer patients. Through these partnerships, the use of Image-Guided Radiotherapy is widespread and the use of Intensity Modulated and Stereotactic Body Radiotherapy is increasing.
Department of Oncology Annual Grant Funding
*CRUK Oxford Centre, CRUK & EPSRC Cancer Imaging Centre in Oxford, NIHR Oxford BRC, Oxford ECMC
36% 33%
31%
CRUK/MRC Oxford Institute for Radiation Oncology
Centres*
Other grants

66 67For more information about our research and details of publications, please go to www.oncology.ox.ac.uk For more information about our research and details of publications, please go to www.oncology.ox.ac.uk
A team of talented and dedicated individuals works together to provide a comprehensive and supportive infrastructure that underpins the outstanding research of the Department of Oncology.
Management of the Department is the responsibility of the Executive Committee, which comprises the Head of Department and up to eight senior academics and managers from the Operations and Strategic Projects groups.
OperationsLead: Pamela Nieto, Head of Administration and Finance
Management of the Department’s operational and financial activities falls to the Operations Group, led by Pamela Nieto and supported by Claire Shingler, Operations Manager. Each functional unit delivers activities in its dedicated area to ensure the smooth running of this large research intensive department. Specialist areas include HR, finance, facilities and health and safety, graduate studies, research facilitation, information technology and public engagement. Personal and Executive Assistants provide
administrative support to the senior researchers, clinicians and their groups and play a vital role in the organisation of meetings, events and seminar series and in the support of department-wide activities. This strong and dedicated support base affords the added value of releasing senior scientific and clinical staff from the daily administrative tasks required to maintain excellence in the Department.
Human ResourcesLead: Claire Matthews, HR Manager
The HR team provides operational management, advice and guidance to managers and staff on all employment-related matters, such as recruitment, policy guidance, legislation and best practice. It runs a successful personal development review process for all staff in the Department and plays a key role in Athena SWAN activities.
Running the Department
Finance Lead: Paul Godden, Strategic Finance Manager
The Finance team provides a wide-ranging service to the Department, which covers all areas of pre- and post-award management, procurement and finance. It offers particular expertise in the financial management of clinical trials. The team supports the Head of Department and Head of Administration and Finance with the management of the Department’s budget and works closely with senior scientific and clinical staff to cost new research proposals and administer internal and external grant awards.
Building and Facilities Lead: Larry Turner, Building and Facilities Manager
The Building and Facilities team provides comprehensive research laboratory and facilities support across the Department. This includes routine and specialist services provision and day-to-day frontline support. The team manages a broad portfolio of equipment service contracts, develops service provisions and plays an active role in equipment procurement. It coordinates bespoke and specialist projects such as space reconfigurations and building refurbishment works. Larry Turner is the Departmental Safety Officer, providing guidance and advice on local and University-wide procedures and best practice.
Graduate Studies Lead: Sarah Norman, Training and Development Lead
The Graduate Studies team works to ensure that all MSc, MRes and DPhil students are supported and developed throughout the course of their studies in the Department. The team also facilitates the admissions process and manages all student funding. It runs a comprehensive graduate training programme and organises careers events and a highly successful annual Student Symposium.
Research Facilitation Lead: Sarah Norman, Training and Development Lead
The Research Facilitation team is a first point of contact for external funding applications. It works with a wide range of scientists and clinicians from early career and postdoctoral researchers to senior academics and professors. The team contributes to the ongoing support for research in the Department, and the input and advice provided assists in preparing the highest quality funding applications.
Information Technology Lead: Claire Shingler, Operations Manager
Our team of IT professionals provides local desktop, server and database support to staff and students, in conjunction with Divisional and University IT staff. The team supports a mixed Mac and PC environment, manages a range of IT-related projects and provides assistance with the Department’s peripherals, mobile devices and other equipment.
Public Engagement Lead: Martin Christlieb, Public Engagement and Communications Manager
Communicating the impact of our research is a key activity in the Department. Assisted by numerous research staff and students from a range of disciplines, our Public Engagement Manager educates and inspires school students, teachers, patients, the general public and scientists alike. This is done through a variety of ways, including lab tours, school visits, science festivals and adult education courses.
Strategic ProjectsLead: Claire Bloomfield, Strategic Projects Manager
The Strategic Projects Group works closely with the Head of Department to take forward key initiatives of strategic importance to the Department. Examples of their work include large funding bids and the establishment of new research facilities. Specialist Project Managers oversee the CRUK Oxford Centre, the BRC Cancer Theme, Experimental Cancer Medicine Centre and the CRUK & EPSRC Cancer Imaging Centre in Oxford.

68 For more information about our research and details of publications, please go to www.oncology.ox.ac.uk

For more information on the Department of Oncology, visit our website at: www.oncology.ox.ac.uk
E-mail: [email protected]
Phone: +44 (0)1865 617331
Address: Department of Oncology University of Oxford Old Road Campus Research Building Roosevelt Drive Oxford OX3 7DQ UK
Contact Us