Department of Kinesiology - Biomechanics University of Waterloo, 2002 Effectiveness of a...
60
Department of Kinesiology - Biomechanics University of Waterloo, 2002 Effectiveness of a Participatory Effectiveness of a Participatory Ergonomics Intervention in Reducing Ergonomics Intervention in Reducing Worker Pain Severity Through Worker Pain Severity Through Physical and Psychosocial Exposure Physical and Psychosocial Exposure Pathways Pathways Andrew Laing
-
Upload
jonathan-thompson -
Category
Documents
-
view
218 -
download
0
Transcript of Department of Kinesiology - Biomechanics University of Waterloo, 2002 Effectiveness of a...
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Effectiveness of a Participatory Ergonomics Effectiveness of a Participatory Ergonomics Intervention in Reducing Worker Pain Intervention in Reducing Worker Pain
Severity Through Physical and Severity Through Physical and Psychosocial Exposure PathwaysPsychosocial Exposure Pathways
Andrew Laing
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Why Ergonomics Research?Why Ergonomics Research?
Effectiveness debatesEffectiveness debates Legislation and PoliciesLegislation and Policies Evidence based decisionsEvidence based decisions
What should should an ergonomist What should should an ergonomist focus on?focus on?
Department of Kinesiology - Biomechanics University of Waterloo, 2002
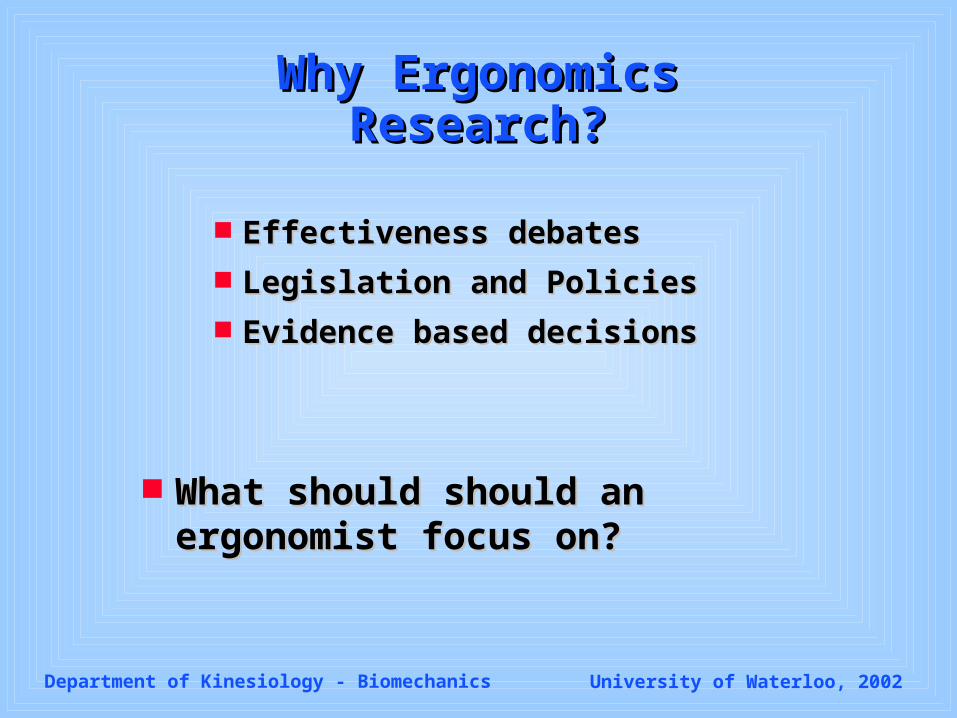
OUBPS Study ResultsOUBPS Study Results
Biomechanical Risk Factors:(Measured):“higher” peak shear“higher” peak hand force “higher” cumulative compression“higher” forward bending“higher” perceived phys demands
Psychosocial Risk Factors:(Perceived / questionnaire)“poorer” workplace social environment“higher” perceived education
(compared to peers)“lower” job control“higher” co-worker support“higher” job satisfaction
Individual Risk Factors:Prior WCB Low Back ClaimHigher body mass index (Ht. Wt.)
11.5%
4.7%31.4%
Biomechanical Risk Factors:(Measured):“higher” peak shear“higher” peak hand force “higher” cumulative compression“higher” forward bending“higher” perceived phys demands
Psychosocial Risk Factors:(Perceived / questionnaire)“poorer” workplace social environment“higher” perceived education
(compared to peers)“lower” job control“higher” co-worker support“higher” job satisfaction
Individual Risk Factors:Prior WCB Low Back ClaimHigher body mass index (Ht. Wt.)
11.5%
4.7%31.4%
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Participatory ErgonomicsParticipatory Ergonomics
A process of ergonomic problem solving A process of ergonomic problem solving that incorporates input from each relevant that incorporates input from each relevant
workplace stakeholder group in workplace stakeholder group in identification of areas for improvement, identification of areas for improvement,
solution development, and implementation solution development, and implementation of physical and work organizational of physical and work organizational
changes in order to minimize risk of injury changes in order to minimize risk of injury and maximize productivity.and maximize productivity.
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Studies on EffectivenessStudies on EffectivenessN = 11N = 11
Inconsistent outcome variablesInconsistent outcome variables Weak study designs (Control Groups: N = 2)Weak study designs (Control Groups: N = 2) Need for:Need for:
high quality longitudinal studieshigh quality longitudinal studies studies that describe and measure studies that describe and measure
interventionsinterventions studies that measure worker health studies that measure worker health
outcomesoutcomes
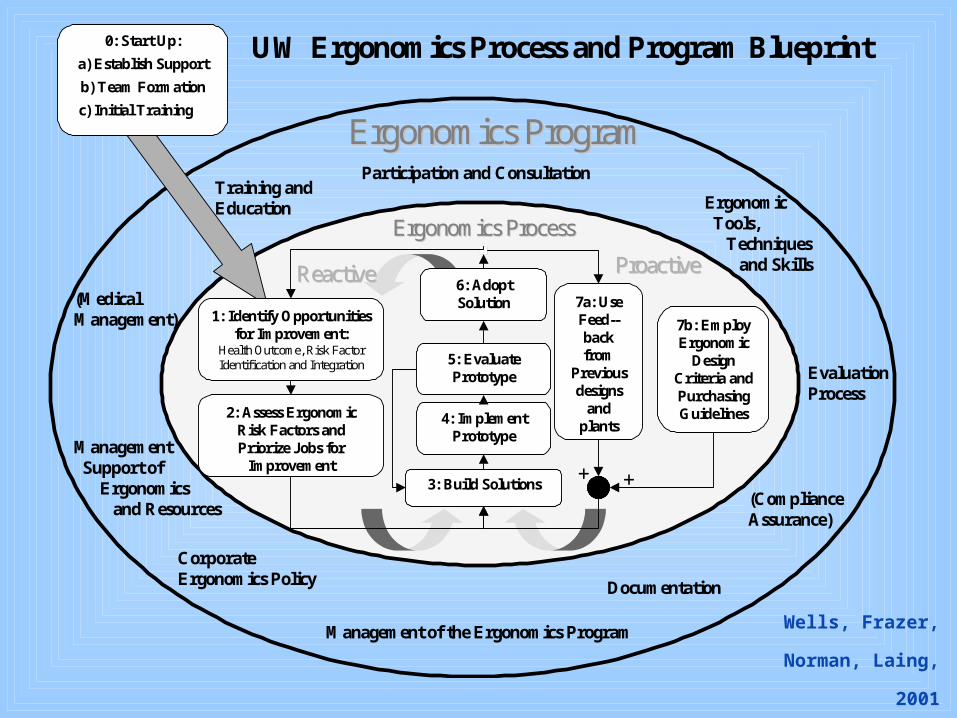
Ergonomics ProcessErgonomics Process
Ergonomics ProgramErgonomics Program
UW Ergonomics Process and Program Blueprint
1: Identify Opportunitiesfor Improvement:
Health Outcome, Risk FactorIdentification and Integration
2: Assess ErgonomicRisk Factors andPriorize Jobs for
Improvement3: Build Solutions
4: ImplementPrototype
5: EvaluatePrototype
6: AdoptSolution
ReactiveReactive ProactiveProactive
7b: EmployErgonomic
DesignCriteria andPurchasingGuidelines
7a: UseFeed--backfrom
Previousdesigns
andplants
Training and Education
Management of the Ergonomics Program
Evaluation Process
0: Start Up:
a) Establish Support
b) Team Formation
c) Initial Training
(Medical Management)
Documentation
++(Compliance Assurance)
Participation and Consultation
Management Support of Ergonomics and Resources
Corporate Ergonomics Policy
Ergonomic Tools, Techniques and Skills
Wells, Frazer, Norman,
Laing, 2001
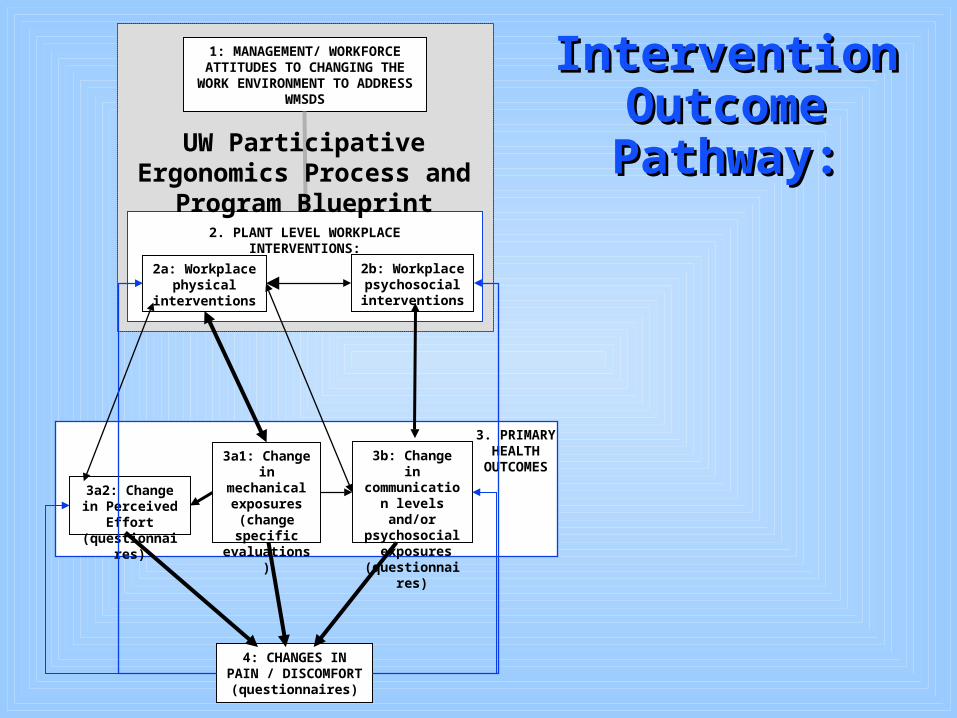
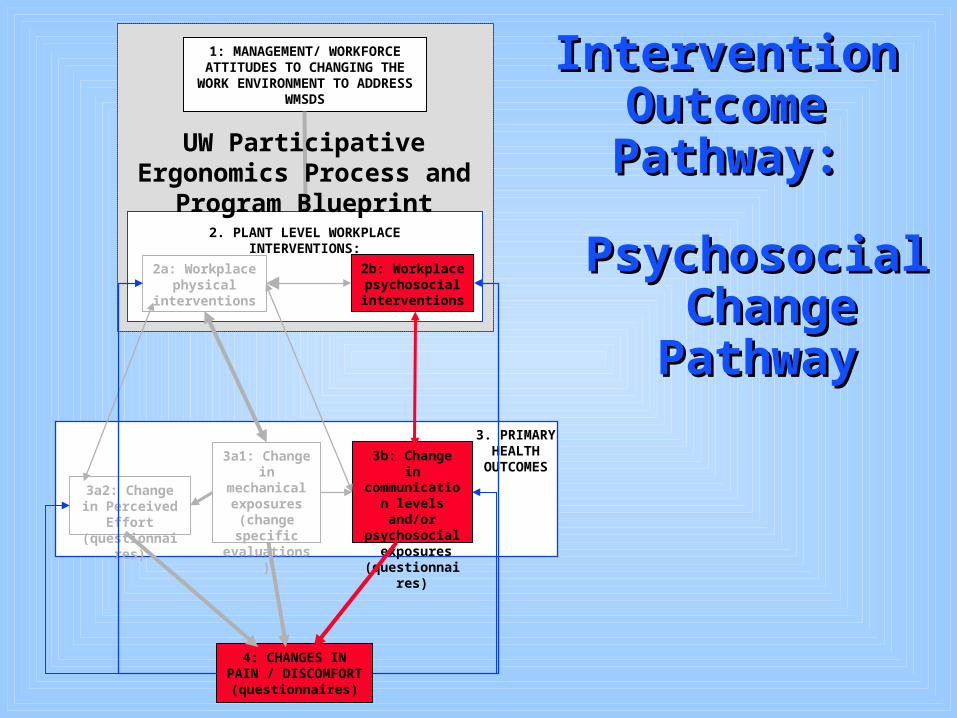
Intervention Intervention Outcome Outcome Pathway:Pathway:
4: CHANGES IN PAIN / DISCOMFORT
(questionnaires)
2a: Workplace physical
interventions
2. PLANT LEVEL WORKPLACE INTERVENTIONS:
2b: Workplace psychosocial interventions
3b: Change in communication
levels and/or psychosocial
exposures (questionnaires)
3a1: Change in mechanical exposures (change specific
evaluations)
3a2: Change in Perceived Effort (questionnaires)
1: MANAGEMENT/ WORKFORCE ATTITUDES TO CHANGING THE
WORK ENVIRONMENT TO ADDRESS WMSDS
UW Participative Ergonomics Process and Program Blueprint
3. PRIMARY HEALTH
OUTCOMES

4: CHANGES IN PAIN / DISCOMFORT
(questionnaires)
2a: Workplace physical
interventions
2. PLANT LEVEL WORKPLACE INTERVENTIONS:
2b: Workplace psychosocial interventions
3b: Change in communication
levels and/or psychosocial
exposures (questionnaires)
3a1: Change in mechanical exposures (change specific
evaluations)
3a2: Change in Perceived Effort (questionnaires)
1: MANAGEMENT/ WORKFORCE ATTITUDES TO CHANGING THE
WORK ENVIRONMENT TO ADDRESS WMSDS
UW Participative Ergonomics Process and Program Blueprint
3. PRIMARY HEALTH
OUTCOMES
Intervention Intervention Outcome Outcome Pathway:Pathway:
Physical Physical Change Change PathwayPathway
4: CHANGES IN PAIN / DISCOMFORT
(questionnaires)
2a: Workplace physical
interventions
2. PLANT LEVEL WORKPLACE INTERVENTIONS:
2b: Workplace psychosocial interventions
3b: Change in communication
levels and/or psychosocial
exposures (questionnaires)
3a1: Change in mechanical exposures (change specific
evaluations)
3a2: Change in Perceived Effort (questionnaires)
1: MANAGEMENT/ WORKFORCE ATTITUDES TO CHANGING THE
WORK ENVIRONMENT TO ADDRESS WMSDS
UW Participative Ergonomics Process and Program Blueprint
3. PRIMARY HEALTH
OUTCOMES
Psychosocial Psychosocial Change Change PathwayPathway
Intervention Intervention Outcome Outcome Pathway:Pathway:
4: CHANGES IN PAIN / DISCOMFORT
(questionnaires)
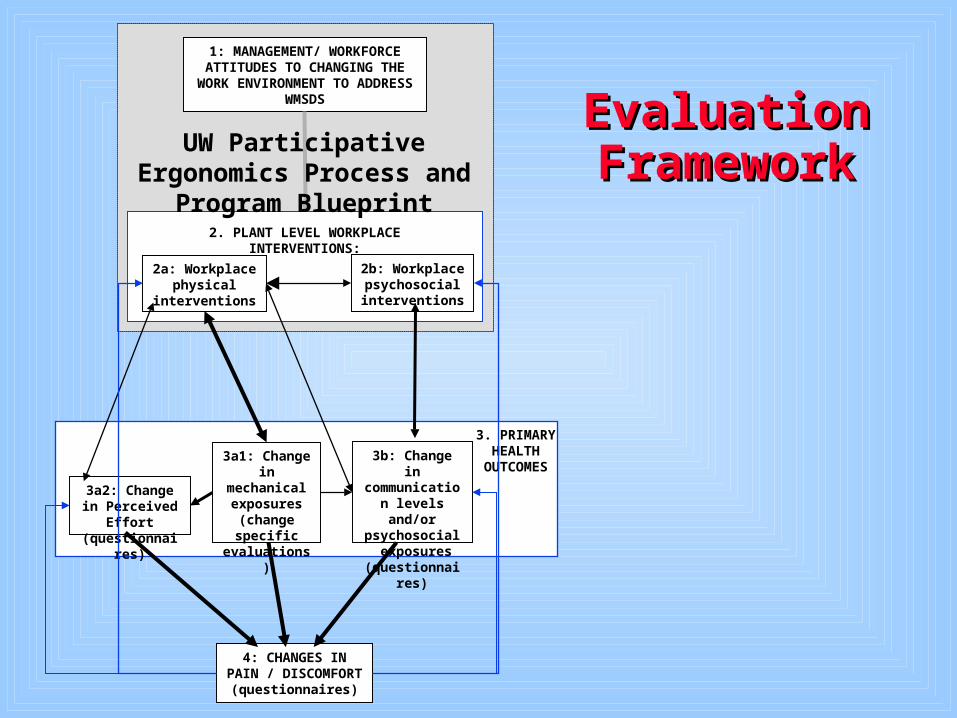
2a: Workplace physical
interventions
2. PLANT LEVEL WORKPLACE INTERVENTIONS:
2b: Workplace psychosocial interventions
3b: Change in communication
levels and/or psychosocial
exposures (questionnaires)
3a1: Change in mechanical exposures (change specific
evaluations)
3a2: Change in Perceived Effort (questionnaires)
1: MANAGEMENT/ WORKFORCE ATTITUDES TO CHANGING THE
WORK ENVIRONMENT TO ADDRESS WMSDS
UW Participative Ergonomics Process and Program Blueprint
3. PRIMARY HEALTH
OUTCOMES
Evaluation Evaluation FrameworkFramework
Department of Kinesiology - Biomechanics University of Waterloo, 2002
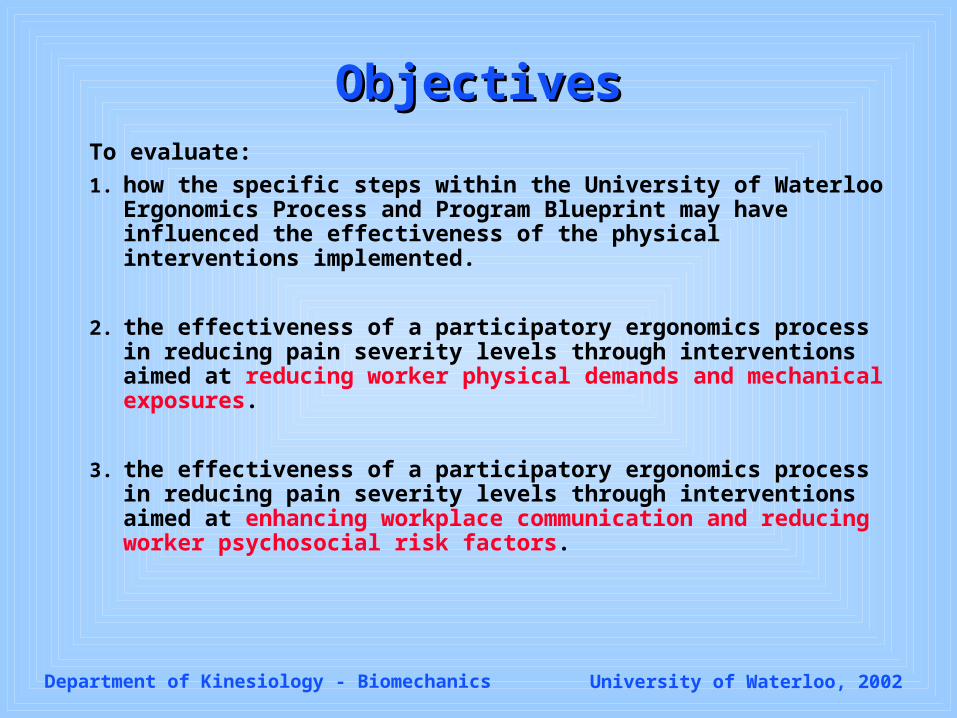
ObjectivesObjectivesTo evaluate:
1. how the specific steps within the University of Waterloo Ergonomics Process and Program Blueprint may have influenced the effectiveness of the physical interventions implemented.
2. the effectiveness of a participatory ergonomics process in reducing pain severity levels through interventions aimed at reducing worker physical demands and mechanical exposures.
3. the effectiveness of a participatory ergonomics process in reducing pain severity levels through interventions aimed at enhancing workplace communication and reducing worker psychosocial risk factors.
Department of Kinesiology - Biomechanics University of Waterloo, 2002
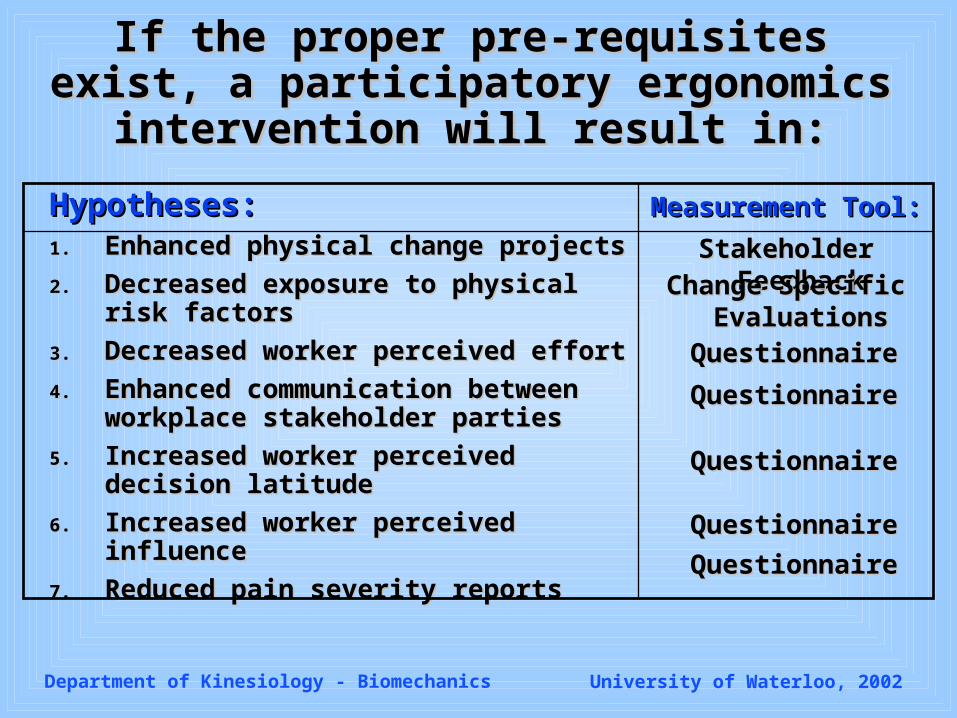
If the proper pre-requisites exist, a If the proper pre-requisites exist, a participatory ergonomics intervention will participatory ergonomics intervention will
result in:result in:
Hypotheses:Hypotheses:1.1. Enhanced physical change projectsEnhanced physical change projects
2.2. Decreased exposure to physical risk Decreased exposure to physical risk factorsfactors
3.3. Decreased worker perceived effortDecreased worker perceived effort
4.4. Enhanced communication between Enhanced communication between workplace stakeholder partiesworkplace stakeholder parties
5.5. Increased worker perceived decision Increased worker perceived decision latitudelatitude
6.6. Increased worker perceived influenceIncreased worker perceived influence
7.7. Reduced pain severity reportsReduced pain severity reports
Measurement Tool:Measurement Tool:
Stakeholder FeedbackStakeholder Feedback
QuestionnaireQuestionnaire
QuestionnaireQuestionnaire
QuestionnaireQuestionnaire
QuestionnaireQuestionnaire
QuestionnaireQuestionnaire
Change Specific Change Specific EvaluationsEvaluations
Department of Kinesiology - Biomechanics University of Waterloo, 2002
METHODSMETHODS
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Study SitesStudy Sites
Automotive Foam ManufacturerAutomotive Foam Manufacturer
Intervention (Whitby) / Control (Tilbury) Intervention (Whitby) / Control (Tilbury) PlantsPlants Subjects performing identical workSubjects performing identical work
Department of Kinesiology - Biomechanics University of Waterloo, 2002
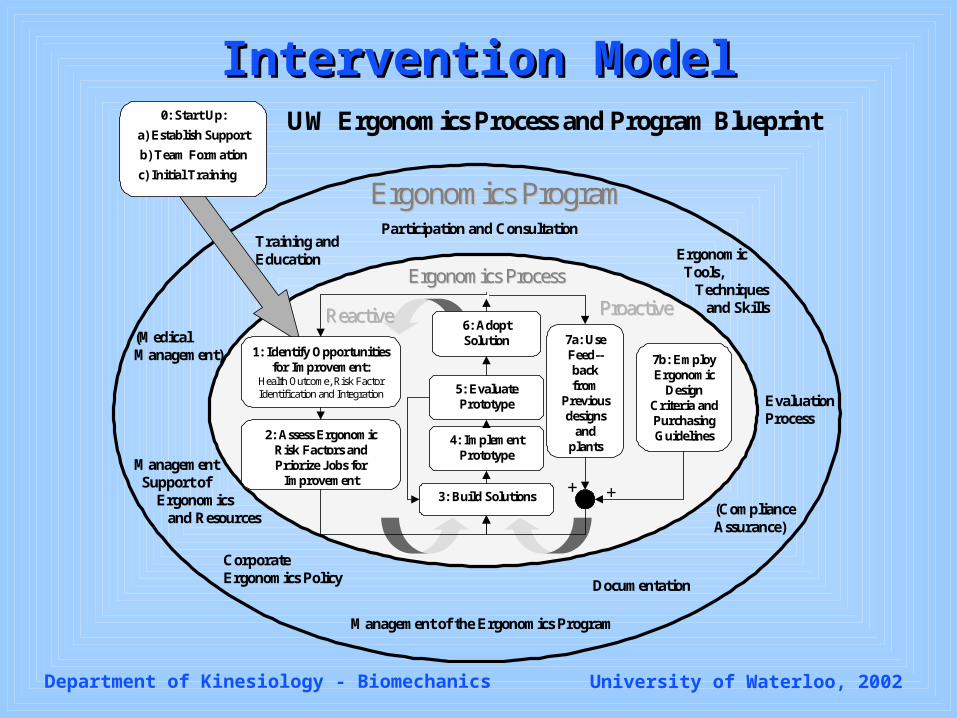
Intervention ModelIntervention Model
Ergonomics ProcessErgonomics Process
Ergonomics ProgramErgonomics Program
UW Ergonomics Process and Program Blueprint
1: Identify Opportunitiesfor Improvement:
Health Outcome, Risk FactorIdentification and Integration
2: Assess ErgonomicRisk Factors andPriorize Jobs for
Improvement3: Build Solutions
4: ImplementPrototype
5: EvaluatePrototype
6: AdoptSolution
ReactiveReactive ProactiveProactive
7b: EmployErgonomic
DesignCriteria andPurchasingGuidelines
7a: UseFeed--backfrom
Previousdesigns
andplants
Training and Education
Management of the Ergonomics Program
Evaluation Process
0: Start Up:
a) Establish Support
b) Team Formation
c) Initial Training
(Medical Management)
Documentation
++(Compliance Assurance)
Participation and Consultation
Management Support of Ergonomics and Resources
Corporate Ergonomics Policy
Ergonomic Tools, Techniques and Skills
Department of Kinesiology - Biomechanics University of Waterloo, 2002
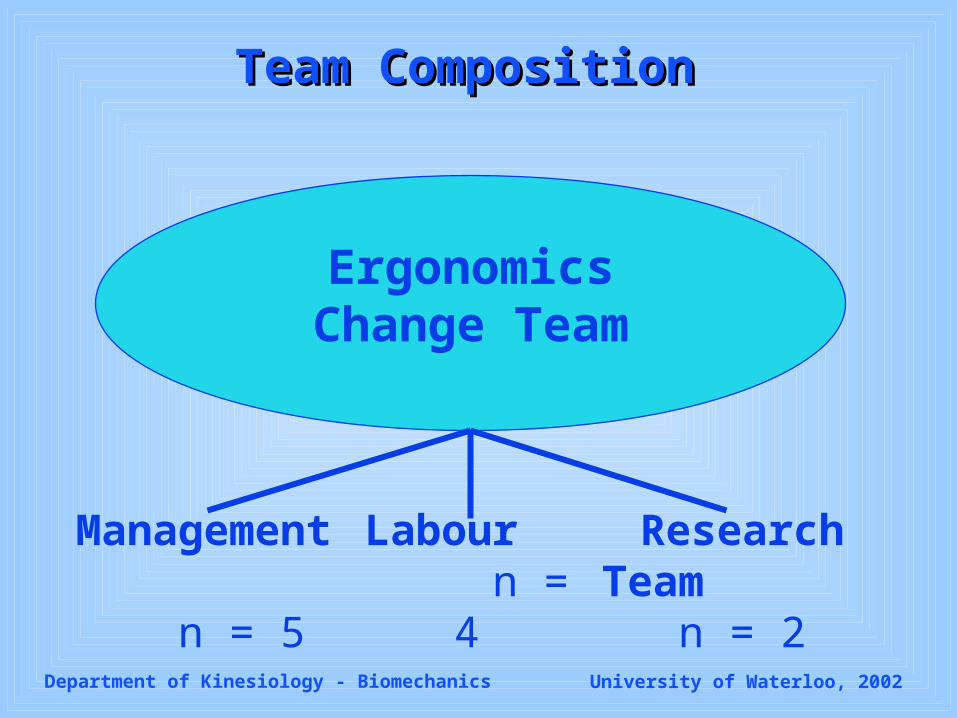
Team CompositionTeam Composition
Research Team n = 2
Management n =
5
Labour n = 4
Ergonomics Change Team
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Input from stakeholder groups on Input from stakeholder groups on the effectiveness of final changes the effectiveness of final changes compared to initial prototypes.compared to initial prototypes.
Evaluation Tools:Evaluation Tools:Stakeholder FeedbackStakeholder Feedback
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Evaluation Tools:Evaluation Tools:Change Specific EvaluationsChange Specific Evaluations
Evaluation of each change using: EMG, accelerometry, biomechanical modeling, worker ratings of preference expert opinion of UW researchers
Peak, Task Level, Shift Long, Overall Exposure Changes
Overall Time Weighted Changes =
Shift-Long Time Weighted Changes * Compliance * # of Workers
Affected At One Time / Total Workers in Department
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Evaluation Tools: Evaluation Tools: QuestionnairesQuestionnaires
Perceived Effort: Borg CR-10 scale (Borg, 1990)
Communication Dynamics: 7 items, 5 point ordinal scale
Perceived Decision Latitude: Karasek’s JCQ (1985) – 9 items, 5 point ordinal scale
Perceived Influence: Greenberger (1981) – 11 items, 5 point ordinal scale
Reported pain severity body-part specific, 5 point ordinal scale
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Qualitative observation of elements implemented, and perceptions of commitment to the participatory process.
Evaluation Tools: Evaluation Tools: Qualitative Process EvaluationQualitative Process Evaluation
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Questionnaire Statistical Questionnaire Statistical Analyses:Analyses:
Perceived effort, decision latitude, influence, reported pain severity Between Plants: 2X2 ANOVAS (Pre/Post X
Whitby/Tilbury). Interaction effects were of primary interest
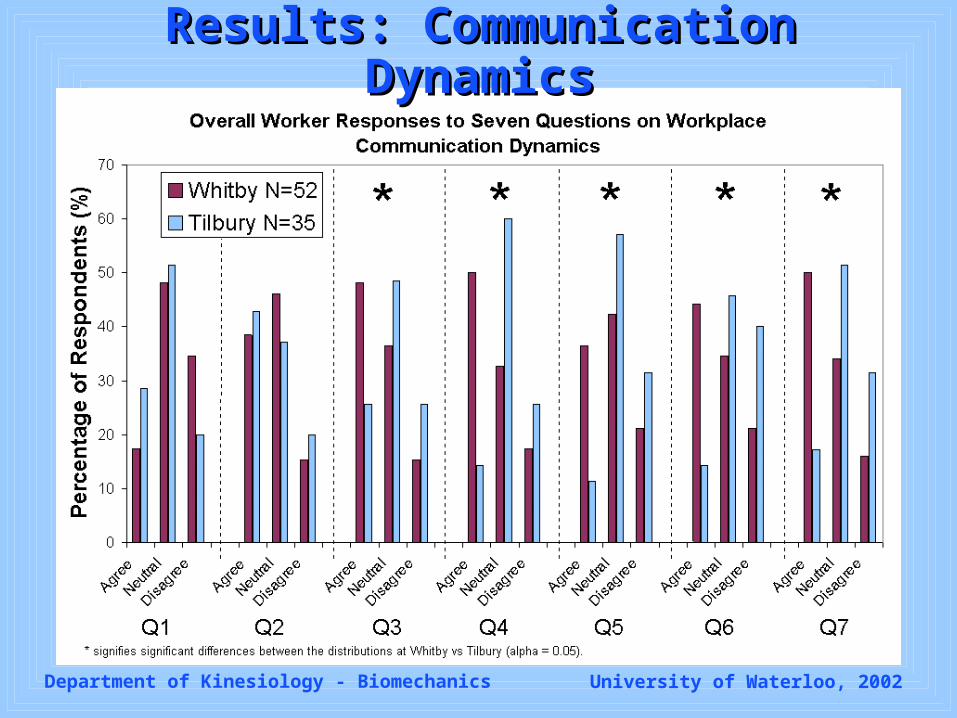
Communication Dynamics (only ‘Post’ responses) Between Plants: Chi Square
Perceived effort, decision latitude, influence, reported pain severity Between Plants: 2X2 ANOVAS (Pre/Post X
Whitby/Tilbury). Interaction effects were of primary interest
Communication Dynamics (only ‘Post’ responses) Between Plants: Chi Square
Department of Kinesiology - Biomechanics University of Waterloo, 2002
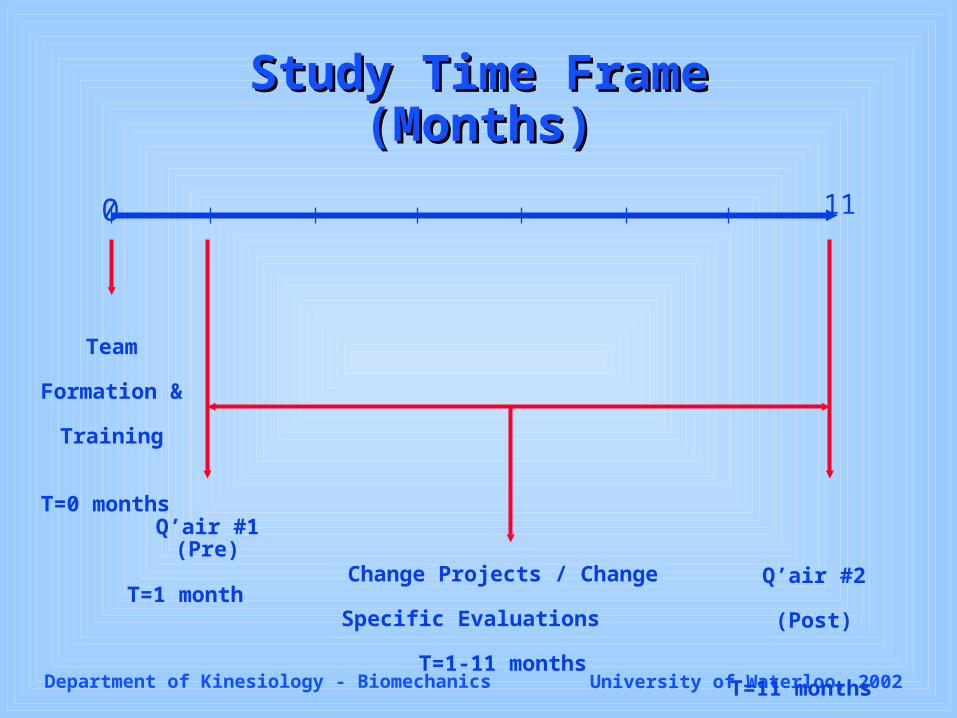
Study Time FrameStudy Time Frame (Months) (Months)
Team
Formation &
Training
T=0 months Q’air #1 (Pre)
T=1 month Change Projects / Change
Specific Evaluations T=1-11
months
Q’air #2 (Post)
T=11 months
0 11

Department of Kinesiology - Biomechanics University of Waterloo, 2002
RESULTSRESULTS
Department of Kinesiology - Biomechanics University of Waterloo, 2002
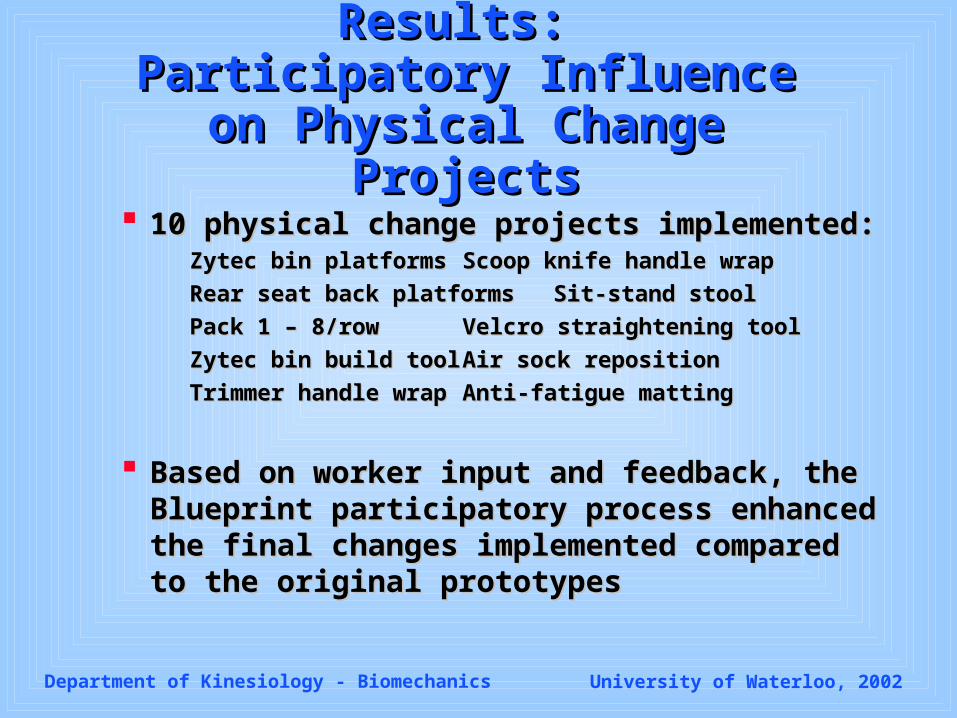
Results: Results: Participatory Influence on Participatory Influence on Physical Change ProjectsPhysical Change Projects
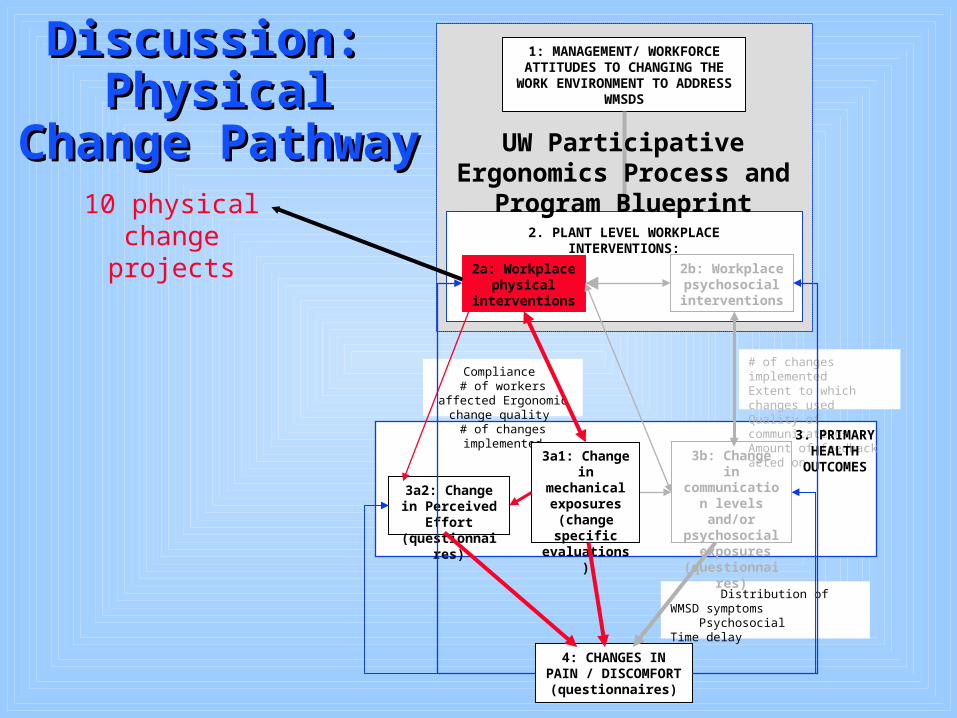
10 physical change projects implemented:10 physical change projects implemented:Zytec bin platformsZytec bin platforms Scoop knife handle wrapScoop knife handle wrap
Rear seat back platformsRear seat back platforms Sit-stand stoolSit-stand stool
Pack 1 – 8/rowPack 1 – 8/row Velcro straightening toolVelcro straightening tool
Zytec bin build toolZytec bin build tool Air sock repositionAir sock reposition
Trimmer handle wrapTrimmer handle wrap Anti-fatigue mattingAnti-fatigue matting
Based on worker input and feedback, the Based on worker input and feedback, the Blueprint participatory process enhanced the Blueprint participatory process enhanced the final changes implemented compared to the final changes implemented compared to the original prototypesoriginal prototypes
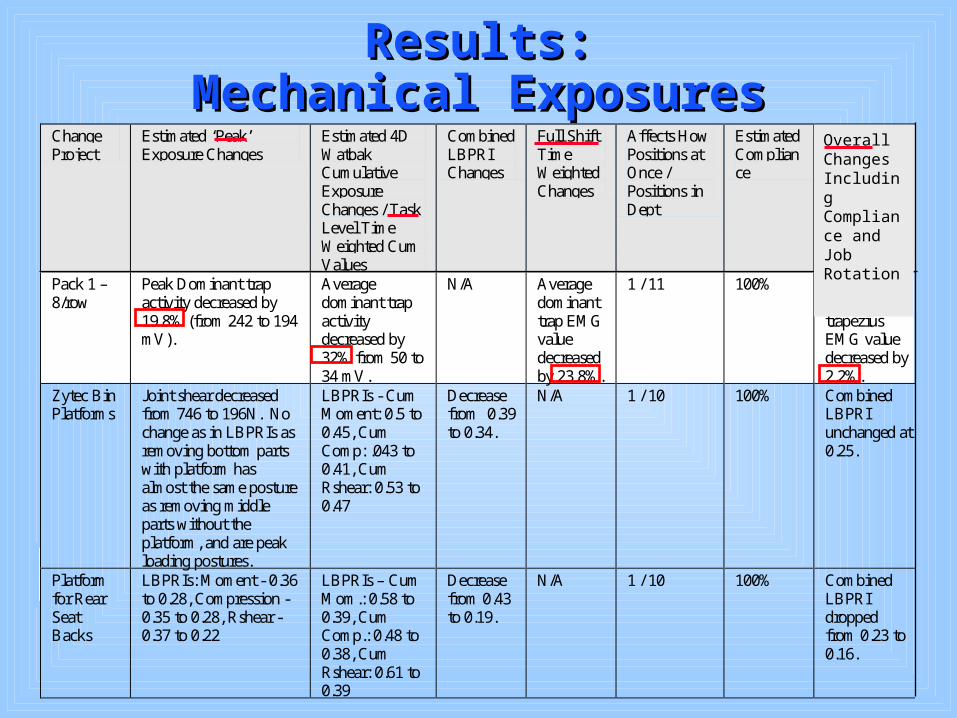
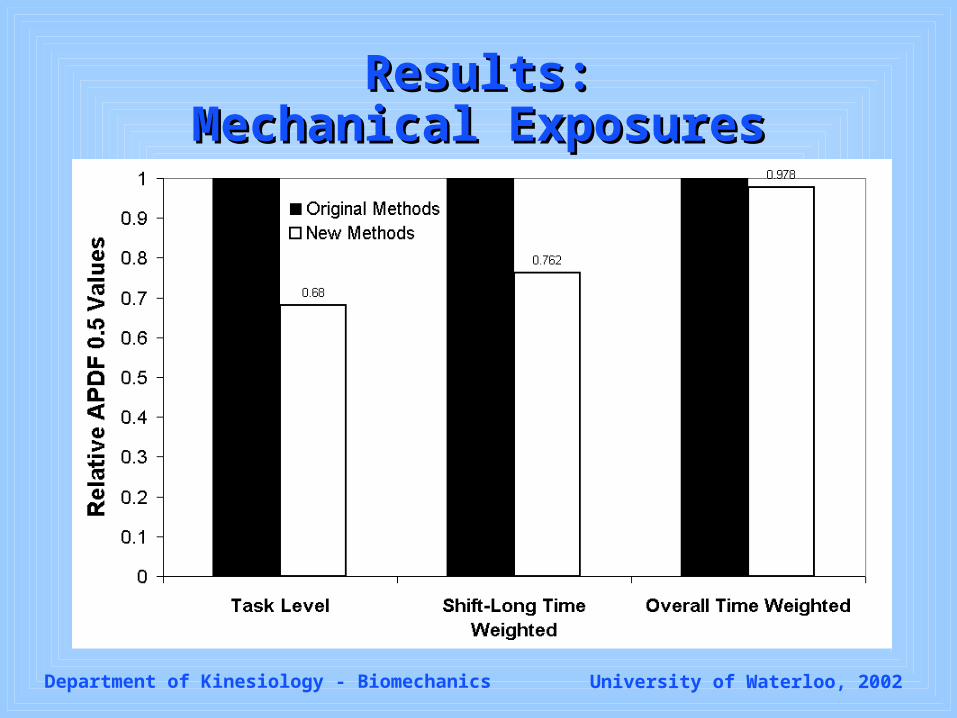
Results:Results:Mechanical ExposuresMechanical Exposures
Change Project
Estimated ‘Peak’ Exposure Changes
Estimated 4D Watbak Cumulative Exposure Changes / Task Level Time Weighted Cum Values
Combined LBPRI Changes
Full Shift Time Weighted Changes
Affects How Positions at Once / Positions in Dept
Estimated Compliance
Time Weighted Changes Considering Compliance and Job Rotation
Pack 1 – 8/row
Peak Dominant trap activity decreased by 19.8% (from 242 to 194 mV).
Average dominant trap activity decreased by 32% from 50 to 34 mV.
N/A Average dominant trap EMG value decreased by 23.8%.
1 / 11 100% APDF0.5 dominant trapezius EMG value decreased by 2.2%.
Zytec Bin Platforms
Joint shear decreased from 746 to 196N. No change as in LBPRIs as removing bottom parts with platform has almost the same posture as removing middle parts without the platform, and are peak loading postures.
LBPRIs - Cum Moment: 0.5 to 0.45, Cum Comp: .043 to 0.41, Cum Rshear: 0.53 to 0.47
Decrease from 0.39 to 0.34.
N/A 1 / 10 100% Combined LBPRI unchanged at 0.25.
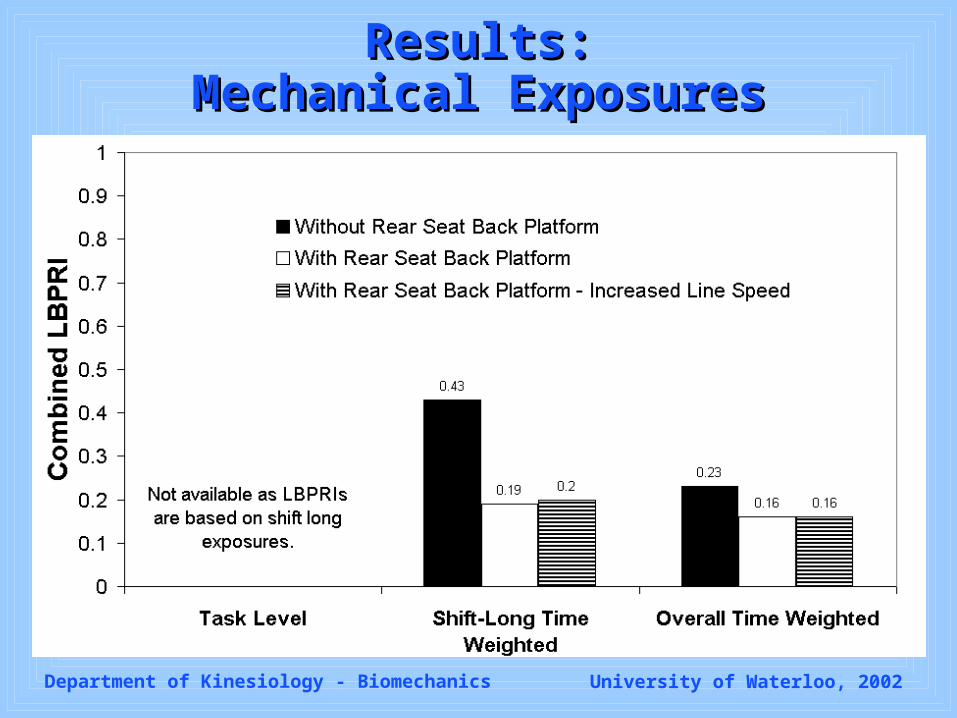
Platform for Rear Seat Backs
LBPRIs: Moment - 0.36 to 0.28, Compression - 0.35 to 0.28, Rshear - 0.37 to 0.22
LBPRIs – Cum Mom.: 0.58 to 0.39, Cum Comp.: 0.48 to 0.38, Cum Rshear: 0.61 to 0.39
Decrease from 0.43 to 0.19.
N/A 1 / 10 100% Combined LBPRI dropped from 0.23 to 0.16.
Overall Changes Including Compliance and Job Rotation
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Results:Results:Mechanical ExposuresMechanical Exposures
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Results:Results:Mechanical ExposuresMechanical Exposures
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Results:Results:Mechanical ExposuresMechanical Exposures
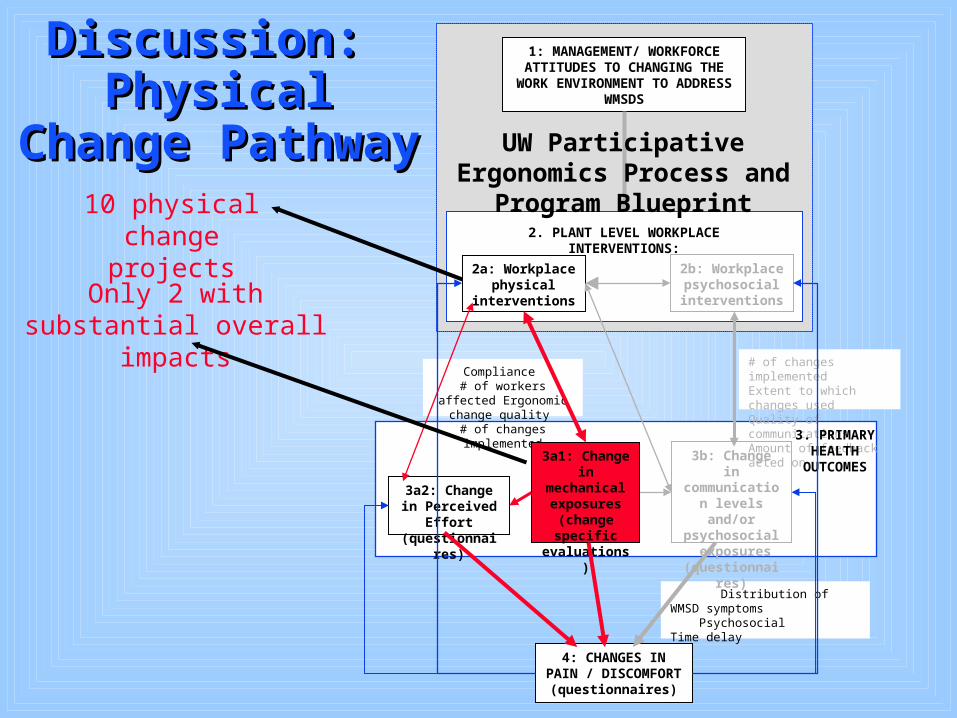
When evaluated at the task level, the When evaluated at the task level, the physical ergonomic changes physical ergonomic changes implemented were successful in implemented were successful in reducing physical demands. reducing physical demands.
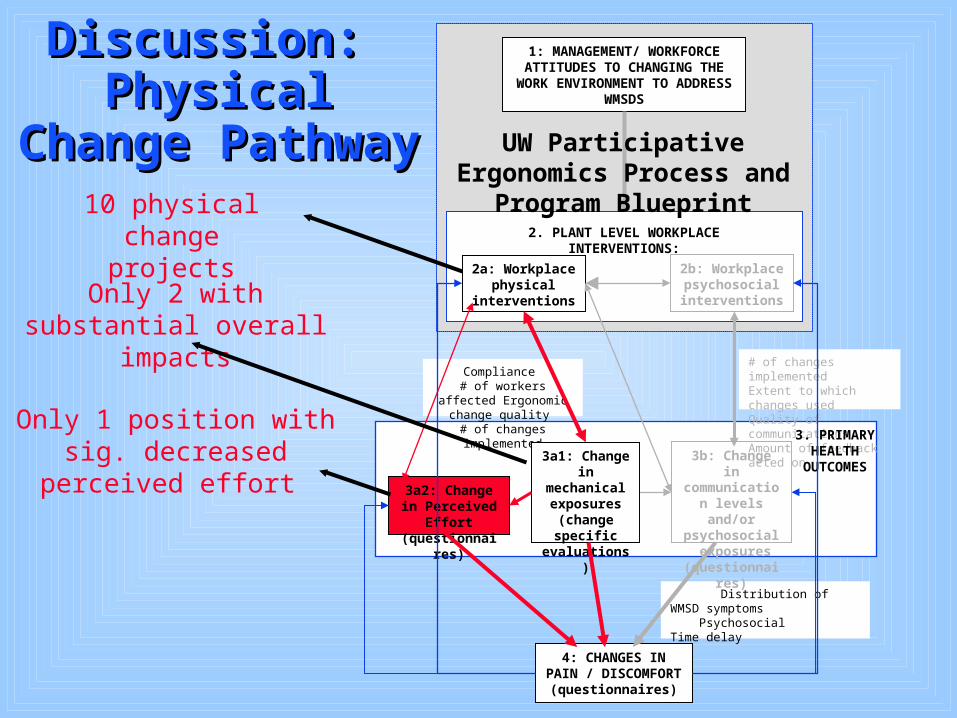
However, oHowever, overall calculations verall calculations (including compliance and job rotation (including compliance and job rotation schemes) showed only 2 changes with schemes) showed only 2 changes with substantial cumulative impacts.substantial cumulative impacts.
Department of Kinesiology - Biomechanics University of Waterloo, 2002
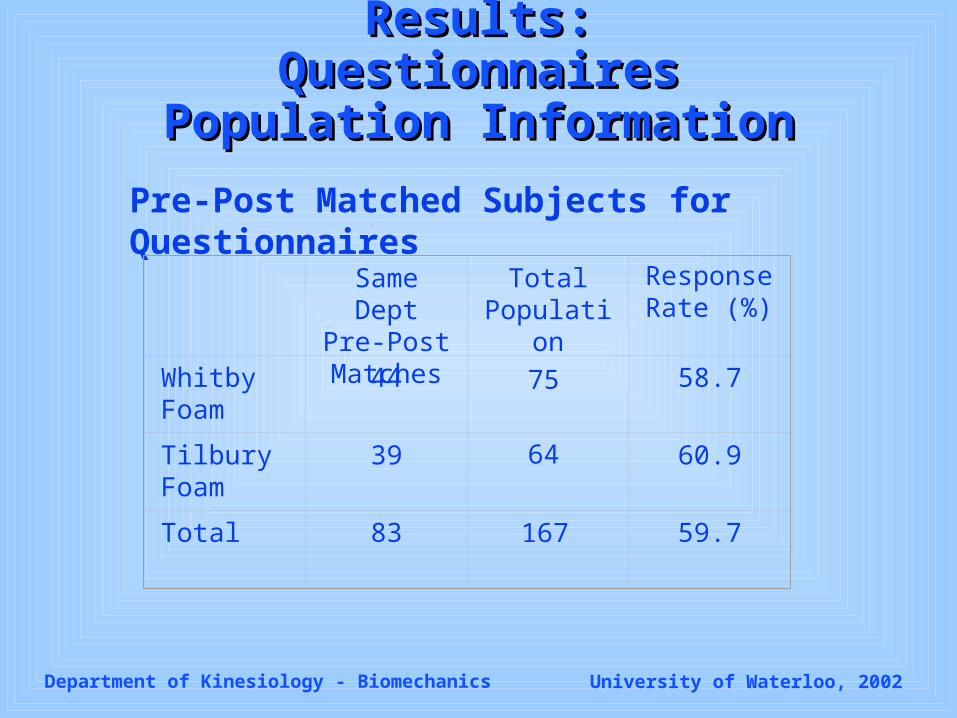
Results: QuestionnairesResults: QuestionnairesPopulation InformationPopulation Information
Pre-Post Matched Subjects for Questionnaires
Same Dept Pre-Post Matches
Total Population
Whitby Foam
44 58.7
Tilbury Foam
39 60.9
Total 83 59.7
75
64
167
Response Rate (%)
Department of Kinesiology - Biomechanics University of Waterloo, 2002
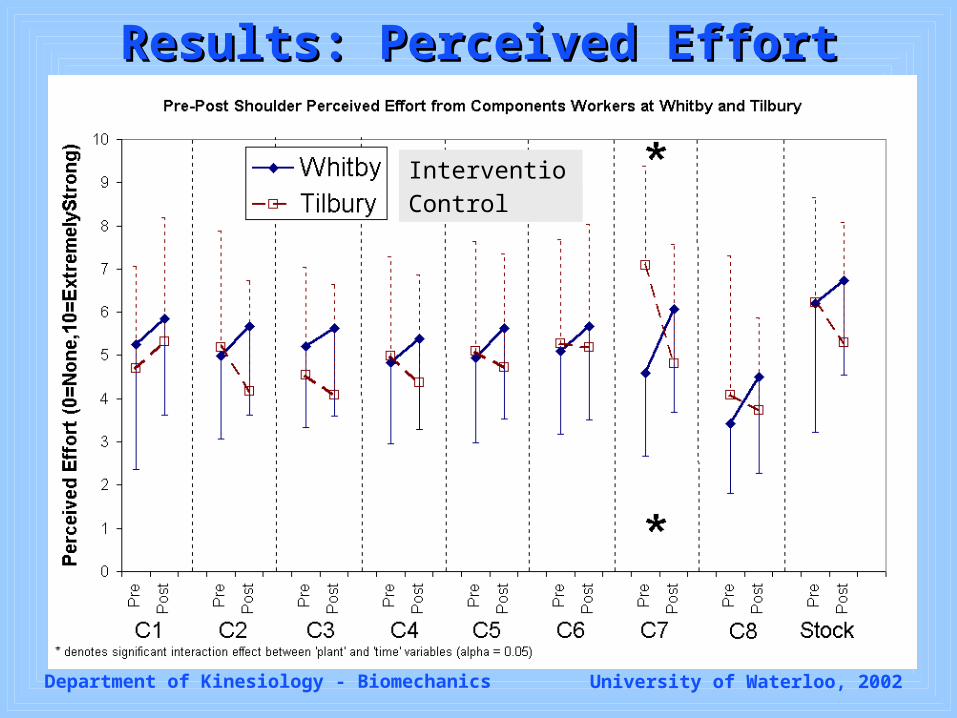
Results: Perceived EffortResults: Perceived Effort
Intervention
Control
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Results: Perceived EffortResults: Perceived Effort
4 body parts x 3 departments
Department of Kinesiology - Biomechanics University of Waterloo, 2002
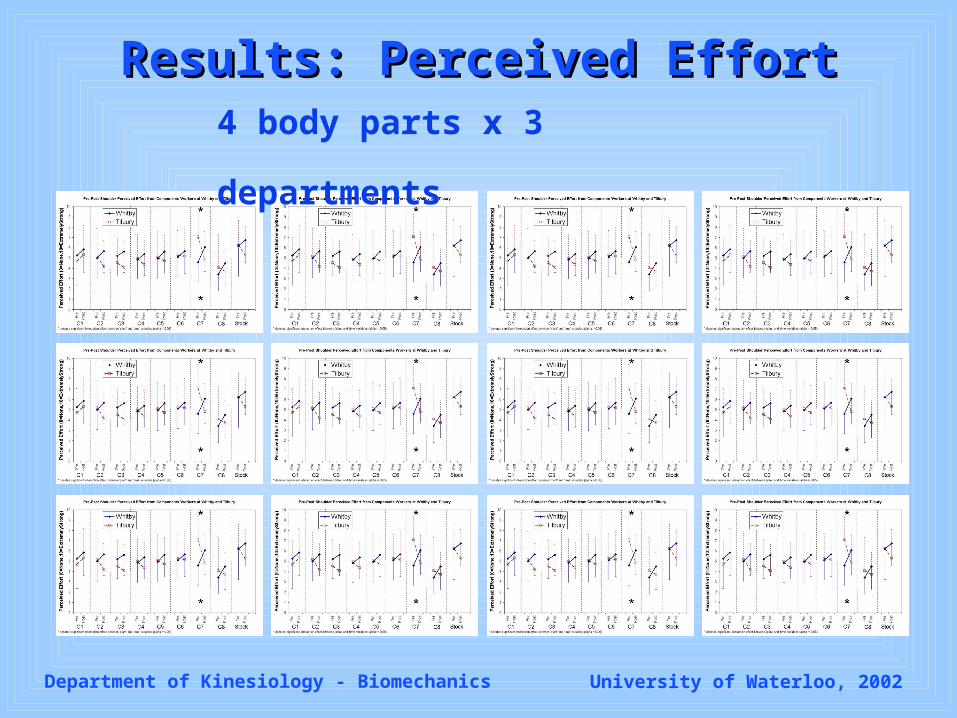
Results: Perceived EffortResults: Perceived Effort
4 body parts x 3 departments
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Results: Perceived EffortResults: Perceived Effort
No systematic changes in perceived No systematic changes in perceived effort at jobs where interventions effort at jobs where interventions were implemented.were implemented.
Department of Kinesiology - Biomechanics University of Waterloo, 2002
10 Psychosocial Elements introduced:User Trials One Minute Surveys
ECT Newsletter Suggestion Box
Bulletin Board Logo Contest
Shift Meetings Corporate Newspaper
ECT Meetings Steering Committee Meetings
Results: Psychosocial Results: Psychosocial InterventionsInterventions
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Results: Communication DynamicsResults: Communication Dynamics
Since completing the last ergonomics project questionnaire (June 2001): Since completing the last ergonomics project questionnaire (June 2001):
1.1. Overall communication between labour and management has been enhanced.Overall communication between labour and management has been enhanced.
2.2. Communication between you and your fellow workers has been enhanced.Communication between you and your fellow workers has been enhanced.
3.3. Communication about general ergonomic issues has been enhanced.Communication about general ergonomic issues has been enhanced.
4.4. Communication about specific ergonomic improvement projects has been Communication about specific ergonomic improvement projects has been enhanced.enhanced.
5.5. Your opinion regarding specific ergonomic projects has been directly asked Your opinion regarding specific ergonomic projects has been directly asked more often.more often.
6.6. You have been encouraged to express your opinions about ergonomic issues You have been encouraged to express your opinions about ergonomic issues more often.more often.
7.7. You have expressed your opinions regarding ergonomic issues more often.You have expressed your opinions regarding ergonomic issues more often.
Since completing the last ergonomics project questionnaire (June 2001):
1. Overall communication between labour and management has been enhanced.
2. Communication between you and your fellow workers has been enhanced.
3. Communication about general ergonomic issues has been enhanced.
4. Communication about specific ergonomic improvement projects has been enhanced.
5. Your opinion regarding specific ergonomic projects has been directly asked more often.
6. You have been encouraged to express your opinions about ergonomic issues more often.
7. You have expressed your opinions regarding ergonomic issues more often.
Since completing the last ergonomics project questionnaire (June 2001):
1. Overall communication between labour and management has been enhanced.
2. Communication between you and your fellow workers has been enhanced.
3. Communication about general ergonomic issues has been enhanced.
4. Communication about specific ergonomic improvement projects has been enhanced.
5. Your opinion regarding specific ergonomic projects has been directly asked more often.
6. You have been encouraged to express your opinions about ergonomic issues more often.
7. You have expressed your opinions regarding ergonomic issues more often.
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Results: Communication DynamicsResults: Communication Dynamics
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Results: Qualitative Observations Results: Qualitative Observations of Psychosocial Interventionsof Psychosocial Interventions
10 Psychosocial Elements introduced:User Trials One Minute Surveys
ECT Newsletter Suggestion Box
Bulletin Board Logo Contest
Shift Meetings Corporate Newspaper
ECT Meetings Steering Committee Meetings
Lack of Commitment to Participatory Process Observed
10 Psychosocial Elements introduced:User Trials One Minute Surveys
ECT Newsletter Suggestion Box
Bulletin Board Logo Contest
Shift Meetings Corporate Newspaper
ECT Meetings Steering Committee Meetings
Department of Kinesiology - Biomechanics University of Waterloo, 2002
10 Psychosocial Elements introduced:User Trials One Minute Surveys
ECT Newsletter Suggestion Box
Bulletin Board Logo Contest
Shift Meetings Corporate Newspaper
ECT Meetings Steering Committee Meetings
Lack of Commitment to Participatory Process Observed
Results: Qualitative Observations Results: Qualitative Observations of Psychosocial Interventionsof Psychosocial Interventions
Department of Kinesiology - Biomechanics University of Waterloo, 2002
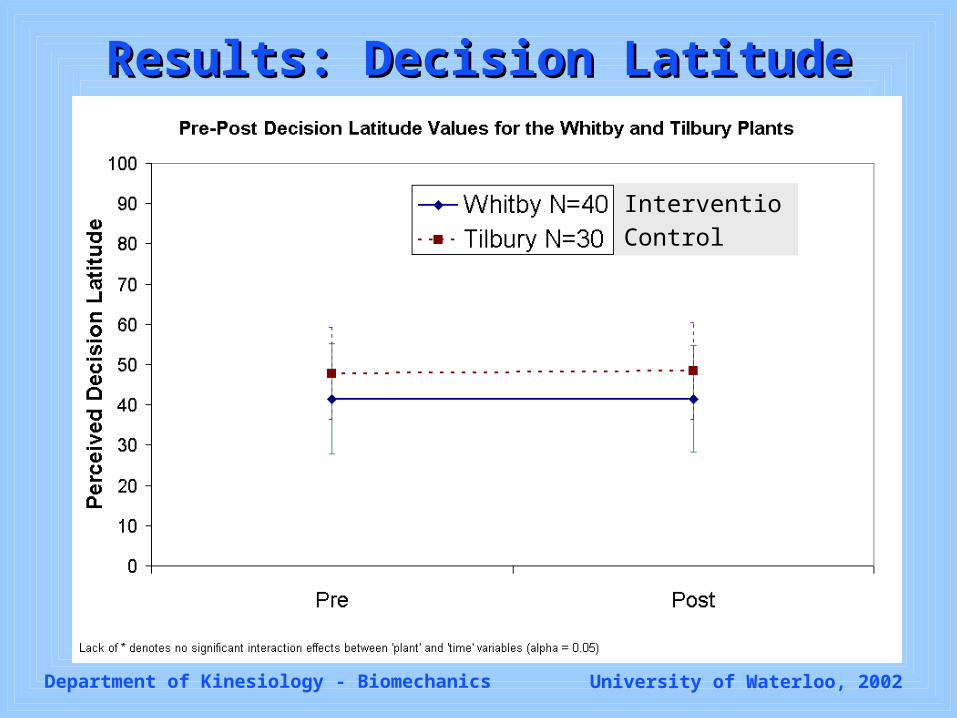
Results: Decision LatitudeResults: Decision Latitude
Intervention
Control
Department of Kinesiology - Biomechanics University of Waterloo, 2002
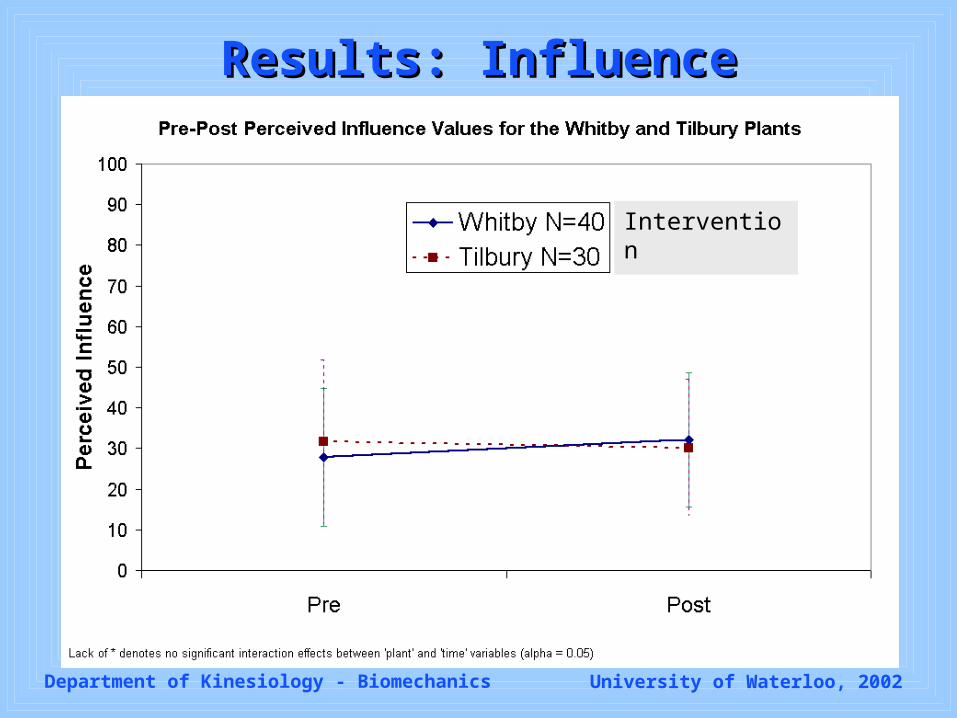
Results: InfluenceResults: Influence
Control
Intervention
Department of Kinesiology - Biomechanics University of Waterloo, 2002
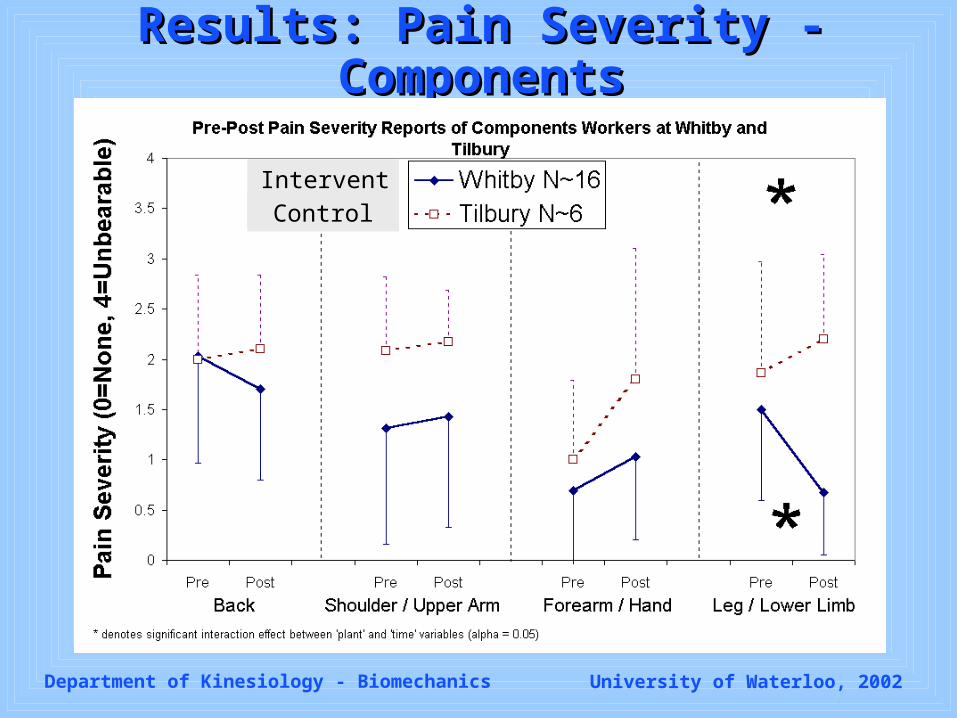
Results: Pain Severity - ComponentsResults: Pain Severity - Components
Intervention
Control
Department of Kinesiology - Biomechanics University of Waterloo, 2002
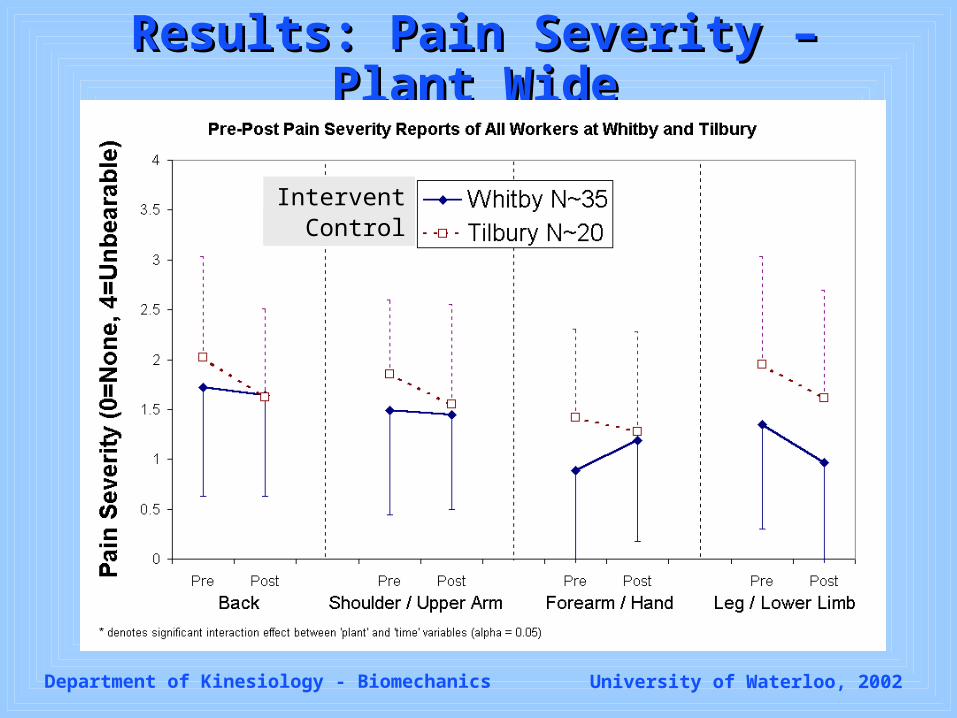
Results: Pain Severity – Plant WideResults: Pain Severity – Plant Wide
InterventionControl
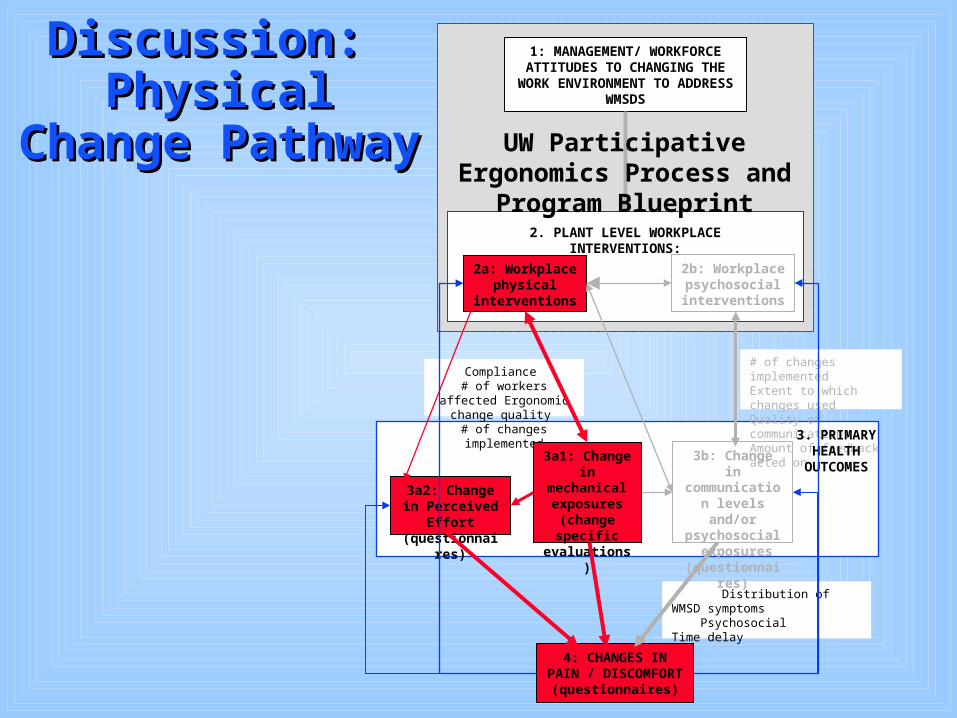
Discussion: Discussion: Physical Change Physical Change
PathwayPathway
Distribution of WMSD symptoms Psychosocial Time delay
4: CHANGES IN PAIN / DISCOMFORT
(questionnaires)
2a: Workplace physical
interventions
2. PLANT LEVEL WORKPLACE INTERVENTIONS:
2b: Workplace psychosocial interventions
3b: Change in communication
levels and/or psychosocial
exposures (questionnaires)
Compliance # of workers affected
Ergonomic change quality # of changes implemented
# of changes implementedExtent to which changes usedQuality of communicationsAmount of feedback acted on
3a1: Change in mechanical exposures (change specific
evaluations)
3a2: Change in Perceived Effort (questionnaires)
1: MANAGEMENT/ WORKFORCE ATTITUDES TO CHANGING THE
WORK ENVIRONMENT TO ADDRESS WMSDS
UW Participative Ergonomics Process and Program Blueprint
3. PRIMARY HEALTH
OUTCOMES
Discussion: Discussion: Physical Change Physical Change
PathwayPathway
Distribution of WMSD symptoms Psychosocial Time delay
4: CHANGES IN PAIN / DISCOMFORT
(questionnaires)
2a: Workplace physical
interventions
2. PLANT LEVEL WORKPLACE INTERVENTIONS:
2b: Workplace psychosocial interventions
3b: Change in communication
levels and/or psychosocial
exposures (questionnaires)
Compliance # of workers affected
Ergonomic change quality # of changes implemented
# of changes implementedExtent to which changes usedQuality of communicationsAmount of feedback acted on
3a1: Change in mechanical exposures (change specific
evaluations)
3a2: Change in Perceived Effort (questionnaires)
1: MANAGEMENT/ WORKFORCE ATTITUDES TO CHANGING THE
WORK ENVIRONMENT TO ADDRESS WMSDS
UW Participative Ergonomics Process and Program Blueprint
3. PRIMARY HEALTH
OUTCOMES
10 physical change projects
Discussion: Discussion: Physical Change Physical Change
PathwayPathway
Distribution of WMSD symptoms Psychosocial Time delay
4: CHANGES IN PAIN / DISCOMFORT
(questionnaires)
2a: Workplace physical
interventions
2. PLANT LEVEL WORKPLACE INTERVENTIONS:
2b: Workplace psychosocial interventions
3b: Change in communication
levels and/or psychosocial
exposures (questionnaires)
Compliance # of workers affected
Ergonomic change quality # of changes implemented
# of changes implementedExtent to which changes usedQuality of communicationsAmount of feedback acted on
3a1: Change in mechanical exposures (change specific
evaluations)
3a2: Change in Perceived Effort (questionnaires)
1: MANAGEMENT/ WORKFORCE ATTITUDES TO CHANGING THE
WORK ENVIRONMENT TO ADDRESS WMSDS
UW Participative Ergonomics Process and Program Blueprint
3. PRIMARY HEALTH
OUTCOMES
Only 2 with substantial overall impacts
10 physical change projects
Discussion: Discussion: Physical Change Physical Change
PathwayPathway
Distribution of WMSD symptoms Psychosocial Time delay
4: CHANGES IN PAIN / DISCOMFORT
(questionnaires)
2a: Workplace physical
interventions
2. PLANT LEVEL WORKPLACE INTERVENTIONS:
2b: Workplace psychosocial interventions
3b: Change in communication
levels and/or psychosocial
exposures (questionnaires)
Compliance # of workers affected
Ergonomic change quality # of changes implemented
# of changes implementedExtent to which changes usedQuality of communicationsAmount of feedback acted on
3a1: Change in mechanical exposures (change specific
evaluations)
3a2: Change in Perceived Effort (questionnaires)
1: MANAGEMENT/ WORKFORCE ATTITUDES TO CHANGING THE
WORK ENVIRONMENT TO ADDRESS WMSDS
UW Participative Ergonomics Process and Program Blueprint
3. PRIMARY HEALTH
OUTCOMES
Only 2 with substantial overall impacts
Only 1 position with sig. decreased perceived effort
10 physical change projects
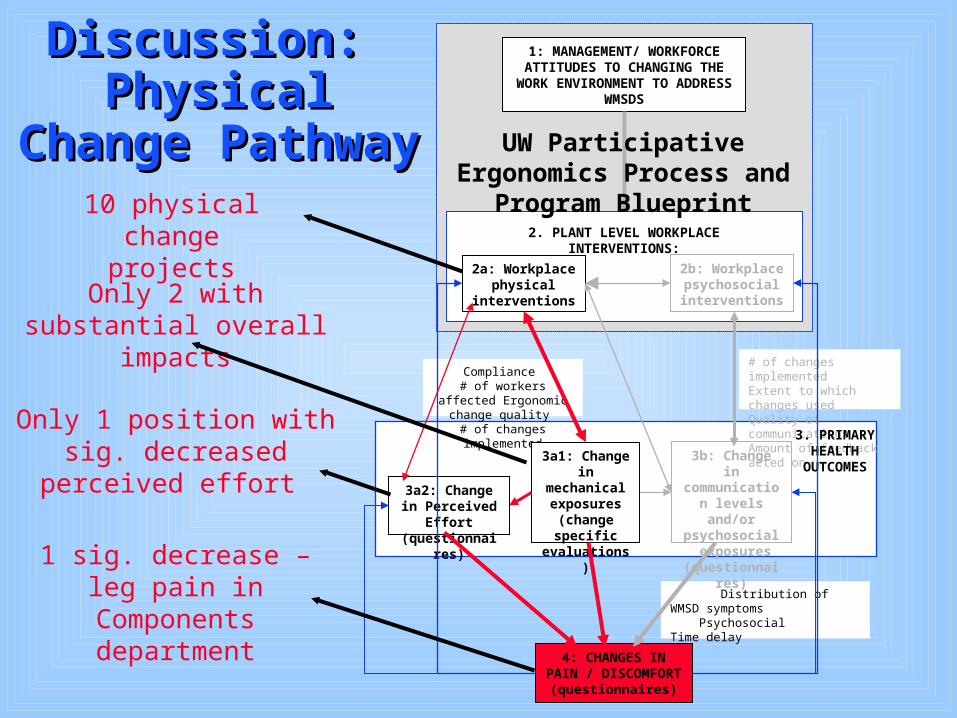
Discussion: Discussion: Physical Change Physical Change
PathwayPathway
Distribution of WMSD symptoms Psychosocial Time delay
4: CHANGES IN PAIN / DISCOMFORT
(questionnaires)
2a: Workplace physical
interventions
2. PLANT LEVEL WORKPLACE INTERVENTIONS:
2b: Workplace psychosocial interventions
3b: Change in communication
levels and/or psychosocial
exposures (questionnaires)
Compliance # of workers affected
Ergonomic change quality # of changes implemented
# of changes implementedExtent to which changes usedQuality of communicationsAmount of feedback acted on
3a1: Change in mechanical exposures (change specific
evaluations)
3a2: Change in Perceived Effort (questionnaires)
1: MANAGEMENT/ WORKFORCE ATTITUDES TO CHANGING THE
WORK ENVIRONMENT TO ADDRESS WMSDS
UW Participative Ergonomics Process and Program Blueprint
3. PRIMARY HEALTH
OUTCOMES
Only 2 with substantial overall impacts
Only 1 position with sig. decreased perceived effort
1 sig. decrease – leg pain in Components department
10 physical change projects
Department of Kinesiology - Biomechanics University of Waterloo, 2002
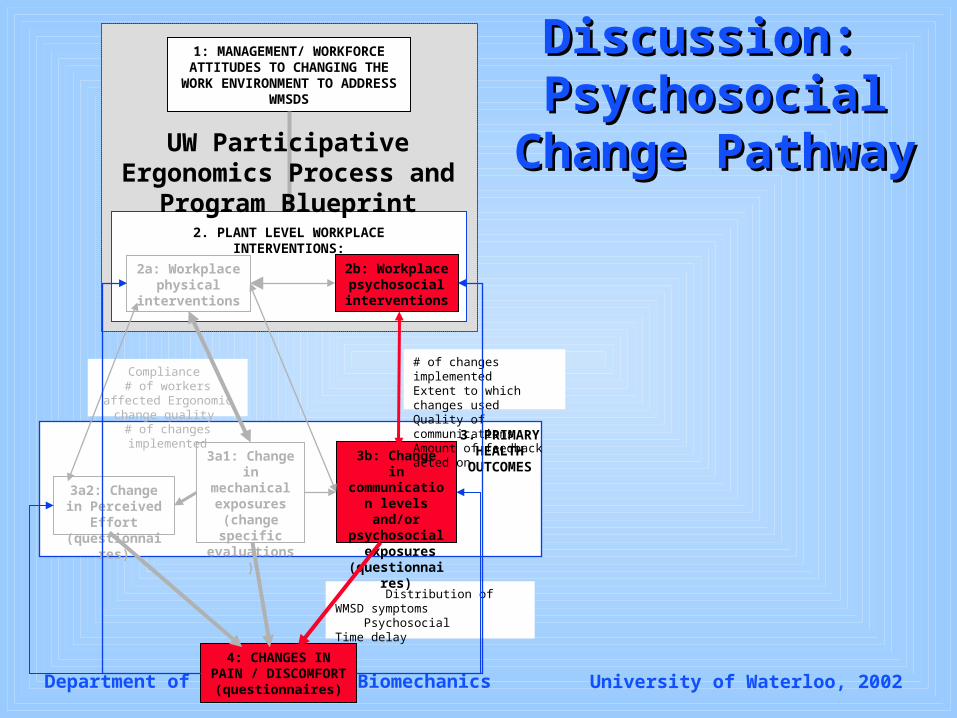
Discussion: Discussion: Psychosocial Psychosocial
Change PathwayChange Pathway
Distribution of WMSD symptoms Psychosocial Time delay
4: CHANGES IN PAIN / DISCOMFORT
(questionnaires)
2a: Workplace physical
interventions
2. PLANT LEVEL WORKPLACE INTERVENTIONS:
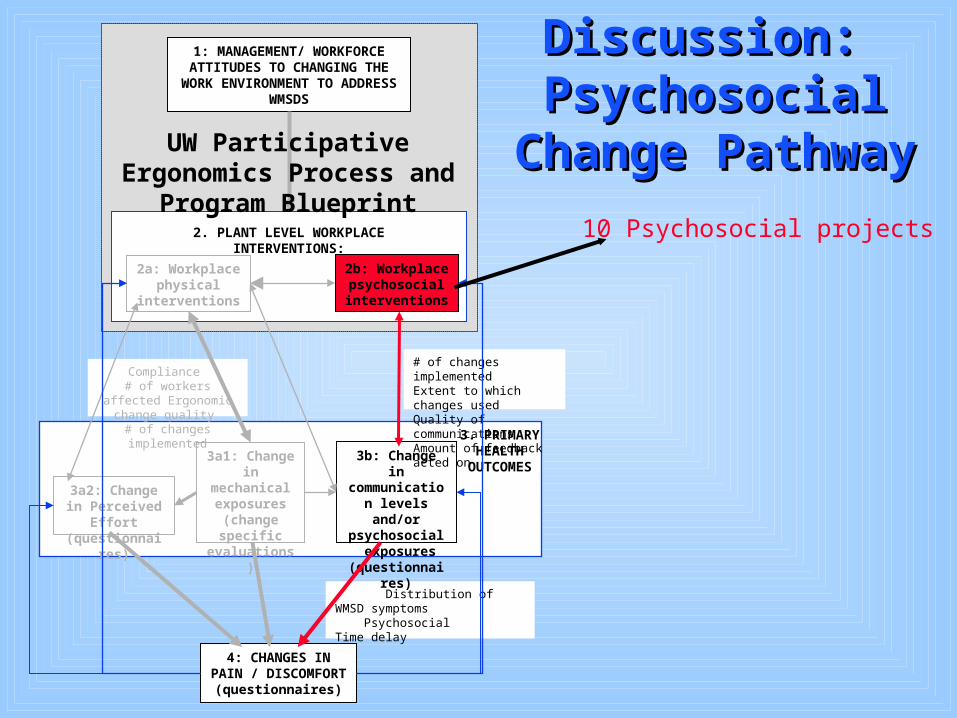
2b: Workplace psychosocial interventions
3b: Change in communication
levels and/or psychosocial
exposures (questionnaires)
Compliance # of workers affected
Ergonomic change quality # of changes implemented
# of changes implementedExtent to which changes usedQuality of communicationsAmount of feedback acted on
3a1: Change in mechanical exposures (change specific
evaluations)
3a2: Change in Perceived Effort (questionnaires)
1: MANAGEMENT/ WORKFORCE ATTITUDES TO CHANGING THE
WORK ENVIRONMENT TO ADDRESS WMSDS
UW Participative Ergonomics Process and Program Blueprint
3. PRIMARY HEALTH
OUTCOMES
Discussion: Discussion: Psychosocial Psychosocial
Change PathwayChange Pathway
Distribution of WMSD symptoms Psychosocial Time delay
4: CHANGES IN PAIN / DISCOMFORT
(questionnaires)
2a: Workplace physical
interventions
2. PLANT LEVEL WORKPLACE INTERVENTIONS:
2b: Workplace psychosocial interventions
3b: Change in communication
levels and/or psychosocial
exposures (questionnaires)
Compliance # of workers affected
Ergonomic change quality # of changes implemented
# of changes implementedExtent to which changes usedQuality of communicationsAmount of feedback acted on
3a1: Change in mechanical exposures (change specific
evaluations)
3a2: Change in Perceived Effort (questionnaires)
1: MANAGEMENT/ WORKFORCE ATTITUDES TO CHANGING THE
WORK ENVIRONMENT TO ADDRESS WMSDS
UW Participative Ergonomics Process and Program Blueprint
3. PRIMARY HEALTH
OUTCOMES
10 Psychosocial projects
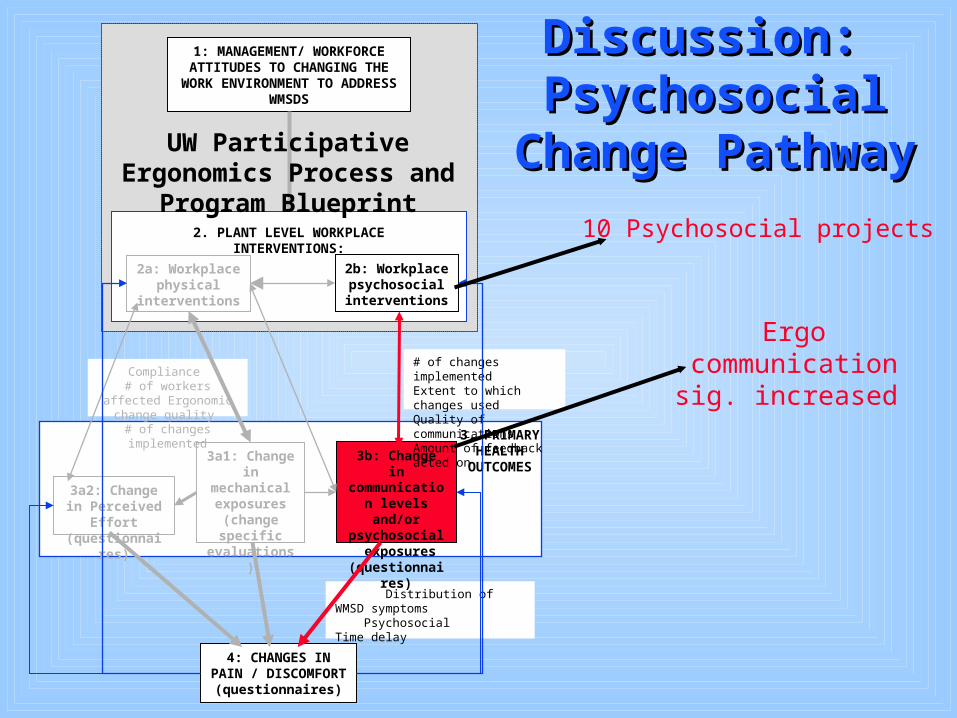
Discussion: Discussion: Psychosocial Psychosocial
Change PathwayChange Pathway
Distribution of WMSD symptoms Psychosocial Time delay
4: CHANGES IN PAIN / DISCOMFORT
(questionnaires)
2a: Workplace physical
interventions
2. PLANT LEVEL WORKPLACE INTERVENTIONS:
2b: Workplace psychosocial interventions
3b: Change in communication
levels and/or psychosocial
exposures (questionnaires)
Compliance # of workers affected
Ergonomic change quality # of changes implemented
# of changes implementedExtent to which changes usedQuality of communicationsAmount of feedback acted on
3a1: Change in mechanical exposures (change specific
evaluations)
3a2: Change in Perceived Effort (questionnaires)
1: MANAGEMENT/ WORKFORCE ATTITUDES TO CHANGING THE
WORK ENVIRONMENT TO ADDRESS WMSDS
UW Participative Ergonomics Process and Program Blueprint
3. PRIMARY HEALTH
OUTCOMES
10 Psychosocial projects
Ergo communication sig. increased
Discussion: Discussion: Psychosocial Psychosocial
Change PathwayChange Pathway
Distribution of WMSD symptoms Psychosocial Time delay
4: CHANGES IN PAIN / DISCOMFORT
(questionnaires)
2a: Workplace physical
interventions
2. PLANT LEVEL WORKPLACE INTERVENTIONS:
2b: Workplace psychosocial interventions
3b: Change in communication
levels and/or psychosocial
exposures (questionnaires)
Compliance # of workers affected
Ergonomic change quality # of changes implemented
# of changes implementedExtent to which changes usedQuality of communicationsAmount of feedback acted on
3a1: Change in mechanical exposures (change specific
evaluations)
3a2: Change in Perceived Effort (questionnaires)
1: MANAGEMENT/ WORKFORCE ATTITUDES TO CHANGING THE
WORK ENVIRONMENT TO ADDRESS WMSDS
UW Participative Ergonomics Process and Program Blueprint
3. PRIMARY HEALTH
OUTCOMES
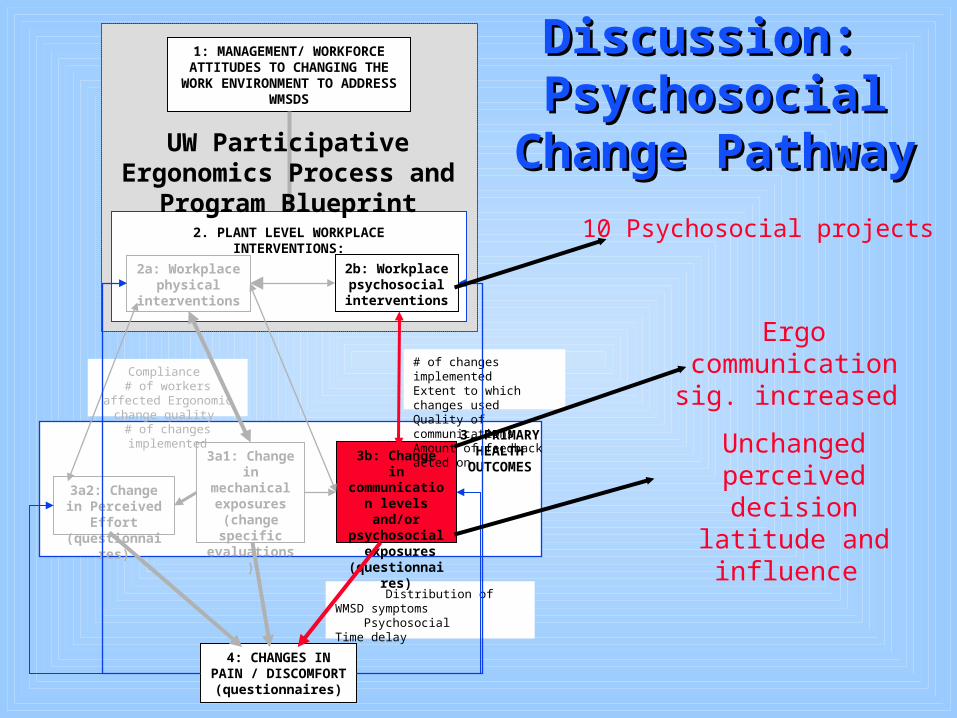
10 Psychosocial projects
Ergo communication sig. increased
Unchanged perceived decision latitude and
influence
Discussion: Discussion: Psychosocial Psychosocial
Change PathwayChange Pathway
Distribution of WMSD symptoms Psychosocial Time delay
4: CHANGES IN PAIN / DISCOMFORT
(questionnaires)
2a: Workplace physical
interventions
2. PLANT LEVEL WORKPLACE INTERVENTIONS:
2b: Workplace psychosocial interventions
3b: Change in communication
levels and/or psychosocial
exposures (questionnaires)
Compliance # of workers affected
Ergonomic change quality # of changes implemented
# of changes implementedExtent to which changes usedQuality of communicationsAmount of feedback acted on
3a1: Change in mechanical exposures (change specific
evaluations)
3a2: Change in Perceived Effort (questionnaires)
1: MANAGEMENT/ WORKFORCE ATTITUDES TO CHANGING THE
WORK ENVIRONMENT TO ADDRESS WMSDS
UW Participative Ergonomics Process and Program Blueprint
3. PRIMARY HEALTH
OUTCOMES
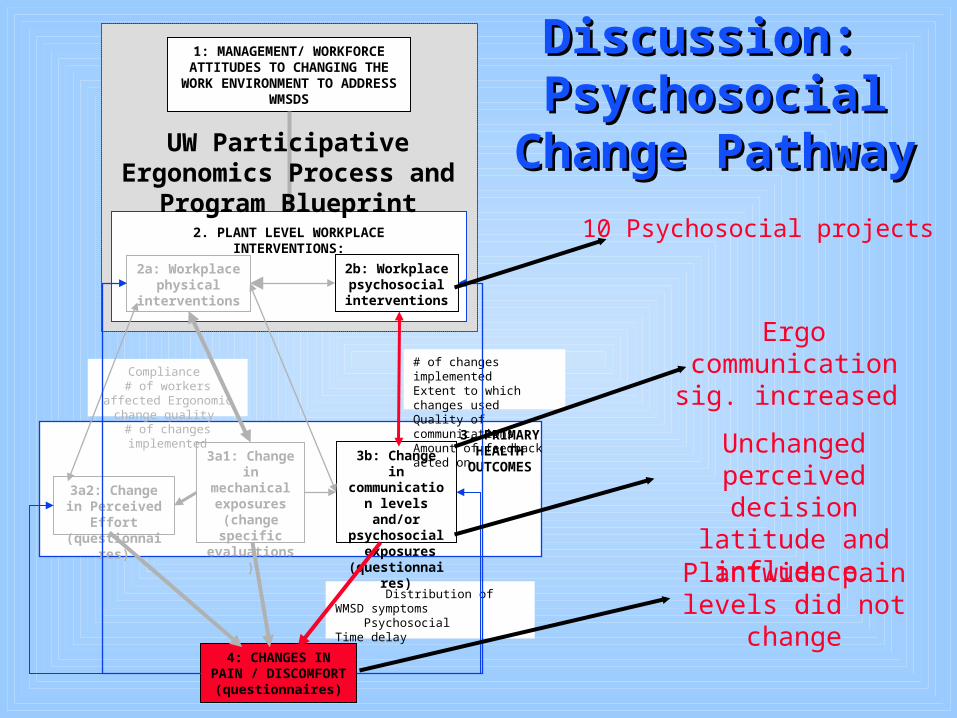
10 Psychosocial projects
Ergo communication sig. increased
Unchanged perceived decision latitude and
influence
Plantwide pain levels did not change
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Potential Confounders:Potential Confounders:
Differential Study Site Experiences
Line speed changesNew plant managersContract negotiations
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Conclusions:Conclusions: The Blueprint participatory model enhanced The Blueprint participatory model enhanced
the quality and impact of each of the final the quality and impact of each of the final physical change projects.physical change projects.
The Intervention Outcome Pathway model was The Intervention Outcome Pathway model was helpful in interpreting the results, and in helpful in interpreting the results, and in performing diagnostic evaluations of the performing diagnostic evaluations of the different elements involved in the different elements involved in the
ergonomic ergonomic intervention. intervention.
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Conclusions:Conclusions:
Peak and task-level cumulative exposures were Peak and task-level cumulative exposures were decreased by each of the 10 change projects. decreased by each of the 10 change projects.
However, when shift long job demands and job However, when shift long job demands and job rotation schedules were considered, the rotation schedules were considered, the cumulative impacts were sufficient to reduce cumulative impacts were sufficient to reduce overall mechanical exposures for only two overall mechanical exposures for only two changes.changes.
Perceived Effort did not systematically changePerceived Effort did not systematically change This might, in part, explain the decreased pain This might, in part, explain the decreased pain
severity values in only one department.severity values in only one department.
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Conclusions:Conclusions: The participatory ergonomics intervention The participatory ergonomics intervention
resulted in enhanced communication dynamics resulted in enhanced communication dynamics regarding ergonomic issues. regarding ergonomic issues.
Lack of commitment lead to lack of Lack of commitment lead to lack of significant change in perceived Decision significant change in perceived Decision Latitude and Influence.Latitude and Influence.
This, in part, explains the lack of changes in This, in part, explains the lack of changes in plant-wide Pain Severity levels.plant-wide Pain Severity levels.
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Recommendations:Recommendations:
Additional research should be performed Additional research should be performed to determine: to determine: • the mechanical exposure changes necessary the mechanical exposure changes necessary
to reduce pain severity levels, to reduce pain severity levels, • the intensity of psychosocial interventions the intensity of psychosocial interventions
necessary to alter perceived decision latitude necessary to alter perceived decision latitude and influence levels, andand influence levels, and
• the magnitude of psychosocial risk factor the magnitude of psychosocial risk factor changes necessary to influence pain severity changes necessary to influence pain severity levels,levels,
• The success of the participatory process in The success of the participatory process in other worksites.other worksites.
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Recommendations:Recommendations:
The Ergonomics Change Team evaluated The Ergonomics Change Team evaluated in this study should:in this study should:• be encouraged to commit to the participatory be encouraged to commit to the participatory
change process, andchange process, and
• continue to implement physical and continue to implement physical and psychosocial ergonomic changes in hopes psychosocial ergonomic changes in hopes that additional interventions will involve that additional interventions will involve enough cumulative benefits to influence enough cumulative benefits to influence primary indicators of health. primary indicators of health.
Department of Kinesiology - Biomechanics University of Waterloo, 2002
Recommendations:Recommendations:
To enhance chances of improved indicators To enhance chances of improved indicators of health, a corporate ergonomist should be of health, a corporate ergonomist should be involved to direct the team’s efforts.involved to direct the team’s efforts.
Department of Kinesiology - Biomechanics University of Waterloo, 2002
THANK YOUTHANK YOU
“You can buy people’s time, you can buy their physical presence at a given place, you can even buy a measured number of their skilled muscular motions per hour.
But you cannot buy loyalty, you cannot buy the devotion of hearts, minds, or souls. You
must earn them.”
- in Saari, 1989