Dento-alveolar Infections - Minia
54
Dento-alveolar Infections Ass. Prof. Dr/ Hamed Gad
Transcript of Dento-alveolar Infections - Minia
Dento-alveolar
Infections Ass. Prof. Dr/ Hamed Gad

Fascial spaces
Fascial spaces are fascia-lined areas
that can be eroded or distended by
purulent exudates.

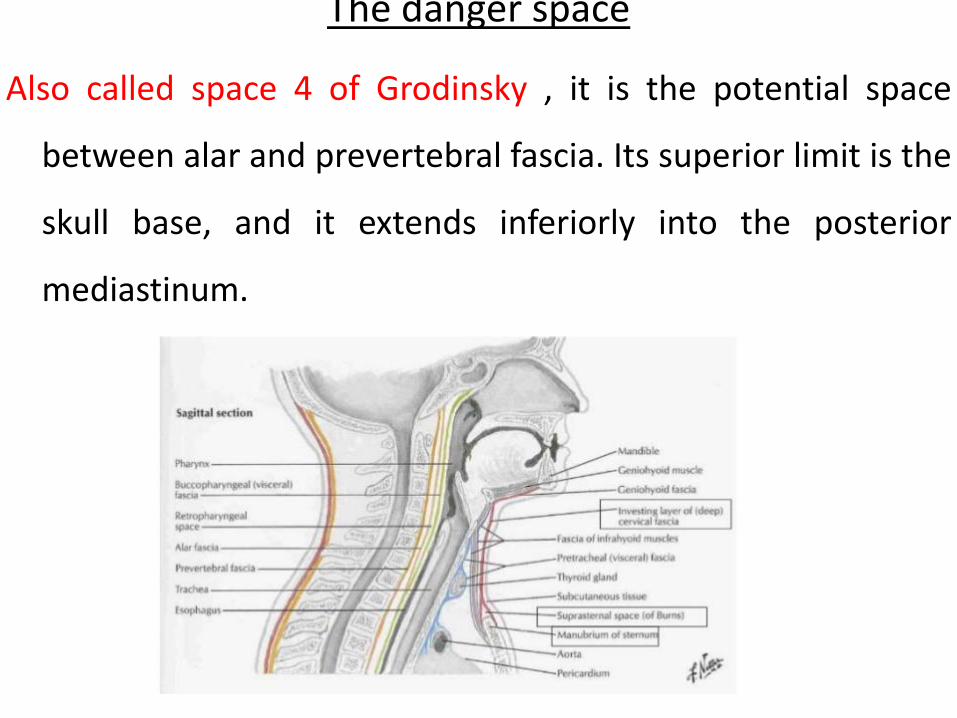
The danger space
Also called space 4 of Grodinsky , it is the potential space
between alar and prevertebral fascia. Its superior limit is the
skull base, and it extends inferiorly into the posterior
mediastinum.

Superficial layer Middle layer Deep layer







What are the primary fascial spaces?
• • Buccal
• • Submandibular
• • Canine
• • Submental
• • Sublingual
• • Vestibul

What are the secondary fascial spaces?
• • Pterygomandibular
• • Superficial and deep temporal
• • Retropharyngeal
• • Masticator
• • Lateral pharyngeal
• • Prevertebral

principles of management of
fascial space infections(ADAA) of
late stage

TREATMENT of INFECTION
• Remove the cause of infection is the most
important of all, by either spontaneously or
surgically drain the pus.
• Antibiotics are merely an adjunctive therapy.

The following factors should be taken into
consideration for management of odontogenic
infections
Stage I 1. Determine the severity of infection.
2. Evaluate host defenses.
3. Indications for hospitalization.
Stage II 4. Treat surgically.
5. Support medically.
6. Choose and prescribe antibiotic therapy.
Stage III
7-. Evaluate the patient frequently.

Following factors should be taken into consideration
for management of odontogenic infections
Stage I- Diagnosis 1. Determine the severity of infection.
2. Evaluate host defenses.
3. Indications for hospitalization.
Following factors should be taken into consideration
for management of odontogenic infections
Stage II- Treatment planning &intervention
4. Surgical intervention (incision &drainage I&D) (decompression)
5. Support medically.
6. principle for antibiotic therapy & prescription.

Following factors should be taken into consideration
for management of odontogenic infections
Stage III- Follow up
7. Evaluate the patient frequently.

A- Determining the severity of
infection
1. Anatomic location.
2. Rate of progression.
3. Airway compromise.

B- Evaluate host defenses.
1. Age
2. Disease related
3. Defective immune system related
4. Drug related

PHYSIOLOGICAL
Relates primarily to the patients inability to deliver the defending agents such as white blood cells, antibodies etc. at the site of Invasion.
For e.g.
- Shock
- Fluid imbalances
- Advanced age

DISEASE RELATED
- Malnutrition syndrome, often as a result of
Chronic alcoholism
- Poorly controlled diabetes
- Patient’s with malignancy & leukemia’s are
more likely to be infected.

DEFECTIVE IMMUNE SYSTEM
RELATED
- A.I.D.S.
- Multiple myeloma
- Whole body radiation
- Congenital defects such as agammaglobulinemia
- Patients with these conditions may be unable to fight
successfully against invading bacteria.

DRUG RELATED
- Cytotoxic drugs : patients may have increased susceptibility to infections for upto 1 yr after the course of cancericidal drugs
- Immunosuppressive drugs :
- glucocorticoids
- azathioprine
- cyclosporine
- steroids

C- indications for hospitalization 1. Temperature > (38.3°C)
2. Threat to the airway or vital structures
3. Infection in high severity anatomic
spaces
4. Need for general anesthesia
5. Need for inpatient control of systemic
disease

II D- surgical intervention
• Extraction or extirpation of the necrotic tooth
pulp
• Soft tissue incision surgical drainage (I&D)
Hilton’s method

Objective of surgical drainage
1. Drain pus from tissue spaces
2. Relives tissue pressure.
3. increase vascular flow.

Principles of I&D
• Timing of I&D:
1) Fluctuation test
2) Erythamatous hallo
3) Pitting on pressure
4) Pus aspiration

Guidelines for placement of incisions in infected cases: 1. Incisions should be placed in the most dependent areas.
2. Incisions should be parallel to the skin creases.
3. Incisions should lie in an esthetically acceptable site as far as possible.
4. Incisions should be supported by healthy underlying dermis and subcutaneous tissue.
5. Incisions placed intraorally, should not cross frenal attachments, and should be placed parallel to nerve fibers in the region of mental nerve.
6. The removal of the cause; such as an infected tooth, a segment of necrotic bone, a foreign body, if not already done, then should be done at the time of incision and drainage procedure.



Principles of I&D
• Timing of I&D:
Fluctuation test Erythamatous hallo Pitting on pressure Pus aspiration

Principles of I&D
• Pre-operative antibiotic prophylaxis
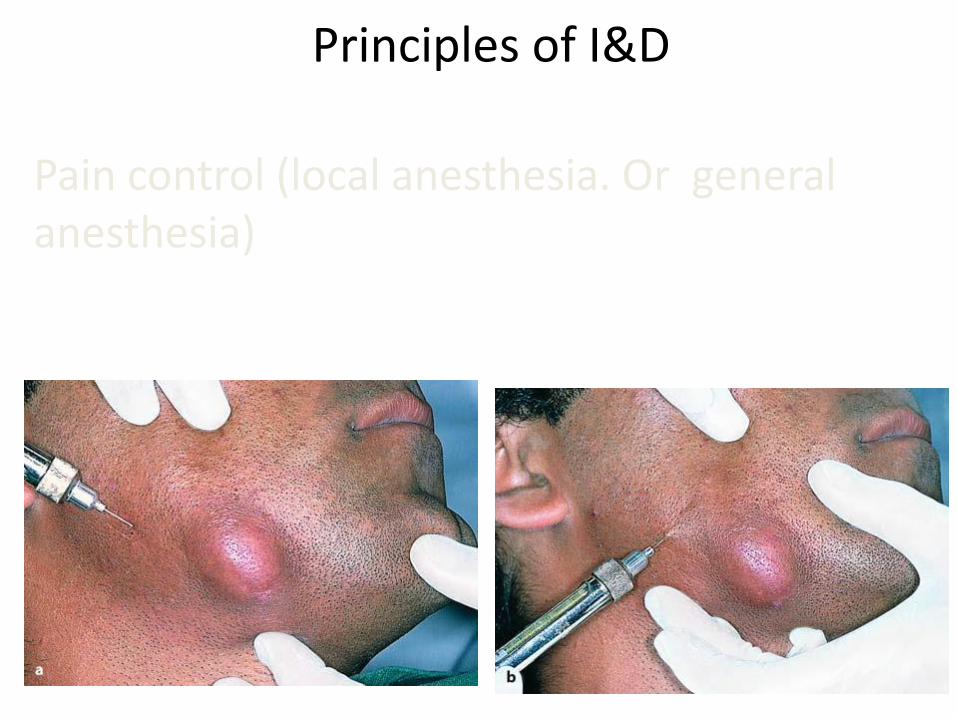
Principles of I&D
Pain control (local anesthesia. Or general anesthesia)

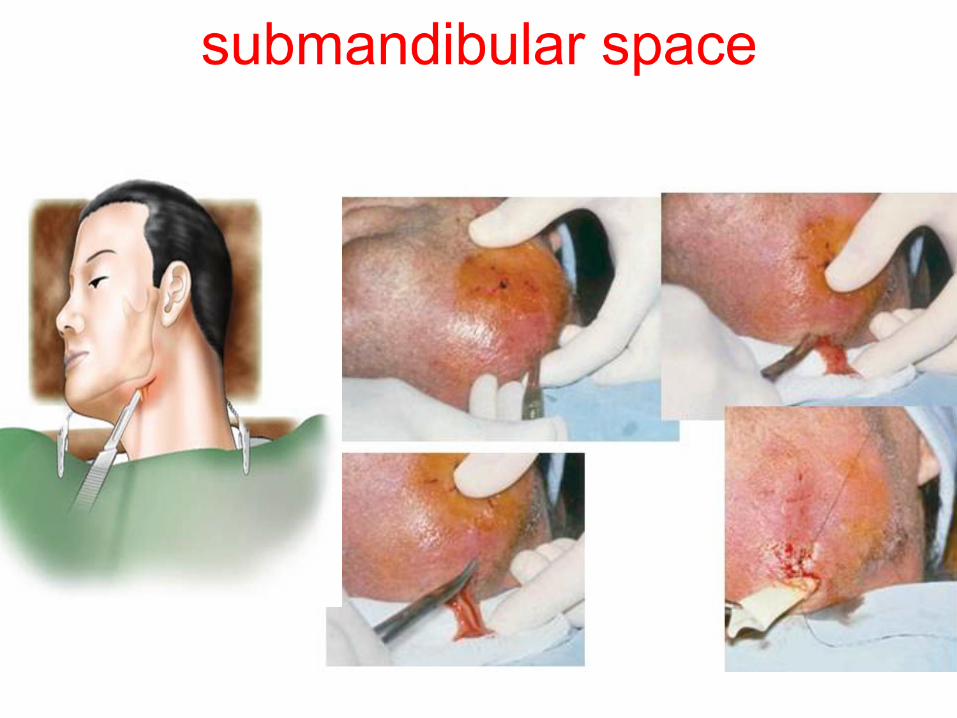
Principles of I&D (sharp incision)

Pus evacuation and continuous drainage

Drainage, Pus evacuation and continuous drainage

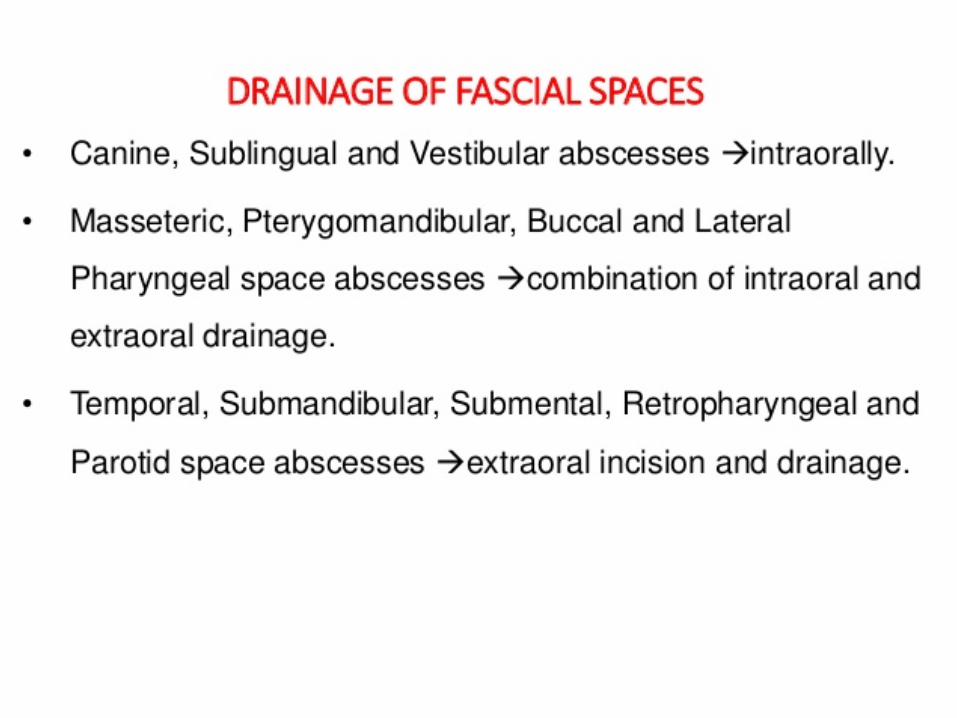
I&D of fascial spaces

• Abscess of Base of
Upper Lip



Buccal Space infection

Submental Abscess

Sublingual Abscess

E-Support medically. 1. Hydration Daily sensible fluid loss, consisting primarily of sweat, is increased by 250 mL per degree of fever.
Insensible fluid loss, consisting mainly of evaporation from lungs and skin, is increased by 50 to 75 mL per degree of fever per day.
2- Nutrition Fever also increases metabolic demand by 5 to 8% per degree of fever per day. Therefore, it may be necessary to
supplement the infected patient’s oral intake
3-Control of fever

Fever below 103°F (39.4°C) is probably beneficial.
Above 103°F, however, fever can become destructive
by increasing metabolic and cardiovascular demands
beyond physiologic reserve capacity.
Daily sensible fluid loss, consisting primarily of sweat,
is increased by 250 mL per degree of fever.
Insensible fluid loss, consisting mainly of evaporation
from lungs and skin, is increased by 50 to 75 mL per
degree of fever per day.

Fever also increases metabolic demand by 5 to
8% per degree of fever per day. Therefore, it
may be necessary to supplement the infected
patient’s oral intake

F- Proper principles for antibiotic
therapy 1. Identification of causative organism
2. Determination of antibiotic sensitivity
3. Use of narrow spectrum antibiotic
4. Use of least toxic antibiotic
5. Patient drug history
6. Use of bactericidal rather than bacteriostatic antibiotic
7. Proper dosage
8. Proper time interval
9. Cost of antibiotic

USE OF NARROW SPECTRUM
ANTIBIOTICS
When a broad spectrum antibiotic is used,
many different bacteria, present in body are
exposed to antibiotic.
However if narrow spectrum antibiotic is
used fewer organisms have opportunity to
become resistant as they are not even
partially sensitive

THANK YOU
THANK YOU