Demonstration of rapid light-induced advances and delays ...
11
Demonstration of rapid light-induced advances and delays of the human circadian clock using hormonal phase markers EVE VAN CAUTER, JEPPE STURIS, MARIA M. BYRNE, JOHN D. BLACKMAN, RACHEL LEPROULT, GILAD OFEK, MIREILLE L’HERMITE-BALERIAUX, SAMUEL REFETOFF, FRED W. TUREK, AND OLIVIER VAN REETH Center for the Study of Biological Rhythms, Universite’ Libre de Bruxelles, B-1070 Brussels Belgium; Department of Neurobiology and Physiology, Northwestern University, Evanston 60208; and Department of Medicine, University of Chicago, Chicago, Illinois 60637. Van Cauter, Eve, Jeppe Sturis, Maria M. Byrne, John D. Blackman, Rachel Leproult, Gilad Ofek, Mireille L’Hermite-Baleriaux, Samuel Refetoff, Fred W. Turek, and Olivier Van Reeth. Demonstration of rapid light- induced advances and delays of the human circadian clock using hormonal phase markers. Am. J. PhysioZ. 266 (Endocri- noZ. Metab. 29): E953-E963, 1994.-To determine the magni- tude and direction of phase shifts of human circadian rhythms occurring within 1 day after a single exposure to bright light, plasma thyrotropin, melatonin, and cortisol levels and body temperature were monitored for 38 h in 17 men who were each studied two times, once during continuous dim light condi- tions and once with light exposure. After a period of entrain- ment to a fixed sleep-wake cycle, a 3-h light pulse (5,000 lux) was presented under constant routine conditions, and the resultant phase shifts were measured, also under constant routine conditions, on the 1st day after pulse presentation. The phase shifts in response to light occurred within 24 h and were in the delaying direction for most of the nocturnal period, with the crossover to phase advances occurring - 1 h after the temperature minimum. Phase shifts averaged 1 h, with delays being larger than advances, and were achieved without signifi- cant changes in rhythm amplitude. The immediate response of the human circadian clock to a single 3-h light pulse is thus characteristic of “type 1” resetting. cortisol; melatonin; thyrotropin; temperature; circadian rhythms WHILE EARLY STUDIES utilizing normal indoor light inten- sity found little or no effect of light on the human circadian pacemaker, more recent studies have demon- strated that bright light has major synchronizing effects on human rhythms. In particular, appropriately timed exposure to bright light is capable of advancing or delaying circadian rhythms independently of changes in the sleep-wake cycle (1, 5, 12, 14, 22). Bright light can accelerate adaptation to shifts, such as those occurring in “jet lag” and shift work, and can widen the limits of entrainment of the human circadian system to periods deviating significantly from 24 h (6,8,9, 15, 33,34). Although there is ample evidence indicating that light is an important zeitgeber for human rhythms, the basic characteristics of the photic control of the human circadian system are still poorly understood. In particu- lar, the response of the human circadian system to a single pulse of light has yet to be defined in detail. Indeed, the vast majority of studies have used protocols involving repeated applications of a light pulse and/or combined exposure to dark pulse(s). Thus, in an early single-case study, Czeisler et al. (5) demonstrated that seven consecutive days of exposure to a 5-h pulse of light of intensity > 10,000 lux in the evening was able to delay the rhythms of body temperature and plasma cortisol by - 7 h. Using the onset of nocturnal melatonin secretion, observed under dim light conditions, as a marker of circadian phase, Lewy and collaborators (22) showed that 1 wk of exposure to 2 h of bright light (2,500 lux) in the evening shifted the onset of the melatonin increase by -2 h. In contrast, no consistent shift was observed when bright light was presented in the morning. With a similar protocol involving morning exposure to 2,000 lux of light for three consecutive days, an - l-h advance of the onset of the melatonin rise was observed (12). In another study, evening exposure to a higher-intensity 5-h pulse of light (4,000-6,000 lux) for three consecu- tive days resulted in phase delays of the temperature rhythm averaging 3 h in magnitude (14). Morning exposure to a single 4-h pulse of bright light followed by sleep in total darkness at the habitual bedtime has been shown to advance the temperature rhythm (10). In the same study, delays were observed when bright light was presented in the evening, just before the sleep/dark episode (10). The most detailed phase-response curve for human rhythms has been generated by Czeisler et al. (7) using a stimulus consisting of exposure to 5 h of bright light (7,000-12,000 lux) followed 12 h later by a 7- to 8-h sleep episode in total darkness. This procedure was repeated for three consecutive days before its effect on circadian phase was determined. This experimental design also involves presentation of the light stimulus during usual sleep times, resulting in a drastic displace- ment in the timing of sleep, and exposure to darkness. The phase-response curve to the repeated application of this mixed stimulus presents the characteristics of a so-called “strong type 0” resetting (7), i.e., there ap- pears to be a critical time of stimulus presentation where very large (6-12 h) phase changes in either direction may occur. The theoretical analysis of these data, coupled with additional experimental observa- tions, suggested that the human circadian system may respond to light in a fashion different from that known of all other mammalian species (18). Thus a single exposure to light of as yet undefined “critical intensity” would not be associated with consistent phase shifts but would instead decrease rhythm amplitude, making the system more sensitive to the second exposure, which would be associated with large phase shifts. Data ob- tained in three trials involving a single presentation of a long (8- to 9-h) stimulus at the critical phase followed by 0193-1849194 $3.00 Copyright o 1994 the American Physiological Society E953
Transcript of Demonstration of rapid light-induced advances and delays ...

Demonstration of rapid light-induced advances and delays of the human circadian clock using hormonal phase markers
EVE VAN CAUTER, JEPPE STURIS, MARIA M. BYRNE, JOHN D. BLACKMAN, RACHEL LEPROULT, GILAD OFEK, MIREILLE L’HERMITE-BALERIAUX, SAMUEL REFETOFF, FRED W. TUREK, AND OLIVIER VAN REETH Center for the Study of Biological Rhythms, Universite’ Libre de Bruxelles, B-1070 Brussels Belgium; Department of Neurobiology and Physiology, Northwestern University, Evanston 60208; and Department of Medicine, University of Chicago, Chicago, Illinois 60637.
Van Cauter, Eve, Jeppe Sturis, Maria M. Byrne, John D. Blackman, Rachel Leproult, Gilad Ofek, Mireille L’Hermite-Baleriaux, Samuel Refetoff, Fred W. Turek, and Olivier Van Reeth. Demonstration of rapid light- induced advances and delays of the human circadian clock using hormonal phase markers. Am. J. PhysioZ. 266 (Endocri- noZ. Metab. 29): E953-E963, 1994.-To determine the magni- tude and direction of phase shifts of human circadian rhythms occurring within 1 day after a single exposure to bright light, plasma thyrotropin, melatonin, and cortisol levels and body temperature were monitored for 38 h in 17 men who were each studied two times, once during continuous dim light condi- tions and once with light exposure. After a period of entrain- ment to a fixed sleep-wake cycle, a 3-h light pulse (5,000 lux) was presented under constant routine conditions, and the resultant phase shifts were measured, also under constant routine conditions, on the 1st day after pulse presentation. The phase shifts in response to light occurred within 24 h and were in the delaying direction for most of the nocturnal period, with the crossover to phase advances occurring - 1 h after the temperature minimum. Phase shifts averaged 1 h, with delays being larger than advances, and were achieved without signifi- cant changes in rhythm amplitude. The immediate response of the human circadian clock to a single 3-h light pulse is thus characteristic of “type 1” resetting.
cortisol; melatonin; thyrotropin; temperature; circadian rhythms
WHILE EARLY STUDIES utilizing normal indoor light inten- sity found little or no effect of light on the human circadian pacemaker, more recent studies have demon- strated that bright light has major synchronizing effects on human rhythms. In particular, appropriately timed exposure to bright light is capable of advancing or delaying circadian rhythms independently of changes in the sleep-wake cycle (1, 5, 12, 14, 22). Bright light can accelerate adaptation to shifts, such as those occurring in “jet lag” and shift work, and can widen the limits of entrainment of the human circadian system to periods deviating significantly from 24 h (6,8,9, 15, 33,34).
Although there is ample evidence indicating that light is an important zeitgeber for human rhythms, the basic characteristics of the photic control of the human circadian system are still poorly understood. In particu- lar, the response of the human circadian system to a single pulse of light has yet to be defined in detail. Indeed, the vast majority of studies have used protocols involving repeated applications of a light pulse and/or combined exposure to dark pulse(s). Thus, in an early single-case study, Czeisler et al. (5) demonstrated that
seven consecutive days of exposure to a 5-h pulse of light of intensity > 10,000 lux in the evening was able to delay the rhythms of body temperature and plasma cortisol by - 7 h. Using the onset of nocturnal melatonin secretion, observed under dim light conditions, as a marker of circadian phase, Lewy and collaborators (22) showed that 1 wk of exposure to 2 h of bright light (2,500 lux) in the evening shifted the onset of the melatonin increase by -2 h. In contrast, no consistent shift was observed when bright light was presented in the morning. With a similar protocol involving morning exposure to 2,000 lux of light for three consecutive days, an - l-h advance of the onset of the melatonin rise was observed (12). In another study, evening exposure to a higher-intensity 5-h pulse of light (4,000-6,000 lux) for three consecu- tive days resulted in phase delays of the temperature rhythm averaging 3 h in magnitude (14). Morning exposure to a single 4-h pulse of bright light followed by sleep in total darkness at the habitual bedtime has been shown to advance the temperature rhythm (10). In the same study, delays were observed when bright light was presented in the evening, just before the sleep/dark episode (10).
The most detailed phase-response curve for human rhythms has been generated by Czeisler et al. (7) using a stimulus consisting of exposure to 5 h of bright light (7,000-12,000 lux) followed 12 h later by a 7- to 8-h sleep episode in total darkness. This procedure was repeated for three consecutive days before its effect on circadian phase was determined. This experimental design also involves presentation of the light stimulus during usual sleep times, resulting in a drastic displace- ment in the timing of sleep, and exposure to darkness. The phase-response curve to the repeated application of this mixed stimulus presents the characteristics of a so-called “strong type 0” resetting (7), i.e., there ap- pears to be a critical time of stimulus presentation where very large (6-12 h) phase changes in either direction may occur. The theoretical analysis of these data, coupled with additional experimental observa- tions, suggested that the human circadian system may respond to light in a fashion different from that known of all other mammalian species (18). Thus a single exposure to light of as yet undefined “critical intensity” would not be associated with consistent phase shifts but would instead decrease rhythm amplitude, making the system more sensitive to the second exposure, which would be associated with large phase shifts. Data ob- tained in three trials involving a single presentation of a long (8- to 9-h) stimulus at the critical phase followed by
0193-1849194 $3.00 Copyright o 1994 the American Physiological Society E953

E954 LIGHT-INDUCED PHASE SHIFTS OF HUMAN ENDOCRINE RHYTHMS
an episode of sleep/dark 12 h later were in agreement with this concept of “type 0 resetting” (18). However, a role of the displacement of the sleep/dark episode in causing these large shifts cannot be excluded. It also remains to be determined whether such large phase shifts could be produced by the additive effects of adequately timed exposure to “subcritical” light and dark pulses during two or three consecutive days. This latter question has major practical implications, because the application of such “additive” protocols may be feasible in real life situations outside of specially de- signed laboratory units. As a first and essential step, a systematic examination of the immediate effects of a single pulse of bright light, i.e., observed within 1 day after exposure, is needed.
The steady-state response of the human circadian system to a single pulse of light has been examined in two laboratories. Using the experimental paradigm of a free run in temporal isolation, Honma and colleagues (17) have exposed four subjects to a single 3- or 6-h pulse of light of ~5,000 lux intensity. Two subjects studied under these conditions demonstrated phase advances when light was applied after sleep offset, i.e., in the beginning of the subjective day, but when light was applied in the late subjective night in two other subjects, no phase shifts were observed. Minors and colleagues (23) obtain e d a phase-response curve to a single pulse of light of 5,000-9,000 lux intensity from 16 trials in subjects maintained in free-running conditions. Al- though the phase advance region was well delineated, phase delays of > 1 h were only observed in two trials. Taken together, these observations support the concept that the steady-state response of the human circadian pacemaker to a single pulse of light is similar to that observed in other mammals but that delays may occur less readily than advances. Although the determination of classical steady-state phase-response curves under free-running conditions is of major theoretical interest, it should be noted that, for the design of additive protocols susceptible of producing rapid large shifts within a few days, it is the response of the circadian pacemaker occurring within the first 24 h after stimulus exposure that is of primary practical interest.
Only one study (2) has examined the rapid phase- shifting effects of a single light pulse, without the dark period intervening between the timing of light exposure and the timing of endogenous phase estimation. Using the melatonin rhythm as a marker of circadian rhythmic- ity, Buresova and colleagues (2) showed that early morning bright light phase advances by l-2 h the nocturnal melatonin rise on the same day. The possible occurrence of immediate phase delays in response to a single “pure” bright light stimulus, i.e., a pulse of bright light not associated with a subsequent dark period or with changes in the sleep-wake cycle, has not yet been demonstrated.
The aim of the present study was therefore to deter- mine the magnitude and direction of rapid phase shifts of human rhythms after a single exposure to a 3-h pulse of bright light presented at various circadian times over a background of dim light. We also attempted to over-
come some of the limitations of previous studies by using multiple endocrine markers, in addition to the rhythm of body temperature, to derive circadian phase and amplitude, and obtain estimations of the actual timing of the stimulus relative to endogenous circadian phase position on the day of exposure. Indeed, in the vast majority of previous studies, estimations of circa- dian phase were derived from a single overt rhythm, and the timing of the stimulus relative to endogenous circa- dian phase was extrapolated from observations obtained one or more days before stimulus exposure. In the present study, the pulse of light was presented under “constant routine” conditions, i.e., a regimen of con- stant wakefulness in the recumbent position, constant dim light, and constant caloric intake, after a period of entrainment to a fixed light-dark and sleep-wake cycle. Measurement of the resultant phase shifts was per- formed under constant routine conditions on the 1st day after pulse presentation. Four overt rhythms that are strongly dependent on circadian timing, i.e., the rhythms of plasma thyrotropin (TSH), plasma melatonin, plasma cortisol, and body temperature, were simultaneously monitored for 38 consecutive hours in 34 individual experiments.
SUBJECTS AND METHODS
Subjects
Seventeen normal young men, ages 20-30 yr, were studied. All were nonobese (body mass index of 22.7 t 2.1 kg/m2) and in good physical condition obtained through regular moderate exercise. All of the subjects were nonsmokers and had no personal history of psychiatric illness, endocrine illness, or sleep disorder. Positive criteria for selection included regular life habits and a habitual total sleep time of at least 7 h. Shift workers and subjects having experienced a transmeridian flight < 6 wk before the start of the study were excluded. The subjects underwent a physical examination and routine labora- tory tests.
Experimental Protocol
The study protocol was approved by the Institutional Re- view Board of the University of Chicago, and all volunteers gave written informed consent. A preliminary description of the study has been previously reported (30).
Each subject participated in two separate studies, one baseline study with measurements of circadian phase posi- tions in the absence of a zeitgeber stimulus and one study with exposure to a 3-h pulse of light. The studies were separated by at least 2 wk. The baseline study was performed first to obtain an estimation of the endogenous circadian phase of the individual. The timing of stimulus administration was based on the analysis of the temperature curves of the baseline study (see below).
Each study was preceded by a 7-day period of entrainment to a fixed light-dark and sleep-wake cycle, including 2 days of habituation to the laboratory conditions. The volunteers were asked to comply with a standardized schedule of sleep in total darkness (2300-0700 h) and meal times (breakfast: 0730 h; lunch: 1200 h; dinner 1900 h; snack 2130 h) for 1 wk before the study. Throughout this prestudy period, the activity-rest cycle was monitored via a wrist monitor (Gahwiler Electronics, Hombrechtikon, Switzerland). Before the study (2 days), the

LIGHT-INDUCED PHASE SHIFTS OF HUMAN ENDOCRINE RHYTHMS E955
volunteers were admitted to the Clinical Research Center of the University of Chicago at - 1400 h. The same sleep-wake cycle and meal schedule was enforced. During sleep, the subjects were in total darkness. During this period of habitua- tion to laboratory conditions, the volunteers continued to wear the wrist activity monitors, and body temperature was re- corded via a telemetry system (Cortemp; Human Technolo- gies, St. Petersburg, FL).
After awakening from the second habituation night, the subjects were served a normal breakfast which constituted their last meal until the end of the study. Monitoring of activity and temperature continued as during the habituation days. At 1200 h, a glucose infusion at a constant rate of 5 gekg-l-24 h-’ was started, and the subjects were maintained on a regimen of bedrest with enforced wakefulness in dim indoor light ( < 300 lux). These conditions of constant light exposure, constant posture, constant wakefulness, and con- stant caloric intake (i.e., constant routine) were maintained for 38 h, i.e., until 0200 h two nights later, when the subjects were allowed to obtain recovery sleep. Constant glucose infu- sion continued until the end of recovery sleep. At 1500 h, a sampling catheter was inserted in the other arm. Blood sampling at 20-min intervals started at 1800 h and continued nonstop for 37-39 h, i.e., until the end of recovery sleep. The delay between the insertion of the sampling catheter and the beginning of blood sampling served to eliminate possible hormonal changes related to the venipuncture stress. The intravenous line was kept patent by a slow drip of heparinized saline (750 IU heparin in 0.9 g NaCl/dl). Blood samples were collected using plastic syringes connected to the lateral arm of a three-way stopcock. During the constant routine, the stop- cock was directly attached to the antecubital catheter. During recovery sleep, the indwelling catheter was connected to plastic tubing (length 200 cm; diameter 1 mm; dead space < 2 ml) extending to an adjacent room. To prevent sample dilu- tion, before collecting a blood sample through the plastic tubing, 2 ml saline solution admixed with blood were removed. After having removed the blood sample, the dead space saline mixed with blood was returned to the subject, and the tubing was rinsed using the dead space volume of heparinized saline.
The subjects had access to external time cues (wristwatch, radio and television programs, social contacts) throughout the study. Water and diet decaffeinated sodas were available ad libitum. The constant routine conditions were enforced at all times during the baseline study. During the study with light exposure, the only deviation from constant routine conditions were the 3 h of exposure to bright light during which the subjects remained recumbent. Upon awakening from recovery sleep, blood sampling was terminated, the glucose infusion was tapered, breakfast was served, and the subjects were discharged. A schematic representation of the protocol as well as mean temperature and activity profiles obtained during baseline studies are shown in Fig. 1.
Timing of Stimulus Exposure
As in previous human studies designed to examine the phase-shifting effects of light (7, 18, 23), the timing of light exposure was referenced to the time of occurrence of the body temperature minimum, as observed during the baseline study. In eight subjects (subjects I-S), the center of the stimulus was timed to coincide with the timing of the body temperature minimum, in three other subjects (subjects g-10, the center of the stimulus was timed to follow the timing of the tempera- ture minimum by 2 h, and in the remaining 6 subjects (subjects 12-l 7), the center of the stimulus was timed to precede the temperature minimum by 3 h. Because the baseline study preceded the study with light exposure by at least 2 wk, it was
expected that, as was previously shown by Dawson et al. (1 l), the timing of the body temperature minimum would not remain constant and that the exact timing of stimulus expo- sure relative to the endogenous circadian phase would have to be inferred a posteriori. In a majority of studies with light exposure, the temperature minimum was masked by a tempera- ture rise induced by light; therefore, hormonal markers of circadian phase had to be used to infer a posteriori the timing of pulse presentation, as described below.
Procedures for Ligh,t Exposure
A mobile panel of mounted fluorescent tubes, size 1 m x 20 m x 0.80 m, providing a light intensity of 5,000-5,500 lux was placed 60 cm in front of the subject (Sunbox, Rockville, MD). Illumination levels at the subject’s eye were regularly checked using a digital light meter (Research Products, Mount Pros- pect, IL). Each 3-h period of exposure to 5,000 lux was bracketed by 30 min of intermediate illumination at 2,000- 2,500 lux intensity to facilitate retinal adaptation to the increased light intensity.
Hormonal Assays
MeZatonin. Plasma melatonin levels were measured using a commercially available procedure (Stockgrand, Dept of Bio- chemistry, University of Surrey, Guilford, Surrey, UK) devel- oped by J. Arendt (University of Surrey) using an antimelato- nin antiserum raised in a rabbit by Dr. J. P. Ravault (Nouzilly, France). This antiserum has been validated for the direct assay of melatonin in human plasma using an iodinated melatonin tracer. The lower limit of sensitivity is 2 pg/ml; the precision of the assay averages 10% in the range of physiologi- cal concentrations.
TSH. Plasma TSH were measured by an immunoradiomet- ric system utilizing two high-affinity monoclonal antibodies forming a sandwich with TSH (Serono Diagnostics, Norwell, MA). The lower level of sensitivity is 0.03 kU/ml. The mean intra-assay coefficient of variation is <6% throughout the physiological range.
CortisoZ. Plasma cortisol levels were determined using the Coat-A-Count kit (Diagnostic Products), a direct solid-phase radioimmunoassay using radioiodinated cortisol. The lower limit of sensitivity is 0.5 pg/dl. The intra-assay coefficient of variation averages 6.6% in the range 0.5-5.0 pg/dl and is < 5% in the range 5.0-30.0 pg/dl (i.e., the physiological range). The interassay coefficient of variation averages 6.3% for a concen- tration of 4.8 pg/dl and is <5% for concentrations in the 5.0-30.0 pg/dl range.
For all three hormones, all samples from the same indi- vidual study were measured in the same assay.
Estimations of Circadian Amplitude
The waveshape of each individual profile of temperature, plasma melatonin, plasma TSH, and plasma cortisol was quantified by a best-fit curve obtained using a robust locally weighted regression procedure proposed by Cleveland (4). The regression window was 8 h for the temperature profiles and 4 h for the hormonal profiles. The acrophases and nadirs were defined as, respectively, the times of occurrence of maxima and minima in the best-fit curve. The amplitude of the best-fit curve is defined as 50% of the difference between the value at the highest acrophase and the value at the lowest nadir and may be expressed in absolute concentration units (i.e., abso- lute amplitude) or as a percentage of the overall mean level (i.e., relative amplitude). An unmasked estimation (i.e., an estimation that is not biased by direct peripheral effects of light on the overt rhythm) of circadian amplitude on day 1

E956 LIGHT-INDUCED PHASE SHIFTS OF HUMAN ENDOCRINE RHYTHMS
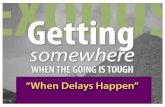
Fig. 1. Mean (+ SE) profiles of wrist activity, body temperature, plasma thy- rotropin (TSH) levels, plasma melato- nin levels, and plasma cortisol levels during baseline study. As evidenced by decline in wrist activity counts, con- stant routine conditions were enforced starting at 1200 h after last night of entrainment. Low relatively constant levels of activity were recorded through- out constant routine conditions, which were maintained for 37-39 consecutive h. Recovery sleep was allowed starting at 0200 h on day 2 and was associated with marked decline in body tempera- ture, TSH levels, and cortisol levels. Arrows: timings of nocturnal TSH, melatonin, and cortisol rises on day 1 and day 2. Black bars, sleep periods.
ENTRAINMENT CONSTANT ROUTINE RECOVERY SLEEP
3 50
1‘ we - >
18 22 02 06
1e
200 -
F 8 150 -
E
z 100 -
& I g SO,
0 -
300 -
F
8 E
5 200 -
i5 z
8 100 -
2
i 0 -
250 -
F 1 200 -
E
5 150 - h 0
a 100 -
8
22 02 06 IO 14 I8 22 02 06 IO 14 18 22 02 06 IO
t I
I I I I I I 1 I.,, If3 22 02 06 IO I4 10 22 02 06 10
50
0 /,, ,;, ,,,,, -,.,
18 22 02 06 IO 14 18 22 02 06 IO I4 10 22 02 06 10
DAY 1 4 DAY2 w

LIGHT-INDUCED PHASE SHIFTS OF HUMAN ENDOCRINE RHYTHMS E957
could be derived from all TSH, melatonin, and cortisol profiles. Indeed, light exposure did not affect TSH or cortisol levels. In the case of melatonin, light exposure was of sufficiently short duration to permit the observation of a nocturnal melatonin maximum either before or after light exposure, and this maximum was used in amplitude estimations. On day 2, estimations of circadian amplitude could only be derived from the melatonin profile, which is not affected by sleep. Indeed, as previously described, recovery sleep exerted inhibitory effects on TSH levels (24) and cortisol levels (32). Because of marked interindividual variations in overall TSH concentrations and the fact that the actual TSH acrophase could not be reached on day 2 due to the inhibitory effects of recovery sleep, the percentage rise above the daytime nadir was used to estimate the amplitude of the TSH variations on both days 1 and 2.
Estimations of Circadian Phase
On day 1, four markers of circadian phase were observed in chronological order: 1) the onset of the circadian rise of TSH, 2) the onset of nocturnal melatonin secretion, 3) the nadir of cortisol secretion, and 4) the minimum body temperature. In some studies, light exposure suppressed the melatonin onset or elevated body temperature, and estimations of circadian phase on day 1 were derived from the other marker(s), as will be described later. On day 2, the following two markers of circadian phase could be observed in the absence of masking effects (25): the onset of melatonin secretion and the onset of TSH secretion. Recovery sleep was indeed associated with a marked decrease in cortisol secretion, masking the timing of the nadir, and with a decrease in body temperature, masking the circadian minimum.
As in previous studies, the timing of the onset of the circadian TSH rise was derived from the best-fit curve to minimize effects of pulsatile variations. The onset of the rise was defined as the time when the value on the best-fit curve reached 50% of the amplitude above the daytime nadir (i.e., the value of the daytime nadir + 25% of the difference between the value at the acrophase and the value at the nadir). On day 2, the inhibitory effect of recovery sleep intervened before TSH levels reached their acrophase; therefore, straightforward calculations of the amplitude based on the best-fit curve resulted in an underestimation and thus an inaccurate evalua- tion of the onset of nocturnal secretion. The analysis of the TSH profiles on day 1 indicated that the level of the acrophase corresponded, on average, to a 10.6 * 15.7% increase over the mean level attained between 0100 and 0200 h. To improve the estimation of amplitude on day 2, the best-fit curve was recalculated after a linear extrapolation of the data over the 0200 to 0300 h period to a 10% rise over the 0100 to 0200 h mean level.
The onset of the nocturnal melatonin rise was identified using an algorithm for hormonal pulse detection, ULTRA (29), and was defined as the start of the first significant pulse not followed by a return to the level at the preceding trough. The threshold for pulse significance was set at two times the intra-assay coefficient of variation, i.e., 20%.
The timing of the nadir of cortisol secretion was defined as the time of occurrence of the nadir of the best-fit curve. Endocrine markers of circadian phase were estimated to the nearest 20 min (i.e., the length of the interval between successive blood samplings).
The timing of the circadian temperature minimum was derived from the best-fit curve as the time of occurrence of the nadir.
Calculation of Phase-Response Curves
Phase shifts of the melatonin and TSH rises were calculated as the difference between the timing of the rise on day 1 and the timing of the rise on day 2. Delays are represented as negative phase shifts, and advances are represented as positive phase shifts. To compare our observations with those of previous studies, the timing of the center of the stimulus was referenced to the minimum body temperature on the day of stimulus exposure (7, 18, 23). An additional representation using the timing of the onset of nocturnal melatonin secretion on the day of stimulus exposure as a reference was also calculated. A three-point moving average of the raw data was calculated to better delineate the overall shape of the phase- response curves.
Statistical Tests
Unless otherwise indicated, all group values are expressed as means 2 SD. Shifts observed during the studies with light exposure were compared with those observed during the baseline (i.e., constant dim light) studies by a two-tailed paired t test. The significance of the dependence of the magnitude and direction of the phase shifts on the timing of stimulus presen- tation was tested by examining the slope of the corresponding linear regression. Differences in amplitude estimations be- tween baseline studies and studies with light exposure on days 1 and 2 were tested by a two-way analysis of variance for repeated measures.
RESULTS
Profiles of Circadian Markers During the Baseline Studies
Mean profiles of body temperature, plasma TSH, plasma melatonin, and plasma cortisol obtained during the baseline studies are shown in Fig. 1.
On day 1 of the constant routine, the amplitude of the temperature rhythm averaged 0.41”, i.e., approximately one-half the amplitude observed during the last habitua- tion day. The minimum was at 0500 h t 85 min. The onset of the rise of plasma TSH occurred at 2122 h t 46 min, and the acrophase was reached at 0310 h t 85 min. The amplitude of the TSH rhythm averaged 47.6 t 8.1% of the 24-h mean TSH level, i.e., approximately two times the amplitude usually observed under entrained conditions in the presence of normal nocturnal sleep (31). This corresponded to a relative rise over the daytime nadir of 174.6 t 54.7%, i.e., the concentration at the nocturnal acrophase was almost threefold that observed during the daytime. The onset of the melato- nin rise occurred on average at 2219 h t 50 min, i.e., roughly 1 h after the TSH rise, and the acrophase was reached at 0306 h t 77 min. The amplitude of the rhythm was 60 - + 28 pg/ml, corresponding to 109.6 t 16.5% of the overall mean level. The nadir of cortisol secretion was reached at 2315 h t 103 min, and the morning acrophase occurred at 0738 h t 51 min. The amplitude of the cortisol rhythm averaged 7.8 t 2.2 pg/dl, i.e., 77.4 t 11.0% of the overall mean level.
On day 2 of the constant routine, the onsets of the TSH and melatonin rises occurred at 2138 h t 71 min and 2235 h t 81 min, respectively. The 16-min delay in

E958 LIGHT-INDUCED PHASE SHIFTS OF HUMAN ENDOCRINE RHYTHMS
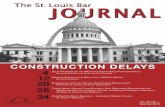
Fig. 2. Profiles of plasma melatonin and plasma TSH in subject 2 during baseline study (A) and during study with light exposure (B >. Broken line: regression curves. Open rectangles, period of bright light exposure. Bars: periods of recovery sleep. Arrows: timings of onset of TSH and melatonin rises on day 1 and on day 2. Note that, in agreement with previous observations (1 l), onsets of TSH and melatonin rises on day 1 of constant routine were not identical in baseline study and in study with light exposure, which was performed 2-4 wk later. For each hormone, phase shift was calculated as difference between timing of rise on day 1 and timing of rise on day 2 in both baseline study and study with light exposure.
50
0 1
4 m 4- 9 L 3,
2,
I-
0 -
18 22 02 06 10 14 16 22 02 06 16 22 02 06 10 14 18 22 02 06 DAY 1 DAY 2 DAY 1 DAY 2
.
CONSTANT ROUTINE RECOVERY
ZEEP CONSTANT ROUTINE REE2!ERy
CLOCK TIME CLOCK TIME
the rising phase of both hormones compared with day 1 was not statistically significant. The amplitude of the melatonin rhythm was similar to that observed on day 1, averaging 62 - + 22 pg/ml or 108.9 t 17.9% of the overall mean. Nocturnal TSH secretion was dampened com- pared with day 1, even before recovery sleep. Indeed, on day 2, the relative rise over the daytime nadir averaged only 78.9 t 22.2%, i.e., approximately one-half the magnitude of the rise on day 1 (P < 0.0001). Recovery sleep delayed the cortisol nadir, which occurred on average 71 t 96 min later than on day 1, and suppressed TSH secretion and body temperature. Because of these
effects of recovery sleep, unmasked estimations of phase shifts could be derived only from the melatonin and TSH profiles.
Effects of Light Exposure on Individual Profiles
In all subjects, light exposure was associated with a rapid decline in melatonin levels, which was reversed upon return to the dim light condition. Examples are shown in Figs. 2 and 3. The profiles of TSH and cortisol were similar during the baseline studies and during the studies with light exposure. Confirming previous obser-
Fig. 3. Profiles of plasma melatonin and plasma TSH in subject 16 during baseline study (A) and during study with light exposure (B). All symbols are as in Fig. 2.
60 A
E
30
2 z 0 P 9 120
Y
16 22 02 06 10 18 22 02 06 16 22 02 06 10 14 18 22 02 06
DAY 1 DAY 2 DAY 1 DAY 2
RECOVERY CONSTANT ROUTINE
RECOVERY CONSTANT ROUTINE SLEEP SLEEP
CLOCK TIME CLOCK TIME

LIGHT-INDUCED PHASE SHIFTS OF HUMAN ENDOCRINE RHYTHMS E959
y0 -17.5+1.06x ra0.52 peO.02 y I - 14.8 + 0.88x rz0.45 pcO.03 y~11.5+0.44~ rr0.47 p~O.01 Fig. 4. A and B: relationships between timing of
~~, ‘;:::i;:--- ~~~,
minimum body temperature and timing of TSH rise (A) and of melatonin rise (B) in baseline studies and in studies in which light exposure was not associated with rise in body temperature, allow- ing for unmasked estimation of timing of tempera- ture minimum. C: relationship between timing of TSH rise and that of melatonin rise in baseline studies and in studies in which light exposure did
20 21 22 23 24 20 21 22 23 24 not mask onset of melatonin rise. Each data point
I@ 20 21 22 23 24
TIMING OF TSH RISE TIMING OF MELATONIN RISE TIMING OF MEUTONIN MSE represents individual study. Lines correspond to (clock tlmi) (clock the)
vations by other investigators (3, 13, ZS), light exposure was associated with a small rise in body temperature (averaging 0.2-0.3’) in 11 out of 17 individual studies.
Figures 2 and 3 show representative examples of TSH and melatonin profiles in baseline studies and in studies with light exposure. In subject 2 (Fig. 2), the light pulse was centered at 0630 h (i.e., 2.25 h after the minimum body temperature), and the associated inhibition of melatonin levels resulted in a shortening of the duration of nocturnal melatonin secretion. The circadian rises of melatonin and TSH on day 2 occurred 80 and 40 min earlier than on day 1, respectively. In subject 16, the light pulse was centered at 0045 h (i.e., 4 h and 10 min before the temperature minimum), and the associated inhibition of melatonin levels resulted in a delay of the nocturnal rise on day 1. The circadian rises of melatonin and TSH on day 2 were delayed by 140 and 120 min, respectively, compared with day 1.
Relationships Between Markers of Circadian Phase on Day 1
As indicated above, the timing of the minimum body temperature was masked by a temperature rise in 11 of 17 studies with light exposure. Estimations of circadian phase could, however, be derived from the TSH profiles and, in 13 out of 17 studies, could be derived from the melatonin profiles. In the four other subjects, the begin- ning of light exposure preceded the onset of the noctur- nal melatonin rise and thus prevented the estimation of this marker of circadian phase.
BASELINE STUDY
31
(clock tIma) simple linear regression.
Figure 4 shows the relationships between the timing of the circadian temperature minimum (in baseline studies and in studies in which light exposure did not raise body temperature), the timing of the onset of the TSH rise, and the timing of the onset of the melatonin rise, as observed on day 1 of the constant routine. These three markers of circadian phase were in good concor- dance, indicating that subjects who have an early TSH rise also tend to have an early melatonin rise and an early minimum body temperature.
The regression line between the timing of the TSH rise and the timing of the temperature minimum shown in Fig. 4A was used to estimate the timing of the temperature minimum in studies in which the mini- mum was masked by a temperature rise induced by light exposure. A second estimation of the timing of the temperature minimum was obtained from the regres- sion line between the timing of the melatonin rise and the timing of the temperature minimum shown in Fig. 4B. In the calculation of the phase-response curves, the average of these two estimations of the timing of the body temperature minimum was used.
Effects of Light Exposure on Circadian Phase
Figure 5 shows the phase-response curves of the two markers of circadian phase in the baseline studies and in the studies with light exposure. The phase shifts ob- served in response to light were plotted using both the timing of the body temperature minimum and the timing of the onset of nocturnal melatonin secretion to
&HOUR LIGHT PULSE 3-HOUR LIGHT PULSE
11, iii
Fig. 5. Phase shifts of melatonin rise (top) and TSH rise (bottom) in baseline studies and in studies with light exposure. Center: timing of center of light pulse is refer- enced to timing of body temperature minimum. Right: timing of center of light pulse is referenced to timing of onset of nocturnal melatonin secretion. Line represents 3-point moving average of data, except for first and last points, which are arithmetic means of first and last 2 data points, respectively. Note that variability of phase shifts in baseline study, i.e., during continuous dim light condi- tions, was much greater for TSH than for melatonin, presumably due to greater pulsatile activity in thyrotropic axis. Trend for more delays than advances in baseline studies was not significant (P > 0.20).
TIMING OF PULSE RELATIVE TO TEMPERATURE MINIMUM
TIMING OF PULSE RELATIVE TO TIMING OF PULSE RELATIVE TO TEMPWfflJl3E MINIMUM MElA;WWN ONSET

E960 LIGHT-INDUCED PHASE SHIFTS OF HUMAN ENDOCRINE RHYTHMS
A 3 1 r = 0.417 p B 0.10
B 3 1 f =0,13 p<o.m
2
E 1 0 /
sHIFTI)I1cIFIcmIAN tsH RISE (how@
Fig. 6. Relationships between phase shift of melatonin rise and phase shift of TSH rise in baseline study (A) and in study with light exposure (B).
reference the timing of the light pulse. Both representa- tions of the light-induced phase shifts yielded remark- ably similar phase-response curves. Further character- izations of the phase-response curves will therefore be limited to the representation referencing the timing of the stimulus to the timing of the temperature minimum to allow for a straightforward comparison of our find- ings with those of previous studies (7, 18, 23). The phase-response curves for the TSH and melatonin rises are in excellent agreement. Indeed, as shown in Fig. 6, there was an excellent correlation between the phase shift of the melatonin rise and the phase shift of the TSH rise in studies with light exposure. For both hormonal markers, the crossover between the phase delay and the phase advance regions occurred > 1 h after the temperature minimum, i.e., > 7 h after the onset of the melatonin rise. The phase delay region encompassed all times of pulse presentation from 5 h before the temperature minimum, i.e., - 2400 h, until - 1 h after the temperature minimum, i.e., -0600 h. Figure 7A shows the phase-response curve for the mean of the shift of the TSH and melatonin rises. A fifth-order polynomial fit of the data clearly delineates the phase advance and the phase delay regions. For both hormonal markers, there was a significant trend from delay shifts to advance shifts associated with later timings of pulse presentation (melatonin: P < 0.001; TSH: P < 0.01). In contrast, in the baseline study, there was no signifi- cant relationship between the value of the phase shifts and the timing of stimulus exposure for either melato- nin or TSH (P > 0.25). In the phase delay region, phase shifts of the melatonin and TSH rises in response to light averaged - 74 t 44 and -67 t 59 min, respec-
tively, in contrast to phase shifts of -9 t 30 min (P < 0.001) and -17 t 71 min (P < 0.07), respectively, in the baseline studies. The mean delay shift derived from both phase markers was - 72 t 45 min in the light study vs. - 16 t 45 min in the baseline study (P < 0.005). In this study, which was limited to the nocturnal and early morning periods, phase advances were only ob- served when the light pulse was centered at least 1 h after the temperature minimum, and they were both less consistent and of smaller magnitude than phase delays. On average, phase shifts of the melatonin and TSH rises were 28 t 48 and 56 t 67 min, respectively, in the advance region, in contrast to -8 t 33 min (P < 0.20) and - 12 t 69 min (P = 0.11) in the baseline studies. The mean shift derived from both phase mark- ers averaged 42 t 35 min in the studies with light exposure vs. -10 t 47 min in the baseline studies (P < 0.01). For both the melatonin and the TSH rises, and for their mean shift, phase shifts in the baseline study were not statistically significant from zero (all P > 0.25) in the phase advance region, the phase delay region, or in the full range of stimulus presentation.
i -6 -6 -4 -2 0 2 4 6
TIMma OF PULSE RELATIVE TO TEYPERATURE uIMIYlJu
(nouW
Fig. 7. A: mean of shifts of melatonin and TSH rises for each study is plotted in relation to timing of center of light pulse, referenced to timing of minimum body temperature. B: simulation of Kronauer equations (Eqs. 6 and 9 in Ref. 19, endogenous circadian period set at 24.2 h) modeling effects of light on human circadian pacemaker with parameters reproducing experimental conditions of our study (i.e., 2 wk of entrainment to 24-h cycle of 16 h of 150 lux and 8 h of O’lux with minimum body temperature occurring 3 h before end of dark period, followed by 13- to 27-h period of continuous light of 150 lux intensity, with presentation of 3-h light pulse of 5,000 lux intensity at various points along 14-h interval, which includes timing of minimum body temperature; 30 min of 2,500 lux illumination preceded and followed each 3-h pulse).

LIGHT-INDUCED PHASE SHIFTS OF HUMAN ENDOCRINE RHYTHMS E961
10
1 T T T
Vl DAI2 DAY1 DAY: i ADVAHCL DELAY
l AILLIWL 8llJDr UaHT STUDY
Fig. 8. Estimations of rhythm amplitude on day 1 and day 2 in baseline studies (filled bars) and in studies with light exposure (open bars) in phase advance and in phase delay regions (as defined by crossover point of 3-point moving average of mean phase shifts shown in Fig. 7). TSH amplitude was lower on day 2 than on day 1 in all studies (P < 0.0001) and was lower in studies in phase delay region than in baseline studies (P < 0.05). All differences in amplitude of melatonin rhythm were nonsignificant. Amplitude of cortisol rhythm was lower on day 2 than on day 1. Differences between baseline studies and studies with light exposure were nonsignificant.
Effects of Light Exposure on Circadian Amplitude
Figure 8 summarizes the differences in estimations of circadian amplitude between day 1 and day 2 as well as between the baseline studies and the studies with light exposure in the phase advance or phase delay regions.
In all studies, the relative TSH rise above the daytime nadir was drastically reduced on day 2 compared with day 1 (P < 0.0001). Ongoing studies in our laboratory indicate that this reduction in amplitude of the TSH rise during the second night of sleep deprivation reflects the negative feedback effect of elevated thyroid hormone levels caused by the TSH rise during the first night of sleep deprivation. There were no differences in estima- tions of TSH amplitudes on day 2 between the baseline study and the study with light exposure in the advance region. However, in the studies with light exposure in the delay region, the TSH rise on day 2 was less than in the baseline studies (P < 0.05) and in the studies with light exposure in the advance region (P < 0.05), consis- tent with a delayed onset of the rise and, consequently, lower maximal levels attained before onset of recovery sleep.
For melatonin, none of the differences in circadian amplitude between day 1 and day 2 or across study conditions were statistically significant.
Because the study period ended before cortisol levels reached their second morning acrophase, estimations of cortisol amplitude shown in Fig. 8 correspond to 50% of the difference between the level at the nadir and the mean level between 0600 and 0700 h (a parameter that could be measured both on day 1 and day 2). The amplitude was lower on day 2 than on day 1 in both baseline (P < 0.004) and light (P < 0.04) studies, reflect- ing the delay in early morning rise induced by recovery sleep. There were no significant differences between the baseline condition and the light condition.
DISCUSSION
The present study demonstrates that a single expo- sure to bright light presented over a background of dim light, without an intervening dark period, may cause shifts of human circadian rhythms within < 24 h, with the direction and magnitude of the shifts depending on the timing of pulse presentation relative to the endog- enous circadian phase. These shifts were achieved de- spite the continuous presence of environmental time cues. This is the first demonstration of rapid phase- shifting effects of light per se since all previous studies on the response of the human circadian system to light pulses have involved protocols in which the phase shifts presumably caused by bright light exposure were mea- sured after the subjects were exposed to one or more episodes of sleep and/or darkness. The only exception concerns the phase advances recently reported by Bu- resova et al. (2) in subjects exposed to morning bright light. Although these previous observations are consis- tent with our findings, the phase-response curve ob- tained in the present study demonstrates that the response to a single light pulse on the 1st day after exposure lies in the delaying direction for most of the nocturnal period, with the crossover point occurring N 1 h after the temperature minimum. Overall, the magni- tude of the phase shifts averages 1 h. The phase shifts are not accompanied by significant alterations in mea- sures of circadian amplitude. The response of the hu- man circadian clock to a single 3-h light pulse is thus characteristic of “type 1” resetting.
Our experimental design allowed for the simulta- neous monitoring of several overt rhythms to obtain multiple estimations of circadian phase and amplitude. This design made it possible to obtain an estimation of the actual endogenous phase position of each subject on the day of pulse presentation. Thus, in studies in which light exposure elicited a temperature rise, which masked the endogenous temperature minimum, circadian phase could be derived from the timings of the onsets of melatonin and/or TSH secretory rises. In studies where evening light exposure masked the onset of the melato- nin rise, an estimation of endogenous circadian phase could be derived from the temperature profile and/or from the TSH profile. In this respect, our study differs from all previous attempts to characterize the response of the human circadian system to photic stimuli. Indeed,

E962 LIGHT-INDUCED PHASE SHIFTS OF HUMAN ENDOCRINE RHYTHMS
the timing of the light pulse in previous studies has always been defined in reference to circadian phase position obtained during a baseline trial preceding the trial with pulse administration. However, as shown by Dawson et al. (11) and as confirmed in the present study, the human circadian system shows considerable day-to- day variability in phase position in a given individual.
The simultaneous monitoring of multiple overt rhythms in the present study also strongly increased the reliability of the estimated phase shifts after exposure to the light pulse. The observation of a remarkably similar phase-response curve using either the onset of the melatonin rise or the onset of the TSH rise as marker of phase position, with an excellent correlation between the shifts of these two markers, essentially exclude the possibility that our findings may represent an experimen- tal artifact or a delayed response to the light stimulus not involving the circadian pacemaker. Indeed, light exposure has direct effects on both the temperature profile and the melatonin profile; therefore, phase changes on the 1st day after light exposure could conceivably reflect a direct effect of light. However, light exposure does not affect the TSH profile; therefore, this possibility appears unlikely. With the noticeable excep- tion of the studies of Czeisler et al. (5, 7,18,27), all other studies examining the photic control of human rhythms have relied on a single-marker rhythm, which was itself affected by light exposure.
The duration and intensity of our light stimulus were chosen so they could be realized in real life situations outside of the laboratory using portable light sources. Attention was also given to limit the duration of the stimulus so that it would not encompass both the putative phase advance and phase delay regions. One of our goals was to determine whether human rhythms would phase shift after a single exposure to this type of photic stimulation (i.e., type 1 resetting) or whether they would just exhibit reductions in rhythm amplitude without consistent phase shifting (i.e., type 0 resetting). The observed phase shifts and amplitude estimations clearly indicate that type 1 resetting is occurring.
Figure 7B illustrates the results of computer simula- tions of our experimental conditions with the mathemati- cal equations proposed by Kronauer et al. (19, 20) to model the effects of light on the human circadian oscillator. There is a remarkable agreement between the experimental findings and the predictions derived from the model. In particular, for light pulses presented during the nocturnal period as is the case in the present study, the phase delay region is larger than the phase advance region. For both experimental and simulated data, the crossover from delays to advances occurs at approximately the same circadian time. Furthermore, the predicted phase shifts are of magnitude comparable to those observed experimentally in both the phase advance and the phase delay regions. Thus these simula- tions may indicate that the light stimulus used in the present study was of subcritical intensity. Ongoing simulations in our laboratory suggest, however, that increasing light intensity up to 10,000 lux would not modify the qualitative characteristics of the phase-
response curve if pulse duration is maintained constant. Thus type 0 resetting would require durations of expo- sure > 3 h. Although our observations are consistent with predictions derived from the model of Kronauer et al. (19, ZO), they do not exclude the possibility that large 8- to 10-h phase shifts could occur as a result of additive effects of repeated exposure to adequately timed light and dark pulses rather than necessarily reflect type 0 resetting.
The results of the present study suggest that the phase delay region of the phase-response curve to light in humans may be of larger amplitude than the phase advance region. However, the range of timings of light exposure did not extend beyond the midmorning, leav- ing open the possibility that larger phase advances may have been observed if light pulses had been presented in the late morning and midday periods. Furthermore, the apparent lower magnitude of advances compared with delays may only apply to the phase shifts observed on the 1st day after light exposure and may be incorrect as far as steady-state phase shifts are concerned. Indeed, studies in hamsters under free-running conditions indi- cate that, although phase delays reach their steady-state magnitude within one or two cycles, phase advances need three to five cycles to be complete (16). In these laboratory animals, shifts achieved within 24 h after light exposure are of the same order of magnitude as those seen in the human subjects who participated in the present study (16). The data from the two human studies that have examined phase shifts during an extended free run in temporal isolation are consistent with the hypothesis that the transient dynamics of phase shifting are similar in humans in that phase advances were observed more consistently than phase delays (17,23).
The present study also demonstrates the existence of linear relationships between the timing of the minimum body temperature, the timing of the onset of the noctur- nal rise in melatonin secretion, and the timing of the onset of the nocturnal rise of TSH secretion, confirming the reliability of the onset of the melatonin rise as a marker of circadian phase (21, 26) and establishing the onset of the TSH rise as a second accurate phase marker. These relationships provide means to derive unmasked estimations of circadian phase in conditions where the temperature or the melatonin rhythms are masked by light exposure. They also indicate that two independent reliable hormonal markers of phase posi- tion, i.e., the onset of the TSH rise and the onset of the melatonin rise, may be observed during an 8-h window (i.e., 1800-0200 h) without enforcement of prolonged sleep deprivation, which represents the major limitation of the constant routine approach. The measurement of these two hormonal phase markers under dim light conditions and constant posture and caloric intake may provide a practical approach for dynamic studies examin- ing changes of human circadian phase on successive days.
In conclusion, the present study has provided a hu- man phase-response curve for the rapid effects of night- time light exposure using a novel approach involving

multiple phase markers to derive reliable estimations of circadian phase. These data constitute an essential step toward an understanding of the dynamics of cumulative effects of exposure to light on successive days.
We thank the volunteers for participation, patience, and coopera- tion and the nursing staff for assistance.
This work was supported by Grants 90-0222 and 93-10188 from the United States Air Force Office of Scientific Research, by Department of Defense Augmentation Award for Science and Engineering Re- search Training 92-50347, and by National Institutes of Health Grant RR-00055.
During the completion of part of this work, F. W. Turek was supported by a National Institutes of Health Senior Fogarty Fellow- ship and a Guggenheim Fellowship.
Address for reprint requests: E. Van Cauter, Dept. of Medicine, MC 1027, University of Chicago, 5841 S. Maryland Ave., Chicago, IL 60637.
Received 5 October 1993; accepted in final form 4 February 1994.
REFERENCES
1. Broadway, J., 3. Arendt, and S. Folkard. Bright light phase- shifts the human melatonin rhythm during the Antarctic winter. Neurosci. Lett. 79: 185-189, 1987.
2. Buresova, M., M. Dvorakova, P. Zvolsky, and H. Illnerova. Early morning bright light phase advances the human circadian pacemaker within one day. Neurosci. Lett. 121: 47-50,199l.
3. Cagnacci, A., R. Soldani, and S. S. C. Yen. The effect of light on core body temperature is mediated by melatonin in women. J. Clin. Endocrinol. Metab. 76: 1036-1038, 1993.
4. Cleveland, W. S. Robust locally weighted regression and smooth- ing scatterplots. J. Am. Stat. Assoc. 74: 829-836, 1979.
5. Czeisler, C. A., J. S. Allan, S. H. Strogatz, J. M. Ronda, R. Sanchez, C. D. Rios, W. 0. Freitag, G. S. Richardson, and R. E. Kronauer. Bright light resets the human circadian pacemaker independent of the timing of the sleep-wake cycle. Science Wash. DC 233: 667-671,1986.
6. Czeisler, C. A., M. P. Johnson, J. F. Duffy, E. N. Brown, J. M. Ronda, and R. E. Kronauer. Exposure to bright light and darkness to treat physiologic maladaptation to night work. N. Engl. J. Med. 322: 1253-1259,199O.
7. Czeisler, C. A., R. E. Kronauer, J. S. Allan, J. F. Duffy, M. E. Jewett, E. N. Brown, and J. M. Ronda. Bright light induction of strong (type 0) resetting of the human circadian pacemaker. Science Wash. DC 244: 1328-1333,1989.
8. Daan, S., and A. J. Lewy. Scheduled exposure to daylight: a potential strategy to reduce “jet lag” following transmeridian flight. Psychopharmacol. Bull. 20: 566-568,1984.
9. Dawson, D., and S. S. Campbell. Timed exposure to bright light improves sleep and alertness during simulated night shifts. Sleep NY 14: 511-516,199l.
10. Dawson, D., L. Lack, and M. Morris. Phase resetting of the human circadian pacemaker with the use of a single pulse of bright light. Chronobiol. Int. 10: 94-102, 1993.
11. Dawson, D., K. Lushington, L. Lack, S. Campbell, and C. Matthews. The variability in circadian phase and amplitude estimates derived from sequential constant routines. Chronobiol. Int. 9: 362-370,1992.
12. Dijk, D. J., D. G. M. Beersma, S. Daan, and A. J. Lewy. Bright morning light advances the human circadian system without affecting NREM sleep homeostasis. Am. J. Physiol. 256 (Regulatory Integrative Comp. Physiol. 25): R106-Rlll, 1989.
13. Dijk, D. J., C. Cajochen, and A. A. Borbely. Effects of a single 3-hour exposure to bright light on core body temperature and sleep in humans. Neurosci. Lett. 121: 59-62, 1991.
14. Drennan, M., D. F. Kripke, and J. C. Gillin. Bright light can delav human temnerature rhvthm indenendent of sleen. Am. J.
Physiol. 257 (Regulatory Integrative Comp. Physiol. 26): R136- R141,1989.
15. Eastman, C. I. High-intensity light for circadian adaptation to a 12-h shift of the sleep schedule. Am. J. Physiol. 263 (Regulatory Integrative Comp. Physiol. 32): R428-R436,1992.
16. Ellis, G. B., R. E. McKlveen, and F. W. Turek. Dark pulses affect the circadian rhythm of activity in hamsters kept in constant light. Am. J. Physiol. 242 (Regulatory Integrative Comp. Physiol. 11): R44-R50, 1982.
17. Honma, K., S. Honma, and T. Wada. Phase-dependent shift of free-running human circadian rhythms in response to bright light pulse. Experientia Base1 43: 1205-1207, 1987.
18. Jewett, M., R. E. Kronauer, and C. A. Czeisler. Light- induced suppression of endogenous circadian amplitude in hu- mans. Nature Lond. 350: 59-62, 1991.
19. Kronauer, R. E. A quantitative model for the effects of light on the amplitude and the phase of the deep circadian pacemaker, based on human data. In: Sleep ‘90, edited by J. Horne. Bochum: Pontenagel, 1990, p. 306-309.
20. Kronauer, R. E., C. A. Czeisler, S. F. Pilato, M. C. Moore- Ede, and E. D. Weitzman. Mathematical model of the human circadian system with two interacting oscillators. Am. J. Physiol. 242 (Regulatory Integrative Comp. Physiol. 11): R3-R17, 1982.
21. Lewy, A. J., and R. L. Sack. The dim light melatonin onset as a marker for circadian phase position. Chronobiol. Int. 6: 93-102, 1989.
22. Lewy, A. J., R. L. Sack, L. S. Miller, and T. M. Hoban. Antidepressant and circadian phase-shifting effects of light. Sci- ence Wash. DC 235: 352-354,1987.
23. Minors, D. S., J. M. Waterhouse, and A. Wirz-Justice. A human phase-response curve to light. Neurosci. Lett. 13: 36-40, 1991.
24. Parker, D. C., A. E. Pekary, and J. M. Hershman. Effect of normal and reversed sleep-wake cycles upon nyctohemeral rhyth- micity of thyrotropin (TSH): evidence suggestive of an inhitory influence in sleep. J. Clin. Endocrinol. Metab. 43: 315-322, 1976.
25. Rietveld, W. J., D. S. Minors, and J. M. Waterhouse. Circadian rhythms and masking: an overview. Int. J. Chronobiol. 10: 306-312,1993.
26. Rosenthal, N. E. Plasma melatonin as a measure of the human clock. J. Clin. Endocrinol. Metab. 73: 225-226, 1991.
27. Shanahan, T. L., and C. A. Czeisler. Light exposure induces equivalent phase shifts of the endogenous circadian rhythms of circulating plasma melatonin and core body temperature in men. J. Clin. Endocrinol. Metab. 73: 227-235, 1991.
28. Strassman, R. J., C. R. Qualls, J. Lisansky, and G. T. Peake. Elevated rectal temperature produced by all-night bright light is reversed by melatonin infusion in men. J. Appl. Physiol. 71: 2178-2182,199l.
29. Van Cauter, E. Estimating false-positive and false-negative errors in analyses of hormonal pulsatility. Am. J. Physiol. 254 (Endocrinol. Metab. 17): E786-E794,1988.
30. Van Cauter, E., J. Sturis, M. M. Byrne, J. D. Blackman, N. H. Scherberg, R. Leproult, S. Refetoff, and 0. Van Reeth. Preliminary studies on the immediate phase-shifting effects of light and exercise on the human circadian clock. J. Biol. Rhythms, Suppl. 8: S99-S108,1993.
31. Van Coevorden, A., E. Laurent, C. Decoster, M. Kerkhofs, P. Neve, E. Van Cauter, and J. Mockel. Decreased basal and stimulated thyrotropin secretion in healthy elderly men. J. Clin. Endocrinol. Metab. 69: 177- 185, 1989.
32. Weitzman, E. D., J. C. Zimmerman, C. A. Czeisler, and J. M. Ronda. Cortisol secretion is inhibited during sleep in normal man. J. Clin. Endocrinol. Metab. 56: 352-358, 1983.
33. Wever, R. A. Bright light affects human circadian rhythms. Pfluegers Arch. 396: 85-87,1983.
34. Wever, R. A. Light effects on human circadian rhythms: A review of recent Andechs experiments. J. Biol. Rhythms 4: 161-185,
LIGHT-INDUCED PHASE SHIFTS OF HUMAN ENDOCRINE RHYTHMS E963