Delirium: Encephalopathy/Acute confusion
24
Delirium: Encephalopathy/Acute confusion Vikas Kumar, MD PhD SSM Neurosciences
Transcript of Delirium: Encephalopathy/Acute confusion

Delirium: Encephalopathy/Acute
confusion
Vikas Kumar, MD PhDSSM Neurosciences

Disclosures
• None

Encephalopathy Definition• Greek: Inside the head, suffering
• Brain disease, disorder or damage: temporary or permanent condition that affects brain structure and function
• Acute or subacute syndrome characterized by disturbance of consciousness, orientation, attention, cognitive function, sleep wakefulness cycle and fluctuation
• Global disturbance of cerebral function
• Hallmark of encephalopathy is altered mental state (AMS), delirium, confusional state
• Can progress to Coma
www.ninds.nih.gov/disorders/encephalopathy/encephalopathy.htm

Delirium or Acute encephalopathy
- Two different terms describing the same condition.- Delirium represents the mental manifestation while encephalopathy
identifies the underlying pathophysiologic process. - DSM-5 classifies acute toxic and metabolic encephalopathic states as
delirium and does not use encephalopathy in its definitions.- ICD-9 and ICD-10 use “encephalopathy” to classify what DSM-5 calls
delirium. Examples include:* Toxic encephalopathy due to phenytoin, causing delirium* Delirium due to metabolic encephalopathy

Incidence- Increases after the age of 65 years.
- People older than 75 years, who reside in nursing homes have a 60% chance of developing encephalopathy.
- Encephalopathy occurs in 10–40% of hospitalized patients older than 65 years.
- Encephalopathy has being registered in 12–16% of patients with thiamine deficiency, every year
- In patients with cirrhosis, the hepatic encephalopathy develops in 45–80% of cases, depending on the severity of liver damage

Causes of encephalopathy• Toxic Metabolic Encephalopathy (TME): Hepatic
(hyperammonemia), uremia, electrolyte imbalance, alcohol, organ failure, chemotherapy
• Drugs: Barbiturates, narcotics, TCAs, Anticholinergics, Phenothiazines, anticonvulsants (VPA, TPM, CBZ etc) corticosteroids, Cephalosporin (cefepime), etc
• Hypertension
• Epileptic
• Hypoxic ischemic
• B1 deficiency (Wernicke)
• Infection: HIV, UTI, pneumonia, lyme, sepsis, pancreatitis etc
• Infectious: Prion disease/CJD, Transmissible spongiform encephalopathy
• Thyroid: Hashimoto
• Glycine
• Paraneoplastic
• PRES
• Mitochondrial encephalomyopathy, MELAS
• NMDAR encephalitis
• Trauma: CTE
• Industrial and environmental toxins: organic solvents, heavy metals

Causes of encephalopathy

Encephalopathy Symptoms/Signs
• Altered mental state: Delirium
• Impairment of alertness, attention, concentration, memory.
• Feeling confused, lethargic, psychomotor hyperactivity, agitation, hallucination
• Physical symptoms: involuntary eye and muscle movements (Roving eye movements, asterixis, myoclonus), seizures
• Autonomic symptoms: insomnia, nausea, heart rhythm disorders

Diagnosis• Clinical history and neurological exam
• Laboratory tests: CBC, CMP, blood culture, ammonia, TSH, Toxicological screen, B12, B1, ESR, CRP, procalcitonin, lactic acid, ABG, U/A, Heavy metal screen, HIV, lactate, pyruvate, NMDAR Ab, paraneoplastic panel, lyme panel
• CSF exam: cell count, protein, glucose, culture, 14-3-3 protein,
• Neuroimaging
• EEG: generalized slowing or focal suppression, FIRDA, PLEDs, Triphasic waves

Pathophysiology- Inflammation —> endothelial activation in the brain —> malfunction of the blood–brain barrier. —> release of inflammatory mediators such as cytokines and chemokines —> damage to the cellular metabolism —> oxidative stress and mitochondrial dysfunction —> disruption of neurotransmission —> apoptosis.
- The cholinergic, GABA, beta-adrenergic, and serotonergic systems are altered and neurotransmission functioning is damaged, especially in the neocortex and hippocampus.
- Release of excitatory amino acids, hyperglycemia, neurotoxic pharmacological agents, hemodynamic changes, coagulopathy, and hypoxemia.
- Increase in the glutamine and glutamate complex peak in magnetic resonance (MR) spectroscopy illustrates the neuronal and astrocytic excitotoxic injury.
- The combined antiepileptic valproate and topiramate therapy causes reduction of topiramate metabolism through cytochromeP 450 pathway.
- Cephalosporins may also induce encephalopathy through GABA A receptor inhibition.
- Decrease in the central cholinergic activation and an increase in the proinflammatory cytokine concentrations (interleukin 8, TNF alpha, interleukin 10)

Pathophysiology

Treatment• Correct the cause
• ABCs
• Hashimoto’s/Thyroiditis: Steroid responsive encephalopathy
• Wernicke: High dose Thiamine IV
• Uremic encephalopathy: Dialysis
• Anticonvulsants
• Sympathomimetic drugs


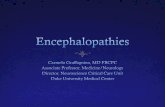
Prion disease (CJD): Cortical signal abnormality
Day 1 Day 11 Day 18
- Rapidly progressive, invariably fatal neurodegenerative disorder - Caused by an abnormal isoform of a cellular glycoprotein
known as the prion protein. - Estimated annual incidence to be about one case per
million population.

Periodic discharges

Hepatic/Uremic encephalopathy
Type A, which is associated with acute liver failure. Type A are more likely to have edema in the brainType B, which is associated a portosystemic shunt (a shunt that bypasses the liver) with no existing liver disease presentType C, which is associated with scarring and poor function of the liver (cirrhosis)

Wernicke encephalopathy- Most important encephalopathy due to a single vitamin (B1
Thiamine) deficiency- Triad of ocular findings, cerebellar dysfunction and
confusion- Most often associated with chronic alcoholosim, poor
nutrition, malabsorption, increased metabolic requirements/systemic illness, renal dialysis hyperemesis of pregnancy, bariatric surgery etc

Autoimmune encephalitis

Autoimmune encephalitis

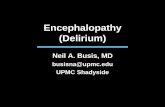
Figure 1 Flowchart of samples and results ADS = acquired demyelinating syndromes; GBS = Guillain-Barré syndrome; LEMS = Lambert-Eaton myasthenic syndrome; OMS = opsoclonus myoclonus syndrome; SC = Sydenham chorea; VGKC = voltage-gated potassium channel.
Yael Hacohen et al. Neurology 2015;85:967-975
© 2015 American Academy of Neurology

NMDA receptor encephalitis
• Paraneoplastic encephalitis
• Psychiatric features
• Involuntary movement
• Autonomic instability
• 80% of patients are female and around 50% have underlying tumor (ovarian teratoma, Lung cancer, thyroid tumor, breast, cancer, colon, neuroblastoma etc)
https://www.rarediseasereview.org/publications/2017/2/9/recent-updates-in-anti-nmda-receptor-encephalitis-research

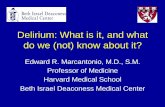
Immunologic triggers in anti–NMDA receptor (NMDAR) encephalitis
Josep Dalmau Neurology 2016;87:2471-2482
© 2016 American Academy of Neurology

Brain reactivity of autoantibodies against neuronal cell surface or synaptic proteins
Josep Dalmau Neurology 2016;87:2471-2482
© 2016 American Academy of Neurology

Ongoing Clinical trials