Defining sepsis - Journal Club (Jason Wu)
22
SMACC & SEPSIS Dr Jason Wu Resident Medical Officer Clinical Tutor Graduate School of Medicine University of Wollongong
-
Upload
bishan-rajapakse -
Category
Health & Medicine
-
view
27 -
download
3
Transcript of Defining sepsis - Journal Club (Jason Wu)

SMACC & SEPSISDr Jason Wu
Resident Medical Officer
Clinical Tutor
Graduate School of Medicine
University of Wollongong

SMACC• Acute MI can be safely ruled out at 3 hours with
contemporary troponin (Rick Body, Louise Cullen)
MAC

Posterior STEMI
Posterior STEMI is 10% of all STEMIs and the most missed
STEMI for cath lab up to 30% of the time. Don’t be fooled
and think this is anterior ischemia.

Right Sided ECG• A complete set of right-sided leads is
obtained by placing leads V1-6 in a mirror-image position on the right side of the chest (see diagram, below).
• It may be simpler to leave V1 and V2 in their usual positions and just transfer leads V3-6 to the right side of the chest (i.e. V3R to V6R).
• The most useful lead is V4R, which is obtained by placing the V4 electrode in the 5th right intercostal space in the midclavicular line. ST elevation in V4R has a sensitivity of 88%, specificity of 78% and diagnostic accuracy of 83% in the diagnosis of RV MI.
Lactate • Lactic Acid is a marker of physiologic stress NOT specific to sepsis, but
if elevated in sepsis means a poor prognosis for patient (John Myburgh @JAMyburgh)
• Low sensitivity and specificity but cheap, immediate and at point of care
• Exact physiology unknown
• Respiratory Rate is the one vital sign least often recorded and most frequently omitted in hospital documentation, but a raised respiratory rate is a strong and specific predictor of serious adverse events such as cardiac arrest and unplanned ICU admission.
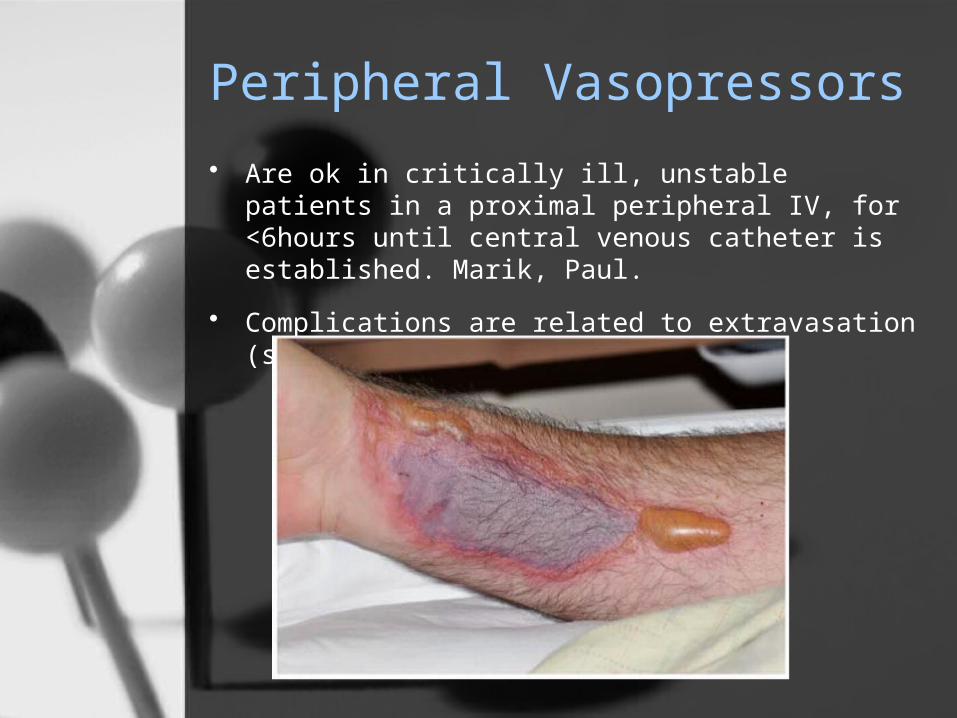
Peripheral Vasopressors
• Are ok in critically ill, unstable patients in a proximal peripheral IV, for <6hours until central venous catheter is established. Marik, Paul.
• Complications are related to extravasation (see below)

History of SIRS Criteria
• Definitions for sepsis and organ failure and guidelines for the use of innovative
therapies in sepsis. The ACCP/SCCM consensus conference committee. American
College of Chest Physicians/Society of Critical Care Medicine. Bone R, Balk R, Cerra
F, et al. Chest. 1992;101(6):1644-1655.
• The conference concluded that the manifestations of SIRS include, but are not
limited to:
1. Temperature < 36°C or > 38°C
2. Heart rate > 90 bpm
3. Tachypnoea > 20 breaths per minute, or an arterial pCO2 < 32 mmHg
4. White cell count (WCC) < 4000 cells/mm³ (4 x 109 cells/L) or > 12,000 cells/mm³
(12 x 109 cells/L), or > 10% immature neutrophils (left-shift)
• SIRS can be diagnosed when two or more of these criteria are present.

Diagnosis of Sepsis
The SIRS criteria, in the setting of sepsis, are traditionally applied thus:
• Infection + SIRS = Sepsis
• Sepsis + hypotension + end-organ damage = Severe sepsis
• Severe sepsis + refractory hypotension = Septic shock

Challenging SIRS Criteria
• Vincent JL. Dear SIRS, I’m sorry to say that I don’t like you…Crit Care Med 1997;25:373-4.
• Vincent JL, Opal SM, Marshall JC, Tracey KJ. Sepsis definitions: time for change. Lancet 2013; 381:774-5.

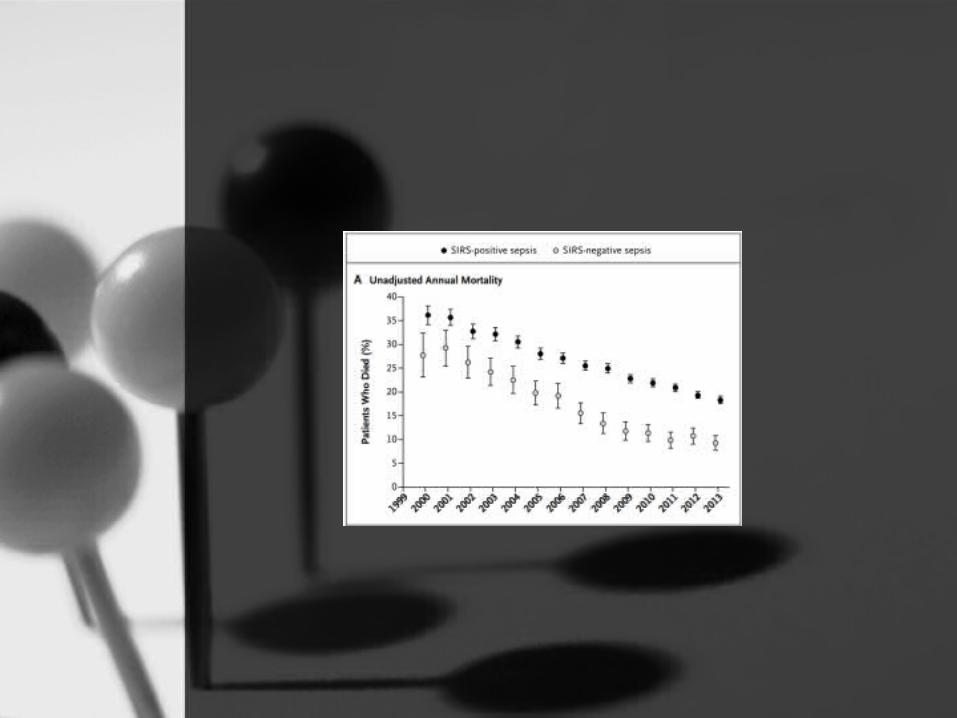
NEJM: Systemic inflammatory response syndrome criteria in defining severe sepsis.Kaukonen KM, et al. N Engl J Med. 2015
• Retrospective study
• 14 years of data from ANZICS Adult Patient Database between Jan 1, 2000, to Dec 31, 2013.
– 172 ICU’s and more than 90% of all ICU admissions
• 1.1 million admissions, with 109,633 severe sepsis cases with organ dysfunction
– 87.9% were SIRS positive
– 12.5% SIRS negative

Definitions
• SIRS negative sepsis within 24 hours of admission to ICU with at least one organ failing, or an APACHE III diagnosis of severe sepsis or septic shock at admission
• SIRS positive severe sepsis within 24 hours of admission to the ICU with two or more SIRS criteria, an APACHE III diagnosis of infection at admission with at least one organ failure, or an APACHE III diagnosis of severe sepsis or septic shock at admission.

APACHE


Outcomes

Mortality
• A simple multiple system organ
failure scoring system predicts
mortality of patients who have
sepsis syndrome. Hebert P,
Drummond A, Singer J, Bernard G,
Russell J. Chest. 1993;104(1):230-
235.


Limitations
• Retrospective study using quality control data
• First 24 hours of ICU admission
• No ED or ward data
• Delayed SIRS not considered
• Treatment interventions not considered
• Did not consider altered mental status or lactate

Take home points
• SIRS negative ≠ not septic
– Neither sensitive nor specific
– Only ~1/3 of SIRS criteria patients have an infection
• Patient observations and SIRS criteria evolves
• Tachycardia is the most common early sign
• Temperature is the least sensitive sign
• Being SIRS positive is still a marker of higher mortality in sepsis
• Nb - ICU study (no ED patients)

NS
W H
ealth
- G
uide
lines

Plug for SMACC 2015!