Appraisal of Recent Progress in Metastatic Castration-Resistant Prostate Cancer

Defining Personalized Care Plans in
Metastatic Castration-Resistant
Prostate Cancer
Tanya B. Dorff, MD
Associate Professor of Clinical Medicine
USC Keck School of Medicine
USC Norris Comprehensive Cancer Center

ACCREDITATIONThis activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint providership of Postgraduate Institute for Medicine and i3 Health. The Postgraduate Institute for Medicine is accredited by the ACCME to provide continuing medical education for physicians.
The Postgraduate Institute for Medicine designates this live activity for a maximum of 1.0 AMA PRA Category 1 Credit™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
The Postgraduate Institute for Medicine is accredited with distinction as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation. This educational activity for 1.0 contact hours is provided by Postgraduate Institute for Medicine. Designated for 0.8 contact hours of pharmacotherapy credit for Advance Practice Registered Nurses.
INSTRUCTIONS TO RECEIVE CREDITIn order to receive credit for this activity, participants must:1. Participate in the live webinar2. Complete and submit the posttest and activity evaluation via the link provided after the webinar3. Download or print their Certificate of Credit
UNAPPROVED USE DISCLOSUREThis educational activity may contain discussion of published and/or investigational uses of agents that are not indicated by the FDA. The planners of this activity do not recommend the use of any agent outside of the labeled indications.
The opinions expressed in the educational activity are those of the faculty and do not necessarily represent the views of the planners. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications, and warnings.
DISCLAIMERParticipants have an implied responsibility to use the newly acquired information to enhance patient outcomes and their own professional development. The information presented in this activity is not meant to serve as a guideline for patient management. Any procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this activity should not be used by clinicians without evaluation of their patient’s conditions and possible contraindications and/or dangers in use, review of any applicable manufacturer’s product information, and comparison with recommendations of other authorities.
COMMERCIAL SUPPORTThis activity is supported by independent educational grants from Bayer HealthCare Pharmaceuticals Inc. and Genzyme.

Disclosures
▶ Dr. Dorff discloses the following commercial
relationships:◼ Consultant: Bayer, Dendreon, Eisai, EMD Serono, Exelixis,
Janssen
◼ Speakers’ Bureau: Exelixis
▶ The PIM planners and managers, Trace Hutchison,
PharmD, Samantha Mattiucci, PharmD, CHCP, Judi
Smelker-Mitchek, MBA, MSN, RN, and Jan Schultz,
MSN, RN, CHCP have nothing to disclose
▶ The i3 Health planners and managers have nothing to
disclose
Learning Objectives
▶ Evaluate recent study findings on combination and
sequential treatment strategies for patients with
metastatic CRPC
▶ Determine which predictive/prognostic biomarker
tests are ready for application in metastatic CRPC
practice
▶ Utilize strategies for evaluating treatment response,
incorporating imaging studies, prostate-specific
antigen levels, and clinical findings
CRPC = castration-resistant prostate cancer.
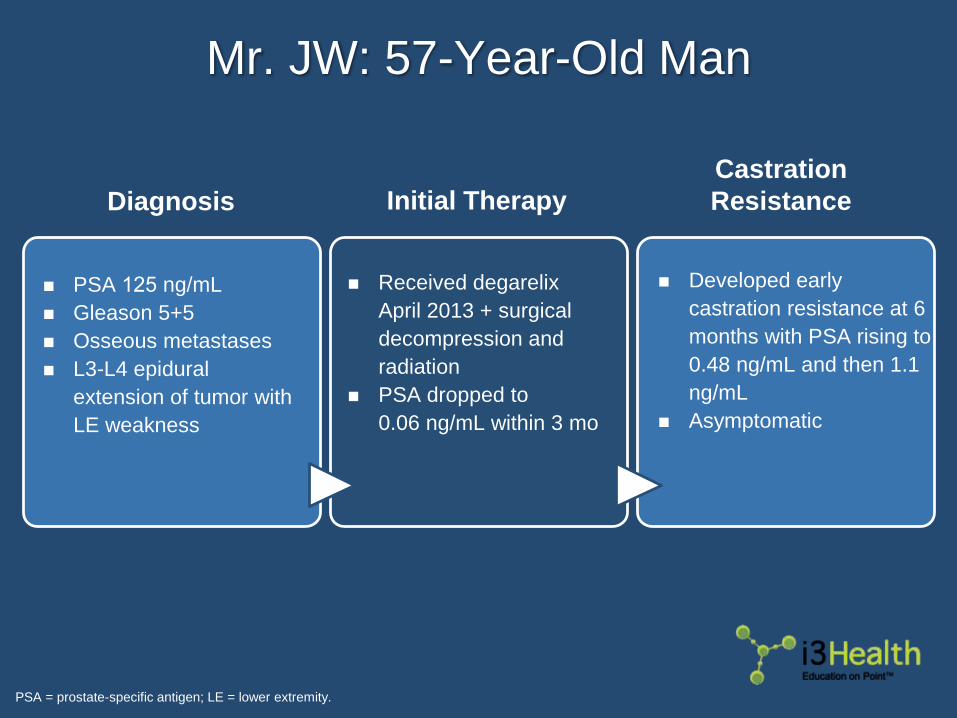
Mr. JW: 57-Year-Old Man
PSA = prostate-specific antigen; LE = lower extremity.
◼ PSA 125 ng/mL
◼ Gleason 5+5
◼ Osseous metastases
◼ L3-L4 epidural
extension of tumor with
LE weakness
◼ Received degarelix
April 2013 + surgical
decompression and
radiation
◼ PSA dropped to
0.06 ng/mL within 3 mo
◼ Developed early
castration resistance at 6
months with PSA rising to
0.48 ng/mL and then 1.1
ng/mL
◼ Asymptomatic
Diagnosis
Castration
ResistanceInitial Therapy

Mr. JW: Castration Resistance
Mr. JW: Next Step?
Sipuleucel-T
Abiraterone
Enzalutamide
DocetaxelCabazitaxel
Radium-223
Combination Therapy
Treatment Options
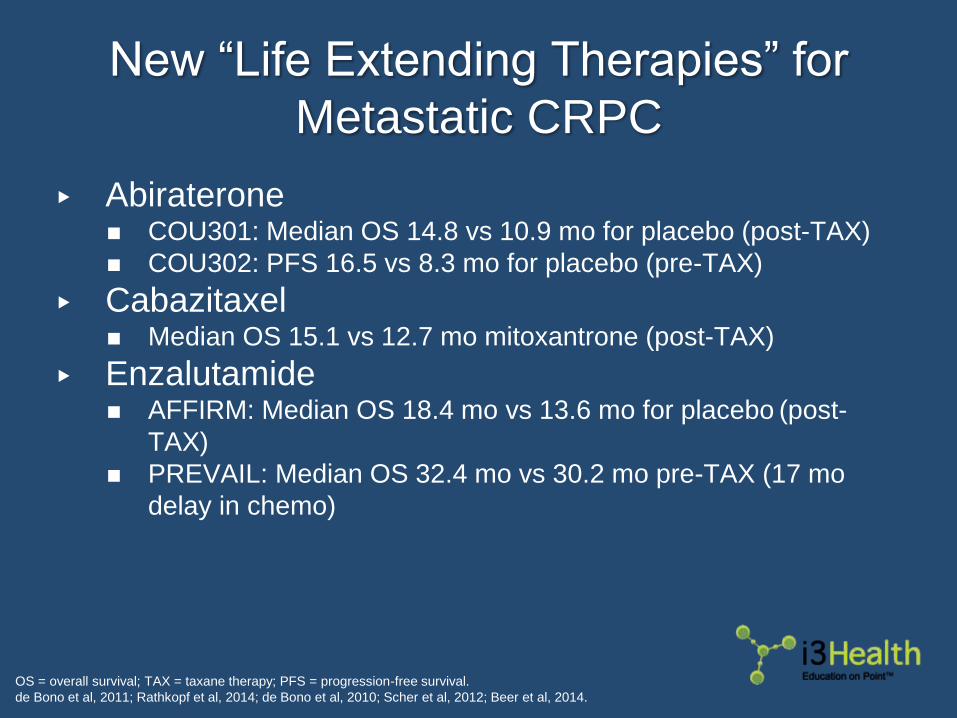
New “Life Extending Therapies” for
Metastatic CRPC
▶ Abiraterone◼ COU301: Median OS 14.8 vs 10.9 mo for placebo (post-TAX)
◼ COU302: PFS 16.5 vs 8.3 mo for placebo (pre-TAX)
▶ Cabazitaxel◼ Median OS 15.1 vs 12.7 mo mitoxantrone (post-TAX)
▶ Enzalutamide◼ AFFIRM: Median OS 18.4 mo vs 13.6 mo for placebo (post-
TAX)
◼ PREVAIL: Median OS 32.4 mo vs 30.2 mo pre-TAX (17 mo
delay in chemo)
OS = overall survival; TAX = taxane therapy; PFS = progression-free survival.
de Bono et al, 2011; Rathkopf et al, 2014; de Bono et al, 2010; Scher et al, 2012; Beer et al, 2014.
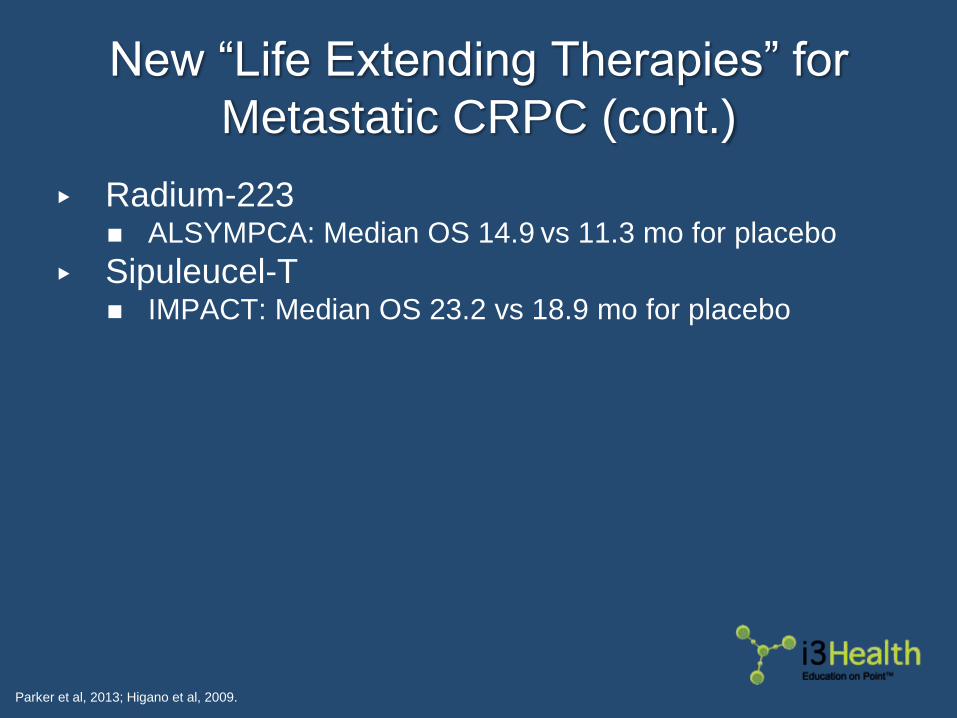
New “Life Extending Therapies” for
Metastatic CRPC (cont.)
▶ Radium-223◼ ALSYMPCA: Median OS 14.9 vs 11.3 mo for placebo
▶ Sipuleucel-T◼ IMPACT: Median OS 23.2 vs 18.9 mo for placebo
Parker et al, 2013; Higano et al, 2009.

Metastatic CRPC: Defining a
“Meaningful” Improvement in OS
Schellhammer et al, 2013.
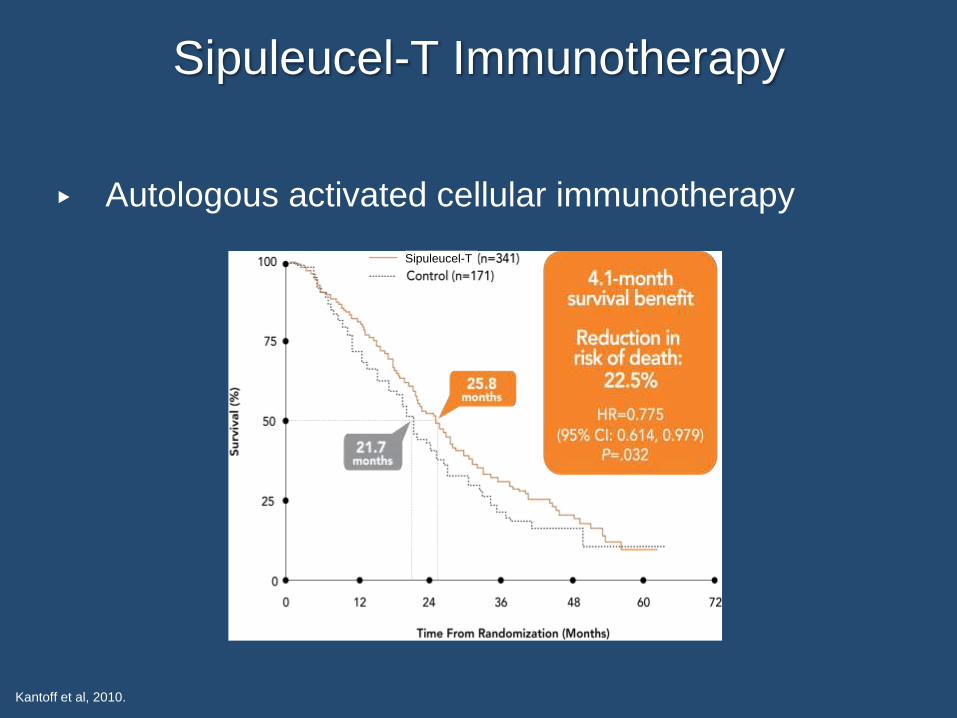
▶ Autologous activated cellular immunotherapy
Sipuleucel-T Immunotherapy
Kantoff et al, 2010.
Sipuleucel-T

Sipuleucel-T Immunotherapy (cont.)
Higano et al, 2009.

Abiraterone (CYP17 Inhibitor)
Boron & Boulpaep, 2003.
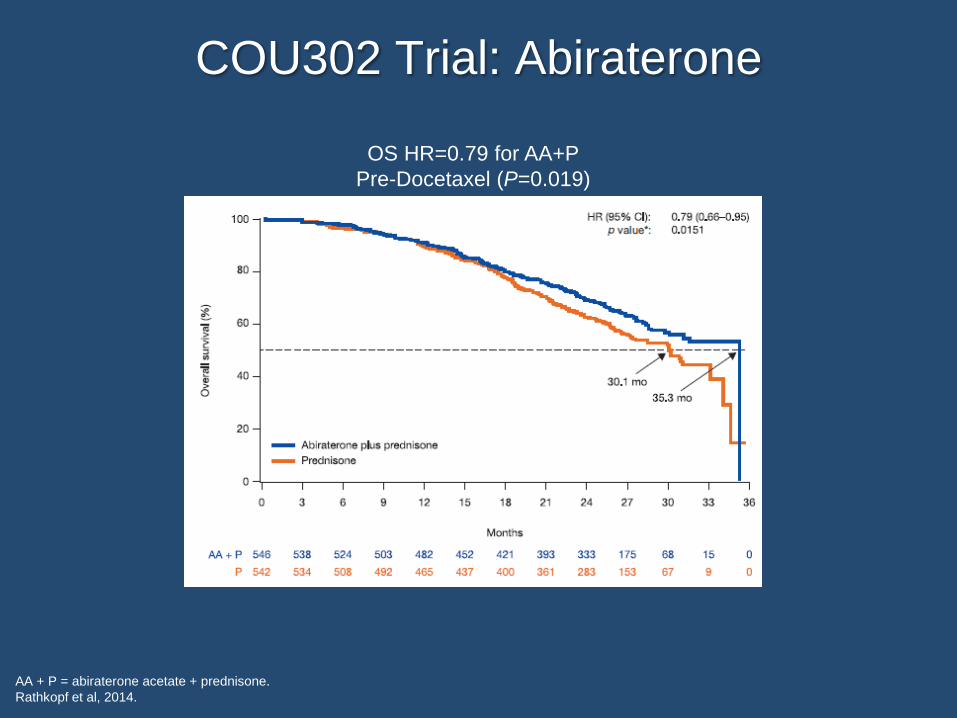
OS HR=0.79 for AA+P
Pre-Docetaxel (P=0.019)
COU302 Trial: Abiraterone
AA + P = abiraterone acetate + prednisone.
Rathkopf et al, 2014.

Abiraterone: Adverse Events
de Bono et al, 2011.

Enzalutamide:
Androgen Receptor Antagonist
Image courtesy of Tanya B. Dorff, MD.
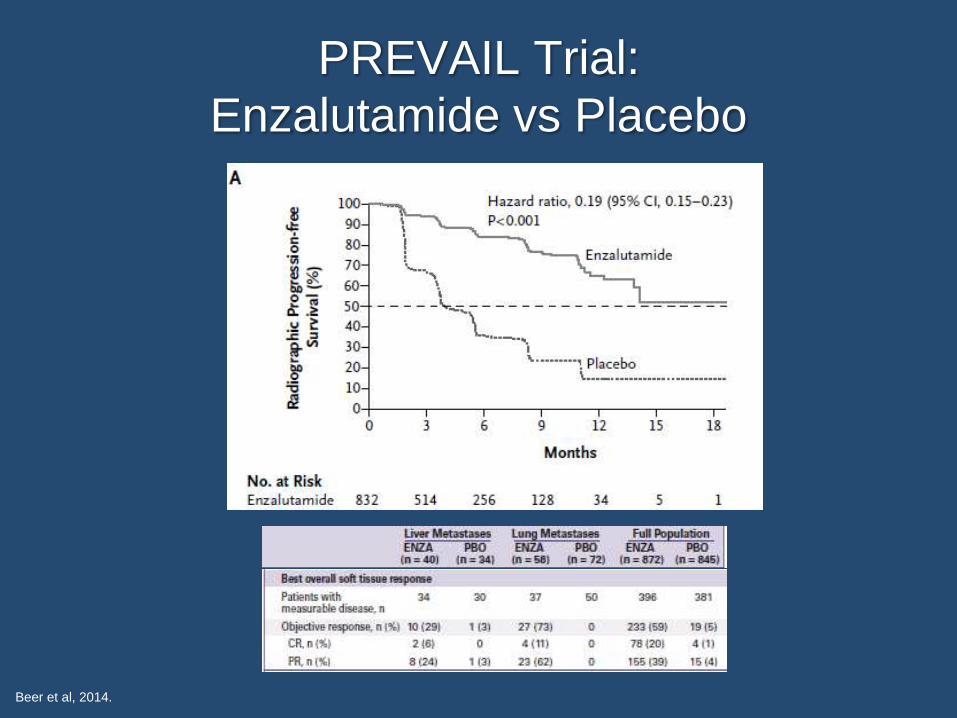
PREVAIL Trial:
Enzalutamide vs Placebo
Beer et al, 2014.

Enzalutamide: Adverse Events
Beer et al, 2014.

Petrylak et al, 2004.
SWOG 9916:
Docetaxel in Metastatic CRPC
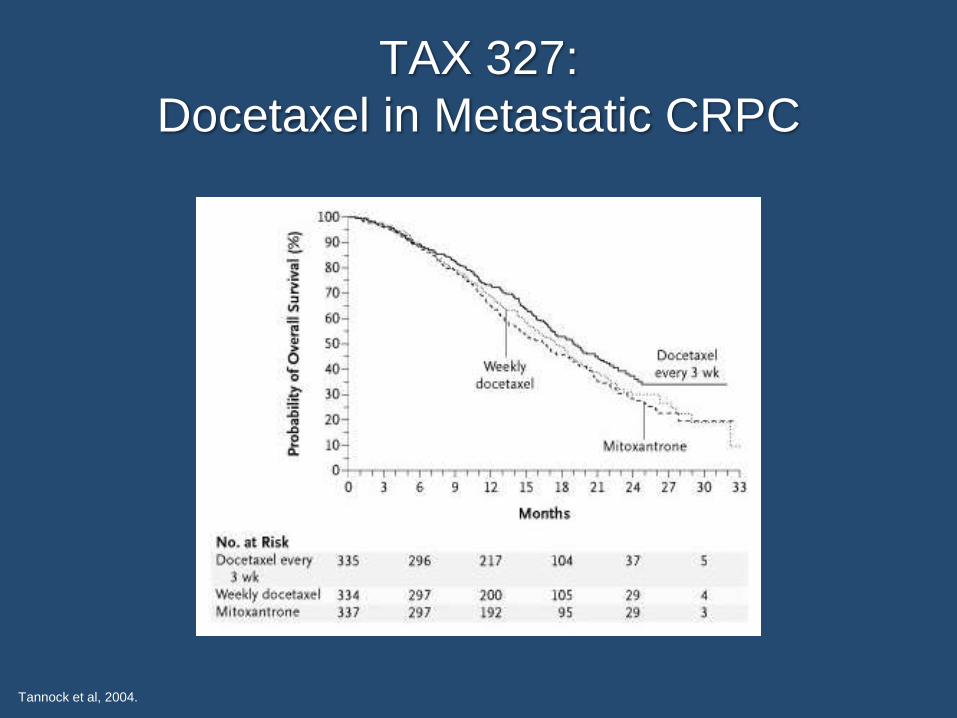
TAX 327:
Docetaxel in Metastatic CRPC
Tannock et al, 2004.

Docetaxel: Adverse Events
Tannock et al, 2004.
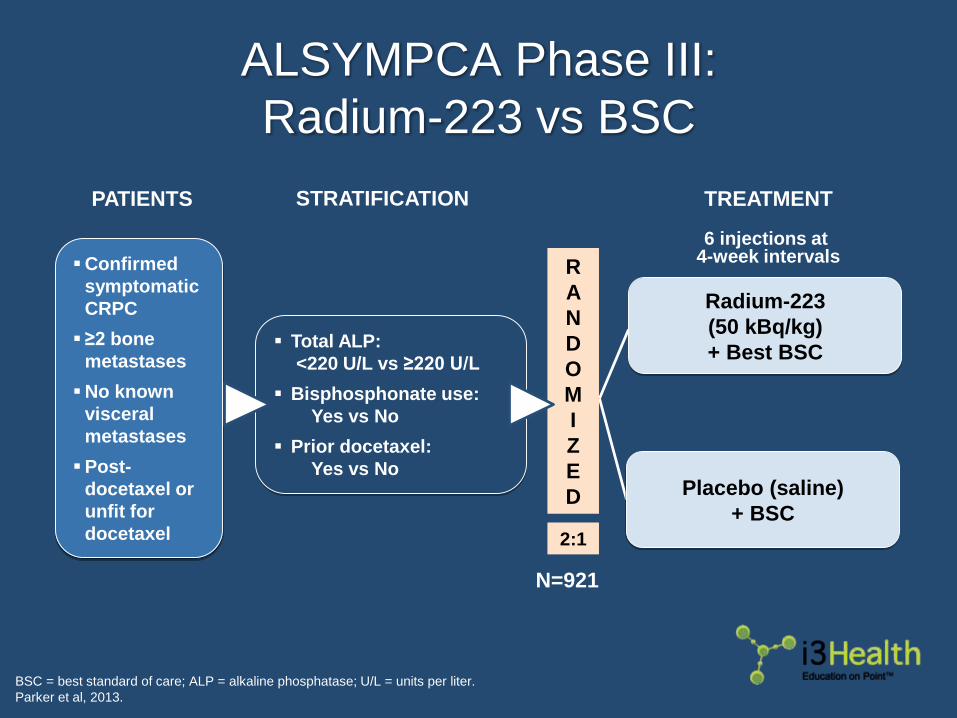
TREATMENT
6 injections at 4-week intervals
Radium-223
(50 kBq/kg)
+ Best BSC
Placebo (saline)
+ BSC
R
A
N
D
O
M
I
Z
E
D
2:1
N=921
PATIENTS
Confirmed
symptomatic
CRPC
≥2 bone
metastases
No known
visceral
metastases
Post-
docetaxel or
unfit for
docetaxel
Total ALP:
<220 U/L vs ≥220 U/L
Bisphosphonate use:
Yes vs No
Prior docetaxel:
Yes vs No
STRATIFICATION
ALSYMPCA Phase III:
Radium-223 vs BSC
BSC = best standard of care; ALP = alkaline phosphatase; U/L = units per liter.
Parker et al, 2013.

ALSYMPCA: Overall Survival
Parker et al, 2013.

ALSYMPCA: Time to First
Symptomatic Skeletal Event
Parker et al, 2016.
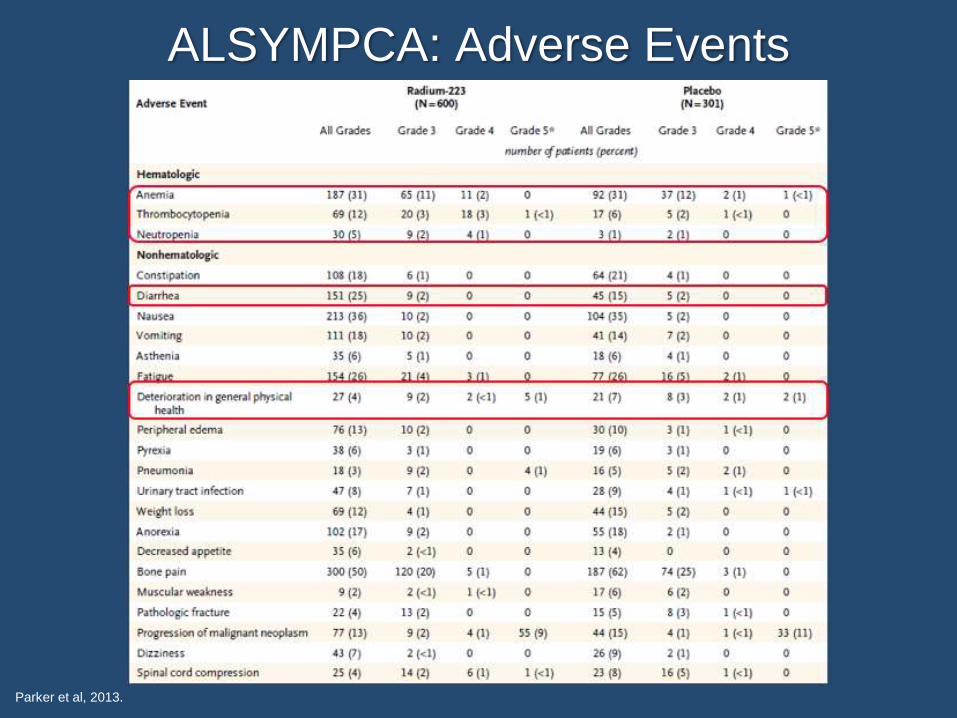
ALSYMPCA: Adverse Events
Parker et al, 2013.
Mr. JW (cont.)
How would you treat this patient?
a. Abiraterone
b. Docetaxel
c. Enzalutamide
d. Sipuleucel-T
e. Other (including combinations)

Considerations for This Patient
▶ Abiraterone◼ Impaired insulin sensitivity
▶ Enzalutamide◼ History of seizures or falls
◼ Visceral disease
▶ Docetaxel◼ Neuropathy (could substitute cabazitaxel)
◼ Risk of infection
▶ Radium-223◼ Symptomatic bone metastases without soft tissue
▶ Sipuleucel-T◼ Venous access (pheresis catheter increases risk of morbidity)
Oudard et al, 2017; NCCN, 2017.
Add bone support
with zoledronic
acid or denosumab!

Novel Combination Strategies
Trial Agents Accrual (N) Status
CTSU A031201Enza
Enza + AbiN=1,311 Completed 8/31/16
Bayer 16544
Rad223
Rad223 + Abi
Rad223 + Enza
N=68Resulted; ORR
favors combination
PEACE IIIEnza
Enza + Rad223N=560 Still recruiting
ERA 223Abi
Abi + Rad223N=806 Completed
NCT02218606Abi
Abi + CabazitaxelN=55 Recruiting
▶ No level 1 data YET to support combinations
▶ Single sequential remains standard outside of clinical
trial
Clinicaltrials.gov, 2017a; Clinicaltrials.gov, 2017b; Clinicaltrials.gov, 2017c;
Clinicaltrials.gov, 2017d; Clinicaltrials.gov, 2017e.
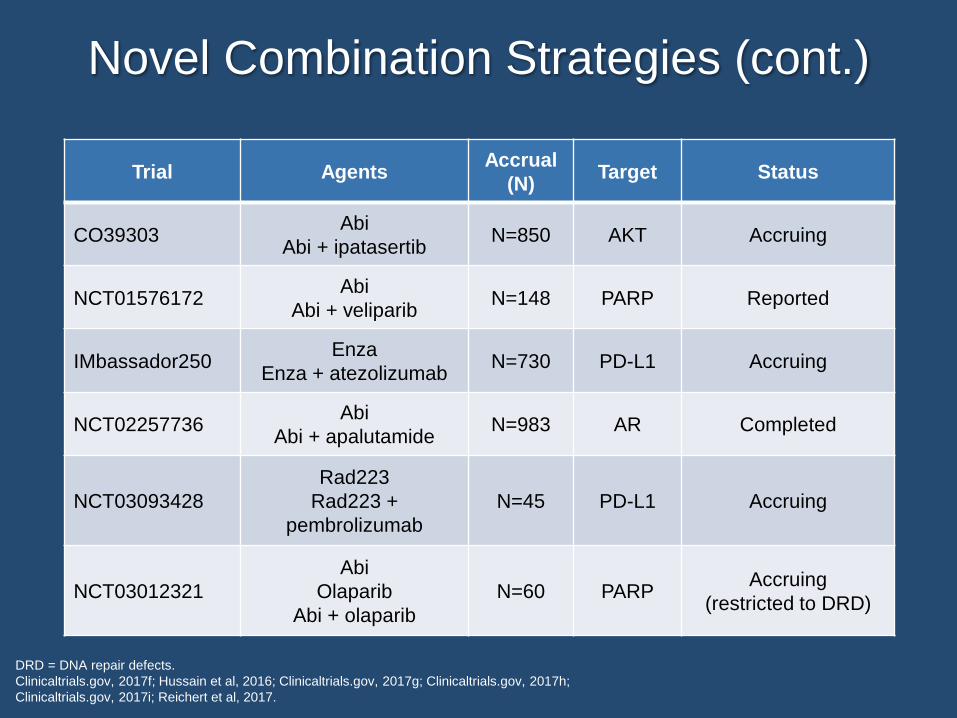
Novel Combination Strategies (cont.)
DRD = DNA repair defects.
Clinicaltrials.gov, 2017f; Hussain et al, 2016; Clinicaltrials.gov, 2017g; Clinicaltrials.gov, 2017h;
Clinicaltrials.gov, 2017i; Reichert et al, 2017.
Trial AgentsAccrual
(N)Target Status
CO39303Abi
Abi + ipatasertibN=850 AKT Accruing
NCT01576172Abi
Abi + veliparibN=148 PARP Reported
IMbassador250Enza
Enza + atezolizumabN=730 PD-L1 Accruing
NCT02257736Abi
Abi + apalutamideN=983 AR Completed
NCT03093428
Rad223
Rad223 +
pembrolizumab
N=45 PD-L1 Accruing
NCT03012321
Abi
Olaparib
Abi + olaparib
N=60 PARPAccruing
(restricted to DRD)
Mr. JW (cont.)
◼ Enrolled on clinical trial
(abiraterone with
prednisone ± dasatinib)
◼ Randomly assigned to
abiraterone
◼ Started treatment in with
baseline PSA of 5.24
ng/mL
◼ PSA decreased to
0.14 ng/mL but then
began to rise slowly
◼ PSA 2.2 ng/mL but
feeling well and no
radiographic change
May 2014 August 2015October 2014
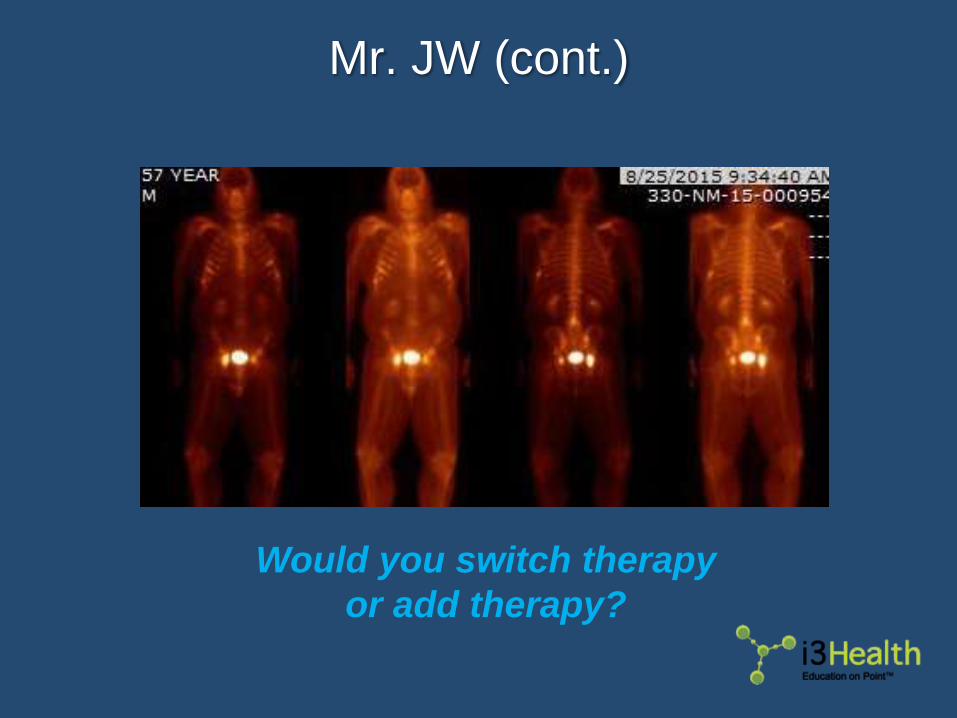
Mr. JW (cont.)
Would you switch therapy
or add therapy?
Monitoring Treatment Response
▶ PSA change alone should not be used as a trigger to
switch therapy if patients feel well and imaging
shows no change
▶ Imaging to evaluate response recommended every
8-9 weeks during first 24 weeks, then every 12
weeks
Scher et al, 2016.
Monitoring Treatment Response (cont.)
▶ Due to “flare” phenomenon (new bone lesions
despite improvement in disease) new lesions on a
bone scan at first assessment do not constitute
disease progression◼ Requires confirmation with additional new lesions on the
following scan
▶ When new lesions detected after 12 weeks,
confirmation of progression requires persistence of
the new lesions but not additional new lesions
Scher et al, 2016.
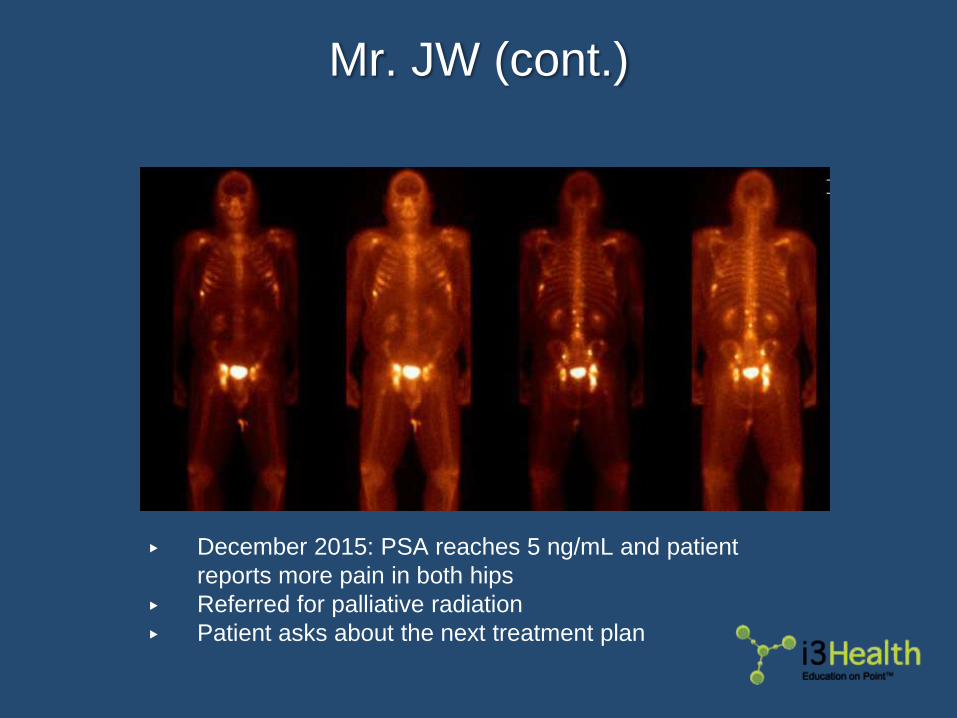
Mr. JW (cont.)
▶ December 2015: PSA reaches 5 ng/mL and patient
reports more pain in both hips
▶ Referred for palliative radiation
▶ Patient asks about the next treatment plan
Mr. JW: 55-Year-Old Man (cont.)
How would you treat this patient now?
a. Cabazitaxel
b. Docetaxel
c. Enzalutamide
d. Radium-223
e. Other (including combinations)
Do you continue abiraterone
“adding” an agent above or do you switch?
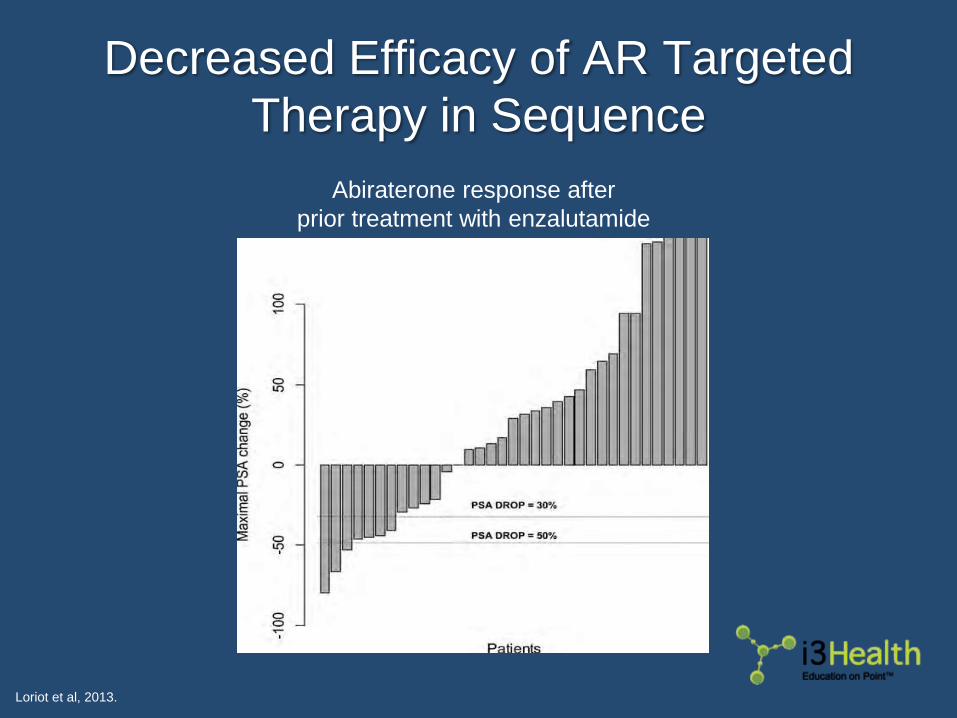
Decreased Efficacy of AR Targeted
Therapy in Sequence
Loriot et al, 2013.
Abiraterone response after
prior treatment with enzalutamide
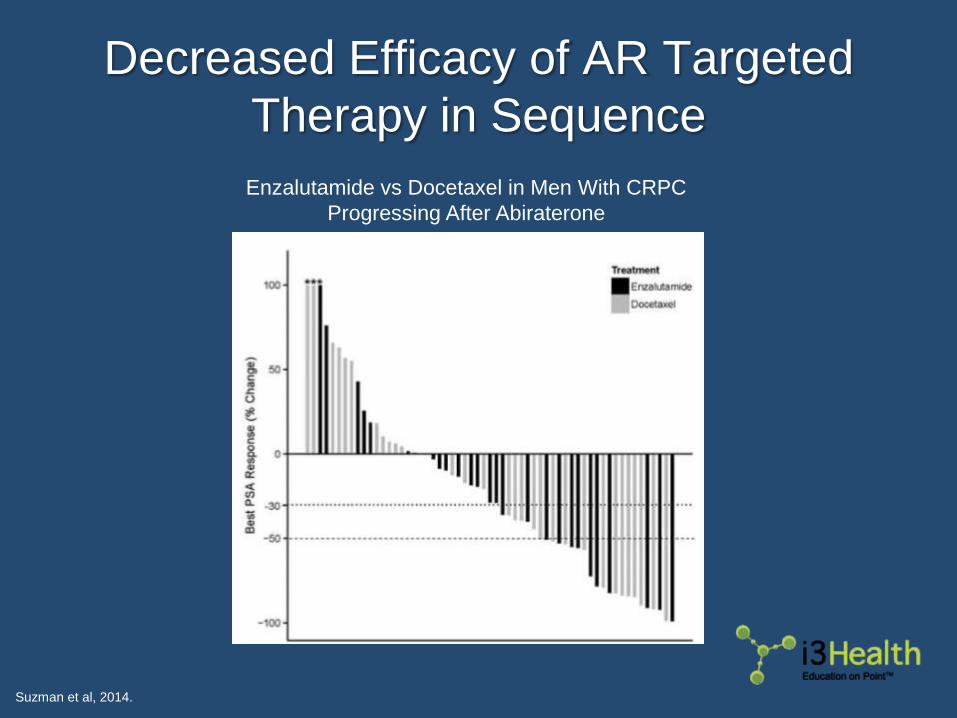
Enzalutamide vs Docetaxel in Men With CRPC
Progressing After Abiraterone
Decreased Efficacy of AR Targeted
Therapy in Sequence
Suzman et al, 2014.

GR = glucocorticoid receptor; SCC = small cell carcinoma; NEPC = neuroendocrine prostate cancer.
Watson et al, 2015.
Androgen Receptor Splice Variant-7
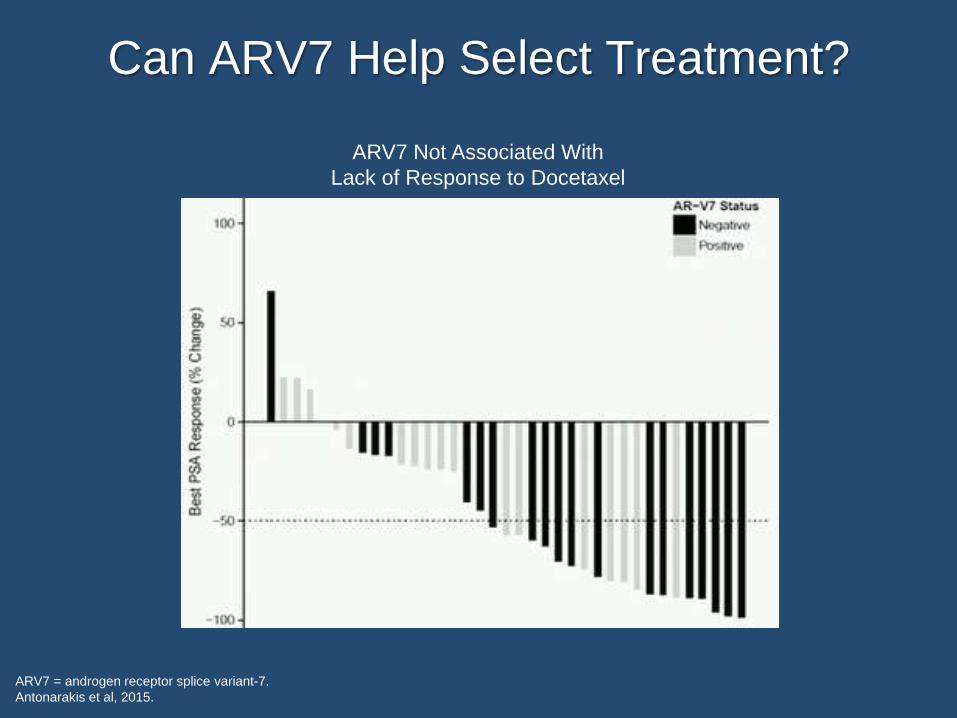
Can ARV7 Help Select Treatment?
ARV7 = androgen receptor splice variant-7.
Antonarakis et al, 2015.
ARV7 Not Associated With
Lack of Response to Docetaxel
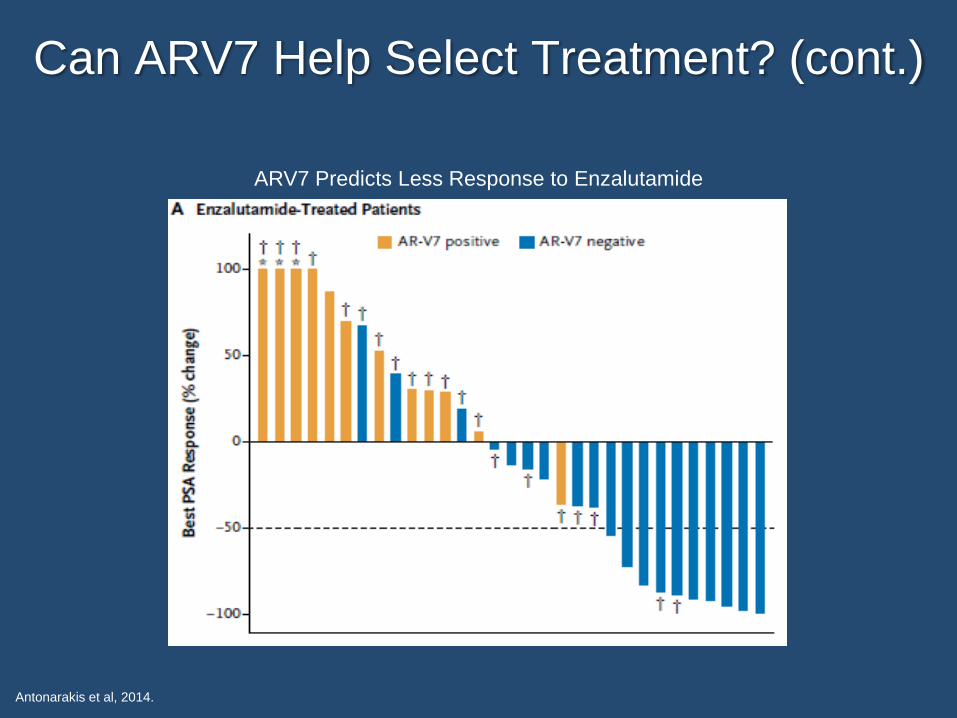
ARV7 Predicts Less Response to Enzalutamide
Antonarakis et al, 2014.
Can ARV7 Help Select Treatment? (cont.)
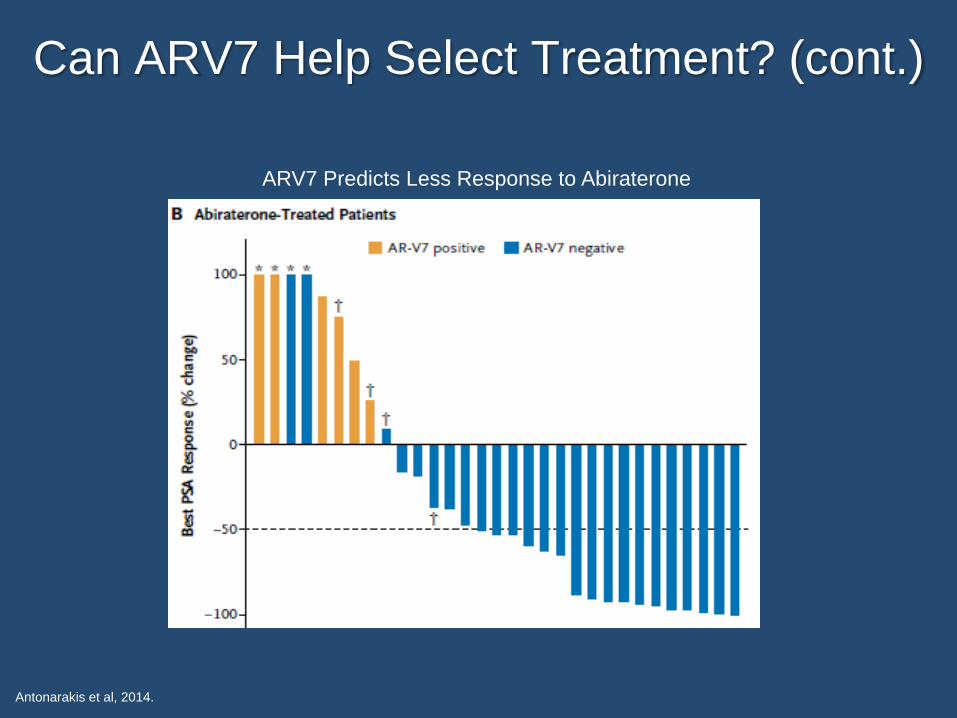
Antonarakis et al, 2014.
Can ARV7 Help Select Treatment? (cont.)
ARV7 Predicts Less Response to Abiraterone

ARV7: Not Yet Ready for Use in
Treatment Selection
TBD = to be determined; CTC = circulating tumor cell;
ddPCR = droplet digital polymerase chain reaction.
Grande et al, 2016; Scher et al, 2017; Clinicaltrials.gov, 2017j.
▶ SOGUG PREMIERE trial of
enzalutamide – PSA responses seen
in ARV7+ patients
▶ ARMOR study (in ARV7 selected
population) closed for futility◼ 953 screened, 73 enrolled
◼ PSA response 13% galeterone,
42% enzalutamide
▶ ARV7 more complicated than
originally thought◼ Amount? Timing (transient)?
◼ Localization of AR
▶ Optimal assay TBD◼ CTC based
◼ Plasma ddPCR for AR
amplification/mutation
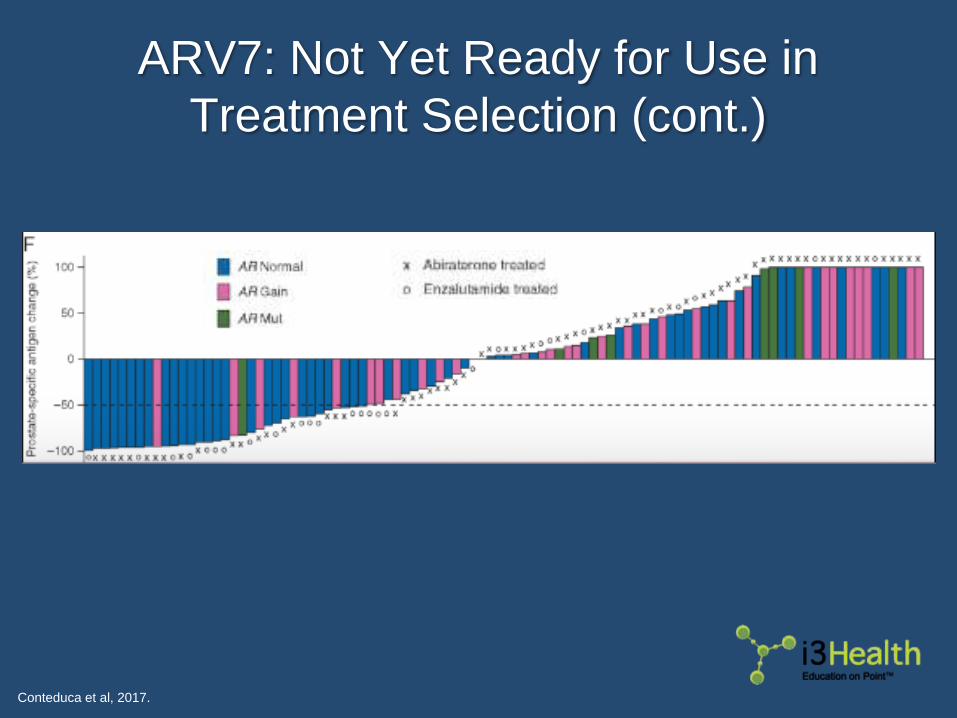
ARV7: Not Yet Ready for Use in
Treatment Selection (cont.)
Conteduca et al, 2017.

Are CTC Counts Useful in Managing
Patients With Metastatic CRPC?
de Bono et al, 2008.

Single Sequential Remains
the Standard Paradigm
Attard et al, 2017.
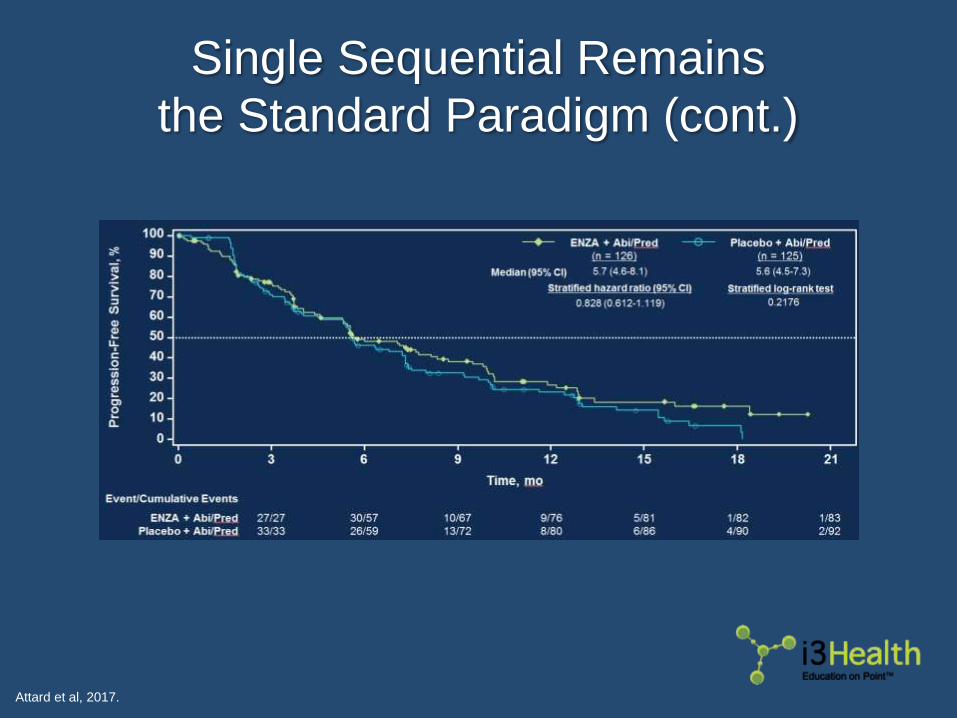
Single Sequential Remains
the Standard Paradigm (cont.)
Attard et al, 2017.

Mr. JW (cont.)
▶ Abiraterone was discontinued
▶ Received docetaxel x 8 cycles with stable disease
▶ Upon PSA progression received enzalutamide ◼ A few months later radium-223 was added due to emerging
bone pain
▶ Now PSA is rising again. Patient has good
performance status and organ function

Non-AR Targeted Agents
Under Investigation
Agent(s) Target Select Population Phase of Trial
Niraparib, Olaparib,
Rucaparib, TalazoparibPARP
DNA repair deficient
or non-selected (in combinations)II and III
Cabozantinib VEGF, c-Met Unselected Ib/II (with ipi/nivo)
Palbociclib CDK4/6 Unselected II
Pembrolizumab PD-1 Progressing on enzalutamide II
Durvalumab ±
Tremelimumab
PD-L1
CTLA4Unselected II
Lu177-j591 PSMA Unselected II
MLN 8237 (alisertib) Aurora
KinaseSmall cell/neuroendocrine II
GSK525762 BET Progression on enza/abi Ib
LY2606368 Chk1/2 BRCA mutated I
Mateo et al, 2015; Ryan et al, 2017; Reinstein et al, 2017; Clinicaltrials.gov, 2017k; Graff et al, 2016a; Silvestri et al, 2016; Tagawa
et al, 2013; Graff et al, 2016b; Clinicaitrials.gov, 2017l; Clinicaltrials.gov, 2017m. Clinicaltrials.gov, 2017n.

DNA Repair Deficiency Predicts
Response to PARP Inhibitors
PARP = poly ADP ribose polymerase.
de Lartigue, 2013.
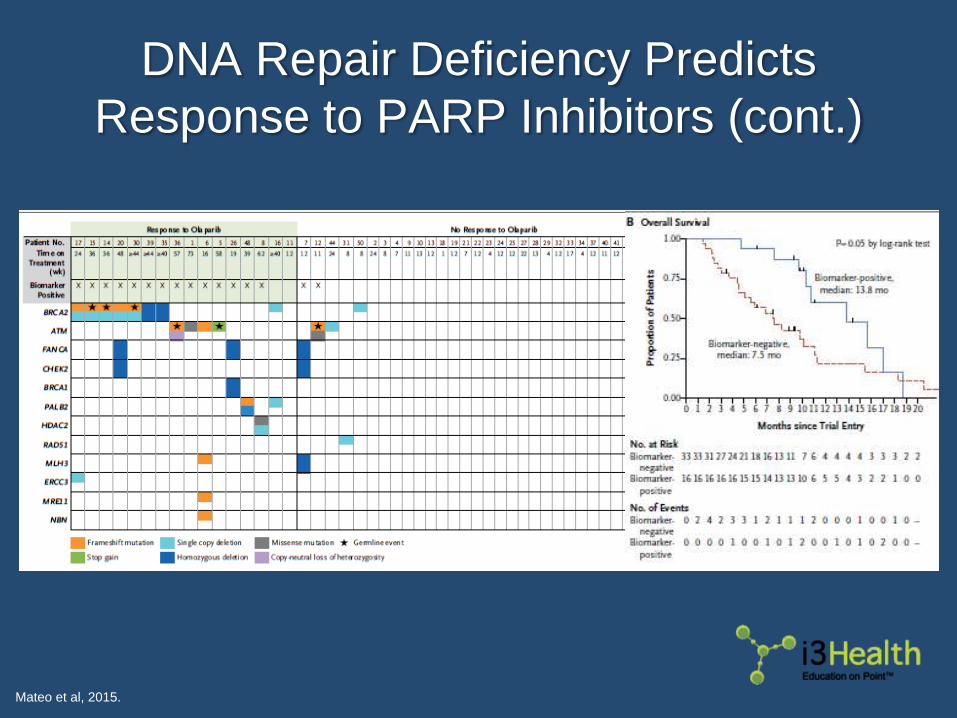
DNA Repair Deficiency Predicts
Response to PARP Inhibitors (cont.)
Mateo et al, 2015.
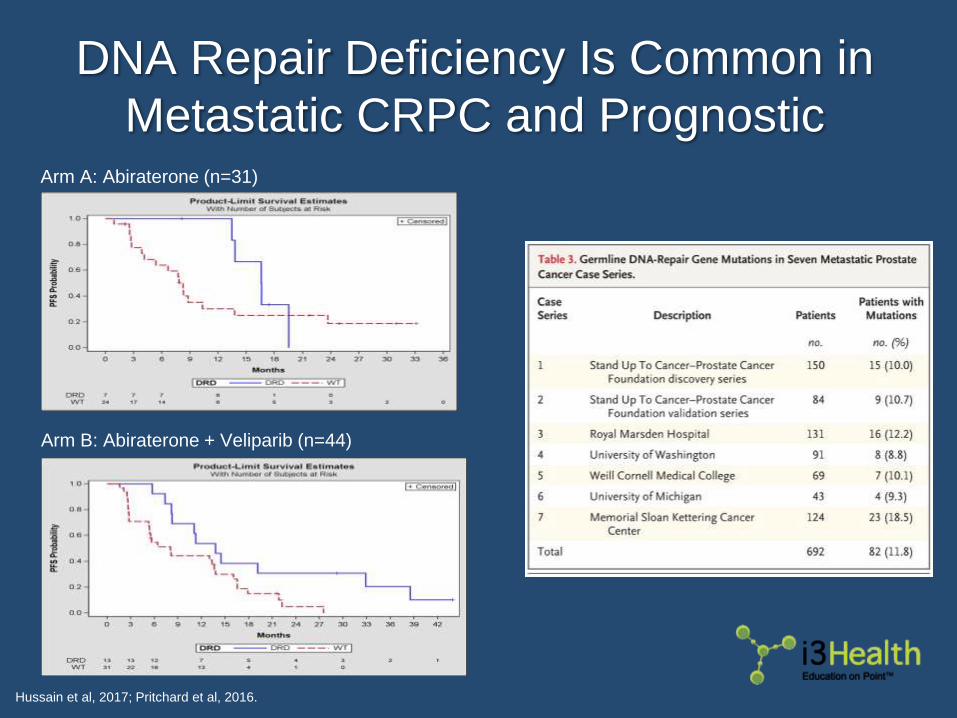
DNA Repair Deficiency Is Common in
Metastatic CRPC and Prognostic
Hussain et al, 2017; Pritchard et al, 2016.
Arm A: Abiraterone (n=31)
Arm B: Abiraterone + Veliparib (n=44)

Key Takeaways
▶ Single sequential treatment remains only strategy with
level 1 evidence◼ Combination trials underway/completed
▶ Imaging is important for monitoring treatment response◼ PSA rise alone usually not enough to indicate treatment
change
▶ No current biomarker to select patients for treatment◼ DNA repair deficiency may select for PARP inhibitor, common
in metastatic prostate cancer. Consider screening
◼ ARV7 assay needs validation before implementation

Key Takeaways (cont.)
▶ Future treatment may include immune checkpoint
inhibitors and/or PARP inhibitors
Consider referring for clinical trials early
given that combination trials with standard
agents are very common.

Audience Q&AsUse the Questions section of your Control Panel
to submit questions to the faculty.

To receive CME/CE credit visit:
www.i3health.com/CRPC

References
Antonarakis ES, Lu C, Chen Y, et al (2015). AR splice variant 7 (AR-V7) and response to taxanes in men with metastatic castration-resistant
prostate cancer (mCRPC). J Clin Oncol (2015 Genitourinary Cancers Symposium Abstracts), 33(suppl 7). Abstract 138.
Antonarakis ES, Lu C, Wang H, et al (2014). AR-V7 and resistance to enzalutamide and abiraterone in prostate cancer. N Engl J Med,
371(11):1028-1038. DOI:10.1056/nejmoa1315815
Attard G, Borre M, Gurney H, et al (2017). A phase IV, randomized, double-blind, placebo (PBO)-controlled study of continued enzalutamide
(ENZA) post prostate-specific antigen (PSA) progression in men with chemotherapy-naive metastatic castration-resistant prostate
cancer (mCRPC). J Clin Oncol (ASCO Annual Meeting Abstracts), 35(uppl 15). Abstract 5004.
Beer TM, Armstrong AJ, Rathkopf DE, et al (2014). Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med,
371(5):424-433. DOI:10.1056/nejmoa1405095
Boron WF & Boulpaep EL (2003). In: Medical Physiology: A Cellular and Molecular Approach, Elsevier/Saunders.
Clinicaltrials.gov (2017a). Enzalutamide with or without abiraterone and prednisone in treating patients with castration-resistant metastatic
prostate cancer. NLM identifier: NCT01949337
Clinicaltrials.gov (2017b). A randomized phase IIa efficacy and safety study of radium-223 dichloride with abiraterone acetate or enzalutamide in
metastatic castration-resistant prostate cancer (CRPC). NLM identifier: NCT02034552
Clinicaltrials.gov (2017c). Phase III radium-223 mCRPC-PEACE III. NLM idenfifier: NCT02194842
Clinicaltrials.gov (2017d). Radium-223 dichloride and abiraterone acetate compared to placebo and abiraterone acetate for men with cancer of
the prostate when medical or surgical castration does not work and when the cancer has spread to the bone, has not been treated with
chemotherapy and is causing no or only mild symptoms (ERA 223). NLM identifier: NCT02043678
Clinicaltrials.gov (2017e). Multicenter trial of abiraterone acetate with or without cabazitaxel in treatment of metastatic castration resistant
prostate cancer. NLM identifier: NCT02218606
Clinicaltrials.gov (2017f). Ipatasertib plus abiraterone plus prednisone/prednisolone, relative to placebo plus abiraterone plus
prednisone/prednisolone in adult male patients with metastatic castrate-resistant prostate cancer (IPATential150). NLM identifier:
NCT03072238
Clinicaltrials.gov (2017g). A study of atezolizumab (anti-PD-L1 antibody) in combination with enzalutamide in participants with metastatic
castration-resistant prostate cancer (mCRPC) after failure of an androgen synthesis inhibitor and failure of, ineligibility for, or refusal of
a taxane regimen (IMbassador250). NLM identifier: NCT03016312
Clinicaltrials.gov (2017h). An efficacy and safety study of apalutamide (JNJ-56021927) in combination with abiraterone acetate and prednisone
versus abiraterone acetate and prednisone in participants with chemotherapy-naive metastatic castration-resistant prostate cancer
(mCRPC). NLM identifier: NCT02257736
References
Clinicaltrials.gov (2017i). Study evaluating the addition of pembrolizumab to radium-223 in mCRPC. NLM idenfier: NCT03093428
Clinicaltrials.gov (2017j). A study of galeterone compared to enzalutamide in men expression androgen receptor splice varian—7 mRNA (AR-
V7) metastatic CRPC (ARMOR3-SV). NLM identifier: NCT002438007
Clinicaltrials.gov (2017k). Cabozantinib-s-malate and nivolumab with or without ipilimumab in treating patients with metastatic genitourinary
tumors. NLM identifier: NCT02496208
Clinicaltrials.gov (2017l). Palbociclib in patients with metastatic castration-resistant prostate cancer. NLM identifier: NCT02905318
Clinicaltrials.gov (2017m). Dose escalation and dose expansion study of GSK525762 in combination with androgen deprivation therapy and
other agents in subjects with castrate-resistant prostate cancer. NLM identifier: NCT03150056
Clinicaltrials.gov (2017n). A phase II single arm pilot study of the ChL1/2 inhibitor (LY2606368) in BRCA1/2 mutation associated breast or
ovarian cancer, triple negative breast cancer, high grade serous ovarian cancer, and metastatic castrate-resistant prostate cancer. NLM
identifier: NCT02203513
Conteduca V, Wetterskog D, Sharabiani MTA, et al (2017). Androgen receptor gene status in plasma DNA associates with worse outcome on
enzalutamide or abiraterone for castration-resistant prostate cancer: a multi-institution correlative biomarker study. Ann Onc, 28:1508-
1516. DOI:10.1093/annonc/mdx155
de Bono JS, Logothetis CJ, Molina A, et al (2011). Abiraterone and increased survival in metastatic prostate cancer. N Engl J Med,
364(21):1995-2005. DOI:10.1056/nejmoa1014618
de Bono JS, Oudard S, Ozguroglu M, et al (2010). Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate
cancer progressing after docetaxel treatment: a randomised open-label trial. Lancet, 376(9747):1147-1154. DOI:10.1016/s0140-
6736(10)61389-x
de Bono JS, Scher HI, Montgomery RB, et al (2008). Circulating tumor cells predict survival benefit from treatment in metastatic castration-
resistant prostate cancer. Clin Cancer Res, 14(19):6302-6309. DOI:10.1158/1078-0432.CCR-08-0872
de Lartigue J (2013). New life for PARP inhibitors: emerging agents leave mark at ASCO. OncLive. Available at:
http://www.onclive.com/publications/oncology-live/2013/august-2013/new-life-for-parp-inhibitors-emerging-agents-leave-mark-at-
asco?p=1
Graff JN, Alumkal JJ, Drake CG, et al (2016a). Early evidence of anti-PD-1 activity in enzalutamide-resistant prostate cancer. Oncotarget,
7(33):52810-52817. DOI:10.18632/oncotarget.10547
Graff JN, Higano CS, Hahn NM, et al (2016b). Open-label, multicenter, phase 1 study of alisertib (MLN8237), an aurora A kinase inhibitor, with
docetaxel in patients with solid tumors. Cancer, 122(16):2524-2533. DOI:10.1002/cncr.30073

References
Grande E, Fernandez Perez MP, Font A, et al (2016). Early responses to enzalutamide in AR-V7 positive first line metastatic castration-resistant
prostate cancer (mCRPC). A prospective SOGUG clinical trial: the PREMIERE study. Ann Onc (ESMO 2016 Annual Meeting
Abstracts), 27(suppl 6). Abstract 726PD.
Higano CS, Schellhammer PF, Small EJ, et al (2009). Integrated data from 2 randomized, double-blind, placebo-controlled, phase 3 trials of
active cellular immunotherapy with sipuleucel-T in advanced prostate cancer. Cancer, 115(16):3670-3679. DOI:10.1002/cncr.24429
Hussain M, Daignault S, Twardowski P, et al (2017). Abiraterone + prednisone (Abi) +/- veliparib (Vel) for patients (pts) with metastatic
castration-resistant prostate cancer (CRPC): NCI 9012 updated clinical and genomics data. J Clin Oncol (ASCO Annual Meeting
Abstracts), 35. Abstract 5001.
Hussain M, Daignault S, Twardowski P, et al (2016). Co-targeting androgen receptor (AR) and DNA repair: a randomized ETS gene fusion-
stratified trial of abiraterone + prednisone (Abi) +/- the PARP1 inhibitor veliparib for metastatic castration-resistant prostate cancer
(mCRPC). J Clin Oncol (ASCO Annual Meeting Abstracts), 34. Abstract 5010.
Kantoff PW, Higano CS, Shore ND, et al (2010). Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med,
363(5):411-422. DOI:10.1056/nejmoa1001294
Loriot Y, Bianchini D, Ileana E, et al (2013). Antitumor activity of abiraterone acetate against metastatic castration-resistant prostate cancer
progressing after docetaxel and enzalutamide (MDV-3100). Ann Oncol, 24(7):1807-1812. DOI:10.1093/annonc/ndt136
Mateo J, Carreira S, Sandhu S, et al (2015). DNA-repair defects and olaparib in metastatic prostate cancer. N Engl J Med, 373(18):1697-1708.
DOI:10.1056/nejmoa1506859
National Comprehensive Cancer Network (2017). NCCN Clinical Practice Guidelines in Oncology: prostate cancer. Version 2.2017. Available
at: http://www.nccn.org
Oudard S, Fizazi K, Sengeløv L, et al (2017). Cabazitaxel versus docetaxel as first-line therapy for patients with metastatic castration-resistant
prostate cancer: a randomized phase III trial-FIRSTANA. J Clin Oncol. [Epub ahead of print] DOI: 10.1200/JCO.2016.72.1068
Parker C, Nilsson S, Heinrich D, et al (2013). Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med, 369(3):213-
223. DOI:10.1056/nejmoa1213755
Petrylak DP, Tangen CM, Hussain MHA, et al (2004). Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced
refractory prostate cancer. N Engl J Med, 351(15):1513-1520. DOI:10.1056/nejmoa041318
Pritchard CC, Mateo J, Walsh MF, et al (2016). Inherited DNA-repair gene mutations in men with metastatic prostate cancer. N Engl J Med,
374(5):443-453. DOI:10.1056/nejmoa1603144

References
Rathkopf DE, Smith MR, de Bono JS, et al (2014). Updated interim efficacy analysis and long-term safety of abiraterone acetate in metastatic
castration-resistant prostate cancer patients without prior chemotherapy (COU-AA-302). Eur Urol, 66(5):815-825.
DOI:10.1016/j.eururo.2014.02.056
Reichert Z, Carneiro BA, Daighnault-Newton S, et al (2017). A randomized phase II trial of abiraterone, olaparib, or abiraterone + olaparib in
patients with metastatic castration-resistant prostate cancer with DNA repair defects. J Clin Oncol, 35(15_suppl).
DOI:10.1200/JCO.2017.35.15_suppl.TPS5086
Schellhammer PF, Chodak G, Whitemore JB, et al (2013). Lower baseline prostate-specific antigen is associated with a greater overall survival
benefit from sipuleucel-T in the immunotherapy for prostate adenocarcinoma treatment (IMPACT) trial. Urology, 81(6):1297-1302.
DOI:10.1016/j.urology.2013.01.061
Scher HI, Fizazi K, Saad F, et al (2012). Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med,
367(13):1187-1197. DOI:10.1056/nejmoa1207506
Scher HI, Graf RP, Schreiber NA et al (2017). Nuclear-specific AR-V7 protein localization is necessary to guide treatment selection in metastatic
castration-resistant prostate cancer. Eur Urol, 71(6):874-882. DOI:10.1016/j.eururo.2016.11.024
Scher HI, Morris MJ, Stadler WM, et al (2016). Trial design and objectives for castration-resistant prostate cancer: updated recommendations
from the prostate cancer clinical trials working group 3. J Clin Oncol, 34(12):1402-1418. DOI:10.1200/jco.2015.64.2702
Silvestri I, Cattarino S, Giantulli S, et al (2016). A perspective of immunotherapy for prostate cancer. Cancers (Basel), 8(7):64.
DOI:10.3390/cancers8070064
Suzman DL, Luber B, Schweizer MT, et al (2014). Clinical activity of enzalutamide versus docetaxel in men with castration-resistant prostate
cancer progressing after abiraterone. Prostate, 74(13):1278-1285. DOI:10.1002/pros22844
Tagawa ST, Milowsky MI, Morris M, et al (2013). Phase II study of Lutetium-177-labeled anti-prostate-specific membrane antigen monoclonal
antibody J591 for metastatic castration-resistant prostate cancer. Clin Cancer Res, 19(18):5182-5191. DOI:10.1158/1078-0432.CCR-
13-0231
Tannock IF, de Wit R, Berry WR, et al (2004). Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl
J Med, 351(15):1502-1512. DOI:10.1056/nejmoa040720
Watson PA, Arora VK & Sawyers CL (2015). Emerging mechanisms of resistance to androgen receptor inhibitors in prostate cancer. Nat Rev
Cancer, 15(12):701-711. DOI:10.1038/nrc4016