
Decentralisation Initiatives in Gujarat Health Sector Reforms Department of Health & FW Government...
34
Decentralisation Decentralisation Initiatives in Gujarat Initiatives in Gujarat Health Sector Reforms Health Sector Reforms Department of Health & FW Department of Health & FW Government of Gujarat Government of Gujarat
-
date post
19-Dec-2015 -
Category
Documents
-
view
228 -
download
2
Transcript of Decentralisation Initiatives in Gujarat Health Sector Reforms Department of Health & FW Government...
Decentralisation Initiatives in Decentralisation Initiatives in Gujarat Gujarat
Health Sector ReformsHealth Sector Reforms
Department of Health & FWDepartment of Health & FWGovernment of GujaratGovernment of Gujarat
Decentralisation Initiatives in Decentralisation Initiatives in Gujarat Gujarat
Health Sector ReformsHealth Sector Reforms
Department of Health & FWDepartment of Health & FWGovernment of GujaratGovernment of Gujarat

Gujarat – A ProfileGujarat – A Profile
Overview
Area 196,000 km 6% of India
Population 50.5 million 5% of India
Urbanization 37% India avg. 28%
SDP(2003-04)
Rs 1,425.60 billion(€ 26.40 bill.)
6.33% of India
Per Capita Income(2003-04)
Rs 26,979 (€ 496.24)
India average -Rs. 20,989 (€ 388.69)
The Planning Commission has set a target growth rate of 10% p.a. for Gujarat

BackgroundBackground
The Sector Investment Programme (SIP) The Sector Investment Programme (SIP) started in Gujarat in January 2000, initially in started in Gujarat in January 2000, initially in two districts, Narmada and Rajkot two districts, Narmada and Rajkot
Following the earthquake in January 2001, 9 Following the earthquake in January 2001, 9 affected districts were also taken up to affected districts were also taken up to implement Reforms with Reconstructionimplement Reforms with Reconstruction
In January 2005 the remaining 14 districts In January 2005 the remaining 14 districts were also covered under the SIP, making a were also covered under the SIP, making a total of 25 districtstotal of 25 districts

Institutional mechanismsInstitutional mechanisms
The State Health Sector Reform Cell The State Health Sector Reform Cell constituted in 1999 for the EC supported SIPconstituted in 1999 for the EC supported SIP
Standing Committee On Voluntary Action Standing Committee On Voluntary Action was created in early 2000 to expedite the was created in early 2000 to expedite the disbursement of fundsdisbursement of funds
The Reconstruction Sub Committee The Reconstruction Sub Committee constituted in 2002 for post earthquake constituted in 2002 for post earthquake activities activities

Following the earthquake the State Programme Following the earthquake the State Programme Implementation Unit established to manage and Implementation Unit established to manage and administer the Repairs and Reconstruction of health administer the Repairs and Reconstruction of health facilities. facilities.
DPIUs were established to monitor and supervise the DPIUs were established to monitor and supervise the Repair and Reconstruction works at local level.Repair and Reconstruction works at local level.
District Agencies at the district level to manage the District Agencies at the district level to manage the reform component. They prepared their own District reform component. They prepared their own District Action Plans in consultation with the community and the Action Plans in consultation with the community and the health functionaries to meet the local needs.health functionaries to meet the local needs.
Flexibility in re-allocation of funds at the State and the Flexibility in re-allocation of funds at the State and the District level according to the need and priority.District level according to the need and priority.

SRC
RSC
SPIU
DPIU District agency
Government Policy Resolutions Government Policy Resolutions
1.1. Delegation of Powers to Medical Officers PHCs, District Delegation of Powers to Medical Officers PHCs, District Societies and Additional Director (Family Welfare)Societies and Additional Director (Family Welfare)
2.2. Delegation of financial and administrative powers to Delegation of financial and administrative powers to Medical Colleges, District Hospitals, Community Health Medical Colleges, District Hospitals, Community Health Centres (CHCs) and PHCsCentres (CHCs) and PHCs
3.3. Establishment of Block Health Offices (BHOs)Establishment of Block Health Offices (BHOs)
4.4. Formation of Rogi Kalyan samitiesFormation of Rogi Kalyan samities

Decentralisational processes in repair and Decentralisational processes in repair and reconstructionreconstruction
Approval from Dy.Eng
Write to Deputy Engineer
Inspection by Section Officer
Prepare plan & estimates
Administrative sanctionby CDHO
Technical Sanction by Executive Engineer
Repair carried out ?
Repair required
Earlier
Total dependence on R&B
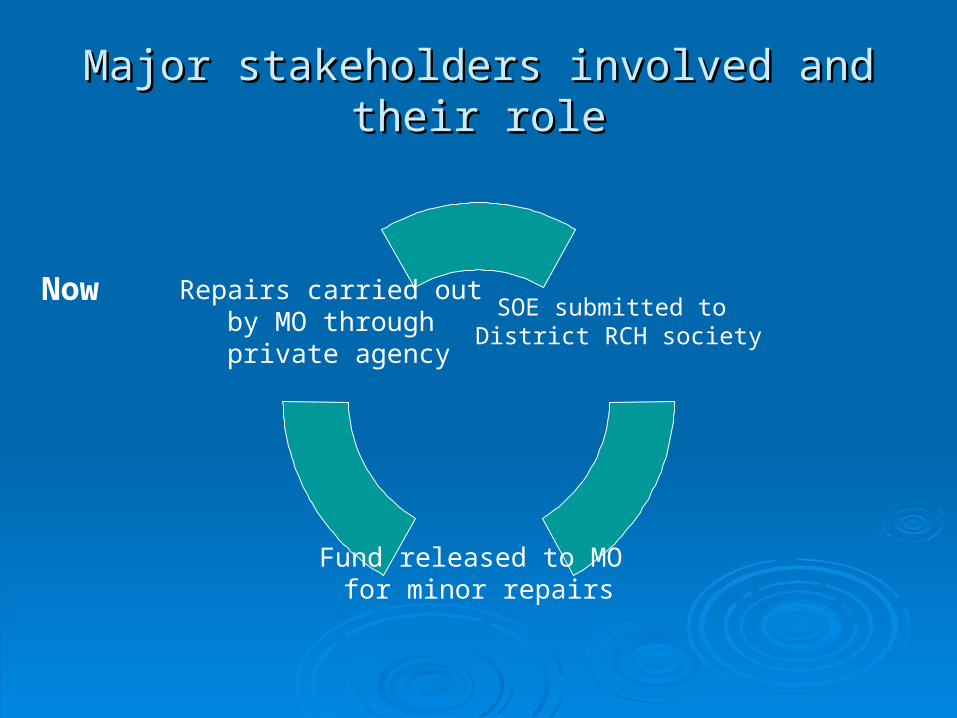
Major stakeholders involved and their roleMajor stakeholders involved and their role
NowSOE submitted to
District RCH society
Fund released to MO for minor repairs
Repairs carried out by MO through private agency

Monitoring and EvaluationMonitoring and Evaluation
Monthly Physical and Financial Monthly Physical and Financial Progress Report (SOE)Progress Report (SOE)
Supervisory visits by state and district Supervisory visits by state and district program managersprogram managers
Review in District RCH society Review in District RCH society meetings and review in state and district meetings and review in state and district level meetings level meetings
IssuesIssues
Lack of trust and fear - Funds could not be utilized Lack of trust and fear - Funds could not be utilized in a few districts where District RCH societies did in a few districts where District RCH societies did not release fund to MOnot release fund to MO
Fund flow to MOs delayed due to lack of Bank Fund flow to MOs delayed due to lack of Bank Account but now streamlinedAccount but now streamlined
Proper orientation to stake holders on purpose, Proper orientation to stake holders on purpose, process and output requiredprocess and output required
Delegation of powers only for donor agency fund, Delegation of powers only for donor agency fund, now being institutionalisednow being institutionalised

Work carried out by PIU (RSRR)Work carried out by PIU (RSRR)
ParticularsParticulars Total Total StructuresStructures
Provisionally Provisionally Handed OverHanded Over
Under Under ProgressProgress
Total Cost Total Cost ((Rs. in Rs. in Crores)Crores)
Major StructuresMajor Structures(GH, CHC,PHC)(GH, CHC,PHC) 177177 5858 118118
59.0659.06Minor StructuresMinor Structures(Disp, SC,SQ)(Disp, SC,SQ) 853853 419419 434434
TotalTotal 10301030 477477 552552

Progress Report NC -1Progress Report NC -1
Particulars Total Structures Under ProgressTotal Cost
(Rs. in Crores)
AH 2 0
33.60
PHC 6 6
Disp 3 1
SC 9 5
Staff Quarters 245 96
Total 264 108

POST EARTHQUAKE REDEVELOPMENT PROGRAMMEPOST EARTHQUAKE REDEVELOPMENT PROGRAMMENEW CONSTRUCTION (Pipeline)NEW CONSTRUCTION (Pipeline)
Particulars Total StructuresTotal Cost
(Rs. in Crores)
CHC 1
76 crores
AH 1
PHC 22
SC 45
DISP 4
TB clinics 1
Staff Quarters 113
Aganwadies 472
CDPO 12
Total 676

ChiranjiviChiranjivi

OBJECTIVES- OBJECTIVES-
Vision 2010, Population Policy & RCH Vision 2010, Population Policy & RCH IIII
Reduce MMR from 389 (in 1998) to Reduce MMR from 389 (in 1998) to 100 per 100,000 live births by 2010100 per 100,000 live births by 2010
Reduce IMR from 60 to 30 by 2010Reduce IMR from 60 to 30 by 2010
Stabilize population by reducing TFRStabilize population by reducing TFR from 3.0 to 2.1 by 2010from 3.0 to 2.1 by 2010

Maternal Mortality: Maternal Mortality: UK 1840–1960UK 1840–1960
0
100
200
300
400
500
MaternalDeaths
Improvements in nutrition, sanitation
Antibiotics, banked blood, surgical improvements
Antenatal care
Maine 1999.

Maternal Mortality ReductionMaternal Mortality ReductionSri Lanka 1940–1985Sri Lanka 1940–1985
0
400
800
1200
1600
2000
1940–45 1950–55 1960–65 1970–75 1980–85Ma
tern
al
De
ath
s p
er
10
0 0
00
liv
eb
irth
s
85% births attended
by trained personnel

Three Delays Responsible for Three Delays Responsible for Maternal DeathsMaternal Deaths
1.1. Delay in deciding to seek careDelay in deciding to seek care (Individual & family) (Individual & family) Lack of understanding of complicationsLack of understanding of complications Gender issues, Low status of womenGender issues, Low status of women Socio-cultural barriers to seeking careSocio-cultural barriers to seeking care Poor economic condition of the familyPoor economic condition of the family
2.2. Delay in reaching careDelay in reaching care ( Community & System) ( Community & System) Lack or underutilization of transport fundsLack or underutilization of transport funds Non availability of referral transportation in remote Non availability of referral transportation in remote
placesplaces Lack of communication networkLack of communication network
3.3. Delay in receiving careDelay in receiving care (System) (System) Poor facilities, personnel and SuppliesPoor facilities, personnel and Supplies Poorly trained personnel with indifferent attitudePoorly trained personnel with indifferent attitude

Service Charges for participating GynecsService Charges for participating Gynecs
Normal delivery Normal delivery 8585 800800 6800068000
Complicated casesComplicated cases
Eclampsia Eclampsia 10001000
Forceps/vacuum/breech Forceps/vacuum/breech 33 10001000 30003000
EpisiotomyEpisiotomy 800800
SepticemiaSepticemia 22 30003000 60006000
Blood transfusionBlood transfusion 33 10001000 30003000
Cesarean (7%) Cesarean (7%) 77 50005000 3500035000
Predelivery visit Predelivery visit 100100 100100 1000010000
Investigation Investigation 100100 5050 50005000
Sonography Sonography 3030 150150 45004500
DaiDai 100100 5050 50005000
TransportTransport 100100 200200 2000020000179501795000

Chiranjivi preliminary resultsChiranjivi preliminary results
DistrictsDistricts Gynecs Gynecs enrolledenrolled
Deliveries Deliveries conductedconducted
KutchKutch 1818 4848
BanaskanthaBanaskantha 3939 349349
SabarkanthaSabarkantha 3737 254254
DahodDahod 1313 212212
PanchmahalsPanchmahals 2222 206206
TotalTotal 129129 10691069

HRD Reforms HRD Reforms
Grading of PHCs, CHCs and special training for poorly performing Grading of PHCs, CHCs and special training for poorly performing districts – manual for MOs – web sitedistricts – manual for MOs – web site
Three month PDP for district and block level officersThree month PDP for district and block level officers
““Karma yogi” motivational training program to change the attitude Karma yogi” motivational training program to change the attitude of government employees- conceptualized by Hon. Chief Ministerof government employees- conceptualized by Hon. Chief Minister
PG seats reserved for admissionsPG seats reserved for admissions to doctors serving in rural areas to doctors serving in rural areas - regular deputation for DPH programmes- regular deputation for DPH programmes
Computerised data base for doctorsComputerised data base for doctors
Filling up of vacant posts of MPHW by SI - three month Bridge Filling up of vacant posts of MPHW by SI - three month Bridge course for sanitary inspectorscourse for sanitary inspectors

InnovationsInnovations Web based Integrated Disease Surveillance ProgrammeWeb based Integrated Disease Surveillance Programme
Improved MIS through computer applications- RCH software;Improved MIS through computer applications- RCH software;
Transparency - information sharing through web siteTransparency - information sharing through web site
CRSCRS
GIS application – spatial distribution of health fcailities - Village wise GIS application – spatial distribution of health fcailities - Village wise data for malaria, and RCH data for malaria, and RCH
Urban healthUrban health
NGOsNGOs

Innovations 2Innovations 2
Decentralised recruitment of Medical Officers Decentralised recruitment of Medical Officers Powers of ad-hoc appointment delegated to Powers of ad-hoc appointment delegated to RDDsRDDs
ChiranjiviChiranjivi
Rogi kalyan SamitiRogi kalyan Samiti
Computerisation of hospitalsComputerisation of hospitals
TelemedicineTelemedicine
MCCDMCCD

Integrated Disease SurveillanceIntegrated Disease Surveillance
Kachchh
Jamnagar Rajkot
Banaskantha
SurendranagarAhmedabad
Mahesana Patan
1 Measles
1 Measles 2 Diptheria
5 Measles
2 Measles,4 Diphtheria
1 Measles

Next phase of reformsNext phase of reforms Strategic planning cellStrategic planning cell Functional managementFunctional management
Computerised financial management, budgeting, and Computerised financial management, budgeting, and auditingauditing
Monitoring and evaluation functionsMonitoring and evaluation functions HRD systemsHRD systems
Extensive use of ITExtensive use of IT Decentralised management through RDDsDecentralised management through RDDs Outsourcing CHCs and DHsOutsourcing CHCs and DHs Revamped CMSORevamped CMSO Communitisation - effectiveVillage health societies Communitisation - effectiveVillage health societies OmbudsmanOmbudsman

Further InformationFurther Information
PROD reference number 2: Medical PROD reference number 2: Medical Officers authorised to arrange Officers authorised to arrange maintenance and repairs on Primary maintenance and repairs on Primary Health Centres, Gujarat.Health Centres, Gujarat.
PROD reference number 31 PROD reference number 31 Establishment of District Health Agencies Establishment of District Health Agencies to manage health services, Various to manage health services, Various States.States.
www.prod-india.comwww.prod-india.com

Government of Gujarat Government of Gujarat and and European European UnionUnion
a a fruitful partnership fruitful partnership
Government of Gujarat Government of Gujarat and and European European UnionUnion
a a fruitful partnership fruitful partnership
January 2006

0
5
10
15
20
251
98
5
19
86
19
87
19
88
19
89
19
90
19
91
19
92
19
93
19
94
19
95
19
96
19
97
Pe
rce
nta
ge
de
ath
s
Circulatory System
Infectious & Parasitic
Symptoms, signs and illdefined
Injury & Poisoning
Certain conditionoriginating
Respiratory system
Trends in leading causes of deathsTrends in leading causes of deaths

ÃðÉßëÖ - ßÀÖìÕkë ìÞÜðýáÞÞí ìØåëÜë_. . .
0.58
21.10
0.00
5.00
10.00
15.00
20.00
25.00
Gujarat State - Towards Elimination of Leprosy ÃðÉßëÖ - ßÀÖìÕkë ìÞÜðýáÞÞí ìØåëÜë_. . .
0.58
21.10
0.00
5.00
10.00
15.00
20.00
25.00
Gujarat State - Towards Elimination of Leprosy

Cataract Surgery rate Achieved per one lakh population (Year 2001-02 to 2004-05)
802815
846863
941
700
750
800
850
900
950
1000
2000-01 2001-02 2002-03 2003-04 2004-05
Cataract Surgery Rate
Year
Cataract surgery

National RNTCP Status – 2Q04/2Q05National RNTCP Status – 2Q04/2Q05
50%
55%
60%
65%
70%
75%
80%
85%
90%
95%
100%
20% 30% 40% 50% 60% 70% 80% 90% 100% 110% 120%
Bihar
Kerala
Pondicherry
J&KUttaranchal
PunjabChattisgarh
UP
Meghalaya
Orissa
MPAssam
HaryanaKarnataka
Maharashtra
ManipurJharkhand
Nagaland
Mizoram
Gujarat
TNWB
Chhatisgarh
Rajasthan
HPDelhi
Arunachal Pradesh
AP
INDIA
Sikkim
Case Detection Rate
Cu
re R
ate

School health programmeSchool health programme
School check up for 10 million children annuallySchool check up for 10 million children annually
1.6 million students treated on site; 75,000 1.6 million students treated on site; 75,000 students referred for tertiary care; more than students referred for tertiary care; more than 70,000 children given spectacles70,000 children given spectacles
More than 5000 children provided super More than 5000 children provided super specialist heart, kidney and cancer care at specialist heart, kidney and cancer care at Government costGovernment cost

Referral Services under School Health Programme (2004-05)
Skin specialist - 4872
Dental surgeon - 10346
E.N.T. surgeon - 6245
Pediatrician - 17679
Ophthalmic surgeon - 32304


















