Death and Complications Conference 10/18/2012 Keri Quinn Trauma Surgery.
36
Death and Complications Conference 10/18/2012 Keri Quinn Trauma Surgery
-
Upload
tamsin-ward -
Category
Documents
-
view
219 -
download
4
Transcript of Death and Complications Conference 10/18/2012 Keri Quinn Trauma Surgery.

Death and Complications Conference10/18/2012Keri QuinnTrauma Surgery

Complication: ICU transfer, delayed diagnosis
48 yo woman, echo trauma alert s/p MCC at 55mph. The bike was laid down when another vehicle pulled out in front of hers. She was helmeted and had no LOC. EMS placed a traction splint on her RLE open femur fracture. Her chief complaint was severe pain in her right thigh.
BP 108/83 HR 82 RR 22 Pox 95% on RA
Alert, oriented, moderate distressPERRL, no facial instabilityNSR, CTABAbd soft, nontenderSpine nontender, no stepoffsRLE open femur fracture2+ pulses, equal throughout

PMH/PSH: substance abuse, anxiety, C-sectionSOC: +tob, +EtOH, +cocaine Meds: citalopram
Imaging:Severely comminuted open right distal femur fractureL4 transverse process fractureRight mandibular angle fractureArea of hypodensity in medial spleen, possible small
splenic laceration




HD#1—ex-fix R femurHD#2—persistent oozing from ex-fix, Hgb 10.1HD#3—ORIF mandible, Hgb 9.8HD#4—persistent oozing, refused labs, hemodynamically
stablehypotension overnight—SBP 70’s-80’s, transient response to fluid bolus
HD#5—SBP 70’s, HR 120’s, lethargic, slight abdominal tenderness, oozing from ex-fix—stat CBC: Hgb 5, started transfusion, transferred to STICU—worsening abdominal exam, RUQ fluid stripe on FAST exam—to OR for ex-lap

Intraop findings: about 800mL blood in abdomen, dark clots in LUQ, torn splenic capsule
Pathology: 70% of capsule absent, remaining capsule on hilar surface, areas of hemorrhage and minute lacerations on hilar surface, small subcapsular hematoma

Splenic trauma
One of the most commonly injured intra-abdominal organs
Fractured ribs and pulmonary contusions most common associated injures
Left upper abdomen, chest wall, or left shoulder pain (Kehr’s sign), seatbelt sign, hematoma, contusion
Negative history/unremarkable abdominal exam do not reliably exclude splenic injury

Diagnostic evaluation FAST exam
Unstable patient Negative exam does not exclude splenic injury
DPL >100,000 RBC’s/HPF High sensitivity
CT scan Stable patient Hemoperitoneum Hypodensity Contrast blush/extravasation

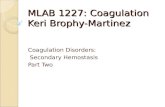
AAST Organ Injury Scale




Initial Management Hemodynamically unstable with positive FAST
or DPL abdominal exploration Peritonitis abdominal exploration Patient with additional abdominal injuries
abdominal exploration
Hemodynamically stable CT scan, initial management is non-operative Monitored bed Serial hgb Serial abdominal exams Consider embolization

EAST Guidelines for NOM of blunt injury to spleen
Initial non-operative management (NOM) of stable patients
Immediate operation or embolization of unstable patients, patients with peritonitis go to OR
Age, grade of injury, and amount of hemoperitoneum are not contraindications to NOM.
Hemodynamic instability is a contraindication to NOM.
CT with IV contrast is the most reliable method to assess severity of spleen injury
Trauma Practice Guideline Update, 24th Annual Scientic Assembly, Eastern Association for the Surgery of Trauma, January 2011.

EAST Guidelines cont’d Angiography with embolization should be considered if
contrast blush is seen on CT AAST grade > 3 moderate hemoperitoneum is present evidence of ongoing bleeding
Angiography is an adjunct to NOM patients at high risk for delayed bleed to look for vascular injuries (pseudoaneurysms) that
may lead to rupture or delayed hemorrhage
Trauma Practice Guideline Update, 24th Annual Scientic Assembly, Eastern Association for the Surgery of Trauma, January 2011.

Guidelines cont’d NOM should only be considered if continuous
monitoring and serial exams can be carried out at your hospital, and OR is immediately available
Clinical status dictates need for followup imaging
Contrast blush is not an absolute indication for operation or angio-embolization.
Trauma Practice Guideline Update, 24th Annual Scientic Assembly, Eastern Association for the Surgery of Trauma, January 2011.

Blunt Splenic Injury in Adults: Multi-Institutional study of the Eastern Association for the Surgery of Trauma. Journal of Trauma. 2000;(49):177-189.
Multi-institutional retrospective study
Factors determining successful NOM of blunt splenic trauma in adults
38.5% direct to laparotomy
61.5% admitted for NOM
10.8% failed NOM, required laparotomy 60.9% of failures occur in first 24 hours Failure rate increased significantly by AAST injury grade

Failure rate for non operative management (adults)
Grade 1 5% Grade 2 10% Grade 3 20% Grade 4 33% Grade 5 75%
Peitzman, A. et al. Blunt Splenic Injury in Adults: Multi-Institutional study of the Eastern Association for the Surgery of Trauma. Journal of Trauma. 2000;(49):177-189.

Successful NOM associated withHigher BP and HCTLess severe trauma based on
Injury Severity Score Glasgow Coma Scale Splenic grade Quantity of hemoperitoneum
54.8% of patients were successfully managed nonoperatively

Learning points Investigate hypotension. Any abdominal trauma, think spleen. Negative history, physical exam, and imaging, still
think spleen. Splenic injury in a hemodynamically stable patient
may be followed non operatively. Splenic injury of any grade can bleed and patient can
die. Don’t let that happen.

Delayed Rupture75% occur within 2 weeks in several seriesCan occur anytime (days, months, years)Actual incidence of delayed rupture very lowNeed to inform patients of this prior to D/C


Nonoperative Management
Patient selectionHemodynamic stabilityPatient ageSeverity of injuryOther associated injuries
Unstable patients suspected of splenic injury and intra-abdominal hemorrhage should undergo exlap and splenectomy











Clinical evaluationAltered level of consciousnessDecreased UOPMottled skinHemodynamic instability