Dead Men Tell (Tall) Tales - ACMT · Dead Men Tell (Tall) Tales: Pitfalls in Interpretation of...
51
Dead Men Tell (Tall) Tales: Pitfalls in Interpretation of Postmortem Drug Tests ACMT ASM Huntington Beach, CA March 17, 2016 Michael G. Holland, MD, FAACT, FACMT, FACOEM, FACEP Associate Professor, SUNY Upstate Medical University Consulting Medical Toxicologist, Upstate New York Poison Center, Syracuse, NY Occupational Medicine Director, Glens Falls Hospital Center for Occupational Health; Glens Falls, NY Senior Medical Toxicologist, Center for Toxicology and Environmental Health; North Little Rock, AR
Transcript of Dead Men Tell (Tall) Tales - ACMT · Dead Men Tell (Tall) Tales: Pitfalls in Interpretation of...

Dead Men Tell (Tall) Tales:Pitfalls in Interpretation of
Postmortem Drug TestsACMT ASMHuntington Beach, CA
March 17, 2016
Michael G. Holland, MD, FAACT, FACMT, FACOEM, FACEPAssociate Professor, SUNY Upstate Medical University
Consulting Medical Toxicologist, Upstate New York Poison Center, Syracuse, NYOccupational Medicine Director, Glens Falls Hospital Center for Occupational Health; Glens Falls, NY
Senior Medical Toxicologist, Center for Toxicology and Environmental Health; North Little Rock, AR
Disclosure:
I have performed medical-legal expert reviews of postmortem
toxicology results for the last 15 years and have testified in court


Drugs of Abuse: Case # 1 28 yo M, chronic pain patient, takes IR and ER
morphine. Found dead in his bed by roommate. Autopsy revealed pulmonary edema and pink frothy
foam in the tracheobronchial tree. Heart blood cocaine 0.189mg/L; BE 0.904mg/L Heart blood free morphine 0.169mg/L, MAM negative. Urine stored frozen, but not tested. Family files suit
against the pain management MD for overprescribing morphine products causing his death.

Drugs of Abuse: Case # 2 29 yo male hx drug abuse, chronic pain Rx with
fentanyl patches is found dead at home after recent filling of prescriptions
One 100mcg fentanyl patch found on skin; many empty whipped cream cans found in his room.
PM fentanyl blood level was 33ng/mL, and norfentanyllevel was 3.3 ng/mL.
ME concludes that death due to fentanyl OD. Family brings suit against pain MD for too-rapid
fentanyl dose escalation.

Drugs of Abuse: Case # 3 CL, 26 yo male, was driving 2014 Dodge Ram truck at
5:30 AM struck the rear of a tractor trailer that was backing up in the lane of traffic (had missed the mandatory weigh station).
At the time of the collision, the speed of the tractor-trailer was estimated at no more than 5 mph. The speed of the Yukon at impact was approximately 71 mph based on the readout from its ECM
ECM indicates brakes not applied until < 0.5 seconds prior to impact
Tractor trailer had all necessary safety lights on and back-up lights functional.

Drugs of Abuse: Case # 3 Tractor trailer driver neg BAC, neg urine drug test
(DOT) CL PM heart blood toxicology showed CL had WB THC
17ng/mL, carboxy-THC 18ng/mL. Qualitative presence of carisoprodol, meprobamate,
and oxycodone (all Rx meds for chronic LBP). CL family brings wrongful death claim against truck
driver You are asked to evaluate CL for impairment
Postmortem Toxicology:Years of Prevailing Wisdom
Circulation stops at time of death Metabolism stops at time of death Blood is the same regardless of
sampling site Post-mortem (PM) drug concentrations
reflect ante-mortem (AM) concentrations

Postmortem Redistribution &Evolving Reality
Circulation stops at death– Movement of body, putrefaction, CPR
Metabolism stops at death– Enzymes, hydrolysis, putrefactive metabolism, post-mortem
production Blood is the same regardless of sampling site
– 2 to 5-fold or higher central vs. peripheral blood Post-mortem (PM) drug concentrations reflect
ante-mortem (AM) concentrations– Now well-known that for many drugs, PM levels done
especially from heart blood do NOT reflect AM conc.– Many published “lethal” levels are from heart blood

Cell Death: Breakdown of Barriers8
Cell integrity depends on:– Aerobic cellular respiration- mitochondria– Maintenance of membrane integrity- pumps– Protein synthesis: enzymes, structural proteins – Nuclear/genetic integrity
Interval between ischemic injury & cell death– Varies by cell type– CNS- 3-5 minutes– Myocardium 30-40 min– Hepatocytes 1-2 hrs

Cell Death: Breakdown of Barriers8
Cellular injury/hypoxia/ischemia leads to:– Reduced ATP production-> Anaerobic
metabolism Lactate accumulation-> Acidotic cellular pH
– Na-K-ATPase pump fails 2o lack of ATP-> Na+
accumulates in cells Once membrane integrity is lost
– Cells leak contents (xenobiotics, electrolytes) into extracellular space
– Drugs diffuse by [gradients] into blood– Vice-versa

BE CAREFUL Most information on PMR and Central-
to-peripheral (C:P) ratios are based on single cases, or case series of a few patients
VERY FEW are based on large #’s PM drug levels must be interpreted in
light of entire Hx & clinical information In addition, average C:P ratios aren’t
useful- range is often more helpful
High likelihood of PMR if: Large Vd of drug or xenobiotic Alkaline drug: pKa >7 Highly lipophilic, with Log P > 0.5 Age of decedent- relates to Δ’s in Vd,
protein binding Manner of death: trauma, specifically
truncal injuries Conditions of death: aspiration of gastric
contents, sea water, etc. PM interval- time from death to blood
sampling

PMR and/or quality of results also depends on:
Manner of death- trauma Stomach contents Conditions of storage of body- refrigeration Amount of decomposition/putrefaction Storage of blood: temp., preserv (NaF)., time Type of blood tube (Li) Site of blood sample- C vs. P; ligated? Method of blood sampling (i.e. blind stick) Interpretation depends on type of blood
tested: serum (plasma) v whole blood
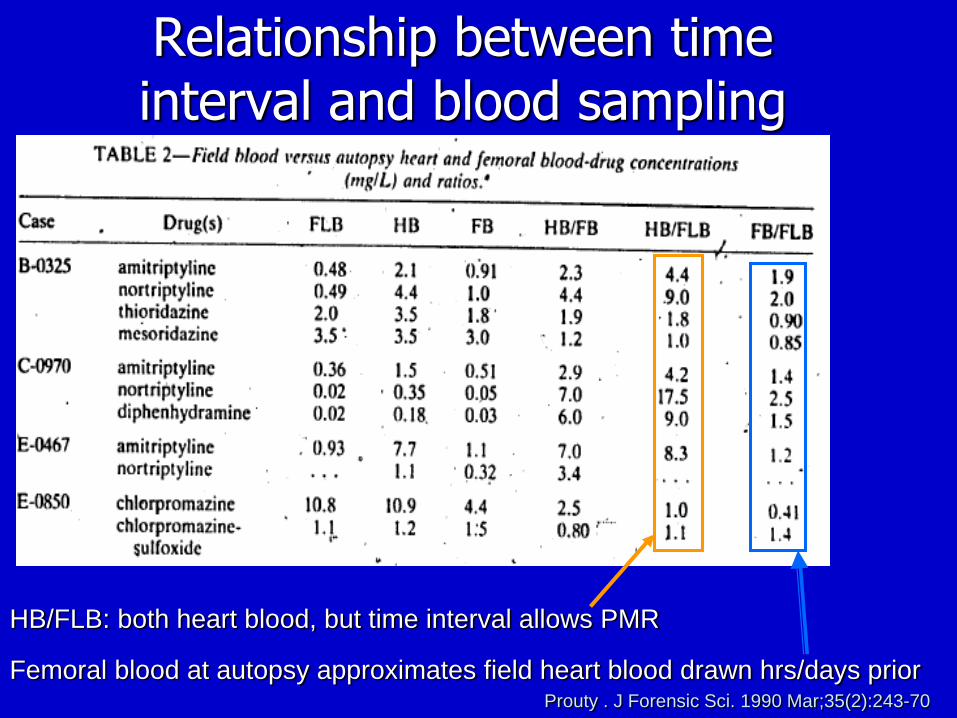
Relationship between time interval and blood sampling
Prouty . J Forensic Sci. 1990 Mar;35(2):243-70
HB/FLB: both heart blood, but time interval allows PMR
Femoral blood at autopsy approximates field heart blood drawn hrs/days prior

Fentanyl postmortem C:P ratios in 179 cases (McIntyre 2012)

Femoral fentanyl postmortem changes in 7 cases drawn at two intervals (Olson 2010)

Method of sampling Blind chest stick to obtain blood
– Most often by local coroners (often morticians, not MD’s)
– Cardiac blood or great vessels– Contaminated with gastric contents, esp.
with thoraco-abdominal trauma– Can markedly elevate ethanol, drug levels
from gastric spillage

Vitreous Humor Sampling Essentially 98% water with salt solution Very little protein Very isolated, not subject to PMR Useful when blood is not acceptable or
available– Severely burned bodies– Exsanguinating trauma – Extensive decomposition: VH can remain sterile

Toxicants/drugs in which PMR is unlikely1
Alcohols Carbon monoxide Carbamazepine Chlordiazepoxide Diflunisal Ephedrine Hydrocodone Hydroxyzine Lorazepam Lamotrigine
Mirtazapine Nitrazepam Phenelzine Pheniramine Phenobarbital Primidone Procyclidine Quinine/Quinidine Theophylline Zopiclone
1. Leikin. J Toxicol Clin Toxicol. 2003;41(1):47-56

Selected drugs in which PMR may occur1 (cardiac: periph. blood ratio)
Alprazolam (1.5) Amitriptyline (3.1) Amoxapine (1.8) Amphetamine (2.0) Bupropion (1.9) Chlorpromazine (4.0) Clomipramine (1.9) Clonazepam (2.0) Clozapine (2.8) Cocaine (1.5 to 2.3) Codeine (1.8) Cyanide (1.3) Cyclobenzaprine (2.2) D-methamphetamine (2.1) Desipramine (2.4) Dextromethorphan (2)
Diazepam (1.6) Diltiazem (2.6) Doxepin (5.5) Flunitrazepam (3) Fluoxetine (2.9) Fluvoxamine (1.7) Gamma hydroxybutyrate (2) Haloperidol (3.6) Imipramine (1.8 to 2.2) Ketamine (1.6) Lidocaine Maprotiline (4.7) Meprobamate (1.7) Mesoridazine (1.3) Methamphetamine (2.4) Methotrimeprazine (1.3))
1. Leikin. J Toxicol Clin Toxicol. 2003;41(1):47-56

Selected drugs in which PMR may occur1 (⇑ C:P blood ratio)
Methylenedioxy methamphetamine MDMA (2.65)
Metoprolol (3.8) Mexiletine (3.6) Midazolam (4) Morphine (heroin) (2.2) Naproxen (1.5) Nicotine (Cotinine-3) Nitrazepam Nortriptyline (2.4) Oxazepam (1.3) Oxycodone (3.1) Paramethoxyamphetamine (1.6) Paroxetine (2.7) Pentazocine (2) Pentobarbital Pethidine or meperidine (2.1)
Phencyclidine (1.8) Phentermine (1.7) Phenylbutazone (2.3) Phenylpropanolamine (2.4) Phenytoin (1.4) Promethazine (1.6) Propoxyphene (3.5) Propranolol (2.5) Quetiapine Strychnine (15) Tetrahydrocannabinol Thiopental (1.9) Tranylcypromine (2.2) Trazadone (1.6) Venlafaxine (1.6) Verapamil Zolpidem (2.1
1. Leikin. J Toxicol Clin Toxicol. 2003;41(1):47-56

Case # 1- Toxicology Report Blood (sample site not specified), mg/L
– Cocaine 0.218; BE 0.812 – Free Morphine 0.078, total morphine not
done Frozen stored urine was initially not
tested
Cocaine (methylbenzoylecgonine)
Parent cocaine (benzoyl-methyl-ecgonine)– Cocaine T½ 30-60 min.– Difficult to detect PM
Rapid, spontaneous hydrolysis (water-splitting) to benzoylecgonine (BE)-50%– BE T½ = 5– 8 hrs– Inhibited by freezing blood specimen
Rapid metabolism by plasma P-AChE & liver esterases into ecgonine methyl ester (EME)-30%– EME T½ = 3.5- 6hrs– Inhibited by 0.5- 2% NaF preservative & freezing

Methyl benzoylecgonine
CYP 3A4

Cocaine Presence of parent molecule in blood
(regardless of site) documents acute cocaine use due to short t½
Cocaine C:P ratio 1.5 to 2.2:1 = PMR Lack of parent molecule means either:
– Poor specimen storage (NaF, -20o C)– Cocaine use was >2+ hours prior to death
BE metabolite not psychoactive, but + CV toxicity
Cocaethylene psychoactive, CV toxic

Heroin (diacetyl morphine)Vd 25L/kg
Heroin t½ is 2-6 minutes Very rapid (enz & non-enz)
metabolism to 6-monoacetylmorphine (6-MAM)– 6-MAM t½ of 5-25 minutes- met to
morphine– NO back metabolism, i.e., Morphine ≠> 6-MAM ≠> Heroin
– 6-MAM presence is proof of acute heroin use

Case #1: Conclusion Urine stored frozen, but not tested. Subsequent urine testing was positive for 6-MAM
0.612mg/L, indicating heroin abuse was likely cause of death
ME conclusion: “acute drug toxicity due to combined effects of morphine and cocaine”
Acute cocaine use, within minutes/hrs of death– Presence of parent molecule proves acute use
Likely “speedball” use- stimulant effects of cocaine allow higher heroin dose, but cocaine’s shorter half life causes heroin/morphine effects to predominate later in OD.

Case #2: Conclusion ME conclusion of fentanyl ignores contribution
of nitrous oxide abuse (negative hydrocarbon inhalant panel)- N2O causes decr. hypoxic drive, can cause unconsciousness
Fails to consider PMR, even with femoral samples– 13 fatalities, the C:P ratio averaged 1.6 (range 0.7-
4.6). – 80 cases, the average C:P ratio was 2.7 (range 0.5-
11).
Case #3: Discussion Impairment in THC shown in live test
subjects with serum THC levels:Deficiency of THC-impaired driver
consistently shown in tracking and divided attentionAlso, impaired high level cognitive function
and concentrationIncreased reaction time and ability to take
sudden evasive action

Grotenhermen- 2007- Addiction Review of epi studies Found impairment with serum
concentrations in 7-10 ng/mL range Correlated roughly with BAC of
0.05g% Suggested per se limit is in this range
Ramaekers- 2006-Drug & Alcohol Dependence
Lab study w controlled dose Impaired critical tracking with serum
concentrations in >2 ng/mLWhen 2- 5 ng/mL, 71% subjects
were impairedWhen 5-10 ng/mL- up to 90%
subjects were impaired Remember: serum [THC]= 2X WB
[THC]
Khiabani- Traffic Inj Prev. 2006
Study of impaired drivers in Norway Impaired drivers averaged higher blood
THC levels than non-impaired drivers Those with levels of THC >3ng/mL
were at increased risk of being judged impaired.

Berghaus G- 1995Adelaide, Australia
Meta-analysis of 78 experimental smoking studies and 21 experimental oral THC studies (all published after 1993).
A mean serum THC of 3.7ng/mL (range 3.1-4.5) for oral THC and a mean serum THC of 3.8 ng/mL (range 3.3-4.5) for smoked THC caused driving impairment equivalent to that of BAC 0.05%.

Heustis Formulas for THC Impairment Estimation
Based on fact that THC impairing for 4-6 hours after smoking
Formula uses serum THC & THC-COOH to estimate time since last use, with Cis
Was based on older, less potent MJ
17 ng THC and 18 ng THCCOOH into Heustis Formula
Model I gives t =0.41 hrs (CI=0.19-0.91)
Model II gives a t = 0.64 hrs (CI= 0.24-1.7hrs)
Has not been validated in PM setting Heustis: Model II might be more
reliable in PM, since it uses the ratio of the two and not absolute values

Cannabis Influence Factor (CIF)
Molar ratio between [THC + THC-OH] ÷ [THCCOOH], then multiplied by 100
Any value >10 = likely THC-impaired Based on study of drivers in Dusseldorf, Germany
1994 ¾ of drivers impaired by THC or alcohol had either a
BAC> 0.11g% or a CIF >10
CIF also has not been validated in the postmortem model, but since it uses a ratio, it may be valid- but no proof

Does serum in living = WB levels in PM?
Holland et al 2011- Forensic Sci Int PMR of cannabinoidsMean and median C:P ratio < 2 1.5 for THC (range: 0.3–3.1) 1.6 for 11-OH-THC (range: 0.3–2.7) 1.8 for THC-COOH (range: 0.5–3.0)
Trend for > PMR with > postmortem interval between death and sampling

PM heart blood THC 17ng/mL,PM WB THCCOOH 18ng/mL So what does one do with PM
cannabinoids in WB?
What does the science show?
What conclusions are valid and supportable?
Drummer: 2004 Accident Anal Prevent
In 3,398 fatal MVAs, if any THC in blood, OR were 2.7 times as likely to have a motor vehicle crash vs drug-free driver
Further, if THC ≥ 5 μg/L, odds ratio increased to 6.6
This was the start of the discussion for per se limit being 5 ng/mL

Biecheler: Traffic Inj Prev2008
727 traffic fatalities in France Assessed driver culpability vs drug-free For those with +THC only- 2.3 times as
likely Alcohol only- 9.4 times
THC + Etoh= 14.1

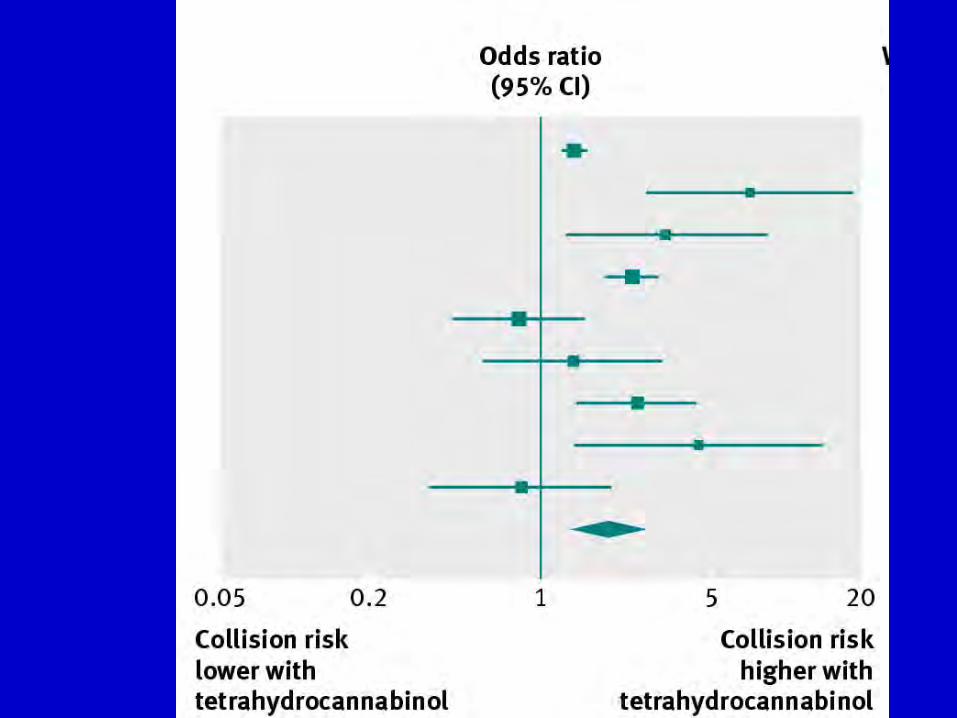
Li: Epi Reviews 2012 Meta-analysis of 9 studies published from
2001-2010 Estimated OR of MJ use to crash risk Pooled OR =1.92 (95% confidence interval
1.35 to 2.73) Collision risk estimates were higher in
case-control studies (2.79) & in studies of fatal collisions (2.10)
Lower in culpability studies (1.65) & non-fatal collisions (1.74)

Asbridge: BMJ 2012
Meta-analysis of 9 studies 1982-2009
Estimated OR of MJ use to crash risk
Combined motor vehicle crash risk OR was 1.9 (CI 1.4- 2.7)

DRUID- 2013 Knoche Culpability study of 7455 drivers
Dose-dependent increased risk for MVA with WB THC concentrations:
– OR of 1 for THC ≤ 1ng/mL in WB– OR of 1.5 for THC 1-3ng/mL in WB – OR of 2.8 for THC > 3 but <5ng/mL– OR of 2.0 for THC > 5ng/mL
Case #3: Conclusion Despite PMR and heart blood, cannabinoids
quite high in this case- Comparison to living impairment levels difficult
due WB vs plasma, PMR, PM interval, etc. Ample scientific evidence that presence of THC
in PM blood gives RR > 2 for culpability in fatal MVA
Case #3: Conclusion Deficiency of THC-impaired driver is reaction
time and ability to take sudden evasive action Accident analyst estimated he had at least ten
seconds of warning that he was rapidly approaching the semi trailer
He never applied brakes until last instant- This type of impairment is typical of THC
Other drugs (sed-hyp & opioid) likely contributory
References1. Flanagan RJ, Connally G. Interpretation of Analytical Toxicology Results in Life and at
Postmortem. Toxicol Rev 2005; 24 (1): 51-622. Flanagan RJ, Connally G, Evans JM. Analytical toxicology: guidelines for sample collection post
mortem. Toxicol Rev 2005; 24: 63-71 3. Prouty RW, Anderson W. The Forensic Science Implications of Site and Temporal Influences on
Postmortem Blood-Drug Concentrations. J Forensic Sci 1990;35(2):243-2704. Baselt RC Disposition of Toxic Drugs and Chemicals in Man, 7th ed.; Biomedical Publications;
Foster City, CA 2004 5. Winek CL, Wahba WW, Winek CL Jr, Balzer TW. Drug and chemical blood-level data 2001.
Forensic Sci Int. 2001 Nov 1;122(2-3):107-23.6. Schulz M, Schmoldt A. Therapeutic and toxic blood concentrations of more than 800 drugs and
other xenobiotics. Pharmazie. 2003 Jul;58(7):447-74. 7. Druid H, Holmgren P. A compilation of fatal and control concentrations of drugs in postmortem
femoral blood. J Forensic Sci. 1997 Jan;42(1):79-87. 8. Yarema MC, Becker CE. Key concepts in postmortem drug redistribution. Clin Toxicol (Phila).
2005;43(4):235-41 9. Repetto MR, Repetto M. Habitual, toxic, and lethal concentrations of 103 drugs of abuse in
humans. J Toxicol Clin Toxicol. 1997;35(1):1-9. Review. PMID: 9022645 10. Repetto MR, Repetto M. Therapeutic, toxic, and lethal concentrations of 73 drugs affecting
respiratory system in human fluids. J Toxicol Clin Toxicol. 1998;36(4):287-93. PMID: 9711193 11. Repetto MR, Repetto M. Therapeutic, toxic, and lethal concentrations in human fluids of 90
drugs affecting the cardiovascular and hematopoietic systems. J Toxicol Clin Toxicol. 1997;35(4):345-51.
12. Repetto MR, Repetto M. Concentrations in human fluids: 101 drugs affecting the digestive system and metabolism. J Toxicol Clin Toxicol. 1999;37(1):1-9. Review.

References13. Winek CL Jr, Winek CL, et al. The role of trauma in postmortem blood alcohol determination.
Forensic Sci Int. 1995 Jan 21;71(1):1-8. 14. Leikin JB, Watson WA. Post-mortem toxicology: what the dead can and cannot tell us. J Toxicol
Clin Toxicol. 2003;41(1):47-56. 15. Moriya F, Hashimoto Y. Postmortem diffusion of drugs from the bladder into femoral venous blood.
Forensic Sci Int. 2001 Dec 1;123(2-3):248-53.16. Prouty RW, Anderson WH. The forensic science implications of site and temporal influences on
postmortem blood-drug concentrations. J Forensic Sci. 1990 Mar;35(2):243-70 17. Sakurada K, Kobayashi M, et al. Production of gamma-hydroxybutyric acid in postmortem liver
increases with time after death. Toxicol Lett. 2002 Mar 28;129(3):207-17. 18. Elliott SP. Gamma hydroxybutyric acid (GHB) concentrations in humans and factors affecting
endogenous production. Forensic Sci Int. 2003 Apr 23;133(1-2):9-16 19. Pelissier-Alicot AL, Coste N, et al. Comparison of ethanol concentrations in right cardiac blood, left
cardiac blood and peripheral blood in a series of 30 cases. Forensic Sci Int. 2006 Jan 6;156(1):35-9.
20. Pelissier-Alicot AL, Fornaris M, et al. An unusual case of post-mortem redistribution of ethanol. Forensic Sci Int. 2005 May 28;150(1):81-3
21. Olson KN, Luckenbill K, Thompson J, Middleton O, Geiselhart R, Mills KM, Kloss J, Apple FS. Postmortem redistribution of fentanyl in blood. Am J Clin Pathol. 2010 Mar;133(3):447-53.
22. McIntyre IM, Anderson. Postmortem Fentanyl Concentrations: A Review. J Forensic Res 2012, 3:823. Ramaekers J et al. Cognition and motor control as a function of Delta9-THC concentration in serum
and oral fluid: limits of impairment. Drug Alcohol Depend. 2006 Nov 8;85(2):114-22.

References24. DRUID- Anja Knoche- Per se limits – recommendations for defining cut-off values for psychoactive
substance use in traffic 201325. Huestis MA, Barnes A, Smith ML. Estimating the time of last cannabis use from plasma delta9-
tetrahydrocannabinol and 11-nor-9-carboxy-delta9-tetrahydrocannabinol concentrations. Clin Chem. 2005 Dec;51(12):2289-95.
26. Holland MG, Schwope DM, Stoppacher R, Gillen SB, Huestis MA. Postmortem redistribution of Δ9-tetrahydrocannabinol (THC), 11-hydroxy-THC (11-OH-THC), and 11-nor-9-carboxy-THC (THCCOOH). Forensic Sci Int. 2011 Oct 10;212(1-3):247-51.
27. Li MC, et al. Marijuana use and motor vehicle crashes. Epidemiol Rev. 2012;34:65-72.28. Biecheler MB, et al. SAM survey on "drugs and fatal accidents": search of substances consumed and
comparison between drivers involved under the influence of alcohol or cannabis. Traffic Inj Prev.29. 2008 Mar;9(1):11-21.Drummer OH, et al. The involvement of drugs in drivers of motor vehicles killed in
Australian road traffic crashes. Accid Anal Prev. 2004 Mar;36(2):239-48.30. Grotenhermen F. Leson G. Berghaus G. Drummer OH. Kruger HP. Longo M. Moskowitz H. Perrine B.
Ramaekers JG. Smiley A. Tunbridge R. Developing limits for driving under cannabis. Addiction. 102(12):1910-7, 2007 Dec.
31. Khiabani HZ, Bramness JG, Bjorneboe A, Morland J. Relationship between THC concentration in blood and impairment in apprehended drivers. Traffic Inj Prev. 2006 Jun;7(2):111-6.
32. Berghaus G, Scheer N, Schmidt P. Effects of Cannabis on Psychomotor Skills and Driving Performance – A Meta-analysis of Experimental Studies. Presented at the 13th International Conference on Alcohol, Drugs and Traffic Safety (T’95), Adelaide, Australia, August 13-18, 1995. Available at http://casr.adelaide.edu.au/T95/paper/s16p2.html. Accessed January 27, 2015.
33. Asbridge M, Hayden JA, Cartwright JL. Acute cannabis consumption and motor vehicle collision risk: systematic review of observational studies and meta-analysis. BMJ. 2012 Feb 9;344