
Davidlsmith globalforum 1
31
-
Upload
center-for-disease-dynamics-economics-policy -
Category
Documents
-
view
220 -
download
0
description
http://www.cddep.org/sites/default/files/davidlsmith_globalforum_1.pdf
Transcript of Davidlsmith globalforum 1


Acknowledgements
• GARP has been funded by a grant to CDDEP from the Bill & Melinda Gates Foundation
• Ramanan Laxminarayan, PI • Modeling:
§ Itamar Megiddo (CDDEP) § David L Smith
Ø Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health
§ Eili Klein Ø Princeton University

Outline
• Introduction • Pneumococcal Modeling • PneuMOD
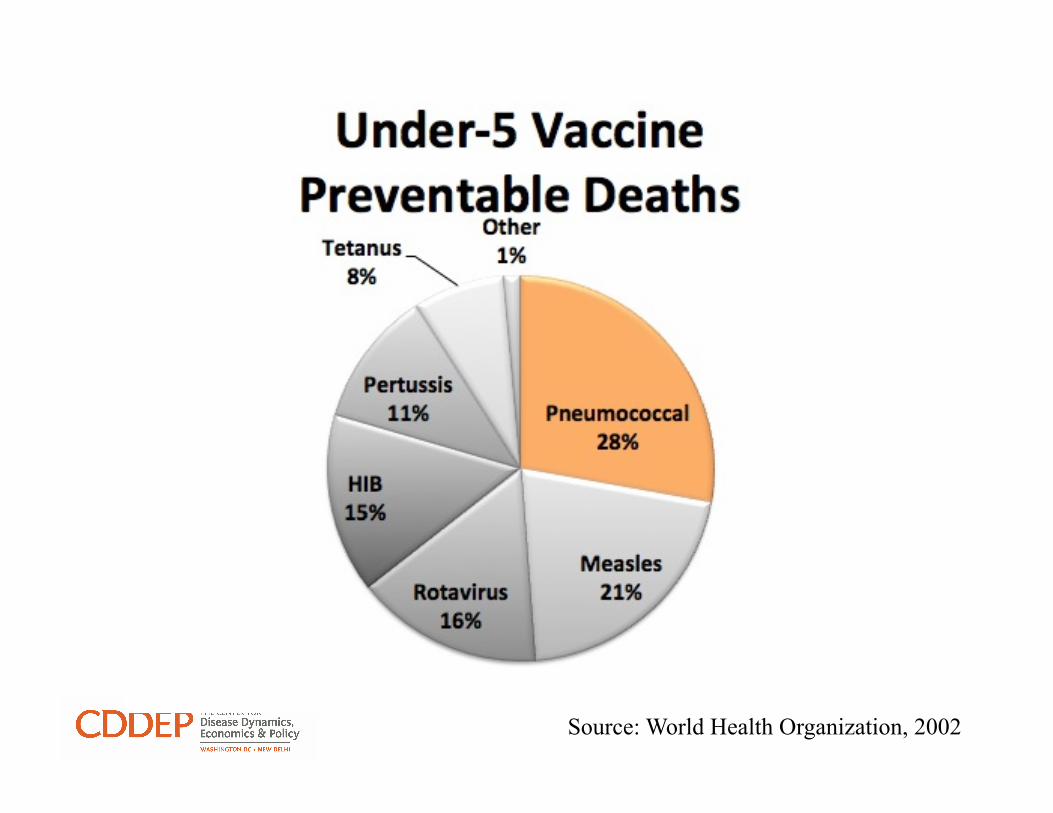
Source: World Health Organization, 2002

Source: World Health Organization, 2002


Interventions to prevent & control pneumococcal disease
Treatment
Prevention
Protection

Policy Questions
• How can we best (most cost-effectively) reduce pneumococcal disease burden through a combination of tools (vaccination, treatment)?
• Can increased treatment access reduce the burden of disease in the long term when drug resistance is likely?
• What is the value of treatment access improvements in countries with pneumo vaccination?
• What population level strategies (like multiple first line treatments or subsidized high quality antibiotics) can most address the challenge of resistance?

Outline
• Introduction • Pneumococcal Models • PneuMOD

Why model pneumococci?
• How many lives could be saved? • At what cost?
§ Purchase cost of interventions § Opportunity cost
• How certain are the answers? • How could uncertainty be reduced?

What is a model?

How does a model of pneumococci work?
From Individuals To Populations

Colonized Infected
Colonization / Infection
Uncolonized

Transmission Shedding/ Mixing / Exposure

Pneumococcal Global Serotype Project
PLoS Medicine | www.plosmedicine.org 7 October 2010 | Volume 7 | Issue 10 | e1000348
Serotypes

Immunity
Age-Specific Incidence of Invasive Pneumococcal Disease in the United States by Serogroup
Lipsitch, M. et al. PLoS Med 2, e15 (2005).

Drug Treatment & Resistance
that are often of greater interest because the lower bloodconcentrations are associated with treatment failure or aselection of resistant parasites, whereas the highest con-centrations are more likely to be associated with toxicity[18,19]. It is therefore important to complete pharmacoki-netic sampling when patients are withdrawn from a studyfollowing adverse events or treatment failure. The greaterthe inter-individual variability and the narrower thetherapeutic range, the greater will be the proportion ofpatients with sub-therapeutic or toxic drug levels. Low oralbioavailability is the main cause of large inter-individualvariability in blood concentrations (e.g. lumefantrine) [9].Inter-individual variability can be exacerbated by the useof use of concomitant medications that interact with theantimalarials [20].
Because therapeutic response is influenced by hostfactors, such as acquired immunity, it is necessary to
define therapeutic drug-concentration ranges in non-immune populations; in stable malaria-transmissionareas, this means young children. Pharmacokinetic stu-dies have usually not been designed to describe ade-quately the relationship between drug concentrationsover time [pharmacokinetics (PK)] and therapeuticresponse and drug safety [pharmacodynamics (PD)](Box 2). As a result, most antimalarials have been intro-duced with dosage regimens derived from dose-findingstudies in non-pregnant adult patients. These dosageregimens have often been too close to the minimumeffective dose required, both for cost-saving and becauseof concerns over drug safety. The dosage regimens ofamodiaquine, primaquine, mefloquine, halofantrine,artemether-lumefantrine and the artemisinin deriva-tives have all been increased after initial deployment[21,22].
Figure 1. The pharmacokinetic determinants of outcome in uncomplicated malaria. Drug concentrations must exceedminimum parasiticidal concentrations (MPCs) until allparasites are eliminated; this usually takes at least four 48-h asexual life cycles in P. falciparum. The area under the blood or plasma concentration time curve (AUC) predictsthe therapeutic response. The maximum concentration (CMAX) is considered less important in the treatment of uncomplicated malaria. For slowly eliminated antimalarialdrugs, the blood or plasma concentration on day 7 is a good correlate of the AUC and thus treatment response.
Figure 2. The pharmacokinetic determinants of outcome in severe malaria. The key determinant is the time taken to exceed the MPC (TMPC), for which the time (TMAX) toachieve the maximum concentration (CMAX) provides a useful correlate, when the in vivo MPC is not known precisely.
Review Trends in Parasitology Vol.xxx No.x
TREPAR-694; No of Pages 8
2
groups based on studies in non-pregnant adult patientsmight be wrong. These special risk groups are of particularconcern because they are more vulnerable to malaria com-plications because of lower levels of malaria immunity.
Young childrenDosage regimens in children have, generally, been derivedfrom the same ‘one dose fits all’ milligram per kilogramdosage recommended for non-pregnant adults: forexample, 4 mg kg!1 artesunate, a combination of25 mg kg!1 sulfadoxine and 1.25 mg kg!1 pyrimethamineor 25 mg kg!1 mefloquine. Yet, the disposition of manydrugs is altered significantly in children and infants.Despite extensive use for four decades, it has only beenrecognized recently that the currently recommendedmg kg!1 doses of both SP and CQ achieve substantiallylower plasma drug concentrations in young children thanin older patients [10,26]. Plasma lumefantrine concen-trations achieved in children under 5 years of age are alsosignificantly lower than in older children and adults [27]. Adecrease in the plasma lumefantrine concentrations isassociated with increased risks of recrudescence and ear-lier reinfections [9,27]. In some cases, the effect of age ondrug disposition is complex. For example, the absorptionand clearance of chlorproguanil, when co-administeredwith dapsone, is lower in young children than in adults,whereas clearance of its active metabolite chlorcycloguanilis higher in young children [28]. The clearance and appar-ent volume of distribution of dapsone increases with bodyweight [28]. However, no differences in safety or efficacy ofchlorproguanil-dapsone have been observed between chil-dren and adults when dosed according to body weight [29].Concentrations of piperaquine, when co-administered withdihydroartemisinin, are lower at the beginning of theterminal elimination phase in children than in adults;low plasma piperaquine concentrations on day 7 wereassociated with treatment failure [30,31].
Young children with severe malaria might be moresusceptible to quinine cardiotoxicity than older children[32]. There is no evidence currently that exposure to arte-misinin derivatives is significantly reduced in young chil-dren, although marked inter-individual variability limitsthe power of small studies to define the effect of age. Most ofthepharmacokinetic studies on this class of antimalarials inyoung children concern rectal artesunate – possibly becauseit has been developed by WHO-TDR. As the apparentvolume of distribution was proportional to weight andage, it appears unlikely that young children are underdosed[33]. Small studies did not find any effect of age on plasmaconcentrations of desethylamodiaquine (the active metab-olite of amodiaquine) or mefloquine [34–36]. Although theabsorption and disposition of many drugs differ betweeninfants and children, there are almost no data on antima-larial pharmacokinetics in the first year of life.
Pregnant womenPregnant women are at greater risk of adverse outcomesfrom malaria than non-pregnant women. In areas of
Figure 3. The association between dose and treatment response. The idealtreatment dose changes over time with the spread of resistance. (a) Initially,because all parasites are drug sensitive, lower drug levels might not increase therisk of treatment failure. (b) With the development of resistance, higher drug
concentrations are required to achieve a cure against more resistant parasites. (c)With higher levels of resistance, the ideal dose is squeezed between the minimumeffective dose and that associated with toxicity.
Review Trends in Parasitology Vol.xxx No.x
TREPAR-694; No of Pages 8
4

Biology, Ecology, Epidemiology, Economics…
• Colonization § Duration
• Transmission § Shedding § Contact § Establishment
• Microbial Competition § Exclusion § Dominance
• Infection
• Immunity § Inhibit Colonization § Prevent Disease § Strain Specificity
• Interventions § Drugs § Vaccines

Outline
• Introduction • Pneumococcal Models • PneuMOD

(...)b
(...)d
(...)b
(...)d
(...)b
(...)d
Colonized Population growth
Population decay
Markov-Chain Carriage Model
(...)d
!
Uncolonized
Shedding Increases

Markov-Chain Carriage Model

Infection
Increasing Risk

Immune Stages
ê Duration of Carriage ê Prob. Colonization after Exposure ê Shedding ê Risk of Infection ê Severity of Disease
Waxing Waning

Competition (Serotypes & Strains) Meets Strong “Neutrality” Conditions
Etc.

Drug Treatment / Compliance
that are often of greater interest because the lower bloodconcentrations are associated with treatment failure or aselection of resistant parasites, whereas the highest con-centrations are more likely to be associated with toxicity[18,19]. It is therefore important to complete pharmacoki-netic sampling when patients are withdrawn from a studyfollowing adverse events or treatment failure. The greaterthe inter-individual variability and the narrower thetherapeutic range, the greater will be the proportion ofpatients with sub-therapeutic or toxic drug levels. Low oralbioavailability is the main cause of large inter-individualvariability in blood concentrations (e.g. lumefantrine) [9].Inter-individual variability can be exacerbated by the useof use of concomitant medications that interact with theantimalarials [20].
Because therapeutic response is influenced by hostfactors, such as acquired immunity, it is necessary to
define therapeutic drug-concentration ranges in non-immune populations; in stable malaria-transmissionareas, this means young children. Pharmacokinetic stu-dies have usually not been designed to describe ade-quately the relationship between drug concentrationsover time [pharmacokinetics (PK)] and therapeuticresponse and drug safety [pharmacodynamics (PD)](Box 2). As a result, most antimalarials have been intro-duced with dosage regimens derived from dose-findingstudies in non-pregnant adult patients. These dosageregimens have often been too close to the minimumeffective dose required, both for cost-saving and becauseof concerns over drug safety. The dosage regimens ofamodiaquine, primaquine, mefloquine, halofantrine,artemether-lumefantrine and the artemisinin deriva-tives have all been increased after initial deployment[21,22].
Figure 1. The pharmacokinetic determinants of outcome in uncomplicated malaria. Drug concentrations must exceedminimum parasiticidal concentrations (MPCs) until allparasites are eliminated; this usually takes at least four 48-h asexual life cycles in P. falciparum. The area under the blood or plasma concentration time curve (AUC) predictsthe therapeutic response. The maximum concentration (CMAX) is considered less important in the treatment of uncomplicated malaria. For slowly eliminated antimalarialdrugs, the blood or plasma concentration on day 7 is a good correlate of the AUC and thus treatment response.
Figure 2. The pharmacokinetic determinants of outcome in severe malaria. The key determinant is the time taken to exceed the MPC (TMPC), for which the time (TMAX) toachieve the maximum concentration (CMAX) provides a useful correlate, when the in vivo MPC is not known precisely.
Review Trends in Parasitology Vol.xxx No.x
TREPAR-694; No of Pages 8
2
groups based on studies in non-pregnant adult patientsmight be wrong. These special risk groups are of particularconcern because they are more vulnerable to malaria com-plications because of lower levels of malaria immunity.
Young childrenDosage regimens in children have, generally, been derivedfrom the same ‘one dose fits all’ milligram per kilogramdosage recommended for non-pregnant adults: forexample, 4 mg kg!1 artesunate, a combination of25 mg kg!1 sulfadoxine and 1.25 mg kg!1 pyrimethamineor 25 mg kg!1 mefloquine. Yet, the disposition of manydrugs is altered significantly in children and infants.Despite extensive use for four decades, it has only beenrecognized recently that the currently recommendedmg kg!1 doses of both SP and CQ achieve substantiallylower plasma drug concentrations in young children thanin older patients [10,26]. Plasma lumefantrine concen-trations achieved in children under 5 years of age are alsosignificantly lower than in older children and adults [27]. Adecrease in the plasma lumefantrine concentrations isassociated with increased risks of recrudescence and ear-lier reinfections [9,27]. In some cases, the effect of age ondrug disposition is complex. For example, the absorptionand clearance of chlorproguanil, when co-administeredwith dapsone, is lower in young children than in adults,whereas clearance of its active metabolite chlorcycloguanilis higher in young children [28]. The clearance and appar-ent volume of distribution of dapsone increases with bodyweight [28]. However, no differences in safety or efficacy ofchlorproguanil-dapsone have been observed between chil-dren and adults when dosed according to body weight [29].Concentrations of piperaquine, when co-administered withdihydroartemisinin, are lower at the beginning of theterminal elimination phase in children than in adults;low plasma piperaquine concentrations on day 7 wereassociated with treatment failure [30,31].
Young children with severe malaria might be moresusceptible to quinine cardiotoxicity than older children[32]. There is no evidence currently that exposure to arte-misinin derivatives is significantly reduced in young chil-dren, although marked inter-individual variability limitsthe power of small studies to define the effect of age. Most ofthepharmacokinetic studies on this class of antimalarials inyoung children concern rectal artesunate – possibly becauseit has been developed by WHO-TDR. As the apparentvolume of distribution was proportional to weight andage, it appears unlikely that young children are underdosed[33]. Small studies did not find any effect of age on plasmaconcentrations of desethylamodiaquine (the active metab-olite of amodiaquine) or mefloquine [34–36]. Although theabsorption and disposition of many drugs differ betweeninfants and children, there are almost no data on antima-larial pharmacokinetics in the first year of life.
Pregnant womenPregnant women are at greater risk of adverse outcomesfrom malaria than non-pregnant women. In areas of
Figure 3. The association between dose and treatment response. The idealtreatment dose changes over time with the spread of resistance. (a) Initially,because all parasites are drug sensitive, lower drug levels might not increase therisk of treatment failure. (b) With the development of resistance, higher drug
concentrations are required to achieve a cure against more resistant parasites. (c)With higher levels of resistance, the ideal dose is squeezed between the minimumeffective dose and that associated with toxicity.
Review Trends in Parasitology Vol.xxx No.x
TREPAR-694; No of Pages 8
4
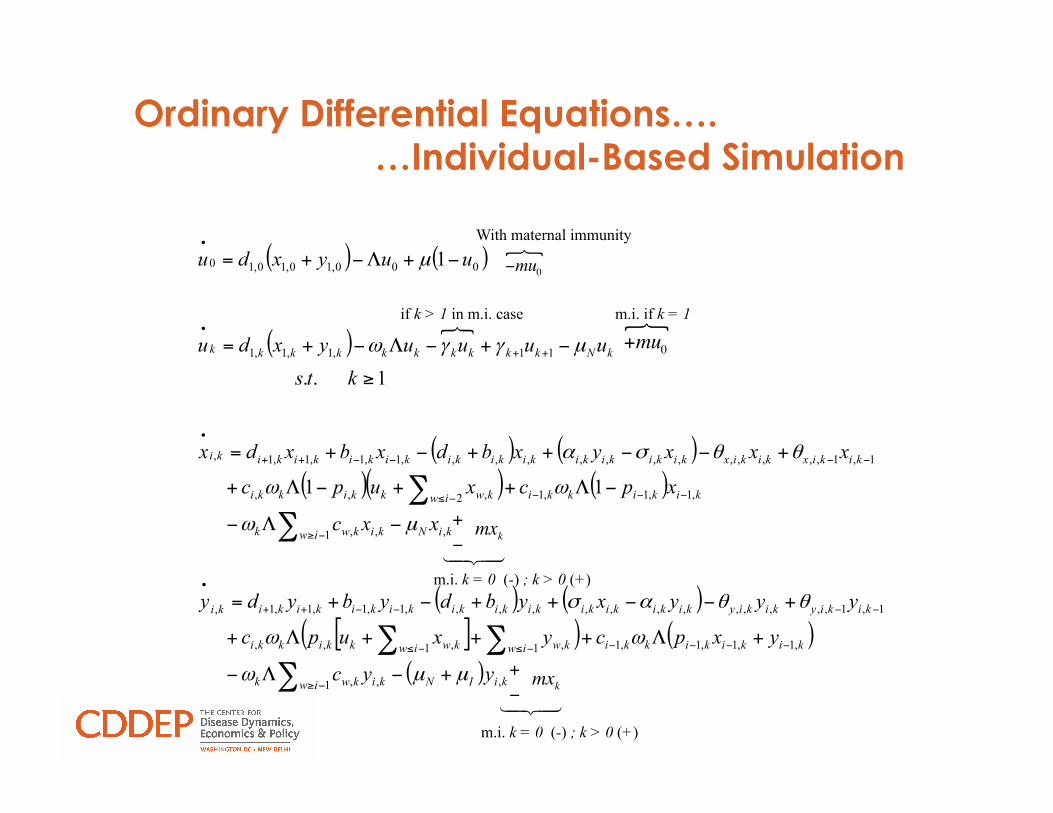
Ordinary Differential Equations…. …Individual-Based Simulation
( ) ( )
( )
( ) ( )( )( ) ( )
( ) ( )[ ]( ) ( )
( ) kiINiw kikwk
kikikikkiiw kwiw kwkkikki
kikiykikiykikikikikikikikikikikiki
kiNiw kikwk
kikikkiiw kwkkikki
kikixkikixkikikikikikikikikikikiki
kNkkkkkkkkkk
yyc
yxpcyxupc
yyyxybdybydy
xxc
xpcxupc
xxxyxbdxbxdx
ktsuuuuyxdu
uuyxdu
,1 ,,
,1,1,1,11 ,1 ,,,
1,1,,,,,,,,,,,,,1,1,1,1,
,1 ,,
,1,1,12 ,,,
1,1,,,,,,,,,,,,,1,1,1,1,
11,1,1,1
000,10,10,10
11
1..
1
µµω
ωω
θθασ
µω
ωω
θθσα
µγγω
µ
+−Λ−
+Λ+++Λ+
+−−++−+=
−Λ−
−Λ++−Λ+
+−−++−+=
≥
−+−Λ−+=
−+Λ−+=
∑∑∑
∑∑
−≥
−−−−−≤−≤
−−−−++
•
−≥
−−−−≤
−−−−++
•
++
•
•
!mu0!
With maternal immunity
+mu0!m.i. if k = 1
+!mxk
!"# $#m.i. k = 0 (-) ; k > 0 (+)
+!mxk
!"# $#m.i. k = 0 (-) ; k > 0 (+)
if k > 1 in m.i. case

5 10 15 20
02000
4000
Vaccination and Antibiotics Campaigns Starting on Year 10
Year
Col
oniz
atio
n pr
eval
ence
per
10,
000
Campaign20% coverage40% coverage20% coverage & antibiotics control40% coverage & antibiotics control
5 10 15 20
020
4060
Year
Infe
ctio
n in
cide
nce
per 1
0,00
0
Discounted Infections333.94204.97439.15110.30
5 10 15 20
020
60100
Year
Res
ista
nce
%
Simulated Vaccination

The model produces important policy relevant results
Calibrate model parameters
Run/solve model implementing interventions
Output: - Mortality - Infection - Colonization - ….

Simulated for Kenya

Need better data for…
• Duration of carriage • Complexity of colonies • Risk of infection • Competitive dominance • Immunity
§ Colonization § Infection § Cross-immunity § Age
• Local strains • Health seeking • Treatment compliance • Non-sterile tissue PK/PD • Underlying populations • Human mobility

Burden of Pneumococci - I
Source: World Bank, 2000; World Health Organization, 2000





![1 1 1 1 1 1 1 ¢ 1 1 1 - pdfs.semanticscholar.org€¦ · 1 1 1 [ v . ] v 1 1 ¢ 1 1 1 1 ý y þ ï 1 1 1 ð 1 1 1 1 1 x ...](https://static.fdocuments.us/doc/165x107/5f7bc722cb31ab243d422a20/1-1-1-1-1-1-1-1-1-1-pdfs-1-1-1-v-v-1-1-1-1-1-1-y-1-1-1-.jpg)








![[XLS] · Web view1 1 1 2 3 1 1 2 2 1 1 1 1 1 1 2 1 1 1 1 1 1 2 1 1 1 1 2 2 3 5 1 1 1 1 34 1 1 1 1 1 1 1 1 1 1 240 2 1 1 1 1 1 2 1 3 1 1 2 1 2 5 1 1 1 1 8 1 1 2 1 1 1 1 2 2 1 1 1 1](https://static.fdocuments.us/doc/165x107/5ad1d2817f8b9a05208bfb6d/xls-view1-1-1-2-3-1-1-2-2-1-1-1-1-1-1-2-1-1-1-1-1-1-2-1-1-1-1-2-2-3-5-1-1-1-1.jpg)

![$1RYHO2SWLRQ &KDSWHU $ORN6KDUPD +HPDQJL6DQH … · 1 1 1 1 1 1 1 ¢1 1 1 1 1 ¢ 1 1 1 1 1 1 1w1¼1wv]1 1 1 1 1 1 1 1 1 1 1 1 1 ï1 ð1 1 1 1 1 3](https://static.fdocuments.us/doc/165x107/5f3ff1245bf7aa711f5af641/1ryho2swlrq-kdswhu-orn6kdupd-hpdqjl6dqh-1-1-1-1-1-1-1-1-1-1-1-1-1-1.jpg)
