d Original Contribution - Smith Ultrasound...
10
d Original Contribution DUAL-MODE IVUS TRANSDUCER FOR IMAGE-GUIDED BRAIN THERAPY: PRELIMINARY EXPERIMENTS CARL D. HERICKHOFF ,* CHRISTY M. WILSON, y GERALD A. GRANT , y GAVIN W. BRITZ, y EDWARD D. LIGHT ,* MARK L. P ALMERI,* P ATRICK D. WOLF ,* and STEPHEN W. SMITH* * Department of Biomedical Engineering; and y Division of Neurosurgery, Duke University Medical Center, Durham, NC, USA (Received 14 February 2011; revised 6 June 2011; in final form 23 June 2011) Abstract—In this study, we investigated the feasibility of using 3.5-Fr intravascular ultrasound (IVUS) catheters for minimally-invasive, image-guided hyperthermia treatment of tumors in the brain. Feasibility was demon- strated by: (1) retro-fitting a commercial 3.5-Fr IVUS catheter with a 5 3 0.5 3 0.22 mm PZT-4 transducer for 9-MHz imaging and (2) testing an identical transducer for therapy potential with 3.3-MHz continuous- wave excitation. The imaging transducer was compared with a 9-Fr, 9-MHz ICE catheter when visualizing the post-mortem ovine brain and was also used to attempt vascular access to an in vivo porcine brain. A net average electrical power input of 700 mW was applied to the therapy transducer, producing a temperature rise of 113.5 C at a depth of 1.5 mm in live brain tumor tissue in the mouse model. These results suggest that it may be feasible to combine the imaging and therapeutic capabilities into a single device as a clinically-viable instrument. (E-mail: [email protected]) Ó 2011 World Federation for Ultrasound in Medicine & Biology. Key Words: Dual-mode catheter transducer, Ultrasound hyperthermia, Intravascular ultrasound. INTRODUCTION The long-term goal of this research is the development of a minimally-invasive, endovascular approach to adminis- tering localized, image-guided, ultrasound-induced hyperthermia in the brain. This localized delivery of hyperthermia would provide targeted control of drug release from thermosensitive liposomes and opening of the blood-brain barrier, which would enhance chemother- apeutic drug delivery to malignant brain tumors. In previous studies, we investigated the feasibility of dual- mode intracranial catheter transducers by two different approaches: first, by using 14-Fr, phased-array prototype transducers for focused tissue heating and real-time three-dimensional (3-D) intracranial imaging and second, by modeling and measuring acoustic output for various 3.5-Fr intravascular ultrasound (IVUS) catheter trans- ducer apertures (Herickhoff et al. 2009, 2010). In this work, we investigate the merit of using a dual- frequency PZT-4 transducer by fabricating and testing in vivo imaging and tissue-heating prototypes. The current treatment options for malignant central nervous system (CNS) tumors are inadequate, due to lack of efficacy, toxicity and poor penetration of the blood-brain barrier (Fadul et al. 1988; Wrensch et al. 1993; Cabantog and Bernstein 1994; Schottenfeld and Fraumeni 1996; Wilkins and Rengachary 1996; Mareel 1998; Mikkelsen 1998; Sawaya et al. 1998; Bernstein et al. 2000; Kleihues et al. 2000; Prados 2000; Lesniak 2005; CBTRUS 2008; ACS 2009). New methods are being developed that show promise to improve brain tumor treatment by enhancing drug delivery and using noninvasive approaches. The many examples of this would include: using localized hyperthermia and targeted, thermosensitive liposomes (drug release threshold 14 C above body temperature); opening the blood-brain barrier using ultrasound, with or without mi- crobubble contrast agent; and transcranial, image- guided focused ultrasound for thermal ablation (Guthkelch et al. 1991; Zunkeler et al. 1996; Hynynen and Jolesz 1998; Kroll and Neuwelt 1998; Hynynen et al. 2001, 2004; Cho et al. 2002; Dayton and Ferrara 2002; Mesiwala et al. 2002; Aubry et al. 2003; Bloch et al. 2004; Ponce et al. 2006; Choi et al. 2007; Kheirolomoom et al. 2007; McDannold et al. 2007, 2008, 2010; Vykhodtseva et al. 2008). Address correspondence to: Carl D. Herickhoff, Department of Biomedical Engineering, Duke University, Room 136 Hudson Hall, Durham, NC 27708 USA. E-mail: [email protected] 1667 Ultrasound in Med. & Biol., Vol. 37, No. 10, pp. 1667–1676, 2011 Copyright Ó 2011 World Federation for Ultrasound in Medicine & Biology Printed in the USA. All rights reserved 0301-5629/$ - see front matter doi:10.1016/j.ultrasmedbio.2011.06.017
Transcript of d Original Contribution - Smith Ultrasound...

Ultrasound in Med. & Biol., Vol. 37, No. 10, pp. 1667–1676, 2011Copyright � 2011 World Federation for Ultrasound in Medicine & Biology
Printed in the USA. All rights reserved0301-5629/$ - see front matter
asmedbio.2011.06.017
doi:10.1016/j.ultrd Original Contribution
DUAL-MODE IVUS TRANSDUCER FOR IMAGE-GUIDED BRAIN THERAPY:PRELIMINARY EXPERIMENTS
CARL D. HERICKHOFF,* CHRISTY M. WILSON,y GERALD A. GRANT,y GAVIN W. BRITZ,y
EDWARD D. LIGHT,* MARK L. PALMERI,* PATRICK D. WOLF,* and STEPHEN W. SMITH**Department of Biomedical Engineering; and yDivision of Neurosurgery, Duke University Medical Center, Durham, NC, USA
(Received 14 February 2011; revised 6 June 2011; in final form 23 June 2011)
ABiomeDurham
Abstract—In this study, we investigated the feasibility of using 3.5-Fr intravascular ultrasound (IVUS) cathetersfor minimally-invasive, image-guided hyperthermia treatment of tumors in the brain. Feasibility was demon-strated by: (1) retro-fitting a commercial 3.5-Fr IVUS catheter with a 5 3 0.5 3 0.22 mm PZT-4 transducerfor 9-MHz imaging and (2) testing an identical transducer for therapy potential with 3.3-MHz continuous-wave excitation. The imaging transducer was compared with a 9-Fr, 9-MHz ICE catheter when visualizing thepost-mortem ovine brain and was also used to attempt vascular access to an in vivo porcine brain. A net averageelectrical power input of 700mWwas applied to the therapy transducer, producing a temperature rise of113.5�Cat a depth of 1.5 mm in live brain tumor tissue in the mouse model. These results suggest that it may be feasible tocombine the imaging and therapeutic capabilities into a single device as a clinically-viable instrument. (E-mail:[email protected]) � 2011 World Federation for Ultrasound in Medicine & Biology.
Key Words: Dual-mode catheter transducer, Ultrasound hyperthermia, Intravascular ultrasound.
INTRODUCTION
The long-term goal of this research is the development ofa minimally-invasive, endovascular approach to adminis-tering localized, image-guided, ultrasound-inducedhyperthermia in the brain. This localized delivery ofhyperthermia would provide targeted control of drugrelease from thermosensitive liposomes and opening ofthe blood-brain barrier, which would enhance chemother-apeutic drug delivery to malignant brain tumors. Inprevious studies, we investigated the feasibility of dual-mode intracranial catheter transducers by two differentapproaches: first, by using 14-Fr, phased-array prototypetransducers for focused tissue heating and real-timethree-dimensional (3-D) intracranial imaging and second,by modeling and measuring acoustic output for various3.5-Fr intravascular ultrasound (IVUS) catheter trans-ducer apertures (Herickhoff et al. 2009, 2010). In thiswork, we investigate the merit of using a dual-frequency PZT-4 transducer by fabricating and testingin vivo imaging and tissue-heating prototypes.
ddress correspondence to: Carl D. Herickhoff, Department ofdical Engineering, Duke University, Room 136 Hudson Hall,, NC 27708 USA. E-mail: [email protected]
1667
The current treatment options for malignant centralnervous system (CNS) tumors are inadequate, due tolack of efficacy, toxicity and poor penetration of theblood-brain barrier (Fadul et al. 1988; Wrensch et al.1993; Cabantog and Bernstein 1994; Schottenfeld andFraumeni 1996; Wilkins and Rengachary 1996; Mareel1998; Mikkelsen 1998; Sawaya et al. 1998; Bernsteinet al. 2000; Kleihues et al. 2000; Prados 2000; Lesniak2005; CBTRUS 2008; ACS 2009). New methods arebeing developed that show promise to improve braintumor treatment by enhancing drug delivery andusing noninvasive approaches. The many examplesof this would include: using localized hyperthermiaand targeted, thermosensitive liposomes (drug releasethreshold 14�C above body temperature); opening theblood-brain barrier using ultrasound, with or without mi-crobubble contrast agent; and transcranial, image-guided focused ultrasound for thermal ablation(Guthkelch et al. 1991; Zunkeler et al. 1996; Hynynenand Jolesz 1998; Kroll and Neuwelt 1998; Hynynenet al. 2001, 2004; Cho et al. 2002; Dayton and Ferrara2002; Mesiwala et al. 2002; Aubry et al. 2003; Blochet al. 2004; Ponce et al. 2006; Choi et al. 2007;Kheirolomoom et al. 2007; McDannold et al. 2007,2008, 2010; Vykhodtseva et al. 2008).

Fig. 1. Schematic of proposed dual-mode intravascular ultra-sound (IVUS) operation. Radial imaging field (gray circle)with tumor (white circle). Hyperthermia beam (straight linesindicate full beamwidth at half-maximum) from catheter (black
circle) directed at tumor volume.
1668 Ultrasound in Medicine and Biology Volume 37, Number 10, 2011
Dual-mode ultrasound devices for image-guidedtherapy have been designed and implemented formany different applications using various approaches(Hynynen 1997; Wu et al. 2001; Barthe et al. 2004;Gentry and Smith 2004; Makin et al. 2005; Ebbini et al.2006; Pua et al. 2007; Bouchoux et al. 2008, 2010).Intravascular ultrasound (IVUS) catheters, which aretypically less than 4 Fr, were developed to navigateinto coronary vessels to visualize and characterizeatherosclerotic plaque (Fishbein and Siegel 1998;Mehran et al. 1998; Nishioka et al. 1998; Uren et al.1998a, 1998b). Mechanical IVUS catheters commonlyuse a single rotating piezoelectric crystal with a surfacearea less than a few square millimeters, and the use ofIVUS catheters for therapeutic applications involvingmicrobubbles is being investigated (Foster et al. 1993;Erbel 1998; Phillips et al. 2008; Kilroy et al. 2009).Furthermore, interventional neuroradiologists have usedminimally-invasive endovascular techniques to treatintracranial diseases, including inserting a 5-Fr catheteras far as the frontal portion of the superior sagittal sinusto treat thrombosis, and these procedures can be extendedto the treatment of intracranial tumors (Horowitz et al.1995; Kuether et al. 1998; Connors and Wojak 1999;Dowd et al. 1999; Opatowsky et al. 1999; Chow et al.2000; Novak et al. 2000; Morris 2002).
Our design goal is a dual-mode ultrasound catheterthat is both thin and flexible enough to navigate a vascularpathway to the brain and be placed immediately adjacentto a brain tumor target, to visualize the tumor and thendirect an ultrasound hyperthermia beam to trigger therelease of drugs contained within thermosensitive lipo-somes molecularly targeted to regions of tumor angiogen-esis (see Fig. 1). Commercially-available IVUS cathetershave an appropriate form factor (are both thin and flexibleenough) to achieve the desired placement within thebrain volume via our intended vascular approach, sothey are considered here as one possible platform fora dual-mode intracranial catheter integrating ultrasoundimaging and hyperthermia.
In this article, we describe the construction andtesting of two prototypes (one for imaging, the otherfor therapy), each using an identical, dual-frequencyPZT-4 transducer element, to independently assessimaging performance and therapeutic potential of theproposed dual-mode, intracranial IVUS catheter design.
MATERIALS AND METHODS
For our prototypes, PZT-4was used because its prop-erties (high kT and Qm, low tan d) make it an excellentchoice of material for dual-mode imaging and therapytransducers. A 9-MHz resonance for imaging correspondsto a PZT-4 thickness of 0.22 mm, and the maximum-
allowable aperture geometry for a flexible 3.5-Fr IVUScatheter was determined to be 53 0.5 mm in consultationwith neurosurgery and interventional neuroradiologycolleagues. In addition to the thickness-mode, a width-mode resonance at 3.3 MHz was designed and utilizedfor increased thermal penetration depth. Consequently,two prototypes were built using 5 3 0.5 3 0.22 mmPZT-4: one to assess imaging performance at 9 MHz ina mechanical IVUS catheter and one to assess therapeuticpotential by hyperthermia generation at 3.3 MHz.
ImagingFor the imaging prototype, a mechanical IVUS cath-
eter was needed as a construction template. A BostonScientific (Natick, MA, USA) Atlantis� SR Pro coronaryimaging catheter, with a nominal frequency of 40 MHz,was chosen and tested prior to modification by connect-ing to a Boston Scientific ClearView Ultra� scanner.Figure 2 shows a 40-MHz image of a portion ofa 2.5-cm-diameter cyst phantom acquired with theunmodified Atlantis.
The Atlantis’ original 40-MHz element was care-fully removed from the distal end of the catheter andthe roundedmetal housing was filed down to create a levelshelf. The 5 3 0.5 3 0.22 mm PZT-4 element was thenbonded to the shelf with silver epoxy (CHO-BOND;Chomerics,Woburn,MA, USA) to secure and electricallyconnect to the ground contact on the back of the element.The front contact was then connected to the signal wire,

Fig. 2. 40-MHz image of 2.5-cm cyst phantom, acquired withAtlantis intravascular ultrasound (IVUS) catheter. Arrows
indicate cyst wall. Tick mark spacing is 1 mm.
Fig. 4. Catheter devices and 9-MHz images of 2.5-cm cystphantom. (a) 9-Fr ICE with 2.1-mm-diameter transducer. (b)ICE catheter cyst image. (c) Modified intravascular ultrasound(IVUS) prototype outside of 3.5-Fr sheath. (d) Modified IVUS
cyst image. Tick mark spacing is 16 mm.
Dual-mode IVUS transducer for image-guided brain therapy d C. D. HERICKHOFF et al. 1669
protruding from the middle of the housing, with silverepoxy. To reinforce the delicate bonds of silver epoxy,a coating of 20-min epoxy (Finish-Cure; Bob SmithIndustries, Atascadero, CA, USA) was applied aroundthe proximal end of the element. Finally, to ensure thatsound was transmitted and received only through the frontface of the transducer, an improvised air backing wascreated using a mixture of 20-min epoxy and phenolicmicroballoons (BJO-0930; Asia Pacific Microballoons,Selangor, Malaysia). Figure 3 shows a top-view andside-view schematic of the prototype.
To initially assess imaging performance, the modi-fiedAtlantis IVUS prototypewas comparedwith a BostonScientific 9-Fr intracardiac echo catheter (Ultra ICE�;see Fig. 4a) as a gold standard for 9-MHz imaging. Usingthe ClearView Ultra scanner, each catheter was used toimage two targets: a 2.5-cm-diameter cyst phantom andthree post-mortem ovine brains. To image the ovine brain30 min post-mortem, a burr hole was made along themidline of the skull, angled posteriorly. This allowed
Fig. 3. Schematic of 9 MHz imaging prototype. (a) Top view oftransducer bonded to metal housing (light gray). (b) Side viewshowing phenolicmicroballoon backing (dark gray). Scale inmm.
catheter insertion into the superior sagittal sinus, suchthat the imaging plane (perpendicular to the catheteraxis) could be swept over the brain volume by push-through or pull-back (see Fig. 5).
The final experiment with the 9-MHz imagingprototype attempted to access the cranial cavity viaa minimally-invasive vascular approach in an in vivoporcine model. The Institutional Animal Care and UseCommittee at Duke University approved the followingprocedure. An intravenous (IV) line was established ina peripheral vein and the animal was sedated with thio-pental sodium, 20 mg/kg administered intravenously.Anesthesia was induced with inhalation of isofluranegas 1% to 5% delivered through a nose cone. The animalwas intubated, placed on a water heated thermal pad andstarted on a ventilator. A line was placed in the leftfemoral artery via a percutaneous puncture or cutdown.Electrolyte and ventilator adjustments were made basedon serial electrolyte and arterial blood gas measurements.

Fig. 5. Diagram of ovine brain imaging scheme. Catheter inser-tion into posterior portion of superior sagittal sinus, withrotating transducer scanning a perpendicular plane (dark
blue). Reproduced with permission (Miselis 2006).
1670 Ultrasound in Medicine and Biology Volume 37, Number 10, 2011
An IV maintenance drip of D-5 lactated Ringer’s solutionwas started and maintained at 5 mL/kg/min. Blood pres-sure, lead II electrocardiogram and temperature werecontinuously monitored throughout the procedure. Theanimal was placed in a supine position and the rightfemoral artery was punctured using the Seldinger tech-nique and dilated over a guide wire. A preliminary angio-gram of the right common carotid and vertebral arterieswas performed and recorded to identify the locationsand anatomy of proximate branch vessels. With a 6-FrEnvoy� XB (670-258-90B; Cordis Corp., Bridgewater,NJ, USA) guiding catheter in place over a wire guide,the modified Atlantis IVUS prototype was advancedtoward the cranial vessels via either the carotid or verte-bral arteries. Real-time images of the vessels andsurrounding tissue were acquired at 9 MHz using theClearView Ultra scanner.
TherapyA therapy prototype designed for high-power opera-
tion was constructed using a piece of PZT-4 identical to
Fig. 6. Therapy experiment procedures. (a) 40-MHz VisualSothe surface in tissue-mimicking material. (b) in vitro therapy e
anesthetized mouse on foil-lined heating pad
that used in the 9-MHz imaging prototype (5 3 0.5 30.22 mm). Double-sided metallized liquid crystal poly-mer (LCP, 20 mm thick) was bonded to the face of theceramic with silver epoxy, to provide both a signal groundcontact and a separate outer ground layer to shield RFnoise. Four feet of IVUS-catheter coaxial cable wasremoved from the inside of a spare Atlantis catheter,and the cable’s ground and signal wires were carefullyexposed and separated at the distal end before beingbonded to the front and back contacts of the PZT-4,respectively. An epoxy-and-microballoons air backingwas applied (similar to the imaging prototype) and thetransducer was secured and sealed in a 9-Fr catheterscrap, in side-viewing configuration.
An impedance analyzer (Model 4194A; Hewlett-Packard, Palo Alto, CA, USA) was used to measurethe electrical impedances of both the therapy prototypeand a 25-W RF power amplifier (Model 525LA; ENI,Rochester, NY, USA) at 3.3 MHz. These impedancevalues were used to calculate the optimal inductanceand capacitance values (7.7 mH and 55 pF, respectively)for the design of a simple L-section impedance matchingnetwork, which would be used to maximize powertransfer from the power source (amplifier) to the load(therapy prototype transducer) at a single frequency(3.3 MHz).
To initially assess therapeutic potential, the trans-ducer was used in vitro with tissue-mimicking material(National Physical Laboratory, Teddington, UK), whichis 4 cm in diameter, 4 mm thick, and has thermalproperties similar to brain tissue (Goss et al. 1978; Baconand Shaw 1993; Shaw et al. 1999). To measure theachievable temperature, a type T, 33-gauge, hypodermicneedle thermocouple (HYP-0; Omega Engineering,Stamford, CT, USA) was used. This small-diameter, fine-wire thermocouple sheathed in stainless steel was chosento minimize the possibility of artifacts (e.g., viscousheating, reflections, conduction along the wire) in the
nics image verifying thermocouple needle 1 mm beneathxperiment setup. (c) in vivo glioblastoma therapy setup:. Arrow indicates transducer position.

Fig. 7. Post-mortem ovine brain: 9-MHz imaging comparisonshowing lateral ventricles. (a) 9-Fr ICE catheter image. (b)Anatomical diagram, reproduced with permission (Fletcheret al. 2006). (c) 3.5-Fr modified intravascular ultrasound
(IVUS) prototype image. Tick mark spacing is 16 mm.
Dual-mode IVUS transducer for image-guided brain therapy d C. D. HERICKHOFF et al. 1671
thermal measurement (Fry and Fry 1954; Hynynen andEdwards 1989). We do not otherwise consider theseeffects in the proof-of-concept experiments describedhere.
The thermocouplewas inserted approximately 1mmbeneath the surface of the material and the depth ofthe thermocouple was verified by imaging the samplewith a Vevo 770� scanner and RMV706� scanhead(VisualSonics, Toronto, Ontario, Canada) at 40 MHz(see Fig. 6a). The prototype transducer was alignedwith the thermocouple and placed within 1 mm of thesurface of the submerged material sample (see Fig. 6b).A waveform generator (Model 33250; Agilent, SantaClara, CA, USA) was connected to the power amplifierto produce continuous-wave (CW) excitation at a netaverage electric power of 700 mWat 3.3 MHz for nearly2 min while the thermocouple recorded temperature.Electrical input to the matching network and therapyprototype transducer, including average forward and re-flected power, was measured using a power reflectionmeter (NRT; Rohde & Schwarz, Munich, Germany).
The therapy prototype transducer was tested on anexcised glioblastoma tumor, which had been grown arti-ficially on the flank of a nudemouse. The tumor measured13 mm along the long axis and 10 mm along the shortaxis. A minimal amount of standard ultrasound transmis-sion gel (Conductor; Chattanooga Group, Hixson, TN,USA) was applied to the face of the transducer beforeplacing it in contact with the tumor. The thermocouplewas inserted approximately 1.5 mm beneath the surfaceof the tissue and aligned with the center of the transducer.The waveform generator and power amplifier created3.3MHzCWexcitation. The power was alternately turnedon and off for 90 s at a time, at levels of 700, 350 and175 mW, while the thermocouple recorded temperature.
Finally, the therapy prototype was tested on a humanglioblastoma xenograft tumor, grown to approximately1 cm 3 2 cm in the flank of a nude mouse. The animalwas anesthetized with 100 mg/kg ketamine/xylazineand monitored by toe pinch reflex. The anesthetic wasre-administered as needed on a per animal basis whenthe animal responded to the toe-pinch. Animal bodytemperature was maintained at 37�C using a homeo-thermic heating blanket. The skin around the tumorwas carefully dissected away so that the transducercould be placed directly on the surface of the tumor,using minimal ultrasound transmission gel. The tumormeasured 18 mm along the long axis and 16 mm alongthe short axis. The thermocouple was inserted approxi-mately 1.5 mm beneath the tissue surface and alignedwith the transducer (see Fig. 6c). The waveform gener-ator and power amplifier produced 3.3-MHz CW excita-tion for 60 s, followed by 120 s of off-time, to allow thetissue temperature to recover to nearer its baseline
temperature. This was done sequentially at power levelsof 700, 350 and 175 mW, while the thermocouplerecorded temperature.
RESULTS
ImagingFigure 4a shows the 9-Fr ICE catheter used as an
imaging gold standard and the modified Atlantis IVUS

Fig. 8. In vivo porcine imaging results. (a) Angiogram showing modified intravascular ultrasound (IVUS) prototype(arrow) in right vertebral artery. (b) 9-MHz image of vertebral artery lumen (arrow) and surrounding tissue near
subclavian junction. Tick mark spacing is 16 mm.
1672 Ultrasound in Medicine and Biology Volume 37, Number 10, 2011
prototype transducer is shown in Figure 4c. The ICEtransducer is 2.1 mm in diameter, while the IVUS proto-type has an aperture 0.5 mm in azimuth. Figures 4b and4d are 9-MHz images of a 2.5-cm cyst phantom acquiredby the commercial 9-Fr ICE catheter and the 3.5-Frmodified IVUS prototype, respectively. Though thegold-standard ICE catheter outperforms the prototype interms of lateral resolution and sensitivity, the imagesare roughly comparable. The IVUS prototype hasa greater degree of beam divergence due to its muchsmaller aperture, resulting in poorer lateral resolutionrelative to the ICE gold standard.
Figure 7 compares the imaging performance of the9-Fr ICE and 3.5-Fr modified IVUS catheter probes ina post-mortem ovine brain, with an anatomical diagramfor reference. In both images, the skull is seen outlining
Fig. 9. Thermocouple data from in vitro therapy experimentwith tissue-mimicking material. Resulting temperature rise
was 6.7�C in under 2 min.
the cranial cavity and the symmetric wings of the lateralventricles are clearly visible in the center of the brainvolume as well.
In the in vivo porcine experiment, the prototypecatheter was unfortunately unable to advance beyondthe pig’s vertebral artery into the basilar artery at thebase of the brain. Figure 8 shows the prototype transducerat its farthest advancement in the vertebral artery, as wellas a real-time, 9-MHz ultrasound image of the vertebralartery near the subclavian junction.
TherapyIn the tissue-mimicking material, the 3.3-MHz
therapy prototype transducer was able to create a temper-ature rise of 6.7�C in less than 2 min with CW
Fig. 10. Thermocouple data showing sequential temperaturerises in excised glioblastoma tumor of 19.1�C, 9.2�C and4.9�C after 90 s of on-time for power levels of 700, 350 and
175 mW, respectively.

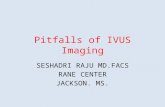
Fig. 11. Thermocouple data for in vivo xenograft glioblastomatumor grown in the flank of a nude mouse, showing sequentialtemperature rises of 13.5�C, 6.8�C and 3.0�C after 60 s of on-time for power levels of 700, 350 and 175 mW, respectively.
Dual-mode IVUS transducer for image-guided brain therapy d C. D. HERICKHOFF et al. 1673
transmission at 700 mW (see Fig. 9). In the excised glio-blastoma brain tumor, the therapy prototype createda temperature rise of 19.1�C in 90 s of CW excitationat 700 mW. Subsequently, temperature rises of 9.2�Cand 4.9�C were created using 350 mW and 175 mW ofCW power, respectively (see Fig. 10). Finally, in thein vivo tumor experiment, the therapy prototype achievedtemperature rises of 13.5�C, 6.8�C and 3.0�C in 60 s ofCW excitation at 700, 350 and 175 mW, respectively(see Fig. 11).
Fig. 12. In vivo porcine vascular imaging results. (a) Angiogramright vertebral artery. (b) Volcano ChromoFlo image showing
puncture site, acquired with 20-MHz Eagle E
DISCUSSION
A 53 0.53 0.22 mm PZT-4 transducer was used tobuild a 9-MHz imaging prototype in a 3.5-Fr mechanicalIVUS catheter and a 3.3-MHz high-power prototypefor therapy. The 3.5-Fr imaging prototype performedcomparably to a 9-Fr commercial ICE catheter in imaginga 2.5-cm cyst phantom and visualizing brain anatomy ina post-mortem ovine brain. The ovine brain images showthat a 3.5-Fr IVUS catheter is capable of resolvingfeatures (including the lateral ventricles and skull) ata depth of up to 3 cm.
To our knowledge, we have shown the first attemptto access and image the brain via a minimally-invasive,vascular approach using an ultrasound catheter. The3.5-Fr, 9-MHz modified-Atlantis imaging prototype wasable to navigate as far as the vertebral artery and imagesurrounding tissue before vessel narrowing and tortuosityprevented further catheter advancement. Although accessto the brain volume was not achieved in the porcinemodel, the authors’ experience in the field of interven-tional neuroradiology gives confidence that such restrict-ing vessel size and tortuosity issues would not be presentin a human procedure.
The results from the 3.5-Fr, 9-MHz IVUS imagingprototype can be compared with the findings of two finalexperiments using a 20-MHz Volcano (San Diego, CA,USA) 3.5-Fr phased-array IVUS imaging catheter withan In-Vision� scanner. First, a Volcano Eagle Eye�Gold was used in the same porcine model experimentas the modified Atlantis, to visualize the vessel and
showing a regional hematoma (arrows) surrounding thenon-uniform flow (arrow) in the lumen near the vesselye Gold. Tick mark spacing is 1 mm.

Fig. 13. In vivo porcine brain imaging results. (a) VolcanoPV018 image showing bordering skull (red arrow) and threegyri in close proximity (green arrows). Tick mark spacing is2 mm. (b) Anatomical diagram, reproduced with permission
(Welker 2011).
1674 Ultrasound in Medicine and Biology Volume 37, Number 10, 2011
its surroundings with a higher-frequency, commercialIVUS catheter. As the Eagle Eye was advanced into thevertebral artery, the wire guide accidentally puncturedthe vessel wall, creating a regional hematoma that wasvisible under fluoroscopy (see Fig. 12a). The turbulentblood flow created by the puncture was visible whenusing the scanner’s ChromaFlo� feature to image thelumen (see Fig. 12b).
The other auxiliary experiment used a VolcanoPV018 catheter to visualize structures near the brainsurface. The 3.5-Fr catheter was inserted through a 1-cmburr hole in a porcine skull, placing the IVUS arraybetween the inner surface of the skull and the dura mater,a few millimeters adjacent to the midline. The scan depthwas maximized to 12 mm and features including cerebralgyri, sulci and pulsating vessels could be clearly seen outto a range of 5–6 mm (see Fig. 13). The findings fromthese auxiliary experiments suggest that additional usefulinformation might be obtained with a more sophisticateddevice designed to operate at a frequency above 9 MHz.
The therapy prototype achieved a temperature rise of6.7�C in tissue-mimicking material before testing tissue-heating capability in glioblastoma tumors. In an excisedtumor, the therapy prototype achieved a temperaturerise as high as 19.1�C in 90 s at 1.5 mm deep. When simi-larly tested on an in vivo tumor, the prototype achieveda temperature rise of 13.5�C in 60 s.
The sharp rise and fall of the temperature dataas power was turned on and off in the tumor therapyexperiments (Figs. 10 and 11) further suggests that theobserved heating was predominantly due to absorptionof ultrasound energy (rather than thermal conduction ofany internal transducer heating), and it alsodemonstrates the range and control of achievable tissuetemperatures using an IVUS-sized transducer (Frinkleyet al. 2005). The sequential excitations were effectivelyset at 100% power, 50% power, and 25% power, andthe resulting increases in temperature were proportional.
The lower temperature increase in the tissue-mimicking material, relative to the tumor experimentresults, is likely due to the fact that the transducer wasnot directly in contact with the tissue. This may haveallowed for some amount of divergence and reflectionof the ultrasound energy beam (Herickhoff et al. 2010).The presence of a water path also served to somewhatisolate the sample from any conductive heating contribu-tions that may have been present. The 19.1�C and 13.5�Cincreases in the excised and in vivo tumor experimentswere much higher than the minimum increase of 4�Cnecessary for drug release from thermosensitive lipo-somes, demonstrating that it is possible to facilitatethermally-targeted drug delivery using a transducer smallenough to be packaged in a 3.5-Fr IVUS catheter.The challenges that remain for realizing a dual-mode,
catheter device for image-guided therapy include furtherimproving transducer efficiency (by incorporatingacoustic matching layers), customizing packaging, andwiring to electronics capable of both higher-frequencypulsed excitation (for imaging) and lower-frequencycontinuous-wave excitation (for therapy).
CONCLUSIONS
In total, the images obtained using the 3.5-Frmodified Atlantis prototype and commercially-availableVolcano catheters in brain and vascular-access experi-ments demonstrate that: (1) it is possible to use an intravas-cular ultrasound device to effectively visualize structuresin the brain that are in close proximity to the transducer,

Dual-mode IVUS transducer for image-guided brain therapy d C. D. HERICKHOFF et al. 1675
and (2) that catheter probes may be placed intracraniallyvia a minimally-invasive vascular approach. It was alsoshown that a 5 3 0.5 3 0.22 mm PZT-4 transducer iscapable of heating a tumor in vivo113.5�C above baselinetemperature, a value well above the 14�C threshold fordrug release from thermosensitive liposomes.
Our results indicate that combining these imagingand therapeutic capabilities into a single dual-modedevice may be feasible, and that this could yield a clini-cally-viable technology for brain tumor treatment. Futureexperiments will investigate the therapeutic effect sucha device may have on an intracranial brain tumor.
Acknowledgments—The authors thank Volcano Corporation for theirsupport in this study, as well as Veronica Rotemberg, Samantha Lipman,Josh Doherty, Tat-Jin Teo, Rick Stouffer and Ellen Dixon-Tulloch fortheir assistance. This work was supported by NIH grant HL089507.
REFERENCES
ACS. Cancer Facts & Figures 2009. Atlanta American Cancer Society,2009:4.
Aubry JF, Tanter M, Pernot M, Thomas JL, Fink M. Experimentaldemonstration of noninvasive transskull adaptive focusing basedon prior computed tomography scans. J Acoust Soc Am 2003;113:84–93.
Bacon DR, Shaw A. Experimental validation of Predicted TemperatureRises in Tissue-Mimicking Materials. Phys Med Biol 1993;38:1647–1659.
Barthe PG, Slayton MH, Jaeger PM, Makin IRS, Gallagher LA,Mast TD, Runk MM, Faidi W. Ultrasound therapy system and abla-tion results utilizing miniature imaging/therapy arrays. Montreal.IEEE Ultrason Symp 2004;3:1792–1795.
Bernstein M, Berger M. American Association of NeurologicalSurgeons, Joint Tumor Section, Congress of Neurological Surgeons.Neuro-oncology: The essentials. New York: Thieme MedicalPublishers; 2000.
Bloch SH, Dayton PA, Ferrara KW. Targeted imaging using ultrasoundcontrast agents. IEEE Eng Med Biol Mag 2004;23:18–29.
Bouchoux G, Lafon C, Berriet R, Chapelon JY, Fleury G, Cathignol D.Dual-mode ultrasound transducer for image-guided interstitialthermal therapy. Ultrasound Med Bio 2008;34:607–616.
Bouchoux G, Owen NR, Chavrier F, Berriet R, Fleury G, Chapelon JY,Lafon C. Interstitial thermal ablation with a fast rotating dual-modetransducer. IEEE Trans Ultrason Ferroelectr Freq Control 2010;57:1086–1095.
Cabantog AM, BernsteinM. Complications of first craniotomy for intra-axial brain-tumor. Can J Neurol Sci 1994;21:213–218.
CBTRUS. Statistical report: Primary brain tumors in the United States,2000-2004. Central Brain Tumor Registry of the United States 2008;10:7–8.
Cho CW, Liu Y, Cobb WN, Henthorn TK, Lillehei K, Christians U,Ng KY. Ultrasound-induced mild hyperthermia as a novel approachto increase drug uptake in brain microvessel endothelial cells. PharmRes 2002;19:1123–1129.
Choi JJ, Pernot M, Small SA, Konofagou EE. Noninvasive, transcranialand localized opening of the blood-brain barrier using focused ultra-sound in mice. Ultrasound Med Biol 2007;33:95–104.
Chow K, Gobin YP, Saver J, Kidwell C, Dong P, Vinuela F. Endovascu-lar treatment of dural sinus thrombosis with rheolytic thrombectomyand intra-arterial thrombolysis. Stroke 2000;31:1420–1425.
Connors JJ, Wojak JC. Interventional neuroradiology: Strategies andpractical techniques. Philadelphia: Saunders; 1999.
Dayton PA, Ferrara KW. Targeted imaging using ultrasound. J MagnReson Imaging 2002;16:362–377.
Dowd CF, Malek AM, Phatouros CC, Hemphill JC. Application ofa rheolytic thrombectomy device in the treatment of dural sinusthrombosis: A new technique. Am J Neuroradiol 1999;20:568–570.
Ebbini ES, Yao H, Shrestha A. Dual-mode ultrasound phased arrays forimage-guided surgery. Ultrason Imaging 2006;28:65–82.
Erbel R. Intravascular ultrasound. St. Louis: Mosby; 1998.Fadul C, Wood J, Thaler H, Galicich J, Patterson RH, Posner JB.
Morbidity and mortality of craniotomy for excision of supratentorialgliomas. Neurology 1988;38:1374–1379.
Fishbein MC, Siegel RJ. Pathology of coronary atherosclerosis: Impli-cations for intravascular ultrasound imaging. In: Siegel RJ, (ed).Intravascular ultrasound imaging in coronary artery disease. NewYork: Dekker; 1998. p. 1–17.
Fletcher TF, Hardy RM, Feeney DA. Canine planar anatomy. (Online),2006. http://vanat.cvm.umn.edu/planar/. Accessed Jun 12, 2008.
Foster FS, Ryan LK, Lockwood GR. High frequency ultrasoundscanning of the arterial wall. In: Roelandt J, (ed). Intravascularultrasound. Dordrecht; Boston: Kluwer Academic Publishers;1993. p. 91–108.
Frinkley K, Palmeri M, Nightingale K. Controlled spatio-temporal heat-ing patterns using a commercial, diagnostic ultrasound system. 2005IEEE Ultrason Symp 2005;1130–1134.
Fry WJ, Fry RB. Determination of absolute sound levels and acousticabsorption coefficients by thermocouple probes–Experiment.J Acoust Soc Am 1954;26:311–317.
Gentry KL, Smith SW. Integrated catheter for 3-D intracardiac echocardiography and ultrasound ablation. IEEE Trans Ultrason Ferroe-lectr Frequency Control 2004;51:800–808.
Goss SA, Johnston RL, Dunn F. Comprehensive compilation of empir-ical ultrasonic oroperties of mammalian-tissues. J Acoust Soc Ama1978;64:423–457.
Guthkelch AN, Carter LP, Cassady JR, Hynynen KH, Iacono RP,Johnson PC, Obbens EAMT, Roemer RB, Seeger JF, Shimm DS,Stea B. Treatment of malignant brain-tumors with focused ultra-sound hyperthermia and radiation–Results of a phase-I trial.J Neuro-Oncol 1991;10:271–284.
Herickhoff CD, Grant GA, Britz GW, Smith SW. Dual-mode IVUScatheter for intracranial image-guided hyperthermia: Feasibilitystudy. IEEE Trans Ultrason Ferroelectr Freq Control 2010;57:2572–2584.
Herickhoff CD, Light ED, Bing KF, Mukundan S, Grant GA, Wolf PD,Smith SW. Dual-mode intracranial catheter integrating 3-D ultra-sound imaging and hyperthermia for neuro-oncology: Feasibilitystudy. Ultrason Imaging 2009;31:81–100.
Horowitz M, Purdy P, Unwin H, Carstens G, Greenlee R, Hise J,Kopitnik T, Batjer H, Rollins N, Samson D. Treatment of dural sinusthrombosis using selective catheterization and urokinase. AnnNeurol 1995;38:58–67.
Hynynen K. Review of ultrasound therapy. Toronto, 1997. IEEE Ultra-son Symp 1997;2:1305–1313.
Hynynen K, Clement GT, McDannold N, Vykhodtseva N, King R,White PJ, Vitek S, Jolesz FA. 500-element ultrasound phased arraysystem for noninvasive focal surgery of the brain: A preliminaryrabbit study with ex vivo human skulls. Magn Reson Med 2004;52:100–107.
Hynynen K, Edwards DK. Temperature-measurements during ultra-sound hyperthermia. Med Phys 1989;16:618–626.
Hynynen K, Jolesz FA. Demonstration of potential noninvasive ultra-sound brain therapy through an intact skull. Ultrasound Med Biol1998;24:275–283.
Hynynen K, McDannold N, Vykhodtseva N, Jolesz FA. NoninvasiveMR imaging-guided focal opening of the blood-brain barrier inrabbits. Radiology 2001;220:640–646.
KheirolomoomA, Dayton PA, LumAFH, Little E, Paoli EE, Zheng HR,Ferrara KW. Acoustically-active microbubbles conjugated to lipo-somes: Characterization of a proposed drug delivery vehicle.J Control Release 2007;118:275–284.
Kilroy JP, Patil AV, Hossack JA. Ultrasound catheter for microbubblebased drug delivery. Rome, 2009. IEEE Ultrason Symp2009;2770–2773.
Kleihues P, CaveneeWK, International Agency for Research on Cancer,International Society of Neuropathology, International Academy of

1676 Ultrasound in Medicine and Biology Volume 37, Number 10, 2011
Pathology, Preuss Foundation for Brain Tumor Research. Pathologyand genetics of tumours of the nervous system. Lyon: IARC Press;2000.
Kroll RA, Neuwelt EA. Outwitting the blood-brain barrier for thera-peutic purposes: Osmotic opening and other means. Neurosurgery1998;42:1083–1099.
Kuether TA, O’Neill O, Nesbit GM, Barnwell SL. Endovascular treat-ment of traumatic dural sinus thrombosis: Case report. Neurosurgery1998;42:1163–1166.
LesniakMS. Targeting Drugs to Tumors of the Central Nervous System.In: Ali-Osman F, (ed). Brain tumors. Totowa, NJ: Humana Press;2005. p. 353.
Makin IRS, Mast TD, Faidi W, Runk MM, Barthe PG, Slayton MH.Miniaturized ultrasound arrays for interstitial ablation and imaging.Ultrasound Med Biol 2005;31:1539–1550.
Mareel M. Anti-invasive brain tumor therapy: General aspects andfuture strategies. In: Mikkelsen T, (ed). Brain Tumor invasion:Biological, clinical, and therapeutic considerations. New York:Wiley-Liss; 1998. p. 391–414.
McDannold N, Clement GT, Black P, Jolesz F, Hynynen K. Transcranialmagnetic resonance imaging-guided focused ultrasound surgery ofbrain tumors: Initial findings in three patients. Neurosurgery 2010;66:323–332.
McDannold N, Vykhodtseva N, Hynynen K. Use of ultrasoundpulses combined with Definity for targeted blood-brain barrierdisruption: A feasibility study. Ultrasound Med Biol 2007;33:584–590.
McDannold N, Vykhodtseva N, Hynynen K. Blood-brain barrier disrup-tion induced by focused ultrasound and circulating preformed mi-crobubbles appears to be characterized by the mechanical index.Ultrasound Med Biol 2008;34:834–840.
Mehran R, Mintz GS, Pichard AD, Kent KM, Satler LF, Popma JJ,Leon MB. Clinical application of intravascular ultrasound imagingin a center with high-volume preintervention ultrasound imaging.In: Siegel RJ, (ed). Intravascular ultrasound imaging in coronaryartery disease. New York: Dekker; 1998. p. 59–73.
Mesiwala AH, Farrell L, Wenzel HJ, Silbergeld DL, Crum LA,Winn HR, Mourad PD. High-intensity focused ultrasound selec-tively disrupts the blood-brain barrier in vivo. Ultrasound MedBiol 2002;28:389–400.
Mikkelsen T. Brain tumor invasion: Biological, clinical, and therapeuticconsiderations. New York: Wiley-Liss; 1998.
Miselis RR. Neuroscience laboratory: Laboratory 2–3: Gross brainand spinal cord. (Online), 2006. http://cal.vet.upenn.edu/projects/neurology/lab2/lab2.htm. Accessed Jun 17, 2008.
Morris P. Interventional and endovascular therapy of the nervoussystem: A practice guide. New York: Springer; 2002.
Nishioka T, LuoH, Eigler NL, Siegel RJ, Tabak SW. Clinical applicationof IVUS imaging in a center with selective use of IVUS imaging. In:Siegel RJ, (ed). Intravascular ultrasound imaging in coronary arterydisease. New York: Dekker; 1998. p. 75–94.
Novak Z, Coldwell DM, Brega KE. Selective infusion of urokinase andthrombectomy in the treatment of acute cerebral sinus thrombosis.Am J Neuroradiol 2000;21:143–145.
Opatowsky MJ, Morris PP, Regan JD, Mewborne JD, Wilson JA. Rapidthrombectomy of superior sagittal sinus and transverse sinusthrombosis with a rheolytic catheter device. Am J Neuroradiol1999;20:414–417.
Phillips LC, Klibanov AL, Wamhoff BR, Hossack JA. Intravascularultrasound mediated delivery of DNA via microbubble carriers toan injured porcine artery in vivo. Beijing, 2008. IEEE UltrasonSymp 2008;1154–1157.
Ponce AM, Vujaskovic Z, Yuan F, Needham D, Dewhirst MW. Hyper-thermia mediated liposomal drug delivery. Int J Hyperther 2006;22:205–213.
Prados MD. Systemic Chemotherapy. In: Bernstein M, Berger MS,(eds). Neuro-oncology: The essentials. New York: Thieme MedicalPublishers; 2000. p. 228–229.
Pua EC, Qiu YP, Smith SW. Integrated endoscope for real-time 3-Dultrasound imaging and hyperthermia: Feasibility study. UltrasonImaging 2007;29:1–14.
Sawaya R, Hammoud M, Schoppa D, Hess KR, Wu SZ, Shi WM,Wildrick DM. Neurosurgical outcomes in a modern series of 400craniotomies for treatment of parenchymal tumors. Neurosurgery1998;42:1044–1055.
Schottenfeld D, Fraumeni JF. Cancer epidemiology and prevention.New York: Oxford University Press; 1996.
Shaw A, Pay NM, Preston RC, Bond AD. Proposed standard thermal testobject formedical ultrasound.UltrasoundMedBiol1999;25:121–132.
Uren NG, Yock PG, Fitzgerald PJ. Intravascular ultrasound image inter-pretation: Normal arteries, abnormal vessels, and atheroma typespre- and postintervention. In: Siegel RJ, (ed). Intravascular ultra-sound imaging in coronary artery disease. New York: Dekker;1998a. p. 19–37.
Uren NG, Yock PG, Fitzgerald PJ. Prognostic implications of intravas-cular ultrasound imaging after coronary intervention. In: Siegel RJ,(ed). Intravascular ultrasound imaging in coronary artery disease.New York: Dekker; 1998b. p. 39–57.
Vykhodtseva N, McDannold N, Hynynen K. Progress and problems inthe application of focused ultrasound for blood-brain barrier disrup-tion. Ultrasonics 2008;48:279–296.
Welker WI. Comparative mammalian brain collections. (Online), 2011.http://brainmuseum.org/Specimens/artiodactyla/pig/index.html. Ac-cessed Jan 18, 2011.
Wilkins RH, Rengachary SS. Neurosurgery. New York: McGraw-Hill,Health Professions Division; 1996.
Wrensch M, BondyML,Wiencke J, Yost M. Environmental risk-factorsfor primary malignant brain tumors–A review. J Neuro-Oncol 1993;17:47–64.
Wu F, Chen WZ, Bai J, Zou JZ, Wang ZL, Zhu H, Wang ZB. Patholog-ical changes in human malignant carcinoma treated with high-intensity focused ultrasound. Ultrasound Med Biol 2001;27:1099–1106.
Zunkeler B, Carson RE, Olson J, Blasberg RG, DeVroom H, Lutz RJ,Saris SC, Wright DC, Kammerer W, Patronas NJ, Dedrick RL,Herscovitch P, Oldfield EH. Quantification and pharmacokineticsof blood-brain barrier disruption in humans. J Neurosurg 1996;85:1056–1065.