Cytotoxic Drug Treatment

of 6
-
Upload
pipidh-cupidd -
Category
Documents
-
view
213 -
download
0
Transcript of Cytotoxic Drug Treatment
-
7/30/2019 Cytotoxic Drug Treatment
1/6
CME Journal of Gynecologic Oncology 6772 67
Cytotoxic drug treatment
of vulval and vaginal cancer
GAVIN M. MAR X, M.D., MICHAEL L.
FRIEDLANDER, M.D., NEVILLE F. HACKER, M.D.
ABSTRACT Patients with operable vulval cancer without nodal
involvement usually have excellent survival rates, but this falls
significantly in those patients with nodal involvement. The role
of cytotoxic drug treatment in vulval cancer is limited. There are
few data on the role of chemotherapy in the management of
patients with vulval cancer. The available data relate to preop-
erative chemotherapy, usually used in combination with radio-
therapy, to downstage advanced tumors in an attempt to ren-
der them operable, reduce the extent of surgery, or the need for
permanent stomas. There are also some data on concurrent
chemo-radiotherapy as an alternative to surgery in selected
patients. There a re virtually no definitive studies in patients with
metastatic vulval cancer. This paper highlights some of these
treatment options using chemotherapy in combination with
radiation as neoadjuvant and definitive therapy. Chemotherapy
has a very limited role in the management of vaginal cancer.
Key words vaginal, vulval, chemotherapy, radiotherapy, metas-tatic
VULVAL CANCER Vulval cancer accounts for about 4% of gyne-
cological malignancies and is highly curable when diagnosed
early. In patients with operable vulval cancer without nodal
involvement the overall survival rate is about 85-90%, but this
falls to 50-60% in those patients with nodal involvement.
Radical radiotherapy, usually combined with surgical resec-
tion of the tumor bed, can result in long-term survival in those
patients in whom surgical resection would necessitate some
type of pelvic exenteration and a permanent stoma.
The role of cytotoxic drug treatment in vulval cancer is limi-
ted. There are few data on the role of chemotherapy in the
management of patients with vulval cancer. The available
data relate to preoperative chemotherapy, usually used in
combination with radiotherapy, to downstage advanced
tumors in an attempt to render them operable, reduce the
extent of surgery, or the need for permanent stomas. There
are also some data on concurrent chemo-radiotherapy as an
alternative to surgery in selected patients. There are virtually
no definitive studies in patients with metastatic vulval cancer
making it impossible to make any evidence-based decisions in
this setting.
PREOPERATIVE TREATMENT A number of investigators have evalu-
ated the potential role of neoadjuvant chemotherapy in
patients with advanced vulval cancer. There have been no
randomised controlled trials assessing the impact of preoper-
ative trea tment. It ha s generally been used in those pa tients in
whom primary surgery was likely to require exenteration or
formation of permanent stomas or if patients were deemed
medically unfit to undergo a major surgical procedure.
COMBINATION CHEMOTHERAPY Combination chemotherapy alone inthe preopera tive setting has been studied by the Italian group
under Benedetti Panici (1). They treated 21 patients with
advanced (FIGO stage IVA) vulval squamous cell carcinoma
with 2-3 cycles of neoadjuvant cisplatin (100 mg/m 2 day 1),
bleomycin (15 mg day 1 and 8) and methotr exate (300 mg/m2
day 8). Ten percent had a partial response in the primary and
67% had a complete or partial response in the nodes. They
reported a 3-year survival rate of 24%, which was influenced
by stage, pathological downstaging and nodal involvement.Sixty-eight percent of the operated patients recurred 3-17
months from the completion of treatment with half having
distant relapses. These results were disappointing and the
authors concluded that there was no substantial benefit from
the addition of chemotherapy, without concurrent radiation,
prior to surgery.
COMBINATION CHEMO-RADIATION The combination of chemotherapywith radiation has been used in an attempt to improve the
results of radiation alone. A number of agents have been used
which act as radiation sensitisers and also may have some
impact on systemic disease.
Moore et al. (2) assessed the impact of neoadjuvant chemo-
radiotherapy on reducing the need for rad ical surgery in T3 and
T4 primary tumors. Seventy-three patients with FIGO stage
III/IV vulval cancer were enrolled in a prospective multi-insti-
tutional study. Treatment consisted of a split course of con-
current chemotherapy with cisplatin and 5-FU and radiother -
apy, followed by surgery to the primary lesion and inguinal
and femoral nodes. Radiation was delivered to the primary
tumour volume via anterior-posterior and postero-anterior
fields in 1.7 Gy fractions to a dose of 47.6 Gy. At surgery
Address correspondence to:
Gavin Mar x, M.D.
Departme nt of Medical Oncology
Prince of Wales Hospital
High St, Randwick NSW 2031, Sydney, Australia
Phone (44 207) 955 5000 Fax (44 207) 955 4939
E-mail [email protected]
-
7/30/2019 Cytotoxic Drug Treatment
2/6
68 CME Journal of Gynecologic Oncology 6772
Cytotoxic drug treatment of vulval and vaginal cancer
46.5% had no visible vulval cancer and 53.5% (38 patients)
had gross residual disease. Seven patients did not undergo
surgery for various reasons. Five of the 38 patients with gross
residual disease had positive re section margins requiring fur-
ther therapy; wide local excision, radiotherapy or vaginecto-
my. Using this therapeutic approach only 2/71 (2.8%) had
residual unresectable disease. Urinary and fecal continence
was preserved in all but 3 patients. They concluded that this
approach was feasible and may reduce the need for more rad-
ical surgery in patients with locally-advanced vulval cancer.
Scheistroen and Trop(3) from the Norwegian Radium H ospi-
tal treated 42 pat ients with advanced squamous cell carcinoma
of the vulva (20 primary lesions and 22 recurrent disease), with
the combination of preoperative bleomycin (180 mg) and
radiotherapy (30-45 Gy). The median survival in the pa tients
with primary disease was only 8 months and did not suggest
any value of neoadjuvant therapy (3). Only a small proportion
of patients in this study actually went on to have surgery
(4 patients with primary disease and no patients who were
treated for recurrent disease). The authors concluded that
even though the patients in their study had advanced disease,
the results were d isappointing and suggested tha t an increase
in the radiation dose and more aggressive surgery might have
improved the results.
Two groups have studied the combination of 5-fluorouracil
with mitomycin-C in combination with r adiation as preopera-
tive or neoadjuvant therapy.Lupi et al. (4) reported on com-
bined preoperative chemo-radiotherapy in 31 patients withlocally-advanced vulval cancer. They were treated with
2 courses of combination chemotherapy with mitomyin-C
(15 mg/m2 day 1) and 5-FU (750 mg/m2 continuous infusion
days 1-5) and concurrent radiotherapy to the inguinal and
pelvic nodes and vulva to a total dose of 36 Gy. Ninety-two
percent of primary cases and all patients with recurrent dis-
ease had an objective response. However, the postoperative
morbidity rate was 56% and mortality was 13.8%. At a median
follow up of 34 months the recurrence rate was 31.8%. They
concluded that if treatment related morbidity could be
decreased this combined approach might have a role in pa-
tients with locally-advanced vulval cancer.
Landoni et al. (5) prospectively evaluated the feasibility and
efficacy of neoadjuvant chemo-radiothe rapy in pa tients with
locally-advanced or recurrent disease. Fifty-eight patients
were treated with preopera tive external radiation to a dose of
54 Gy, divided into 2 cour ses with an inte rval of 2 weeks. 5-FU
(750 mg/m2 daily for 5 days) and mitomycin-C (15 mg/m 2 sin-
gle bolus) were commenced at the start of each course.
Eighty-nine percent of patients completed treatment and
72% underwent surgery. An objective response rate of 80%
was observed and pathologic complete responses were seen in
31%. Early severe toxicity occurred in 3 patients and there
was 1 treatment-related death. They felt that this treatment
provided good local control with acceptable toxicity (5).
Recent results presented at the ASTRO 1999 meeting in
abstract form also suggested a possible role for neoadjuvant
therapy.Montana and colleagues (6) on behalf of the Gyneco-
logic Oncology Group used a split course of chemo-radiothe-
rapy preoperatively in patients with locally-advanced disease.
Forty-six patients were treated with 2 cycles of combination
cisplatin-5-FU and radiotherapy. The radiotherapy was deliv-
ered using a AP/PA technique, delivering a dose of 23.8 Gy in
1.7 Gy per fraction bid on days 1-4 and 1.7 Gy per day for the
remainder of the treatment. The patients then had a 2-week
rest period then an additional treatment of radiation to bring
the total dose to 47.6 Gy. The chemotherapy was adminis-
tered at the start of each course of radiation. Cisplatin was
administered as 50 mg/m2 on days 1-4 and 5-FU was adminis-
tered as 1000 mg/m2/day on days 1-4, in week 1 of each cycle.
All but 6 patients were able to complete the chemo-radiothe-
rapy treatment. The response rate was promising with local
control in the nodal areas in 97% and in the primary in 76%.
Although there are some data to suggest that neoadjuvant
(preoperative) chemotherapy, in combination with radiation,
may downstage advanced vulval cancers and possibly permit
less aggressive surgery in selected patients this is still consid-
ered investigational, and only recommended in the context of
a clinical trial. There is no evidence to suggest that this
approach is associated with a survival bene fit. Clearly patientsneed to be carefully selected in view of the potential morbid-
ity associated with these treatments.
CONCURRENT CHEMO-RADIATION AS PRIMARY TREATMENT The role
of concurrent chemo-radiotherapy as a primary treatment
option is also unclear and has also not been studied in large
randomized trials. There is however reasonably extensive
experience with this approach as it is often used as an alter-
native to radical surgery in those patients deemed inoperable,
for various reasons.
Berek et al. (7) at UCLA conducted a phase II study of com-bination chemo-radiotherapy in 12 patients with FIGO stage
III-IV squamous cell carcinoma of the vulva. They used a
combination of cisplatin and 5-FU as a radiosensitizer. Cis-
platin was administered as an intravenous dose of 50 mg/m2/day
on day 1 and 2, or as 100 mg/m2 on day 1 or 2. The 5-fluoroura-
cil was administered as a continuous infusion of 1000 mg/m2/day
for 4-5 days. These treatments were given on the first and
28th day of radiation therapy. Pelvic radiation to a dose of
44-54 Gy was administered to the primary, groin and iliac ves-
sels to the level below the common iliac nodes. Responses
were seen in 92% with complete responses in 67%. At the
-
7/30/2019 Cytotoxic Drug Treatment
3/6
Chapter 18
CME Journal of Gynecologic Oncology 6772 69
completion of chemo-radiation radical vulvectomy or excision
was used in 3 patients and 1 patient had a posterior exentera-
tion. The treatment was well tolerated with no treatment-
related deaths. This group concluded that this combination
may provide an alternative to primary radical surgery in
patients with advanced cancer o f the vulva.
In a retrospective single institution study by Koh et al. (8) the
combination of chemo-radiotherapy was shown to be effec-
tive in the management of locally-advanced cancer of the
vulva. Twenty patients with locally-advanced or recurrent dis-
ease, who were not considered candidates for primary
surgery, were treated with concurrent 5-FU and radiotherapy.
Five patients also received cisplatin and 1 received mitomy-
cin-C. Ten pa tients had a complete response and 8 had partial
responses. Six patients with partial responses had re sidual tu-
mor successfully resected. The 5-year local control rate was
48%. Overall the trea tment was well tolerated with cutaneous
toxicities being the most common side effect observed.
Whalen et al. (9) concluded that combined chemo-radiation
was a reasonable alterna tive to radical vulvectomy in patients
with advanced disease (AJCC stage II-III). They evaluated
the combination of radiotherapy given concurrently with 5-FU
and mitomycin-C in 19 patients. With a median follow-up of
34 months a complete response rate of 53% and partial
response rate of 37% was observed. The combined modality
of chemo-radiation with or without wide local excision resulted
in a local control rate of 74% (14/19). Four of the 5 patients
with local recurrences were rendered disease free after radi-
cal surgery, for an overall local control rate of 95%.
Investigators from theMD A nderson Cancer Center(10) simi-
larly demonstrated that the combination of cisplatin/5-FU
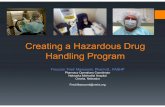
Table 1. Neoadjuvant treatment
Study Patients Chemotherapy Radiotherapy Results Toxicity Conclusions
Moore et al. 73 patients Split course 47.6 Gy to P 7 no surgery 3/71 unable to Preop chemoradiation is fea-
1998 FIGO III/IV Cisplatin and groins if nodes 33/71 no visible disease preserve urin/fecal sible and may decrease need
(2) Squamous 5-FU inoperable 38/71 gross residual disease continence for more radical surgery
Prospective 5/38 positive margins
multicentre 2/71 resid unresect disease (2.8%)
Benedetti- 21 patients 2-3 cycles Nil 2/21 (10%) PR at primary Acceptable morbidity Chemotherapy did not addPanici et al. FIGO IVA Cis 100 mg/m2 day 1 14/21 (67%) PR at nodes significant benefit to surgery
1993 Squamous bleo 15 mg day 1 and 8 3-year survival 24%
(1) MTX 300 mg/m2 day 8 68% recurrence at 3-17 months
Scheistroen 42 patients Bleomycin 180 mg 30-45 Gy P RR 15/20 (75%) 5 CR 10 PR Acceptable toxicity Results disappointing
et al. 1993 20 P, 22 Recurrent P MS 8 months No treatment related deaths ? Benefit if increase RT dose
(3) Squamous Rec 13/22 (59%) 2 CR 11 PR
Recurrent MS 6.4 months
Lu pi et al. 31 patients 2 cycles P inguinal and pelvic P R R 22/24 ( 92% ) Postoperative morbidity 65% Chemoradiation effective
1996 24 P, 7 recurrent Mito-C 15 mg/m2 day 1 nodes up to 36 Gy Rec RR 7/7 (100%) Mortality rate 13.8% May be an option if reduction
(4) Locally advanced 5-FU 750 mg/m2 CI day 1-5 2nd course after 55% nodal pathologic CR in morbidity/mortalitySquamous 2 weeks break to Recurrence rate 32% at
vulva only 18 Gy median FUP 34 months
Lando ni et al. 58 patients 2 cycles 54 Gy in 2 divided RR 80% 89% completed treatment Allows good control with
1996 41 P, 17 recurrent 5-FU 750 mg/m2 CI day 1, 5 doses Pathologic CR 31% 72% underwent postop surgery acceptable toxicity
(5) Squamous mito-C 15 mg/m2 day 1 Early severe tox in 3 patients Further FUP and long-term
Locally advaced 1 treatment-related death outcome FUP required
P primary Cis cisplatin Bleo bleomycin MTX methotr exate Mito-C mitomycin-C 5-FU 5-fluorouracil PR partial response MS median survival Resid residual
Rec recurrent CR complete response FUP follow-up CI continuous infusion RR response rate
-
7/30/2019 Cytotoxic Drug Treatment
4/6
70 CME Journal of Gynecologic Oncology 6772
Cytotoxic drug treatment of vulval and vaginal cancer
with rad iation was well tolerated with high response ra tes in
patients with loco-regionally advanced vulval cancer. Eleven
out of 12 patients had at least a partial clinical response. Of
the 8 patients who had post-therapy resection 50% had a
pathological complete response. Half the patients remained
disease free at 17-30 months post-treatment .
Cunningham et al. (11) evaluated a combination of chemo-
therapy and radiation as an alternative for those patients in
whom the location or extent of disease made pelvic exentera tion
the only surgical option. Fourteen patients with stage III-IV
vulval carcinoma were treated with cisplatin/5-FU and radia-
tion (vulva and groins 50-65 Gy, and pelvic doses of 45-50 Gy).
They reported a response rate of 92% with complete respon-
ses in 64%. In those patients with complete responses there
has only been 1 recurrence with a follow-up of 7-81 months.
All patients with partial responses died with a mean survival of
15.7 months (8-25). They concluded tha t surgical resection was
not necessary in patients with complete response.
In patients deemed inoperable for various reasons (presence
of initially unresectable disease, disease extent which would
necessitate part ial or tota l exenteration, severe comorbid ill-
ness precluding surgical management), combination chemo-
therapy and radiotherapy was studied by Russell et al. (12).
They trea ted 25 patients with stage II-IV squamous cell vul-
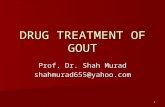
Table 2. Primary chemoradiotherapy
Study Patients Chemotherapy Radiotherapy Results Toxicity Conclusions
Berek et al. 12 patients 2 cycles 44-54 Gy CR 8/12 (67%) No treatment deaths Data support use of
(7) Phase II, Cis 50 mg/m2 day 1 and 2 to P. groin and PR 3/12 (25%) No grade IV toxicity this combination as
retrospective or 100 mg/m2 day 1 iliac nodes 10 pts disease-free Grade III desq 2 pts alternative to surgery
Sur g F IG O II I/I V 5-F U 1 g/m2 CI day 1-4 1 DVT
Med FUP 37 months
Koh et al. 20 patients 2-3 cycles 54 Gy CR 10/20 (50%) Well tolerated An effective option in Mx
(8) Retrospective 5-FU PR 8/20 (40%) Major acute toxicity was
FIGO III/IV 5 pts received cisplatin 5-year DFS (49%) skin
Non-surgical candidates 1 pt received mito-C
Med FUP 37 months
Whalen et al. 19 patients 2 cycles 45-50 Gy CR 10/19 (53%) Concurrent chemoradiation with
(9) AJCC II-III 5-FU 1 g/m2 CI day 1-4 to pelvis and grain nodes PR 7/19 (37%) local excision as required
Med FUP 34 months from 1991 1 dose of 10 pts had boosts Local control in 14/19 is a reasonable alternative
mito-C 10 mg/m2 day 1 6 had local resection 4/5 failures rendered disease- to radical surgery
free with surgery 95%
Eifel 12 patients 4 cycles (weekly) 40-50 Gy PR 11/12 (92%) Well tolerated Well tolerated
(10) Locally advanced Cis 4 mg/m2/d day 1-4 4/8 patho logical CR Min he mato l toxicity High R R in large vulval
5-FU 250 mg/m2/d day 1-4 6/12 disease-free 17-30 months No tr eatme nt delays tumors
Cunningham 14 patients 2 cycles 50-65 Gy RR in 92% Treatment delays in 5 pts Combination effectiveet al. Non-surgical candidates Cis 50 mg/m2 day 1 to vulva/groins CR in 9/14 (64%) DVT in 1 pt Acceptable toxicity
(11) Stage III/IV 5-FU 1 g/m2 CI day 1-4 45-50 Gy CR pts 1 recurrence Colonic stricture in 1 pt Surg excision not required in CR
to pelvis PR all died, MS 15.7 months
Russell et al. 25 patients P CR 16/18(89%) May hold a curative potential
(12) Non-surgical candidates Rec 4/7 (57%) for pts with unresectable or
Stage II-IV 14 disease-free medically inoperable disease
at median FUP 24 months
Med median FU P follow-up Surg surgery Cis cisplatin 5-FU 5-fluorouracil D day mito-C mitomycin-C CI continuous infusion PR partial response CR complete
response DVT deep venous throm bosis pts patients MS median survival DSF disease-free survival Mx management RR respon se rate
-
7/30/2019 Cytotoxic Drug Treatment
5/6
Chapter 18
CME Journal of Gynecologic Oncology 6772 71
val cancer. Seven patients had recurrent disease. Complete
responses were seen in 16/18 (89%) of previously untreated
patients and in 4/7 (57%) with recurrent disease. Fourteen
patients remained disease free 2-52 months (median 24
months) after tr eatment. They suggested that this might be an
alternative treatment option for such patients (12).
Results from the Yale group (13) were reported at ASTRO 1999.
They analyzed the impact of chemo-radiation in 54 patients with
locally-advanced vulval cancer. Fourteen patients were treated
with primary chemo-radiation, 12 with primary radiation, 6 with
adjuvant chemo-radiation and 22 with adjuvant radiation thera-
py. Chemotherapy consisted of infusional 5-FU and either cis-
platin or mitomycin-C, at the discretion of the physician. Radi-
ation doses when given with chemotherapy ranged from 45-46
Gy to the pelvis, vulva and inguinal regions with a boost of 56-
60 Gy to all gross disease. Those patients treated with radiation
alone were treated with 40-50 Gy with a boost to gross disease
to 60 Gy. Although this data was not randomised the primary
chemo-radiotherapy group had a statistically significant
increase in cause-specific survival, relapse-free survival and
overall survival over the primary radiotherapy group.
Combination chemo-radiation may be an alternative to exten-
sive surgery in patients with locally-advanced vulval cancer
but needs to be evaluated in randomized controlled studies.
For those pat ients unsuitable for pr imary radical surgery, con-
current chemo-radiotherapy may be a reasonable alternative
approach. Clearly, however, early detection with curative
surgery remains the optimal approach.
METASTATIC DISEASE The prognosis of patients with systemic
metastases from vulval cancer is poor. There are few data
available on effective treatment options for this group of
patients and no recommendations can be made due to the
paucity of published series. Most patients have squamous cell
carcinomas and it is the authors opinion that if chemotherapy
is to be used the approach should be similar to that taken for
patients with metastatic squamous cell cancer arising at other
sites.
VAGINAL CANCER Cancer of the vagina is an uncommon gyne-cological malignancy and it accounts for about 1-2 % of gyne-
cological malignancies. Squamous cell cancer is the most
common histological subtype. The standard treatment for
stage I disease is surgery or radiotherapy, which is associated
with a high rate of cure. Patients with stage IIA-IVA disease
are treated with radiation alone. No satisfactory treatment
exists for stage IVB and recurrent d isease.
There are only limited data available on the role of chemo-
therapy in these patients. Chemotherapy has generally only
been used in the salvage setting and the results have been
poor. Prior irradiation or surgery may reduce the delivery of
these agents to the tumor. Patients also tend to be older and
prior rad iation may also impact on hematologic reserves mak-
ing them less suitable candidates for chemotherapy.
Although numbers are small, there are reported studies of
both single-agent and combination chemotherapy in patients
with vaginal cancer. Overall the results have been disappoint-
ing. Mitoxantrone was assessed by the Gynecologic Oncology
Group (15). Nine patient s with advanced vaginal cancer were
treated with 12 mg/m2 mitoxantrone at 3 weekly intervals.
There were no responses to treatment and the median sur-
vival in patients with vaginal cancer was 2.7 months. Piver et
al. (16) demonstrated some activity in a small number of
patients with single-agent adriamycin. Etoposide has also
been studied and has not demonstrated any activity in
patients with advanced or recurrent vaginal tumors. Slayton et
al. (17) treated 16 pat ients with e toposide 100 mg/m2 on days
1, 3, 5 and demonstrated no anti-tumor activity.
Cisplatin as a single agent ha s also been shown to be ineffec-
tive in the trea tment of advanced or recurrent vaginal cancer.
The GOG (18) performed a phase II study of cisplatin
(50 mg/m2 q 3/52) in 22 evaluable patients with advanced or
recurrent cancer no longer amenable to control with surgery
or radiotherapy. Toxicity was acceptable but this agent did not
demonstrate activity in patients with vaginal cancer.
Newer agents may have some potential activity and Umesaki
et al. (19) repor ted the efficacy of the combination of cisplatinand irinotecan as neoadjuvant therapy in a pa tient with stage
II vaginal cancer. This patient had a clinical and pathological
complete response after 1 cycle of treatment.
There are few data regarding the role of combination chemora-
diation in vaginal cancer.Evans et al. (20) treated 7 patients with
stage II and III squamous cell vaginal cancer with mitomycin-C
and 5-fluorouracil with concurrent radiation. Fifty-seven per-
cent (4/7) achieved a complete response and remained disease
free at 8-39 months. Roberts et al. (21) treated 1 patient with
concominant radiation and cisplatin/5-fluorouracil and had a
complete response for an undefined period of time.
The prognosis for patients with metastatic disease remains
poor with no chemotherapeutic agents consistently demon-
strating efficacy in these patients. The introduction of newer
agents provides the opportunity for multi-institutional cooper-
ative clinical trials to identify agents with activity in this disease.
REFERENCES
1. Bendetti Pan ici P, Greggi S, Scambia G, Salerno G , Mancuso S. Cisplatin, bleomycin,
and methotrexate preoperative chemotherapy in locally advanced vulvar carcinoma.
Gynecol Oncol 1993; 50(1):49-53.
-
7/30/2019 Cytotoxic Drug Treatment
6/6
72 CME Journal of Gynecologic Oncology 6772
Cytotoxic drug treatment of vulval and vaginal cancer
2. Moore DH, Thomas GM, Montana GS, Saxer A, Gallup DG, Olt G. Preoperative
chemoradiation for a dvanced vulvar cancer: a ph ase II study of the G ynecologic Oncol-
ogy group. Int J Radiat Oncol Biol Phys 1998; 42(1):79-85.
3. Scheistroen M, Trope C. combined bleomycin and irradiation in preoperative treat-
ment of advanced squamous cell carcinoma of the vulva. Acta Oncol 1993; 32(6):657-
661.
4. Lupi G, Raspagliesi F, Zucali R, Fontanelli R, Palandini D, Kenda R, di Re F. com-
bined preoperative chemoradiotherapy followed by radical surgery in locally advanced
vulvar carcinoma. A pilot study. Cancer 1996; 77(8):1472-1478.
5. Landoni F, Maneo A, Zanetta G, Colombo A, Nava S, Placa F, et al. Concurrent pre-
operative chemotherapy with 5 fluorouracil and mitomycin C and radiotherapy
(FUMIR) followed by limited surgery in locally andvanced and recurrent vulvar carci-
noma. Gynecol Oncol 1996; 61(3):321-327.
6. Montana GS, Thomas GM, Moore DH, et al. Preoperative chemoradiotherapy for
carcinoma of the vulva with unr esectable lymph nodes: a G ynecologic Oncology Group
study. Proc ASTRO 1999 no.118.
7. Berek JS, Heaps JM, Fu YS, Juillard GJ, Hacker NF. Concurrent cisplatin and 5 flu-
orouracil chemotherapy and radiation therapy for advanced-stage squamous cell carci-
noma of the vulva. Gynecol Oncol 1991; 42(3):197-201.
8. Koh WJ, Wallace HJ, Gre er BE, Cain J, Stelzer KJ, Russell KJ, et al. Combined radio-
therapy and chemotherapy in the management of local-regionally advanced vulvar can-
cer. Int J R adiat Oncol Biol Ph ys 1993; 26(5):809-816.
9. Wahlen SA, Slater JD, Wagner RJ , Wang WA, Keeney ED , Hocko JM, e t al. Concur-rent radiation therapy and chemotherapy in the treatment of primary squamous cell car-
cinoma of the vulva. Cancer 1995; 75(9):2289-22294.
10. Eifel PJ, Morris M, Burke TW, Levenback C, Gershenson DM. Prolonged continu-
ous infusion cisplatin and 5-fluorouracil with radiation for locally advanced carcinoma
of the vulva. Gynecol Oncol 1995; 59(1):51-56.
11. Cunningham MJ, Goyer RP, Gibbons SK, Kredenster DC, Malfetano JH, Keys H.
Primary radiation, cisplatin, and 5-fluoroura cil for advanced squam ous carcinoma of the
vulva. Gynecol Oncol 1997; 66(2):258-261.
12. Russell AH, Mesic JB, Scudder SA, Rosenberg PJ, Smith LH, Kinney WK, et al. Syn-
chronous radiation and cytotoxic chemotherapy for locally advanced or recurrent squa-
mous cancer of the vulva. Gynecol Oncol 1992; 47(1):14-20.
13. Han SC, Kim DH, Kacinski BM. Addition of 5-fluorouracil and mitomycin-C or 5-
fluorouracil and cisplatin to radiation therapy decreases the local relapse rate and
improves cause specific survival in patients with vulva cancer. Proc ASTRO 1999 no.
119.
14. Jaakkola M, Ranatanen V, Grenman S, Kulmala J, Grenman R. Vulvar squamous
cell carcinoma cell lines are sensitive to paclitaxel in vitro. Anticancer Res 1997;
17(2A):939-943.
15. Muss HB, Bundy BN, Christopherson WA. Mitoxantrone in the treatment of
advanced vulvar and vaginal carcinoma. A Gynecologic Oncology Group study. Am J
Clin Oncol 1989; 12(2):142-144.
16. Piver M S, Barlow JJ, Xynos FP. Adriamycin alone or in combination in 100 patients
with carcinoma of the cervix or vagina. Am J Obstet Gynecol 1978; 131:311-313.
17. Slayton RE, Blessing JA, Beecham J, DiSaia PJ. Phase II trial of etoposide in the
management of advanced or recurrent squamous cell carcinoma of the vulva and carci-
noma of the vagina: a Gynecologic Oncology Group study. Cancer Treat Rep 1987;
71(9):869-870.
18. Thigpen JT, Blessing JA, Homesley HD, Berek JS, Creasman WT. Phase II trial of
cisplatin in advanced or recurren t cancer of the vagina: a G ynecologic Oncology Group
study. Gynecol Oncol 1986; 23(1):101-104.
19. Umesaki N, Ka wamura N, Tsujimura A, Ichimura T, Tanaka T, Ogita S. Stage II vagi-nal cancer. Responding to chemotherapy with irinotecan and cisplatin: a case report.
Oncol Rep 1999; 6(1):123-125.
20. Evans LS, Kersh CR, Con stable WC, et a l. Concominant 5-fluorouracil, mitomycin-
C, and radiotherapy for advanced gynecologic cancer. Int J Radiat Biol Phys 1998;
15:901-906.
21. Roberts WS, Kavanagh JJ, Greenberg H, et al. Concominant radiation therapy and
chemotherapy in the treatment of advanced squamous carcinoma of the female genital
tract. Gynecol Oncol 1989; 34:183-186.