Cytogenetics of infertile men - Human Reproduction
26
Cytogenetics of infertile men E.Van Assche 1 * 3 , M-Bonduelle 1 , H.Tournaye 2 , HJoris 2 , G.Verheyen 2 , P-Devroey 1 , A.Van Steirteghem 2 and I.Liebaers 1 'Centre for Medical Genetics and 2 Centre for Reproductive Medicine, University Hospital, Dutch-speaking Free University of Brussels (Vrije Universiteit Brussel), Laarbeeklaan 101, B-1090 Brussels, Belgium 3 To whom correspondence should be addressed Chromosomally derived sterility has long been recognized. A review of the literature of somatic chromosome investigations in infertile males has shown that 13.7% of azoospermic males and 4.6% of oligozoospermic males have an abnormal karyotype. In the first group, sex chromosome abnormalities predominate (mainly 47,XXY), whereas in the latter, autosome anomalies (i.e. Robertsonian and reciprocal translocations) are the most frequent. A similar review on meiotic studies revealed that meiotic chromosome anomalies can explain male infertility in 4.3-40.4% of patients. Recently, fluorescent in-situ hybridization studies on spermatozoa from infertile men were pub- lished; it was suggested that both X-Y pairing and pairing of the autosomes were impaired, resulting in spermatogenic disruption. We investigated cytogenetically 694 infertile men with abnormal sperm parameters. More patients are needed for this research to investigate the relationship, if any, between the type of chromosome abnormality and its influence on the number, morphology and motility of spermatozoa. To be able to provide proper counselling for those couples whose male infertility can now be treated by intracytoplasmic sperm injection, it is suggested that clinical investigations should include mitotic and meiotic studies, an analysis of the chromosome content of individual spermatozoa and a DNA analysis of blood and spermatozoa to detect partially deleted Y chromosome material. Key words: chromosome aberration/infertility/meiosis/spermatogenesis Introduction Infertility, the inability to produce living offspring after attempting to do so for 1 year, affects 13% of couples in Western Europe. Some 3% of all marriages are involuntarily childless, and 6% of couples are not able to have as many children as they would wish (Greenhall and Vessey, 1990). In a proportion of these cases, a genetic factor affecting gamete formation or function is responsible. 'Chromosomally derived' sterility, i.e. chromosome aberration as a possible cause of infertility because of 'abnormal' spermatogenesis, has long been known (Searle et al, 1978). Only recently have other genetic causes at the molecular level been Human Reproduction Volume 11 Supplement 4 1996 C European Society for Human Reproduction and Embryology 1 Downloaded from https://academic.oup.com/humrep/article/11/suppl_4/1/641247 by guest on 18 February 2022
Transcript of Cytogenetics of infertile men - Human Reproduction

Cytogenetics of infertile men
E.Van Assche1*3, M-Bonduelle1, H.Tournaye2, HJoris2,G.Verheyen2, P-Devroey1, A.Van Steirteghem2 and
I.Liebaers1
'Centre for Medical Genetics and 2Centre for Reproductive Medicine,University Hospital, Dutch-speaking Free University of Brussels (Vrije
Universiteit Brussel), Laarbeeklaan 101, B-1090 Brussels, Belgium3To whom correspondence should be addressed
Chromosomally derived sterility has long been recognized. A review of theliterature of somatic chromosome investigations in infertile males has shownthat 13.7% of azoospermic males and 4.6% of oligozoospermic males havean abnormal karyotype. In the first group, sex chromosome abnormalitiespredominate (mainly 47,XXY), whereas in the latter, autosome anomalies(i.e. Robertsonian and reciprocal translocations) are the most frequent. Asimilar review on meiotic studies revealed that meiotic chromosome anomaliescan explain male infertility in 4.3-40.4% of patients. Recently, fluorescentin-situ hybridization studies on spermatozoa from infertile men were pub-lished; it was suggested that both X-Y pairing and pairing of the autosomeswere impaired, resulting in spermatogenic disruption. We investigatedcytogenetically 694 infertile men with abnormal sperm parameters. Morepatients are needed for this research to investigate the relationship, if any,between the type of chromosome abnormality and its influence on thenumber, morphology and motility of spermatozoa. To be able to provideproper counselling for those couples whose male infertility can now betreated by intracytoplasmic sperm injection, it is suggested that clinicalinvestigations should include mitotic and meiotic studies, an analysis of thechromosome content of individual spermatozoa and a DNA analysis of bloodand spermatozoa to detect partially deleted Y chromosome material.Key words: chromosome aberration/infertility/meiosis/spermatogenesis
Introduction
Infertility, the inability to produce living offspring after attempting to do so for1 year, affects 13% of couples in Western Europe. Some 3% of all marriages areinvoluntarily childless, and 6% of couples are not able to have as many childrenas they would wish (Greenhall and Vessey, 1990). In a proportion of thesecases, a genetic factor affecting gamete formation or function is responsible.'Chromosomally derived' sterility, i.e. chromosome aberration as a possible causeof infertility because of 'abnormal' spermatogenesis, has long been known (Searleet al, 1978). Only recently have other genetic causes at the molecular level been
Human Reproduction Volume 11 Supplement 4 1996 C European Society for Human Reproduction and Embryology 1
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

E.Van Assche et al
studied and described (Anderson et al, 1988; Ma et al, 1992; Voght et al, 1992;Chandley and Cooke, 1994; Reijo et al, 1995).
As early as 1957, Ferguson-Smith et al. suspected the existence of chromosomeabnormalities in patients attending a male fertility clinic. They found a Barrbody in 10 of the 91 males studied for azoospermia or severe oligozoospermia.Some 2 years later, Jacobs and Strong (1959) showed that these men withKlinefelter's syndrome had a 47,XXY chromosome constitution.
Since then, several surveys have been conducted to determine the chromosomefactor in male infertility. Only a few studies were performed before theintroduction of chromosome banding (Kjessler, 1966; Philip et al, 1970;Dutrillaux et al, 1971); most were carried out after banding techniques hadbecome routine in human cytogenetic laboratories (Koulischer and Schoysman,1974; Chandley et al, 1975; Hendry et al, 1976; Abramsson et al, 1982;Zuffardi and Tiepolo, 1982; de Gardelle et al, 1983; Chandley, 1984; Micicet al, 1984; Retief et al, 1984; Bourrouillou et al, 1985; Matsuda et al, 1989;Yoshida et al, 1995).
In the largest series, reported without the application of banding techniques(Kjessler, 1966), 1363 male partners from infertile couples were investigatedcytogenetically. In all, 70 males revealed numerical sex chromosome abnormalitiesin their constitutional karyotype, 16 had a translocation and four had an extramarker chromosome. Moreover, this study also pointed to a relationship betweendeclining sperm counts and increasing frequencies of chromosome abnormalities.
In this review, based on several surveys reported during the last 20 years, thetypes and frequencies of chromosome aberrations are discussed according to thetype of male infertility problem. Data on the relationship between meioticabnormalities and male infertility will be provided. Cytogenetic studies ofspermatozoa from infertile men will be highlighted. Finally our own results,based on a cytogenetic investigation of 694 men with aberrant sperm parameters,will be presented and discussed briefly.
Somatic chromosome investigations in male infertility
There are important variations in the incidence of constitutional chromosomeanomalies in the populations of infertile men investigated in different publishedseries. Different ascertainment procedures have been used in these surveys, whichmakes it difficult to analyse and compare the results. In some studies, all menattending infertility clinics were karyotyped, while in others an analysis was onlycarried out in cases of absence of spermatozoa or low sperm counts (azoospermicand oligozoospermic men). Furthermore, some authors reported on oligozoo-spermic males with a sperm count <10Xl06/ml and others on oligozoospermicmen with a count <30 or 40Xl06/ml. This illustrates the 'variation' in thedefinition of oligozoospermia. Smith and Steinberger (1977) suggested thatoligozoospermia should be characterized as a sperm count <10Xl06/ml, buttheir suggestion has not been accepted by all authors. In our hospital, the latestWorld Health Organization (WHO) guidelines are followed (WHO, 1987); thus
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

Chromosome studies in infertile men
Table I. Number (%) of chromosome abnormalities observed in seven series of infertile men[including azoospermic and oligozoospermic males, except for Matsuda et al. (1989; theseauthors considered 295 normozoospermic males)]
References
Koulischer and Schoysman (1974)Chandley (1979)Zuffardi and Tiepolo (1982)Abramsson et al. (1982)de Gardelle et al. (1983)Matsuda et al. (1989)Yoshida et al. (1995)Total
Newborn infants
No.
100023722542342318295
10077876
94 465
Sex chromosomes
27 (2.7)33 (1.4)
175 (6.9)6 (1.8)
13 (4.1)0(0)
41 (4.1)295 (3.8)
131 (0.14)
Autosomes
6 (0.6)18 (0.7)
40 (1.6)4 (1.2)7 (2.2)5 (1.7)
24 (2.4)104 (1.3)
232 (0.25)
Total
33 (3.3)51 (2.1)
215 (8.6)10 (2.9)20 (6.3)5 (1.7)
65 (6.5)399 (5.1)
366 (0.38)
men presenting sperm counts <20X106/ml are defined as oligozoospermic.Finally, the presentation of chromosome results in certain studies includedkaryotypes with minor abnormalities or variant chromosomes (i.e. polymorph-isms), such as pericentric inversion of the heterochromatic region of chromosome9, although these are also known to be common among normal fertile individualsin the general population (Court-Brown et al., 1965).
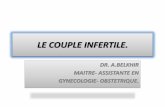
The cytogenetic results of the seven largest and most relevant studies ofinfertile men (including azoospermic and oligozoospermic males) are summarizedin Tables I-HJ and will be compared with those determined in studies of newbornchildren (Table IV). Tables V-VII present the cytogenetic results from the twolargest series of men with sperm counts <10X106/ml and the three largest seriesof men with sperm counts <20X106/ml. Tables VIQ-X show the cytogeneticresults from the six largest studies of azoospermic men.
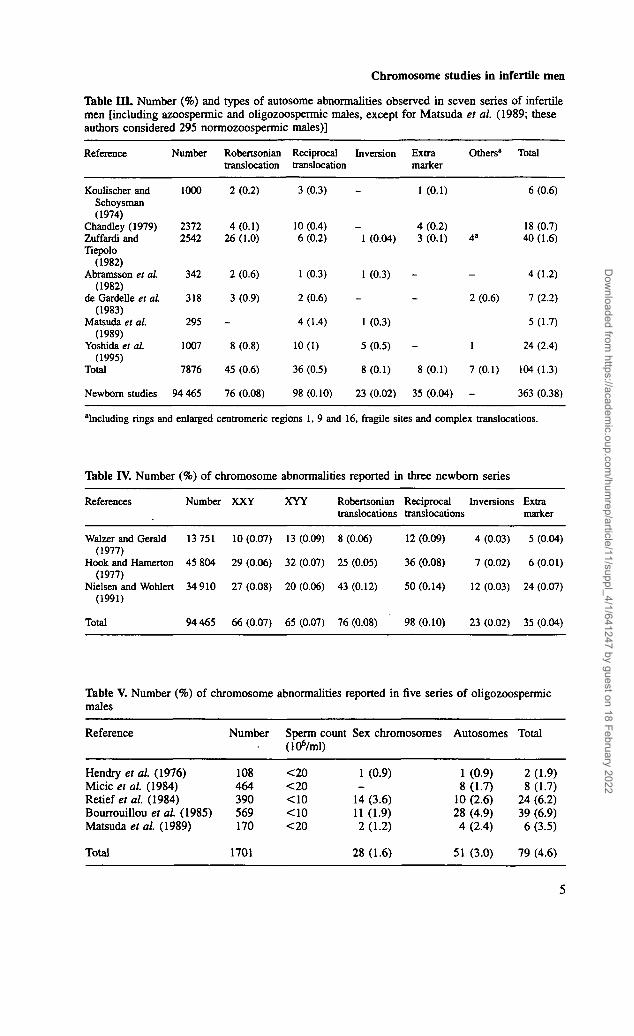
On pooling data from seven surveys of infertile men (Table I), we calculateda total of 7876 males with a 5.1% incidence of chromosome abnormalities: 3.8%involved the sex chromosomes and 1.3% the autosomes. These frequencies weresignificantly higher than those reported in the newborn series considered (TableIV), where the equivalent figures were 0.38% with chromosome anomalies,comprising 0.14% sex chromosome and 0.25% autosome aberrations. (It isobvious that only chromosome abnormalities compatible with a normal phenotypeare mentioned in Table IV. The more severe unbalanced anomalies are notincluded in the data.)
On averaging the overall incidence of chromosome anomalies in the fivesurveys of oligozoospermic men (Table V) and the six studies of azoospermicmen (Table VIII), frequencies of 4.6 and 13.7% were obtained respectively. Itshould be noted that in the oligozoospermic group the sperm count cut-off valuesdo influence the percentages of chromosome anomalies. Moreover, the ratiobetween gonosome and autosome abnormalities differs considerably between thetwo groups. In the azoospermic group, sex chromosome abnormalities predomin-ate (12.6%; Table VEH), whereas in the oligozoospermic group, autosomeanomalies are the most frequent (3.0%; Table V). Because men with Klinefelter's
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

E.Van Assche et aL
Table n . Number (%) and types of sex chromosome abnormalities observed in seven series ofinfertile men [including azoospermic and oligozoospermic males, except for Matsuda et al.(1989; these authors considered 295 normozoospermic males)]
Reference Number XXY* XYY» XXYY XO/XY XX inv Y del Y ring Y Others Total
1 (0.04) -
Koulischer & 1000 21 (2.1) 71"Schoysman(1974)
Chandley 2372 24(1.0) 7(0.3) -(1979)
Zuffardi & 2542 147 (5.8) 2 (0.8) 2 (0.08) 3C (0.1) 3 (0.1) 12 (0.5) 6 (0.2) -Tiepolo(1982)
Abramsson 342 4(1.2) ?> 7* 7* -* - ~ -et al.(1982)
de Gardelleet al.(1983)
Matsudaet al.(1989)
Yoshidaet al.(1995)
Total
1 (0.04)
318 12(3.8) -
295
1007 31 (3.1) 3 (0.3)
7876 239 (3.03)
1(0.3) - 1 (0.3)
27 (2.7)
33 (1.3)
175 (6.9)
6 (1.8)
14 (4.1)
Newborn 94 465 66 (0.07) 65 (0.07)'studies
7 (0.7) 41 (4.1)
296 (3.7)
-' 131 (0.14)
'Includes mosaics.bSix cases grouped as XYY, deletions and rings.cdel(Y) pter -» ql l , one case; idic (Yp), two cases.dTwo cases grouped as mixoploidies; others t(Y,A) and iso(Yp).'Percentage was so low that it was left out of consideration.
syndrome are normally azoospermic, they account for >10% (Table IX) ofthis group; this explains the high percentage of gonosome anomalies detected.Finally, these studies confirm an earlier observation by Kjessler (1966): as meansperm count increases, the numbers of chromosomally abnormal individualsdeclines.
Sex chromosome anomalies and their effect on fertility
Aneuploidy
Among the 10 728 men karyotyped, 47,XXY individuals numbered 373 (i.e.3.48%, with mosaics included). This was 49 times higher than the frequencyreported in the series of newborn children, and was also the most frequentlydetected abnormality. Mosaics of 46,XY/47,XXY were a relatively commonevent and were more likely to be seen in azoospermic and severe oligozoospermicmales. Because some authors made no distinction between the mosaics or full47.XXY karyotypes, the two conditions were grouped.
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022
Chromosome studies in infertile men
Table III. Number (%) and types of autosome abnormalities observed in seven series of infertilemen [including azoospermic and oligozoospermic males, except for Matsuda et al. (1989; theseauthors considered 295 normozoospermic males)]
Reference
Koulischer andSchoysman(1974)
Chandley (1979)Zuffardi andTiepolo
(1982)Abramsson et al
(1982)de Gardelle et al.
(1983)Matsuda et al.
(1989)Yoshida et al.
(1995)Total
Newborn studies
Number
1000
23722542
342
318
295
1007
7876
94 465
Robertsoniantranslocation
2 (0.2)
4(0.1)26(1.0)
2 (0.6)
3 (0.9)
_
8 (0.8)
45 (0.6)
76 (0.08)
Reciprocaltranslocation
3 (0.3)
10 (0.4)6 (0.2)
1 (0.3)
2 (0.6)
4 (1.4)
10(1)
36 (0.5)
98 (0.10)
Inversion
-1 (0.04)
1 (0.3)
_
1 (0.3)
5 (0.5)
8 (0.1)
23 (0.02)
Extramarker
1 (0.1)
4 (0.2)3 (0.1)
-
_
-
8 (0.1)
35 (0.04)
Others"
4"
-
2 (0.6)
1
7 (0.1)
-
Total
6 (0.6)
18 (0.7)40 (1.6)
4(1.2)
7 (2.2)
5 (1.7)
24 (2.4)
104(1.3)
363 (0.38)
"Including rings and enlarged centromenc regions 1, 9 and 16, fragile sites and complex translocations.
Table IV. Number (%) of chromosome abnormalities reported in three newborn series
References Number XXY XYY Robertsonian Reciprocal Inversions Extratranslocations translocations marker
Walzer and Gerald 13 751 10(0.07) 13(0.09) 8(0.06) 12(0.09) 4(0.03) 5(0.04)(1977)
Hook and Hamerton 45 804 29 (0.06) 32 (0.07) 25 (0.05) 36 (0.08) 7 (0.02) 6 (0.01)(1977)
Nielsen and Wohlert 34 910 27(0.08) 20(0.06) 43(0.12) 50(0.14) 12(0.03) 24(0.07)(1991)
Total 94 465 66(0.07) 65(0.07) 76(0.08) 98(0.10) 23(0.02) 35(0.04)
Table V. Number (%) of chromosome abnormalities reported in five series of oligozoospermicmales
Reference Number Sperm count Sex chromosomes Autosomes Total(106/ml)
Hendry et al. (1976) 108 <20 1 (0.9) 1 (0.9) 2 (1.9)Micic et al. (1984) 464 <20Relief et al. (1984) 390Bourrouillou et al. (1985) 569Matsuda et al. (1989) 170 <20
Total 1701 28 (1.6) 51 (3.0) 79 (4.6)
-14112
(3.6)(1.9)(1-2)
8 (1.7)10 (2.6)28 (4.9)4 (2.4)
8 (1.7)24 (6.2)39 (6.9)6 (3.5)
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

E.Van Assche et al
Table VI. Number (%) and types of sex chromosome abnormalities observed in five series ofoligozoospermic males
Reference Number XXY" XYY3 del Y Total
Hendry et al. (1976)Micic et al. (1984)Retief et al. (1984)Bourrouillou et al. (1985)Matsuda et al. (1989)
Total
108464390569170
1 (0.9)-7 (1.8)4 (0.7)
—_3 (0.8)5 (0.9)2 (1.2)
--4(1)2 (0.4)-
1 (0.9)_
14 (3.6)11 (1-9)2 (1.2)
1701 10 (0.7) 10 (0.6) 6 (0.4) 28 (1.6)
"Includes mosaics.
Table VII. Number (%) and types of autosome abnormalities observed in five series ofoligozoospermic males
Reference
Hendry et al.(1976)
Micicet al. (1984)
Retiefet al. (1984)
Bourrouillouet al. (1985)
Matsuda et al.(1989)
Total
Number
108
464
390
569
170
1701
Robertsoniantranslocations
1 (0.9)
6 (1.3)
4 (1.0)
14 (2.5)
2 (1.2)
27 (1.6)
Reciprocaltranslocations
1 (0.2)
3 (0.8)
5 (0.9)
2 (1.2)
11 (0.6)
Inversion
1 (0.2)
1 (0.3)
5 (0.9)
-
7 (0.4)
Extramarker
-
2 (0.5)
4 (0.7)
-
6 (0.4)
Total
1 (0.9)
8 (1.7)
10 (2.6)
28 (4.9)
4 (2.4)
51 (3.0)
Table VHI. Number (%) of chromosome abnormalities reported in six series of azoospermicmales
Reference
Hendry et al. (1976)Micic et al. (1984)Retief et al. (1984)Bourrouillou et al. (1985)Rivas et al. (1987)Matsuda et al. (1989)
Total
Number
5435610638316389
1151
Sex chromosomes
3 (5.6)28 (7.9)19 (1.9)54 (14)36 (22.1)
5 (5.6)
145 (12.6)
Autosomes
2 (3.7)2 (0.6)_5 (1.3)2 (1.2)2 (2.2)
13(1.1)
Total
5 (9.2)30 (8.4)19 (17.9)59 (15.4)38 (23.3)
7 (7.9)
158 (13.7)
The gonadal defect in XXY men seems to be related to germ cell survival andsex chromosome constitution (De Braekeleer and Dao, 1991). Burgoyne (1978)claimed that the testicular atrophy seen in Klinefelter's syndrome patients iscaused by a maturation breakdown of the germ cells containing two X chromo-somes (instead of one). Indeed, Mikamo et al (1968) found the numbers ofspermatogonia in the testes of three 47.XXY boys to be between 1 and 24% of
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

Chromosome studies in infertile men
Table K . Number (%) and types of sex chromosome abnormalities observed in six series ofazoospermic males
Reference
Hendryet al (1976)
Micicet al (1984)
Retiefet al. (1984)
Bourrouillouet al (1985)
Rivas et al(1987)
Matsudaet al. (1989)
Total
Number
54
356
106
383
163
89
1151
XXV
3 (5.6)
26 (7.3)
12(11.3)
49 (12.8)
31 (19)
3 (3.4)
124 (10.8)
XYY1
1 (0.3)
1 (0.9)
-
-
2 (0.2)
XO/XY XX
1 (0.3)
2 (1.9)
1 (0.3) 3 (0.8)
1 (0.6)
1 (0.1) 7 (0.6)
inv Y del Y Ring Y Others Total
3 (5.6)
28 (7.9)
T6 ? b T6 19(17.9)
1 (0.3) - 54 (14.1)
2(1.2) 2(1.2) 36(22.1)
2 (2.2) 5 (5.6)
2 (0.2) 145 (12.6)
"Mosaics are included.bCases grouped as variant Y and del(Yq); others t(Y;A), iso(Yp).
Table X. Number (%) and types of autosome abnormalities observed in six series ofazoospermic males
Reference Number Robertsonian Reciprocal Inversion Totaltranslocations translocations
Hendry et al. (1976) 54 - 2(3.7) - 2(3.7)Micic et al. (1984) 356 - 2 (0.6) - 2 (0.6)Reliefs al. (1984) 106 - -Bourrouillou et al. (1985) 383 1(0.3) 4(1) - 5(1.3)Rivas et al. (1987) 163 - 1 (0.6) 1 (0.6) 2 (1.2)Matsuda et al. (1989) 89 - 1(1.1) 1(1.1) 2(2.2)
Total 1151 1(0.09) 10(0.9) 2(0.2) 13(1.1)
the control values, but little or no sign of spermatogenic activity remainedat puberty.
The spermatogenic picture in 47,XYY men ranges from one of severeimpairment to apparent normality (Skakkebaek et al, 1973). Nevertheless,individuals with a supernumerary Y present in their karyotype are more frequentlyobserved among infertile men (0.26%) than in the series of newborn males(0.07%).
46,XX males
The condition of 46,XX maleness is characterized by testicular developmentdespite the lack of a normal Y chromosome. Their frequency in the generalpopulation is very low (1 in 10 000; de la Chapelle et al, 1990). Because XXmen are azoospermic (de la Chapelle, 1972), they are found most frequently insurveys of azoospermia (Table IX).
Several aetiologies have been proposed and subsequently observed, on thebasis of a genetic heterogeneity, to explain 46,XX maleness (Fechner et al,
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

E.Van Assche et al
1993): (i) translocation of the testis-determining factor (TDF), equated morerecently with the sex-determining region Y gene (SRY), from the Y to the distalshort arm of the X chromosome during male meiosis (Ferguson-Smith, 1966;Anderson et al, 1986; Page et al, 1987; Petit et al, 1987; Rouyer et al, 1987;Van der Auwera et al, 1992); (ii) mutation in an autosomal or X chromosomegene which permits testicular determination in the absence of TDF (Ferguson-Smith et al, 1990). The presence of testicular tissue in these individuals may bethe result of a mutation in a gene that functions in the cascade triggered by SRY.A mutation in such a gene could lead to constitutive activation and permittesticular determination in the absence of SRY; and (iii) undetected 46.XX/47.XXY mosaics or other mosaics with a Y-bearing cell line.
Structural anomalies of the Y chromosome
The frequency of Y chromosome structural rearrangements was found to behigher in infertile men (Tables II, VI and IX) than in newborn infants (Table II).Only pericentric inversions and deletions of the euchromatic part of the longarm were considered in this study. These rearrangements were seen more oftenin azoospermic males.
Spermatogenic failure was reported in a few cases of Y chromosome structuralabnormalities, including a dicentric Y chromosome (Me Ilree et al, 1966), aring Y chromosome (Chandley and Edmond, 1971) and a pericentric inversionof the Y chromosome (Me Ilree et al, 1966).
Meiotic studies performed by these authors revealed that the X and Y shortarms could not pair at meiosis because the short arm pairing region of the Ychromosome was present in the centre of the abnormal chromosome and thereforeunavailable to make an end-to-end association with the X. The suggestion wastherefore made that the pairing failure between the XY bivalent at metaphase Iwas the cause of the breakdown in spermatogenesis.
The association between deletions of the Y chromosome long arm andazoospermia was first suggested by Tiepolo and Zuffardi in 1976. Since thattime, the azoospermia factor gene (AZF) has been mapped in interval 6 of theY chromosome within band Yqll.23 (Anderson et al, 1988; Ma et al, 1992;Voght et al, 1992; Chandley and Cooke, 1994), which at least puts it in thecontrol centre for spermatogenesis. Recently, evidence at a molecular level hasaccumulated with regards to a candidate gene of the Yq region, DAZ (deleted inazoospermia), which is mutated in azoospermic men (Reijo et al, 1995). Anexplanation of azoospermia at the molecular level is therefore in sight.
Reciprocal translocations involving a sex chromosome
Reciprocal translocations between a sex chromosome and an autosome havebeen reported sporadically in surveys of infertile men (Chandley, 1979; Retiefet al, 1984; Rivera and Diaz-Costafios, 1992). Madan (1983) concluded, afterstudying nine male carriers of X autosome (X;A) translocations, that, regardlessof the position of the breakpoint in the X, these men are likely to suffer from adisturbance in spermatogenesis leading to severe subfertility or infertility.
8
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

Chromosome studies in infertile men
To explain the usual sterility of human (and mouse) reciprocal (X;A) maleheterozygotes, Lifschytz and Lindsley (1972) advanced the hypothesis that thejuxtapositioning of early replicating, transcriptionally active autosomal materialmight be the cause of germ cell failure. They held that a transcriptionally inactiveX chromosome might be a requirement for normal spermatogenesis, because anyreactivation of the X chromosome under the spreading influence of an activeautosome might perhaps upset the biochemical balance within the cell. Thehypothesis still remains to be proved, but some evidence for X reactivation atmeiotic prophase has been found in certain male-sterile stocks of mice, including(X;A) heterozygotes (Hotta and Chandley, 1982; Speed, 1986).
Y autosome (Y;A) translocations (for an overview see Rivera and Diaz-Costanos, 1992) cause similar testicular changes (compare with Laurent et al,1982) whenever the breakpoint is located in Yqll (where the azoospermia factoris mapped) or near its boundaries.
In patients with a Yp breakpoint, the outcome would depend on whether thebreakage occurred within the pseudoautosomal segment: a faulty XY pairingand subsequent meiotic breakdown will then occur. Such an aetiopathogenicheterogeneity correlates with the different histological patterns documented sofar: arrest at or after diakinesis in translocations involving Yq (Gonzales et al,1981; Laurent et al, 1982) and Sertoli cell-only syndrome appearance intranslocations involving Yp (Anderson et al, 1988).
One can accept the hypothesis anyway that any balanced Y;A translocationwith a breakpoint within the Yq critical segment or near the pseudoautosomalsegment (Yp) may severely damage germ cell maturation, resulting in azoospermiaor severe oligozoospermia (Rivera and Diaz-Costanos, 1992).
Autosome anomalies and their effect on fertility
Robertsonian translocations
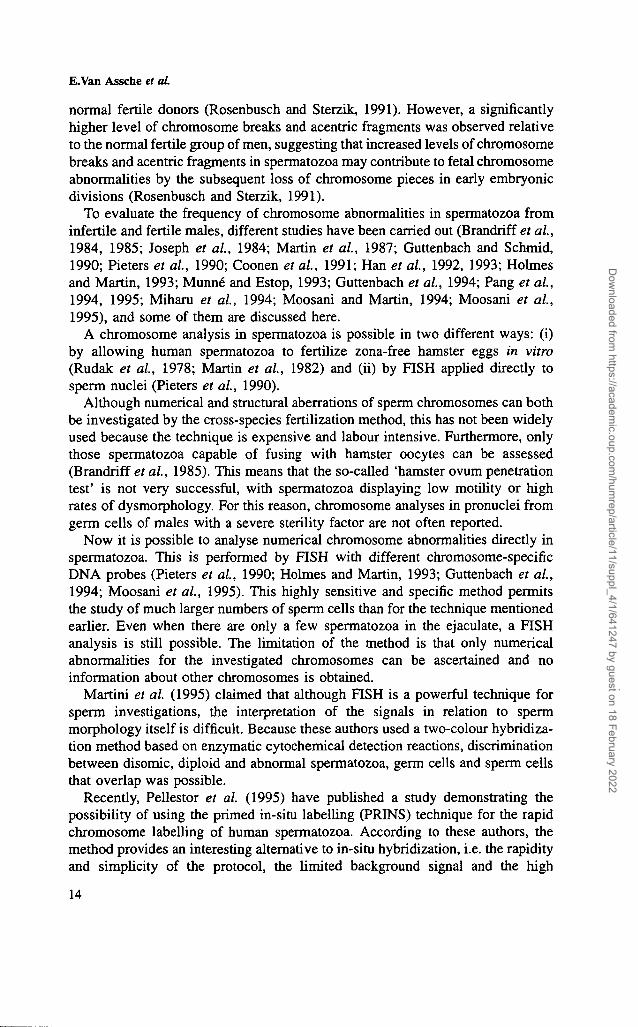
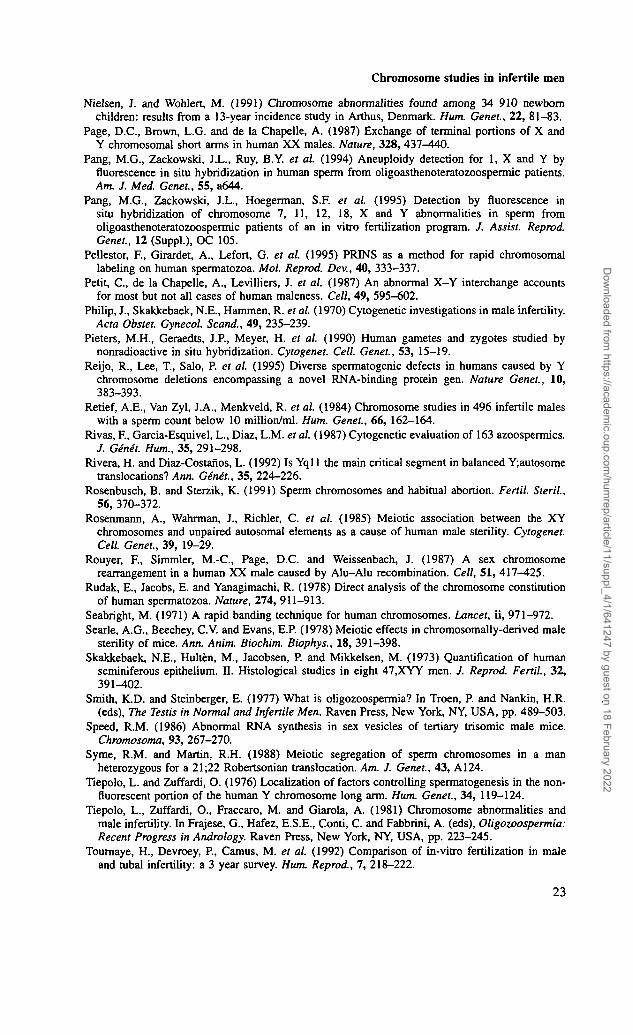
Robertsonian translocations (Figure 1) were seen in 0.7% (73/10 728) of all themales karyotyped. This is 8.5 times higher than the frequency reported in thenewborn studies used. In azoospermic males, this type of rearrangement wasrarely observed (0.09%; Table X); on the other hand, it was much more frequentin the oligozoospermic group (1.6%; Table VII).
The chromosomes involved in these Robertsonian translocations were knownin 58 of the 73 cases. In 71.4% a 13; 14 translocation was involved, which iscomparable with the figure for the newborn series.
Although Robertsonian translocations are more likely to be found in chromo-some investigations of infertile men, their role in oligozoospermia is not clear.The testicular histology of the men carrying such a rearrangement shows a variablepicture, ranging from severe impairment to near normality (Chandley, 1975).
From family studies on male carriers of Robertsonian translocations, it hasbeen shown that the infertile subjects often have male relatives carrying the same
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

E.Van Assche et al
:: i l '>•-5 ia n n n
:s 88
Figure 1. GTG-banded karyotype from a male with a Robertsonian translocation between chromosomes 13and 14. The arrow indicates the translocation chromosome 13-14.
translocation but who are themselves fertile, indicating that the translocationitself is not the only and consistent cause of infertility. Genetic background couldalso be important (Chandley, 1986). Tiepolo et al. (1981) have tested thehypothesis that infertility in balanced carriers of human Robertsonian transloca-tions could result from a loss of ribosomal cistrons. However, [3H]rRNA/DNAhybridization experiments failed to demonstrate any significant difference in thenumber of rDNA genes (Guanti et al, 1980).
Meiotic studies of sterile carriers of a 13ql4q Robertsonian translocation(Luciani et al., 1984; Johannisson et al., 1993) and of sterile carriers of 14q21qtranslocations (Rosenmann et al., 1985) have revealed that the spermatogenicimpairment is related to — and is indeed a reflection of — an increase in thefrequency of the XY bivalent and the Robertsonian trivalent association duringthe pachytene stage. According to Johannisson et al. (1993), it can be concludedthat a correlation exists between the increased frequency of the XY bivalent andthe Robertsonian trivalent association and the extent of germ cell impairment.
Reciprocal translocations
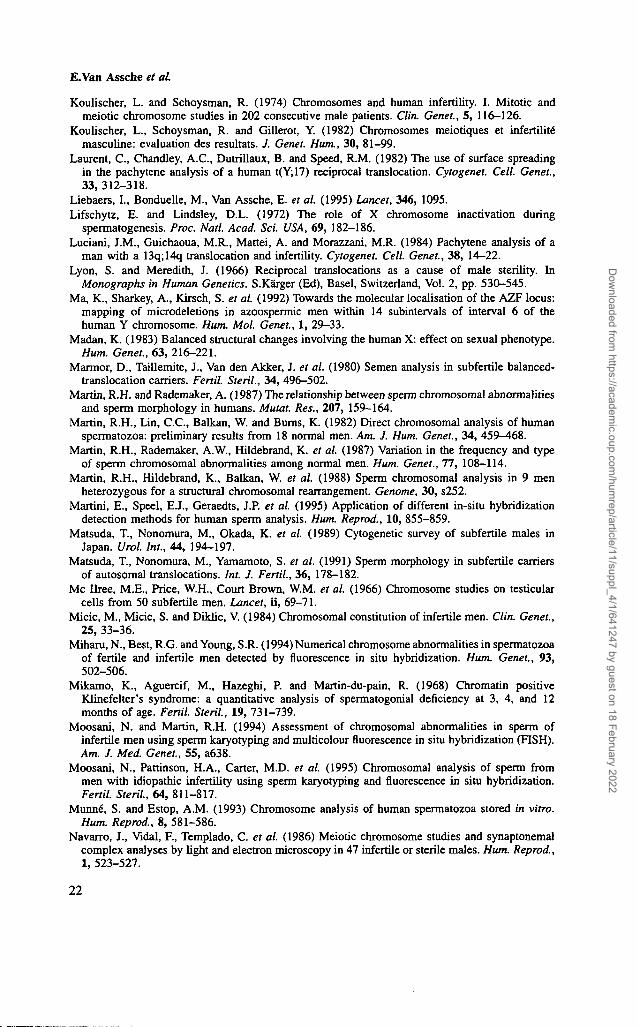
On pooling the data from the different series of infertile males (Tables IQ, VIIand X), 0.5% reciprocal translocations (Figure 2) were observed as opposed to0.1% in the newborn children. This means that the probability of finding such achromosome rearrangement is five times higher in series of infertile men than inthe newborn series. In addition, an increased frequency of reciprocal translocationswas observed among azoospermic (0.9%) and severe oligozoospermic (0.8% inRetief et al, 1984; 0.9% in Bourrouillou et al, 1985) men.
The correlation between some reciprocal translocations and the impairment ofsperm production is a well known event (Chandley et al, 1986; Martin et al,1988; Syme and Martin, 1988). Lyon and Meredith (1966) were the first to show
10
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

Chromosome studies in infertile men
K n >i it KI Ci !) is sc n *.;
Figure 2. GTG-banded karyotype from a male with a pericentric inversion of the heterochromatic region ofchromosome 9 and a reciprocal translocation between chromosomes 15 and 16 with breakpoints ql2 andq24.
that certain purely autosomal translocations of the mouse cause sterility in maleheterozygotes because of spermatogenic impairment. The occurrence of suchtranslocations in man has also been noted (Chandley, 1981, 1984). Meioticstudies could elucidate the mechanism by which purely autosomal rearrangementsmight bring about spermatogenic disturbance (Forejt, 1974; Chandley, 1982). Itwas observed that a high frequency of centromeric contacts between thetranslocation configuration and the XY bivalent was formed at the pachytenestage of meioses I, especially with chain configurations rather than rings. Suchcontacts were not seen to any great extent among the pachytene cells of fertilemale translocation carriers. Forejt (1974) suggested that non-random associationsmight produce interference with the precocious X chromosome inactivation inthe primary spermatocyte which would be required, according to the hypothesisof Lifschytz and Lindsley (1972), for normal spermatogenesis.
Inversions
The probability of finding inversions (Figure 3) (paracentric and pericentric butexcluding the pericentric inversion of the heterochromatic region of chromosome9) is eight times higher in the series of infertile men (0.16%) than in the newbornseries (0.02%). Chromosomes 1-3, 5-7 and 9 were involved [only in the studyof Yoshida et al. (1995) was the chromosome involved in inversions not specified].In particular, pericentric inversions of chromosome 1 appear to carry a specialrisk of male infertility regardless of the breakpoint position. Chandley et al.(1987) performed meiotic studies on carriers of chromosome 1 inversions andthe same phenomenon was observed as for translocation carriers, i.e. an extensivedisturbance of synapses across the inverted region at metaphase I resulting in aminority of complete loop formations. The disturbance in spermatogenesis has
11
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

E.Van Assche et aL
u
itl\ >i is »1 IS l« :s
** H hi it•> 14
Figure 3. GTG-banded karyotype from a male with a pericentric inversion of chromosome 5 withbreakpoints pi 3 and ql3.
been suggested to arise principally from the synapses observed not only withinthe inversion bivalent itself but also in other members of the complement, theseperhaps arising as a secondary consequence of the primary anomaly. Thus, thesterilizing effects of chromosome 1 inversion in the human male could beaccommodated on models that link germ cell maturation impairment to failureof synapses (Burgoyne and Baker, 1984).
Extra marker chromosomes and rings
A supernumerary marker chromosome or a ring was observed in 21 out of the10 728 fertile men, which is almost five times higher than the frequency calculatedfrom the newborn studies. Several authors have reported an association betweenthe presence of a ring chromosome and spermatogenic impairment (Kjessler,1966; Me Hree et aL, 1966; Chandley, 1979), in particular with almost completearrest at the spermatocyte stage.
Meiotic studies of chromosome anomalies in male infertility
Abnormal segregation of chromosomes during male meiosis can be responsiblefor the birth of a child with an abnormal karyotype (trisomies, balanced orunbalanced translocations, etc.) or for spontaneous abortions and stillbirths. Theseabnormalities are also responsible for male infertility. Only this latter aspect willbe discussed here.
Because testicular biopsies are not routinely performed in infertile men andthe investigation of meiotic chromosomes presents a special technical challenge,this has remained a research tool restricted to just a few laboratories. Ford andHamerton carried out the first human meiotic studies in 1956 using the so-called
12
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

Chromosome studies in infertile men
'squash method' (preparations made from small pieces of testicular tissue). Nowthis method has been superseded by the air-drying technique (Evans et al, 1964;Chandley, 1977) and the surface-spreading technique (Counce and Meyer, 1973;Dresser and Moses, 1979; Fletcher, 1979). Chromosomes from premeioticspermatogonial cells, first and second spermatocytes, spermatids and spermatozoacan be observed after staining [C- and Q-banding or fluorescence in-situhybridization (FISH) with centromere-specific probes] the preparations obtainedby the air-drying method. On the other hand, the surface-spreading techniquepermits an analysis of the synaptonemal complexes of the first prophase by lightmicroscopy or electron microscopy.
There are still several problems in interpretation of the results and in comparisonof the several published studies. A major problem is the kind of technique usedto study meiotic chromosomes. All such techniques have advantages anddisadvantages, and it is still not clear that the results obtained by a particulartechnique are comparable with those obtained using another technique.
Blockage or arrest at any stage of spermatogenesis is observed in a numberof infertile men with and without chromosome abnormalities (Hendry et al,1976; Chandley, 1979; Koulischer et al, 1982; Egozcue et al, 1983; Navarroet al, 1986). These meiotic abnormalities include low chiasma count (<50/cellaccording to Chandley, 1988) the presence of univalents (sign of desynapsis),bivalent fragmentation, asymmetrical bivalents and polyploidy. A full descriptionof the several types of meiotic chromosome abnormality found in infertile menis reported by Koulischer et al. (1982).
If we compare the surveys of Hendry et al (1976; air-drying technique),Koulischer et al. (1982; air-drying technique), Egozcue et al. (1983; air-dryingtechnique) and Navarro et al. (1986; air-drying and surface-spreading techniques)with meiotic studies of 200, 450, 1100 and 47 infertile males respectively, apercentage range of 4.3-40.4% with meiotic chromosome abnormalities wasfound. This variation can be explained by the method of presentation of theresults of the different authors (some include polymorphisms, minor abnormalitiesand constitutional anomalies) and patient selection itself (variation in theinterpretation of subfertility, infertility and oligozoospermia).
Nevertheless, it is clear from the different studies that in a number of patientsmeiotic chromosome anomalies can explain their infertility.
Chromosome studies in spermatozoa of infertile men
It has been established that there is an increase in the frequency of constitutionalchromosome abnormalities in the infertile male population relative to that seenin the general population. Apart from constitutional chromosome abnormalities,there is a possibility that the fertility problem itself is related to chromosomeinstability. This instability may predispose the sperm chromosomes to non-disjunction and/or structural abnormalities. In males with a 46,XY karyotypewho had experienced recurrent reproductive losses, a sperm karyotype analysisdid not reveal a significant difference in the aneuploidy rate from that seen in
13
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022
E.Van Assche et aL
normal fertile donors (Rosenbusch and Sterzik, 1991). However, a significantlyhigher level of chromosome breaks and acentric fragments was observed relativeto the normal fertile group of men, suggesting that increased levels of chromosomebreaks and acentric fragments in spermatozoa may contribute to fetal chromosomeabnormalities by the subsequent loss of chromosome pieces in early embryonicdivisions (Rosenbusch and Sterzik, 1991).
To evaluate the frequency of chromosome abnormalities in spermatozoa frominfertile and fertile males, different studies have been carried out (Brandriff et aL,1984, 1985; Joseph et aL, 1984; Martin et aL, 1987; Guttenbach and Schmid,1990; Pieters et aL, 1990; Coonen et aL, 1991; Han et aL, 1992, 1993; Holmesand Martin, 1993; Munne and Estop, 1993; Guttenbach et aL, 1994; Pang et aL,1994, 1995; Miharu et aL, 1994; Moosani and Martin, 1994; Moosani et aL,1995), and some of them are discussed here.
A chromosome analysis in spermatozoa is possible in two different ways: (i)by allowing human spermatozoa to fertilize zona-free hamster eggs in vitro(Rudak et ah, 1978; Martin et aL, 1982) and (ii) by FISH applied directly tosperm nuclei (Pieters et aL, 1990).
Although numerical and structural aberrations of sperm chromosomes can bothbe investigated by the cross-species fertilization method, this has not been widelyused because the technique is expensive and labour intensive. Furthermore, onlythose spermatozoa capable of fusing with hamster oocytes can be assessed(Brandriff et aL, 1985). This means that the so-called 'hamster ovum penetrationtest' is not very successful, with spermatozoa displaying low motility or highrates of dysmorphology. For this reason, chromosome analyses in pronuclei fromgerm cells of males with a severe sterility factor are not often reported.
Now it is possible to analyse numerical chromosome abnormalities directly inspermatozoa. This is performed by FISH with different chromosome-specificDNA probes (Pieters et aL, 1990; Holmes and Martin, 1993; Guttenbach et aL,1994; Moosani et aL, 1995). This highly sensitive and specific method permitsthe study of much larger numbers of sperm cells than for the technique mentionedearlier. Even when there are only a few spermatozoa in the ejaculate, a FISHanalysis is still possible. The limitation of the method is that only numericalabnormalities for the investigated chromosomes can be ascertained and noinformation about other chromosomes is obtained.
Martini et aL (1995) claimed that although FISH is a powerful technique forsperm investigations, the interpretation of the signals in relation to spermmorphology itself is difficult. Because these authors used a two-colour hybridiza-tion method based on enzymatic cytochemical detection reactions, discriminationbetween disomic, diploid and abnormal spermatozoa, germ cells and sperm cellsthat overlap was possible.
Recently, Pellestor et al. (1995) have published a study demonstrating thepossibility of using the primed in-situ labelling (PRINS) technique for the rapidchromosome labelling of human spermatozoa. According to these authors, themethod provides an interesting alternative to in-situ hybridization, i.e. the rapidityand simplicity of the protocol, the limited background signal and the high
14
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

Chromosome studies in infertile men
specificity of the oligonucleotide primers. The current limitation of PRINS isthat only one chromosome can be identified; a double PRINS protocol to performsimultaneous labelling of two chromosomes on human spermatozoa has still tobe developed.
Cytogenetic studies in spermatozoa
Fertile males
From three large studies from independent laboratories (Brandriff et al, 1985;Kamiguchi and Mikamo, 1986; Martin et al, 1987), using the hamster ovumpenetration test, it can be estimated that the mean frequency of chromosomeabnormalities in spermatozoa from normal males is -10%. A correlation betweenincreasing age (>40 years) and an increased risk of spermatozoa with structuralchromosome abnormalities was found by Martin and Rademaker (1987) andMartin et al. (1987). A recent study by Estop et al. (1995) using the samemethod found no statistical evidence for this event, although they agreed that atrend towards higher numbers of structural rearrangements with increasing agedoes exist.
Aneuploidy rates determined by investigators using the in-situ hybridizationtechnique accord well with each other (Joseph et al., 1984; Pieters et al, 1990;Coonen et al, 1991; Guttenbach et al, 1994). The rates determined by analysingsperm chromosome complements are, however, ~ 10-fold lower (Martin andRademaker, 1990). These lower frequencies may have been a result of technicallimitations.
Infertile males
The first FISH studies in idiopathic infertile males have been published recentlyin the USA and Canada.
Pang et al. (1995) compared their FISH results of chromosomes 7, 11, 12, 18,X and Y in four proven fertile donors with those obtained in nine males witholigoasthenoteratozoospermia. A > 10-fold increase in frequency was observedin the oligoasthenoteratozoospermic men (19.61 versus 1.45%). The results showa highly significant increase in the frequencies of diploidy, autosomal disomy,autosomal nullisomy, sex chromosome number (not further specified) and thetotal number of abnormalities for oligoasthenoteratozoospermic males versusnormal fertile donors.
Moosani et al. (1995) investigated five infertile males (two oligozoospermics,two teratozoospermics and one asthenozoospermic) and 12 normal fertile males.As well as the FISH technique, using probes for the centromeric regions ofchromosomes 1, 12, X and Y, they also applied the hamster ovum penetrationtest. The FISH results showed two interesting trends: (i) a significant increase inthe frequency of disomy for chromosome 1 was found in three of the five men;and (ii) the frequency of XY disomy was significantly higher in four of the five
15
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

E.Van Assche et aL
patients, suggesting malsegregation of the sex chromosomes. Oligozoospermicmen in particular show an increase in the frequency of aneuploidy, as revealedin the sperm karyotypes and by FISH.
It is interesting to note that all sterile males in both studies had a normalconstitutional karyotype. The results of both surveys also show similar trends,and they suggest that not only XY pairing but also pairing of the autosomes isimpaired in infertile males, resulting in spermatogenic disruption.
In another study of infertile males by Miharu et al. (1994), with fertile malesas a control group, no significant differences for chromosome diploidies ordisomies were observed for chromosomes 1, 16, X and Y. Unfortunately it isnot known whether these patients had a normal or low sperm count or anabnormal constitutional karyotype.
It is obvious that more investigations on many more patients are needed tocharacterize the occurrence of all possible autosomal disomies in spermatozoafrom infertile men.
Chromosome investigation of 694 infertile men with abnormal sperm values
Materials and methodsTo investigate a possible correlation between one, two or three abnormal spermparameters and the somatic chromosome constitution, we performed a cytogeneticinvestigation of lymphocyte cultures to study 694 men who had been found tohave abnormal sperm values in two or three consecutive semen samples. Thesemen samples were analysed according to the WHO (1987) criteria andwere considered to be abnormal if the sperm counts were <20 XlO6/ml(oligozoospermia), progressive sperm motility was <50% (asthenozoospermia)or normal sperm morphology was <14% (teratozoospermia).
We compared the cytogenetic results for these patients with those of 395normal fertile males. The latter had normal sperm values, no fertility problemsand attended our fertility clinic because their wives suffered from tubal infertility(control group from the study by Toumaye et al, 1992).
For each proband at least 15 metaphases were analysed by GTL banding (G-banding obtained after trypsine treatment and Leishman's stain) (Seabright,1971). When a chromosome abnormality was noted, high resolution banding(Yunis et al, 1978) was performed on a new blood sample and a further 10metaphases were analysed.
Our own results
Results and discussion
The general results are given in Table XI.In general the frequency of chromosome abnormalities observed in the infertile
men differed statistically from the control group (2.02 versus 0.25%; Table XI).This means that the probability of finding a chromosome abnormality in infertilemales was eight times higher than in the control group.
16
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

0ATOAOTATOATTotal
Control population
293346339147
415694
395
Chromosome studies in infertile men
Table XI. Number (%) of chromosome abnormalities observed in infertile men with oligo- (O)and/or astheno- (A) and/or teratozoospermia (T)
Abnormal sperm values Number Sex chromosomes Autosomes Total
171 - 2(2.2) 2(2.2)b
2 (0.5) 10 (2.4) 12 (2.9)b
2 (0.3) 12 (1.7) 14 (2.02)"
1 (0.25) 1 (0.25)a
aP < 0.014 (Fisher's exact test) compared with the frequency in men with normal sperm values.bP < 0.007 (Fisher's exact test) if the number of chromosome abnormalities was compared withthose subgroups composed of males with respectively zero (control population), two (OA + OT+ AT) or three (OAT) aberrant sperm values.
Unfortunately, the number of cytogenetically investigated individuals in thedifferent subgroups was too low for us to draw any conclusions. However, astatistically significant difference was found between the frequency of chromo-some abnormalities in all three subgroups with two abnormal sperm parametersand that in the control population.
To compare the frequency of chromosome abnormalities observed in our seriesof infertile men with those published previously (Table V), only males sufferingfrom at least oligozoospermia may be considered. In our survey, 568 men wereat least oligozoospermic and 2.5% were found to have a chromosome aberration,i.e. 0.4% had sex chromosome abnormalities and 2.1% autosome abnormalities.This is in line with the studies of Hendry et al (1976), Micic et al. (1984) andMatsuda et al. (1989), where sperm counts <20xl06 /ml were considered toindicate oligozoospermia (Table V).
Details about the chromosome abnormalities themselves are given in Table XII.Four reciprocal translocation carriers, three inversion carriers and two Robert-
sonian translocation carriers were observed. Genetic counselling and a riskevaluation for all these patients were offered. Attempts were made to obtainblood samples to karyotype other family members, but in most cases the patientsdid not concur. Except for the reciprocal translocation 2;7, which was inheritedfrom a normally fertile mother, no further information was obtained for theother cases.
It is possible that a correlation exists between the frequency of chromosomeabnormalities and the type of aberrant sperm value. In this respect, three studieshave already been published (Chandley et al, 1975; Marmor et al, 1980;Matsuda et al, 1991). In the study by Chandley et al. (1975), a relative frequencydistribution of sperm count, sperm motility and sperm morphology for fertile,chromosomally normal subfertile and chromosomally abnormal groups wasdetermined. Significantly poorer sperm counts, sperm motility and sperm morpho-
17
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

E.Van Assche et at
Table XII. Chromosome abnormalities in the oligoteratozoospermia (OT) andoligoasthenoteratozoospermia (OAT) subgroups
Abnormalities OT OAT
Sex chromosomes46.X, i(Y)(qter -» cen -» qter) 146.XX, t(3;6)(q25;pll.2)/46,XY, t(3;6)(q25;pll.2) 1
AutosomesRobertsonian translocations
45.XY, t(13ql4q) 145,XY, t(14q21q) 2
Reciprocal translocations46.XY, t(l;ll)(P22;q23) 146.XY, t(2;7)(q23;p22) 146.XY, t(15;16)(ql2;q24) 146.XY, t(2O;22)(ql2;qll.21) 1
Inversions46.XY, inv(l)(p34.3q32) 146.XY, inv(5)(pl3ql3) 146.XY, inv(10)(pll.2q22) 1
Others46,XY, inv(3)(pl3q25), t(8;ll)(q24.1;pl5.2) 147,XY, +mar(15) 1
Total 2 12
logy were found in carriers of chromosome aberrations. However, we considerthis approach to be biased because, for example, the same individuals witholigoasthenoteratozoospermia and chromosome abnormalities will occur in thethree surveys (sperm count, sperm motility and sperm morphology) and con-sequently influence the distribution.
The groups of Marmor et al. (1980) and Matsuda et al. (1991) found nosignificant difference in the proportions of abnormally shaped spermatozoabetween the subfertile translocation carriers and the subfertile controls withnormal karyotype. As Matsuda et al. (1991) matched each subfertile translocationcarrier with a subfertile male with the same sperm count, they suggested thattheir results were much more reliable than those of Chandley et al. (1975).
As mentioned above, more research is needed to be able to confirm or disprovea possible relationship between the type of chromosome aberration and itsinfluence on the number and/or morphology and/or motility of spermatozoa ininfertile men.
Conclusion
It is estimated that 20% of male infertility can be explained by abnormalities inmitotic and/or meiotic chromosomes. To learn more about male infertility on theone hand, and to be able to provide proper counselling for couples faced with
18
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

Chromosome studies in infertile men
infertility caused by a male sterility factor (i.e. oligozoospermia, oligoasthenotera-tozoospermia or non-obstructive azoospermia) on the other, clinical investigationsshould ideally include: (i) a peripheral blood karyotype; (ii) a testicular biopsyfor the study of spermatogenesis as well as chromosome and meiotic studies;(iii) an analysis of the chromosome content of individual spermatozoa; and (iv)a DNA analysis of blood and spermatozoa to detect partially deleted Ychromosome material.
These investigations have become more important because male infertility cannow be treated by intracytoplasmic sperm injection (ICSI; Van Steirteghem et al,1995). Indeed, couples elected for artificial reproduction treatment should becounselled on the cause of their infertility and the possible 'genetic' risks whenICSI is performed. If the male partner is a carrier of a constitutional chromosomeaberration then the couple should be told that: (i) in cases of an autosomalstructural aberration the success rate of ICSI is lowered, an increased risk formiscarriage exists and, in ongoing pregnancies in the presence of a chromosomeaberration, multiple congenital abnormalities and/or mental retardation are pos-sible; (ii) in cases of a sex chromosome aneuploidy (e.g. 47,XXY or 47.XYY)the success rate of the treatment is variable, but if successful the risk ofaneuploidy in the offspring is probably low or unknown; (iii) in cases of structuralaberrations of a sex chromosome there is a greater risk of transmitting infertility,depending on the position of the breakpoint.
If the male partner has a normal constitutional karyotype a slightly increasedrisk of sex chromosome aberration seems to exist, based on Liebaers et al.(1995), as explained by Moosani et al. (1995) and Pang et al. (1995). The risksof transmitting infertility because of molecular defects on the long arm of the Ychromosome are beyond the scope of this article.
We can conclude that an increase in future research activities, especially inandrology and reproductive genetics, is needed to analyse in more detail thecausal agents of genetically determined sterility factors at the molecular leveland perhaps to correlate numerical and structural aberrations with gene defects.
Acknowledgements
The authors thank the technical staff of the Centre for Medical Genetics and the Centre forReproductive Medicine. We thank Mr Frank Winter of the Language Centre for correcting theEnglish text.
References
Abramsson, L., Beckman, G., Duchek, M. and Nordenson, I. (1982) Chromosomal aberrations andmale infertility. /. UroL, 128, 52-53.
Anderson, M., Page, D.C. and de la Chapelle, A. (1986) Chromosome Y-specific DNA is transferredto the short arm of the X chromosome in human XX males. Science, 233, 786-788.
Anderson, M., Page, D.C, Pettay, D. et al. (1988) Y;autosome translations and mosaicism in
19
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

E.Van Assche et al
the aetiology of 45,X maleness: assignment of fertility factor to distal Yqll. Hum. Genet., 79,2-7.
Bourrouillou, G., Dastugue, N. and Colombies, P. (1985) Chromosome studies in 952 infertilemales with a sperm count below 10 million/ml. Hum. Genet., 71, 366-367.
Brandriff, B., Gordon, L., Ashworth, L. et al. (1984) Chromosomal abnormalities in human sperm:comparisons among four healthy men. Hum. Genet., 66, 193-201.
Brandriff, B., Gordon, L., Ashworth, L. et al. (1985) Chromosomes of human sperm: variabilityamong normal individuals. Hum. Genet., 70,18-24.
Burgoyne, P.S. (1978) The role of sex chromosomes in mammalian germ cell differentation. Ann.Biol. Anim. Biochim. Biophys., 18, 317-325.
Burgoyne, P.S. and Baker, T. (1984) Meiotic pairing and gametogenetic failure. In Evans, C.W.and Dickinson, H.G. (eds), Controlling Events in Meiosis. Co. of Biologists., Cambridge,UK, p. 349.
Chandley, A.C. (1975) Human meiotic studies. In Emery, A.E.H. (ed.), Modem Trends in HumanGenetics. Butterworths, London, UK, pp. 31-82.
Chandley, A.C. (1977) Karyotyping of infertile men. In Hafez, E.S.E. (ed.), Techniques of HumanAndrology. Biomedical Press, Elsevier, Amsterdam, The Netherlands.
Chandley, A.C. (1979) The chromosomal basis of human infertility. Br. Med.-Bull., 35, 181-186.Chandley, A.C. (1981) The origin of chromosomal aberrations in man and their potential for
survival and reproduction in the adult human population. Ann. Ginit., 24, 5-11.Chandley, A.C. (1982) A pachytene analysis of two male-fertile paracentric inversions in
chromosome 1 of the mouse and in male-sterile double heterozygote. Chromosoma, 85,127-135.Chandley, A.C. (1984) Infertility and chromosome abnormality. In Clarke, J. (ed.), Oxford Reviews
of Reproductive Biology. Oxford University Press, Oxford, UK, Vol. 6, pp. 1-46.Chandley, A.C. (1986) The genetics of human reproduction. Experientia, 42, 1109-1117.Chandley, A.C. (1988) Meiosis in men. Trends Genet., 4, 79-84.Chandley, A.C. and Cooke, H.J. (1994) Human male fertility — Y-linked genes and spermatogenesis.
Hum. Mol. Genet., 3, 1449-1452.Chandley, A.C. and Edmond, P. (1971) Meiotic studies on a subfertile patient with a ring Y
chromosome. Cytogenetics, 10, 295-304.Chandley, A.C, Edmond, P., Christie, S. et al. (1975) Cytogenetics and infertility in man. I.
Karyotype and seminal analysis. Ann. Hum. Genet., 39, 231-254.Chandley, A.C, Speed, R.M., McBeath, S. and Hargreave, T.B. (1986) A human 9;20 reciprocal
translocation associated with male infertility analyzed at prophase and metaphase I of meiosis.Cytogenet. Cell. Genet., 41, 145-153.
Chandley, A.C, McBeath, S., Speed, R.M. et al. (1987) Pericentric inversion in human chromosome1 and the risk for male sterility. J. Med. Genet., 24, 325-334.
Coonen, E., Pieters, M.H., Dumoulin, J.C. et al. (1991) Nonisotopic in situ hybridization as amethod for nondisjunction studies in human spermatozoa. Mol. Reprod. Dev., 28, 18-22.
Counce, S.J. and Meyer, G.F. (1973) Differentiation of the synaptonemal complex and thekinetochore in Locusta spermatocytes studied by whole mount electron microscopy. Chromosoma,44, 231-253.
Court-Brown, W.M., Jacobs, P. and Brunton, M. (1965) Chromosome studies on randomly chosenmen and women. Lancet, ii, 561-562.
De Braekeleer, M. and Dao, T.N. (1991) Cytogenetic studies in male infertility: a review. Hum.Reprod., 6, 245-250.
de la Chapelle, A. (1972) Nature and origin of males with XX sex chromosomes. Am. J. Hum.Genet., 24, 71-105.
de la Chapelle, A., Hastbacka, J., Korhonen, T. and Maenpa, A. (1990) The etiology of XX sexreversal. Reprod. Nutr. Dev., (Suppl. 1), 39s-49s.
de Gardelle, G.R., Jaffray, J.Y., Geneix, A. and Malet, P. (1983) Les anomalies du caryotype dansles sterilitds hypofertilite's masculines. Pathologica, 75, 687^691.
Dresser, M.E. and Moses, M.J. (1979) Silver staining of synaptonemal complexes in surfacespreads for light and electron microscopy. Exp. Cell Res., 121, 416-419.
Dutrillaux, B., Le Lorier, G., Salat, J. and Rotman, J. (1971) Incidence des anomalieschromosomiques dans la sterilite masculine. Presse Med., 79, 1231-1234.
20
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

Chromosome studies in infertile men
Egozcue, J., Templado, C , Vidal, F. et al. (1983) Meiotic studies in a series of 1100 infertile andsterile males. Hum. Genet., 65, 185-188.
Estop, A.M., Marquez, C , Munne, S. et al. (1995) An analysis of human sperm chromosomebreakpoints. Am. J. Hum. Genet., 56, 452-460.
Evans, E.P., Breckon, G. and Ford, C.F. (1964) An air-drying method for meiotic preparationsfrom mammalian testis. Cytogenetics, 3, 289-291.
Fechner, P.Y., Marcantonio, S.M., Jaswaney, V. et al. (1993) The role of the sex-determining regionY gene in the etiology of 46.XX maleness. J. Clin. Endocrinol. Metab., 76, 690-695.
Ferguson-Smith, M.A. (1966) X-Y chromosomal interchange in the aetiology of truehermaphroditism and of XX Klinefelter's syndrome. Lancet, ii, 475-476.
Ferguson-Smith, M.A., Lennox, B., Mack, W.S. and Stewart, J.S.S. (1957) Klinefelter's syndrome.Frequency and testicular morphology in relation to nuclear sex. Lancet, ii, 167-169.
Ferguson-Smith, M., Cooke, A., Affara, N. et al. (1990) Genotype-phenotype correlations in XXmales and the bearing on current theories of sex determination. Hum. Genet., 84, 198-202.
Fletcher, J.M. (1979) Light microscope analysis of meiotic prophase chromosomes by silverstaining. Chromosoma, 72, 241-248.
Ford, C.E. and Hamerton, J.L. (1956) The chromosomes of man. Nature, 178, 1020.Forejt, J. (1974) Nonrandom association between a specific autosome and the X chromosome in
meiosis of the male mouse: possible consequences of homologous centromere separation.Cytogenet. Cell. Genet., 13, 369-383.
Gonzales, J., Lesourd, S. and Dutrillaux, B. (1981) Mitotic and meiotic analysis of a reciprocaltranslocation t(Y;3) in an azoospermic male. Hum. Genet., 57, 111-114.
Greenhall, E. and Vessey, M. (1990) The prevalence of subfertility: a review of the currentconfusion and a report of two new studies. Fertil. Steril, 54, 978-983.
Guanti, G., Zuffardi, O. and Tiepolo, L. (1980) rDNA levels in infertile male carriers ofRobertsonian translocations. Cytogenet. Cell. Genet., 27, 162-167.
Guttenbach, M. and Schmid, M. (1990) Determination of Y chromosome aneuploidy in humansperm nuclei by nonradioactive in situ hybridization. Am. J. Hum. Genet., 46, 553-558.
Guttenbach, M., Schakowski, R. and Schmid, M. (1994) Incidence of chromosome 3, 7, 10, 11,17 and X disomy in mature human sperm nuclei as determined by nonradioactive in situhybridization. Hum. Genet., 93, 7-12.
Han, T.L., Webb, G.C., Flaherty, S.P. et al. (1992) Detection of chromosome 17- and X-bearinghuman spermatozoa using fluorescence in situ hybridization. Mol. Reprod. Dev., 33, 180-194.
Han, T.L., Ford, J.H., Webb, G.C. et al. (1993) Simultaneous detection of X- and Y-bearing humansperm by double fluorescence in situ hybridization. Mol. Reprod. Dev., 34, 308-313.
Hendry, W.F., Polani, P.E., Pugh, A.C.B. et al. (1976) 200 infertile males: correlation of chromosome,histological, endocrine and clinical studies. Br. J. Urol, 47, 899-908.
Holmes, J.M. and Martin, R.H. (1993) Aneuploidy detection in human sperm nuclei usingfluorescence in situ hybridization. Hum. Genet., 91, 20-34.
Hook, E.B. and Hamerton, J.L. (1977) The frequency of chromosome abnormalities detected inconsecutive newborn studies — differences between studies — results by sex and by severityof phenotypic involvement. In Hook, E.B. and Porter. H. (eds), Population Cytogenetics: Studiesin Humans. Academic Press, New York, NY, USA, pp. 80-92.
Hotta, Y. and Chandley, A.C. (1982) Activities of X-linked enzymes in spermatocytes of micerendered sterile by chromosomal alterations. Gamete Res., 6, 65-72.
Jacobs, P.A. and Strong, J.A. (1959) A case of human intersexuality having a possible XXY sex-determining mechanism. Nature, 183, 302-303.
Johannisson, R., Schwinger, E., Wolff, H.H. et al. (1993) The effect of 13;14 Robertsoniantranslocations on germ-cell differentiation in infertile males. Cytogenet. Cell. Genet., 63,151-155.
Joseph, A.M., Gosden, J.R. and Chandley, A.C. (1984) Estimation of aneuploidy levels in humanspermatozoa using chromosome specific probes and in situ hybridisation. Hum. Genet., 66,234-238.
Kamiguchi, Y. and Mikamo, K. (1986) An improved efficient method for analyzing human spermchromosomes using zona-free hamster ova. Am. J. Hum. Genet., 38, 724-740.
Kjessler, B. (1966) Karyotype, meiosis and spermatogenesis in a sample of men attending aninfertility clinic. In Monographs in Human Genetics. S.KSrger (Ed), Basel, Switzerland, Vol. 2.
21
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022
E.Van Assche et al
Koulischer, L. and Schoysman, R. (1974) Chromosomes and human infertility. I. Mitotic andmeiotic chromosome studies in 202 consecutive male patients. Clin. Genet., 5, 116-126.
Koulischer, L., Schoysman, R. and Gillerot, Y. (1982) Chromosomes meiotiques et infertilitymasculine: evaluation des resultats. J. Genet. Hum., 30, 81-99.
Laurent, C , Chandley, A.C., Dutrillaux, B. and Speed, R.M. (1982) The use of surface spreadingin the pachytene analysis of a human t(Y;17) reciprocal translocation. Cytogenet. Cell. Genet.,33, 312-318.
Liebaers, I., Bonduelle, M., Van Assche, E. et al. (1995) Lancet, 346, 1095.Lifschytz, E. and Lindsley, D.L. (1972) The role of X chromosome inactivation during
spermatogenesis. Proc. Natl. Acad. Sci. USA, 69, 182-186.Luciani, J.M., Guichaoua, M.R., Mattei, A. and Morazzani, M.R. (1984) Pachytene analysis of a
man with a 13q;14q translocation and infertility. Cytogenet. Cell. Genet., 38, 14-22.Lyon, S. and Meredith, J. (1966) Reciprocal translocations as a cause of male sterility. In
Monographs in Human Genetics. S.Karger (Ed), Basel, Switzerland, Vol. 2, pp. 530-545.Ma, K., Sharkey, A., Kirsch, S. et al. (1992) Towards the molecular localisation of the AZF locus:
mapping of microdeletions in azoospermic men within 14 subintervals of interval 6 of thehuman Y chromosome. Hum. Mol. Genet., 1, 29-33.
Madan, K. (1983) Balanced structural changes involving the human X: effect on sexual phenotype.Hum. Genet., 63, 216-221.
Marmor, D., Taillemite, J., Van den Akker, J. et al. (1980) Semen analysis in subfertile balanced-translocation carriers. Fertil. Steril., 34, 496-502.
Martin, R.H. and Rademaker, A. (1987) The relationship between sperm chromosomal abnormalitiesand sperm morphology in humans. Mutat. Res., 207, 159-164.
Martin, R.H., Lin, C.C., Balkan, W. and Burns, K. (1982) Direct chromosomal analysis of humanspermatozoa: preliminary results from 18 normal men. Am. J. Hum. Genet., 34, 459-468.
Martin, R.H., Rademaker, A.W., Hildebrand, K. et al. (1987) Variation in the frequency and typeof sperm chromosomal abnormalities among normal men. Hum. Genet., 77, 108-114.
Martin, R.H., Hildebrand, K., Balkan, W. et al. (1988) Sperm chromosomal analysis in 9 menheterozygous for a structural chromosomal rearrangement. Genome, 30, s252.
Martini, E., Speel, E.J., Geraedts, J.P. et al. (1995) Application of different in-situ hybridizationdetection methods for human sperm analysis. Hum. Reprod., 10, 855-859.
Matsuda, T., Nonomura, M., Okada, K. et al. (1989) Cytogenetic survey of subfertile males inJapan. Urol. Int., 44, 194-197.
Matsuda, T., Nonomura, M., Yamamoto, S. et al. (1991) Sperm morphology in subfertile carriersof autosomal translocations. Int. J. Fertil., 36, 178-182.
Me Dree, M.E., Price, W.H., Court Brown, W.M. et al. (1966) Chromosome studies on testicularcells from 50 subfertile men. Lancet, ii, 69-71.
Micic, M., Micic, S. and Diklic, V. (1984) Chromosomal constitution of infertile men. Clin. Genet.,25, 33-36.
Miharu, N., Best, R.G. and Young, S.R. (1994) Numerical chromosome abnormalities in spermatozoaof fertile and infertile men detected by fluorescence in situ hybridization. Hum. Genet., 93,502-506.
Mikamo, K., Aguercif, M., Hazeghi, P. and Martin-du-pain, R. (1968) Chromatin positiveKlinefelter's syndrome: a quantitative analysis of spermatogonial deficiency at 3, 4, and 12months of age. Fertil. Steril., 19, 731-739.
Moosani, N. and Martin, R.H. (1994) Assessment of chromosomal abnormalities in sperm ofinfertile men using sperm karyotyping and multicolour fluorescence in situ hybridization (FISH).Am. J. Med, Genet., 55, a638.
Moosani, N., Pattinson, H.A., Carter, M.D. et al. (1995) Chromosomal analysis of sperm frommen with idiopathic infertility using sperm karyotyping and fluorescence in situ hybridization.Fertil. Steril., 64, 811-817.
Munnd, S. and Estop, A.M. (1993) Chromosome analysis of human spermatozoa stored in vitro.Hum. Reprod., 8, 581-586.
Navarro, J., Vidal, R, Templado, C. et al. (1986) Meiotic chromosome studies and synaptonemalcomplex analyses by light and electron microscopy in 47 infertile or sterile males. Hum. Reprod.,1, 523-527.
22
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022
Chromosome studies in infertile men
Nielsen, J. and Wohlert, M. (1991) Chromosome abnormalities found among 34 910 newbornchildren: results from a 13-year incidence study in Arthus, Denmark. Hum. Genet., 22, 81-83.
Page, D.C., Brown, L.G. and de la Chapelle, A. (1987) Exchange of terminal portions of X andY chromosomal short arms in human XX males. Nature, 328, 437-440.
Pang, M.G., Zackowski, J.L., Ruy, B.Y. et al. (1994) Aneuploidy detection for 1, X and Y byfluorescence in situ hybridization in human sperm from oligoasthenoteratozoospermic patients.Am. J. Med. Genet., 55, a644.
Pang, M.G., Zackowski, J.L., Hoegerman, S.F. et al. (1995) Detection by fluorescence insitu hybridization of chromosome 7, 11, 12, 18, X and Y abnormalities in sperm fromoligoasthenoteratozoospermic patients of an in vitro fertilization program. J. Assist. Reprod.Genet., 12 (Suppl.), OC 105.
Pellestor, R, Girardet, A., Lefort, G. et al. (1995) PRINS as a method for rapid chromosomallabeling on human spermatozoa. Mol. Reprod. Dev., 40, 333-337.
Petit, C , de la Chapelle, A., Levilliers, J. et al. (1987) An abnormal X-Y interchange accountsfor most but not all cases of human maleness. Cell, 49, 595-602.
Philip, J., Skakkebaek, N.E., Hammen, R. et al. (1970) Cytogenetic investigations in male infertility.Acta Obstet. Gynecol. Scand., 49, 235-239.
Pieters, M.H., Geraedts, J.P., Meyer, H. et al. (1990) Human gametes and zygotes studied bynonradioactive in situ hybridization. Cytogenet. Cell. Genet., 53, 15-19.
Reijo, R., Lee, T., Salo, P. et al. (1995) Diverse spermatogenic defects in humans caused by Ychromosome deletions encompassing a novel RNA-binding protein gen. Nature Genet., 10,383-393.
Retief, A.E., Van Zyl, J.A., Menkveld, R. et al. (1984) Chromosome studies in 496 infertile maleswith a sperm count below 10 million/ml. Hum. Genet., 66, 162-164.
Rivas, F., Garcia-Esquivel, L., Diaz, L.M. et al. (1987) Cytogenetic evaluation of 163 azoospermics.J. Genet. Hum., 35, 291-298.
Rivera, H. and Diaz-Costafios, L. (1992) Is Yqll the main critical segment in balanced Y;autosometranslocations? Ann. Ginet., 35, 224-226.
Rosenbusch, B. and Sterzik, K. (1991) Sperm chromosomes and habitual abortion. Fertil. Steril,56, 370-372.
Rosenmann, A., Wahrman, J., Richler, C. et al. (1985) Meiotic association between the XYchromosomes and unpaired autosomal elements as a cause of human male sterility. Cytogenet.Cell. Genet., 39, 19-29.
Rouyer, F., Simmler, M.-C, Page, D.C. and Weissenbach, J. (1987) A sex chromosomerearrangement in a human XX male caused by Alu-Alu recombination. Cell, 51, 417-425.
Rudak, E., Jacobs, E. and Yanagimachi, R. (1978) Direct analysis of the chromosome constitutionof human spermatozoa. Nature, 274, 911-913.
Seabright, M. (1971) A rapid banding technique for human chromosomes. Lancet, ii, 971-972.Searle, A.G., Beechey, C.V. and Evans, E.P. (1978) Meiotic effects in chromosomally-derived male
sterility of mice. Ann. Anim. Biochim. Biophys., 18, 391-398.Skakkebaek, N.E., Hulten, M., Jacobsen, P. and Mikkelsen, M. (1973) Quantification of human
seminiferous epithelium. II. Histological studies in eight 47.XYY men. J. Reprod. Fertil, 32,391-402.
Smith, K.D. and Steinberger, E. (1977) What is oligozoospermia? In Troen, P. and Nankin, H.R.(eds), The Testis in Normal and Infertile Men. Raven Press, New York, NY, USA, pp. 489-503.
Speed, R.M. (1986) Abnormal RNA synthesis in sex vesicles of tertiary trisomic male mice.Chromosoma, 93, 267-270.
Syme, R.M. and Martin, R.H. (1988) Meiotic segregation of sperm chromosomes in a manheterozygous for a 21;22 Robertsonian translocation. Am. J. Genet., 43, A124.
Tiepolo, L. and Zuffardi, O. (1976) Localization of factors controlling spermatogenesis in the non-fluorescent portion of the human Y chromosome long arm. Hum. Genet., 34, 119-124.
Tiepolo, L., Zuffardi, O., Fraccaro, M. and Giarola, A. (1981) Chromosome abnormalities andmale infertility. In Frajese, G., Hafez, E.S.E., Conti, C. and Fabbrini, A. (eds), Oligozoospermia:Recent Progress in Andrology. Raven Press, New York, NY, USA, pp. 223-245.
Toumaye, H., Devroey, P., Camus, M. et al. (1992) Comparison of in-vitro fertilization in maleand tubal infertility: a 3 year survey. Hum. Reprod., 7, 218-222.
23
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

E.Van Asscbe et aL
Van der Auwera, B., Van Roy, N., De Paepe, A. et al. (1992) Molecular cytogenetic analysis ofXX males using Y-specific DNA sequences, including SRY. Hum. Genet., 89, 23-28.
Van Steirteghem, A., Tournaye, H., Van der Elst, J. et al. (1995) Intracytoplasmic sperm injection3 years after the birth of the first ICSI child. Hum. Reprod., 10, 2527-2528.
Voght, P., Chandley, A.C., Hargreave, T.B. et al. (1992) Microdeletions in interval 6 of the Ychromosome of males with idiopathic sterility point to disruption of AZF, a human spermatogenesisgene. Hum. Genet., 89, 491-496.
Walzer, S. and Gerald, P. (1977) A chromosome survey of 13 751 male newboms. In Hook, E.B.and Porter, H. (eds), Population Cytogenetics: Studies in Humans. Academic Press, New York,NY, USA, pp. 45-61.
World Health Organization (1987) WHO Laboratory Manual for the Examination of Human Semenand Semen-Cervical Mucus Interaction. 2nd edn, Cambridge University Press, Cambridge, UK.
Yoshida, A., Tamayama, T., Nagao, K., Takanami, M. et al. (1995) A cytogenetic survey of 1007infertile males. Contracept Fertil. Sex., 23, 103a.
Yunis, J.J., Sawyer, J.R. and Ball, D.W. (1978) Characterization of banding patterns of metaphase-prophase G-banded chromosomes and their use in gene mapping. Cytogenet. Cell. Genet., 22,679-683.
Zuffardi, O. and Tiepolo, L. (1982) Frequencies and types of chromosome abnormalities associatedwith human male infertility. In P.G. Crosignani and B.L. Rubsin (eds), Genetic Control ofGamete Production and Function. Serono Clinical Colloquia on Reproduction III. AcademicPress and Guine and Stratton, London, UK, pp. 261-273.
24
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

Discussion
Edwards: Could I start the discussion by asking you about the low chiasmafrequency in the meiotic stages of some men? Do you have any evidence if thisis familial or is it a local factor, for example due to a varicocele or some of thefactors which may reduce oxygen tension. I ask this question because oxygentension is important in chiasma frequency formation.Van Assche: I have read about this phenomenon; it is just an hypothesis.Edwards: It would be helpful to gain more data. In the female, chiasma frequencyis very important in the causation of trisomies and monosomies. Presumably, itmust also be important in the male, e.g. in relation to sex chromosome monosomiesand trisomies.Simpson: You mention that there was non-random distribution with respect toinversions, especially chromosome 1. Did you find any evidence of non-randomreciprocal translocations when you looked at that chromosome? The answer isno, I suppose.Van Assche: This is correct.Simpson: The second question is that when I have attempted much moremodest surveys of the frequency of autosomal aneuploidy and sex chromosomalaneuploidy in infertile men, I found that there are many surveys that have a very,very low frequency of XXY mosaics, e.g. one or two XXY cells in comparisonwith 40 to 50 normal cells. I have never been able to determine whether thiswas a genuine finding or arose through some bias e.g. because that is what thelab technician thought that he or she wanted to find. I wonder if you could giveus a sense of the frequency of very low-grade mosaics in relation to the numbersthat you gave when you calculated the increased risk?Van Assche: We considered the possibility of mosaicism when at least threemetaphases were observed with the same chromosomal loss, or at least twometaphases with the same chromosomal addition, when at least 50 metaphaseswere examined.Diedrich: I am sure you are aware of the letter to Lancet by In't Veld (1995)about the sex chromosomal abnormalities after ICSI: five out of 15 prenatalabnormal karyotypes were reported. Do you have an explanation from yourstudies why this percentage is so high?Van Steirteghem: Our group replied to this letter (Liebaers et al. 1995). This isone of the aspects we shall discuss later this afternoon, when we talk about thepregnancies and the children. We are very fortunate because In't Veld, the seniorauthor of this letter to the Lancet is also in this room.Silber: I enjoyed your paper. I understand that out of 694 infertile men therewere chromosomal abnormalities in a total of 14 of these men. May we concludethat these 14 men would be the group in which the increased risk of sexchromosomal abnormalities or chromosomal abnormalities in the newboms wouldbe seen? Are you suggesting that we study all these men before ICSI?Van Assche: These 14 men do have a constitutional abnormality in their karyotype.It also needs to be investigated that more aneuploidies are present in the
25
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022

Discussion
spermatozoa of these men. Further studies are also required on spermatozoa ofinfertile men who have a normal karyotype.Silber: Concerning the FISH studies, you mentioned three studies. One of them(Miharu, 1995) did not report any difference between 12 infertile men, that werepoorly defined, and nine fertile men. Could you describe in detail how you viewthat discrepancy between their study and the two other studies (Pang et al. 1995and Moosani et al. 1995).Van Assche: In the latter two publications differences were reported which maybe related to the selection of their patients. Miharu did not give any details aboutthe infertility problem of the patients whose spermatozoa were studied. In orderto detect significant differences, one has to examine a large number of spermato-zoa: this may explain why only a small number of patients were studied.Doyle: I am uncertain about the control group. You said they were a fertilecontrol group, but in fact they were men without proven fertility. You are lookingat the semen values of men, but you do not know that the sperm eventually willturn out to be functional.Van Assche: In our study, there was in fact a control group obtained from a studycarried out here at the hospital. It is certain that the couples suffered fromlongstanding infertility. The husbands had normal sperm values.Van Steirteghem: I agree with Doyle that there is always the possibility that anunknown male factor may be present.Doyle: So the point is that you do not know how many of the so-called 'normal'men have these abnormalities in their sperm.Tournaye: Perhaps it is important to know that those men had wives followingan IVF programme and that they had a normal fertilization rate in IVF. It is notcorrect to define them as fertile men. We do know that in an FVF programmethey were performing normally.
References
Liebaers, I., Bonduelle, M., Van Assche, E. ex al. (1995) Lancet, 346, 1095.Moosani, N., Pattinson, H.A., Carter, N.D. el al. (1995) Chromosomal analysis of sperm from
men with idiopathic infertility using sperm karyotyping and fluorescence in situ hybridization.Fertil. Steril., 64, 811-817.
Pang, M.G., Zackowski, J.L., Hoegerman, S.F. et al. (1995) Detection by fluorescence insitu hybridization of chromosome 7, 11, 12, 18, X and Y abnormalities in sperm fromoligoasthenoteratozoospermic patients of an in vitro fertilization program. J. Assist. Reprod.Genet., 12 (Suppl.), OC 105.
26
Dow
nloaded from https://academ
ic.oup.com/hum
rep/article/11/suppl_4/1/641247 by guest on 18 February 2022