CYSTS OF THE JAWS Part II
128
Cysts of JAWS Prepared by Dr. Abhishek PT PG RESIDENT Dept OMFS
-
Upload
abhishek-pt -
Category
Healthcare
-
view
545 -
download
0
Transcript of CYSTS OF THE JAWS Part II
Cysts of JAWS
Prepared byDr. Abhishek PTPG RESIDENT
Dept OMFS

DENTIGEROUS CYST
• The dentigerous cyst is defined as a cyst that originatesby the separation of the follicle from around the
crownof an unerupted tooth
• Encloses crown of unerupted tooth and attached to tooth at cementoenamel junction.
Paget 1863

Click icon to add picture
Dentigerous cystGross specimen of a dentigerous cyst. Cyst encloses the crown of the tooth and is attached to its neck

CLINICAL FEATURES
• AGE : 1st to 3rd decades.•
• GENDER : more frequently in males than in females.• SITE :
• 2/3rd associated with unerupted mandibular teeth, primarily III molar.
• Maxillary canine• Mandibular premolar• Maxillary 3rd Molar• Supernumerary tooth also can be involved
Signs & symptoms
• Most cysts grow to a large size before being discovered accidentally while observing a dental x ray to detect the cause of an unerupted tooth.
• Large lesions can cause cortical expansion, leading to facial asymmetry, teeth displacement, root resorption, even pain, if infected.

RADIOLOGICAL FEATURES
• Manifests as unilocular, • well defined, ‘lucency with sclerotic margins, associated
with crown of impacted / unerupted tooth.
• A large DC may show persistence of boney trabeculae, giving the appearance of multilocularity.

RADIOLOGICAL FEATURES
• CENTRAL TYPE/CORONAL:
• • LATERAL TYPE :
•
• CIRCUMFERENTIAL • TYPE :

Click icon to add picture
Radiographic features
A central type of dentigerous cyst. Note resorption of the root of the first mandibular molar

Click icon to add picture
Radiographic features
Radiograph of two dentigerous cysts in the same patient. The cyst on the right is a lateral type; that on the left is a circumferential type

Radiographic featuresCT scan of a maxillary dentigerous cyst extending to, and impinging on, the floor of the nose.
HISTOLOGICAL FEATURES
A. NON INFLAMMED TYPE:
• Lining derived from reduced dental epithelium, consists of 2-4 cell layers of non keratinized epithelium, without rete ridges.
• Wall composed of thin fibrous connective tissue appearing immature, as it is derived from the dental papilla.
HISTOLOGICAL FEATURES
B. INFLAMED TYPE :
• Lining shows varying degrees of hyperplasia with rete ridges and occasionally even keratinization.
• Wall is composed of mature connective tissue which shows infiltration by chronic inflammatory cells.

Copyright © 1999 The British Association of Oral and Maxillofacial Surgeons. Published by Elsevier Ltd. All rights reserved.
‘ASSYMPTOMATIC DOESN’T
MEAN DISEASE FREE !!!’
- No tooth had a follicular space greater than 2.4 mm

DIFFERENTIAL DIAGNOSIS
Although it presents a unique feature, yet some lesions must be considered in its differential diagnosis :
1. Unicystic ameloblastoma2. Adenomatoid odontogenic tumor.
COMPLICATIONS
1. Recurrence due to incomplete surgical removal.
2. Development of ameloblastoma either from lining epithelium or from odontogenic islands in the connective tissue wall.
3. Development of squamous cell carcinoma from same two sources.
4. Development of mucoepidermoid carcinoma from mucus secreting cells in the lining.

These figures show that ameloblastoma is very much more common in Blacks than Whites in the population at risk. Conversely, dentigerous cysts are much more common in Whites.
0.5% DCs were associated with other cysts or tumours at the same site or the opposite side of the jaw. DCs can co-exist with other more serious conditions, such as cystic ameloblastoma. This association with more significant conditions indicates the importance of histologically confirming any jaw cyst, even when it presents clinically as a classic DC.

Treatment
J AMERICAN DENT ASSO
J Dent Soc. 2012 Spring;61(1):18-21.A conservative approach in the management of inflammatory dentigerous cyst in transitional dentition: a case report.Marwah N1, Bishen KA, Prabha V, Goenka P.Author information
Dentigerous cysts are benign odontogenic cysts that develop from the reduced enamel epithelium related to the crown of an unerupted and/or impacted tooth. Inflammatory dentigerous cyst is a variety of dentigerous cyst that is mostly found in the mixed dentition, and the treatment modalities range from enucleation to marsupialization. By extracting the infected primary teeth, opening the cyst, and ensuring continuous drainage, spontaneous eruption of the involved permanent teeth occurs into the dental arch even if they are severely dislocated. The purpose of this report is to describe the successful treatment of a large dentigerous cyst by conservative surgical management.

ODONTOGENIC KERATOCYST
• 1956 – philipson termed odonyogenic kertocyst
• There is general agreement that the odontogenic keratocyst arises from cell rests of the dental lamina.
• Believed to be benign potentially aggressive&reccurrent odontogenic cyst
• Several investigators suggest that odontogenic keratocysts be regarded as benign cystic neoplasms rather than cysts

2013 clinics review articles february

HISTOLOGIC FEATURES
• The epithelial lining is composed of a uniform layer of stratified squamous epithelium
• The basal cell layer has columnar / cuboidal cells with reversely polarized nuclei, imparting a “picket fence” or “tombstone” appearance.
Orthokeratinised
•Have lower incidence of reccurance
parakeratinised
•Premitive nature of epithelium shows premalignant potential•Cystic lesion behiving more like a tumor
Clinical behaviour• High reccuranece rate• Histologic appearance• Presence of tumor markrs within the
cystSpecifically proliferating nuclear antigen ki67 Matrix
metaloprotineaseP53

GENETICS

2005 Classification
Untill further reclasssification orthokeratinised will be Grouped in benign odontogenic cyst

CLINICAL FEATURES
• AGE : occur over a wide age range and cases have been• recorded as early as the first decade and as late as
the nineth.• In most series there has been a pronounced peak
frequency in the second and third decades.• GENDER : more frequently in males than in females.• SITE : The mandible is involved far more frequently than
the maxilla• 50% cases occur in angle region and extend to
ascending ramus and forwards to body of mandible.
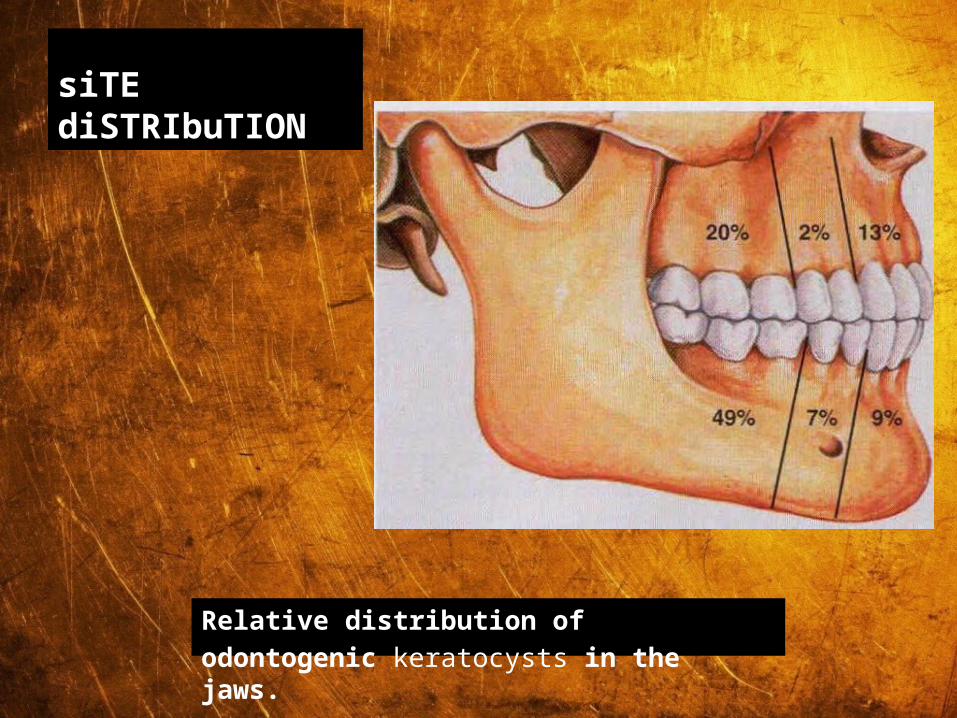
siTE diSTRIbuTION
Relative distribution ofodontogenic keratocysts in the jaws.
CLINICAL FEATURES
• Pain, swelling or discharge.• May or may not with missing teeth• Occasionally, paraesthesia of the lower lip or teeth. • In many instances, patients are remarkably free of symptoms
until the cysts have reached a large size, involving the maxillary sinus and the entire ascending ramus, including the condylar and coronoid processes.
• occurs because the OKC tends to extend in the medullary cavity and clinically observable expansion of the bone occurs late.

RADIOGRAPHIC FEATURES
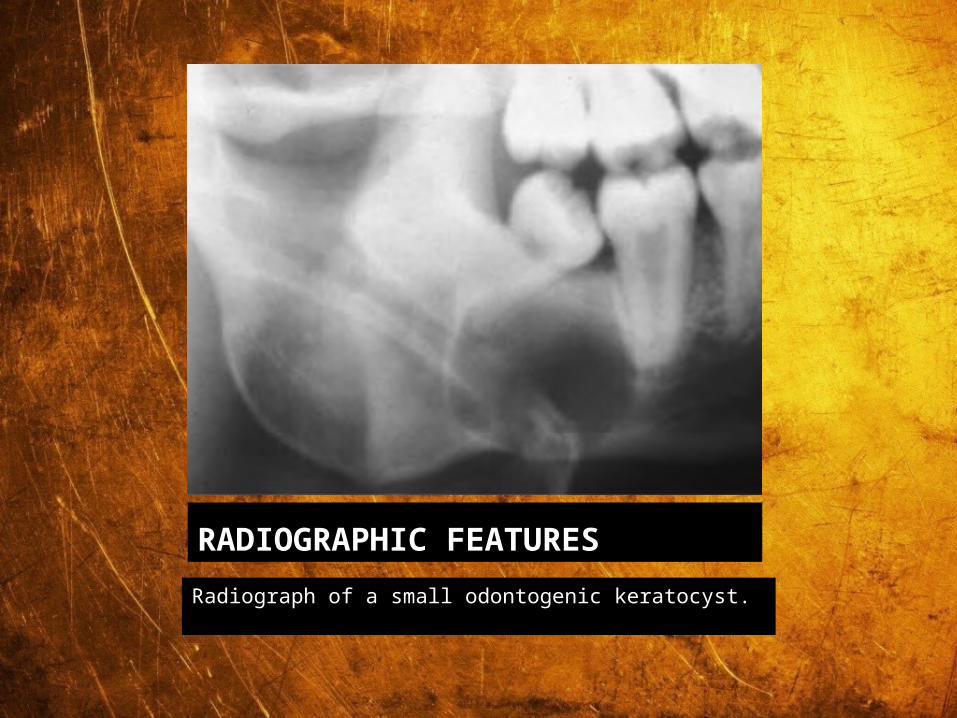
• OKC demonstrate a well-defined radiolucent area with smooth and often corticated margins.
• Large lesions, particularly in the posterior body and ascending ramus of the mandible, may appear multilocular
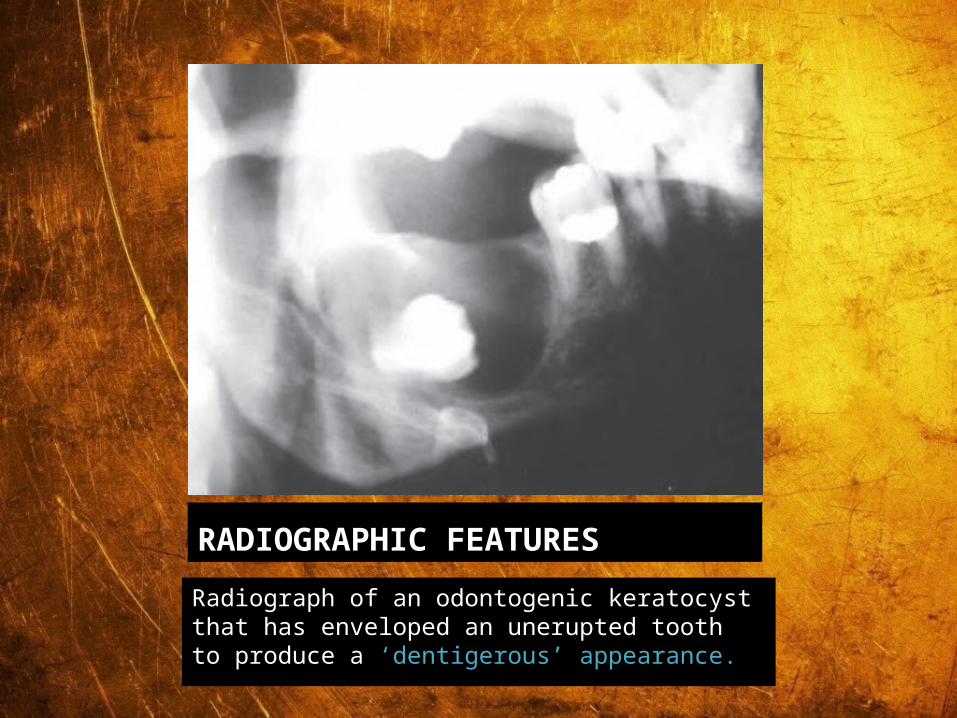
• An unerupted tooth is involved in the lesion in 25% to 40% of cases; in such instances, the radiographic features suggest the diagnosis of dentigerous cyst
RADIOGRAPHIC FEATURES
Radiograph of a small odontogenic keratocyst.

Click icon to add picture
RADIOGRAPHIC FEATURES
Radiograph of a multilocular odontogenic keratocyst.
RADIOGRAPHIC FEATURES
Radiograph of an odontogenic keratocyst that has enveloped an unerupted tooth to produce a ‘dentigerous’ appearance.

DIFFERENTIAL DIAGNOSIS
• In case of unilocular ‘lucencies – Dentigerous cyst, Eruption cyst, COC, AOT, Unicystic ameloblastoma etc.
• In case of multilocular ‘lucencies – Conventional ameloblastoma, CEOT, Central giant cell granuloma, Aneurysmal bone cyst etc.

3 FOLD REASONS OF RECURRANCE
1) FRIABLE THIN LINING Chances of portions to be left behind
2)Daughter cysts occur beyond visible margins of the lesion
3)Some of these lesions origins from oral mucosa and some will be associated with Gorlin gots syndrome
Daughter cyst originate between oral mucosa and cyst

• GORLIN-GOLTZ syndrome, characterized by
• Multiple nevoid basal cell epitheliomas• Odontogenic Keratocyst of the jaws• Bifid ribs– sixth rib• Plantar & palmar pits• Occular hypertelorism• Frontal bossing• Ectopic calcifications

TREATMENTThe recurrence rates were 0% for resection, 0% for enucleation with peripheral ostectomy and Carnoy's solution, 18.18% for enucleation with peripheral ostectomy, 26.09% for enucleation alone, 40% for marsupialisation, and 50% for enucleation with Carnoy's solution. The overall recurrence rate was 23.15% A systematic review of the recurrence rate for keratocystic odontogenic tumour in relation to treatment modalities. Available from: https://www.researchgate.net/publication/221974195_A_systematic_review_of_the_recurrence_rate_for_keratocystic_odontogenic_tumour_in_relation_to_treatment_modalities [accessed Jan 14, 2016].

Authors current technique
1. Obtain a tissue biopsy of the cyst .At the same time, a drainage tube is placed.
2. If the diagnosis comes back a KCOT drainage tube is left in place and saline irrigation done.
The size of the cyst is monitered3.When radiolucency decreased to
about 2 cm or less and not in contact with adjacent teeth and other vital structure

Cavity treated with LIQUID NITROGEN CRYOTHERAPY BY MEANS OF A CRYOSPRAY.
At the same time enucleation of the lesion also occurred.
Overlying mucosa is excisedAfter cryotherapy excellent soft tissue closure is
required to void wound breakdown

An approach that recently has gained popularity in the management of keratocysts is a combination of methods.
-The first step is to decompress the cyst. A plastic (or other suitable material) drain is secured in place to ensure that the opening remains patent. After 6 to 8 weeks, the lining of the cyst becomes generally thick and tough.
-The second step is to carefully enucleate the cyst. At this time, the thickened cyst wall is much more easily removed than is the usual OKC.
-The next step is to perform a peripheral ostectomy with a large bone bur. A margin of 2 to 3 mm is taken, depending on adjacent vital structures involved.

-The final step is to treat the residual bone bed with chemical cautery (Carnoy’s solution). This systematically thorough method, although time consuming and demanding much patient co-operation, has achieved good results.-

-To obliterate the cavity after cyst enucleation, various filling materials have been recommended for packing into the defect prior to closure of the wound.
-Primarily, these are forms of haemostatic resorbable sponge, some of which may be soaked in a solution containing an antibiotic or thrombin. These materials are inserted to prevent excessive bleeding and to form a scaffold into which granulation tissue can migrate

ERUPTION CYST

ERUPTION CYST
–• Typical c/f of an eruption
cyst. Note a bluish colored, dome shaped swelling over the unerupted tooth–
• The dentigerous cyst develops around the crown of an unerupted tooth lying in the bone,
• The eruption cyst occurs when a tooth is impeded in its eruption within the soft tissues overlying the bone.
Eruption cysts involving the maxillary permanentincisors.
PATHOGENESIS
It imparts purple / deep blue color
Hence known as
• ERUPTION HEMATOMA

CLINICAL FEATURES
AGE : found in children of different ages, and occasionallyin adults if there is delayed eruption
SITE : most commonly associated with the first permanentmolars and the maxillary incisors

Radiological features
• The cyst may throw a soft-tissue shadow, but there isusually no bone involvement except that the dilated andopen crypt may be seen on the radiograph.
RADICULAR CYST
RADICULAR CYST
• Also called APICAL PERIODONTAL CYST
• Radicular cysts are the most common inflammatory cysts and arise from the epithelial residues in the periodontal ligament as a result of periapical periodontitis following death and necrosis of the pulp.
• Quite often a radicular cyst remains behind in the jaws after removal of the offending tooth and this is referred to as a residual cyst.
PATHOGENESIS
1. PHASE OF INITIATION:• Accepted generally that rests of Malassez included within a
developing periapical granuloma proliferates to form the lining of radicular cyst.
• How these cells are stimulated is not clear.
• Some product of non vital pulp can be responsible which simultaneously evokes an inflammatory response in CT.
• Immune factors also held responsible as plenty of plasma cells are seen in a periapical granuloma.

CLINICAL FEATURES
• Age : peak in 3rd, 4th and 5th decades.
• Sex : Slightly more in males.
• Site : Maxillary anterior region.
• Frequency: Commonest cystic lesion of jaws.
Signs & symptoms
• Primarily symptom less.
• Discovered accidentally during routine dental X ray exam.
• Slowly enlarging hard bony swelling initially. Later, if cysts breaks through cortical plates, lesion becomes fluctuant.
• Diagnostic criteria – associated teeth are non vital
• Rare in deciduous teeth.

RADIOLOGICAL FEATURES
• Classically presents as round / ovoid lucency with sclerotic borders and associated with pulpally affected tooth / teeth.
• If infection supervenes, the margins become indistinct, making it impossible to distinguish it from a peripaical granuloma.
Radiograph of a radicular cyst. The lesion is a well defined radiolucency associated with the apex of a non-vital root filled tooth.

HISTOLOGICAL FEATURES
• Lined partly / completely by non keratinized epithelium of varying thickness.
• The connective tissue wall shows inflammatory infiltrate mainly in the form of lymphocytes and plasma cells.
• Hyaline / Rushton bodies are found in epithelium and rarely in connective tissue wall.
• These are curved or linear structure with eosinophilic staining properties
HISTOLOGICAL FEATURES
• Cholesterol crystals in from of clefts are often seen in the connective tissue wall, inciting a foreign body giant cell reaction.
• Different types of dystrophic calcification are also seen in connective tissue wall.
• Mucus cell metaplasia as well as respiratory cells may be seen in the epithelial lining.
• Keratinization if found is due to metaplasia and must not be confused with an OKC.

Residual cysts
• Radiographic appearance of a large residual cyst left behind after extraction of 1st mandibular molar.
• The histopathological features of the residual cyst are similar to those described above for conventional radicular cysts. However, because the cause of the cyst has been removed, residual cysts may progressively become less inflamed so that eventually the cyst wall is composed of uninflamed
• The epithelial lining may be thin and regular and indistinguishable from a developmental cyst such as a dentigerous cyst or lateral periodontal cyst. collagenous fibrous tissue.
DIFFERENTIAL DIAGNOSIS:
• Following lesions must be distinguished from other periapical radiolucencies–
•1. Periapical granuloma2. Peripaical cemento – osseous dysplasia (early lesions)

Paradental Cysts
Paradental Cysts
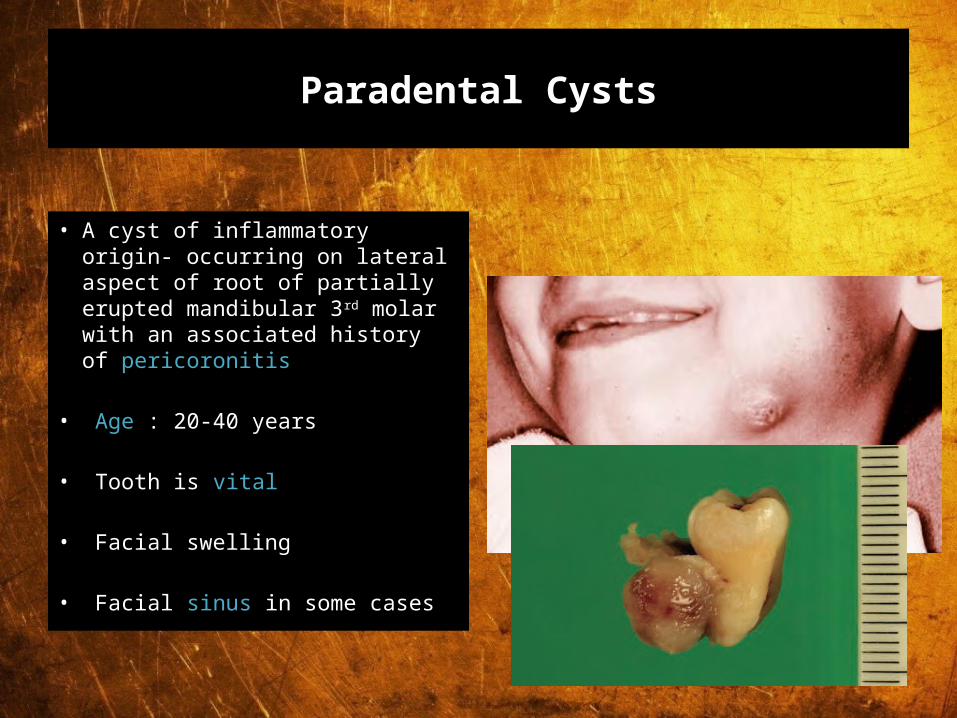
• A cyst of inflammatory origin- occurring on lateral aspect of root of partially erupted mandibular 3rd molar with an associated history of pericoronitis
• Age : 20-40 years
• Tooth is vital
• Facial swelling
• Facial sinus in some cases

Radiographic features
• Affected tooth is tilted Well demarcated RadioLucency Distal to partially erupted tooth
• Lamina Dura is intact
• New bone may be laid down
a
b
(a,b) Two cases of bilateral paradental cysts associated with erupting mandibular third molar teeth. The cysts are distal and buccal to the involved teeth. Note that the periodontal ligament space is not widened and that the distal part of the cyst is separate from the distinct distal follicular space.
GINGIVAL CYST OF ADULTS

PATHOGENESIS
• A number of suggestions have been made about thepathogenesis of the gingival cyst in adults.
• It was originallyproposed that they may arise from odontogenicepithelial cell rests; or by traumatic implantation ofsurface epithelium; or by cystic degeneration of deep projectionsof surface epithelium

ORIGIN
• Cystic transformation of dental lamina, traumatic implantation of surface epi
• Dome shaped soft, fluctuant swelling which is <1cm in diameter
• Lesion is slow growing and painless
• Adjacent teeth usually vital

CLINICAL FEATURES
• Signs and symptoms:• Slowly enlarging, well
circumscribed painless swelling.
• Invariably occurs on facial aspect of free / attached gingiva.
• Surface of lesion is smooth and of normal color.
• Fluctuant lesion, adjacent teeth are vital
Clinical photograph of a gingival cyst of an adult
AGE : 5th – 6th decade of life
SITE : mand. canine and Pre Molar area; attached gingiva or I/D papilla
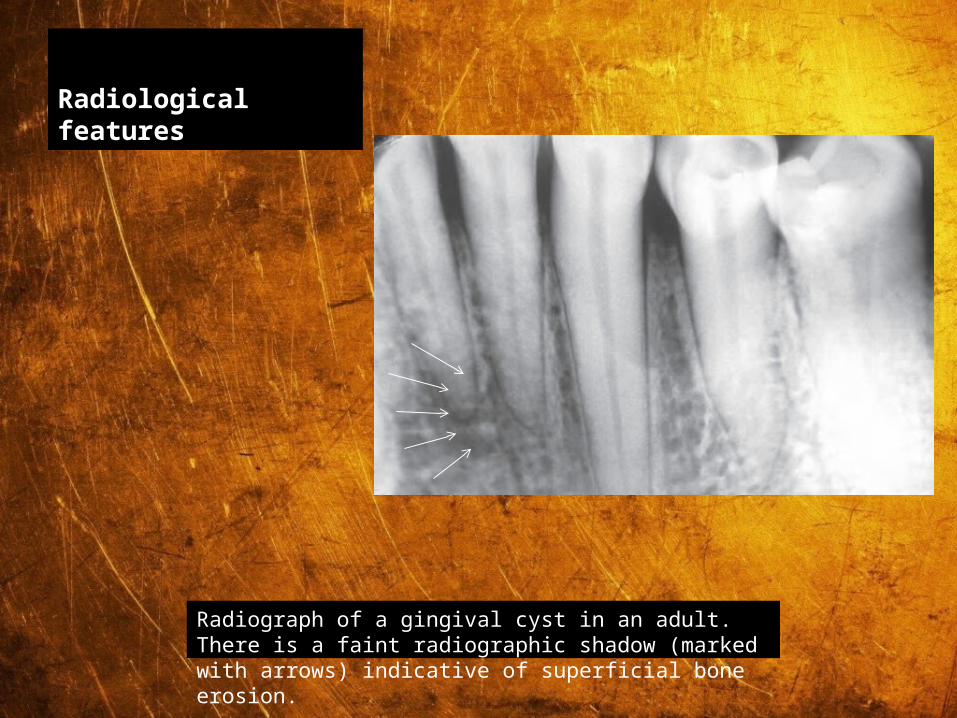
Radiological features
Radiograph of a gingival cyst in an adult. There is a faint radiographic shadow (marked with arrows) indicative of superficial bone erosion.
Histology
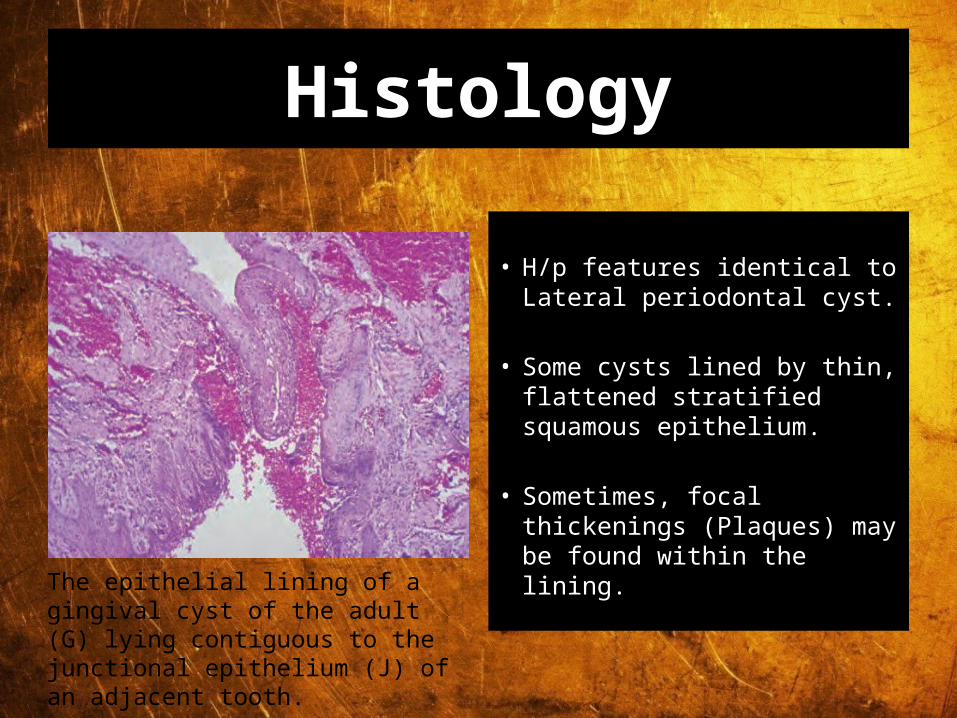
• H/p features identical to Lateral periodontal cyst.
• Some cysts lined by thin, flattened stratified squamous epithelium.
• Sometimes, focal thickenings (Plaques) may be found within the lining.
The epithelial lining of a gingival cyst of the adult (G) lying contiguous to the junctional epithelium (J) of an adjacent tooth.

LATERAL PERIODONTAL CYST

LATERAL PERIODONTAL CYST
• Uncommon, but well recognized type of odontogenic cyst.
• The designation ‘lateral periodontal cyst’ is confined to those cysts that occur in the lateral periodontal position and in which an inflammatory etiology and a diagnosis of collateral OKC have been excluded on clinical and histological grounds
• (Shear and Pindborg, 1975).

CLINICAL FEATURES
• Age : 20 – 60 years, peak in 6th decade.
• Sex : Male predilection.
• Site : Lateral PDL regions of mandibular premolars, followed by anterior maxilla

Signs & symptoms
• Usually asymptomatic as it occurs on the lateral aspect of root of tooth.
• Associated teeth are vital, unless otherwise affected.
• Cysts rarely < 1cm in size, except for BOTRYOID VARIETY which is larger and also a multilocular lesion.

Radiological features
• Round to ovoid ‘lucency with sclerotic margins.
• Cyst can be present anywhere between cervical margin to root apex.
• Radiographically, it can be confused with collateral OKC.
Radiograph of a lateral periodontal cyst lying between the mandibular premolar teeth. The margins are well corticated, indicative of slow enlargement.

RADIOLOGICAL FEATURES
Lateral periodontal cyst. Radiolucent lesionbetween the roots of a vital mandibular canine and first premolar.
Lateral periodontal cyst. A larger lesion causingroot divergence.

HISTOLOGICAL FEATURES
• The lateral periodontal cysts were lined by a thin, non-keratinising layer of squamous or cuboidal epithelium usually ranging from 1 to 5 cell layers wide, which resembled the reduced enamel epithelium
• The epithelial cells were sometimes separated by intercellular fluid. Their nuclei were small and pyknotic.
• An interesting feature seen in many of the lateral periodontal cysts was the presence of what appear to be localised plaques or thickenings of the epithelial lining
• Small epithelial nests may be seen in connective tissue wall, which may show signs of mild inflammation.

HISTOLOGICAL FEATURES
Lateral periodontal cyst which in part has a thin, nonkeratinised stratified squamous epithelial lining resembling reduced enamel epithelium. Two epithelial plaques are seen. The one on the right is convoluted

CALCIFYING ODONTOGENIC CYST
CALCIFYING ODONTOGENIC CYST
• Also called as Odontogenic ghost cell cyst or Gorlin cyst.
• It Has many features of odontogenic tumor, therefore it is placed in the category of tumors in the latest WHO classification of odontogenic cysts and tumors.
• In the latest WHO publication on odontogenic tumours (Prætorius and Ledesma-Montes, 2005) it was classified as a benign odontogenic tumour and was renamed calcifying cystic odontogenic tumour (CCOT).

.REFERENCE 1. Boss, J. H.: A Rare Variant of Ameloblastoma, A. M. A. Arch. Path, 68: 299-305, 195

Clinical FeAtures
• Age : Wide range, peak in 2nd decade.
• Sex : Equal.
• Site : Anterior segment of both jaws

PATHOGENESIS
• COC is a unicystic process and develops from the reduced dental epithelium or remnants of dental lamina.
• The cyst lining has the potential to induce formation of dentinoid or even odontoma in adjacent CT wall.

CLASSIFICATION OF THE ODONTOGENIC GHOST CELL LESIONS
• Group 1 : ‘Simple’ cysts Calcifying odontogenic cyst (COC)
• Group 2 : Cysts associated with odontogenic hamartomas or benign neoplasms: calcifying cystic odontogenic tumours (CCOT).

Signs & symptoms
• Swelling is the commonest complaint, seldom associated with pain.
• Intraosseous lesions can cause hard bony expansion and resulting facial asymmetry.
• Displacement of teeth can also occur.

RADIOLOGICAL FEATURES
• Intraosseous lesions produce well defined lucency which is usually unilocular.
• Irregular calcified masses of varying sizes may be seen within the lucency.
• Displacement of root/roots with or without root resorption and expansion of cortical plates also seen
Radiograph of a calcifying odontogenic cyst of the maxilla. There is a well-demarcated margin and calcifications suggestive of tooth material.
RADIOLOGICAL FEATURES
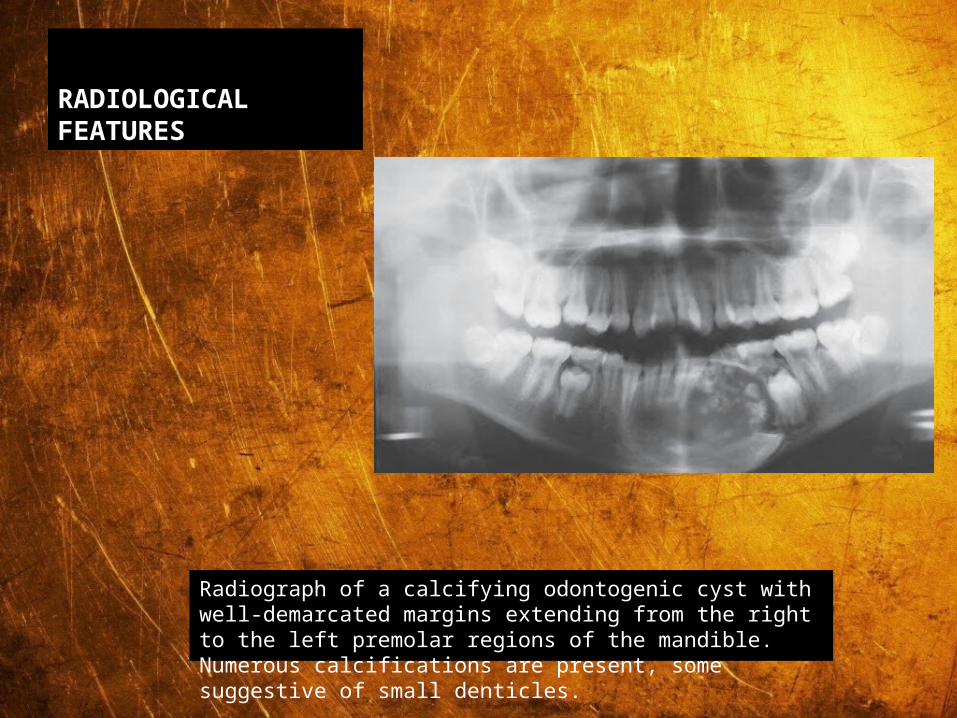
Radiograph of a calcifying odontogenic cyst with well-demarcated margins extending from the right to the left premolar regions of the mandible. Numerous calcifications are present, some suggestive of small denticles.
Histological features
• Lining is usually thin about 6 – 8 cell thick, may be thickened in other areas.
• TYPICALLY – GHOST CELLS may be seen in thicker areas of lining.• Ghost cells are enlarged, ballooned, ovoid, eosinophilic cells with
well defined cell boundaries..• They represent abnormal keratinization and frequently calcify.• Tubular dentinoid and even complex odontome may be found in
connective tissue wall close to epithelial lining.

DIFFERENTIAL DIAGNOSIS
• Based on radiographic appearance, following lesions must be included in the provisional diagnosis –• Ameloblastoma• CEOT• AOT• Ameloblastic fibro odontoma
-SURGICAL EXCISSION-BLOCK EXCISSION-SEGMENTAL RESECTION-PERIPHERAL LESIONS –CONSERVATIVE MANAGEMENT

Nasopalatine Duct (Incisive Canal) Cyst

Nasopalatine Duct (Incisive Canal) Cyst
• Also classified as “FISSURAL CYSTS”.
• Believed to be derived from epithelial remnants included during closure of embryonic facial processes.
• Controversy – actual “closure” of embryonic processes does not occur. Grooves between processes is smoothed by proliferation of underlying mesenchyme.
• Usually occurs within the nasopalatine canal or in soft tissue of palate at the opening of canal.

CLINICAL FEATURES
• Age : 4th, 5th & 6th decades.
• Sex : More in females
• Frequency: Commonest non odontogenic developmental cyst

PATHOGENESIS
• In lower animals, the NP duct concerned with olfactory sensation – in humans only vestigial remnants persist in incisive canal in form of epithelial islands, ducts, cords etc.
• These nests can show central degenration to form cysts. Etiology for cyst transformation is yet unclear.
• Some believe, it may arise spontaneously like an OKC.

Signs & symptoms
• Commonest symptom is swelling, usually in anterior region of mid palate.
• Swelling can also occur in midline on labial aspect of alveolar ridge.
• If pressure on NP nerves – pain
• Exclude possibility of periapical cyst by testing vitality of incisors.
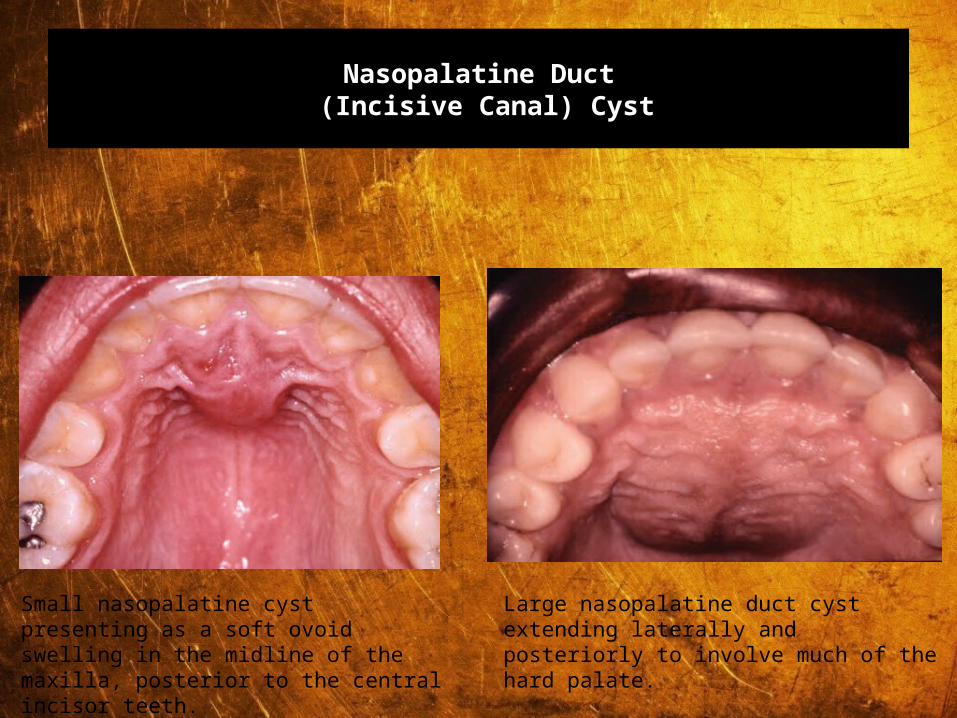
Nasopalatine Duct (Incisive Canal) Cyst
Small nasopalatine cyst presenting as a soft ovoidswelling in the midline of the maxilla, posterior to the central incisor teeth.
Large nasopalatine duct cyst extending laterally andposteriorly to involve much of the hard palate.

RADIOLOGICAL FEATURES
• Seen as lucency usually in incisive canal – DIFFICULT TO DISTINGUISH FROM A NATURALLY LARGE INCISIVE CANAL.
• Lucency with AP dimension upto 10 mm considered as enlarged incisive canal, but if lucency < 14 mm, then NP duct cyst.
• The lucency appears well defined with sclerotic borders, in midline of palate between roots of incisors.

RADIOLOGICAL FEATURES
Radiograph of a nasopalatine duct cyst showing a pear-shaped radiolucency in the anterior maxilla. The lamina dura on the left is intact although the apex appears to be in the cyst.
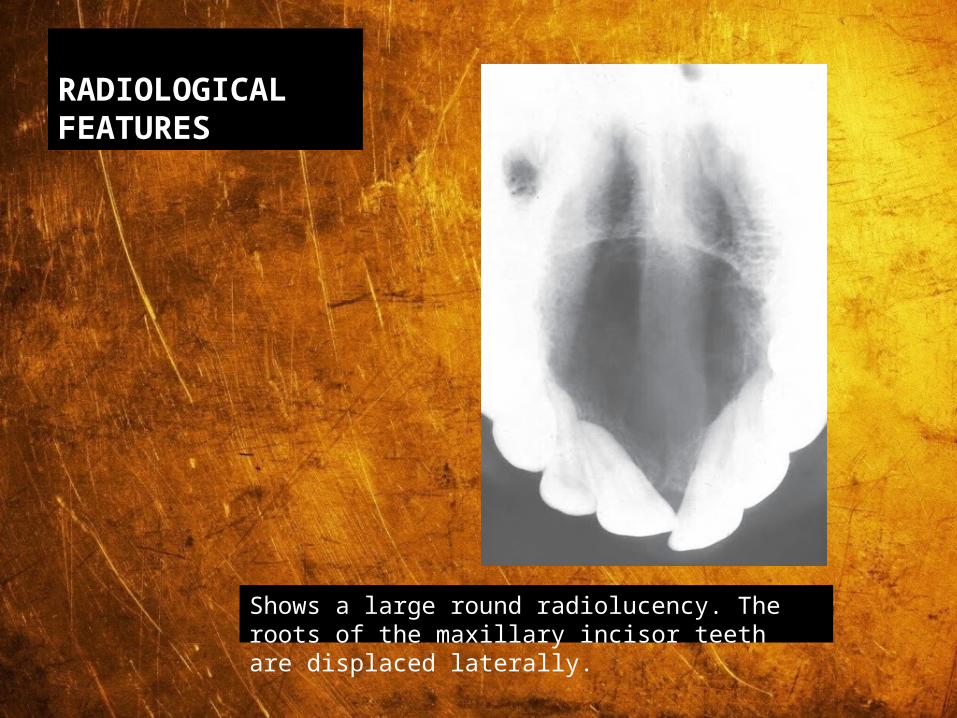
RADIOLOGICAL FEATURES
Shows a large round radiolucency. The roots of the maxillary incisor teeth are displaced laterally.
Histological features
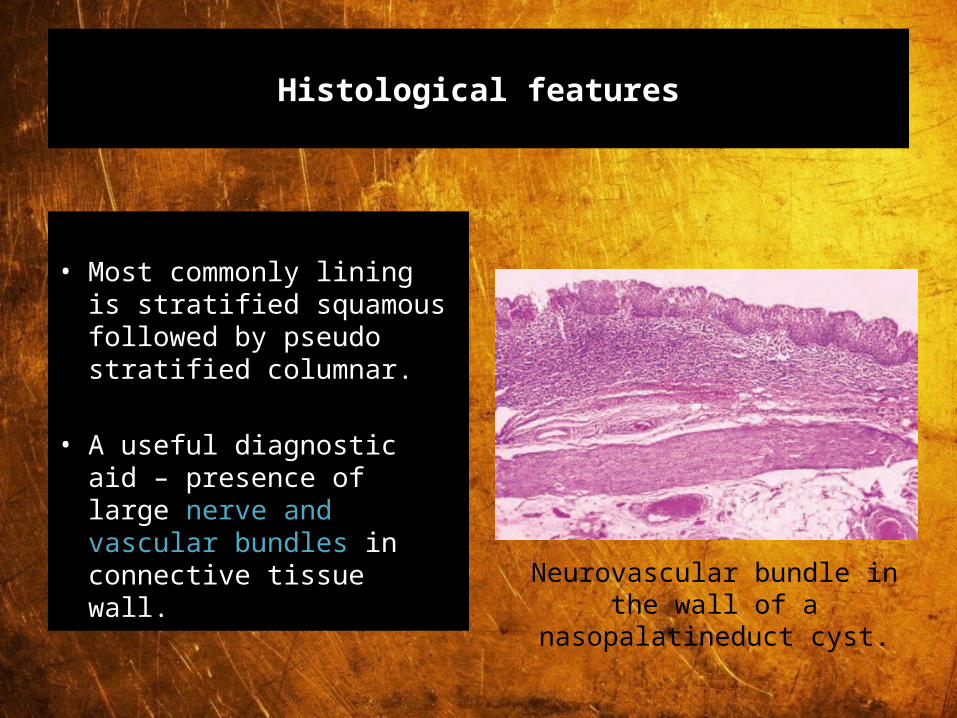
• Most commonly lining is stratified squamous followed by pseudo stratified columnar.
• A useful diagnostic aid – presence of large nerve and vascular bundles in connective tissue wall.
Neurovascular bundle in the wall of a nasopalatineduct cyst.

DIFFERENTIAL DIAGNOSIS
• Radicular cyst, if it is associated with a pulpally involved tooth.
• Large incisive canal.

NASOLABIAL CYST

NASOLABIAL CYST
• The nasolabial cyst occurs outside the bone in the nasolabial folds below the alae nasi.
• It is traditionally regarded as a jaw cyst although strictly speaking it should be classified as a soft tissue cyst.

Clinical features
• Age : Peak incidence in 4th & 5th decades.
• Sex : More in females.
• Frequency: Rare in occurrence.

Signs & symptoms
• Commonest complaint – slowly growing swelling and occasionally, pain and difficulty in nasal breathing.
• Extra orally – filling out of nasolabial fold and may lift ala nasi.
• Intra orally – bulge in labial sulcus.
• Fluctuant lesion.
Nasolabial cyst producing a swelling of the right upper lip, forming a bulge in the labial sulcus.
PATHOGENESIS
• Believed to develop from lower anterior portion of nasolacrimal duct.
• When margins of lateral and maxillary processes fuse, ectoderm along boundary between them gives rise to solid cellular rod which first develops as a linear surface elevation (Nasolacrimal ridge) and then sinks into underlying mesenchyme.
• This solid rod canalizes to form NL duct.
• The NL cysts are located such that it is possible that they develop from embryonic remnants of NL duct.
• Importantly, a mature NL duct is lined by pseudo stratified columnar epithelium, which is also the lining of NL cyst.

RADIOLOGICAL FEATURES
• Difficult to interpret on radiograph.
• May be seen as localized increased lucency of alveolar process above apices of incisors.
• Lucency results from pressure resorption on labial surface of maxilla.
Standard occlusal radiograph of a patient with a nasolabial cyst. There is a posterior convexity of the left half of the radiopaque line that forms the bony border of the nasal aperture.

Aneurysmal Bone Cyst

Aneurysmal Bone Cyst
• Uncommon cyst, found mostly in long bones and spine.
• CLINICAL FEATURES: -1. Age : First 3 decades.2. Sex : Mainly females.3. Site : molar regions of mandible & maxilla.
• Signs & symptoms: • Hard, rapidly growing swelling which can cause malocclusion. • If lesion perforates cortical plates, can cause “egg shell crackling”.
PATHOGENESIS
• Controversy whether lesion arises de novo or from a vascular disturbance in the form of sudden venous occlusion or development of an AV shunt occurring secondarily in a pre existing lesion like central giant cell granuloma, Osteosarcoma etc.
• Due to the malformation, change in hemodynamic forces occurs which can lead to ABC.

RADIOLOGICAL FEATURES
• Classically seen as a unilocular, ovoid / fusiform lucency which balloons the cortical plates.
• Teeth displacement and root resorption also observed.
• Lesions are usually unilocular but longer-standing lesions may show a ‘soap-bubble’ appearance and may become progressively calcified

Radiograph of an aneurysmal bone cyst involving the angle and ascending ramus of the mandible. There is a ballooning expansion of the cortex.

Histological features
• It consist of many capillaries and blood-filled spaces of varying size lined by flat spindle cells and separated by delicate loose-textured fibrous tissue
• Most lesions contain small multinucleate cells and scattered trabeculae of osteoid and woven bone.
• In some of the solid areas, sheets of vascular tissue, containing large numbers of multinucleate giant cells, fibroblasts, haemorrhage and haemosiderin, look very much like giant cell granuloma of the jaws
• The diagnosis is made primarily on the basis of the clinical and radiological features because histologically such solid lesions may be indistinguishable from giant cell granuloma.

Histological features
Aneurysmal bone cyst in which the solid areas have histological features identical to those of the central giant cell granuloma of the jaws (H & E).
Aneurysmal bone cyst of the mandible. The solid areas show the features of cemento-ossifying fibroma and a portion of one of the many cystic spaces is present at the top of the photomicrograph(H & E).

DIFFERENTIAL DIAGNOSIS
• Conventional ameloblastoma• CEOT• Central giant cell granuloma

In 36 cases, including the present ones. The mandible was affected in 28 cases (78%) and the maxilla in 8 (22%). Aneurysmal bone cyst was observed to occur most frequently between the mandibular body and the ramus. Patient age ranged from 6 to 87 years, with a mean age of 27.7 years. Patients under 30 years of age occupied 60% of the total. Treatment options suggested in the literature include percutaneous sclerotherapy, therapeutic embolization, curettage, block resection and reconstruction, radiotherapy, and systemic calcitonin therapy.

Solitary Bone Cyst
SOLITARY BONE CYST
• Also called as Hemorrhagic bone cyst, or Traumatic bone cyst.
• Commonly seen in mandible, rare in maxilla.
• Identical to solitary bone cyst of humerus in children and adolescents.


CLINICAL FEATURES
• Age : Young individuals
• Sex : Equal
• Site : Body and symphysismenti of mandible.
PANAROCHA ET AL

PATHOGENESIS
• None of the theories are certain about exact cause.
• First theory – cyst may follow trauma to bone which causes intra medullary hemorrhage which fails to organize. This clot subsequently liquefies - CYST.
• Recent theory osteogenic cells fail to differentiate locally and thus instead of bone, the undifferentiated cells form synovial tissue.

Alternative developmental pathways include cystic degeneration of primary tumors of the bone,
such as central giant cell granuloma, disorders of calcium metabolism, and ischemic necrosis of bone
marrow. (bleeding in jaw with clot resorption)
Signs & symptoms
• Asymptomatic.
• Rarely, swelling and pain may be seen.
• Half of all patients give a history of trauma to the area.
RADIOLOGICAL FEATURES
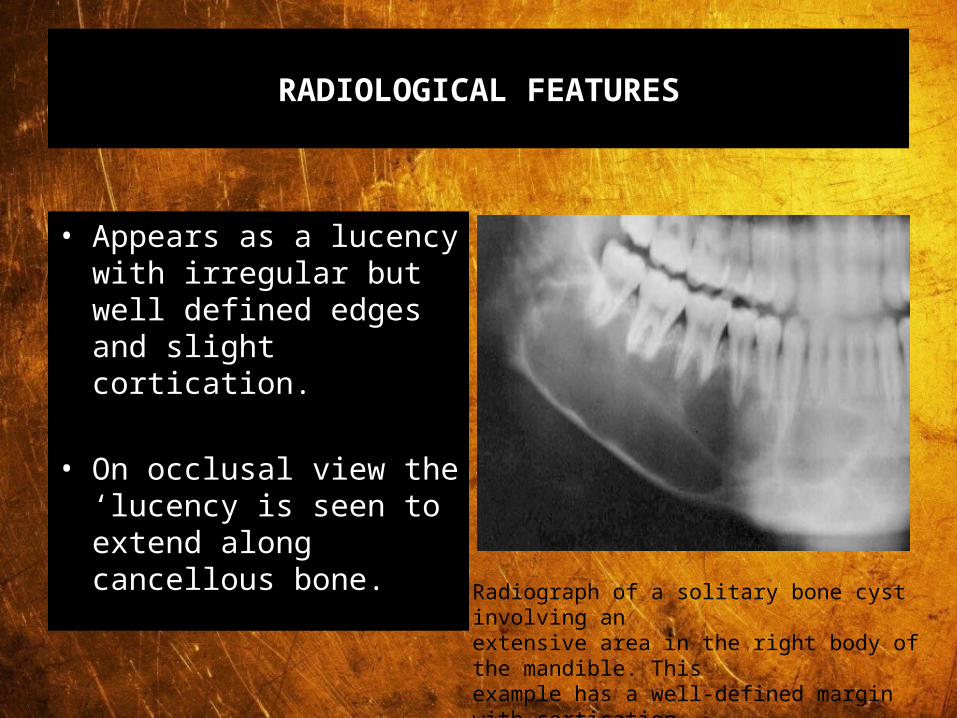
• Appears as a lucency with irregular but well defined edges and slight cortication.
• On occlusal view the ‘lucency is seen to extend along cancellous bone.
Radiograph of a solitary bone cyst involving anextensive area in the right body of the mandible. Thisexample has a well-defined margin with cortication.Interradicular scalloping is a prominent feature.

Traumatic bone cyst

• H/P:• Grossly, only minimal amount of fibrous tissue
from the bony wall are seen. The lesion may occasionally contain blood or serosanguinous fluid . Microscopically, delicate ,well vascularized fibrous connective tissue without evidence of an epithelial component is identified.
• Rx & prognosis:• Once entry into the cavity is accomplished, the
clinician need merely established bleeding into the lesion before closure. Organization of the bony clot results in complete bony repair without recurrence.

RADIOGRAPHIC FEATURES
• A well-delineated area of radiolucency with an irregular but defined edge is noted. Interadicular scalloping of varying degrees is characteistic & occasionally slight root resorption may be observed.
• Empty “ dead” space in medullary bone, esp mandible.
• Traumatic bone cyst have often been seen in association with florid osseous dysplasia ( fod). The relationship b/w these 2 entities is not understood.
TREATMENT MODALITIES
Results suggest that piezosurgery may be considered effective in cyst enucleation
compared to traditional
procedures with burs, since it grants
patients significantly less post-surgical pain
and swelling

• It is now recognised that grafting with autogenous cancellous bone can be performed successfully within oral wounds. In case of large defects, when pathologic fractures are possible or there would be considerable loss of contour in a future denture-bearing area, this procedure can be used to obliterate the cavity and stimulate osteogenesis. Should grafting be indicated, autogenous bone provides the best results if a second wound is not a major consideration (Boyne-1970; Flint-1964; Mowlem-1944; Scott, Peterson and Grant-1949).
• A risk of bone grafting cyst cavities is the possibility of bone fragments becoming infected if wound breakdown occurs. The risk of failure in these cases is greater than when grafts are introduced after resection of a segment of mandible, because of the greater difficulty in ensuring watertight wound closure.

CONCLUSION• Cystic lesions are very common in jawbones and it
includes those of both odontogenic and non-odontogenic origin. Odontogenic cysts are unique to the jawbones.
• The diagnosis of these lesions is often delayed because of their innocent presentation.
• This leads to various sequelae such as fractures. Other complications eventhough rare such as malignant transformation of cystic lining is of considerable importance
• Enucleation with primary closure should be treatment of choice wherever possible because of the least unfavourable sequelae.
•