Cynthia M. Dorsey, Ph.D. Director, Sleep Research Program McLean Hospital, Belmont, MA Assistant...
49
Cynthia M. Dorsey, Ph.D. Director, Sleep Research Program McLean Hospital, Belmont, MA Assistant Professor of Psychology (Dept. of Psychiatry) Harvard Medical School, Boston, MA Sleep Disturbances in Substance Abuse: Assessment and Management Humana Lecture Humana Lecture
-
Upload
leslie-james -
Category
Documents
-
view
256 -
download
0
Transcript of Cynthia M. Dorsey, Ph.D. Director, Sleep Research Program McLean Hospital, Belmont, MA Assistant...

Cynthia M. Dorsey, Ph.D.
Director, Sleep Research ProgramMcLean Hospital, Belmont, MA
Assistant Professor of Psychology (Dept. of Psychiatry)Harvard Medical School, Boston, MA
Sleep Disturbances in Substance Abuse:
Assessment and Management
Humana LectureHumana Lecture

Sleep Disturbance in Those Who Abuse Drugs
Can Occur During:
• acute use
• chronic use
• withdrawal

Sleep Disturbance in Those Who Abuse Drugs
Can Involve:
• insomnia
• hypersomnia
• disruption of sleep-wake cycle
Differing profile for different drugs
Thompson et al., Biol Psychiatry 1995;38

Sleep Disturbance in Substance Abuse
• Opiates
• Stimulants
• Alcohol
• Hypnotics

Sleep Disturbance:Opiates
Acute/Chronic Use:
• Disrupted sleep: - frequency of awakenings- sleep time, “deep sleep”
• Sleep architecture abnormalities:- REM sleep (supression)
(latency prolonged/amount reduced) Kay et al., Br J Clin Pharmacol 1981;11 Davison et al., Pharmacology and Clinical Implications. 1973

Sleep Disturbance:Opiates
Withdrawal:
• Pronounced insomnia that often contributes to relapse
• Sleep architecture abnormalities- REM (“rebound”):
(latency is shortened/time increased)
Gillin et al. In:Principles and Practice of Sleep Medicine, 2000
Kay, Electroenceph Clin Neurophysiol. 1975.

Sleep Disturbance:Cocaine
Acute/Chronic Use: • Sleep continuity and architecture
abnormalities:- frequency of awakenings- REM sleep supression- disrupted sleep cycle

Sleep Disturbance:Cocaine
Withdrawal:
• hypersomnia
• • Sleep Architecture Abnormalities- REM “rebound”- SWS (deep sleep) is reduced(persists for 3 wks in chronic users)
Kowatch, J Addict Dis 1992

Sleep Disturbance:Alcohol
Acute Use by non-Alcholics:
• latency to sleep• disruption of sleep 2nd 1/2 of night• gastric irritation, headache• sympathetic arousal (tachycardia,
sweating, etc.)• additive effect with sleep deprivation
Lobo et al. 1997

Sleep Disturbance:Alcohol
Chronic Use by Alcoholics:
• insomnia: latency, awakenings• hypersomnia• sleep architecture abnormalities• sleep cycle disturbance• increased frequency/severity of other sleep disorders

Sleep Disturbance:Alcohol
Withdrawal:
• Insomnia latency to sleep, deep sleep
• Disrupted architecture (acute): REM sleep, REM latency
• Sleep disruption often persists and may predict relapse
Brower et al. 1998

Insomnia is a Risk FactorFor Developing Alcohol Abuse:
• Sleep disturbance due to worry higher risk of alcohol-related problems
• Risk highest for those with depression or anxiety
Crum et al, 2004

Insomnia is a Risk FactorFor Developing Alcohol Abuse:
• Insomniacs self-medicate with alcohol
• 10-15% persistent insomnia inthe general population
• 30% persistent insomniacs have used alcohol to help sleep
• 67% of those found it effective Roehrs et al., 2000; Ancoli Israel and Roth, 2000

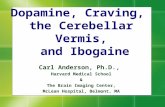
Insomnia is a Risk Factor for Substance Abuse
0
2
4
6
8
10
12
14
16
18
Depression Anxiety Alcohol Drug
Insomnia n=240
No Insomnia n=739
Incidence (%) over 3.5 years
****
**
* 95% C.I. for Odds Ratio excludes 1.0
Adapted from Breslau N et al. Biol Psychiatry 1996;39.
Od
ds
Rat
io

Substance Abuse is a Risk Factor for Developing Insomnia
• Previous history of insomnia
• Increasing age
• Female gender
• Psychiatric symptoms and disorders
• Medical symptoms and disorders
• Substance abuse/dependence

Insomnia Substance Abuse
Reciprocal Relationship

Prevalence of Insomnia
• Insomnia is the most common sleep complaint in the industrialized world
• Complaints in 30% to 40%
• Complaint with distress or impairment: 8% to 19%
Sateia MJ et al. SLEEP 2000;23.

Prevalence of Insomniain Urban South America
Buenos Aires, Mexico City, Sao Paulo
• Complaints in 23%
• Complaints of moderate or severe insomnia: 6% (26% of sufferers)
• Sufferers who sought help from a physician: 31%
Blanco et al. BMC Fam Pract. 2003;4(1).

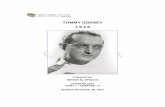
Insomniacs Under-Report Sleep Problems to Physicians
Percent of insomniacs who discussed any sleep problems with their physicians
Adapted from Ancoli-Israel S et al. SLEEP 1999;22.
Never discussed (69%)
Discussed sleep during visit for other purpose (26%)
Visited specifically to discuss sleep problem (5%)

What is Insomnia ?A complaint of:
• Difficulty falling asleep
• Difficulty staying asleep
• Poor quality sleep
Associated with:
• Distress
• Impaired function

Insomnia: Daytime Complaints• Fatigue, sluggishness
• Sleepiness
• Somatic complaints
• Worry about insomnia
• Mood disturbances
• Poor concentration
• Impaired performance

Insomnia: Consequences• Decreased quality of life• Increased healthcare costs• Increased absenteeism• Decreased productivity• Increased risk for psychiatric disorders
and substance abuse• Increased accident risk
Chesson A Jr. et al. SLEEP 2000;23.Sateia MJ et al. SLEEP 2000;23.

Assessment: Patient History
• History of sleep complaint
• Daytime symptoms
• Sleep habits (24-hour sleep / wake cycle)
• Risks / Precipitating Factors
• Medical/neurological/psychiatric history
• Medications
• Health habits

Assessment: Sleep/wake Diary

Assessment: Polysomnography• Indications
– Suspect other sleep disorder
– Poor treatment response
• Not routinely indicated for the evaluation of insomnia
Practice parameters for the evaluation of chronic insomnia. SLEEP 2000;23.

Obstructive Sleep ApneaRepetitive upper airway obstruction during sleep:
Symptoms: snoring, sleepiness, witnessed pauses in breathing, increased BMI/neck size
Results: oxygen desaturation,arousal from sleep, increased risk
for HTN, arrhythmia.

Obstructive Apnea on Polysomnogram

Treatment for Obstructive ApneaContinuous Positive Airway Pressure
Over 1 Million People Sleep at Night with CPAP in the U.S.
Flow Generator
Nasal Mask
Tubing
Headgear

Periodic limb movement disorder (PLMD)
•Repetitive stereotyped movements of foot/leg
•Usually only recognized by bedpartner, as “restlessness” or “kicking” during sleep

Pathophysiology of RLS/PLMD
Idiopathic
Familial (30-50%)
Iron Deficiency
Renal Failure
Peripheral Neuropathy
Antidepressants
Fibromyalgia
Rheumatoid Arthritis
Pregnancy
Caffeine

Treatment for RLS/PLMDDopaminergic agents:
Pramipexole .25 – 1.0 mg q8pm or
L-Dopa/Carbidopa 25/100-100/400 qhs
Persistent sleep disruption
Partial response
No response
Add sedative (e.g.,
Trazodone, benzo, gabapentin)
Add gabapentin or opiate
Reassess diagnosis

Clinical Presentation: Psychophysiologic Insomnia
Frustration, fear negative thinking
Intuitive efforts to self-treat:
bad sleep habits develop
Physiological activation
Difficulty sleeping

Evolution of Chronic Insomnia
poor sleep habits
negative cognitions and emotions
bedroom environment elicits wakefulness
• exacerbation of insomnia
growing sense of loss of control
•extreme frustration • trying too hard to sleep

Treatment of Insomnia

Why to do it with patients with substance abuse:
Cognitive-Behavior Therapy
• medication contraindications• pt. preference for a more “natural”
solution• patient sense of self-efficacy• it is effective

Behavioral Treatments
Strengthen bed & bedroom as sleep stimulus
Reset or reinforce biological rhythm Circadian rhythm entrainment
Reduce arousal & decrease anxietyRelaxation training
Address thoughts and beliefs that interfere with sleep.
Cognitive therapy
Restrict time in bed to improve sleep depth & consolidation
Sleep restriction
Stimulus control
Promote habits that help sleep; provide rationale for subsequent instructions.
Sleep hygiene
AimTechnique

Multi-modal CBT Approach
• Outcome Data
• Total WT 69 min. on average;45% improvement rate
• medication use by 59%;9/21 in DDI group became drug free
• treatment gains were maintained at 6 mo.

Key factors for Success :Empower the patient :
• explain rationale of all techniques
• make pt. an active participant
• encourage consistency and motivation
• reinforce therapeutic gains and patient sense of control

Pharmacotherapy
• Benzodiazepine receptor agonists
• Antidepressants
• Antihistamines
• Melatonin
• Others

Benzodiazepinesestazolam (Prosom)flurazepam (Dalmane)quazepam (Doral)temazepam (Restoril)triazolam (Halcion) clonazepam (Klonopin)lorazepam (Ativan)alprazolam (Xanax)diazepam (Valium)
Pharmacotherapy: Benzodiazepine Receptor Agonists
Nonbenzodiazepineszolpidem (Ambien)zaleplon (Sonata)
zopiclone (Imovane)eszopiclone (Lunesta)

Pharmacotherapy: Benzodiazepine Receptor Agonists
Actions
• Hypnotic
• Anxiolytic
• Myorelaxant
• Anticonvulsant
Side effects
• Sedation
• Anterograde amnesia
• Ataxia, falls
• Respiratory depression
• Tolerance, dependence, abuse

Antidepressants: Rationale
• No antidepressant is FDA-approved for treatment of insomnia
• However, some antidepressants have sedative, sleep-promoting effects
• Many insomnia patients have symptoms of depression or anxiety
• Low risk of abuse, but psychological dependence occurs

Pharmacotherapy: Antihistamines
• Mechanism of action– H1 receptor antagonism– Variable antagonism of cholinergic,
serotonergic, adrenergic receptors• Adverse effects
– Sedation, grogginess– Dry mouth– Psychomotor impairment– Delirium

Pharmacotherapy: Melatonin
• Naturally occurring hormone secreted during darkness at night
• Broad range of physiological effects• Inconclusive findings concerning sleep
promotion in insomnia• Not FDA approved or regulated• Potential vasoactive, CNS, and
reproductive side effects• May be useful in shifting circadian phase

Pharmacotherapy: Valerian
• Substance derived from Valeriana officinalis• Not FDA approved or regulated• Mild hypnotic effect (active component
unknown)• Some anxiolytic and muscle relaxant activity• Some studies show improved sleep latency and
quality of sleep, without change in sleep architecture
• No evidence of tolerance or abuse

Other Pharmacologic Agents
• Hormone replacement therapy
• Herbal therapies
• Over-the-counter agents

Pharmacologic Treatment: Specific Populations
• Sleep apnea: consider antidepressant rather than benzodiazepine receptor agonist
• Elderly: low-dose, short-acting benzodiazepine receptor agonist
• Substance abuse history: antidepressant preferred or non-pharmacologic techniques
• Co-morbid depression or anxiety disorder:– SSRI + benzodiazepine receptor agonist– SSRI + trazodone– Nefazodone, mirtazapine

Treatment and Management of Insomnia: A Suggested Approach
• Education and sleep hygiene • Nonpharmacologic approaches when
feasible• Pharmacologic approach:
• low-dose sedating antidepressant • Combination of nonpharmacologic and
pharmacologic methods• Referral to sleep specialist

Summary• Insomnia is prevalent and persistent in
abuse and withdrawal
• Substance abuse is a risk factor for insomnia and insomnia is a risk factor for developing substance abuse
• Efficacious treatment is available