
Current Treatment and Future Trends Anthony J. Palazzo, M.D.F.A.C.S.
32
Surgical Management of Valvular Heart Disease Current Treatment and Future Trends Anthony J. Palazzo, M.D.F.A.C.S.
-
Upload
hugo-golden -
Category
Documents
-
view
215 -
download
0
Transcript of Current Treatment and Future Trends Anthony J. Palazzo, M.D.F.A.C.S.

Surgical Management of Valvular Heart Disease
Current Treatment and Future Trends
Anthony J. Palazzo, M.D.F.A.C.S.
ObjectivesBrief discussion of most common pathologic
valvular disease involving aortic and mitral valves
Focus on aortic stenosis and mitral regurgitation
Indications for surgical interventionBest choice of prosthetic deviceCurrent and future trends
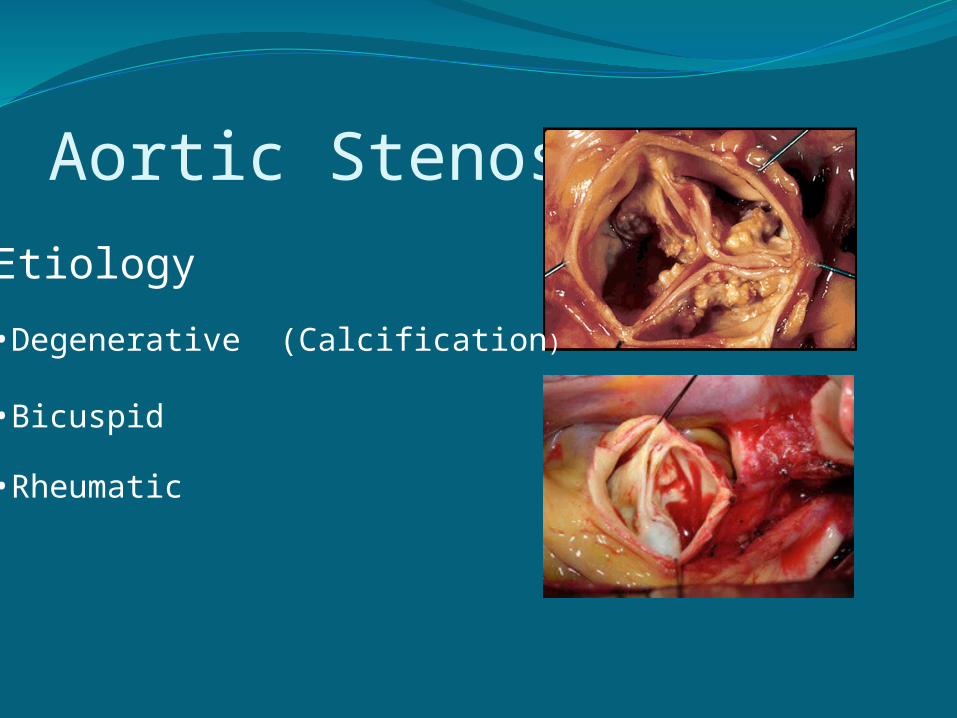
Aortic StenosisEtiology
•Degenerative (Calcification)
•Bicuspid
•Rheumatic

Aortic Stenosis - ClassificationIndicator Mild Moderate Severe
Jet Velocity (m/s)
< 3.0 3.0-4.0 >4.0
Mean Gradient(mm Hg)
<25 25-40 >40
Aortic Valve Area(cm²)
>1.5 1.0-1.5 <1.0
Normal Aortic Valve Area 2-4 cm²

Aortic Stenosis-PathophysiologyIncreased transvalvular gradientIncreased left ventricular afterloadLeads to development of LVH
Aortic Stenosis-Natural HistoryMultiple echocardiographic studies have
demonstrated that the average rate of decrease in aortic valve area is approximately 0.12 cm² per year
Ross and Braunwald study (1968)- landmark paper revealing natural history as it relates to symptoms
average survival with angina/syncope 3 yrs
average survival with dyspnea 2 yrs
average survival with CHF 1.5 yrs

Aortic Stenosis-Natural HistoryLoma Lima studyRetrospective review of 453 patients with
documented severe aortic stenosis on ECHOTreated non-surgicallySurvival at 1, 5, and 10 years was 62%, 32%
and 18%Demonstrated grave prognosis of patients
with severe aortic stenosisAnnThorSurg, 2006

Aortic Stenosis-Indications for Surgery
Patients with symptomsAsymptomatic patients with evidence of
diminished left ventricular function (EF < 50%)
Asymptomatic patients with normal ventricular function should be followed closely with serial echocardiography every 6 months due to known history of progression of 0.1-0.12 cm² and risk of death of 1-3% per year
Aortic Stenosis-Salient PointsOnce diagnosis is suspected echocardiogram
is single best non-invasive diagnostic test to determine aortic valve morphology, gradient and jet velocity
Symptomatic patients should be referred for surgical evaluation
Asymptomatic patients need to be followed closely for natural progression of disease
Asymptomatic patients with diminished left ventricular function should be referred for surgery

Aortic Regurgitation-Etiology
•Calcific degeneration (mixed lesion with stenosis)•Bicuspid aortic valve•Connective tissue disease (Marfan’s)•Aortic aneursym•Aortic dissection•Endocarditis

Aortic Regurgitation-PathophysiologyIncreased left ventricular overloadLeft ventricular dilatation Diminishing left ventricular function

Aortic Regurgitation-Indications for SurgerySymptomatic patients with severe aortic
regurgitation patients with angina have >10%
mortality/year >20% mortality/year with CHFEndocarditis with hemodynamic
decompensationAsymptomatic patients •surgery for patients with EF <50% •surgery for patients with evidence of left ventricular distension (end-diastolic dimension > 75 mm and end-systolic dimension > 55 m)

Mitral Stenosis
•Normal mitral valve area 4-6 cm²•Rheumatic heart disease most common cause•prevalence decreased significantly•Thickening and calcification of leaflets•Thickening of subvalvular structures (chords)•May have mixed lesions-MS/MR•Stenosis tends to progress slowly
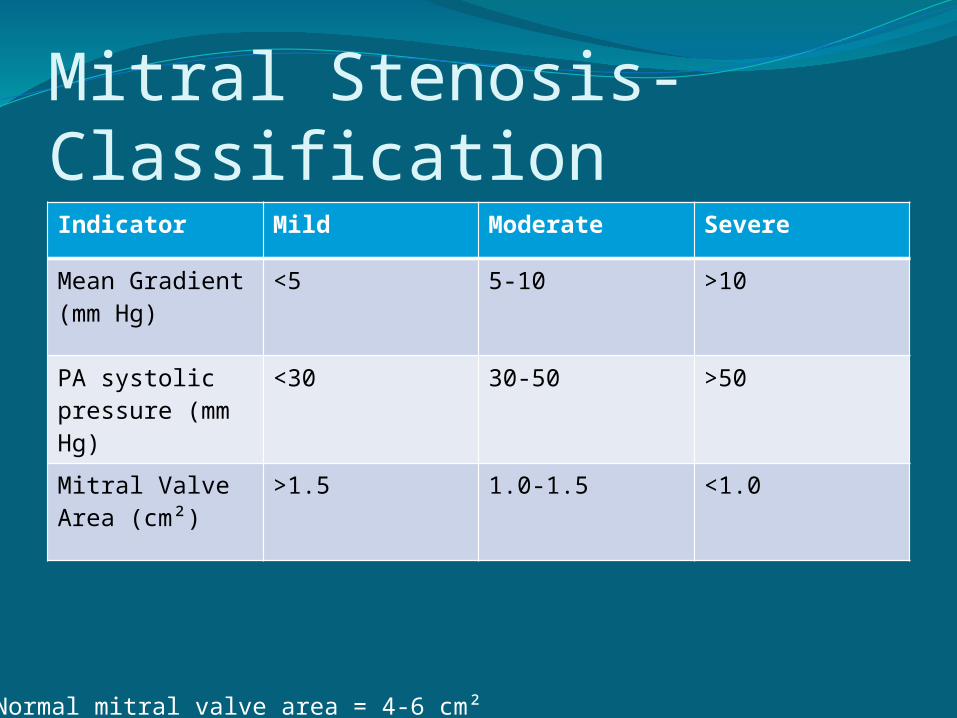
Mitral Stenosis-ClassificationIndicator Mild Moderate Severe
Mean Gradient (mm Hg)
<5 5-10 >10
PA systolic pressure (mm Hg)
<30 30-50 >50
Mitral Valve Area (cm²)
>1.5 1.0-1.5 <1.0
Normal mitral valve area = 4-6 cm²

Mitral Stenosis-Indications for SurgeryPatients with severe mitral stenosis with
class NYHA class III and IV symptoms who are not candidates for percutaneous balloon mitral valvulotomy (patients with mixed lesions or heavy calcification)
Asymptomatic patients with severe MS and severe pulmonary hypertension (PAP > 60 mm Hg)
No therapy recommended in asymptomatic patients without evidence of severe pulmonary hypertension

Mitral Regurgitation-EtiologyDegenerative “myxomatous” isolated leaflet prolapse Barlow’s diseaseIschemic acute- ruptured papillary muscle/chord 2°
AMI chronic- chronic myocardial ischemiaEndocarditis
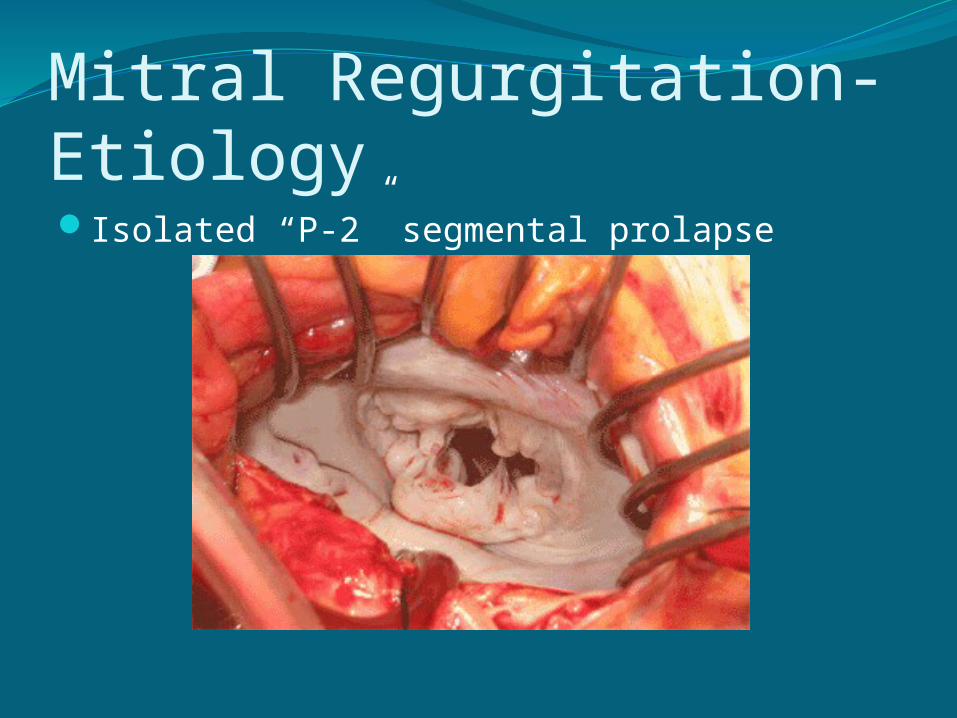
Mitral Regurgitation-EtiologyIsolated “P-2” segmental prolapse
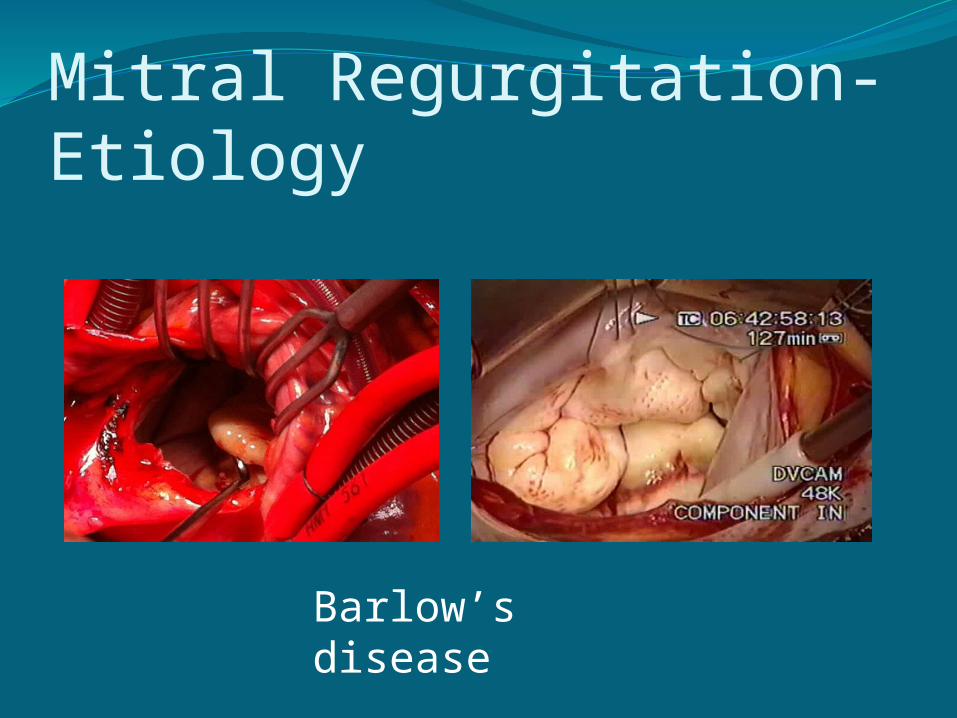
Mitral Regurgitation-Etiology
Barlow’s disease

Ischemic Mitral RegurgitationChronic ischemic mitral regurgitation annular dilatation papillary muscle retraction
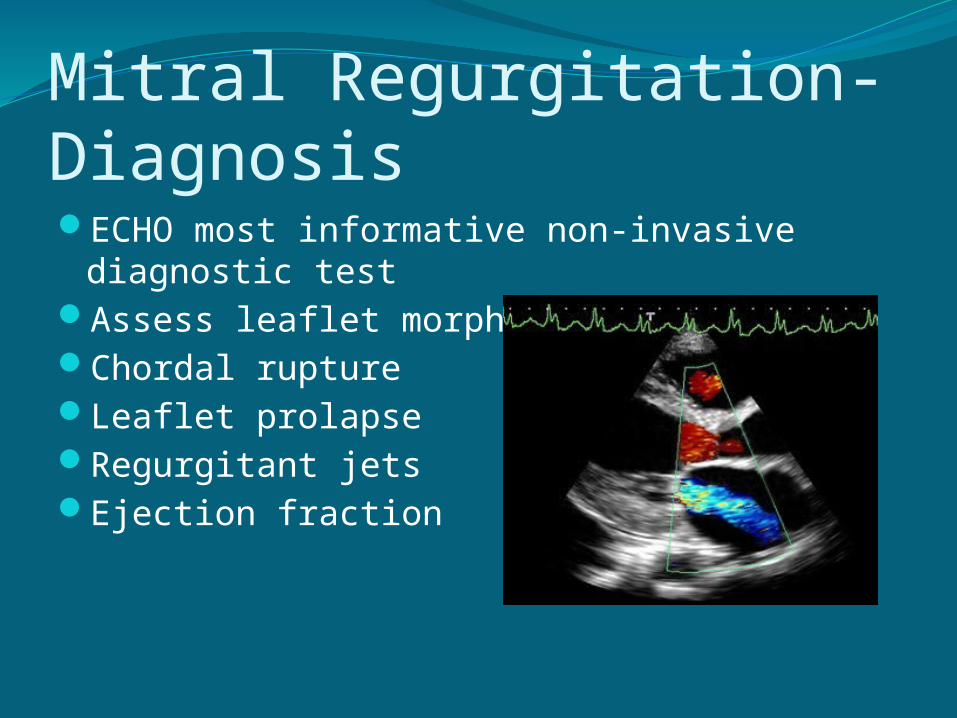
Mitral Regurgitation-DiagnosisECHO most informative non-invasive
diagnostic testAssess leaflet morphologyChordal ruptureLeaflet prolapseRegurgitant jetsEjection fraction
Mitral Regurgitation-Indications for Surgery (Class I indications)Symptomatic acute mitral regurgitation ruptured chord ruptured papillary muscleSymptomatic patients with chronic severe
MR as long as EF > 30%Acute endocarditis with hemodynamic
compromise, persistent sepsis, annular abscess, recurrent
emboliAsymptomatic patients with severe MR and
EF 30-60%

Mitral Regurgitation-Class IIa and IIb IndicationsPatients with severe MR with class III-IV
symptoms and EF < 30% and/or end-systolic dimension > 55 mm and if a repair is highly likely
There are 2 class IIb indications with asymptomatic patients with severe MR with EF > 60% who develop new onset atrial fibrillation and/or pulmonary hypertension (PAP > 50 mm Hg)

Mitral Regurgitation-AsymptomaticAsymptomatic patients with severe MR
should be followed closely with ECHO every 6 months
If there is evidence of left ventricular dysfunction with a decreased EF < 60 %, patients should be referred for surgery
Preoperative EF important predictor of long term survival after mitral valve surgery

Effect of preoperative EFLong term postoperative prognosis is related
to preoperative EF
Pre-op EF Normal EF EF 50-60% EF < 50%
10 yr survival
73 % 53 % 32 %
Circulation, 1995
Mitral Regurgitation-Salient PointsIn asymptomatic patients with severe mitral
regurgitation ventricular function should be followed closely
If EF decreases to < 60% or left ventricular end systolic diameter dimension exceeds 40 mm patient should be referred for surgery
Mitral valve repair is the ideal procedure

Prosthetic ValvesNo “perfect” prosthetic valveBioprosthetic valves versus mechanical
bioprosthetic
Avoids long-term anticoagulation
Limited durability

Prosthetic Valves
porcine bovine pericardial
mechanical
Prosthetic Valves-SelectionGenerally, if patient is > 65 a tissue valve is
recommendedDue improvements in the manufacturing
process tissue valves have increased durability
demineralization to prevent calcification “zero pressure” tissue fixationGeneral trend to place tissue valves in
younger patientsUltimate decision is patient’s

Prosthetic Valve SelectionSome tissue valves have demonstrated 85% 15
year structural free deteriorationSome evidence to suggest antiplatelet therapy
may be sufficient anticoagulation in select patients with mechanical AVR (not a guideline)
select cohort normal LV function normal sinus rhythym bileaflet mechanical valve ongoing clinical trails to determine efficiacy

Early Anticoagulation in bioprosthetic valvesHistorically “early” anticoagulation
recommended in immediate postoperative period for tissue valves is warfarin for 3 months (AHA/ACC guidelines)
Expanding clinical evidence to support use of antiplatelet therapy alone after aortic tissue valve placement in early postoperative period unless there is some other indication for warfarin¹΄²
1. JTCS,20052. JTCS,2010
Percutaneous TherapyTAVI (transcatheter aortic valve
implantation)Reserved for patients with severe aortic
stenosis who are not surgical candidates for open procedure
Recently FDA approvedLikely will be regulatedShould involve societal (STS) oversights and
databaseShould be collaborative, multidisciplinary
approach

Percutaneous Aortic Valve
•? Long term durability•Aortic insufficiency• equivalent 1 year survival¹ compared to open surgery in some studies
1. NEJM, 2010


















