Current state of breast cancer classification Marcella Mottolese UOC Anatomia Patologica.
55
Current state of breast cancer classification Marcella Mottolese UOC Anatomia Patologica
-
Upload
curtis-fields -
Category
Documents
-
view
216 -
download
0
Transcript of Current state of breast cancer classification Marcella Mottolese UOC Anatomia Patologica.

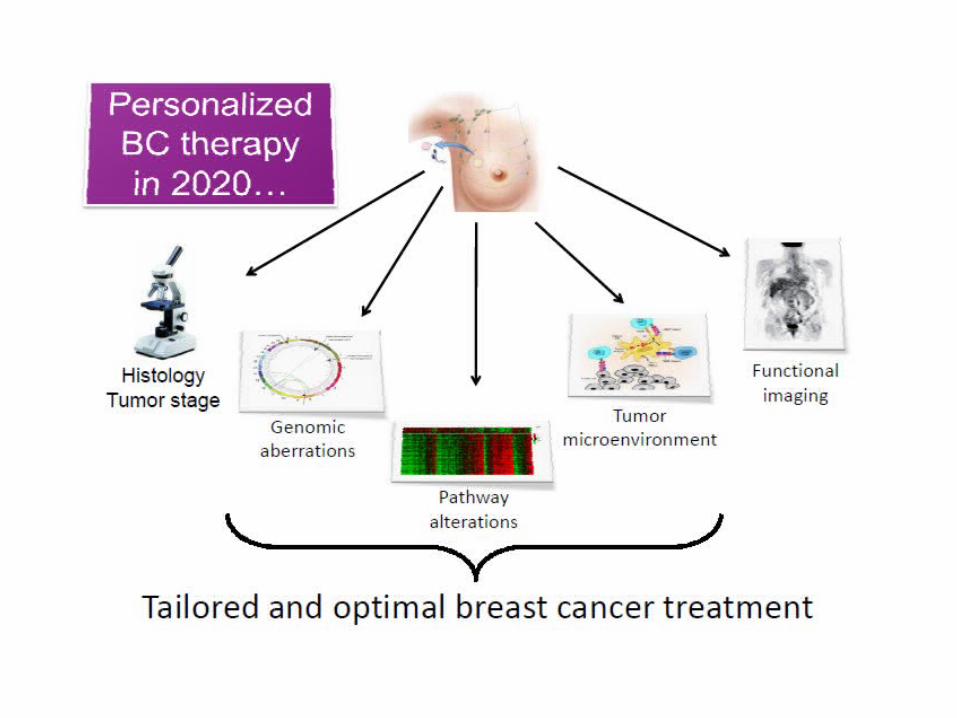
Current state of breast cancer classification
Marcella Mottolese
UOC Anatomia Patologica

screening programs and adjuvant therapy changed the management of breast cancer
impact in outcome with a decrease in mortality in most of the western world despite increasing breast cancer incidence

OPEN QUESTIONS ?
How to predict the response to currently available cytotoxic chemotherapy ?
How to identify tumor targets for directed therapies?
How to identify patients with node negative disease at very low risk of relapse for whom the risk/benefit ratio might be in favour of chemotherapy?

Response to the adjuvant chemotherapy , mainly in early stage of the disease, are affected by a
complex interplay of factors
Prognostic factors in breast cancer
Biomarkers Categories
1. Those that predict relapse or progression independent of future treatment effects designate as PROGNOSTIC FACTORS 2. Those that predict response or resistance to a specific therapy designate as PREDICTIVE FACTORS

Routinely used clinico-pathological parameters
Agetumor Size
lymph nodes lympho-vascular invasion
ER, PR; HER2;Ki67
Tumor grade
Clinico-pathological(tumor burden)
Biological (intrinsic chacteristics)
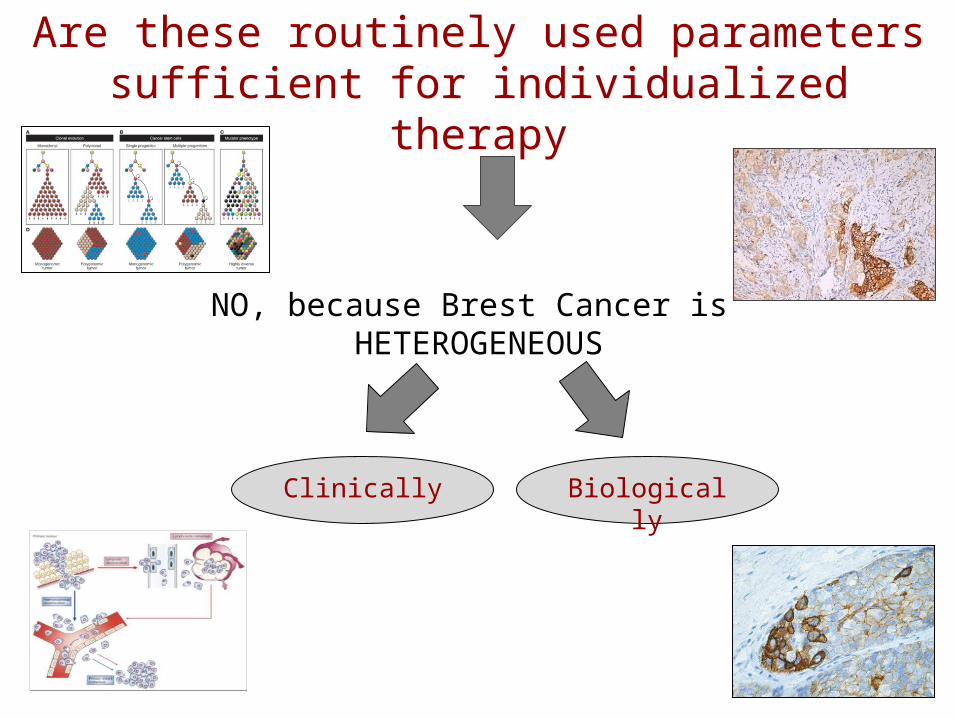
Are these routinely used parameters sufficient for individualized therapy
NO, because Brest Cancer is HETEROGENEOUS
Clinically Biologically
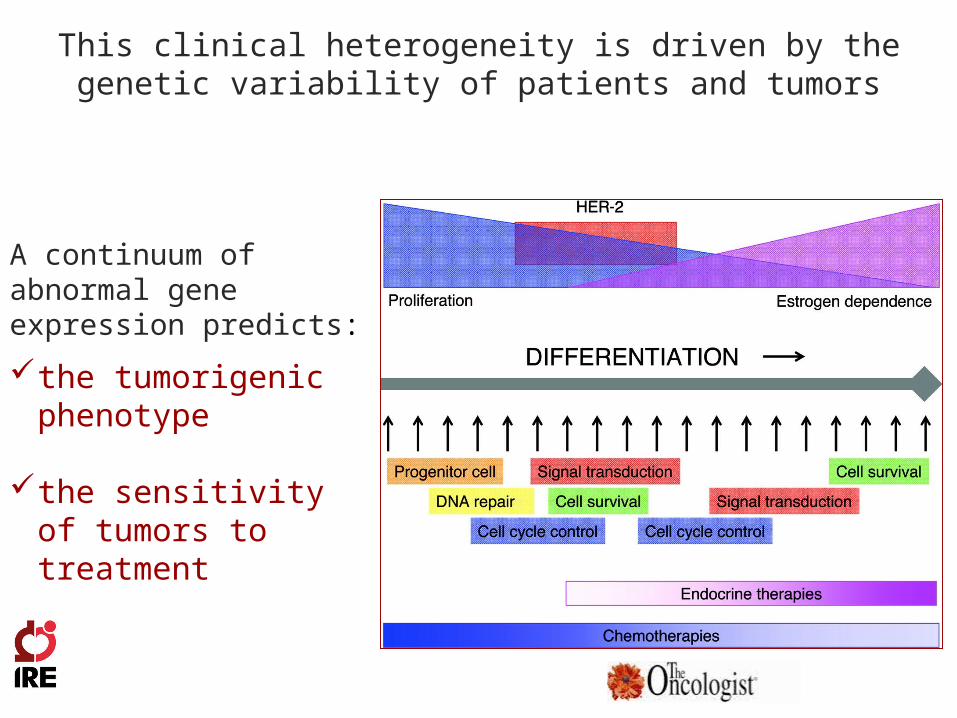
This clinical heterogeneity is driven by the genetic variability of patients and tumors
A continuum of abnormal gene expression predicts:
the tumorigenic phenotype
the sensitivity of tumors to treatment

Clinical tools
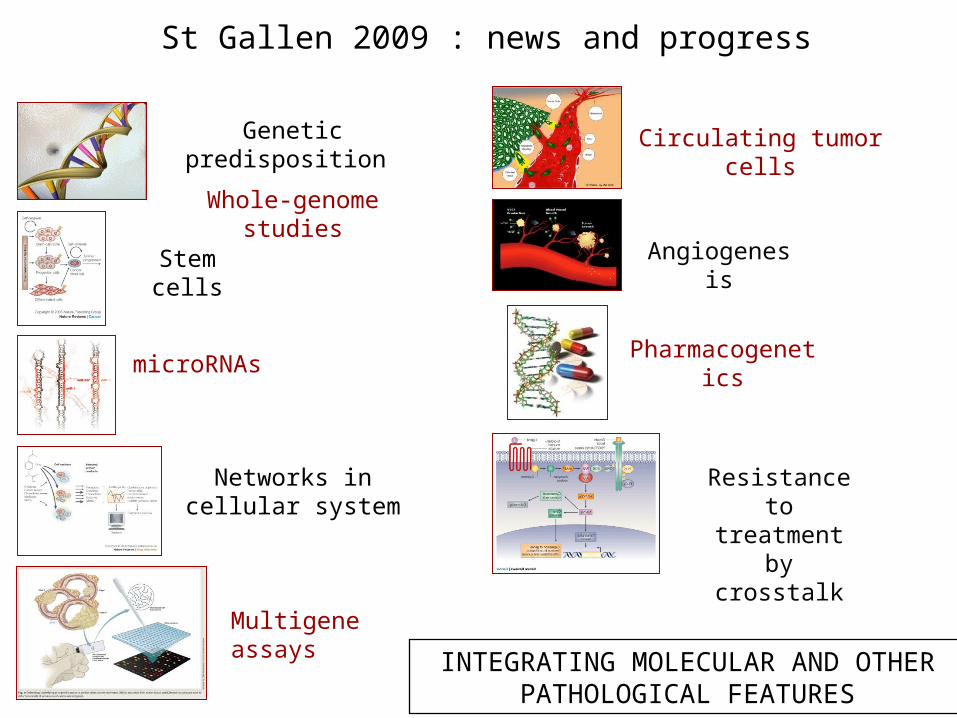
St Gallen 2009 : news and progress
INTEGRATING MOLECULAR AND OTHER PATHOLOGICAL FEATURES
Genetic predisposition
Whole-genome studies
Stem cells
microRNAs
Networks in cellular system
Circulating tumor cells
Angiogenesis
Pharmacogenetics
Resistance to treatment by
crosstalk
Multigene assays
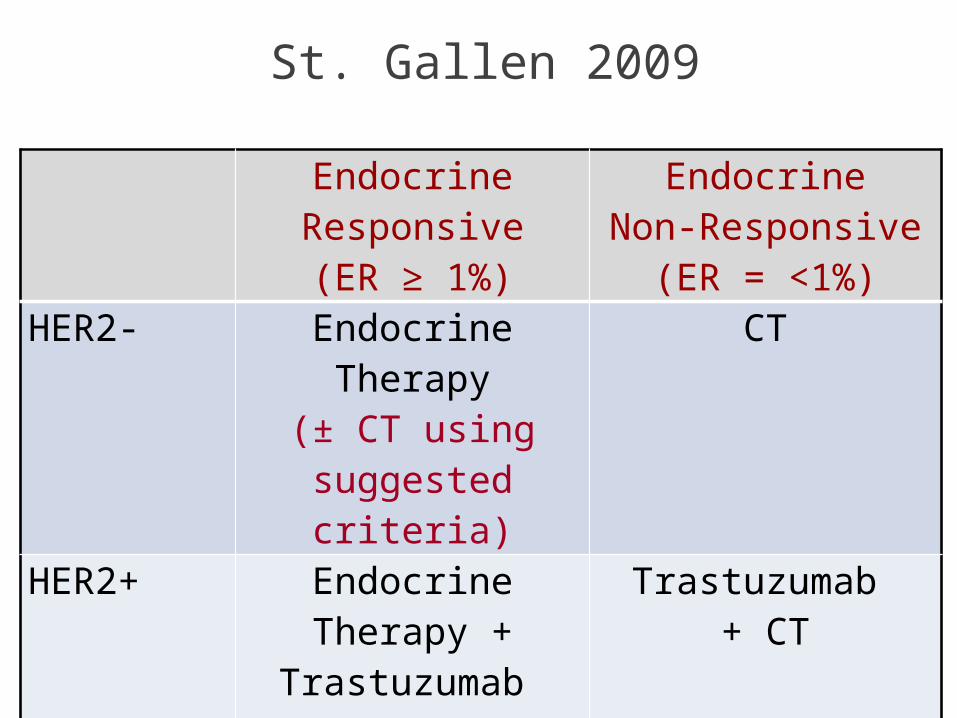
St. Gallen 2009
EndocrineResponsive(ER ≥ 1%)
EndocrineNon-Responsive
(ER = <1%)
HER2- Endocrine Therapy
(± CT using suggested criteria)
CT
HER2+ Endocrine Therapy +
Trastuzumab + CT
Trastuzumab + CT

St Gallen 2011
Focus on the identification of “tumor subtypes” to plan therapy
more accurately
Morphological evaluation of special histological types
Immunohistochemical characterization as molecular classification surrogate
Tumor Subtypes defined starting from molecular classification

Biology-driven trials
Andre F et al 2011 JCO

How can molecular tools help standard pathology?
Standardization, reproducibility & qualification
• Molecular sub-grouping
• Prognosis/Stratification
• Predictive markers
• Functional pathway read-outs

Molecular sub-grouping

….very distinct gene expression patterns irrespective of stage (size, nodal, status) !
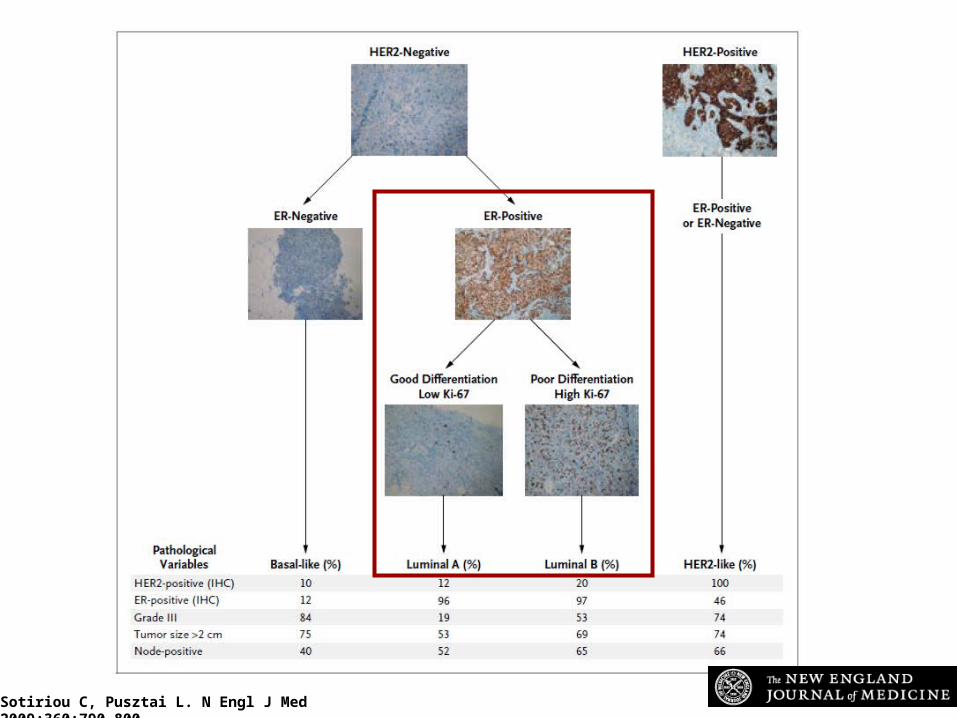
Sotiriou C, Pusztai L. N Engl J Med 2009;360:790-800
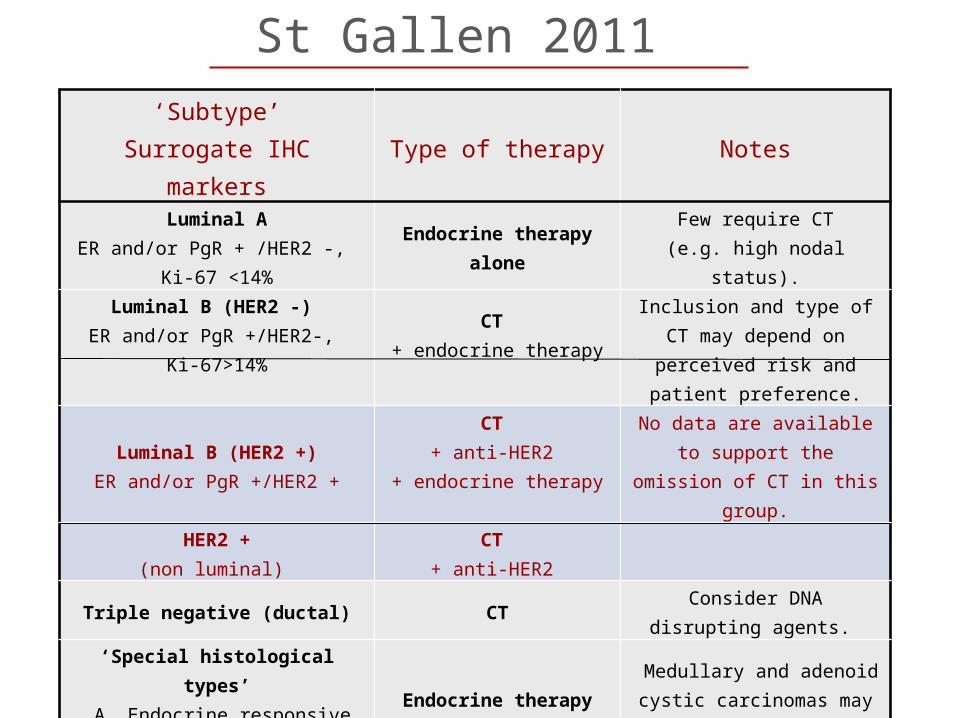
‘Subtype’Surrogate IHC markers
Type of therapy Notes
Luminal AER and/or PgR + /HER2 -,
Ki-67 <14%
Endocrine therapy alone
Few require CT(e.g. high nodal status).
Luminal B (HER2 -) ER and/or PgR +/HER2-,
Ki-67>14%
CT + endocrine therapy
Inclusion and type of CT may depend on perceived
risk and patient preference.
Luminal B (HER2 +)ER and/or PgR +/HER2 +
CT + anti-HER2
+ endocrine therapy
No data are available to support the omission of CT
in this group.
HER2 +(non luminal)
CT + anti-HER2
Triple negative (ductal) CTConsider DNA disrupting
agents.
‘Special histological types’ A. Endocrine responsive
B. Endocrine non responsive
Endocrine therapy
CT
Medullary and adenoid cystic carcinomas may not require any adjuvant CT.
St Gallen 2011

Ki67 (IHC)
British Journal of Cancer (2007)

Ki-67 prognostic cut-off point for all breast cancer subtypes (multivariate analysis)
The best cut-off point with the lowest p-value and highest HR was found at the Ki-67 index of 20%

Clinically, the majority of claudin-low tumors : are triple negative invasive ductal carcinomas with a high frequency of metaplastic and medullary differentiation. have a response rate to standard preoperative chemotherapy intermediate between that of basal-like and luminal
tumors. resembles the mammary epithelial stem cell.
Claudin-low breast cancer are characterized by: low to absent expression of luminal
differentiation markers, high enrichment for epithelial-to-
mesenchymal transition markers, immune response genes and cancer stem cell like features.
Prognosis/stratification

Breast cancer should be considered according to Hormonal Receptor, HER2, Ki-67
DistinctClinical
outcome
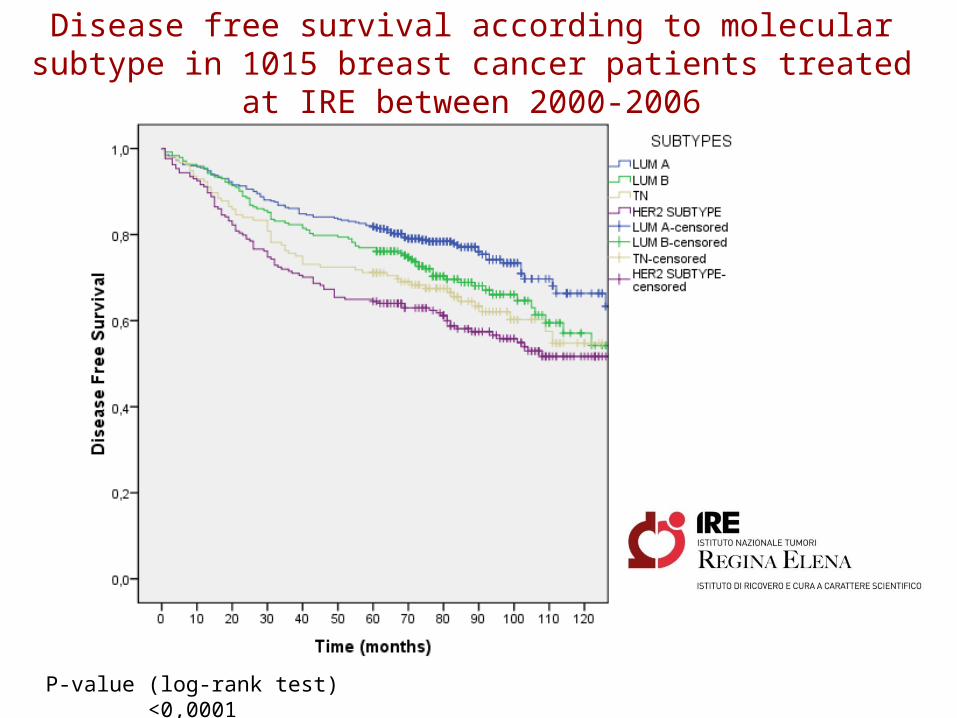
Disease free survival according to molecular subtype in 1015 breast cancer patients treated at IRE between
2000-2006
P-value (log-rank test) <0,0001

S Borgquist J Clin Pathol 2008;61:197-203
Estrogen receptors α and β show different associations to clinicopathological parameters and their co-expression might predict
a better response to endocrine treatment in breast cancer
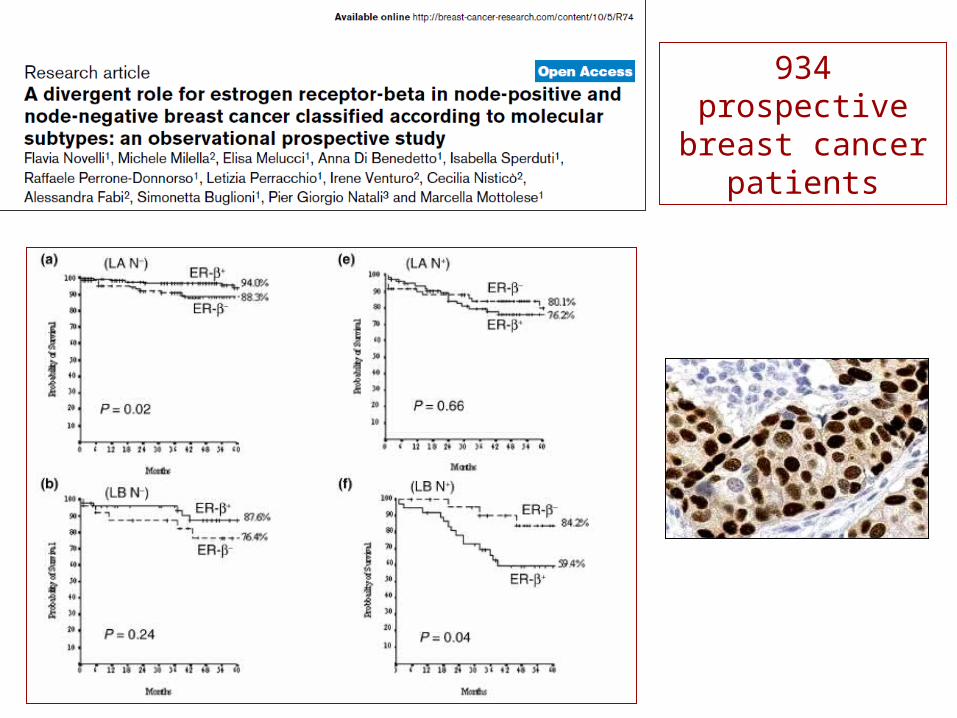
934 prospective breast cancer
patients
To replace or to complement the traditional biological parameters?
This may be highly misleading, because the molecular classes are heterogeneous and encompass different tumor types with different risk profiles and different responsiveness to the therapy

Not all the tumors with the basal-like profile are high risk tumors. This molecular class also includes:
low-grade metaplastic carcinomas
adenoid-cystic carcinomas,
medullary carcinomas
low grade apocrine carcinomas
Heterogeneity may be evident in breast cancer with basal-like profile since:
which have a very favorable prognosis

Predictive markers
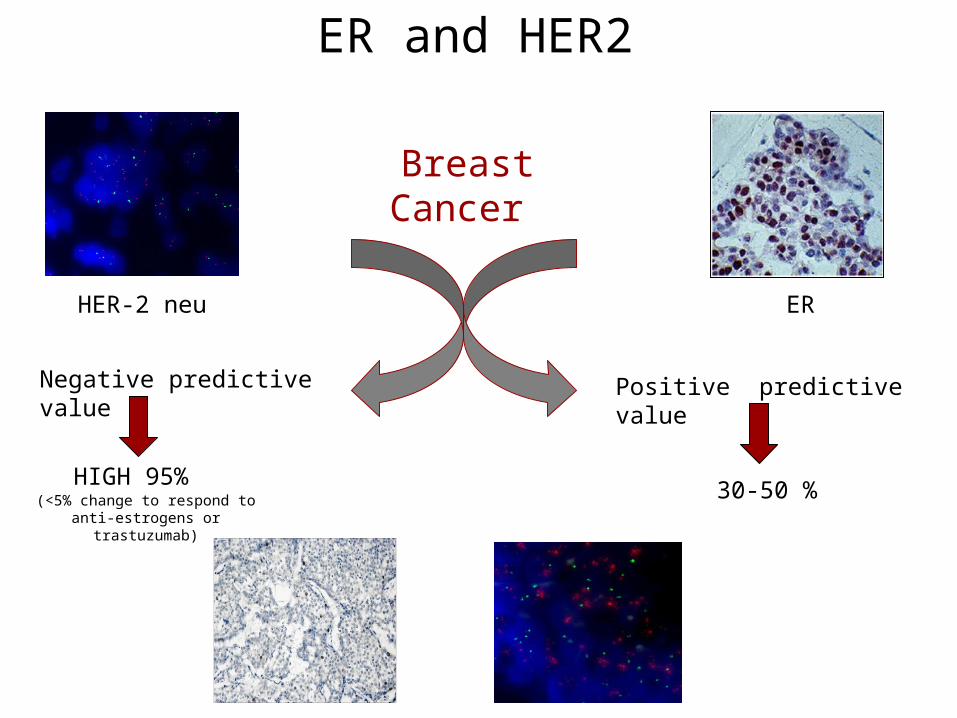
ER and HER2
Breast Cancer
HER-2 neu ER
Negative predictive value Positive predictive value
HIGH 95% 30-50 %(<5% change to respond to anti-estrogens or trastuzumab)
ab
30μ 30μ
a b
10μ
10μ
c d
b
What about geneExpression signatures ?
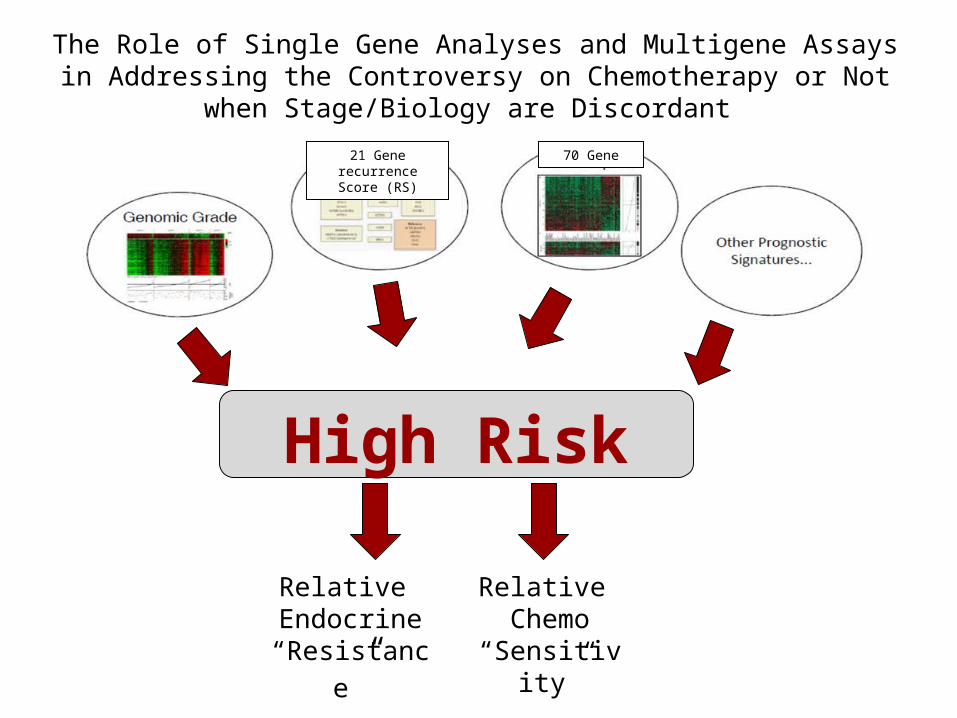
The Role of Single Gene Analyses and Multigene Assays in Addressing the Controversy on Chemotherapy or Not when
Stage/Biology are Discordant
High Risk
Relative Endocrine
“Resistance”
Relative Chemo
“Sensitivity”
21 Gene recurrence Score
(RS)
70 Gene

Three Strategies for the Development of a Gene-Expression Prognostic Signature
1. “top-down” approach: gene- expression data from patients with known clinical outcomes are compared to identify genes that are associated with prognosis without any a priori biologic assumption.2. “bottom-up” approach: gene-expression patterns associated with a specific biologic phenotype or a deregulated molecular pathway are first identified and then correlated with the clinical outcome.3. candidate-gene approach: selected genes of interest on the basis of existing biologic knowledge are combined into a multivariate predictive model.

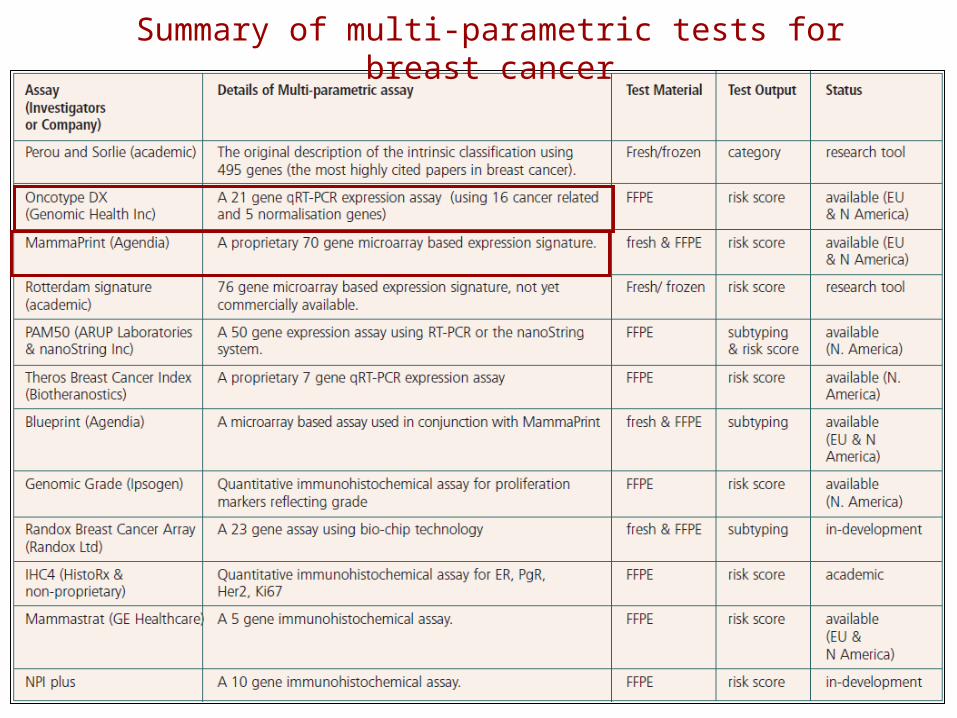
Summary of multi-parametric tests for breast cancer
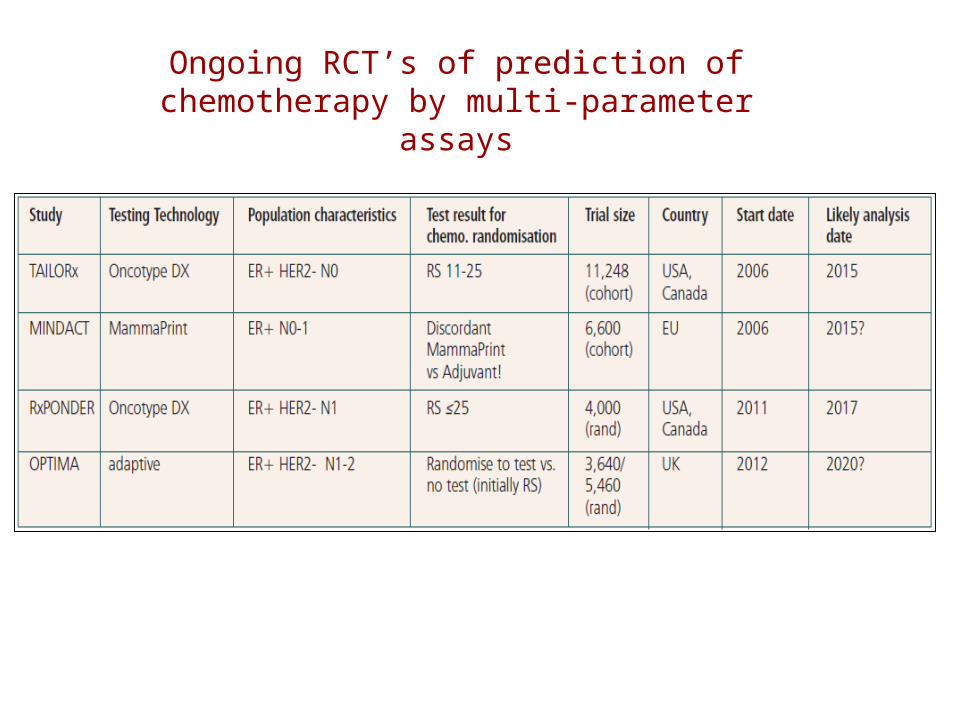
Ongoing RCT’s of prediction of chemotherapy by multi-parameter
assays

21 gene Recurrence Score Assay: Strongly Predictive in NSABP B-20 (ER+No)

Mammaprint TM adds prognostic information in pT1 tumors
N=965 patients wit T1a,b,c tumors; adjuvant systemic treatment in 41%; median 7 years
Distant Metastasis-Free Survival
PT1ab PT1c

T1A,BNoMo: ONCOTYPE DX and MAMMAPRINT
TM prolifiles

1 st generation signatures add prognostic information to current “best”clinical tools

Breast Cancer Gene Expression Signatures and Cell proliferation
70 gene signature van’t Veer et al,2002 70
Cell cycle, angiogenesis, invasion and metastasis
76 gene signatureWang et al, 2005 76
Cell cycle, proliferation, DNA repair, immune
response and apoptosis
OncotypeDX RSPaik et al, 2004 16
Proliferation, ER and HER2 invasion
Genomic grade indexSotiriou et al, 2006 97
Cell cycle and proliferation
44

Learning about adverse biological features of T1a,bNoMo breast cancers

47
Stromal Subtypes are Associated with Outcome
Stromal Gene Expression Identifies Distinct Tumor Subclasses
Epithelia Stroma
Stromal Clusters Reflect Different Microenvironments

48
The tumor microenviroment plays a key role in tumor progression
Better understanding of intra-tumor diversity and epithelial-stromal cell interactions will lead to more efficacious cancer
treatment

Functional Pathway

PI3K pathway gene signatures
Best way to develop these signatures

PIK3CA mutations produce characteristic change in
gene expression
The mutant and the associated gene signature
were associated with a good prognosis in
TAM- treated ER+/HER2- BC
Loi et al, PNAS 2010
A PIK3CA-GS developed from PIK3CA mutant ER+breast cancers

Unfavourable Biologic Profile (UBP≥3 ABF) versus
Favourable Biologic Profile (FBP<3 ABF)
121 breast cancer patients CMF treated
Novelli F, Mottolese M SABCS 2009
P-AKT PI3K Ki-67 HER2

A gene signatures may be useful as a functional read-out of pathway activity
TAKE MESSAGES
Gene signatures will probably be most useful in combination with genotype, ER, HER2, Ki-67
All predictive gene signatures need clinical validation in appropriate clinical trials