Cumulative probability of a false-positive screening ... · Cumulative probability of a...
56
MASTER’S THESIS Cumulative probability of a false-positive screening result in the Finnish breast cancer screening program Ilona Siljander Master’s thesis University of Helsinki Faculty of Science Department of Mathematics and Statistics August 2016
Transcript of Cumulative probability of a false-positive screening ... · Cumulative probability of a...

MASTER’S THESIS
Cumulative probability of a false-positivescreening result in the Finnish
breast cancer screening program
Ilona SiljanderMaster’s thesis
University of HelsinkiFaculty of Science
Department of Mathematics and StatisticsAugust 2016

Matemaattis-luonnontieteellinen Matematiikan ja tilastotieteen laitos
Ilona Siljander
Cumulative probability of a false-positive screening result in the Finnish breast cancerscreening program
Tilastotiede
Pro gradu -tutkielma Marraskuu 2016 56 s.
GEE, GLM, Monte Carlo simulation, Breast cancer screening, False-positive result
Kumpulan tiedekirjasto
Tässä pro gradu -tutkielmassa tutkitaan väärän positiivisen (FP) tuloksen kumulatiivista to-dennäköisyyttä Suomen 20-vuotisessa rintasyöpäseulonnassa. Tutkielmassa käytetään Suomenjoukkotarkastusrekisterin, Suomen Syöpärekisterin aineistoa, joka koostuu 50–51-vuotiaista vuosi-na 1992–1995 ensimmäisen seulontakutsun saaneista naisista.
Työn tilasto-osuudessa esitellään yleistettyjen lineaaristen mallien ja yleistettyjen estimoin-tiyhtälöiden teoriaa. Kumulatiivisen todennäköisyyden mallintamiseen käytetään yleistettyjäestimointiyhtälöitä (GEE), joilla mallinnetaan yksittäisen mammografian FP-tuloksen todennäköi-syyttä. Tästä lasketaan kumulatiivinen todennäköisyys käyttämällä ehdollisen todennäköisyydenkaavoja. Mallinnus huomioi erityisesti sen, että yksittäiset mittaustulokset eivät ole toisistaanriippumattomia. Luottamusvälien (Lv) laskemiseen käytetään GEE-estimaattien asymptoottiseenjakaumaan perustuvaa Monte Carlo -simulointia.
Lopputuloksena kumulatiivisen todennäköisyyden arvo oli 15.84 % (95 % Lv: 15.49–16.18 %).Aiemman FP-tuloksen todettiin lisäävän uuden FP-tuloksen riskiä: yhdellä aiemmalla, odds ratio(OR) 1.91 (95 % Lv: 1.78–2.04) ja usealla aiemmalla OR 3.09 (95 % Lv: 2.49–3.83). Lisäksiepäsäännöllinen seulontoihin osallistuminen lisäsi FP-tuloksen riskiä OR 1.46 (95 % Lv: 1.37–1.56).
The purpose of this thesis is to study the cumulative probability of a false-positive (FP) test resultduring the Finnish 20-year breast cancer screening program. This study is based on breast cancerscreening data provided by the Mass Screening Registry of the Finnish Cancer Registry, whichconsists of women aged 50–51 years at the time of their first invitation to mammography screeningin 1992–1995.
Generalized estimating equations (GEE) are used to estimate the cumulative probability of aFP screening result. In the theoretical part we present the corresponding theory together withreviewing the theory of generalized linear models (GLM). The cumulative probabilities are calcula-ted from the modeling of individual examinations by using the theory and formulas of conditionalprobability. The confidence intervals (Cl) are calculated by using Monte Carlo simulation relyingon the asymptotic properties of the GEE estimates.
The estimated cumulative risk of at least one FP during the screening program was 15.84% (95%Cl: 15.49–16.18%). Previous FP findings increased the risk of (another) FP results with an oddsratio (OR) of 1.91 (95% Cl: 1.78–2.04), and OR 3.09 (95% Cl: 2.49–3.83) for one or more previousFP results, respectively. Irregular screening attendance increased the risk of FP results with an ORof 1.46 (95% Cl: 1.37–1.56).
Tiedekunta/Osasto — Fakultet/Sektion — Faculty Laitos — Institution — Department
Tekijä — Författare — Author
Työn nimi — Arbetets titel — Title
Oppiaine — Läroämne — Subject
Työn laji — Arbetets art — Level Aika — Datum — Month and year Sivumäärä — Sidoantal — Number of pages
Tiivistelmä — Referat — Abstract
Avainsanat — Nyckelord — Keywords
Säilytyspaikka — Förvaringsställe — Where deposited
Muita tietoja — Övriga uppgifter — Additional information
HELSINGIN YLIOPISTO — HELSINGFORS UNIVERSITET — UNIVERSITY OF HELSINKI

Contents
1 Introduction 4
2 Background 5
2.1 Process of breast cancer screening and setting . . . . . . . . . . . . 5
2.2 Benefits and harms of screening . . . . . . . . . . . . . . . . . . . 6
2.3 An overview of false-positive screening result . . . . . . . . . . . . 7
2.4 Methods used estimating cumulative probability . . . . . . . . . . . 8
2.5 Study population . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
2.6 Definitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
3 Statistical methods 13
3.1 Generalized linear model . . . . . . . . . . . . . . . . . . . . . . . 13
3.1.1 Preliminaries . . . . . . . . . . . . . . . . . . . . . . . . . 13
3.1.2 The exponential family . . . . . . . . . . . . . . . . . . . . 14
3.1.3 Linear predictor . . . . . . . . . . . . . . . . . . . . . . . . 17
3.1.4 Link function . . . . . . . . . . . . . . . . . . . . . . . . . 17
3.1.5 Likelihood equation and asymptotic distribution for GLM . 18
3.2 Generalized estimating equations . . . . . . . . . . . . . . . . . . . 19
3.2.1 Parameter estimation . . . . . . . . . . . . . . . . . . . . . 20
3.2.2 Sandwich estimator . . . . . . . . . . . . . . . . . . . . . . 22
3.2.3 Correlation matrix . . . . . . . . . . . . . . . . . . . . . . 23
3.3 Cumulative probability . . . . . . . . . . . . . . . . . . . . . . . . 24
3.4 Confidence intervals . . . . . . . . . . . . . . . . . . . . . . . . . 27
4 Analysis 30
4.1 Data description . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
4.2 Modeling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
4.2.1 The validity of specifying previous FP and regularity of theattendance as categorical variables . . . . . . . . . . . . . . 36
4.2.2 The relation between the age and the probability of FP result 38
2

4.2.3 The capability of the model to explain the typical behaviorfor each combination of age, previous FP and regularity ofthe attendance . . . . . . . . . . . . . . . . . . . . . . . . . 41
4.2.4 Variability of the data . . . . . . . . . . . . . . . . . . . . . 43
5 Results 46
6 Discussion and conclusion 49
References 55
3

1 Introduction
A false-positive result represents disadvantage in a population-based mammographyscreening program. In this study we estimate the cumulative risk of at least one false-positive (FP) mammography test result during 10 biennial screening examinationsfor women aged between 50 to 69 years.
A retrospective cohort study was performed for 84, 475 women aged 50–51 yearsat the time of their first invitation to mammography screening in 1992–1995. Thesewomen underwent altogether 477, 047 screening mammograms in the Finnish 20-year breast cancer screening program. The attendance rate overall in the cohort groupwas 88.4% during the screening program.
Generalized estimating equations (GEE) were used to estimate the cumulative prob-ability of a false-positive screening result. The cumulative risk was calculated fromthe parameters estimates by using simple probability theory. We studied the e�ect ofage, previous FP result and regularity of the women attending the screening roundson obtaining (another) FP test result. The 95% confidence intervals for the risk ofa false-positive screening result at each age group was estimated using a suitablemodification of bootstrapping.
Out of all screenings 2.8% were recalled for further examinations and of these82.0% were false-positive results. The estimated cumulative risk of at least oneFP result during the screening program was 15.84% among the attendees (95% CI:15.49–16.18%). Out o� the whole study population 12.3% received at least one false-positive screening result. In addition, age, regularity of attendance and a previous FPwere used to model the risk of an FP. The odds ratios were 0.61, 1.46, respectively,as well as 1.91 and 3.09 for one or more previous FPs.
Approximately one in every six women will be recalled for further examinationswith at least one negative outcome, provided they attend the biennial mammographyscreenings between ages 50 to 69 years. Irregular screening attendance and previousFP findings increased the risk of (another) FP test result. False-positive results inmammography screening are a disadvantage in a breast cancer screening program.Understanding the burden of false-positive results to the target population helps inanalyzing the viability of the screening program.
4

2 Background
Organized screening means cancer screening programs with a systematic, population-based approach with quality assurance at all appropriate levels (EU Council, 2003).The main goal of organized cancer screening is to reduce the mortality throughthe early detection of the disease (IARC, 2002). However, screening provides bothbenefits and harms. Therefore, benefits of screening must be weighted against itsdisadvantages.
Recall for assessments after mammography screening without detecting breast canceris referred to as a false-positive screening result, which is considered a disadvantageof screening. In this work, we concentrate on false-positive (FP) screening test result,which may cause psychological harms, increased hospital visits, increased diagnostictests as well as increased radiation exposure and additional costs. The cumulativeprobability of a false positive screening test result is defined as woman experiencingat least one FP screening result after certain time period defined beforehand.
An accurate estimation of the cumulative probability of FP screening test results,from the long running screening programs, is important for program evaluation(Hubbard et al., 2010). Life-time risk of di�erent screening outcomes, includingscreen-detected cancers and false-positive results have been estimated after multiplescreening rounds to study the e�ectiveness of screening program (Otten et al., 2013).Moreover, the psychological harms can also be reduced by suitable informing ofindividuals undergoing organized population based screening, regarding what theyshould expect from testing over time (Hubbard et al., 2010).
In the next sections we present the overall process of breast cancer screening andsetting in Finland. There will be a brief overview about the benefits and disadvantagesof cancer screening overall. Furthermore, we concentrate on the disadvantages of afalse-positive screening result and present an overview on the earlier studies about therisk of receiving a false-positive screening test result. In addition, we discuss brieflyabout the methods used in estimating the cumulative risk of receiving a false-positiveresult. Finally we will describe the study population and define the concepts used inthe study and analysis.
2.1 Process of breast cancer screening and setting
In Finland, the population-based breast cancer screening program, administered bythe Finnish Cancer Registry (FCR), started in 1987 (FCR, 2010). It is based on theGovernment Decree on Screenings 1339/2006 (Ministry of Social A�airs and Health,2006). According to the Ministry of Social A�airs and Health (2006), populationbased breast cancer screening is to be o�ered free of charge by the municipalitiesto women between 50–69 years every 2 years. Screening is part of the preventive
5

health care and means examination of the population, certain part of the populationor sampling, in order to discover a certain disease, its precursor, or to identify apathogen (Ministry of Social A�airs and Health, 2006).
Based on the FCR (2010), a personal invitation letter is sent by mail with a prefixedtime and place of screening as well as the results of the mammogram afterwards.All women in the target age are invited. Breasts are examined by mammography.Two radiologists will interpret the results. Women with positive results, or womenrecommended for further assessment, are recalled for further examination (FCR,2010). The program is administered according to the European guidelines (Perryet al., 2006).
This study is based on breast cancer screening data provided by the Mass ScreeningRegistry of the Finnish Cancer Registry. The Mass Screening Registry providesinformation about the name and address of women to be invited for the screening unitsregularly (FCR, 2010). Stated by FCR (2010), screening units receive informationabout the age groups that are included in the screening program in each year. Theinformation about the name and address of women are gathered from the PopulationRegister Centre.
According to the FCR (2010), the data about the invitations and the screeningmammogram examinations are stored in the Mass Screening Registry at the FinnishCancer Registry. The Registry maintains the database for breast cancer screeningand it provides the annual statistics about the breast cancer screening. In addition,the Registry evaluates the impact of screening on mortality and the quality of thescreening program.
2.2 Benefits and harms of screening
Positive e�ects of screening have been largely studied and well established. Preven-tion of disease-specific mortality is the main aim of cancer screening (IARC, 2002).Earlier diagnosis may improve the outcome of the treatment reducing disease-specificmortality and increase the treatment options such as breast-conserving therapy.The organized mammography screening in Finland has been studied to be e�ective(Sarkeala et al., 2008b). The incidence-based mortality from breast cancer has beenreported to reduce approximately by 22–28% among the invited women (Sarkealaet al., 2008a).
Screening can have various disadvantages. The most important harms of screeningare due to the adverse events of the diagnosis and management of cancer. This isrelated to overdiagnosis, overtreatment and treatment related complications (Pulitiet al., 2012; Heinävaara et al., 2014; Lauby-Secretan et al., 2015; Harris et al., 2014).Most reliable estimates indicate overdiagnosis of approximately 1–10% among allinvited (Puliti et al., 2012).
Various psychological harms may occur during the screening process, including
6

pain from the screening test, confirmation and information about the test result. Lowdiagnostic specificity and false-positive test results can increase adverse psychosocialconsequences (Brett et al., 2005). False-positive results in screening process areinevitable in breast cancer screening and therefore it needs to be endured to someextent. It is important to keep the further assessment rate as low as possible withoutmissing breast cancer cases.
2.3 An overview of false-positive screening result
The negative e�ects of false-positive screening results have been widely studied.False-positive results increase the psychological harms (Brodersen and Siersma,2013; Bond et al., 2013). Recalls increase additional hospital visits, diagnostic tests,radiation exposure and additional costs (Lerman et al., 1991; Bull and Campbell,1991; Harris et al., 2014). False-positive screening result may also lead to decreasedparticipation in future screening rounds (Salz et al., 2011).
The risk of a false-positive test result is influenced by the screening procedures, suchas screening interval, single versus double reading by radiologist, the method howscreening tests are performed, training and the experience of the radiologist (Romanet al., 2014). In addition, characteristics of the women, such as age, screening history,use of hormone therapy, breast density and previous invasive procedures are prone toimpact the risk for false-positive screening test result (Roman et al., 2014). Indeed,dense breast tissue makes it more di�cult to detect the possible cancer. Women withdense breast tissue are most likely to be younger at age. Therefore younger womenhave more increased risk of receiving FP screening result.
A population based study in Spain (Castells et al., 2006) stated that factors asso-ciated with a higher cumulative risk of false-positive recall were previous benignbreast disease, premenopausal status, body mass index above 27, 3 and age 50–54years. Another study from the USA (Christiansen et al., 2000) states that previousbreast biopsies, number of previous breast biopsies, family history of breast cancer,premenopausal status and hormonal therapy were all associated with higher proba-bility of false-positive mammograms. Contrary to Castells et al. (2006), Christiansenet al. (2000) found that BMI was not statistically significant factor contributing tothe higher risk of FP result.
In Europe, the cumulative risk of a false-positive screening result after 10 biennialscreening rounds has been estimated to be 19.7% (Hofvind et al., 2012) and inthe U.S. the cumulative risk of a false-positive test result after 10 years of biennialscreening has been reported higher ranging from 41.6% to 49.1% (Elmore et al.,1998; Christiansen et al., 2000; Hubbard et al., 2011).
The overall cumulative risk of a false-positive screening test for all centers in Norwe-gian breast cancer screening program was 20% (95% Cl: 19.7–20.4%) (Roman et al.,2013) by using generalized linear mixed models (GLMM) for estimation with theregularity of attendance as the explanatory variable. Roman et al. (2013) found that
7

irregular screening attendees had a higher risk of receiving FP screening test resultwith odds ratio 1.12 (95% Cl: 1.06–1.20%). In Spain the cumulative false-positiverisk was estimated at 20.39% (95% Cl: 20.02–20.76%) by using the same regressionmodel as was used in the Norwegian study (Roman et al., 2012). In addition, a studyfrom Denmark, Njor et al. (2007) demonstrated that after completing 3–5 screen-ing rounds, the extrapolated cumulative risk of false-positive test over a program of10 screening rounds was predicted to be 15.8% for a woman participating in theprogram.
2.4 Methods used estimating cumulative probability
In an international level the calculation methods for cumulative probability varyacross the countries. Example studies are gathered in a Table 2.1 to describe thedi�erent methods used in estimating the cumulative probability of FP results.
Estimating the cumulative risk of FP with particular model is challenging because ofthe di�erences between the programs, screening population, radiologist interpretationdi�erences and resources (Hubbard et al., 2010). The estimation is also di�cultwithin the country itself. In Finland, even though the breast cancer screening is basedon government law, the process still varies between the municipalities, some invitingmore extensively than others. The estimation is also challenging due to the fact, thatnot all individuals receive the intended screening examinations due to non-adherenceor drop-outs.
Hubbard et al. (2010) bring up another challenging issue concerning the estima-tion of FP results. Since not all subject will attend all the recommended screeningrounds, nor will receive all the intended invitations, it results in right censoring ofscreening round. Hubbard et al. (2010) studied statistical methods used in estimatingthe cumulative risk of a false-positive screening test result. They discovered twoapproaches used in the estimation: conditional approaches and marginal approaches.Conditional probabilities estimate the risk of an FP result for the subdatasets, forwomen who attend certain number of screening rounds, relying on the assumptionthat the probability of an FP result at each screening round is independent of thetotal number of screening rounds attended. Contrary to conditional approach, themarginal approach relies on the assumption that the probability of a first FP result ateach screening round is constant after censoring (Hubbard et al., 2010).
We use conditional probability approach to estimate the cumulative risk of an FPscreening result conditional on age, attendance, previous FP result and regularityof attendance. We are estimating the probability that after undergoing j screeningexaminations, the subject has received at least one FP test result. In addition, weare interested on how certain characteristics, such as a woman receiving several FPresults and regularity of attending the screening program influence the FP probability.These are the same variables used by Baker et al. (2003) and Roman et al. (2013)respectively.
8

The question of calculating the cumulative probability has been previously studiedfor instance by Baker et al. (2003) and Gelfand and Wang (2000). For a morecomprehensive review of the methodological aspects we refer to Hubbard et al.(2010).
In this study we use generalized estimating equations (GEE) to model the probabilityof an FP test result, as a basis for calculating the cumulative probability. Indeed, asingle probability is modeled using GEE. Cumulative probability is then countedfrom single cases as it has been done in previous studies by using simple probabilitytheory. Various methods have been used to calculate the confidence intervals. Weuse a suitable modification of standard bootstrapping.
We use GEE because it allows for within subject correlations between observations.GEE is a robust method for a longitudinal epidemiological study and it seems rea-sonable choice for the problem in hand. Previous studies (Roman et al., 2012, 2013;Hubbard et al., 2011; Christiansen et al., 2000) have used, for instance, Bayesian orGLMM methods, and for a further overview of the methodology we refer to Table 2.1.
9

Table
2.1.Su
mm
ary
ofstu
dies
perfo
rmed
toes
timat
eth
ecu
mul
ativ
epr
obab
ility
ofa
FPsc
reen
ing
resu
lt.
Coun
tryPo
pula
tion
Age
grou
pSc
reen
Inte
rval
Obs
erve
dsc
reen
ing
roun
ds
Scre
enin
gro
unds
estim
ated
Cum
ulat
ive
risk
ofFP
Met
hod
Refe
renc
e
Euro
pe36
4,99
150
–69
1019
.7%
�N
ote*
†(H
ofvi
ndet
al.,
2012
)N
orw
ay23
1,31
050
–69
26
§10
20%
GLM
M¶
(Rom
anet
al.,
2013
)Sp
ain
1,56
5,36
445
–69
26
§10
20.3
9%G
LMM
¶(R
oman
etal
.,20
12)
Den
mar
k21
,261
†50
–69
25
§10
15.8
%N
ote*
†(N
jore
tal.,
2007
)9,
039‡
50–6
92
5§
108.
1%N
ote*
†(N
jore
tal.,
2007
)Ita
ly28
,500
50–6
92
7§
715
.2%
(Pul
itiet
al.,
2011
)U
SA††
169,
456
40–5
92
1310
41.6
%‡‡
GLM
M¶
(Hub
bard
etal
.,20
11)
2,40
0�40
–69
29
1049
.1%
MCM
C��(E
lmor
eet
al.,
1998
)2,
227�
40–6
99
943
.1%
Baye
sian
(Chr
istia
nsen
etal
.,20
00)
� Poo
led
estim
ate
base
don
thre
estu
dies
(Hof
vind
etal
.,20
04;N
jore
tal.,
2007
;Sal
aset
al.,
2011
).† C
open
hage
n‡ Fyn
� Bos
ton
††7
mam
mog
raph
yre
gistr
ies
§ Val
uesf
orre
stof
the
scre
enin
gro
unds
are
base
don
the
last
obse
rved
scre
enin
gro
und.
‡‡41.6
%w
ithbi
enni
alsc
reen
ing
and
61.3
%w
ithan
nual
scre
enin
g.¶ G
ener
alise
dlin
earm
ixed
mod
el(G
reen
woo
d’sa
ppro
xim
atio
nfo
rCls)
��M
arko
vCh
ain
Mon
teCa
rlovi
aG
ibbs
sam
pler
tosa
mpl
efro
mth
epo
sterio
rdist
ribut
ion
(Gel
fand
and
Smith
,199
0)*† E
stim
atio
nus
edby
Hof
vind
(Hof
vind
etal
.,20
04)
10

2.5 Study population
The study population included 84, 475 women aged 50–51 years at the time of theirfirst mammography invitation in 1992–1995. The women are identified by a uniquepersonal identification number given to all citizens in Finland. Information aboutthe invitations, attendance, further examinations and screening outcome is registeredin the Finnish Mass Screening Registry database, with the personal identificationnumber used as identifier for each woman.
The breast cancer screening is administered by digital mammography. Finnish breastcancer screening program uses independent double reading by radiologists. An in-terpretation is given for both breasts from both readers by scoring. Score ranges from0 to 5. A score 0 indicates test failure, 1 a normal screening result and 5 is highlysuspicious for malignancy. If the result indicates malignancy, the woman is recom-mended for further assessment and she receives an invitation for further examinationor referral for surgical procedure.
Further examination covers additional mammography, clinical breast examination,ultrasound, pneumocystography or fine-needle/core-needle biopsy. Surgical proce-dure covers lumpectomy or partial/radical mastectomy. If no malignancy is found,women are referred back to routine screening. All malignancies, invasive or ductalcarcinoma in situ, are histologically verified. Women who receive a diagnosis ofbreast cancer are referred for treatment.
2.6 Definitions
Recall is defined as woman receiving an invitation for further examinations. In thisrespect further examination procedures can be classified as additional mammography,ultrasound, pneumocystography or biopsy. Referral is defined as woman receivingan invitation for surgical procedure.
Positive diagnostic finding is classified as true positive if breast cancer (invasive orductal carcinoma in situ) is diagnosed in the woman on the basis of histologicalfindings.
The outcome of mammography screening examination is defined as a false-positivetest result, normal test result or true positive test result. In this study, a screening testwas defined as false-positive test result if a woman attended the screening test andwas recalled or referred for further assessment without being diagnosed with eitherinvasive carcinoma or ductal carcinoma in situ. Any recall or referral for furtherassessments was considered a false-positive screening result if breast cancer was notdiagnosed during the diagnostic workup, regardless of the procedures performed.
We also examined whether there was independence between the outcomes of subse-quent screens as in if the probability of woman receiving a FP result influenced thefact whether the woman already had a previous FP result. Therefore we identified a
11

variable of previous FP result as well.
Previous FP was also studied as accumulated factor, meaning that women weredivided into three groups, whether they had no FP results, one previous FP results ormore than one previous FP result during the screening program.
Regularity of the attendance was used to model the risk of an FP screening result.Woman was considered an irregular attendee at those screening rounds when shehad missed her last screening examination, meaning that there were �3.5 years(42 months) in between the screening rounds. See more specific definitions for thevariables used in the model in the section 3.3.
The cumulative risk of a false-positive screening result is defined as the risk ofexperiencing at least one false-positive test result in the biennial 20-year screeningprogram. The estimates of the cumulative probability of having a false-positive testresult was calculated by using formula provided in the section 3.3.
12

3 Statistical methods
We start by introducing the generalized linear model (GLM). First we will present theelements of GLM in more detail together with the likelihood equation and asymp-totic distribution for GLM. Furthermore, we will follow the GLM with generalizedestimating equations (GEE). We will address the specific elements of GEE method,including asymptotic behavior, sandwich estimator and corresponding correlationmatrix.
In the last two sections we introduce the calculation for the cumulative probabilityand calculation method based on bootstrapping argument for the confidence intervals.
3.1 Generalized linear model
This section is based on Agresti (2015), Fitzmaurice et al. (2012) and Hardin (2005).
3.1.1 Preliminaries
Given a dataset (yi
, xi
)n
i=1 our aim is to build a model which explains the e�ect of theindependent variables x on the studied dependent variable y. In the standard linearmodel, one studies the model
yi
= x
0i
� + "i
, i = 1, 2, . . . , n,for
x
i
=
*.....,
1x
i1...
x
ip
+/////-, � =
*.....,
�1�2...�
p
+/////-,
and for the error "i
, i = 1, 2, . . . , n, where the aim is to determine the coe�cientvector �.
In the generalized linear model (GLM) the relation between the response and inde-pendent variables is not necessarily linear, and thus one introduces an additional linkfunction to describe the modeled relation. In this setting, it is also more natural tomodel the mean E(y
i
|xi
) instead of the true value with some error, as above.Definition 3.1. The generalized linear model is defined via the following threeelements:
1. a probability distribution of the response variable y from the exponentialfamily:
(3.1) f (yi
; ✓i
, �) = exp y
i
✓i
� b(✓i
)a(�)
+ c(yi
, �)!
;
13

2. a linear predictor ⌘ = X�;3. a link function g such that
(3.2) g⇥E(y|X)
⇤= ⌘,
where in (3.2) we have abused the notation as on the left hand side the functiong : R! R is to be interpreted as acting on the components of the vector E(y|X).
The first element is the assumption of the distribution. GLMs are an extended familyof probability models for a univariate response variable y
i
. For each element i inthe dataset, we have a particular distribution depending on ✓
i
, where ✓i
is typicallydetermined via the data x
i
. This relation can also be seen in (3.2), as we will laterexplain.
The exponential family includes the normal distribution for a continuous response,binomial distribution for binary response, and the Poisson distribution for counts.In addition, it also includes several other distributions, such as gamma, beta andnegative binomial distribution.
Each element ⌘j
of the linear predictor is a function of the observed independentvariables x
j
of the j’th element in the dataset (xi
)n
i=1. Given the observed dataset
X =*..,
x11 . . . x1p
......
x
n1 . . . x
np
+//-=*..,x
01...
x
0n
+//-
we obtain the linear predictor ⌘ = X� which is then used to obtain the fitted valuefor the mean of the random component y = (y1, . . . , yn
)0 via the model (3.2). Unlikeearlier, here y is now a random variable corresponding to the response variable, andin particular, it is not observed in the dataset. (Agresti, 2015, 2–4.)
3.1.2 The exponential family
All distributions that belong to the exponential family can be expressed in the samegeneral form (3.1), where ✓ is the location parameter (natural parameter), a is knownas prior weight and � is a scale or dispersion parameter. Although the probabilitydistributions have quite di�erent data types, such as continuous, dichotomous andcount, the members of the distributions have much in common. The function c ismerely a normalization constant. Indeed, for f to be a probability distribution, itsintegral need to equal 1. As the distribution may vary with �, we let the normalizationconstant to depend on this parameter.
The location parameter ✓ is closely related to the mean of the distribution and � isrelated to the variance of the exponential distributions. For some distributions � isconstant and does not require estimation. When � is known, y has one-parameterdistribution. However for some distributions, � is unknown parameter and while � isunknown, it has two-parameter distribution.
14

Example 3.1. Recall that the probability density function of the normal distributionis
(3.3) f (y; µ,�2) =1p
2⇡�2exp
� (y � µ)2
2�2
!,
which can be written as
(3.4)
f (y; µ,�2) = expf� 1
2 log�2⇡�2�g · exp
"� (y � µ)2
2�2
#
= exp"� y
2 � 2yµ + µ2
2�2 � log(2⇡�2)2
#
= exp266664yµ � 1
2 µ2
�2 � 12
y2
�2 + log(2⇡�2)!377775 .
From this representation we observe that the normal distribution is a member of theexponential family, with the canonical location parameter ✓ = µ and the dispersionparameter � = �2. These correspond to the mean and the variance. Indeed, bychoosing a(�) = � as well as
(3.5) b(✓) = 12 ✓
2 = 12 µ
2
and
(3.6)c(y, �) = �1
2
"y2
�+ log(2⇡�)
#
= �12
"y2
�2 + log(2⇡�2)#,
we immediately see that (3.4) is of the form (3.1).
For the sake of completeness, we next calculate the mean and variance of y in thissetting. For f defined in (3.1) we have
15

(3.7)
E✓
"@
@✓log f (y; ✓)
#= E✓
266664@@✓ f (y; ✓)
f (y; ✓)
377775=
1Z
�1
@@✓ f (y; ✓)
f (y; ✓)f (y; ✓)dy
=
1Z
�1
@
@✓f (y; ✓)dy
=@
@✓
1Z
�1
f (y; ✓)dy =@
@✓1 = 0,
provided f is di�erentiable and regular enough for the above change of the orderof integration and di�erentiation to be justified. Here we also used the fact, that thetotal mass of the probability density function is 1.
Since
(3.8) @
@✓log f (y; ✓, �) =
@
@✓
"y✓
a(�)� b(✓)
a(�)
#=
y
a(�)� b
0(✓)a(�)
,
we obtain that
(3.9) µde f
= E✓ (y) = b
0(✓).
Similarly for the variance we have
(3.10) @2
@✓2log f (y; ✓, �) = �b
00(✓)a(�)
.
By using the standard properties of the Fisher information we obtain
�E✓"@2
@✓2log f (y; ✓, �)
#= E✓
266664 @
@✓log f (y; ✓, �)
!2377775 .This together with (3.9) implies
(3.11)
b
00(✓)a(�)
= �E✓"@2
@✓2log f (y, ✓, �)
#= E✓
266664 @
@✓log f (y; ✓, �)
!2377775= E✓
266664 y � b
0(✓)a(�)
!2377775 =E
⇥(y � µ)2⇤
a(�)2 =Var(y)a(�)2 .
Finally, we obtain
(3.12) Var(y) = b
00(✓)a(�),
where b
00(✓) is called the variance function. It describes how the variance relates tothe mean parameter ✓. (Agresti, 2015, 120–123.)
16

3.1.3 Linear predictor
The second element is the linear predictor. The linear predictor specifies the e�ectsof the covariates x
i
on the mean of yi
and it is expressed as
(3.13) ⌘i
= �1x
i1 + �2x
i2 + · · · + �p
x
ip
=
pX
j=1�
j
x
i j
= x
0i
�.
The linear predictor is a linear combination of the unknown vector of regressioncoe�cients � = (�1, . . . , �p
)0, and the vector of covariates x
i
. The objective ofthe statistical analysis is to determine an estimate for the regression coe�cient �.(Agresti, 2015, 123.)
3.1.4 Link function
The last element is the link function. The link function connects the random compo-nent and linear predictor of the GLM. It describes the relation between E(y|X) andthe linear predictor ⌘. The link function is a known function g(·), which is predeter-mined in the model specifications. Now the random and systematic components aredirectly related via
(3.14) g⇥E(y
i
|X)⇤= g
⇥E(y
i
|xi
)⇤= ⌘
i
= x
0i
�.
In the sequel, we will denote µi
de f
= E(yi
|xi
).
Example 3.2. The standard linear regression model can be represented as a GLMby choosing the identity link function g(µ
i
) = µi
.
In principle, any function g(·) can be chosen to link the mean of the yi
to the linearpredictor. However, every distribution that belongs to the exponential family has aspecial link function called the canonical link. The canonical link function is definedas
(3.15) g(µi
) = ✓i
,
where ✓i
is the canonical location parameter ✓i
=P
p
j=1 � j
x
i j
= ⌘i
. The link functionrelates the mean of y
i
to the linear predictor and determines the scale on which theadditive e�ects of covariates have an impact on the mean response. The link functionhas no other limitations except, that it is monotone and di�erentiable. (Fitzmauriceet al., 2012, 327–335.) and (Agresti, 2015, 123.)
17

3.1.5 Likelihood equation and asymptotic distribution for GLM
The parameter � can be estimated using maximum likelihood. By maximizing thelikelihood function, the method is bound to choose values of the coe�cients that aremost likely to have generated from the data. In GLM the response is assumed to havea distribution belonging to the aforementioned exponential family of distributions.Recall that for independent observations y1, . . . , yn
the likelihood function is definedas
L(✓ | y)de f
=
nY
j=1f✓ (y j
)
where f is a continuos probability distribution with density function depending onthe parameter ✓.
We will study the log-likelihood, and for that we define
l (�) =nX
i=1l
i
(�) = lognY
i=1f (y
i
)
=
nX
i=1log f (y
i
; ✓i
, �) =nX
i=1
yi
✓i
� b(✓i
)a(�)
+
nX
i=1c(y
i
, �).(3.16)
The notation l (�) reflects the dependence of � on the parameters ✓1, . . ., ✓n
. Wemaximize the likelihood function via the first-order condition
(3.17) 0 =nX
i=1
@l
i
@ �j
=
nX
i=1
@l
i
@✓i
@✓i
@µi
@µi
@⌘i
@⌘i
@ �j
,
where we used the chain rule to di�erentiate the log-likelihood (3.16).
Since µi
= b
0(✓i
) as well as Var(yi
) = b
00(✓i
)a(�) (cf. (3.9) and (3.12)) and
@l
i
@✓i
=y
i
� b
0(✓i
)a(�)
,
we have
(3.18)@µ
i
@✓i
= b
00(✓i
) =Var(y
i
)a(�)
and@l
i
@✓i
=y
i
� µi
a(�).
In addition, since
⌘i
=
pX
k=1�
k
x
ik
18

we have @⌘i@ �j
= x
i j
. Finally, since ⌘i
= g(µi
), @µi@⌘i
depends on the link function forthe model. In summary, substituting into (3.17), we obtain
(3.19) @l
i
@ �j
=(y
i
� µi
)a(�)
a(�)Var(y
i
)@µ
i
@⌘i
x
i j
=(y
i
� µi
)x
i j
Var(yi
)@µ
i
@⌘i
.
By summing over i we obtain the estimating equations for the GLM:
(3.20)@l (�)@ �
j
=
nX
i=1
(yi
� µi
)x
i j
Var(yi
)@µ
j
@⌘j
= 0, j = 1, 2, . . . , p,
where ⌘j
=P
p
j=1 � j
x
i j
= g(µj
) for the link function g. These are j equations for j
unknown variables �1, . . . , � j
.
Let V denote the diagonal matrix of variances of the observations, and let D denotethe diagonal matrix with elements @µi@⌘
i
. For what follows, we observe that with thisnotation, we may write the estimating equations in the matrix form as
(3.21) X
0DV�1(y � µ) = 0.
After solving the parameter vector �, we also need this to have the proper asymptoticproperties. Indeed, the estimating equations produce an unbiased estimator, with theasymptotic large sample distribution of �̂ given by
(3.22) N[�, (XT
WX)�1],
where W is the diagonal matrix with elements
(3.23) wi
=
⇣@µ
i
@⌘i
⌘2
Var(yi
).
(Agresti, 2015, 123–126.)
3.2 Generalized estimating equations
Generalized estimating equations (GEE) is an extension of the generalized linearmodels developed by Liang and Zeger (1986). It is a semi-parametric approachused in longitudinal, repeated measures or clustered study designs. GEE permitsa specification of a working correlation matrix that accounts for the within-subject
19

correlation of response variables. Indeed, in longitudinal data there are often repeatedmeasures over time. This may result in correlation within a subject or clusters ofobservations over repeated measures. If the correlation is not taken into account inthe analysis, the inferences about the parameter estimates may be incorrect.
Ballinger (2004) state that, when using a linear regression, we may face the non-constant variance of the dependent variable, especially when modeling probabilities,as is our goal. In addition, error terms are not usually normally distributed. In suchcases, power transformation on the dependent variable prior to running an OLSregression is an alternative option.
The GEE model is specified similarly to GLM as
(3.24) g(µi
) = x
0i
�.
However, contrary to GLM, full specification of the joint distribution as well asthe maximum likelihood estimation (MLE) is not required for the estimation of thecoe�cient vector. GEE uses quasi-likelihood estimation rather than MLE or ordinaryleast squares (OLS) to estimate the parameters. The quasi-likelihood method a�rmsa model for the mean function µ
i j
= E(yi j
), and specifies a variance function V (µi j
).The estimate of � is called the quasi-likelihood estimate when we maximize thenormality-based log-likelihood without the assumption, that the response is normallydistributed. (Agresti, 2015, 316–317.)
3.2.1 Parameter estimation
GEE consists of the same components as GLM:
1. a probability distribution of the response variable y from the exponentialfamily;
2. a linear predictor ⌘ = X�;
3. a link function g such that
(3.25) g⇥E(y|X)
⇤= ⌘.
Here we have again used the same abuse of notation as in (3.2). Now the covariancestructure of the correlated responses are specified and modeled. Contrary to GLM,the responses (y1, y2, . . . , yn
) are allowed to be correlated or clustered. This meansthat the cases do not need to be independent. In addition, also the errors are allowedto be correlated and the homogeneity of the variances does not need to be satisfied.
In the Chapter 3.1 we obtained the estimating equations for the GLM (3.20), thatincluded a linear predictor with an associated coe�cient vector to be estimated.
20

Assuming n clusters with n
i
observations in each clusture, the estimating equationcan now be written as
(3.26) (�) =2666664*,
nX
i=1
n
iX
t=1
yit
� µit
V (µit
)
@µ
@⌘
!
it
x
jit
+-
j=1,...,p
3777775px1
= 0.
Typically the observations in each cluster are measurements in di�erent time points,and thus the corresponding indexing is usually denoted by t.
Using a matrix notation, the equation (3.26) can be rewritten as
(3.27) (�) =2666664*,
nX
i=1x
0ji
D
⇥V(µ
i
)⇤�1 �
y
i
� µi
�+-
j=1,...,p
3777775px1
= 0,
where D is the diagonal matrix as specified in (3.21), and
(3.28) V(µi
) =fV(µ
it
)1/2I(n
i
xn
i
)V(µit
)1/2g
n
i
xn
i
.
Observe, that here we assumed the responses to be independent. Correspondingly,the identity matrix I can be interpreted as the correlation matrix, where I correspondsto the assumption that the observations are mutually independent. Next, the aim isto model the expected value with mutually dependent observations. Indeed, GEE isa modification of the limited information maximum likelihood estimating equationfor GLMs that simply replaces the identity matrix with a more general correlationmatrix, since the variance matrix for correlated data does not have a diagonal form.Formally, we replace the identity matrix I with the corresponding correlation matrixR(↵):
(3.29) V(µi
) =fV(µ
it
)1/2R(↵)V(µ
it
)1/2g
n
i
xn
i
,
where ↵ is a parameter vector used to represent the correlation data. Now replacingthe identity matrix I in the estimating equation (3.27) by (3.29), we obtain thegeneralised estimating equations. (Hardin, 2005, 57–58.) By solving the equationswe find the coe�cient vector � which is used in the model for the expected value µ
it
via g(µit
) = x
0it
�.
While the derivation of the estimating equations, we explained, is not valid anymoredue to not having independent covariates, it turns out that the equations can still bejustified. Indeed, similarly to the formula (3.22) in the case of GLM, under suitableregularity assumptions, we now have the asymptotic behavior given by
(3.30)p
n(�̂ � �)d! N (0,V
G
),
21

where the asymptotic covariance matrix VG
is given by(3.31)
V
G
:= limn!1
n
266664nX
i=1D
0i
V
�1i
D
i
377775�1 266664
nX
i=1D
0i
V
�1i
cov(yi
)V�1i
D
i
377775266664
nX
i=1D
0i
V
�1
i
D
i
377775�1
.
(Liang and Zeger, 1986).
3.2.2 Sandwich estimator
For inferences about �, valid standard errors can be obtained from the sandwichestimator for (3.31) given by
(3.32) n
266664nX
i=1D̂
0i
V̂
�1i
D̂
i
377775�1 266664
nX
i=1D̂
0i
V̂
�1i
(yi
� µ̂i
)(yi
� µ̂i
)0V̂�1i
D̂
i
377775266664
nX
i=1D̂
0i
V̂
�1i
D̂
i
377775�1
,
where compared to (3.31) D and V have been replaced by the sample estimates D̂
and V̂ (Fitzmaurice et al., 2012, 357–359). In other words, GEE estimates regressioncoe�cients and standard errors with sampling distributions that are asymptomaticallynormal.
Observe, that if the working covariance structure R(↵) is correct, i.e. V
i
= cov(yi
),the approximation V
G
for the asymptotic covariance matrix simplifies to the model-based covariance matrix
V
G
= limn!1
n
*,
nX
i=1D
0i
V
�1i
D
i
+-�1
.
(Agresti, 2015, 317–318.)
Moreover, we note that by using the notation
B =
nX
i=1D
0i
V
�1i
D
i
M =
nX
i=1D
0i
V
�1i
cov(yi
)V�1i
D
i
,
(3.33)
the asymptotic covariance of �̂ can be expressed as
avar(�̂) := B
�1MB
�1.
Here the notations B and M are sometimes referred as bread and meat of thesandwich.
Considering the convergence results, in which the asymptotic properties rely, as usualthe most important assumption is that the model is correctly specified. Secondly, in
22

case of missing data, the consistency of the estimates requires the data to be missingcompletely at random. In particular, contrary to maximum likelihood estimation theprobability of a missing data point should not depend on the value of the missingitem. (Fitzmaurice et al., 2012, 357–361.)
3.2.3 Correlation matrix
Common patterns of correlation matrices R(↵) are exchangeable (corr (yi j
, yik
) =↵), autoregressive (corr (y
i j
, yik
) = ↵ | j�k |, independence (corr (yi j
, yik
) = 0) andunstructured (corr (y
i j
, yik
) = ↵j k
) (Agresti, 2015, 316). These correlation structurescan be expressed in matrix form as follows: identity matrix
(3.34)
266666641 0 00 1 00 0 1
37777775,
where correlation between time points is independent, V
i
is diagonal; for exchange-able matrix
(3.35)
266666641 p p
p 1 p
p p 1
37777775,
where all measurements on the same unit are equally correlated; for autoregressivematrix of order 1 (AR1)
(3.36)
266666641 p p
2
p 1 p
p
2p 1
37777775,
where correlation depends on time or distance between measurements i and m; e.g.first order auto-regressive model has terms p, p2, p3; and finally, for the unstructuredcorrelation matrix we have
(3.37)
266666641 p12 p13
p21 1 p23
p31 p32 1
37777775,
where there are no assumptions about the correlations.
23

Finally, we point out that the GEE estimates are valid even if the correlation matrixR(↵) is not correctly specified. Indeed, we specify the supposed correlation structurein (3.29), but the convergence result of (3.30) holds for any such R(↵). Of course, thismay a�ect the value of the sandwich estimator for a given number of observations n.In other words, mis-specifying the correlation structure may cause the convergenceto be slower, but it still is asymptotically convergent.
3.3 Cumulative probability
Definition 3.2. We define a random variable to be a real-valued function f : ⌦!(Varadhan, 2001).
Definition 3.3. Let ⌦ represent the rows of our dataset including all the screeninginvitations, independent of the attendance. Let ⌦
i
be the set of all rows for person i
and denote by !ik
the chronologically ordered k’th row for i’th individual. Denote
(3.38) sumFP
ik
:=kX
j=1FP(!
i j
).
Here FP : ⌦ ! {0, 1} is the random variable corresponding to a false-positive testresult. We define the categorial variable measuring the number of previous false-positive results as
prevFP
ik
= min{sumFP
ik
, 2}.
In the sequel, we will not pay attention to any particular individual or any particularscreening round, and thus, we will drop the subindices i and k to represent a genericdata row for a generic individual.
Woman is considered to be an irregular attendee at those screening rounds when shehas missed her last screening examination. Since the screening program in Finlandis biennial for breast cancer screening, this means that for a irregular attendee in thisstudy, there were � 3.5 years (42 months) in between the screening rounds. We definefor non-attended screening invitations irregular = N A and for attended screenings
irregular
i,1 = 0 for every i,
and for k � 2 that
irregular
ik
=8><>:
1, if � 3.5 years (42 months) after the last screening examination,0, otherwise.
Next we calculate the conditional cumulative probability of a false-positive screeningresult. Here the probability is calculated with the condition of a woman attending
24

the screening, having no previous FP result and a woman either being an irregular orregular attendee.
{! 2 ⌦ | age(!) = j, prevFP(!) = 0, attend(!) = 1}= [1
i=0{! 2 ⌦ | age(!) = j, prevFP(!) = 0, attend(!) = 1, irregular (!) = i},
age, prevFP, attend, irregular: ⌦ ! . Therefore, age, prevFP, attend and irregularare random variables. In the future, we will denote
{! 2 ⌦ | age(!) = j, prevFP(!) = 0}= {age = j, prevFP = 0}
and
{! 2 ⌦ | age(!) = j, prevFP(!) = 0, attend(!) = 1, irregular (!) = i}de f
= {age = j, prevFP = 0, attend = 1, irregular = i}.
We begin by using the decomposition
�age = j, prevFP = 0, attend = 1
=
1[
i=0
�age = j, attend = 1, prevFP = 0, irregular = i
to deduce
P
��FP = 1
\ �age = j, prevFP = 0, attend = 1
�
= P
��FP = 1
\1[
i=0
�age = j, attend = 1, prevFP = 0, irregular = i
�
=
1X
i=0P
��FP = 1
\ �age = j, attend = 1, prevFP = 0, irregular = i
�.
(3.39)
25

By using this identity and the definition of the conditional probability we obtain
P
�FP = 1 �� age = j, prevFP = 0, attend = 1
�
=P
��FP = 1
\ �age = j, prevFP = 0, attend = 1
�
P
�age = j, prevFP = 0, attend = 1
�
=
P1i=0 P
��FP = 1
\ �age = j, attend = 1, prevFP = 0, irregular = i
�
P
�age = j, prevFP = 0, attend = 1
�
=
1X
i=0
P
��FP = 1
\ �age = j, attend = 1, prevFP = 0, irregular = i
�
P
�age = j, attend = 1, prevFP = 0, irregular = i
�
⇥ P
�age = j, attend = 1, prevFP = 0, irregular = i
�
P
�age = j, prevFP = 0, attend = 1
�
=
1X
i=0P
�FP = 1 �� age = j, attend = 1, prevFP = 0, irregular = i
�
⇥ P
�irregular = i
�� age = j, prevFP = 0, attend = 1�
= P
�FP = 1 �� age = j, attend = 1, prevFP = 0, irregular = 0
�
⇥ P
�irregular = 0 �� age = j, prevFP = 0, attend = 1
�
+ P
�FP = 1 �� age = j, attend = 1, prevFP = 0, irregular = 1
�
⇥ P
�irregular = 1 �� age = j, prevFP = 0, attend = 1
�.
(3.40)
This is used later to identify the risk of a FP screening result with respect to age.
Next we calculate the cumulative probability of a false-positive test result. We definenew random variables FP
k and prevFP
k which describe the corresponding value atthe k’th examination for the i’th individual !i. In other words, we define
FP
k (!i) := FP(!ik)
prevFP
k (!i) := prevFP(!ik
).
We formally obtain
P("FP = 0 for the first k screenings")
= P
�{FP
1 = 0} \ {FP
2 = 0} \ · · · \ {FP
k = 0}�
=P
�{FP
1 = 0} \ {FP
2 = 0} \ · · · \ {FP
k = 0}�
P
�{FP
1 = 0} \ {FP
2 = 0} \ · · · \ {FP
k�1 = 0}�
⇥ P
�{FP
1 = 0} \ {FP
2 = 0} \ · · · \ {FP
k�1 = 0}�
= P(FP
k = 0 �� prevFP
k = 0)
⇥ P
�{FP
1 = 0} \ {FP
2 = 0} \ · · · \ {FP
k�1 = 0}�,
26

for every k � 1. Inductively, we obtain
P("FP = 0 for the first k screenings")
= P
�{FP
1 = 0} \ {FP
2 = 0} \ · · · \ {FP
k = 0}�
= P(FP
k = 0 �� prevFP
k = 0) ⇥ P(FP
k�1 = 0 �� prevFP
k�1 = 0)
⇥ P
�{FP
1 = 0} \ {FP
2 = 0} \ · · · \ {FP
k�2 = 0}�
...
= P(FP
k = 0 �� prevFP
k = 0) ⇥ P(FP
k�1 = 0 �� prevFP
k�1 = 0)⇥· · · ⇥ P(FP
2 = 0 �� prevFP
2 = 0) ⇥ P
�{FP
1 = 0}� .
For the cumulative probability we will only consider the regular attendees, whoparticipate the screening regularly for every two years starting from age 50. Thus, fork’th examination the corresponding whole population is the set of regular attendees(i.e. irregular = 0) of age 50 + 2(k � 1). We obtain
P("FP = 0 for the first k biennial screenings")= P(FP = 0 | age = 50, prevFP = 0, irregular = 0)⇥· · · ⇥ P(FP = 0 | age = 50 + 2(k � 1), prevFP = 0, irregular = 0)
=
kY
n=1
⇥1 � P(FP = 1 | age = 50 + 2(n � 1), prevFP = 0, irregular = 0)
⇤
=
kY
n=1(1 � q
n
),
where we have denoted
q
n
de f
= P(FP = 1 | age = 50 + 2(n � 1), prevFP = 0, irregular = 0).
Therefore, the cumulative probability of at least one FP during the first k screeningsis
(3.41) p
k
de f
= 1 �kY
n=1(1 � q
n
).
3.4 Confidence intervals
For calculating the confidence intervals for the cumulative probability, we use amethod based on a bootstrapping argument with some computational simplifications.The bootstrapping method gives possibility to form confidence intervals estimatesfor unknown parameter � when the distribution of the estimator �̂ is unknown. Withthe given dataset and a model we form the confidence intervals by generating a largenumber of bootstrap estimates.
27

Without going to excessive details about the methodology of bootstrapping, weconsider the question through a simple example developed for our setting. In ourcase, we consider the model
Pr (FP) = logit�1[�0 + �1 log(age
months
� 580) + �2 · prevFP + �3 · irregular],
where the logit function is defined as
(3.42) logit(p) = log
p
1 � p
!, p 2 (0, 1).
Now the model, with the estimated parameter vector �̂, provides an estimate forPr (FP) given the data, and we can use this estimate Pr (FP) to produce a new set ofbinary variables FPgenerated
generated by using these probabilities. In practice, weobtain a dataset, with newly generated values of FPgenerated
, similarly to Table 3.1.
Table 3.1. Illustration matrix of bootstrapping.
FP
generated
Pr (FP)model
Age
months
Irregular prevFP FP
0 0.01 590 0 1 00 0.02 600 0 0 01 0.03 610 1 0 1...
......
......
...
In the bootstrapping argument, we ignore the original values of FP, and produce anew estimate �̃ for � based on the newly generated values of FPgenerated
. Next, wecalculate the cumulative probabilities corresponding to a large number of generatedparameter vectors �̃. Finally, we obtain the confidence intervals directly from thedistribution of this set of cumulative probabilities.
However, since our dataset is very large consisting of over 470,000 examinations,generating a large number of new datasets is not computationally feasible. Assumingthat our originally estimated parameter vector �̂ represents the true value of �, andthat our model is correctly specified, the asymptotic behavior of the GEE estimatesgives
(3.43)p
n(�̃ � �̂)d�! N (0,V
G
),
where V
G
is the covariance matrix given in (3.31).
Therefore, in order to simplify the computational requirements, we directly use thisasymptotic distribution for the values of � = �̃, assuming that the originally estimatedparameter vector �̂ represents the true value. Thus, we generate the distribution ofcumulative probabilities by randomizing a number of new parameter vectors fromthe probability distribution given by
N (�̂,VG
/n).
28

We acknowledge that this approach is most likely not as robust as the standardbootstrapping argument. Relying on the large number of observations it, however,seems reasonable to assume that �̂ is very close to the true value, supporting ourchoice. In the next chapter we will consider our modeling in detail, to also argue thatour modeling is correctly specified, providing further support for this computationalsimplification.
29

4 Analysis
Generalized estimating equations was used to estimate the cumulative probability of afalse-positive screening result. We studied the e�ect of age, previous FP and regularityof the women attending the screening rounds on obtaining (another) FP test result.Age was used as a continuous variable and previous FP and regularity variables werecategorised. The 95% confidence intervals for the risk of a false-positive screeningresult at each age group was estimated using a suitable modification of bootstrapping,see Section 3.4.
We used the cohort data, where the first invitation was sent to women aged 50–51,the program lasting until the age of 69. We then used the modeling to estimatethe cumulative probability of a FP result for women attending all the 10 biennialscreenings of the program.
The analysis was performed with R (R Development Core Team, 2008), using geepackpackage (Halekoh et al., 2006; Yan and Fine, 2004; Yan, 2002).
4.1 Data description
The women were invited for screening mammography examination every two years.There were altogether 539, 512 invitations and a total of 477, 047 screening mam-mograms were carried out (see Table 4.1). The attendance rate overall was 88.4%.Altogether 13, 454 screening examinations, 2.8% out of the total, resulted in a recallfor further examination and of these 82% received a false-positive result. Altogether,9,981 women (12.3%) received at least one false-positive tests result. Moreover,3, 207 referrals were given, and a total of 2, 310 (0.5% of the attended women) breastcancers were diagnosed.
The largest number of false-positive test results (3, 399) were received at the firstscreening round, at age 50–51. The number of false-positive results diminished byage, older women receiving less FP results. Note that the number of women attendeddiminishes also along with the age, with a total of 18, 287 invited and 15, 258 attendedwomen at the age of 68–69. The distribution of invitations, attendance rates, recalls,referrals and test results by age is shown in the Table 4.1.
In the Table 4.2 the distribution of invited women are presented in an individuallevel. The Table describes the variety of how many women have received howmany invitations, and how many women have attended how many screening rounds.Overall, 576 women received one invitation in the cohort group and 3, 722 receivedten invitations. 1, 874 women participated only in one screening round and 2, 430women attended all ten screening rounds. However, the most concentration of thestudy population can be seen in the screening rounds 5, 6 and 7, where over 10, 000women received either 5, 6 or 7 invitations and attended at least 5, 6 or 7 screenings.
30

The Table 4.2 also describes the number of women who received more than oneinvitation at same age and the number of women who attended mammographyscreening two times a row at same age. This is referred to as a double invitation. Therewere altogether 1, 228 double invitations and 620 women attended the screeningsecond time during the same age. Altogether 120 women received 11 invitations andout of those 64 women attended 11 screening examinations. In addition, 3 womenreceived 12 invitations and out of these 1 attended all 12 screening examinations.
All women were included in the analysis, including those who received doubleinvitations and attended both times and women who received more than ten invitationsand attended them all. There were 3040 women who did not attend any screeningexaminations.
The number of women, both in invited and attendees, decreased over time. The cohortdata was received only until the end of 2012, therefore there are some age groupswhich have not yet received all 10 invitations during the study period. This meansthat all the invitations and screening examinations that should be included in thecohort data were not yet available. We note, that this can have an biased e�ect on theestimates. We could have based our estimates on the data from 7 screening roundsand extrapolate the cumulative risk of false-positive result over a program of 10screening rounds. However, there seems to be no reason to expect di�erent behaviorof women with di�erent year of birth with respect to obtaining a FP screening result.Therefore, we expect there to be no bias and for simplicity use the whole datasetwithout correction.
31

Table
4.1.D
istrib
utio
nof
invi
tatio
ns,a
ttend
ance
,rec
alls,
refe
rral
s,TP
and
FPfro
m19
92th
roug
h20
12by
age.
Age
Invi
tatio
nsA
ttend
ance
(%)
Reca
ll(%
)Re
ferr
al(%
)TP
(%)
FP(%
)
50–5
184
,704
75,3
90(8
9.0)
3,70
8(4
.9)
631
(0.8
)29
1(0
.4)
3,39
9(4
.5)
52–5
376
,098
67,5
01(8
8.7)
2,03
0(3
.0)
357
(0.5
)23
3(0
.4)
1,78
4(2
.6)
54–5
576
,180
68,1
52(8
9.5)
1,72
5(2
.5)
323
(0.5
)21
6(0
.3)
1,49
6(2
.2)
56–5
781
,141
72,4
81(8
9.3)
1,56
2(2
.2)
391
(0.5
)30
0(0
.4)
1,25
0(1
.7)
58–5
980
,426
72,0
75(8
9.6)
1,53
7(2
.1)
453
(0.6
)36
4(0
.5)
1,16
4(1
.6)
60–6
134
,261
30,7
04(8
9.6)
669
(2.2
)20
6(0
.7)
173
(0.6
)48
6(1
.6)
62–6
325
,114
21,6
07(8
6.0)
434
(2.0
)14
9(0
.7)
131
(0.6
)30
0(1
.4)
64–6
530
,630
26,1
50(8
5.4)
670
(2.6
)26
5(1
.0)
237
(0.9
)42
7(1
.6)
66–6
732
,671
27,7
29(8
4.9)
685
(2.5
)25
1(0
.9)
215
(0.8
)46
0(1
.7)
68–6
918
,287
15,2
58(8
3.4)
434
(2.8
)18
1(1
.2)
150
(1.0
)27
0(1
.8)
Tota
l53
9,51
247
7,04
7(8
8.4)
13,4
54(2
.8)
3,20
7(0
.7)
2,31
0(0
.5)
11,0
36(2
.3)
32

Table
4.2.D
istrib
utio
nof
wom
enin
anin
divi
dual
leve
l.N
umbe
rofi
nvita
tions
obse
rved
atsc
reen
ing
roun
ds1
to10
and
over
alln
umbe
rof
wom
en.N
umbe
rofw
omen
atte
nded
atsc
reen
ing
roun
ds1
to10
and
into
tal.
Num
bero
fwom
enw
ithnu
mbe
rofd
oubl
etim
esin
vite
ddu
ring
one
year
with
one,
two
orth
ree
times
.Num
bero
fwom
enat
tend
edtw
otim
esdu
ring
the
sam
eye
ar.N
umbe
rofw
omen
with
num
bero
frec
alls,
refe
rral
sand
into
tal.
Num
bero
fwom
enw
ithnu
mbe
roft
rue
posit
ives
,fal
sepo
sitiv
esan
din
tota
l.
No.
ofw
omen
with
no.o
fin-
vita
tions
into
-ta
l
No.
ofw
omen
with
no.
ofat
-te
nded
scre
en-
ings
No.
ofw
omen
with
no.
ofdo
uble
invi
tatio
ns
No.
ofw
omen
with
no.
ofat
tend
eddo
uble
times
No.
ofw
omen
with
no.o
fre-
calls
No.
ofw
omen
with
no.o
fre-
ferr
als
No.
ofw
omen
with
no.
ofTP
No.
ofw
omen
with
no.o
fFP
N(%
)N
(%)
NN
N(%
)N
(%)
N(%
)N
(%)
No.
157
6(0
.7)
1,87
4(2
.3)
1,17
010
,657
3,03
52,
244
9,01
22
748
(0.9
)2,
203
(2.7
)55
1,19
286
3388
73
1,23
7(1
.5)
3,40
9(4
.2)
312
778
45,
179
(6.1
)8,
329
(10.
2)8
45
24,4
21(2
8.9)
22,8
90(2
8.1)
615
,870
(18.
8)14
,868
(18.
3)7
13,2
02(1
5.6)
11,0
56(1
3.6)
89,
875
(11.
7)7,
641
(9.4
)9
9,52
2(1
1.3)
6,67
0(8
.2)
103,
722
(4.4
)2,
430
(3.0
)
Tota
l84
,475
�81
,435
(96.
4)�†
1,22
862
011
,984
(14.
7)3,
121
(3.8
)2,
277
(2.8
)9,
981
(12.
3)
� 120
wom
enre
ceiv
ed11
invi
tatio
nsan
dou
toft
hose
64w
omen
atte
nded
11sc
reen
ing
exam
inat
ions
.� 3
wom
enre
ceiv
ed12
invi
tatio
nsan
dou
toft
hose
1at
tend
ed12
scre
enin
gex
amin
atio
ns.
† 3,0
40(3
.6%
)wom
endi
dno
tatte
ndan
ysc
reen
ing
roun
ds.
33

4.2 Modeling
Similarly to Roman et al. (2013) and Baker et al. (2003) we use age, previous FPscreening results and regularity of attendance as explanatory variables. Previousstudies (Roman et al., 2012, 2013) have estimated the model-based cumulative prob-ability of an FP screening result by screening round. This can be considered to beequivalent to modeling with the age, assuming the women start the mammographyscreening program at a certain age and attend the screenings regularly.
In this study we estimate the probability of an FP result by age. We make this choice,because the underlying medical characteristics vary according to the age of thepatient, and not according to the screening round. For instance, younger breasts aremore dense, making them to be more di�cult for radiological interpretation (Romanet al., 2014). In the model building we use age as a continuous variable in monthsto be able to get the most data points for the model formation. Then we define twocategorical variables. For variable definitions, see Sections 2.6 and 3.3.
We use the logit-model specified as
(4.1) logit FP = �0 + �1 log(age
months
� 580) + �2 · prevFP + �3 · irregular .
Here we have normalized the monthly age variable to 580 months corresponding tothe minimum age of 588 months (49 years) in the data. Also other normalizationsare possible, but we expect the reasonable ones to present similar results. Observethat log(0) = �1.
For the GEE modeling binomial family was used together with the logit link function.For the correlation structure an independence structure was used in both models,when modeling the FP and when modeling the irregular variable.
For the correlation matrix independence, exchangeable and AR1 structures weretested. For the exchangeable structure the value of the correlation parameter ↵ provedto be ↵ = 0.00718 which indicated low correlation within the observations. There-fore, an independence correlation structure was chosen. We emphasize that this isnot an assumption on the data, as GEE is robust with respect to a incorrect choice ofthe correlation structure. However, with a proper choice of the structure, we obtainthe best standard deviations, leading to the most reliable modeling. In particular, wedot not assume independence between the observations.
Since GEE estimates are sensitive for unrandom missing data, we comment that inour setting the missing data can be considered random, since the screening programcovers the whole target population. In particular, there is no reason to assume thatthe population studied during the cohort years, is not a proper representation of thegeneral phenomenon. However, since the cohort data was received only until the endof 2012, all the women have not yet received all 10 invitations. This raises a questionwhether the data is randomly missing. However, here we refer to previous discussion
34

in the Section 4.1 about the possible bias due to missing data.
Next we consider the feasibility of our modeling (see Table 4.3).
Table 4.3. GEE model with logit link function and independence correlationmatrix.
Model Estimate Std.Error Wald Sig OR LowerOR
UpperOR
Intercept �1.7975 0.0421 1821 <2e-16*** 0.17 0.15 0.18log(Age-580)† �0.5024 0.0109 2125 <2e-16*** 0.61 0.60 0.62Irregular 0.3778 0.0324 136 <2e-16*** 1.46 1.37 1.56FP 0.6462 0.0349 342 <2e-16*** 1.91 1.78 2.04> 1 FPs 1.1270 0.1105 104 <2e-16*** 3.09 2.49 3.83Signif.codes: 0’***’ 0,001’**’ 0,01’*’ 0,05’.’
†Age in months.The monthly age variable is normalized to 580 months corresponding to theminimum age of 588 months.
As a first check we observe that all the variables are statistically significant. Age,regularity of the attendance and a previous FP were used to model the risk of a FPscreening result. The corresponding odds ratios are 0.61, 1.46, respectively, as wellas 1.91 and 3.09 for one or more previous FPs. Women with irregular attendanceand previous FP result have an increased risk of receiving FP screening result.
The primary question in the modeling is to determine the true model representingthe studied phenomenon. This is important, not only for the asymptotic of the GEEmodeling, but also for the bootstrapping argument, which relies on the model baseddata generating process being truthful.
We concluded that all the variables in the model were statistically significant factors.Next we concentrate further to study the validity of the model. We will concentrateon following four main questions:
1. the validity of specifying previous FP and regularity of the attendance ascategorical variables,
2. the proper relation between the age and the probability of FP screening testresult e.g. logarithmic or power like relation,
3. the capability of the model to explain the typical behavior for each combinationof age, previous FP and regularity of the attendance,
4. how much the model explains the variability of the data.
First thing is to consider, that categorizing the variables previous FP and regularityof the attendance are justified. In the first subsection we will examine whether thecategorization fits the data.
35

In the second subsection we verify the proper relation between the age and theprobability of FP screening test result. We look at the data to obtain a first indicationof a proper transformation. It turns out that a logarithmic or power like relation seemsplausible, and then we use a Boxcox analysis for further examination.
Next we examine the capability of the model to explain the typical behavior foreach combination of the variables age, previous FP and regularity of the attendance.Finally, we study how much the chosen model explains the variability of the data.
4.2.1 The validity of specifying previous FP and regularity of the attendance
as categorical variables
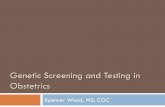
In the following, we will, for simplicity, compare the model fitted values to theordinary least squares (OLS) regression computed for each subdatasets. Indeed, inthe Figure 4.1 we fit an OLS regression into the subdatasets with each possiblevalues of the categorical variables. When we have a categorical variable (irregular
and prevFP), it means that when either variable receives value 1, it adds a constantinto the fitted value. This indicates that the regression line moves while the slopestays the same.
36

600 650 700 750 800 850
−6−5
−4−3
−2−1
Age(month)
logit(P
r(FP))
prevFP=0, irregular=0
R2 = 0.298
600 650 700 750 800 850
−6−5
−4−3
−2−1
Age(month)
logit(P
r(FP))
prevFP=0, irregular=1
R2 = 0.0191
600 650 700 750 800 850
−6−5
−4−3
−2−1
Age(month)
logit(P
r(FP))
prevFP=1, irregular=0
R2 = 0.039
600 650 700 750 800 850
−6−5
−4−3
−2−1
Age(month)
logit(P
r(FP))
prevFP=1, irregular=1
R2 = −0.0054
600 650 700 750 800 850
−6−5
−4−3
−2−1
Age(month)
logit(P
r(FP))
prevFP=2, irregular=0
R2 = −0.000335
600 650 700 750 800 850
−6−5
−4−3
−2−1
Age(month)
logit(P
r(FP))
prevFP=2, irregular=1
R2 = 0.165
Figure 4.1. OLS regression for each subdata.
We see a similar slope in the first four graphs. This indicates that the categoricalvariable seems at least at a first glance reasonable. Because the slope stays the same
37

in the first four graphs, it seems reasonable to assume that changing the categoricalvalue does not change the relation between the age and the response variable.
The last two graphs represent a di�erent behavior. However, we note that there is alow number of the observations. When prevFP = 2, i.e. the women has two or moreprevious false-positive results, the slope di�ers significantly. It is hard to elaboratewhy this happens, other than due to the low number of observations (see Table 4.4),although we do not rule out other possibilities either.
Table 4.4. Number of observations for the cases represented in Figure 4.1.
prevFP Irregular No. Observations
0 0 398,0730 1 46,3211 0 27,4051 1 3,2822 0 1,7482 1 218
Total 477,047
4.2.2 The relation between the age and the probability of FP result
In addition, in the first graph (see Figure 4.1) where prevFP and irregular have thevalue 0, we notice a convex behavior that indicates that some transformation wouldbe recommended to the age variable. Indeed, this is not only a question of fittingdata, but has deep underlying medical reasons.
The fact that the risk for a FP test result is substantially higher for younger women iswell-documented in the literature (Castells et al., 2006). The reason for this could beexplained by not having previous mammograms to compare the new ones. Anotherreason can be that younger breasts are more dense, which makes the interpretationof the mammogram more di�cult (Roman et al., 2014).
Now, the convexity of the first graph in the Figure 4.1 suggests logarithmic or possiblypolynomial transformation. By using a Boxcox analysis, with the transformation
(4.2)x
� � 1�,
we get the optimal Boxcox variable � = 0.34.
38

−2 −1 0 1 2
−155
−150
−145
−140
−135
λ
log−
Like
lihoo
d
95%
Figure 4.2. Boxcox analysis.
The value 0.34 being close to 0, recalling that by the l’Hospital rule
lim�!0
x
� � 1�= log x,
we choose to use the logarithmic transformation.
Thus we next compare the model fit, with the logarithmic transformation, versusthe OLS fit of the logit-model for each subdatasets. This can be seen in the Figure4.3. The red line describes the OLS fit for the observed subdata and the blue line isthe estimated value from the model. Since logit 0 = �1, we first study the modelfit versus the Pr(FP) to be able to study the OLS also considering for 0 cases,corresponding to logit Pr (FP) = �1.
39

600 650 700 750 800 850
0.00
0.02
0.04
0.06
0.08
0.10
log(Age(month))
Pr(FP)
prevFP=0, irregular=0
R2 = 0.591
600 650 700 750 800 8500.00
0.02
0.04
0.06
0.08
0.10
log(Age(month))
Pr(FP)
prevFP=0, irregular=1
R2 = 0.038
600 650 700 750 800 850
0.00
0.02
0.04
0.06
0.08
0.10
log(Age(month))
Pr(FP)
prevFP=1, irregular=0
R2 = 0.152
600 650 700 750 800 850
0.00
0.02
0.04
0.06
0.08
0.10
log(Age(month))
Pr(FP)
prevFP=1, irregular=1
R2 = 0.0016
Figure 4.3. Inverse logit with the OLS fit of the observed data (red) andmodeling (blue).
In the most typical case of prevFP = 0, irregular = 0, we have a very good fit forthe data (398,073 observations). There is a slight di�erence in the fit in the second(46,321 observations) and fourth (3,282 observations) graphs. However, accountingfor the complexity of the question in hand, the model fit is reasonably close to theOLS fit of the subdata. In the third graph (27,405) the OLS fit (red line) does not seem
40

to represent the data. This happens probably because the cases, where Pr (FP) = 1,corresponding to a low number of observations within that age group, distort thedata.
Observe also that in the last three graphs some age groups have zero cases, whichcan be seen as Pr (FP) = 0 for the corresponding ages in the Figure 4.3. It meansthat there are no event in certain age groups with the model parameters. Indeed, theprobability is calculated from probability sampling, and there are age groups withoutany events. The adjusted R
2 is calculated from OLS fit (red line).
Finally, here we can also see that height of both the OLS fit (red line) as well as themodel fit (blue line) vary depending on the values of the categorial variables. Thiscorresponds to the di�erent probabilities of obtaining the FP test result dependingon the individual screening history. In addition, the convex behavior can only beseen in the first graph, but this is expected, since by definition, the later graphs haveobservations only for older ages. For instance, prevFP = 1 immediately impliesthat at least one screening test has already been done, indicating that the womanis typically at least 52 years old. The same applies also for the regularity of theattendance.
4.2.3 The capability of the model to explain the typical behavior for each
combination of age, previous FP and regularity of the attendance
To be able to see more comparable fitted lines, especially for the graph three in theFigure 4.3, for the model fit versus the OLS fit of the logit-model, lastly we do anexponential transformation. For log(Age(month)), when we have
(4.3) log
p
1 � p
!
and take an exponent of this, we are left with
(4.4)p
1 � p
.
This transformation can be seen in the Figure 4.4.
41

600 650 700 750 800 850
0.00
0.02
0.04
0.06
0.08
0.10
log(Age(month))
p/(1−p)
prevFP=0, irregular=0
R2 = 0.594
600 650 700 750 800 8500.00
0.02
0.04
0.06
0.08
0.10
log(Age(month))
p/(1−p)
prevFP=0, irregular=1
R2 = 0.0333
600 650 700 750 800 850
0.00
0.02
0.04
0.06
0.08
0.10
log(Age(month))
p/(1−p)
prevFP=1, irregular=0
R2 = 0.0285
600 650 700 750 800 850
0.00
0.02
0.04
0.06
0.08
0.10
log(Age(month))
p/(1−p)
prevFP=1, irregular=1
R2 = −0.00166
Figure 4.4. Exponential transformation with the OLS fit of the observed data(red) and modeling (blue).
Here we again have a reasonable fit for first, second and fourth graph, but now alsofor the third graph.
A priori, it is clearly possible that the model fit (blue line) and the subdata OLSfit (red line) would have significant di�erences, as the red line only optimizes withrespect to the subdata, whereas the blue line has to fit for all the data combined from
42

each of the four (or six) graphs. Apparently, the di�erences being relatively small,this is not the case. In overall, we seem to have a reasonable good fit when comparingthe model and the subdata OLS fits.
4.2.4 Variability of the data
Finally we see the model fit in the Figure 4.5. Observe that now, according to themodeling, the vertical axis is for the logit Pr (FP).
43

600 650 700 750 800 850
−6−5
−4−3
−2−1
log(Age(month))
logit(P
r(FP))
prevFP=0, irregular=0
R2 = 0.459
600 650 700 750 800 850−6
−5−4
−3−2
−1log(Age(month))
logit(P
r(FP))
prevFP=0, irregular=1
R2 = 0.0342
600 650 700 750 800 850
−6−5
−4−3
−2−1
log(Age(month))
logit(P
r(FP))
prevFP=1, irregular=0
R2 = 0.0571
600 650 700 750 800 850
−6−5
−4−3
−2−1
log(Age(month))
logit(P
r(FP))
prevFP=1, irregular=1
R2 = −0.00389
Figure 4.5. Model fit.
The model seems to explain significant part of the variability in the first graph(adjusted R
2 = 0.459). Also we saw already in the previous Figures, that in the mosttypical case of prevFP = 0, irregular = 0, we have a very good fit when comparedto the subdata fit, where adjusted R
2 = 0.594. In the other cases, the adjusted R
2 is,however, rather low.
The idea in the di�erent Figures is that the fitted value raises especially in cases
44

where the prevFP = 1, meaning that the probability rises. Even though the otherfits do not explain the variability in the same level, the values are higher, with astatistically significant di�erence. The model does not explain the variation in thedataset but it shows the di�erence in the probability levels. Indeed, while we havesignificant di�erences in the fitted values, we also need to consider the variability ofthe data explained by the model.
Because the adjusted R
2 is really low, it raises the question about the reliability ofthe model. In particular, the bootstrapping heavily relies on the model being the truedata generating process. This clearly undermines the reliability of our results. On theother hand, the dataset we are using is very large compared to many of the typicallongitudinal settings. Relying on the size of the dataset it is reasonable to assume thatthe GEE estimates are very close to the true ones. The problem, if any, rises fromthe bootstrapping based calculation of the confidence intervals, and these estimatesshould be considered with caution.
45

5 Results
In this thesis, we produced a retrospective cohort study concerning the Finnish breastcancer screening program. The cohort was chosen to include the women who were50–51 years old at the time of their first mammography invitation in 1992–1995.
We used generalized estimating equations to model the probability of a false-positivetest result in a screening examination during the 10 biennial screening examinationsin the Finnish 20-year breast cancer screening program. The cumulative probabilitywas then calculated by these estimates with the formula (3.41) which is based onan iterative use of the conditional probability. The calculation of the cumulativeprobability assumes that women attend screenings every two years starting from age50.
Previous studies from Denmark and Italy (Njor et al., 2007; Puliti et al., 2011)estimated the cumulative risk of a FP screening result in a 10-visit program tobe 15.2–15.8%. In Norway and Spain, in turn, the estimated cumulative risk of aFP test result has been estimated at 20% (Roman et al., 2012, 2013). While theseEuropean studies are the most comparable to ours, we also point out that in theUSA the cumulative risk has been demonstrated to be significantly higher, 41.6–49.1% (Hubbard et al., 2011; Christiansen et al., 2000; Elmore et al., 1998).
Our modeling estimates the cumulative probability of at least one FP screening resultduring 10 screening examinations to be 15.84% (95% CI: 15.49–16.18%) among the81, 435 attendees. The odds ratios for age and regularity of the attendance were 0.61,1.46, respectively. For one or more previous FP screening results the correspondingodds ratios were 1.91 and 3.09 respectively. Women with irregular attendance andprevious FP result have increased risk of receiving FP screening result.
There were altogether 2,430 women who attended 10 screenings. Out of these women15.54% received at least one false-positive test result. The observed risk beingrelatively close to the model-fitted value, our modeling seems to explain the data,and also the underlying phenomena, relatively well.
The cumulative probability of at least one FP screening result is shown in the Figure5.1 together with the estimated confidence intervals.
46

3.55
5.88
7.71
9.26
10.62
11.84
12.96
13.98
14.94
15.84
3.61 2.47 2.01 1.75 1.57 1.45 1.36 1.29 1.24 1.2
0
5
10
15
50 52 54 56 58 60 62 64 66 68Age
Prob
abilit
y (%
)Cumulative probability of a false positive result
Figure 5.1. Estimated cumulative probability of a false-positive screening testresult by using generalized estimating equations.
We also calculated the probability of receiving at least one FP at certain age (cf.the bar graphs) by using the conditional probability (3.40). Here the probability was
47

calculated with the condition of woman attending, having no previous FP results andwoman either being irregular or regular attendee. The point estimates for every agegroup is shown in the Figure 5.1. We observe that the probability is not preciselythe same as in the cumulative probability. This is due to allowing the attendeeto be "irregular" as defined in the modeling. For the cumulative probability, weinstead account only the women who attend all ten screenings, implying that all theattendances are specified as "regular".
Observe that here we also need to model whether the attendee is regular or notaccording to (3.40). To be completely precise, justifying this calculation wouldrequire us to check whether the model for the attendance being regular or not iscorrectly specified. In our analysis, we used age as a linear explanatory variablein the logit-model for the irregularity of attendance. However, we did not checkin detail whether this is the correct model. We acknowledge that this may have asmall impact on our estimates, and reduces their reliability. Nevertheless, we believethese estimates to be somewhat reasonable, and since our emphasis is rather on thecumulative probability, we bypass the more thorough analysis.
48

6 Discussion and conclusion
We estimated that approximately one in every six women, who attend the biennial 20-year Finnish breast cancer screening program, will be recalled for further examinationwith at least one false-positive screening result. This result is similar to the otherEuropean screening programs (Hofvind et al., 2012; Roman et al., 2013; Njor et al.,2007; Puliti et al., 2011). The estimates in the U.S. are higher (Hubbard et al., 2011;Elmore et al., 1998; Christiansen et al., 2000).
Estimates on the cumulative probability of FP screening result rate vary between or-ganized screening programs. This can be explained by the di�erences in the screeningprograms, management policies and screening interval (Smith-Bindman et al., 2005).There are various factors that can have an e�ect on the probability of a woman receiv-ing a false-positive screening test result. These factors can relate to either screeningprogram itself or the characteristics of a woman (Roman et al., 2014; Castells et al.,2006; Christiansen et al., 2000).
The estimation of Pr (FP) is an immensely di�cult problem. The number of factorscontributing to physician decisions, to recall the woman for further examination,are very large, including the complete patient history, data of biomarkers, and alsofamily medical history. The increased risk of receiving a FP screening result after aprevious FP test result could indicate, that there might be the same transformation inthe breast tissue which was already interpreted as a previous false-positive test result.
The radiologist performance has been suggested to be one of the explanations in thevariation of the recall rates and false-positive screening results between the countriesand organised screening programs (Elmore et al., 2009). Roman et al. (2013) elabo-rate on di�erent recall rates for further assessment. They discuss possible di�erencesin mammography reading procedures, whether it is independent double reading (Eu-rope) or single reading (USA). The diagnostic performance of a radiologist is relatedto the radiologist’s years of experience and number of mammograms interpreted(Elmore et al., 2009).
There is also a di�erence in the recommendation to read certain number of screeningmammograms per year between the countries. The European guidelines for qualityassurance in breast cancer screening and diagnosis recommend that radiologist readat least 5000 screening mammograms annually (Perry et al., 2006). The di�erencemight also be among the physicians, whether the mammogram is interpreted byspecialised physician or by general radiologist. In addition, perhaps any kind ofuncertainty, whether the physician interprets any kind of abnormality, might triggerthe recall just in case.
Moreover, since a received FP result might influence the attendance for the nextscreening examinations (Salz et al., 2011), the radiologist might also have a reducednumber or previous mammographies to compare the result in later rounds. In other
49

words, FP results are related to irregular later screening attendance, further a�ectingthe radiologist decision making.
There are also individual characteristic of a woman that may increase the risk ofreceiving a FP result from screening. As stated by Castells et al. (2006) the factorsassociated with a higher cumulative risk of false-positive recall include previousbenign breast disease, premenopausal status, body mass index above 27, 3 and age50–54 years. In particular, women should be informed about the risk of receivinga FP test result if they attend regularly breast cancer screenings. It would also beimportant to inform the women about the likelihood of experiencing a false-positivescreening result based on certain risk factors that increase the probability of receivinga false-positive test result.
Altogether, there is a very large number of possible reasons for a false-positivemammography test result. Therefore, it is unreasonable to expect a perfect, nearperfect, or even a good general fit with such a simple model, as used in this work.In particular, we have only used the variables based on previous literature (Romanet al., 2013; Baker et al., 2003), and we have deliberately avoided any kind of adhoc reasoning where the variables or the modeling are retrospectively fitted for thespecific data in hand.
A natural extension would be to include a larger number of relevant variables intothe modeling, but in the present case, we are restricted by data availability. In anycase, similarly to the existing literature (Roman et al., 2013; Baker et al., 2003), anddue to the large dataset, we expect our approach to be su�cient for estimating thecumulative risk of a false-positive test result in the 10-visit 20-year Finnish screeningprogram.
We would like to point out that the modeling methods for estimating the cumulativeprobability of a false-positive screening result also vary depending on the dataavailability and assumptions made about the independence of the screening rounds(Hubbard et al., 2011; Baker et al., 2003; Gelfand and Wang, 2000).
We obtained the cumulative risk of a FP test result in the biennial 20-year screeningprogram to be 15.84%. While the cumulative probability seems to fit the data,our modeling does not explain the variability we observe. This raises the questionwhether our estimates are reliable. The asymptotic behavior of GEE rely on themodel being correctly specified. This assumption applies also for the bootstrappingmethod applied for the confidence intervals. Since the model does not explain thevariability, it indicates that the model is not necessarily completely correct. On theother hand, GEE produce an unbiased estimator of the parameter vector, with theproper asymptotic large sample distribution. Thus, it seems safe to assume, thatGEE provides asymptotically correct modeled probabilities, even if the confidenceintervals would not be completely justified.
On the other hand, the observed cumulative risk 15.54 being very close to the model-fitted cumulative probability of a false-positive screening result 15.84, our modelingseems to explain the data relatively well. Indeed, in the standard case of no previous FP
50

test results, with regular attendance habits, and with the logarithmically transformedage variable, we receive an adjusted R
2-value of 0.459, which is rather high. Inparticular, this is the case, which dominates in our calculation of the cumulativeprobability, which further supports our conclusions.
Considering the data, we also saw a substantially di�erent behavior among the womenwho had more than 1 previous FP test results. Indeed, in this case the probability ofyet another FP result seemed to be increasing with age. To best of our knowledge,this kind of behavior has not been observed in earlier studies. Additional studiesare needed, in order to verify or confirm this observation. Moreover, our modelingdoes not fit into this case, and does not aim to explain the phenomena. Instead, weconcentrate on the cumulative probability of an FP test result, where the dominatinge�ect comes from the standard attendee with no previous FP test result and withregular attendance habits.
Finally, we acknowledge another question; namely that of how many women receivea false-positive result in the whole population regardless how many times they attendthe screenings or whether they attend at all. This can be seen as the burden of thepopulation based screening program to the society with respect to the disadvantagesof FP screening results. In this study 12.3% received at least one false-positivescreening result. However, this does not take into account, that all the women havenot yet finished the whole screening program. Nevertheless, this question would beinteresting to study, although we do not cover this issue.
51

References
Agresti, A. (2015). Foundations of Linear and Generalized Linear Models. JohnWiley & Sons.
Baker, S.G., Erwin, D., and Kramer, B.S. (2003). Estimating the cumulative risk offalse positive cancer screenings. BMC Medical Research Methodology, 3(1), 1.
Ballinger, G.A. (2004). Using generalized estimating equations for longitudinal dataanalysis. Organizational Research Methods, 7(2), 127–150.
Bond, M., Pavey, T., Welch, K., Cooper, C., Garside, R., Dean, S., and Hyde, C.(2013). Systematic review of the psychological consequences of false-positivescreening mammograms. Health Technology Assessment, 17(13), 1–170.
Brett, J., Bankhead, C., Henderson, B., Watson, E., and Austoker, J. (2005). Thepsychological impact of mammographic screening. A systematic review. Psycho-Oncology, 14(11), 917–938.
Brodersen, J., and Siersma, V.D. (2013). Long-term psychosocial consequences offalse-positive screening mammography. The Annals of Family Medicine, 11(2),106–115.
Bull, A.R., and Campbell, M.J. (1991). Assessment of the psychological impactof a breast screening programme. The British Journal of Radiology, 64(762),510–515.
Castells, X., Molins, E., and Macià, F. (2006). Cumulative false positive recall rateand association with participant related factors in a population based breast cancerscreening programme. Journal of Epidemiology and Community Health, 60(4),316–321.
Christiansen, C.L., Wang, F., Barton, M.B., Kreuter, W., Elmore, J.G., Gelfand,A.E., and Fletcher, S.W. (2000). Predicting the cumulative risk of false-positivemammograms. Journal of the National Cancer Institute, 92(20), 1657–1666.
Elmore, J.G., Barton, M.B, Moceri, V.M., Polk, S., Arena, P.J., and Fletcher, S.W.(1998). Ten-year risk of false positive screening mammograms and clinical breastexaminations. New England Journal of Medicine, 338(16), 1089–1096.
Elmore, J.G., Jackson, S.L., Abraham, L., Miglioretti, D.L., Carney, P.A., Geller,B.M., Yankaskas, B.C., Kerlikowske, K., Onega, T., Rosenberg, R.D., et al. (2009).Variability in interpretive performance at screening mammography and radiolo-gists’ characteristics associated with accuracy. Radiology, 253(3), 641–651.
EU Council (2003). EU Council Recommendation (EC) 878/2003 of 2 December2003 on cancer screening. O�cial Journal of the European Union, L327, 34–38.
Finnish Cancer Registry (FCR, 2010). Mass screening. Breast Cancer Screen-ing. Retrieved (August 24, 2016) from http://www.cancer.fi/syoparekisteri/en/mass-screening-registry/breast_cancer_screening/.
52

Fitzmaurice, G.M., Laird, N.M., and Ware, J.H. (2012). Applied longitudinal anal-ysis. Vol. 998. John Wiley & Sons.
Gelfand, A.E., and Smith, A.F.M. (1990). Sampling-based approaches to calculatingmarginal densities. Journal of the American Statistical Association, 85(410),398–409.
Gelfand, A.E., and Wang, F. (2000). Modelling the cumulative risk for a false-positiveunder repeated screening events. Statistics in Medicine, 19(14), 1865–1879.
Halekoh, U., Højsgaard, S., and Yan, J. (2006). The R package geepack for generalizedestimating equations. Journal of Statistical Software, 15(2), 1–11.
Hardin, J.W. (2005). Generalized estimating equations (GEE). Wiley Online Library.
Harris, R.P., Sheridan, S.L., Lewis, C.L., Barclay, C., Vu, M.B., Kistler, C.E., Golin,C.E., DeFrank, J.T., and Brewer, N.T. (2014). The harms of screening: a proposedtaxonomy and application to lung cancer screening. JAMA Internal Medicine,174(2), 281–286.
Heinävaara, S., Sarkeala, T., and Anttila, A. (2014). Overdiagnosis due to breastcancer screening: updated estimates of the Helsinki service study in Finland.British Journal of Cancer, 111(7), 1463–1468.
Hofvind, S., Thoresen, S., and Tretli, S. (2004). The cumulative risk of a false-positive recall in the Norwegian Breast Cancer Screening Program. Cancer,101(7), 1501–1507.
Hofvind, S., Ponti, A., Patnick, J., Ascunce, N., Njor, S., Broeders, M., Giordano,L., Frigerio, A., and Törnberg, S. (2012). False-positive results in mammographicscreening for breast cancer in Europe: a literature review and survey of servicescreening programmes. Journal of Medical Screening, 19(suppl 1), 57–66.
Hubbard, R.A., Miglioretti, D.L., and Smith, R.A. (2010). Modelling the cumulativerisk of a false-positive screening test. Statistical Methods in Medical Research,19(5), 429–449.
Hubbard, R.A., Kerlikowske, K., Flowers, C.I., Yankaskas, B.C., Zhu, W., andMiglioretti, D.L. (2011). Cumulative probability of false-positive recall or biopsyrecommendation after 10 years of screening mammography: a cohort study. Annalsof Internal Medicine, 155(8), 481–492.
International Agency for Research on Cancer (IARC, 2002). IARC Handbooks ofCancer Prevention. Breast cancer screening. Vol. 7. Lyon: IARC Press.
Lauby-Secretan, B., Scoccianti, C., Loomis, D., Benbrahim-Tallaa, L., Bouvard, V.,Bianchini, F., and Straif, K. (2015). Breast-cancer screening - viewpoint of theIARC Working Group. New England Journal of Medicine, 372(24), 2353–2358.
Lerman, C., Track, B., Rimer, B.K., Boyce, A., Jepson, C., and Engstrom, P.F. (1991).Psychological and behavioral implications of abnormal mammograms. Annals ofInternal Medicine, 114(8), 657–661.
53

Liang, K-Y., and Zeger, S.L. (1986). Longitudinal data analysis using generalizedlinear models. Biometrika, 13–22.
Njor, S.H., Olsen, A.H., Schwartz, W., Vejborg, I., and Lynge, E. (2007). Predictingthe risk of a false-positive test for women following a mammography screeningprogramme. Journal of Medical Screening, 14(2), 94–97.
Otten, J.D.M., Fracheboud, J., Den Heeten, G.J., Otto, S.J., Holland, R., De Kon-ing, H.J., Broeders, M.J.M., and Verbeek, A.L.M. (2013). Likelihood of earlydetection of breast cancer in relation to false-positive risk in life-time mammo-graphic screening: population-based cohort study. Annals of Oncology, 24(10),2501–2506.
Perry, N., Broeders, M., de Wolf, C., Törnberg, S., Holland, R., and von Karsa, L.(2006). European guidelines for quality assurance in breast cancer screeningand diagnosis. Luxembourg: O�ce for O�cial Publications of the EuropeanCommunities.
Puliti, D., Miccinesi, G., and Zappa, M. (2011). More on Screening mammography.The New England Journal of Medicine, 364, 281–286.
Puliti, D., Du�y, S.W., Miccinesi, G., De Koning, H., Lynge, E., Zappa, M., andPaci, E. (2012). Overdiagnosis in mammographic screening for breast cancer inEurope: a literature review. Journal of Medical Screening, 19(1), 42–56.
R Development Core Team (2008). R: A Language and Environment for StatisticalComputing. R Foundation for Statistical Computing, Vienna, Austria. ISBN3-900051-07-0.
Roman, M., Skaane, P., and Hofvind, S. (2014). The cumulative risk of false-positive screening results across screening centres in the Norwegian Breast CancerScreening Program. European Journal of Radiology, 83(9), 1639–1644.
Roman, M., Hubbard, R.A., Sebuodegard, S., Miglioretti, D.L., Castells, X., andHofvind, S. (2013). The cumulative risk of false-positive results in the NorwegianBreast Cancer Screening Program: Updated results. Cancer, 119(22), 3952–3958.
Roman, R., Sala, M., Salas, D., Ascunce, N., Zubizarreta, R., Castells, X., et al.(2012). E�ect of protocol-related variables and women’s characteristics on thecumulative false-positive risk in breast cancer screening. Annals of Oncology,23(1), 104–111.
Salas, D., Ibáñez, J., Román, R., Cuevas, D., Sala, M., Ascunce, N., Zubizarreta,R., Castells, X., et al. (2011). E�ect of start age of breast cancer screeningmammography on the risk of false-positive results. Preventive Medicine, 53(1-2),76–81.
Salz, T., DeFrank, J.T., and Brewer, N.T. (2011). False positive mammograms inEurope: do they a�ect reattendance? Breast Cancer Research and Treatment,127(1), 229–231.
54

Sarkeala, T., Heinävaara, S., and Anttila, A. (2008a). Breast cancer mortality withvarying invitational policies in organised mammography. British Journal of Can-cer, 98(3), 641–645.
Sarkeala, T., Heinävaara, S., and Anttila, A. (2008b). Organised mammographyscreening reduces breast cancer mortality: a cohort study from Finland. Interna-tional Journal of Cancer, 122(3), 614–619.
Smith-Bindman, R., Ballard-Barbash, R., Miglioretti, D.L., Patnick, J., and Ker-likowske, K. (2005). Comparing the performance of mammography screening inthe USA and the UK. Journal of Medical Screening, 12(1), 50–54.
Ministry of Social A�airs and Health (2006). Ministry of Social A�airs andHealth. Government Decree on Screenings (1339/2006). http://www.finlex.fi/en/laki/kaannokset/2006/en20061339.pdf.
Varadhan, S.R.S. (2001). Probability theory (Vol. 7). American MathematicalSociety.
Yan, J. (2002). Geepack: Yet another Package for Generalised Estimating Equations.R-News 2/3: 12–14.
Yan, J., and Fine, J. (2004). Estimating equations for association structures. Statisticsin Medicine, 23(6), 859–874.
55