Cultural factors impacting misdiagnosis of PTSD in …...Cultural factors impacting misdiagnosis of...
1
Cultural factors impacting misdiagnosis of PTSD in a Puerto Rican female Lorangelly Rivera, MD and Telva Olivares, MD Department of Psychiatry, University of Rochester Medical Center • Hispanics are the fastest growing ethnic group in the US and are expected to make up more than 20% of the US population by 2060 • Several studies have shown that 10–25% of the general (non-psychiatric) Latino population have had hallucinatory experiences, both visual and auditory, with no identified underlying psychiatric issue 1 • Despite high prevalence of psychotic symptoms in this population most patients do not meet criteria for a thought disorder 2 • Various factors including language barrier, difference in beliefs, tendency to under report certain symptoms, racial bias, and decreased access to care are some of the factors that complicate formulation of a correct assessment and accurate diagnosis in this population • We will discuss factors leading to an initial diagnosis of Schizophrenia in a Puerto Rican female later found to have PTSD Case report • This is the case of a 79 year old Puerto Rican woman with a medical history significant for SCC of the lung (s/p radiation tx) , PVD, T2DM and HTN and a psychiatric history of Depression and Schizophrenia who presented with a chief complaint of depression. She was referred by her PCP who was prescribing Quetiapine 800mg nightly and Fluoxetine 20 mg daily. • Psychiatric ROS: • + : depressed mood, sleep disturbances, persistent feelings of guilt, low energy, low appetite, low concentration, anhedonia, hopelessness, anxious mood, racing thoughts, ruminations and intermittent suicidal ideation without intent. She auditory, visual and tactile hallucinations (felt that she was held while in bed, heard a male voice, heard whispers during the day, sees shadows in the corner of her eye) that occur independent of mood symptoms and do not improve with Quetiapine. • - : paranoid delusions, ideas of reference, thought insertion/broadcasting, symptoms of mania, flashbacks, trauma related nightmares, panic attacks, violent/homicidal ideation, intent or plan. • Medical ROS: Constitutional: positive for fatigue, Musculoskeletal: positive for stiff joints and tongue movements. Neurological: positive for memory problems • Past History: Multiple hospitalizations in Puerto Rico for depression. Trauma history of childhood physical, emotional and verbal abuse from her mother and domestic violence from ex husband. One episode of suicidal attempt with low lethality where she wrapped a rope around her neck but did not attempt to hang herself and had no medical repercussions. Family history was non- contributory. Interventions and results • MSE: Appears stated age, Well-groomed, Casual. Cooperative with interview. Motor activity was within normal limits. Direct eye contact. Slurred speech. Affect was depressed with decreased range. Mood was depressed. Thought process was linear, logical and goal oriented. Though content was normal without unusual themes. Perception was within normal limits and there was no evidence of internal preoccupation. She endorsed vague passive thoughts of suicide. Concentration was initially impaired but improved as interview progressed. Remote memory was intact and recent memory was impaired. Orientation was intact to person and place but not to time. Cognitive function was average Judgement and Insight were intact. • Week 1: Quetiapine was discontinued. Fluoxetine was increased to 40mg. Trazodone was started at 50mg nightly. • Week 3: Trazodone was increased to 100mg. Resolution of tremors and tongue movements was seen. • Week 4: Visible improvement in mood. Fluoxetine 40mg and Trazodone 100mg were continued. Intermittent AVH endorsed without changes to thought content. References Differential diagnosis • Hispanics with depression and anxiety commonly describe atypical auditory and visual hallucinations in the context of an otherwise unremarkable mental status exam • Approximately one in ten Latinos in a US national probability sample endorsed at least one lifetime psychotic symptom on the CIDI screener. Diagnostic evaluation, however, revealed that only 7% of Latinos in the NLAAS who endorsed psychotic symptoms met SCID criteria for psychotic disorder 4 • Examples of psychosis-like symptoms include hearing “someone calling”, “knocking at the door” or the “phone ringing in the house” • Symptoms are commonly based around religion and family (eg seeing a dead relative) and occur independently of disorganization of thought • Limited data has shown that neuroleptics are not more efficacious at treating these attenuated psychotic symptoms when compared to antidepressants or anxiolytics 5 • Non psychotic hallucinations can be easily misinterpreted as a symptom of a thought disorder by clinicians who lack cultural training or experience with latinx population • Patients may minimize trauma related symptoms and multiple evaluations may be necessary to make accurate diagnosis • Non psychotic experiences should be considered in all cases where symptoms occur independently of a progressive cognitive process • Though not related to a primary thought disorder NPH increase risk of poor social functioning and suicide • Even in patients with co-morbid mood or anxiety disorders, NPH can occur during moments of stabilization and interview should focus on patient’s reported experience of symptoms • Antipsychotics may have a role in treatment of NPH in certain patients but do not appear to have an impact on outcomes Discussion 1. Moreira-Almeida, A., & Koss-Chioino, J. D. (2009). Recognition andtreatment of psychotic symptoms: Spiritists compared to mental health professionals in Puerto Rico and Brazil. Psychiatry: Interpersonal and Biological Processes, 72(3), 268–283. 2. Geltman D, Chang G. Hallucinations in Latino psychiatric outpatients: a preliminary investigation. Gen Hosp Psychiatry. 2004;26(2):153-157. doi:10.1016/j.genhosppsych.2003.09.002 3. Olfson M, Lewis-Fernández R, Weissman MM, et al. Psychotic symptoms in an urban general medicine practice. Am J Psychiatry. 2002;159(8):1412-1419. doi:10.1176/appi.ajp.159.8.1412 4. Lewis-Fernández R, Horvitz-Lennon M, Blanco C, Guarnaccia PJ, Cao Z, Alegría M. Significance of endorsement of psychotic symptoms by US Latinos. J Nerv Ment Dis. 2009;197(5):337-347. doi:10.1097/NMD.0b013e3181a2087e 5. Mischoulon D, Lagomasino IT, Harmon C. Atypical psychotic symptoms in a Hispanic population: diagnostic dilemmas and implications for treatment. Psychiatry (Edgmont). 2005;2(10):38-46. 6. Cassano P, Chang T, Trinh NH, Baer L, Fava M, Mischoulon D. Differential impact of isolated psychotic symptoms on treatment outcome of major depressive disorder in the STAR*D cohort of Whites, Blacks and Latinos. J Affect Disord. 2013;150(2):578-584. doi:10.1016/j.jad.2013.02.012 7. Lewis-Fernández R, Gorritz M, Raggio GA, Peláez C, Chen H, Guarnaccia PJ. Association of trauma-related disorders and dissociation with four idioms of distress among Latino psychiatric outpatients. Cult Med Psychiatry. 2010;34(2):219-243. doi:10.1007/s11013-010- 9177-8 Non psychotic hallucinations Introduction Schizoaffective disorder MDD with psychotic features Complex PTSD Schizotypal personality disorder MDD with anxious distress Schizophrenia MDD with psychotic features and PDD PTSD and GAD Figure 1. Relational representation of pertinent diagnosis 18 16 3 1 2 3 4 5 6 7 8 9 10 PHQ 9 PHQ 9 Weeks • Week 10: Gains maintained with no psychotropic changes. • Month 9: PHQ 9 remains negative. Intermittent non distressing AVH endorsed. Medication adherence endorsed
Transcript of Cultural factors impacting misdiagnosis of PTSD in …...Cultural factors impacting misdiagnosis of...

Cultural factors impacting misdiagnosis of PTSD in a Puerto Rican female Lorangelly Rivera, MD and Telva Olivares, MD
Department of Psychiatry, University of Rochester Medical Center
• Hispanics are the fastest growing ethnic group
in the US and are expected to make up more
than 20% of the US population by 2060
• Several studies have shown that 10–25% of
the general (non-psychiatric) Latino population
have had hallucinatory experiences, both visual
and auditory, with no identified underlying
psychiatric issue 1
• Despite high prevalence of psychotic symptoms in this population most
patients do not meet criteria for a thought disorder 2
• Various factors including language barrier, difference in beliefs, tendency to
under report certain symptoms, racial bias, and decreased access to care are
some of the factors that complicate formulation of a correct assessment and
accurate diagnosis in this population
• We will discuss factors leading to an initial diagnosis of Schizophrenia in a
Puerto Rican female later found to have PTSD
Case report• This is the case of a 79 year old Puerto Rican woman with a medical history
significant for SCC of the lung (s/p radiation tx) , PVD, T2DM and HTN and a
psychiatric history of Depression and Schizophrenia who presented with a
chief complaint of depression. She was referred by her PCP who was
prescribing Quetiapine 800mg nightly and Fluoxetine 20 mg daily.
• Psychiatric ROS:
• + : depressed mood, sleep disturbances, persistent feelings of guilt, low energy,
low appetite, low concentration, anhedonia, hopelessness, anxious mood, racing
thoughts, ruminations and intermittent suicidal ideation without intent. She auditory,
visual and tactile hallucinations (felt that she was held while in bed, heard a male voice,
heard whispers during the day, sees shadows in the corner of her eye) that occur
independent of mood symptoms and do not improve with Quetiapine.
• - : paranoid delusions, ideas of reference, thought insertion/broadcasting, symptoms of
mania, flashbacks, trauma related nightmares, panic attacks, violent/homicidal ideation,
intent or plan.
• Medical ROS: Constitutional: positive for fatigue, Musculoskeletal: positive
for stiff joints and tongue movements. Neurological: positive for memory
problems
• Past History: Multiple hospitalizations in Puerto Rico for depression. Trauma
history of childhood physical, emotional and verbal abuse from her mother and
domestic violence from ex husband. One episode of suicidal attempt with low
lethality where she wrapped a rope around her neck but did not attempt to
hang herself and had no medical repercussions. Family history was non-
contributory.
Interventions and results
• MSE: Appears stated age, Well-groomed, Casual. Cooperative with interview.
Motor activity was within normal limits. Direct eye contact. Slurred speech.
Affect was depressed with decreased range. Mood was depressed. Thought
process was linear, logical and goal oriented. Though content was normal
without unusual themes. Perception was within normal limits and there was no
evidence of internal preoccupation. She endorsed vague passive thoughts of
suicide. Concentration was initially impaired but improved as interview
progressed. Remote memory was intact and recent memory was impaired.
Orientation was intact to person and place but not to time. Cognitive function
was average Judgement and Insight were intact.
• Week 1: Quetiapine was
discontinued. Fluoxetine was
increased to 40mg. Trazodone
was started at 50mg nightly.
• Week 3: Trazodone was
increased to 100mg. Resolution
of tremors and tongue
movements was seen.
• Week 4: Visible improvement in
mood. Fluoxetine 40mg and
Trazodone 100mg were
continued. Intermittent AVH
endorsed without changes to
thought content.
References
Differential diagnosis
• Hispanics with depression and anxiety commonly describe atypical auditory
and visual hallucinations in the context of an otherwise unremarkable mental
status exam
• Approximately one in ten Latinos in a US national probability sample endorsed
at least one lifetime psychotic symptom on the CIDI screener. Diagnostic
evaluation, however, revealed that only 7% of Latinos in the NLAAS who
endorsed psychotic symptoms met SCID criteria for psychotic disorder 4
• Examples of psychosis-like symptoms include hearing “someone calling”,
“knocking at the door” or the “phone ringing in the house”
• Symptoms are commonly based around religion and family (eg seeing a dead
relative) and occur independently of disorganization of thought
• Limited data has shown that neuroleptics are not more efficacious at treating
these attenuated psychotic symptoms when compared to antidepressants or
anxiolytics 5
• Non psychotic hallucinations can be easily misinterpreted as a symptom of a
thought disorder by clinicians who lack cultural training or experience with
latinx population
• Patients may minimize trauma related symptoms and multiple evaluations may
be necessary to make accurate diagnosis
• Non psychotic experiences should be considered in all cases where symptoms
occur independently of a progressive cognitive process
• Though not related to a primary thought disorder NPH increase risk of poor
social functioning and suicide
• Even in patients with co-morbid mood or anxiety disorders, NPH can occur
during moments of stabilization and interview should focus on patient’s
reported experience of symptoms
• Antipsychotics may have a role in treatment of NPH in certain patients but do
not appear to have an impact on outcomes
Discussion
1. Moreira-Almeida, A., & Koss-Chioino, J. D. (2009). Recognition andtreatment of psychotic symptoms: Spiritists compared to mental health
professionals in Puerto Rico and Brazil. Psychiatry: Interpersonal and Biological Processes, 72(3), 268–283.
2. Geltman D, Chang G. Hallucinations in Latino psychiatric outpatients: a preliminary investigation. Gen Hosp Psychiatry.
2004;26(2):153-157. doi:10.1016/j.genhosppsych.2003.09.002
3. Olfson M, Lewis-Fernández R, Weissman MM, et al. Psychotic symptoms in an urban general medicine practice. Am J Psychiatry.
2002;159(8):1412-1419. doi:10.1176/appi.ajp.159.8.1412
4. Lewis-Fernández R, Horvitz-Lennon M, Blanco C, Guarnaccia PJ, Cao Z, Alegría M. Significance of endorsement of psychotic symptoms
by US Latinos. J Nerv Ment Dis. 2009;197(5):337-347. doi:10.1097/NMD.0b013e3181a2087e
5. Mischoulon D, Lagomasino IT, Harmon C. Atypical psychotic symptoms in a Hispanic population: diagnostic dilemmas and implications for
treatment. Psychiatry (Edgmont). 2005;2(10):38-46.
6. Cassano P, Chang T, Trinh NH, Baer L, Fava M, Mischoulon D. Differential impact of isolated psychotic symptoms on treatment outcome
of major depressive disorder in the STAR*D cohort of Whites, Blacks and Latinos. J Affect Disord. 2013;150(2):578-584.
doi:10.1016/j.jad.2013.02.012
7. Lewis-Fernández R, Gorritz M, Raggio GA, Peláez C, Chen H, Guarnaccia PJ. Association of trauma-related disorders and dissociation
with four idioms of distress among Latino psychiatric outpatients. Cult Med Psychiatry. 2010;34(2):219-243. doi:10.1007/s11013-010-
9177-8
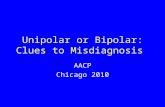
Non psychotic hallucinations Introduction
Schizoaffective disorderMDD with psychotic features
Complex PTSDSchizotypal personality
disorder
MDD with anxious distress
Schizophrenia MDD with psychotic features and PDD
PTSD and GAD
Figure 1. Relational representation of pertinent diagnosis
0
2
4
6
8
10
12
14
16
18
20
0 5 10 15 20 25
PHQ 9
1816
3
1 2 3 4 5 6 7 8 9 10
PHQ 9PHQ 9
Weeks
• Week 10: Gains maintained with no
psychotropic changes.
• Month 9: PHQ 9 remains negative.
Intermittent non distressing AVH
endorsed. Medication adherence
endorsed