
Removing the collaboration barriers for connected healthcare

0
0
Institutionen för folkhälso- och vårdvetenskap
Cultural Barriers in Healthcare Delivery
from the Perspective of Patients
Author Supervisor
Fru Ngum Awasom Johanna Sjömar
Examiner
Katarina Hjelm
Examensarbete i sjukskoterskeprogrammet, 15 hp 2021

1
ABSTRACT
Background
Many patients especially from minority backgrounds are typically faced with cultural barriers
during health care encounters and this hinders the delivery of culturally competent healthcare.
This study seeks to understand how cultural barriers faced by patients are crucial in attaining
the delivery of culturally competent healthcare.
Aims
The aim of this study is to examine cultural barriers in the delivery of healthcare services from
the patient’s perspective.
Method
The method is a literature review based on qualitative primary research. Ten articles were
selected from the CINAHL, PUBMED and Google scholar databases. All articles selected were
published between 2010 and 2020. The quality of the articles used were assessed using a review
template for qualitative studies. Data was analysed using the literature review matrix method.
Results
The results suggest that four main cultural barriers from the perspectives of patients impacted
healthcare delivery. These cultural barriers included the following; communication problems
arising during verbal and nonverbal interactions, mistrust and discrimination arising as a result
of previous contact with the health care system, socio-economic status and finally low
propensity to seek healthcare.
Conclusion
To conclude it is evident that patients face a plethora of cultural barriers during their
interactions with health care services and their experiences can be shaped by a number of
variables and factors. These cultural challenges hinder accessibility to proper health care
services might lead to inequality in the provision of health care services.
Keywords: Cultural barriers, Patients perspectives, Cultural competent care.

2
ABSTRAKT
Bakgrund
Många patienter, särskilt de med minoritetsbakgrund, står vanligtvis inför kulturella barriärer
när de blir bemötta av hälso-och sjukvårdspersonal. Detta hindrar utformandet av kulturellt
kompetent vård. Studien syftar till att förstå hur kulturella barriärer som patienter står inför är
avgörande för att uppnå kulturellt kompetent omvårdnad.
Mål
Syftet med denna studie är att undersöka kulturella barriärer vid leverans av vårdtjänster ur
patientens perspektiv.
Metod
Metoden är en litteraturstudie baserad på kvalitativ primär forskning.Tio artiklar valdes från
databaserna CINAHL, PUBMED och Google. Alla utvalda artiklar är publicerade mellan 2010
och 2020. Kvaliteten på de artiklar som valdes är granskade med hjälp av en granskningsmall
för kvalitativa studier. Data analyserades med hjälp av litteraturgranskning enligt en
matrismetod.
Resultat
Analysen och resultaten från studien tyder på att fyra huvudsakliga kulturella barrier ur
patientens perspektiv hade avgörande inverkan på bemötandet inom vården. Dessa kulturella
barriärer inkluderade följande; kommunikationsproblem som uppstår under verbala och icke-
verbala interaktionen, misstro och diskriminering till följd av tidigare kontakt med hälso- och
sjukvården, socioekonomisk status och slutligen låg benägenhet att söka vård som är vanligt
för människor med samma kulturella bakgrund.
Slutsats
Avslutningsvis är det uppenbart att patienter möter kulturella barriärer under sin interaktion
med vården och deras erfarenheter kan formas av ett antal variabler och faktorer. Dessa
kulturella utmaningar hindrar adekvat tillgång till hälso sjukvård och kan leda till ojämlikhet i
tillgången till hälso- och sjukvårdstjänster.
Nyckelord: Kulturella barriärer, Patientperspektiv, kulturellt kompetent omvårdnad.

3
TABLE OF CONTENTS
INTRODUCTION…………………………………………………………………………4
Patients perspective………………………………………………………………………..5
The Impact of Cultural Competence……………………………………………………..6
Theoretical framework ……………………………………………………………………7
Formulation of research question………………………………………………………...8
Aims of the study……………………………………………………………………,,,,…..9
METHOD………………………………………………………………………………….9
Design………………………………………………………………………………………9
Search strategy………………………………………………………………………….....10
Inclusion and Exclusion criteria…………………………………………………………11
Quality assessment of data……………………………………………………………….12
Data analysis………………………………………………………………………………12
Ethical Considerations……………………………………………………………………14
RESULTS…………………………………………………………………………………14
Communication…………………………………………………………………………,,.14
Mistrust and discrimination……………………………………………………………..16
Socio-economic status……………………………… …………………………………..17
Low propensity to seek health services………………………………………………….19
DISCUSSION ……………….……………………………………………………………19
Discussion of results……………………………………………………………………...20
Communication……………………………………………………………………………………..20
Mistrust and discrimination……………………………………………………………………….21
Socio-Economic status…………………………………………………………………………….22
Low propensity to seek health care………………………………………………………………23
Clinical relevance and basis for further research…………………………………………,24
Discussion of method…………………………………………………………………….25
Conclusion………………………………………………………………………………..26
REFERENCES…………………………………………………………………………..27
APPENDIX 1 Table presented of the quality of the reviewed articles……………….34

4
INTRODUCTION
Globalisation and migration have led to an increase in the number of patients with diverse
cultural backgrounds resulting in the need for healthcare delivery mechanisms to be culturally
friendly and competent when delivering healthcare services to patients (Ergin & Akin, 2017).
The rise of migration and globalisation has promulgated the concept of cultural competency in
healthcare delivery to patients as a major objective and outcome amongst healthcare policy
makers over the last couple of decades. Several studies have defined cultural competency from
different perspectives including the organisational, individual and societal, and the education
of healthcare students at various levels (Hultjö, Bachrach-Lindström, Safipour & Hadziabdic,
2019). However, most of the definitions are all grounded in the seminal work of Cross, Bazron,
Denis and Isaacs (1989). These authors conceptualise cultural competence as:
…a set of congruent behaviours, attitudes, and policies that come
together in a system, agency or among professionals and enable that
system, agency or those professions to work effectively in cross-cultural
situations (Cross et al., 1989, p 7)
In their monograph, Cross et al (1989) opine that the definition of culture is used to signify the:
¨integrated pattern of human behavior that includes thoughts,
communications, actions, customs, beliefs, values, and institutions of a
racial, ethnic, religious, or social group” (Cross et al., 1989, p 7)
On the other hand, the word competence is used to describe the effectiveness of a system. Thus,
according to Cross et al.’s seminal work, a culturally competent system of care;
”…acknowledges and incorporates at all levels--the importance of
culture, the assessment of cross-cultural relations, vigilance towards the
dynamics that result from cultural differences, the expansion of cultural
knowledge, and the adaptation of services to meet culturally-unique
needs” (Cross et al., 1989, p 7)
Handtke, Mösjo and Schiligen (2019), argue that cultural competence plays an important role
in resolving problems faced by ethnic minority patients who are often the primary victims of
cultural barriers in the delivery of healthcare. Achieving cultural competence entails joint

5
collaboration from various healthcare stakeholders such that the quality of healthcare services
rendered to patients are not compromised irrespective of their cultural background including
their race, ethnicity and religious beliefs (Saha, Beach & Cooper, 2008).
Patients Perspectives
As mentioned earlier, attaining cultural competent care is a collaborative effort which includes
many stakeholders including patients and healthcare practitioners. Drawing from the
perspectives of patients, Cornelison (2001) argues that cultural barriers faced in the healthcare
sector affect the quality of services patients receive. This situation is further exacerbated by
patients’ inability to understand the cultural context and environment in which healthcare
services are delivered. Patients’ stereotypes about health professionals impact the manner in
which they interpret their professional support. For example, patients have different ways
through which they respond and manage pain including stereotypes and perceptions harboured
by healthcare professionals about patients from minority and different backgrounds
(Cornelison, 2001).
Ngo-Metger et al (2006) state that the provision of culturally competent care is an effective
strategy used to reduce or eliminate disparities in service quality among people from different
ethnic, racial or cultural backgrounds. These authors highlight five cultural barriers cited by
patients as crucial in health care delivery; experiences of discrimination; patient – health
provider communication; experiences affecting trust or distrust; respecting patient preferences
or engaging patient in decision-making and linguistic ability. They argue that patients
especially from minority populations are sensitive to the provision of culturally competent
healthcare and this is only achievable when the patients' cultural perspectives and dimensions
highlighted above are effectively incorporated in existing conventional measures to improve
the quality of healthcare delivery. Achieving culturally competent care is a challenging task
given that many healthcare providers tend to be unaware of their deficiencies in the provision
of culturally competent care. This is so because people from minority racial and ethnic groups
tend to give lower ratings about the quality of care they received across healthcare service
providers in the country (Ellins & Glasby, 2016). This suggests there is a need to improve
responsiveness to the needs of minority service users.
In the same light, Saha et al (2008) argue that cultural competence and patient centeredness
have been promoted over the last several years as benchmarks in the practice of contemporary

6
health service provision. The authors argue that adopting a patient centred approach ensures
that patients’ perspectives are considered during decision making. Patient centeredness
contributes to an improvement in the quality of services delivered because the ultimate goal of
health service provision is to restore the health of patients or support them to cope with their
condition. The underlying motive of patient-centred service is to achieve these goals and
patient satisfaction with the quality of services received and to equally respond to the needs of
patients during illness while taking into consideration their beliefs and values (Hjelm, Bard,
Nyberg & Apelquist, 2003; Hjelm & Nambozi, 2008).
The Impact of Cultural competence
There is a general consensus about the positive impact of cultural competence on healthcare
service quality. Betancourt, Green, Carilla and Park (2005) note that cultural competence
improves quality of care and eliminates ethnic/racial disparities in the quality of health care
services. Betancourt et al (2005), conducted primary research on cultural competence and
interviewed government, management and patients to get their perspectives and found that
many health care stakeholders were both conscious of the importance of cultural competence
and were working to develop initiatives that improve cultural competence. Raja et al (2015),
pointed out that achieving cultural competence is a complex task that requires the collaboration
of various healthcare stakeholders and support from the minority communities. These
communities need to cooperate by identifying their challenges and the factors which they deem
key contributors to low quality health. This approach will ensure that cultural competency
interventions are tailored to meet the challenges that they are designed to tackle.
There is an overwhelming general consensus that cultural barriers have an adverse impact on
the quality of healthcare services received by patients especially from minority backgrounds.
Furthermore, these studies suggest that the primary victims of cultural barriers existing in the
healthcare sector are patients from minority backgrounds. The main sources of cultural barriers
amongst patients include language, religious beliefs, ethnicity, and other socio-economic
factors that hinge on cultural stereotypes and biases (Raja et al, 2015; Betancourt et al, 2005).
This study also highlights a general consensus amongst scholars that it is crucial to
continuously improve cultural competency through providing person centred services to
diverse groups of patients .

7
Theoretical Framework
This study is conducted within the underlying assumptions and framework of Leininger's
Culture Care Theory (Leininger, 1991; Leininger, 1994). This theory gives insights into a
holistic and cultural care worldview of a configuration of factors that are crucial in shaping the
wellbeing of patients and the practice of nursing. These include several cultural and socio-
structural factors such as religion, philosophical beliefs, kinships systems, social status,
politics, economics, and lifestyles, the environmental context, language, and ethno-history.
These factors are crucial in shaping the wellbeing of patients because they are embedded and
intertwined with people’s cultural values and belief systems. Figure 1 illustrates some of the
important factors and components of the Culture Care Theory and its relationship and relevance
in shaping cultural competent care delivery to diverse groups of patients worldwide.
Figure 1. Leininger’s Sunrise Model to depict Theory of Culture Care Diversity and
Universality (McFarland & Wehbe-Alama, 2019 p. 542).

8
The main assumption here is that if all these factors are incorporated during the care process,
then health care professionals such as nurses would be able to provide holistic care to patients
of all backgrounds, including the under-privileged and undeserving. The theory therefore
provides a robust framework through which issues of culture, values and belief with the
provision of health care can be understood and explored (McFarland & Wehbe-Alama, 2019)),
In this light the Cultural Care Theory is relevant in understanding this study for the following
reasons; Firstly, the cultural care theory has been chosen because of its relevance in attempting
to explain culturally congruent nursing care practices that could be used to deliver health care
to diverse individuals, families, groups, communities and institutions.
Secondly, the theory is unique and remains the only nursing theory which explicitly focuses on
culture care. It helps to better explain the problem of cultural barriers from both the nursing
and patient perspective making it a more comprehensive model (McFarland & Wehbe-Alama,
2019).
Thirdly, the cultural care theory is holistic and covers a broad immersion of factors and
components such as politics, beliefs, values, religion and economics that are intrinsically linked
to the cultural attitudes and perspectives of patients (Leininger, 1991; Leininger, 1994). The
theory lays emphasis on care values, beliefs, lifestyles and other socio-cultural dimensions. It
seeks to explore culturally based factors that play a key role in promoting the health and well-
being of individual patients, families, or groups (Leininger, 1991; Leininger, 1994). Finally,
the components of the theory will facilitate the choice and selection of the relevant articles
based on prior themes in our general review and analysis of literature on the cultural barriers
faced by patients during healthcare delivery.
Formulation of Research Question
Today, because of the diverse backgrounds of most patients and their cultural attributes and
expectations, the provision of healthcare services is increasingly challenged to provide
culturally competent care that meets the needs of the diverse patient populations (McFarland
& Wehbe, 2015). Health care professionals are now expected to acknowledge patients’ and
families’ cultural differences and incorporate their beliefs and values in their treatment and
care plan (Wasserman et al., 2014). For example, in Sweden, Hultsjö and Hjelm (2005) found
that the main problems faced by nurses and other healthcare practitioners included difficulties

9
related to caring for asylum-seeking refugees. Nurses reported some unexpected behaviours
amongst migrants because of cultural differences. For example, some migrants refused to eat
or drink in the psychiatric ward because they were not familiar with most of the types of food
served. The challenge is huge because providing culturally competent care has become a
strategic priority in healthcare organisations not just in the cosmopolitan cities, but at the
national level (Almutairi, Gardner & McCarthy, 2013). Nurses are therefore under increasing
pressure to better manage cultural barriers that are likely to have a negative impact on the
quality of services they provide to service users.
Although healthcare professionals receive the theoretical and practical training required to look
after patients, cultural barriers affect and shape the quality of healthcare services delivered to
patients. This problem is exacerbated by the fact that globalisation has resulted in a more
culturally diverse population across the northern hemisphere as people with diverse cultural
backgrounds travel to Britain, Europe, North America and Australia in search of better
economic opportunities and livelihood and are consequently part of the patient’s population
needing culturally competent healthcare (Hull, 2016).
Aim of the study
The aim of this study is to examine cultural barriers in the delivery of healthcare services from
the patient’s perspective.
METHOD
Design
This study is a general literature review based on qualitative studies of the general literature
review framework and protocol recommended for nursing research practice (Polit & Beck,
2017). A literature review is a summary of a research topic aimed at placing the research
question in context. This method was suitable because it helped in understanding the current
state of knowledge regarding the patients´ perspective on cultural barriers in health care
delivery. This design was also appropriate because it enabled data to be collected
systematically and analysed coherently.

10
Search strategy
The search of relevant literature was conducted on three main databases including CINAHL,
and PUBMED and Google scholar. These databases were chosen because they were reputable
for the vast variety and quantity of journal articles they contain. Each of these databases held
more than 12 million articles. MeSH (medical subject heading) was utilised as a control
vocabulary , boolean operators And/or were used to increase or restrict the search.
The keywords used were “Patients” And “Cultural Barriers” AND “Healthcare Delivery”
including modified words such as AND, OR and NOT to ensure that the search results was
narrowed to articles that had at least one or more of the key search terms (Bettany-Saltikov,
2010).
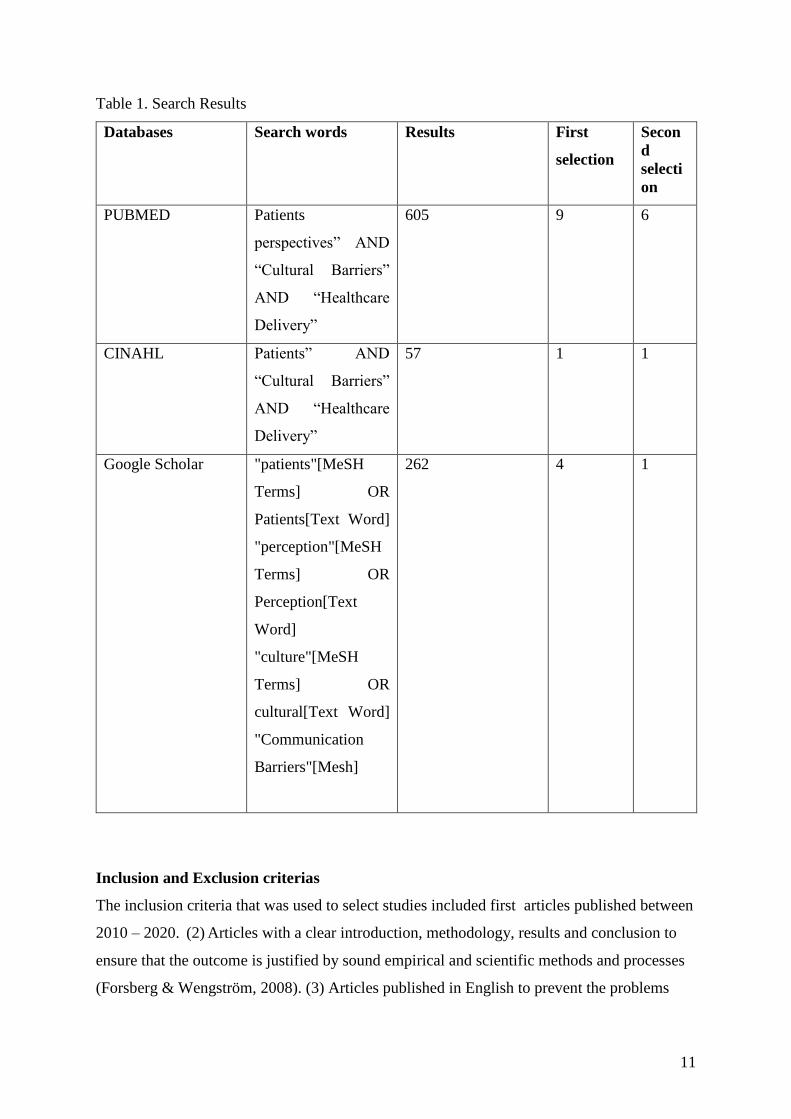
Results following our search strategy are illustrated in Table 1. Articles obtained during the
search were first selected based on the relevance of their titles and their abstracts to the thesis.
This led to a total of fourteen articles in the first selection. In the second selection process all
articles were read diligently following the inclusion and exclusion criterias leading to the final
selection of eight articles. Two articles were obtained using what Polit and Beck (2017) refer
to as the ancestral approach, where the author traced data from reference lists of already
published articles.
11
Table 1. Search Results
Databases Search words Results First
selection
Secon
d
selecti
on
PUBMED Patients
perspectives” AND
“Cultural Barriers”
AND “Healthcare
Delivery”
605 9 6
CINAHL Patients” AND
“Cultural Barriers”
AND “Healthcare
Delivery”
57 1 1
Google Scholar "patients"[MeSH
Terms] OR
Patients[Text Word]
"perception"[MeSH
Terms] OR
Perception[Text
Word]
"culture"[MeSH
Terms] OR
cultural[Text Word]
"Communication
Barriers"[Mesh]
262 4 1
Inclusion and Exclusion criterias
The inclusion criteria that was used to select studies included first articles published between
2010 – 2020. (2) Articles with a clear introduction, methodology, results and conclusion to
ensure that the outcome is justified by sound empirical and scientific methods and processes
(Forsberg & Wengström, 2008). (3) Articles published in English to prevent the problems

12
associated with language barriers and misrepresentation of facts. (4) Articles that carried one
or more of the search words to ensure that articles included were relevant to the research
topic and study (5) and only articles with abstracts were selected because it was possible to
screen or get a clear synopsis of the article and make an informed choice over whether or not
to include it. (6) All articles included in the review were based on primary research implying
the authors performed original studies. Articles included were solely qualitative studies.
Articles were excluded based on the following. Firstly all articles published before 2010,
which do not have a clear methodology and structure and published in languages other than
English with no abstract were excluded. All articles based on secondary sources were also
excluded. Articles from secondary sources are based on analysis and findings from original
and primary research such as in literature reviews (Polit and Beck, 2017).
Quality Assessment of data
When carrying out a general literature review, it is important for the researcher to do a research
critique. In other words, an appraisal of the strength and weaknesses of the peer review articles
used in the study (Polit & Beck, 2017). In order to identify areas of inadequacy and adequacy
of articles SBU´s quality assessment checklist for qualitative research studies – patients’ and
clients’ perspectives has been used (Statens Beredning for Medicinsk Utvärdering [SBU],
2016). The articles are ranked high, moderate and low quality. The assessment is made on the
basis of the ‘yes’ and ‘no’ questions on the templates. There were a total of 21 questions based
on the aim, sample selection, data collection, analysis and results. A system was created for
allocating points where each question scored one point implying there was a total of 21 points.
Articles whose ‘yes’ responses ranged between 80 – 100 percent have been ranked as high
quality; this implied they scored between 17 to 21 points. Those that fell between 60 to 79
percent scored between 13 to 16 were ranked medium quality and articles under 60 percent
were ranked as low quality implying they scored less than 13. Only articles of high qualities
have been used.
Data analysis
The use of qualitative data processing and analysis helps in understanding real life research
phenomenons such as the issue of patient’s perspectives on cultural barriers in healthcare
delivery examined in this study. The qualitative analysis helps to explore our research questions

13
on how cultural barriers affect and impact health care delivery. To analyse the literature the
author made use of what Polit and Beck (2017) referred to as a literature review matrix. The
author first began by formulating the research questions. The research questions and the
inclusion and exclusion criteria were then used as the basis for searching for data in the
electronic database. Selected articles were then read thoroughly by the author.
Articles reviewed were displayed on a table with detailed and crucial information drawn from
the inclusion and exclusion criteria in order to showcase the results and findings obtained and
the quality of the analysis (Polit & Beck, 2017). Additionally, these articles were placed in
alphabetical order based on the authors’ names. Pertinent information about the aims, objective,
methods, results were used as subjects in columns (See appendix 1).
This process was done with the aim of identifying, regularities, inconsistencies, patterns and
themes as well as possible gaps for future research. The information gathered was synthesised
and analysed. This method facilitated the work as data was arranged on a table making it easier
for the author to get a general overview rather than working with a stack of papers to redraw
information.
This process reinforces the trustworthiness of our study and highlights the robustness of the
results and conclusion about cultural barriers of healthcare delivery from the patients’
perspectives.
The figure below explains steps used in analyzing data.
Formulation of aim of the study
( Selecting articles, ,reading articles, making sense of data,
insert in literature review matrix)
Identifying Regularities, inconsistencies and
categories
Communication Discrimination
and mistrust
Socio-economic
status
Low propensity to
seek healthcare

14
Figure 2. Authors’ figure on steps in analyzing data.

15
Ethical Considerations
To avoid jeopardizing the quality of our study which is based on qualitative studies and to
ensure that our results and findings are valid and reliable, all literature review protocols listed
are followed appropriately (Polit & Beck, 2017). Articles that have an ethical clearance were
selected (Forsberg & Wengström, 2008). Search strategies have been recorded including all
relevant search words used and dates of searches. These ethical procedures are crucial in
ensuring that our methodological approach is effective and our research results and findings
are reliable and valid.
RESULTS
This study is based on ten qualitative articles from the United States of America (Cuevas,
O’Bien & Sara, 2016; Hu et al., 2013), the Netherlands (Paternotte et al., 2017), Belgium
(Peeters et al., 2015), Switzerland (Scheermesser, Bachman, Oesch & Kool, 2012), Canada
McKeary & Newbold, 2010; Singh, King-Shier & Sinclair 2020) , Norway (Straiton, Ledesma
& Donelly, 2018), Sweden (Habziabdic, Albin & Hjelm 2014) and Ghana (Sumankuuro et al.,
2019). The participants in the studies were both male and female and mostly immigrants who
were settled in another country rather than their country of origin. Participants were between
18-85 years (check appendix 1 for summary of the selected articles). The four major themes
identified from the literature review include, communication, discrimination and mistrust,
socio-economic status and low propensity to seek healthcare.
Communication
Good communication is a prerequisite to obtain fair and equal treatment for patients during
health care delivery (Cuevas et al., 2016; Habziabdic et al., 2014). The review suggested that
language barriers was one of the problems experienced by patients and was crucial in impeding
good communication between patients and health care practitioners. Patients were not
proficient in the language of their host countries and this led to misunderstanding and confusion
(Hadziabdic et al., 2014; McKeary & Newbold, 2010; Paternotte et al., 2017; Scheermesser et
al., 2012; Singh et al., 2020; Straiton et al, 2018).

16
Scheermesser et al. (2012) analysed lower back pain patients’ recovery and return to work and
found out that due to communication problems, some patients from different backgrounds
misunderstood instructions. Furthermore, language barrier was also demonstrated as a major
cultural barrier in the quality of health care delivery among refugees in Canada. Language
barriers was not only restricted during consultations, but had an impact on issues regarding
subsequent appointments, prescriptions and follow ups (McKeary & Newbold, 2010).
Habziabdic et al. (2014) cited language barriers as one of the problems experienced by patients
and indicated that patients instead shied away from hospitals or took up self -treatment.
Singh et al (2020), equally identified ethnic and language differences amongst South Asian
patients in Canada as a barrier to access quality health care. However, according to Singh et al.
(2020), these barriers could be overshadowed if the healthcare professionals provided
compassion during care.
In order to overcome this cultural barrier when patients and health practitioners do not share
the same language, many health service providers used the services of professional interpreters
(Hazbiadic et al., 2014; Paternotte et al., 2017) Even though interpreters acted as guides and
communication aids, their services were unable to completely eradicate the communication
barriers that affected the quality of healthcare delivery (Habziabdic et al., 2014; Paternotte et
al., 2017). The use of interpreters made some patients insecure and others saw it as a form of
physical handicap. Some patients even felt that using interpreters could decrease their level of
interactions with healthcare practitioners, as well as increasing the chances of them to forget
vital information (Habziabdic et al, 2014).
In the same light, Paternotte et al. (2017) identified language barrier as one of the most pressing
problems faced by patients in the current globalised environment. They highlighted the
important role of intercultural communication training in improving communication between
healthcare practitioners from different backgrounds. The study highlighted the importance of
good interpretation which meets patients’ desire, irrespective of their linguistic and cultural
background. Patients also underscored the need to promote the use of interpreters who could
interpret both literally and with the use of the appropriate medical terminology including a
professional attitude. Paternotte et al (2017) indicated that due to inadequate familiarity the
Dutch healthcare system issues of interpretation and language influenced the prevalence of
poor communication between health practitioners of Dutch origin.

17
Communication barriers was not just restricted at the level of verbal and oral interaction but
also extended to the doctor’s ability to interact with patients and making them comfortable. As
illustrated, patients preferred doctors to pay attention to them rather than engage in other
activities like working on the computer during patient-doctor interactions. According to them,
this made them feel they were not understood by the health practitioners (Paternotte et al 2017;
Scheermesser et al., 2012). Paternotte et al. (2017) stated that simple gestures like shaking
hands with the patients, asking them to take a seat facilitated the interaction between patients
and health practitioners. Paternotte et al. (2017) further indicated that patients felt it was crucial
for doctors to use simple language and avoid complicated medical jargons. Patients
underscored that it was necessary for health professionals to speak slowly and seek
confirmation from them.
In addition, Cueva et al. 2016, patients perceived that verbal domination by health professionals
during conversations rendered them less involved in decision making resulting in less
satisfaction. This was seen in a study carried out in America, were HIV positive African
Americans felt they were victims of discrimination in the health care setting as a result of poor
communication when compared to European Americans, hence affecting the manner in which
they enjoyed healthcare services. In another study carried out in Norway, patients who were
involved in decision making with regards to their health issues felt they were listened to by
their health professionals and this established grounds for good communication (Straiton et al.,
2018).
Mistrust and discrimination
Mistrust typically arose when recommendations given in the health care sector clashed with
already established belief and cultural values (Peeters et al., 2015; Sumankuuro et al., 2019).
In Belgium, Turkish immigrants who did not trust the level of expertise of health care
professionals did not take instructions seriously with regards to managing their type two
diabetes. Some of the Turkish immigrants preferred the use of herbal medicine than oral
hypoglycaemic agents prescribed to them in the hospitals. Furthermore, patients believed the
cause of their diabetes was as a result of stress in the Belgian society and as a result, most of
the participants did not adhere to their prescriptions when on holidays in their country of origin
(Peeters et al., 2015).

18
Similarly, Sumankuuro et al. (2019), also suggested that in spite of the ban placed on the usage
of traditional birth attendants during delivery, most women in the upper west region of Ghana
felt more comfortable using the services of these traditional birth agents. The negative attitude
of nurses reinforced patients' mistrust in the healthcare system in Ghana.
In terms of discrimination Cuevas et al (2016), found out that African Americans indicated that
they experienced higher levels of discriminatory practices in the healthcare system when
compared with European Americans. This study further suggests that many African American
patients, especially women believed that their health problems and symptoms were discredited
by medical practitioners.
In some instances, medical practitioners failed to treat African American patients with respect
and upon experiencing discriminatory treatment and this left many of these patients frustrated.
Patients also felt that healthcare practitioners rejected their opinions during medical and
hospital experiences and they felt these practices were discriminatory. According to most
patients, the consequences of centuries of racial injustices were still visible in the American
society and this explained why African American patients continued to experience
discrimination and mistrust in the healthcare system (Cuevas et al., 2016).
Socio-economic status
Socio-economic factors also shaped cultural barriers to healthcare. This is because people from
diverse or similar cultural backgrounds tend to experience diverse or similar socio-economic
conditions (McKeary & Newbold, 2010; Hu, Amirehsani, Wallace & Letvak, 2013). In the
United States, many Hispanic immigrants travelled into the country under similar
circumstances and typically arrived with little or no resources, spoke no English and had to
take up low-income jobs. Consequently, they had similar socio-economic status in addition to
their cultural similarity. For example, Hispanics depicted poorer self-management of type two
diabetes when compared with non-Hispanic whites (Hu et al., 2013). The purpose of Hu et al.
(2013) study explored perceived barriers to diabetic management among Hispanic immigrants
diagnosed with diabetes and their families. The major cultural barriers faced by the Hispanic
diabetes patients were mainly socio-economic as a result of lack of resources.

19
McKeary and Newbold (2010), indicate that case socio-economic barriers hinder accessibility
to competent cultural care among refugees in the Canadian society. Resettling in a new country
in most cases resulted in a loss of both economic and social status. This implied living under
the poverty line and threshold. McKeary and Newbold, (2010), noted that paying for
transportation fare to the hospital was a major challenge that restricted refugees from having
access to proper health care services. In addition, most refugees who arrived in an already
established society which felt insecure and uncomfortable since they lacked the information,
knowledge and resources needed to get quality health care
In a similar study conducted in Ghana although most maternal healthcare policy programmes
such as Antenatal care (ANC) were fee-exempted under the National Health Insurance Scheme,
there was low skilled care utilisation during pregnancy and delivery (Sumankuuro et al., 2019).
Many women did not sign up for ANC because of their low socio-economic status within their
households. This was because the decision-making power at the household level is left to the
men especially in the rural communities and many of them still believed in the traditional
maternal care customs and practices. According to Sumankuroo et al 2019, this lack of
autonomy made it difficult for many women to shift from traditional birth attendants to
attending modern maternal services.
Straiton et al (2018) noted that immigrant women experienced less access to health care in
general and mental services in particular than non-immigrant women. Immigrants were highly
diversified and came from a range of different cultural, personal, social and economic settings
which impacted their propensity to seek healthcare. Straiton et al. (2018), further examined
factors that influenced Filipina immigrants’ perceptions about seeking medical help from
general practitioners in Norway. The study found out that factors such as educational
background, socioeconomic status, and familiarity with health care services as well as
experience of mental health affected immigrant women’s impressions about seeking mental
health. Mental health disorders are highly stereotyped and stigmatised within the society hence
was a major cultural barrier that deterred Filipina women from seeking mental health support.
The case was even more severe among Filipina women who had low levels of education and
income. Overcoming this challenge was a complex task because these stereotypes had been
developed before most of these women migrated to Norway. After settling in Norway, it was
difficult for them to change their initial perceptions about mental health and wellness.

20
Low propensity to seek health services
Another major barrier to cultural competent healthcare delivery was the prevalence of low
propensity to seek healthcare in some cultures (Sumankuroo et al., 2019). In addition to western
medicine, there are alternative medicines and not all immigrants believed western medicine
was the best. Consequently, many immigrants stuck to their medical belief propagated by their
cultures even after migrating to western countries. When many of them fell ill, they stayed
home and treated themselves with their traditional medication. For many of them, the hospital
was a last resort and unless they were seriously sick, they did not go to the hospital. This was
a major cultural barrier to accessing quality healthcare services (Paternotte et al 2017; Straiton
et al 2018). For example some Chinese immigrants who were unfamiliar with the Dutch
healthcare system used alternative medicine. This constituted a barrier among immigrants from
China who had been used to an alternative form of medicine in treating certain ailment (Straiton
et al, 2018).
Straiton et al. (2018) supported this view and noted that immigrant women experienced greater
barriers to quality health care in general and mental services in particular than non-immigrant
women. Based on their study, some Filipino women did not consider mental health was an issue
that could be addressed by health professionals. Another similar situation could be seen in
Ghana where women in labour due tend not to disclose early that they were in labour because
they feared that revealing it, could lead to prolong labour. As a result, most of the women ended
up giving birth on their way to the hospital exposing them to more danger and reducing their
ability to receive proper care (Sumankuroo et al., 2019).
DISCUSSION
The findings of the results of the literature show that four types of cultural barriers from the
patient’s perspective shape delivery of culturally competent healthcare. These include
communication problems arising during verbal and nonverbal interactions, mistrust and
discrimination arising as a result of previous contact with the health care system, socio-
economic status and finally low propensity to seek healthcare which are common with people
of same cultural background. These cultural barriers have shaped the delivery of a cultural
competent healthcare system, hence crucial for many healthcare stakeholders. The discussions
below is categorized into these four cultural perspectives (communication, mistrust and
discrimination, socio-economic status, low propensity to seek healthcare) and highlight issues

21
relating to the aim of the study, theoretical framework, previous research and clinical and
ethical relevance of the results and findings.
Discussion of results
Communication
In the results communication challenges were seen as a major cultural barrier in the delivery
of health care services. Communication difficulties emerged as a result of language barriers
when patients were not proficient in the language used at the hospital setting (Habziabdic et al.
2014). Communication difficulties were also non-verbal (Paternotte et al., 2017). This reflects
the claims of authors such as Roter, Frankel, Hall and Sluyter (2006) who indicate that facial
expressions such as smiling, eye contact can help build a relationship between patients and
health practitioners of different cultural backgrounds.
It is important to note that non-verbal communication styles vary from one culture to another.
For instance, addressing an elderly person by name and looking into the person’s eyes in certain
cultures can be considered as disrespectful. This means that health practitioners should be able
to understand the implications of diverse cultural non-verbal communicative values, attitudes
and behaviours. Implying they should be able to provide what Betancourt et al. (2005) refer to
as cultural competent care. This does not insinuate that healthcare professionals have to have a
mastery of all cultures. Rather they should acknowledge the fact that different cultures exist,
in order to enhance the process of bridging cultural barriers. This is congruent with the tenets
of the cultural care theory which calls for health practitioners to increasingly acknowledge the
existence of diverse cultural values such as language during care delivery. Acknowledging and
respecting the existence of different cultural values will foster the process of meeting up with
the needs of patients (Leininger, 1991; Leininger, 1994).
One of the ways following the literature review through which these communication challenges
and differences are currently being resolved is by using interpreters to help patients from
different backgrounds (such as immigrants) communicate effectively with healthcare
practitioners (Habziabdic et al.,2014; Hultjö et al.,2019). Leininger's theory strongly
recommends that nurses should be culturally competent (Leininger, 1991; Leininger, 1994).
This means they should be able to identify the linguistic needs of a patient and provide the

22
required resources that will help eradicate communication barriers. However, this theory does
not take into consideration the fact that the presence of an interpreter implies extra costs which
in some cases the health practitioner might not have control over, but rather policy makers. In
addition, the presence of an interpreter might also be time consuming, making it practically
impossible given that health practitioners work on an already very tight schedule.
As expected from the study the presence of interpreters in most cases did not guarantee a bridge
in the communication barrier (Hadziabdic, 2014). This is congruent with the assertion of some
authors who acknowledge that the use of interpreters cannot be considered as a guarantee to
effective communication because not all interpretations can be trusted (Robb & Greenhalgh,
2006). Communication barriers can have an adverse effect on the patient's ability to receive
proper health care treatment. According to The Swedish Association of Nursing (2017b) it is
mandatory that the patient or relatives should be able to comprehend all given instructions so
that they might be able to contribute and participate in their wellbeing.
Mistrust and discrimination
From the review mistrust and discrimination are major cultural barriers to competent cultural
healthcare provision. Mistrust arouses when the patients have an already established belief
system (worldview) that clashes with established health care recommendations and procedures
(Peeters et al, 2013). This falls in line with Leininger’s cultural care theory where an
individual's cultural value and religious background influences their behavior in a different
environmental context. This implies patients typically respond to the services provided to them
based on their cultural values (Leininger, 1991; Leininger, 1994). Mistrust shapes people’s
attitude and perception towards the provision of health services and also leads to dissatisfaction
(Alpers, 2018). According to Ngo-Metger et al (2006), mistrust and discrimination is a cultural
barrier that might impede access to quality health care.
In addition, historical factors and existing social prejudice and injustices have created rifts in
the society at large. It is important to acknowledge that the healthcare system operates within
a wider society which has issues of social injustice and inequality (Cuevas et al 2016; Griffith,
Bergner, Fair, & Wilkins, 2020). These discriminatory experiences have unfortunately shaped
negative perceptions embedded within patients from these backgrounds about their health
encounters. This is consistent with the emic experiences as highlighted in Leininger's theory,
whereby the direct and indirect experiences of groups can be transmitted intergenerationally,

23
hence shaping the way they perceive the health care system. Patients who perceive
discrimination based on past experiences are less likely to be interactive and not participate
verbally during health encounters and consultations. This can make it difficult to obtain the
required information needed to help patients hence might lead to inequality in the production
of health care services (Cuevas et al, 2016; Hausmann et al, 2012). These inequalities create
ethical dilemmas which are not in conformity with the international nursing code where care
should be given equally to all those in need (International Council of Nurses, 2013).
For example, in the USA, African Americans and Latinos have a long history of receiving
inferior care in comparison to some privileged groups. Periods of unethical medical experience
on African Americans have been well documented; hence it is only logical and rational for
African Americans to be doubtful towards the health care system (Griffith et al, 2020). In some
instances, due to mistrust when healthcare practitioners make genuine mistakes it is interpreted
as discrimination. To mitigate the challenges presented by issues of mistrust and discrimination
it is crucial that the care delivery process incorporates tenets of the Leininger’s theory which
advocates for the need to maintain, negotiate and reshape the cultural values and worldviews
of patients from minority groups into the health care delivery process (Leininger, 1991;
Leininger, 1994). However, the incorporation of these cultural values and belief into the health
care delivery process poses both technical and structural difficulties as it requires resources,
time and can be costly.
Socio-economic status
Findings and results from the literature review indicated that cultural barriers emanated from
people with low socio-economic status and background (Hu, Amirehsani, Wallace & Letvak,
2013; McKeary & Newbold, 2010). This was in conformity with the socio-economic
components in Leininger’s cultural care theory which mentioned that education and an
individual's social and economic status shaped people’s attitude and behavior within a given
environment. However, no clear explanation is given to show how socio-economic factors can
be attributed as a cultural barrier that impedes access to proper care. Whilst there is little
evidence to show linkages between socio-economic status and culture, the findings from the
literature review highlight that people from certain cultural backgrounds tend to be more likely
to have different levels of socio-economic status (Hu et al, 2013; ;McKeary & Newbold, 2010).

24
In addition, socio-economic status encompasses access to material capital, human capital and
social capital, which can be defined as knowledge (education), wealth and occupation. People
with high educational levels are generally more knowledgeable about health issues and tend to
face fewer barriers to healthcare services. This is the case in countries such as the USA where
Black Americans and Latinos with low socio-economic status typically have worst health
outcomes in comparison with European American (Crimmins, Hayward, & Seeman, 2004).
Equally, in Norway for example about 71 % of Somali women refugees lacked the knowledge
on how to utilize information obtained from the hospital to improve on their health situation
(Gele, Pettersen, Torheim & Kumar, 2016). Immigrants from low-income countries tend to be
more likely to live in deprived communities and do menial jobs with low pay and are more
stressed up with integration issues into the labor market and do not prioritize health (Ahmed et
al, 2016).
From the above these imply a segment of the society will receive limited or no care because of
their socio-economic status. Accessibility to proper healthcare is a basic human right and it's
mandatory for health professionals to see that all patients regardless of their background have
accessibility to proper care (International council of nurses, 2013; The Swedish Association of
Nursing 2017a).
Low propensity to seek health Care.
Results and findings from the literature review also suggest that people of a particular
background have a low propensity to seek for health care services as a result of patients having
a strong affinity in using alternative medicines that they feel provide equal or better services
than modern hospitals (Sumankuroo et al., 2019; Paternotte et al; Straiton et al 2018). These
attitudes and behaviour are typically shaped by customary and religious beliefs. This aspect is
reflected in Leininger's theory, where she illustrates in her sunrise model how ‘cultural beliefs
and way of life’ influences an individual’s patterns or perception of the health care system. For
example, there is a general consensus that patients from the Arab cultures and traditions have
the tendency to avoid modern hospital services and resources because there is a strong belief
about the powers of their religious deity as a solution to their health issues. More specifically,
Muslim women avoid medical procedures such as breastcancer screening because the screening

25
procedures are not a priority and more often clash with their cultural and religious practices
and belief system (Salman, 2012).
Contrary to the findings from the study suggesting that migrants display low propensity to seek
health mainly because of customary and religious beliefs, it has also been noted that migrants
are not familiar with modern healthcare facilities and procedures. They typically rely on self-
medication, home remedies and view modern health facilities and procedures as stressful and
daunting, too bureaucratic and often feel their illness will be exacerbated (Kimbrough, 2007).
However, low propensity of seeking health care is also shaped by individual and household
choices about how issues of healthcare and illnesses are prioritized and not necessarily by
customary or societal beliefs. For example, people who prioritize preventive measures rather
than curable measures when faced with illnesses, have different levels of healthcare seeking
attitudes and behavior. Low propensity to seek health care will therefore lead to a rise in more
complicated medical procedures which may be more costly for both individuals and the society.
Clinical relevance and basis for further research.
This thesis highlights the cultural difficulties faced during patient and health worker
interactions during the provision of healthcare services. It can be used to alleviate cultural
barriers that are encountered and evident between health practitioners and patients. This study
highlights how cultural barriers can be mitigated and managed by identifying specific
circumstances and conditions that subject patients to cultural barriers.
The thesis can also be used as a basis for further research For example, issues of cultural
barriers from the patient's perspective in relation to nurse patient interaction is pivotal in the
health care set up and their role can never be undermined given that they provide direct care to
the patient. It is therefore crucial that more research should be done
within this area.
Discussion of method
This study was a general literature review where qualitative studies were examined with the
main purpose of identifying all relevant information that exists based on the research questions
(Polit & Beck, 2017). One of the strengths of this type of study is that it is free from bias given

26
that the analysis of the results was based on findings from the ten selected articles (Polit &
Beck, 2017). In addition, this design provides a comprehensive, thorough and up-to-date
literature that exist within the selected field given that articles selected were between 2010-
2020. More so results obtained are reproducible, as the process used to carry out the research
has been clearly defined. However, one of the weaknesses of this study was that the results
were interpreted based on the authors understanding of the articles. This in some cases can give
room to misinterpretation of data (Graneheim & Lundman, 2004).
Three main databases were used to collect relevant materials. These databases were selected
based on their reputability in having a variety of journals and articles. The three main databases
used were CINAHL, PUBMED and Google scholar (Polit & Beck, 2017). The author made
use of selected keywords to find relevant articles. Most articles found were based on the
perspectives of the health practitioners and nurses, very few articles were found based on the
perspectives of the patients. The author made use of what Polit and Beck (2017) refer to as the
ancestral approach where the author tracked down data from the reference lists of already
published articles or reports.
One of the major strengths of this work is that all articles used were graded high quality
following the SBU´s quality assessment checklist for qualitative research studies – patients’
and clients’ perspectives (Statens Beredning for Medicinsk Utvärdering [SBU], 2016). As a
result, all articles selected had a clear methodology with reliable results making the study robust
and credible. In addition, the SBU quality assessment was perfect for our research area as it
dealt with the patient´s perspectives as well.
The inclusion and exclusion criteria used helped to select the most relevant and recent articles
for this study. The ten articles selected were case studies from the United States of America
(Cuevas., et al., 2016; Hu et al., 2013), the Netherlands (Paternotte et al., 2017), Belgium
(Peeters et al., 2015), Switzerland (Scheermesser et al., 2012), Canada (McKeary & Newbold,
2010; Singhet al., 2020), Norway (Straiton et al., 2018) , Sweden (Habziabdic et al., 2014) and
Ghana (Sumankuuro et al., 2019).This reflects the fact that cultural barrier within the care
section is an international problem and challenge. It also implies the results can be applicable
in countries with different backgrounds and settings, making the work trustworthy. The results
are also applicable to today’s nursing practice, because these barriers are visible during patient-

27
nurse day to day interactions. However, it is important to recognize that each individual is
unique and has subjective experiences (Leininger, 1991,1994).
To analyse the result a literature review matrix in accordance with the description of Polit and
Beck (2017) was used. This method was suitable because it enabled the author to make use of
the large textual data and identify categories that were informed from the research question of
the study. The author thus read every article diligently with the aim of bringing out information
that was relevant to various categories. This process was time consuming given that the author
had to read several times through the ten articles in order to identify categories. In doing so the
author was able to identify patterns and regularities as well as gaps within this area of study.
In addition, when categorizing there is always the risk that the author might not be objective
but rather subjective because the researcher's personal experience has the potential of
influencing his or her interpretation. To minimise the risk of subjectivity the author had to read
the articles thoroughly. Articles used were those with an ethical clearance (Forsberg &
Wengström, 2008). These ethical procedures are very important in ensuring that our findings
are reliable and valid. More so, ethical considerations in alliance to what Polit and Beck (2016)
refer to as research misconduct was taken into consideration, including avoiding plagiarism
and accrediting all information and sources that was not from the author.
Conclusion
To conclude it is evident that patients face a plethora of cultural barriers during their
interactions with health care services and their experiences can be shaped by a number of
variables and factors. These cultural challenges might hinder accessibility to proper health care
services thus leading to inequality in the provision of health care services.

28
REFERENCES
All articles with the asterisk * sign were used for the literature review.
Ahmed, S., Shommu, N. S., Rumana, N., Barron, G. R. S., Wicklum, S. & Turin, T. C. (2016).
Barriers to access of primary healthcare by immigrant populations in Canada: A literature
review.Journal of Immigrant and Minority Health, 18(6), 1522
1540. https://doi.org/10.1007/s10903-015-0276-z
Almutairi, A. F., Gardner, G. & McCarthy, A. (2013). Perceptions of clinical safety climate of
the multicultural nursing workforce in Saudi Arabia: A cross-sectional survey. Collegian
(Royal College of Nursing, Australia), 20(3), 187-194. doi:10.1016/j.colegn.2012.08.002
Alpers, L. (2018). Distrust and patients in intercultural healthcare: A qualitative interview
study. Nursing Ethics, 25(3), 313-323. doi:10.1177/0969733016652449
Betancourt, J. R., Green, A. R., Carrillo, J. E. & Park, E.R. (2005). Cultural competence and
health care disparities: Key perspectives and trends. Health Affairs, 24(2), 499-505.
doi:10.1377/hlthaff.24.2.490
Bettany-Satikov, J. (2010). Learning how to undertake a systematic literature review: Part2.
Nursing Standard. 24(51), 47-55. doi: 10.7748/ns2010.08.24.50.47.c7939.
Cornelison, A.H. (2001). Cultural barriers to compassionate care-patients' and health
professionals' perspectives. Bioethics Forum, 17(1), 7-14.
Crimmins, E. M., Hayward, M. D. & Seeman, T. E. (2004). Race/Ethnicity, Socioeconomic
Status, and Health. N B. Anderson., R A. Bulato & B. Cohen (Eds). Critical Perspectives on
Racial and Ethnic Differences in Health in Late Life (9). Washington D C. available from
https://www.ncbi.nlm.nih.gov/books/NBK25526/
Cross, T., Bazron, B.J., Dennis, K.W. & Isaacs, M.R. (1989). Towards a cultural system of
care , A Monograph on effective services for minority children who are severely emotionally

29
disturbed. Washington, DC: Georgetown University Child Development Center, CASSP
Technical Assistance Center, 1, 1-99.
*Cuevas, A. G., O'Brien, K. & Saha, S. (2016). African american experiences in healthcare: "I
always feel like I'm getting skipped over". Health Psychology,35(9), 987-995.
doi:10.1037/hea0000368
Ellins, J. & Glasby, J. (2016) “You don't know what you are saying ‘Yes’ and what you are
saying ‘No’ to”: hospital experiences of older people from minority ethnic communities.
Ageing and Society, 36(1), 42-63. doi:10.1017/S0144686X14000919
Ergin, E. & Akin, B. (2017). Globalization and its Reflections for Health and Nursing.
International Journal of Caring Science, 10(1),607-613.
Forsberg, C. & Wengström, Y. (2008). Att göra systematiska litteraturstudier: Värdering,
analys och presentation av omvårdnadsforskning (2., [uppdaterade] utg. ed.). Stockholm:
Natur & Kultur.
Gele, A. A., Pettersen, K. S., Torheim, L. E. & Kumar, B. (2016). Health literacy: The missing
link in improving the health of somali immigrant women in Oslo. BMC Public Health, 16(1),
1134-1134. doi:10.1186/s12889-016-3790-6
Graneheim, U. H. & Lundman, B. (2004). Qualitative content analysis in nursing research:
Concepts, procedures and measures to achieve trustworthiness. Nurse Education Today, 24(2),
105-112. doi:10.1016/j.nedt.2003.10.001
Grifith, D, M., Bergner, E, M. & Fair, A, S. (2020). Using mistrust, distrust, and low trust
precisely in medical care and medical research advances health equity. American Journal of
Preventive Medicine, 60(3), 442-445 . doi:10.1016/j.amepre.2020.08.019
Hausmann, L. R. M., Hannon, M. J., Kresevic, D. M., Hanusa, B. H., Kwoh, C.K. & Ibrahim,
S. A. (2011). Impact of perceived discrimination in healthcare on patient-provider
communication. Medical Care, 49(7), 626-633. doi:10.1097/MLR.0b013e318215d93c

30
*Hadziabdic, E., Albin, B. & Hjelm, K. (2014). Arabic-speaking migrants' attitudes, opinions,
preferences and past experiences concerning the use of interpreters in healthcare: A postal
cross-sectional survey. BMC Research Notes. 7(1), 71-71. doi:10.1186/1756-0500-7-71
Handtke, O., Schilgen, B. & Mösko, M. (2019). Culturally competent healthcare–A scoping
review of strategies implemented in healthcare organizations and a model of culturally
competent healthcare provision. PloS one, 14(7). doi: 10.1371/journal.pone.0219971
Hausmann, L. R. M., Hannon, M. J., Kresevic, D. M., Hanusa, B. H., Kwoh, C.K. & Ibrahim,
S. A. (2011). Impact of perceived discrimination in healthcare on patient-provider
communication. Medical Care, 49 (7), 626-633. doi:10.1097/MLR.0b013e318215d93c.
Hjelm, K., Bard, K., Nyberg, P., & Apelqvist, J. (2003). Religious and cultural distance in
beliefs about health and illness in women with diabetes mellitus of different origin living in
sweden. International Journal of Nursing Studies, 40(6), 627-
643. https://doi.org/10.1016/S0020-7489(03)00020-8
Hjelm, K., & Nambozi, G. (2008). Beliefs about health and illness-a comparison of men and
women with diabetes mellitus living in Uganda. International Nursing Review, 55(4), 434-441.
https://doi-org.ezproxy.its.uu.se/10.1111/j.1466-7657.2008.00665.x
*Hu, J., Amirehsani, K., Wallace, D. C. & Letvak, S. (2013). Perceptions of barriers in
managing diabetes: Perspectives of hispanic immigrant patients and family members. The
Diabetes Educator, 39(4), 494-503. doi:10.1177/0145721713486200
Hull, M. (2016). Medical language proficiency: A discussion of interprofessional language
competencies and potential for patient risk. International Journal of Nursing Studies, 54, 158-
172. doi:10.1016/j.ijnurstu.2015.02.015
Hultsjö, S., Bachrach-Lindström, M., Safipour, J. & Hadziabdic, E. (2019). “Cultural
awareness requires more than theoretical education”-Nursing students’ experiences. Nurse
education in practice, 39, 73-79.https://doi.org/10.1016/j.nepr.2019.07.009

31
Hultsjo, S. & Hjelm, K. (2005). Immigrants in emergency care: Swedish health care staff ’s
experiences. International Nursing Review 52(4), 276–285. https://doi.org/10.1111/j.1466-
7657.2005.00418.x
International Council of Nurses.(2013). Cultural and Linguistic Competence.Geneva:
International Council of Nurses. Accessed the 15/02/2021 from
https://www.icn.ch/sites/default/files/inline-files/B03_Cultural_Linguistic_Competence.pdf
Kimbrough Bennet Jennifer (2007) Health Literacy as a Contributor to Immigrant Health
Disparities. Journal of Health Disparities Research and Practice 1(2). Accessed: 15 february
2021. From
http://digitalscholarship.unlv.edu/cgi/viewcontent.cgi?article=1114&context=jhdrp
Leininger, M. (1991). Culture care and diversity: A theory of nursing. New York: National
League for Nursing Press.
Leininger, M. (1994). Transcultural nursing education: A worldwide imperative. Nursing and
Healthcare, 15(5), 254-257.
McFarland, M. & Wehbe, H. (2015). Leininger’s Culture Care Diversity and Universality: A
Worldwide Nursing (3rd ed). Jones y Bartlett Pub (Ma), editor. Burlington.
McFarland, M. R., & Wehbe-Alamah, H. B. (2019). Leininger’s theory of culture care
diversity and universality: An overview with a historical retrospective and a view toward the
future. Journal of Transcultural Nursing, 30(6), 540-557.
https://doi.org/10.1177/1043659619867134

32
*McKeary, M. & Newbold, B. (2010). Barriers to care: The challenges for canadian refugees
and their health care providers. Journal of Refugee Studies, 23(4), 523-545.
doi:10.1093/jrs/feq038
Ngo-Metzger, Q., Telfair, J., Sorkin, D. H., Weidmer, B., Weech-Maldonado, R., Hurtado, M.
& Hays, R. D. (2006). Cultural Competency and Quality of Care: Obtaining the Patient’s
Perspective. New York: The Commonwealth Fund.
*Paternotte, E., Dulmen, S. v., Bank, L., Seeleman, C., Scherpbier, A. & Scheele, F. (2017).
Intercultural communication through the eyes of patients: Experiences and
preferences. International Journal of Medical Education, 8, 170-175.
doi:10.5116/ijme.591b.19f9
*Peeters, B., Van Tongelen, I., Duran, Z., Yüksel, G., Mehuys, E., Willems, S., . . . Boussery,
K. (2015). Understanding medication adherence among patients of turkish descent with type
2 diabetes: A qualitative study. Ethnicity & Health, 20(1), 87-105.
doi:10.1080/13557858.2014.890174
Polit, D. F. & Beck, C. T. (2017). Nursing research: Generating and assessing evidence for
nursing practice. (10th ed). Lippincott Williams & Wilkins.
Raja, S., Hasnain, M., Vadakumchery, T., Hamad, J., Shah, R. & Hoersch, M. (2015)
Identifying Elements of Patient-Centered Care in Underserved Populations: A Qualitative
Study of Patient Perspectives. PLoS One, 10(5). doi:10.1371/journal.pone.0126708
Robb, N. & Greenhalgh, T. (2006). "You have to cover up the words of the doctor":the
mediation of trust in interpreted consultations in primary care. Journal of Health Organisation
Management, 20(5), 434–455.https://doi.org/10.1108/14777260610701803
Roter, D. L., Frankel, R. M., Hall, J. A., & Sluyter, D. (2006). The expression of emotion
through nonverbal behavior in medical visits: Mechanisms and outcomes. Journal of General
Internal Medicine, 21(1), 28-34. doi:10.1111/j.1525-1497.2006.00306.x

33
Saha, S., Beach, M. C., Cooper, L. A. (2008) Patient Centeredness, Cultural Competence and
Healthcare Quality. Journal of the National Medical Association, 100(11), 1275-1285.
doi:10.1016/S0027-9684(15)31505-4
Salman, K. F. (2012). Health beliefs and practices related to cancer screening among arab
muslim women in an urban community. Health Care for Women International, 33(1), 45-
74. doi.org/10.1080/07399332.2011.610536
*Scheermesser, M., Bachmann, S., Schämann, A., Oesch, P. & Kool, J. (2012). A qualitative
study on the role of cultural background in patients' perspectives on rehabilitation. BMC
Musculoskeletal Disorders, 13(1). doi:10.1186/1471-2474-13-5
*Singh, P., King-Shier, K. & Sinclair, S. (2020). South Asian patients' perceptions and
experiences of compassion in healthcare. Ethnicity & Health, 25(4), 606-624.
doi:10.1080/13557858.2020.1722068
Statens beredning för medicinsk och social utvärdering (SBU). (2016). Evaluation and
synthesis of studies using qualitative methods of analysis. Stockholm. Obtained 15 december
2020, from
https://www.sbu.se/globalassets/ebm/metodbok/sbuhandbook_qualitativemethodsofanalysis.p
df.
*Straiton, M. L., Ledesma, H. M. L. & Donnelly, T. T. (2018). "it has not occurred to me to
see a doctor for that kind of feeling": A qualitative study of Filipina imigrants perceptions of
help seeking for mental health problems. BMC Women's Health, 18(1), 73-73.
doi:10.1186/s12905-018-0561-9
*Sumankuuro, J., Mahama, M. Y., Crockett, J., Wang, S. & Young, J. (2019). Narratives on
why pregnant women delay seeking maternal health care during delivery and obstetric
complications in rural ghana. BMC Pregnancy and Childbirth, 19(1), 260-260.
doi:10.1186/s12884-019-2414-4
Svensk sjuksköterskeförening (The Swedish Association of Nursing). (2017a). ICN:s etiska
kod for sjukskoterskor. Stockholm: Svensk sjuksköterskeförening. Accessed: the 15 /02/2021
from
34
https://www.swenurse.se/download/18.9f73344170c0030623146a/1584003553081/icns%20e
tiska%20kod%20f%C3%B6r%20sjuksk%C3%B6terskor%202017.pdf.
Svensk sjuksköterskeförening (The Swedish Association of Nursing). (2017b).
Kompetensbeskrivning for legitimerad sjukskoterska. Stockholm: Svensk
sjuksköterskeförening. Accessed the 15/02/2021 from
https://www.swenurse.se/download/18.9f73344170c003062317be/1584025404390/kompeten
sbeskrivning%20legitimerad%20sjuksk%C3%B6terska%202017.pdf.
Wasserman, M., Renfrew, M. R., Green, A. R., Lopez, L., Tan‐McGrory, A., Brach, C. &
Betancourt, J. R. (2014). Identifying and preventing medical errors in patients with limited
english proficiency: Key findings and tools for the field. Journal for Healthcare
Quality, 36(3), 5-16. doi:10.1111/jhq.12065

35
APPENDIX 1
TABLE PRESENTED OF THE QUALITY REVIEWED ARTICLES.
Author, year,
country
Titel Aim Method Participants Results Quality
Articles1
Cuevas, A. G., O'Brien, K. &
Saha, S., 2016
United States
of America
African American
experiences in
healthcare: "I always feel like
I'm getting
skipped over"
The aim of the study is to
examine
Africans Americans
experience and
the barriers they face in
health during
health encounters.
The article also
examines their perception
when it come
to race in the patient
provider
relationship.
Qualitative method Focus groups
69 african Americans
Ranging from
the ages of 24
to 89
Patients, especially women, felt they
were being
discriminated upon if their symptoms
were not taken into
consideration. Poor communication,
disrespect affected
patients' perspectives of the
care section.
High 18 points
Hadziabdic, E.,
Albin, B. &
Hjelm, K., 2014
Sweden
Arabic-speaking
migrants'
attitudes, opinions,
preferences and
past experiences concerning the
use of
interpreters in healthcare:
The aim of the
study is to
study Arabic speaking
individual
attitudes, expectations
and preferences
when it comes to using
interpreters
within the health care
sector in
Sweden.
Qualitative
Method. A post
cross-sectional survey using
structured self-
administered questionnaires.
53 Arab
speaking
immigrants
Ranging from
the ages of 18-59 years
Most participants
perceived
interpreters as a communicator aid.
They also felt it was
of importance to be able to trust your
interpreters. Trust
was also solidified based on the quality
of the interpreter. A
good interpreter should have a good
mastery of the
language, the medical
terminologies, have
the same background and
sex.
High
17 points
Hu, J.,
Amirehsani, K., Wallace, D, C.
& Letvak, S., 2013
United States of America
Perceptions of
barriers in managing
diabetes: Perspectives of
Hispanic
immigrant patients and
family
members.
To examine the
barriers faced by Hispanic
immigrants in managing their
diabetes.
Qualitative
Method. Focus groups
73 Hispanic
immigrants with 37 family
members. Participants
where from 18
years
Language barrier
was a major problem. Socio
economic problems and little
understanding as to
how the health care system function was
another factor.
High
19 points
McKeary, M. & Newbold, B.,
2010
Canada
Barriers to care: The challenges
for canadian
refugees and their health care
providers.
To examine the barriers faced
by hispanic
immigrants in managing their
diabetes.
Qualitative Methods. Semi
structured in depth
interviews
14 health professionals
Language barrier was a major
problem. Socio
economic problems and little
understanding as to
High 18 points
1 SBU´s quality assessment checklist for qualitative research studies – patients’ and clients’ perspectives (Statens
Beredning för Medicinsk Utvärdering [SBU], 2016) was used in grading articles quality. This manual had a total
of 21 questions and one point was allocated per question. Grades were awarded on the basis of Yes or No, that is
to say a point was allocated to every yes and zero to every NO. An article could be awarded a maximum of 21
points. Articles were then ranked based on high, medium and low scores and quality. Articles which scored
between 17-21 points were considered as having high quality. Articles that scored between 12-16 were seen as
medium and those that scored less than 12 were considered having low quality. All selected articles scored high.

36
how the health care
system function was
another factor.
Paternotte, E.,
Dulmen, S. v., Bank, L.,
Seeleman, C.,
Scherpbier, A. & Scheele, F.,
2017.
Netherlands
Intercultural
communication through the eyes
of patients:
Experiences and preferences.
To observe
how patients with non dutch
background
perceived intercultural
communication
between themselves and
their doctors
Qualitative
Methods. Semi-structured
interviews.
30 patients
were interviewed.
Language barrier
was a major problem but it was
much better when
the health giver was professional. The
doctor's attitude
also helped est2ablish the
patient's
relationship.
High
17 points
Peeters, B.,
Van Tongelen,
I., Duran, Z., Yüksel, G.,
Mehuys, E.,
Willems, S., Pemon Jean
Paul., &
Boussery, K., 2015.
Belgium
Understanding
medication
adherence among patients
of turkish
descent with type 2 diabetes:
A qualitative
study.
To have an
understanding
of factors that determine
adherence to
medications to patients of
turkish origins
in Belgium
Qualitative
Methods
In Depth interviews
21 patients
were
interviewed. Ages 30-69
Religious and
cultural beliefs help
in determining how patients will adhere
to their medications.
The lack of social support, the doctors
medical expertise
and depression were other
determinants.
High
18 points
Scheermesser,
M., Bachmann,
S., Schämann, A., Oesch, P. &
Kool, J., 2012.
Switzerland
A qualitative
study on the role
of cultural background in
patients'
perspectives on rehabilitation
To explore
possible
barriers that hinder patients
with
southeastern backgrounds t
o attain a
successful
rehabilitation.
Qualitative
Methods. Semi
structured in depth interviews
13 patients
were
interviewed ages
38-60 years
Patients prefer
passive rather than
active strategies recommended by
doctors in dealing
with health issues. Communication
problems between
the patients and the
doctors can be seen
to be a major
barrier.
High
17 points
Singh, P., King-Shier, K.
& Sinclair, S.,
2020
Canada
South asian patients'
perceptions and
experiences of compassion in
healthcare.
Aim at identifying
south Asians
patients' views on the use of
compassion in
the delivery of health care
studies.
Qualitative Methods
Semi structured
interviews
19 patients were
interviewed.
Participants believed
compassion had a
great role in bridging cultural,
ethnic differences
between healthcare professionals
High 18 points
Straiton, M. L., Ledesma, H.
M. L. &
Donnelly, T. T., 2018
Norway
It has not occurred to me
to see a doctor
for that kind of feeling": A
qualitative study
of Filipina immigrants'
perceptions of
help seeking for mental health
problems.
To explore the perceptions of
Filipina women
in accessing healthcare in
Norway.
Qualitative Method. Semi-
structured
interviews
14 women were interviewed
Ages 34-49 years.
The women's values, experience
and stigma
influenced their perception of
seeking health care.
Structural barriers also impede their
access to the health
care systems.
High 18 points
Sumankuuro,
J., Mahama, M.
Y., Crockett, J., Wang, S., &
Young, J., 2019
Ghana
Narratives on why pregnant
women delay
seeking maternal health
care during
delivery and obstetric
complications in
rural Ghana
Aim at identifying
south asians
patients views on the use of
compassion in
the delivery of health care
studies.
Qualitative Method. Individual
depth interviews
and focus group
discussions.
16 health professionals,
three traditional
birth attendants and 240
community
members Range from the
ages of 20-69
Participants believe compassion had a
great role in
bridging cultural, ethnic differences
between healthcare
professionals and patients.
High 18 points


















