CT imaging of acute E. Coli -related colitis
3
CASE REPORT CT imaging of acute E. Coli-related colitis John Morgan & Megan Bell & Michael A. Sadler Received: 5 December 2006 / Accepted: 31 January 2007 / Published online: 28 February 2007 # Am Soc Emergency Radiol 2007 Abstract Patients with abdominal pain and bloody diarrhea often present in the acute setting to the emergency department for evaluation. After the appropri- ate clinical assessment, cross-sectional imaging is often utilized to evaluate for the severity of the disease. Although a wide spectrum of findings may be seen, diffuse colonic mural thickening, consistent with panco- litis, is most common. We report an Escherichia coli 0157:H7-related pancolitis in a patient with spinach intake linked to the recent outbreak. Keywords Pancolitis . Colon . Infection . CT . Diarrhea . E. Coli 0157:H7 A 22-year-old man with no significant past medical history was admitted to the emergency department after complain- ing of abdominal pain and bloody diarrhea for 2 days. The patient reported approximately 20 loose, bloody bowel movements on the day before admission. He described the abdominal pain as constant and diffuse but most severe in the right lower quadrant. He reported nausea but no vomiting, chills, and fever and reported no recent travel history. His history was only remarkable for eating salads frequently over the past few weeks, most of which contained spinach. Physical exam was remarkable for moderate general discomfort and a nondistended abdomen with tenderness to palpation in the bilateral lower quad- rants. No rebound or guarding was noted. His exam was otherwise within normal limits. A blood sample was obtained for complete blood count (CBC), basic metabolic panel (BMP), liver panel, amylase, and lipase. Stool was sent for occult blood, routine cultures, and Escherichia coli O157:H7 culture. The patient was given 10 mg of metoclopramide intravenously for nausea, and a continuous intravenous normal saline infusion was begun. CBC results showed leukocytosis (14,900 white blood cells) with a left shift (88.6% neutrophils). Stool was positive for occult blood. BMP, liver function tests, amylase, and lipase were normal. Because of the patient’ s symptoms, signs, and abnormal blood tests, a computed tomography (CT) scan of the abdomen and pelvis with oral and intravenous contrast was obtained. The CT scan (16 slice multidetector GE Lightspeed) showed diffuse colonic wall thickening and adjacent pericecal fat stranding consistent with pancolitis (Fig. 1). The entire colon was involved contiguously with no evidence of skip lesions. There were no ascites or bowel dilatation. The patient was admitted to the hospital for bowel rest, hydration, and pain control. Stool cultures taken on admission subsequently grew E. Coli O157:H7. The surgical and infectious disease services were consulted. No antibiotics were given. As the patient’ s diarrhea and pain began to improve, his diet was advanced, which he tolerated well. The patient’ s symptoms and leukocytosis resolved, and he was discharged home on the fifth hospital day in stable condition. E. coli O157:H7 is one a highly virulent strain of the bacterium E. coli and a leading cause of food-borne illness. Its virulence stems from its ability to create a potent toxin. Usually, infection with O157:H7 occurs from eating under- cooked and contaminated ground beef. However, infection Emerg Radiol (2007) 14:187–189 DOI 10.1007/s10140-007-0585-1 J. Morgan (*) : M. Bell : M. A. Sadler Department of Radiology, St. Vincent’ s Hospital and Medical Center, 170 West 12th Street, New York, NY 10011, USA e-mail: [email protected]
-
Upload
john-morgan -
Category
Documents
-
view
213 -
download
1
Transcript of CT imaging of acute E. Coli -related colitis

CASE REPORT
CT imaging of acute E. Coli-related colitis
John Morgan & Megan Bell & Michael A. Sadler
Received: 5 December 2006 /Accepted: 31 January 2007 / Published online: 28 February 2007# Am Soc Emergency Radiol 2007
Abstract Patients with abdominal pain and bloodydiarrhea often present in the acute setting to theemergency department for evaluation. After the appropri-ate clinical assessment, cross-sectional imaging is oftenutilized to evaluate for the severity of the disease.Although a wide spectrum of findings may be seen,diffuse colonic mural thickening, consistent with panco-litis, is most common. We report an Escherichia coli0157:H7-related pancolitis in a patient with spinach intakelinked to the recent outbreak.
Keywords Pancolitis . Colon . Infection . CT. Diarrhea .
E. Coli 0157:H7
A 22-year-old man with no significant past medical historywas admitted to the emergency department after complain-ing of abdominal pain and bloody diarrhea for 2 days. Thepatient reported approximately 20 loose, bloody bowelmovements on the day before admission. He described theabdominal pain as constant and diffuse but most severe inthe right lower quadrant. He reported nausea but novomiting, chills, and fever and reported no recent travelhistory. His history was only remarkable for eating saladsfrequently over the past few weeks, most of whichcontained spinach. Physical exam was remarkable formoderate general discomfort and a nondistended abdomen
with tenderness to palpation in the bilateral lower quad-rants. No rebound or guarding was noted. His exam wasotherwise within normal limits. A blood sample wasobtained for complete blood count (CBC), basic metabolicpanel (BMP), liver panel, amylase, and lipase. Stool wassent for occult blood, routine cultures, and Escherichia coliO157:H7 culture. The patient was given 10 mg ofmetoclopramide intravenously for nausea, and a continuousintravenous normal saline infusion was begun. CBC resultsshowed leukocytosis (14,900 white blood cells) with a leftshift (88.6% neutrophils). Stool was positive for occultblood. BMP, liver function tests, amylase, and lipase werenormal. Because of the patient’s symptoms, signs, andabnormal blood tests, a computed tomography (CT) scan ofthe abdomen and pelvis with oral and intravenous contrastwas obtained. The CT scan (16 slice multidetector GELightspeed) showed diffuse colonic wall thickening andadjacent pericecal fat stranding consistent with pancolitis(Fig. 1). The entire colon was involved contiguously withno evidence of skip lesions. There were no ascites or boweldilatation. The patient was admitted to the hospital forbowel rest, hydration, and pain control. Stool cultures takenon admission subsequently grew E. Coli O157:H7. Thesurgical and infectious disease services were consulted. Noantibiotics were given. As the patient’s diarrhea and painbegan to improve, his diet was advanced, which hetolerated well. The patient’s symptoms and leukocytosisresolved, and he was discharged home on the fifth hospitalday in stable condition.
E. coli O157:H7 is one a highly virulent strain of thebacterium E. coli and a leading cause of food-borne illness.Its virulence stems from its ability to create a potent toxin.Usually, infection with O157:H7 occurs from eating under-cooked and contaminated ground beef. However, infection
Emerg Radiol (2007) 14:187–189DOI 10.1007/s10140-007-0585-1
J. Morgan (*) :M. Bell :M. A. SadlerDepartment of Radiology,St. Vincent’s Hospital and Medical Center,170 West 12th Street,New York, NY 10011, USAe-mail: [email protected]

may also occur from eating contaminated vegetables suchas bean sprouts, lettuce, and spinach. This latter host,spinach, was responsible for the major outbreak in latesummer of 2006 (http://www.cdc.gov/ncidod/dbmd/diseaseinfo/escherichiacoli_g.htm). After exposure toO157:H7, the onset of illness is 2–8 days (average of 3–4 days) (http://www.cdc.gov/ncidod/dbmd/diseaseinfo/escherichiacoli_g.htm). Typical presenting symptoms aregenerally nonspecific and include severe bloody diarrhea andabdominal cramps (http://www.cdc.gov/ncidod/dbmd/diseaseinfo/escherichiacoli_g.htm; as in our patient). Withtime, some patients may progress to kidney failure orhemolytic uremic syndrome (HUS; 10%) characterized byhemolysis, thrombocytopenia, uremia, and in some in-stances, death [2]. Although definite diagnosis of E. coliO157:H7 is often made by detecting the bacterium in thestool, imaging with CT may narrow the differential diagnosisas well as assess disease severity.
Most patients recover without specific treatmentwithin 5–10 days (http://www.health.state.ny.us/diseases/communicable/e_coli/fact_sheet.htm). Antibiotics shouldnot be used to treat this infection, and it is thought thattreatment with some antibiotics could lead to renalcomplications (http://www.health.state.ny.us/diseases/communicable/e_coli/fact_sheet.htm) [1]. HUS is morelikely to develop in patients with E. coli 0157:H7 infectionwho received antimotility agents such as loperamide orpatients treated with an antibiotic (http://www.health.state.ny.us/diseases/communicable/e_coli/fact_sheet.htm) [1].Treatment of E. coli colitis is primarily supportive anddirected toward maintaining hydration and electrolytebalance. Presumptive therapy should not be institutedbecause of the potential risks associated with antibiotic
treatment for diarrhea caused by E. coli 0157:H7. Oralrehydration therapy is the preferred treatment for fluid andelectrolyte losses caused by diarrhea with mild-to-moderatedehydration. Intravenous hydration often is administeredfor severe dehydration or when vomiting prevents oralrehydration therapy (http://www.health.state.ny.us/diseases/communicable/e_coli/fact_sheet.htm) [1].
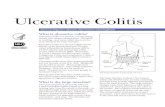
Diagnostic imaging generally may not be required forthe diagnosis of E. coli colitis because the diagnosis isclassically made from clinical findings and a history ofingestion of infected food. Imaging studies combined withan appropriate clinical history can aid in the early diagnosisof E. coli colitis and at the very least, can help narrow thedifferential diagnosis and prevent improper surgical ormedical treatment. Imaging studies are particularly usefulwhen the clinical findings are nonspecific. A CT scan of theabdomen and pelvis with intravenous and oral contrast isthe imaging modality of choice to diagnose E. coli-inducedcolitis [1], as it is more sensitive than conventionalradiographs for detection. As CT becomes standard in theinitial workup of patients with acute abdominal pain, it iscrucial for the radiologist to consider E. coli colitis if giventhe appropriate clinical information. Our patients’ CT scanshowed features of pancolitis that included diffuse colonicmural thickening with adjacent pericolonic stranding(Fig. 2). These features can be seen with other colitides,including pseudomembranous colitis, typhlitis, ischemiccolitis, inflammatory bowel disease, and other infectiouscolitides.
To our knowledge, this is the first known case inradiology literature that describes the CT findings of E.coli colitis that was traced to spinach containing the recentE. coli outbreak strain. E. coli is a relatively under-
Fig. 1 A 22-year-old man with bloody diarrhea. Contrast-enhancedCT shows cecal and descending colonic thickening with pericecal fatstranding
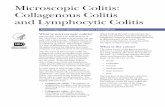
Fig. 2 A 22-year-old man with bloody diarrhea. Contrast-enhancedCT shows thickening of the hepatic flexure
188 Emerg Radiol (2007) 14:187–189

recognized cause of colitis that mimics other medical andsurgical illnesses but can rapidly progress to hemolyticuremic syndrome, a life-threatening condition [1]. As CT isbeing utilized more frequently to determine the severity ofdisease in patients with acute abdominal pain, it is crucial inthe appropriate clinical setting for the radiologist torecognize and consider E. coli colitis.
References
1. Miller FH, Ma JJ, Scholz FJ (2001) Imaging features of entero-hemorrhagic Escherichia coli colitis. Am J Roentgenol 177(3):619–623
2. Koutkia P, Mylonakis E, Flanigan T (1997) EnterohemorrhagicEscherichia coli O157:H7—an emerging pathogen. Am Fam Phys56(3):853–856, 859–861
Emerg Radiol (2007) 14:187–189 189