CSPH Works-in-Progress
60
CSPH Works-in-Progress Cost-Effectiveness Analysis of Thromboprophylaxis for the Prevention of Venous Thromboembolism Associated with Major Urologic Cancer Surgery Ye Wang, PhD Center for Surgery and Public Health August, 2014
-
Upload
hector-hoffman -
Category
Documents
-
view
18 -
download
1
description
CSPH Works-in-Progress. Cost-Effectiveness Analysis of Thromboprophylaxis for the Prevention of Venous Thromboembolism Associated with Major Urologic Cancer Surgery Ye Wang, PhD Center for Surgery and Public Health. August, 2014. Presentation Overview. Background. - PowerPoint PPT Presentation
Transcript of CSPH Works-in-Progress

CSPH Works-in-Progress
Cost-Effectiveness Analysis of Thromboprophylaxis for the Prevention of Venous
Thromboembolism Associated with Major Urologic Cancer Surgery
Ye Wang, PhDCenter for Surgery and Public Health
August, 2014

Presentation Overview
• Background
• PhD Dissertation Project
• Q & A
• Current Project at the Center

Background – Disease Burden in the US
≤4cm
Venous thromboembolism (VTE):
• Deep vein thrombosis (DVT)
• Pulmonary embolism (PE)
Annual incidence:
• > 250,000 clinically evident cases
• ≈ 25,000 deaths per year
Annual VTE-associated health care expenses:
• $1.9 to 4.2 billion
• > $ 5.0 billion in patients with cancers
Heit et al., Arch Intern Med 2008Spyropoulos et al., J Manag Care Pharm 2007
1/3 deaths occur in patients undergoing invasive procedures
Prevention of post-surgical VTE in patients with cancers

Thromboprophylaxis for VTE
≤4cm
Thromboprophylaxis advocated for VTE according to
the ACCP:
ACCP = American College of Chest Physicians
Gould et al., Chest 2012
• Mechanical devicei.e., intermittent pneumatic compression
• Pharmacological agentsi.e., injectable anticoagulants

Cost-Effectiveness of Thromboprophylaxis
≤4cm
Reduced incidence of VTE
Increased costs
Thromboprophylaxis
Complications

Cost-Effectiveness Analysis
≤4cm
The economic, clinical and humanistic outcomes model:
Any disease management should aim to achieve balanced outcomes so that gains in one outcome would not sacrifice the opportunity gains in other outcomes and that the overall gains can be maximized and optimized.
Gunter, Am J Manag Care 1999

Optimize the allocation of limited health care resources
Identify Measure Compare
Costs (e.g., resource consumption) Consequences (e.g., clinical or humanistic outcomes)
Cost-Effectiveness Analysis (continued)
Gunter, Am J Manag Care 1999

Four types of cost-effectiveness analysis:
• Cost-minimization analysis
• Cost-effectiveness analysis
• Cost-benefit analysis
• Cost-utility analysis
Siegel et al., JAMA 1996
Recommended:• Quality-adjusted life
years (QALYs)
• Comparisons across various diseases and health interventions
Cost-Effectiveness Analysis (continued)
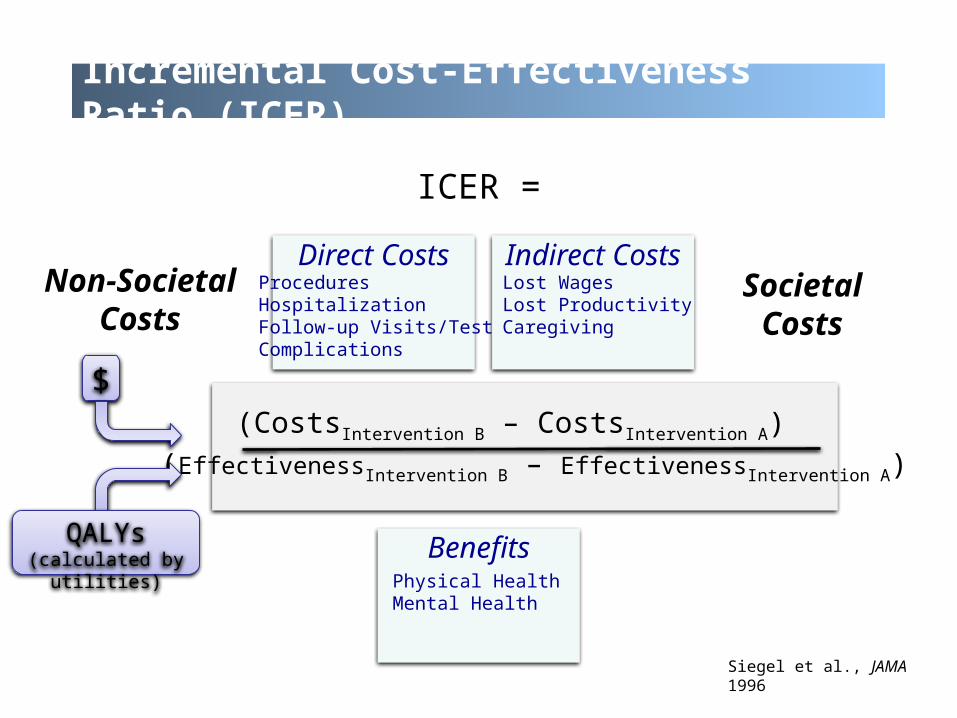
Incremental Cost-Effectiveness Ratio (ICER)
ICER =
(CostsIntervention B – CostsIntervention A)
(EffectivenessIntervention B – EffectivenessIntervention A)
Direct CostsProceduresHospitalizationFollow-up Visits/TestsComplications
Indirect CostsLost WagesLost ProductivityCaregiving
SocietalCosts
BenefitsPhysical HealthMental Health
QALYs(calculated by utilities)
$
Non-SocietalCosts
Siegel et al., JAMA 1996

Utility
Best possible health state
1
Worst possible health state
Death 0
Quality of Life (Utility)
0.4 Symptomatic Metastatic Prostate Cancer
0.2 Above the Knee Amputation
0.6 Severe Congestive Heart Failure
0.8 Disability after Hip Fracture
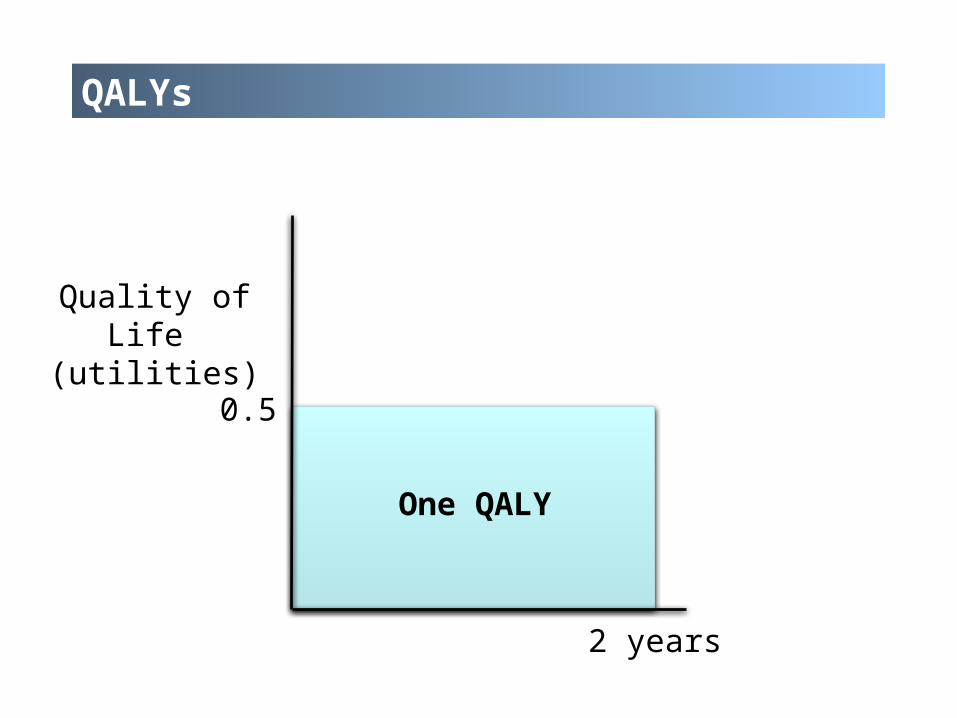
QALYs
0.5
2 years
One QALY
Quality of Life (utilities)
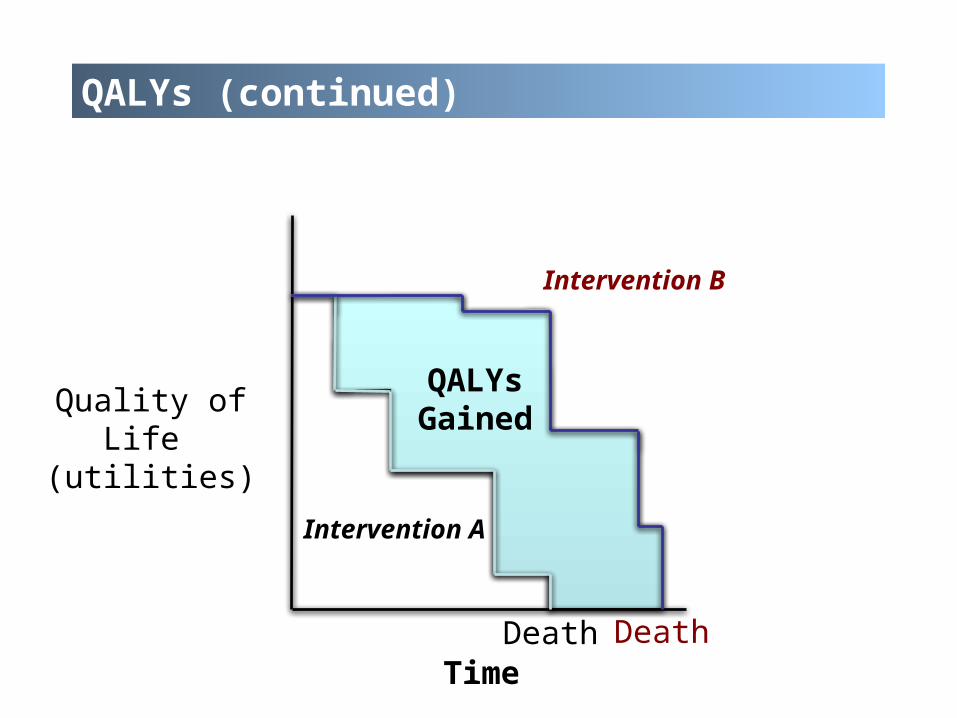
QALYs (continued)
Time
Intervention A
Death Death
Intervention B
QALYsGained
Quality of Life (utilities)

✔
✗
Cost-Effectiveness Analysis
QALYsGained
QALYsLost
Increased Cost
Saves MoneyImproves Health
Costs MoneyWorsens Health
Saves MoneyWorsens Health
Cost MoneyImproves Health
?
?
Decreased Cost
Cost-Effectiveness Plane

Willingness-to-Pay (WTP) Thresholds
Interpreting ICER(US Perspective)
Less than $50,000 per QALY gained Good Value
$50,000 to $100,000 per QALY gained Sometimes Good Value
Greater than $100,000 per QALY gained Rarely Good Value
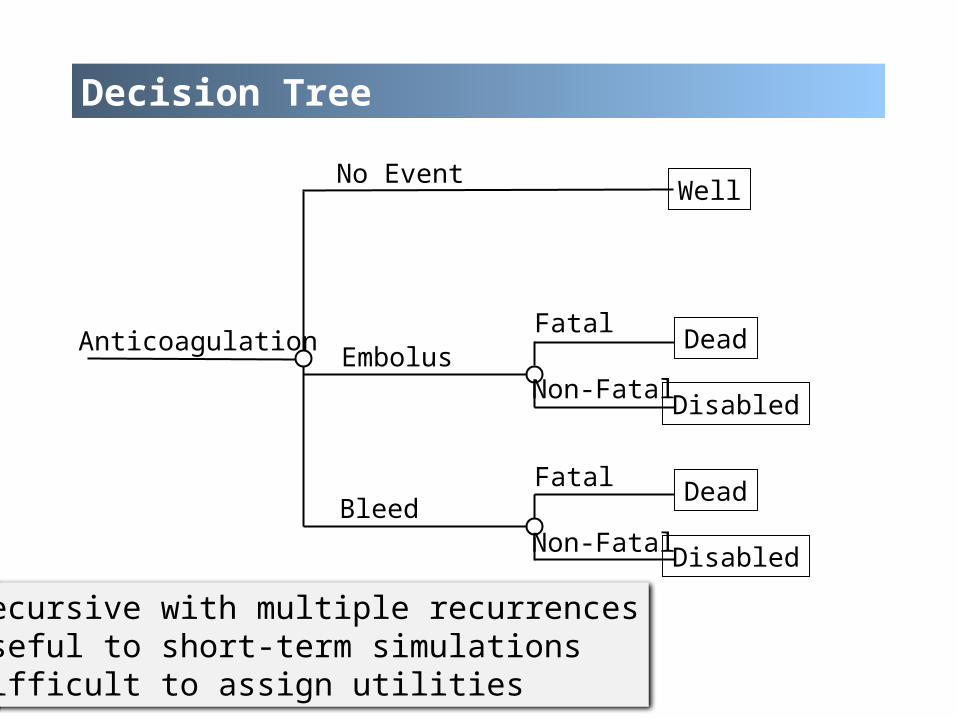
Decision Tree
Anticoagulation
No Event
Embolus
Bleed
Well
Dead
Disabled
Dead
Disabled
Fatal
Non-Fatal
Fatal
Non-Fatal
Recursive with multiple recurrencesUseful to short-term simulationsDifficult to assign utilities
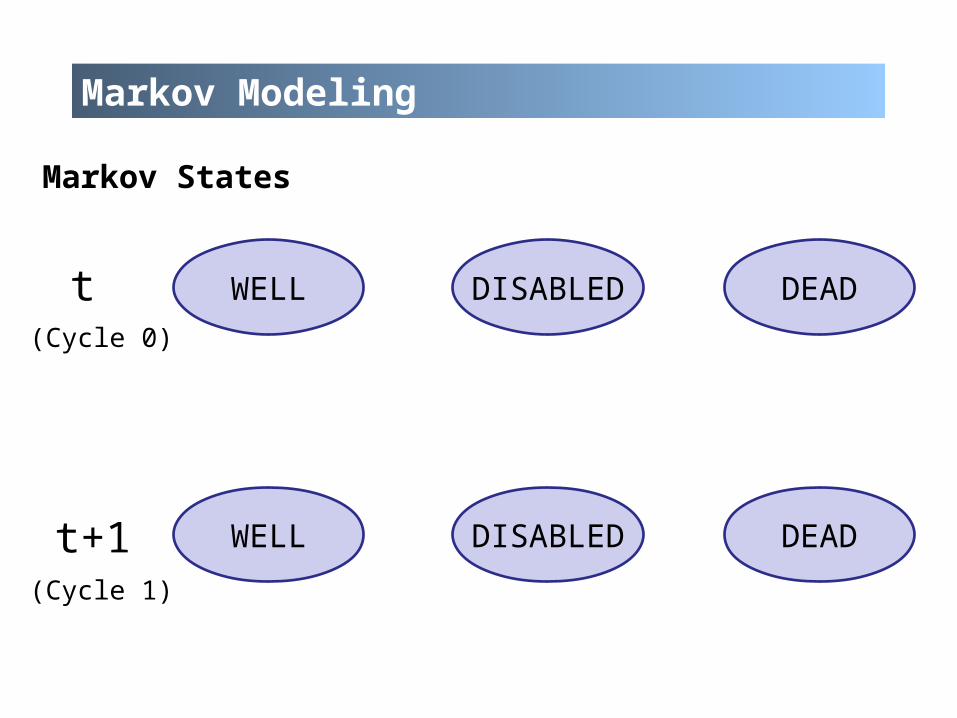
Markov Modeling
WELL DEADDISABLEDt
DEADDISABLEDWELL
Markov States
(Cycle 0)
(Cycle 1)
t+1

Markov Modeling (continued)
WELL DEADDISABLEDt
DEADDISABLEDWELLt+1
Markov States
(Cycle 0)
(Cycle 1)

Markov Modeling (continued)
WELL DEADDISABLEDt
DEADDISABLEDWELLt+1
Markov States

Markov Modeling (continued)
WELL DEADDISABLEDt
DEADDISABLEDWELLt+1
Markov States

Markov Modeling (continued)
WELL
DEADDISABLED
Events can recurSimulate over a lifetime horizonUtilities dependent on the cycle length
Markov States

Markov Modeling (continued)
WELL
DEADDISABLED
Markovian Assumption
Markov States
“memory-less”

PhD Dissertation Project
Part I. Patient-Reported Outcomes of Anticoagulants
• Psychometric properties (validation) of a medication adherence scale
• Evaluation of patients’ knowledge, satisfaction, and barriers to anticoagulant therapy
• …
Part II. Pharmacoeconomics of Anticoagulants• Utility evaluation for anticoagulant-related outcomes• Cost-effectiveness of oral anticoagulants for stroke
prevention in patients with atrial fibrillation

Study 1
Utility evaluation for anticoagulant-related outcomes

Study Design
Study design:• Cross-sectional patient survey
Sample size:• 100 patients
Inclusion criteria• ≥ 21 years old• Taking warfarin• Able to comprehend English or Chinese
Utility elicitation methods:• Standard gamble technique

Health States
Seven long-term health states
• Well on warfarin• Well on dabigatran• Well on rivaroxaban• Major ischemic stroke• Minor ischemic stroke• Intracranial hemorrhage (ICH)• Current health state
Four short-term health states
• Transient ischemic attack (TIA)• Major extracranial hemorrhage (ECH)• Minor ECH• Myocardial infarction (MI)
DescriptionsPublished literature
Preference assessment guidelines
Medical textbooks
Expert opinions
Gage et al., Arch Intern Med 1996Torrance, J Health Econ 1986Warrell et al., Oxford Textbook of Medicine 2003
Health State Descriptions
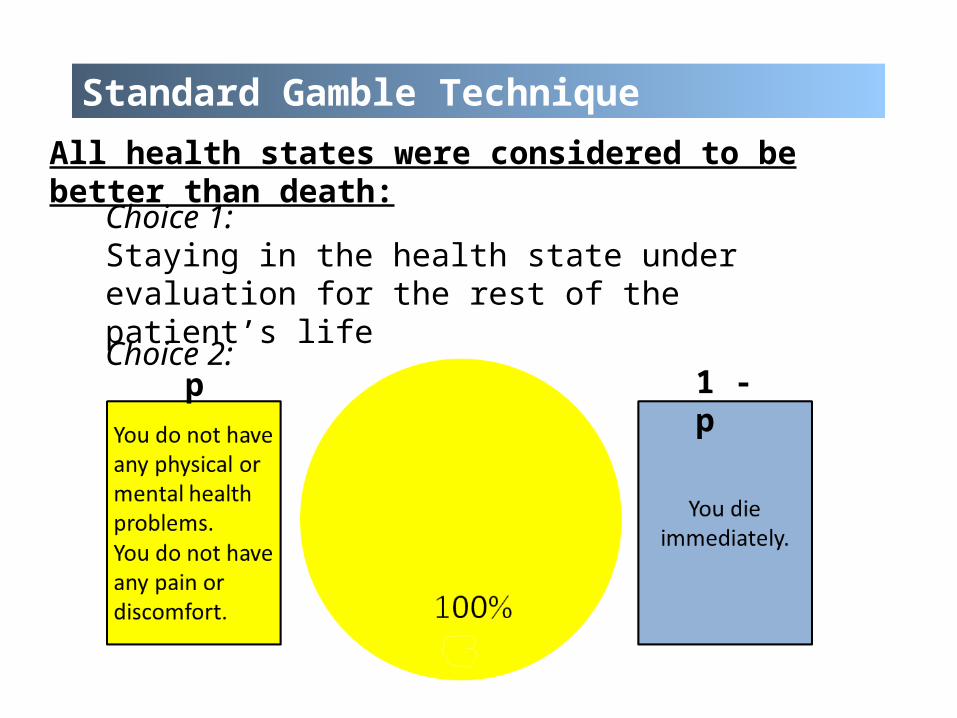
Methods – SGAll health states were considered to be better than death:
Choice 1: Staying in the health state under evaluation for the rest of the patient’s life
p 1 - pChoice 2:
Standard Gamble Technique

p 1 - p
Standard Gamble Technique (continued)
All health states were considered to be better than death:

p 1 - p
Standard Gamble Technique (continued)
All health states were considered to be better than death:
Indifferent – utility value
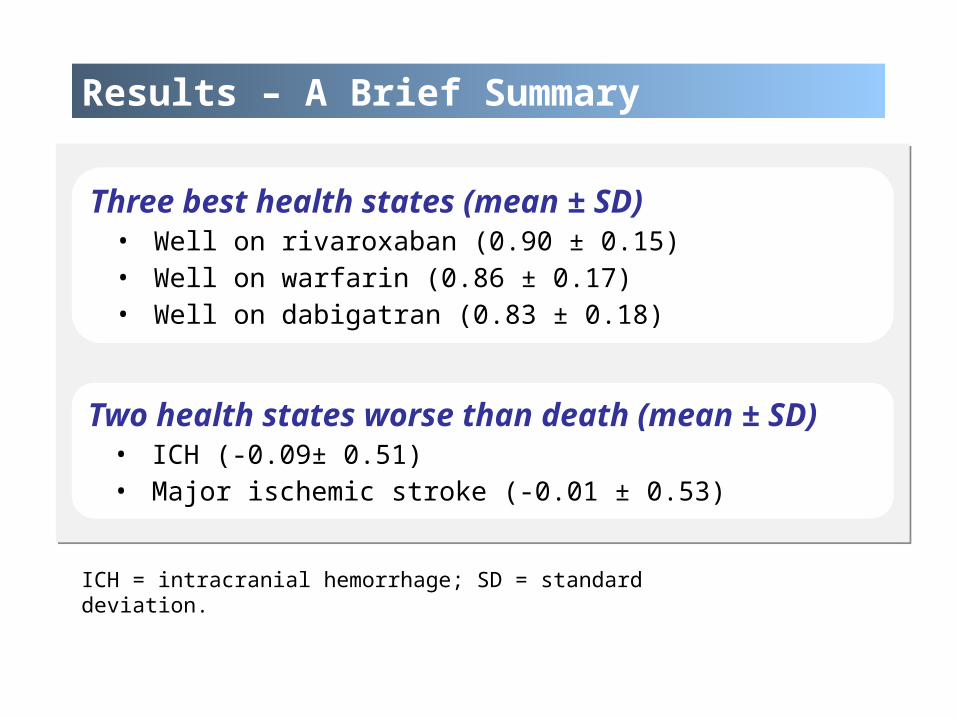
Results – A Brief Summary
Three best health states (mean ± SD)• Well on rivaroxaban (0.90 ± 0.15)• Well on warfarin (0.86 ± 0.17)• Well on dabigatran (0.83 ± 0.18)
Two health states worse than death (mean ± SD)• ICH (-0.09± 0.51)• Major ischemic stroke (-0.01 ± 0.53)
ICH = intracranial hemorrhage; SD = standard deviation.

Study 2
Cost-effectiveness of oral anticoagulants for stroke prevention in patients with atrial fibrillation

Methods – Treatment Options
Treatment options:
• Dabigatran 150 mg twice daily
• Dabigatran 110 mg twice daily
• Rivaroxaban once daily
• Adjusted-dose warfarin

Base case
A hypothetical cohort of patients, who were:
• 65 years old
• Newly diagnosed with atrial fibrillation
• Having no contraindications to anticoagulation
Model Information
Model type:• Markov model
Perspective:• The Singapore health care system
Horizon:• Lifetime
Cycle length:• Monthly
Model Information
Outcomes:• Direct medical costs • QALYs• ICERs
Willingness-to-pay (WTP) threshold: • Singapore’s 2012 per-capita gross domestic product
(SGD 65,000/QALY)
Software: • TreeAge Pro Suite 2013 (TreeAge Software, Inc.,
Williamstown, MA)
Clinical inputs:• Published clinical trials
Utility inputs:• Patient survey
Cost inputs:• Hospital databases
Model Inputs

AF = atrial fibrillation, ECH = extracranial hemorrhage, ICH = intracranial hemorrhage, MI = myocardial infarction, RIND = reversible ischemic neurological deficit, TIA = transient ischemic attack.
Markov Model

AF = atrial fibrillation, ECH = extracranial hemorrhage, ICH = intracranial hemorrhage, MI = myocardial infarction, RIND = reversible ischemic neurological deficit, TIA = transient ischemic attack.
Markov Model

AF = atrial fibrillation, ICH = intracranial hemorrhage, RIND = reversible ischemic neurological deficit.
Markov Model (continued)
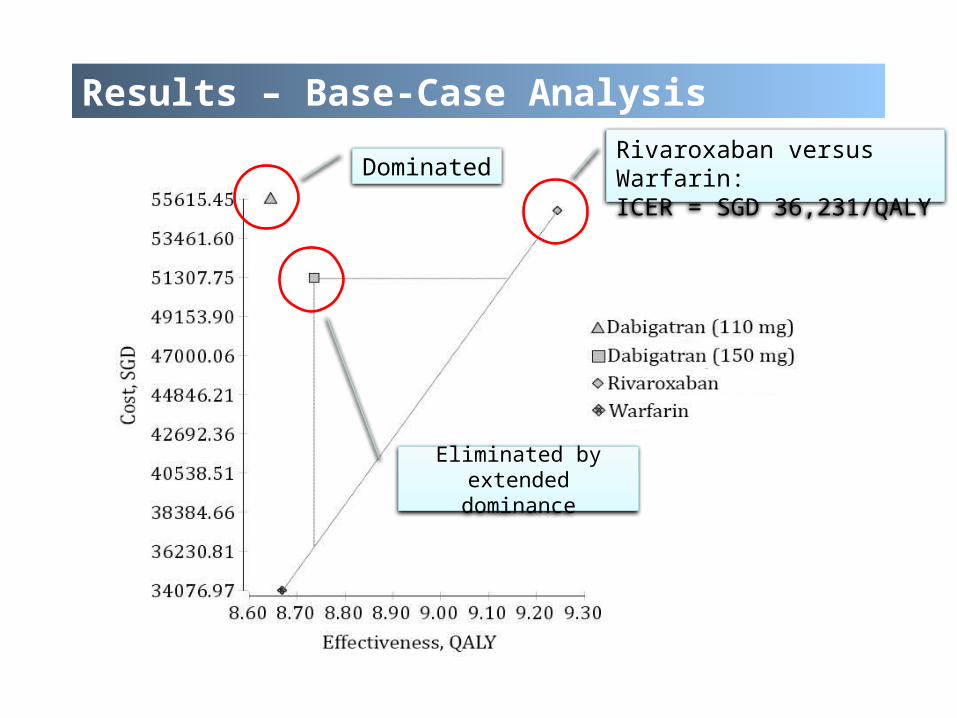
Dominated
Eliminated by extended dominance
Results – Base-Case Analysis
Rivaroxaban versus Warfarin:ICER = SGD 36,231/QALY
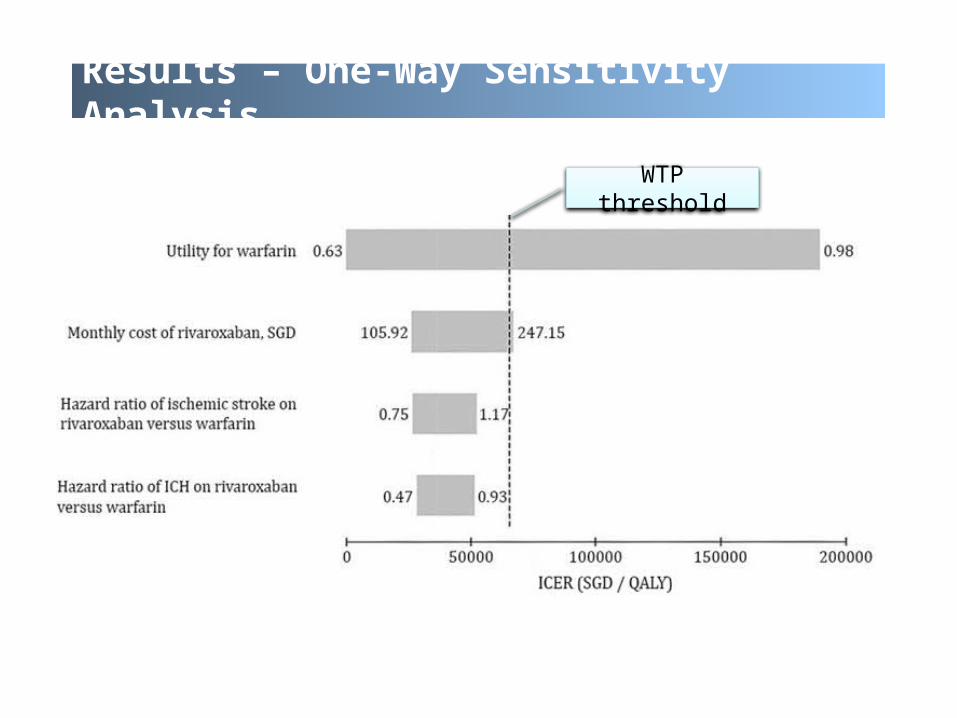
Results – One-Way Sensitivity Analysis
WTP threshold

42
Results – Two-Way Sensitivity Analysis
WTP threshold
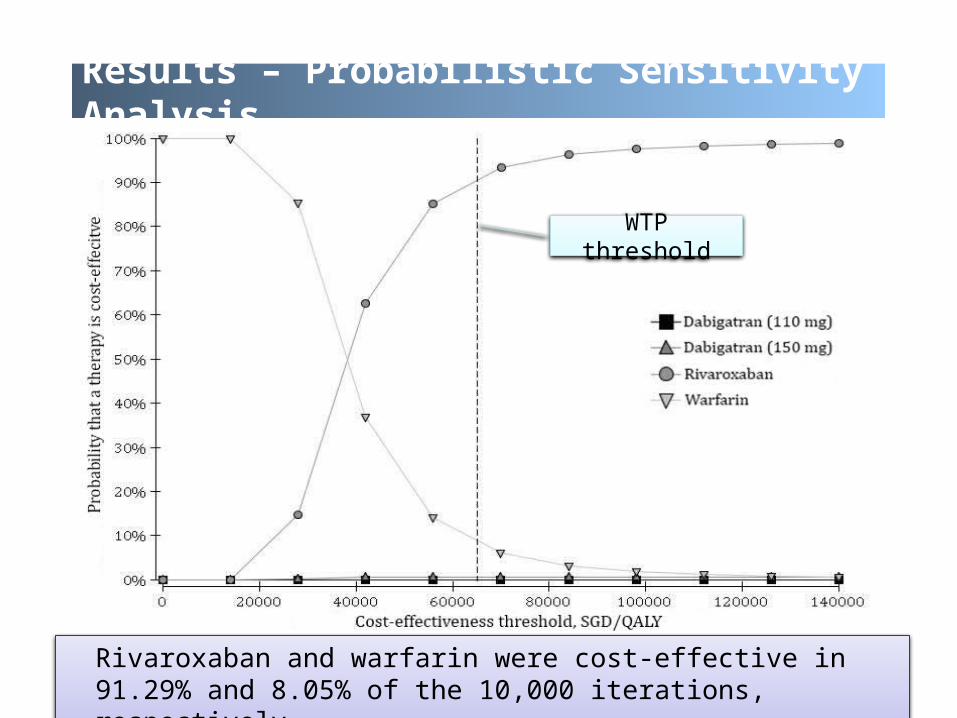
Rivaroxaban and warfarin were cost-effective in 91.29% and 8.05% of the 10,000 iterations, respectively.
Results – Probabilistic Sensitivity Analysis
Results – A Brief Summary
Base-case analysis• Rivaroxaban was the optimal choice compared to warfarin.
• The ICER of dabigatran 150 mg versus warfarin exceeded the WTP threshold.
• Dabigatran 110 mg was dominated by warfarin and rivaroxaban.
Probabilistic sensitivity analysis• Using a WTP threshold of SGD 65,000/QALY, rivaroxaban
and warfarin were cost-effective in 91.29% and 8.05% of the 10,000 iterations, respectively.

Current Project at the CSPH
Cost-Effectiveness Analysis of Thromboprophylaxis for the Prevention of Venous Thromboembolism Associated with Major Urologic Cancer Surgery

Urologic Cancer in the US
≤4cm
National Caner Institute, Surveillance, Epidemiology, and End Results (SEER) Program 2014
Percentage of new cancer cases in the US in 2014
Prostate cancerBladder cancerKidney cancerTesticles cancerOthers
% Ranking14.00 1st 4.50 6th 3.80 8th 0.50 25th
77.20 -

Effect of VTE in patients with urologic cancer
≤4cm
Lyman, Cancer 2011
Prevention of post-surgical VTE in patients with urologic cancer

Thromboprophylaxis for VTE (continued)
≤4cm
Paucity of studies on VTE in the urologic literature
The ACCP recommendations for major urologic cancer
surgery are extrapolated from General Surgery
Ideal use of VTE prophylaxis remains unclear
ACCP = American College of Chest PhysiciansGould et al., Chest 2012

Effectiveness of Thromboprophylaxis for VTE
≤4cm
Study design:• Retrospective data analysis (the Premier)
Inclusion criteria:• Adults (≥18 years old)• Admitted due to major urologic cancer surgery
Major urologic cancer surgery:• Radical prostatectomy• Radical nephrectomy• Partial nephrectomy• Radical cystectomy

Research Question
Are thromboprophylaxis strategies cost-effective for the prevention of post-surgical VTE in patients with
urologic cancer?

Methods – Treatment Options
Mechanical prophylaxis:• Intermittent pneumatic compression (IPC)
Pharmacological prophylaxis (injectable anticoagulants):• Low dose unfractionated heparin (LDUH)• Enoxaparin• Dalteparin• Tinzaparin• Fondaparinux• Argatroban
Comparator:• No prophylaxis

Base case
A hypothetical cohort of patients, who are:
• 65 years old
• Undergoing major urologic cancer surgery
• Radical prostatectomy
• Radical cystectomy• Radical nephrectomy• Partial nephrectomy

Model Information
Model type:• Markov model
Perspective:• Societal
Horizon:• Lifetime
Cycle length:• Monthly

Model Information
Outcomes:• Direct & indirect medical costs • QALYs• ICERs
WTP threshold: • US$50,000/QALY-gained
Software: • TreeAge Pro Suite 2014 (TreeAge Software, Inc.,
Williamstown, MA)

Clinical inputs:• Published literature
Utility inputs:• Published literature
Cost inputs:• The Perspective Database (Premier, Inc, Charlotte, NC)
Model Inputs
Direct medical costs:• Prophylaxis strategy• Complications (minor & major)
Indirect medical costs:• Health care for recovery
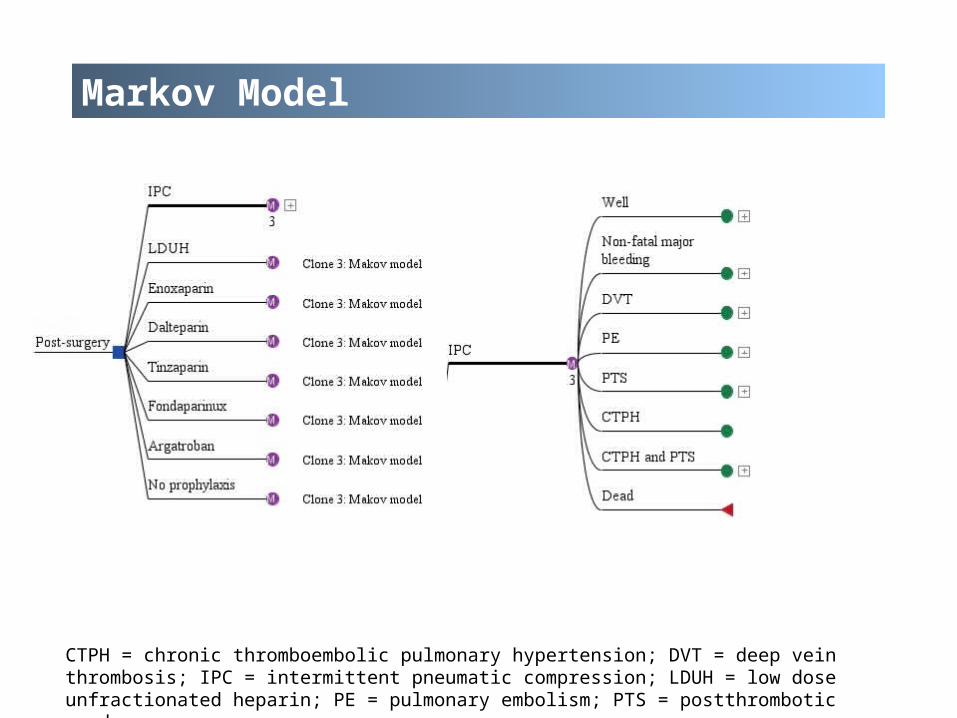
CTPH = chronic thromboembolic pulmonary hypertension; DVT = deep vein thrombosis; IPC = intermittent pneumatic compression; LDUH = low dose unfractionated heparin; PE = pulmonary embolism; PTS = postthrombotic syndrome.
Markov Model

CTPH = chronic thromboembolic pulmonary hypertension; DVT = deep vein thrombosis; PE = pulmonary embolism; PTS = postthrombotic syndrome.
Markov Model (continued)

Further work (specific to this project)
Collect Data:• Costs• Utilities• Probabilities
Perform data analyses:• Base-case analysis• Sensitivity analyses (one-way, multiple-way and
probabilistic sensitivity analyses)

Thanks to Mentor & Other Staff at the CSPH
Thank you!
Questions and Comments
Thank you!
Questions and Comments
Methods – Health state descriptions (cont’d)
• One side of your body is totally paralyzed and/or one side of your face droops.
• You are not able to walk or take care of yourself (e.g., bathing, dressing and feeding) without help.
• You are not able to perform most of your usual activities. • Your speech is unclear, and people have difficulty understanding
you. • You find it hard to write, but you may think clearly.
Major ischemic stroke
The descriptions for each health state consisted of one to six bullet points that described the health state’s important attributes.
An Example of health state descriptions


![FIRST ISSUE PM Rev Description By Date - epd.gov.hk · Chimney Chimney Works in progress Works in progress Works in progress] U ... Õ‡R• ˝‡ C« C ...](https://static.fdocuments.us/doc/165x107/5b586ff37f8b9a527f8c2618/first-issue-pm-rev-description-by-date-epdgovhk-chimney-chimney-works-in.jpg)






![SAHM AM20 Works in Progress Research Symposium … · SAMPLE WORKS IN PROGRESS ABSTRACT SUBMISSION FORMAT Page 4 of 4 [PAGE 2] – ABSTRACT DETAILS & FORMAT PARAMETERS Maximum length](https://static.fdocuments.us/doc/165x107/5f8433535be46c1d22530446/sahm-am20-works-in-progress-research-symposium-sample-works-in-progress-abstract.jpg)