CS 2015 Audiometry Tutorial Christian Stricker Associate Professor for Systems Physiology...
25
CS 2015 Audiometry Tutorial Christian Stricker Associate Professor for Systems Physiology ANUMS/JCSMR - ANU [email protected] http://jcsmr.anu.edu.au/~stricker /Audiometry.pptx THE AUSTRALIAN NATIONAL UNIVERSITY
-
Upload
anissa-cross -
Category
Documents
-
view
221 -
download
3
Transcript of CS 2015 Audiometry Tutorial Christian Stricker Associate Professor for Systems Physiology...

CS 2015
Audiometry TutorialChristian Stricker
Associate Professor for Systems PhysiologyANUMS/JCSMR - ANU
[email protected]://jcsmr.anu.edu.au/~stricker/Audiometry.pptx
THE AUSTRALIAN NATIONAL UNIVERSITY

CS 2015
AimsAt the end of this tutorial students should be able to
• describe afferent anatomical pathways for hearing;
• describe efferent pathways of sensory modulation;
• outline the acustic performance range of the ear in
regard to sound intensities;
• explain how mid-ear changes affect lateralisation;
• locate and discuss how mid-year ossicles are
positioned and affect hearing;
• outline principles involved in sound localisation; and
• interpret simple pathologies revealed in audiogram.

CS 2015
Question 1• Why is the threshold for bone conduction typically
higher than that for air conduction? State the
physical reasons why this is the case.
• Sound wave conduction is inversely related to the
density of the material it is traveling through.
Bone is much denser than air and therefore will
absorb much more energy from the traveling
wave than air.

CS 2015
Question 3• After partially filling the middle ear with serous fluid, how
would bone and air conduction be affected in a case of
early otitis media? How would this change after the otitis
transformed into a purulent and chronic form? Give
physical reasons for your answer.
• Early otitis media: kids typically suffer from hyperacusis –
i.e. they perceive the sound much louder since sound
attenuation is reduced in the middle ear due to water
(serious fluid). As the effusate becomes purulent, it is
becoming more viscous and therefore will dampen the
sound waves much more (hypoacusis).

CS 2015
Question 4• If the left middle ear is damaged, why is a test of
bone conduction lateralized to the left ear?
• Because the sensitivity of the hair cells on the side
of the damaged ear is upregulated due to efferent
innervation; therefore, the same sound intensity
from a tuning fork is perceived to be much louder
in the inner ear of the ear affected by middle ear
damage.

CS 2015
Question 5• Describe/draw the afferent pathways from the inner
ear to the brain that are involved in sound
perception. How many synapses are involved from
the hair cells to the thalamic nucleus?

CS 2015

CS 2015
Question 5• Describe/draw the afferent pathways from the inner ear to
the brain that are involved in sound perception. How many
synapses are involved from the hair cells to the thalamic
nucleus?
• (For details consult a neuroanatomical book).
• The answer to the 2nd part is 4 or 5; depending which
anatomical route is taken. In short, the relay stations are:
Hair cells in organ of Corti → cells of spiral ganglion → cells
of the cochlear nucleus → cells of the lateral lemniscus →
cells of the medial geniculate.

CS 2015
Question 6• Describe/draw the efferent pathways and where the
appropriate nuclei are located in the control of
hearing. State how the activity of these control
neurons affect the perception of sound pressures.

CS 2015

CS 2015
Question 6• Describe/draw the efferent pathways and where the
appropriate nuclei are located in the control of
hearing. State how the activity of these control
neurons affect the perception of sound pressures.
• (For details consult a neuroanatomical book).
• The essence is to be familiar with the olivo-cochlear
reflex. The efferent pathway innervates the outer
hair cells in the cochlea. These then set the
sensitivity of the sound receptors.

CS 2015
Question 7• Draw the pathways for reflectic control of the
middle ear hearing muscles.
• (Again consult a neuroanatomical book).
• Crucial is that from the dorsal superior olivary
nucleus, there are two paths; one to the ventral
cochlear nucleus and the other to the inferior
colliculus from where the innervation of the V and
VII nerve is controlled.

CS 2015
Question 8
• Discuss how sound pressure is
transduced into nerve activity of the
cochlear nerve.
• The hair cell is modulating the firing rate
of the spiral ganglion cell.

CS 2015
Question 9 • Discuss the role of the middle ear in relaying air conduction, in
particular the role of M. tensor tympani and M. stapedius. Why can a
paresis of the N. facialis and/or trigeminus result in a loss of air but
not bone conduction? Also comment on the size of the motor unit in
these two muscles in contrast to for example M. soleus.
• There are two muscles: M. tensor tympani, innervated by V3 moves
the malleus; and the M. stapedius, innervated by VII moves the
stapes.
• If inappropriately innervated, sound is attenuated
• Smallest motor units in the body; one or few muscle fibres controlled
by one motoneurone.

CS 2015
Question 10• Does hypokalaemia affect hearing? Justify your answer by giving the
physiological role of K+ in hearing both in the organ of Corti and the
brain.
• Yes, it does. K+ is essential for the receptor potential of the hair cells.
The apical, sensory surfaces of the hair cells are exposed to the K+-rich
endolymph of the scala media and their lateral and ventral surfaces are
exposed to the perilymph of the scala tympani whose chemical
composition resembles that of other extracellular fluids. The high K+
concentration of the endolymph (150 mM) results from the activity of
electrogenic K+ pumps located in the stria vascularis, which lines the
lateral walls of the cochlea. In hypokalaemia, the receptor potential is
reduced and, therefore, the patient may perceive a hearing loss (not all
patients perceive a hearing loss).

CS 2015
Question 11• Sound localization is a phenomenon on which we rely daily to identify
sources of sound (traffic, conversation), however, the neuronal
mechanisms that allow the localization are not well understood. The
problem is as follows: auditory nerve discharge is maximally around 400
Hz, which would allow a temporal resolution of 2.5 ms between action
potentials. However, the interaural distance is of the order of 20 cm with
a sound velocity of 330 m/s. This results in a maximal timing difference
of ≤ 0.6 ms, which is scaled even more given the angular resolution of a
few degrees. State potential mechanisms that would allow the nervous
system to still perceive this difference even though it is ≥ 4 times faster
than the resolution allowed between two action potentials.
• There is no correct answer to this question. It is a topic of intense
research (delay line? correlation between two ear signal?).

CS 2015
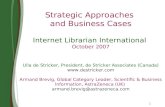
Question 12• The following clinical audiogram was
obtained from a 25 yo man who had a
6-year exposure of loud noises at a
metal factory. He has repeatedly
refused to wear earmuffs thinking that
his ears would tough it out. His
girlfriend had noticed that he on
occasion could not follow normal
conversation, in particular consonants.
Describe and discuss his audiogram.
Are all findings consistent with a single
diagnosis?• Reduction of high frequency perception L > R (C4 reduction) resulting in
“high frequency deafness”. Consistent with single diagnosis (likely more
exposure on the left).

CS 2015
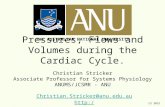
Normal Hearing

CS 2015
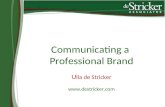
Question 13
This is an audiogram of a 50 yo female
who regularly needs her ears checked.
The audiologist commented that the
hearing was the same at an earlier check
some 6 months ago. Describe and
interpret the audiogram and comment on
the female’s ability to listen and
comprehend normal conversation. What
would help this patient?
• Increased sound perception threshold over the whole range, particularly
accentuated for the higher frequencies. Since her perception of speech
is significantly reduced, she is an excellent candidate for a hearing aid.

CS 2015
Question 14This audiogram of a 23 yo male was
obtained 10 days after an altercation in
which the man received a blow to his right
year. The man complained that he partially
lost his ability to locate a sound source in
his office when the background noise was
increased. Describe and interpret the
audiogram and comment on the male’s
ability to listen and comprehend normal
conversation. What would help this
patient?
• Right sound perception threshold lowered over the whole range. If this
persists and since his perception of speech is significantly reduced on
the right ear, he may become a candidate for a one sided hearing aid.

CS 2015
Question 15The following audiogram was obtained
from a 75 yo male. He visited the
audiologist because his family members
complained that he could not follow normal
conversation. Describe and interpret this
audiogram. Comment on the patient’s
ability to listen to normal conversation, if
and how it is different from presbyacusis
and explore avenues by which this person
could be helped. In particular, discuss
factors involved in peripheral and central
forms of hearing loss.
• Bilateral hearing loss, more at higher frequencies. Slightly affected in the
normal speech range. This is presbyacusis. At the moment, does
unlikely require hearing aid (yet…).

CS 2015
Question 2
• For the following sound pressure levels,
calculate the corresponding sound intensities:
a. 25 dB (a whisper):
b. 75 dB (a car horn)
c. 125 dB (Australian hornet flying over the
War Memorial on
ANZAC day)
d. 175 dB (space shuttle launch)

CS 2015
Answer 2• Crucial is the relationship between sound pressure and
intensity levels: where Jx is the
sound intensity sought and J0 is the reference intensity
value of 10-12 Wm-2. We therefore solve for
• Inserting the correct numbers, you obtain for
a. 25 dB:
b. 75 dB:
c. 125 dB:
d. 175 dB:

CS 2015
Question 2’• Explain why even though the sound levels
increase by 50 dB in each case from a – d,
the sound intensities are so different. What
are the implications for the performance of
the human ear?
• The sound intensities grow by 105 from a – d.
This comes simply out of the formalism. The
human ear therefore spans a performance
range over 12 orders of magnitude.

CS 2015
That’s it folks…