Crit Care Nurse 2004 Albert 14 29
18
Nancy M. Albert, Cathy A. Eastwood and Michelle L. Edwards Evidence-Based Practice for Acute Decompensated Heart Failure Published online http://www.cconline.org © 2004 American Association of Critical-Care Nurses 2004, 24:14-29. Crit Care Nurse http://ccn.aacnjournals.org/subscriptions Subscription Information http://ccn.aacnjournals.org/misc/ifora.xhtml Information for authors www.editorialmanager.com/ccn Submit Manuscript http://ccn.aacnjournals.org/subscriptions/etoc.xhtml E-mail alerts 362-2049. Copyright © 2011 by AACN. All rights reserved. Telephone: (800) 899-1712, (949) 362-2050, ext. 532. Fax: (949) The InnoVision Group 101 Columbia, Aliso Viejo, CA 92656. by American Association ofCritical-Care Nurses, published bi-monthly Critical Care Nurse is the official peer-reviewed clinical journal of the by guest on June 20, 2014 http://ccn.aacnjournals.org/ Downloaded from by guest on June 20, 2014 http://ccn.aacnjournals.org/ Downloaded from
-
Upload
neng-fajar -
Category
Documents
-
view
17 -
download
3
Transcript of Crit Care Nurse 2004 Albert 14 29
-
Nancy M. Albert, Cathy A. Eastwood and Michelle L. EdwardsEvidence-Based Practice for Acute Decompensated Heart Failure
Published online http://www.cconline.org 2004 American Association of Critical-Care Nurses
2004, 24:14-29. Crit Care Nurse
http://ccn.aacnjournals.org/subscriptionsSubscription Information
http://ccn.aacnjournals.org/misc/ifora.xhtmlInformation for authors
www.editorialmanager.com/ccnSubmit Manuscript
http://ccn.aacnjournals.org/subscriptions/etoc.xhtmlE-mail alerts
362-2049. Copyright 2011 by AACN. All rights reserved.Telephone: (800) 899-1712, (949) 362-2050, ext. 532. Fax: (949)The InnoVision Group 101 Columbia, Aliso Viejo, CA 92656.
byAmerican Association ofCritical-Care Nurses, published bi-monthly Critical Care Nurse is the official peer-reviewed clinical journal of the
by guest on June 20, 2014http://ccn.aacnjournals.org/Downloaded from by guest on June 20, 2014http://ccn.aacnjournals.org/Downloaded from
-
14 CRITICALCARENURSE Vol 24, No. 6, DECEMBER 2004
Nancy M. Albert is certified as a clinical nurse specialist and has a dual role of director of nursing research in the division of nursingand clinical nurse specialist at the George M. and Linda H. Kaufman Center for Heart Failure of the Cleveland Clinic Foundation,Cleveland, Ohio. She codeveloped heart failure programs along the continuum of care, including emergency care, critical care, and acutecare, at the Cleveland Clinic Foundation.
Cathy A. Eastwood graduated with a master of nursing degree from the University of Calgary, Canada, after specializing in the care ofpatients with heart failure. She developed and managed the outpatient heart failure center and oversaw the flow of inpatients with heartfailure at St. Lukes Episcopal Hospital, Houston, Tex. Currently, she is a lecturer at Memorial University of Newfoundland, School ofNursing, in St. Johns, Newfoundland, Canada.
Michelle L. Edwards earned a master of science degree in nursing from the University of Alabama at Birmingham and is a board-certified family and acute care nurse practitioner. She practiced several years in critical care, specializing in the care of cardiovascularpatients. She currently is a cardiology nurse practitioner/outcomes manager at St. Lukes Episcopal Hospital.
Each year, chronic left ventric-ular systolic and diastolic dysfunc-tion, or heart failure, causes 1million hospitalizations in theUnited States.1 Heart failure is themost common Medicare diagnosisrelated group at discharge1,2 and isassociated with poor survival andquality of life. In addition, cost ofcare is high; in 1998, Medicare paid
out $3.6 billion for care related toheart failure.1
The Acute Decompensated HeartFailure National Registry (ADHERE)3
recently reported data on 14 716patients hospitalized for heart failurein the United States (Tables 1 and 2).Generally, patients admitted to thehospital for heart failure were elderly,were female, had a history of heart
CoverArticle
Authors
CE This article has been designated forCE credit. A closed-book, multiple-choiceexamination follows this article, which testsyour knowledge of the following objectives:
1. Identify the core drug therapies for decompensated heart failure
2. Describe the role of B-type natriuretic peptide in decompensated heart failure
3. Explain the pharmacological managementof decompensated heart failure
Nancy M. Albert, RN, MSN, CCNS, CCRN, CNACathy A. Eastwood, RN, MNMichelle L. Edwards, RN, MSN, FNP, ACNP
To purchase reprints, contact The InnoVision Group, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 809-2273 or (949) 362-2050 (ext 532); fax, (949) 362-2049; e-mail,[email protected].
CEContinuing EducationEvidence-Based Practice forAcute DecompensatedHeart Failure
by guest on June 20, 2014http://ccn.aacnjournals.org/Downloaded from
-
failure, and were unable to carry outactivities of daily living without exer-cise intolerance. The most commonsymptom was dyspnea, which wasmost often associated with other signsand symptoms of fluid retention.Comorbid conditions were common,and patients were equally likely tobe admitted with systolic dysfunction(reduced ventricular contractility;ejection fraction 0.40) or diastolicdysfunction (impaired ventricularrelaxation or ventricular stiffness
tion that led to signs and symptomswas impaired ventricular relaxation,which was associated with increasedage, obesity, hypertension, and car-diovascular disease.4 In addition,ADHERE data were comparable todata from other reports6-8 in thatretention of fluid and sodium, asevidenced by admitting signs andsymptoms, was a primary factor inhospitalization. This knowledge pro-vides an opportunity for care improve-ment that can be championed bynurses, because hospitalization forfluid and sodium retention in patientswith systolic or diastolic dysfunctionmay be avoidable, especially whensuch retention is due to patients fail-ure to adhere to medication regimensor self-care instructions.
In this article, we discuss evidence-based practices for managing patientswith acutely decompensated heartfailure because in-hospital actionsmay facilitate an improved experiencefor patients after hospitalization.The intent is to provide management
that decreases theventricles abilityto fill). One quar-ter of patients wererehospitalizedwithin 6 monthsof a previous hos-pitalization, andMedicare was theprimary hospitalpayor. Mostpatients spenttime in the emer-gency department
before admission as an inpatient, andthe most common level of initial carewas telemetry. Median length of staywas 4.4 days.3
The ADHERE data are similar todata from other studies4,5 in whichinvestigators found an equal split ofpatients with impaired and preservedleft ventricular systolic function, sig-nifying hospitalization of patientswith systolic dysfunction and patientswith diastolic dysfunction. The pri-mary mechanism of diastolic dysfunc-
CRITICALCARENURSE Vol 24, No. 6, DECEMBER 2004 15
Table 2 Outpatient medications before hospitalization andmedications at discharge: data from the Acute DecompensatedHeart Failure National Registry3
Medication class
% of patients
8758
1345
3372
5422372748343
7242
1134
2854
4423302338307
DiureticAngiotensin-converting
enzyme inhibitorAngiotensin II receptor blockerHydralazine plus nitrateHydralazineNitrateAngiotensin-converting enzyme
inhibitor, hydralazine, plusnitrate or angiotensin IIreceptor blocker
-BlockerCalcium channel blockerDigoxinWarfarinAspirinLipid-lowering agentNonsteroidal anti-inflammatory
drugs
Before hospitalization(n = 14 716)
At discharge(n = 11 187)
Table 1 Characteristics of patients, clinical signs and symptoms, and hospital placement: data from the AcuteDecompensated Heart Failure National Registry3
Characteristics at hospital admission % of patients
5268507725
433271315830
442816
8
9234726935
384920
7722
6513
8
FemaleMedicare, primary payerEjection fraction 177 mol/L (2.0 mg/dL)Point of entry to the hospital
Emergency departmentDirect admission
First inpatient unitTelemetryWard or intensive or coronary careStepdown
*Dyspnea, fatigue, palpitations, or chest pain with minimal activity.Dyspnea, fatigue, palpitations, or chest pain at rest.Percentage of each.Mean serum level of sodium was 138 mmol/L, and median level of B-typenatriuretic peptide was 784 pg/mL.
by guest on June 20, 2014http://ccn.aacnjournals.org/Downloaded from
-
goals and actions associated with themost common clinical manifestation,fluid retention, and not to focus onmanagement of cardiogenic shock,profound hypoperfusion, or complexdecompensation (severe hyper-volemia, hypoperfusion, and acidosisor other conditions such as pneumo-nia). Assessment of patients, man-agement strategies, and education ofpatients are highlighted. Mythsassociated with acute care manage-ment are discussed so that nurseswill be more aware of appropriateinterventions that are safe and effec-tive. Heart failure management hasprogressed rapidly in recent years.Ultimately, nurses must be proactivein ensuring that their behaviors arebased on current evidence.
Heightened Expectations for Evidence-Based Care
Nurses are challenged to plan andprovide care that promotes the bestpossible clinical and health-relatedoutcomes. The Joint Commission onAccreditation of Healthcare Organi-zations9 recently established 4 coremeasures in the acute managementof patients with heart failure to pro-mote adherence to basic standards ofevidence-based care (Table 3). Becauseof the large number of patients andthe high cost of care associated withhospital readmissions, acute andcritical care nurses must developand implement strategies that areassociated with improved outcomesfor patients and hospitals. In addi-tion, in 2001, the American Collegeof Cardiology (ACC) and the Ameri-can Heart Association (AHA) pub-lished practice guidelines10 for adultswith chronic heart failure. Theseguidelines provide caregivers withrecommendations for nonacute care
and include the rationale and levelof evidence for support of each man-agement strategy. Table 4 providesa list of management strategies,including core drug therapies, thatshould be a part of each patientstreatment plan at discharge afteran admission for decompensatedheart failure stemming from vol-ume overload.10,11
If the medica-tion expectationslisted in Table 4are compared withthe actual med-ication therapiesbefore hospital-ization and at dis-charge indicatedin the ADHEREdata (Table 2), aneed for change isevident. Newefforts must beundertaken topromote use of
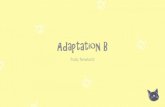
consensus guidelines and therapiesto meet the overall goal of manag-ing heart failure: promoting regres-sion and preventing progression ofleft ventricular enlargement (remod-eling) to decrease disease progres-sion and improve survival.11-14 SeeFigure 1 and Table 5 for definitionand description of consequences ofventricular remodeling.
16 CRITICALCARENURSE Vol 24, No. 6, DECEMBER 2004
Table 3 The 4 core measures of the Joint Commission onAccreditation of Healthcare Organizations
Written discharge instructions or educational material must begiven to the patient or caregiver and include all of the follow-ing: activity level, diet, discharge medications, follow-upappointment, weight monitoring, and symptom management
Left ventricular function must be documented in the hospitalrecord to indicate that it was assessed before or during hos-pitalization, or will be assessed after discharge
Patients with known systolic dysfunction of moderate tosevere impairment (ejection fraction 130 ms), and other inclusion
criteria to determine if cardiac resynchronization devices are appropriate
Angiotensin-converting enzyme inhibitors-BlockersDigitalisDiureticsSpironolactone (if condition is unstable with preceding drugs and patient is in New
York Heart Association functional class IV)
*Stage C is referenced in American College of Cardiology/American Heart Association practice guidelines10and is part of a 4-stage classification of heart failure by evolution and progression of the disease. In stageC, patients have structural heart disease of the myocardium, pericardium, or cardiac valves with prior orcurrent symptoms (shortness of breath, fatigue, exercise intolerance) of heart failure.
by guest on June 20, 2014http://ccn.aacnjournals.org/Downloaded from
-
No standardized evidence-basedguidelines are available to direct acutecare; however, randomized, placebo-controlled research studies providestrong support for actions that areeffective and safe. In addition, manyactions promoted in the currentguidelines for long-term outpatientmanagement of heart failure can betranslated to the acute setting and
are not in cardiogenic shock or donot have profound hypoperfusion orcomplex decompensation. Imple-mentation of the following strategiesmight require a change in the philos-ophy of care, further education, andcontinuous quality monitoring toensure that evidence-based strategiesare used regardless of the type ofphysician, a patients placement(telemetry or nonmonitored bed), anurses background (cardiac, heartfailure, or generalist), or a hospitalsresources.
Assessment of PatientsBefore planning interventions for
a patient hospitalized with heart fail-ure, the healthcare team must conducta systematic assessment that includesidentification of the cause of the heartfailure, aggravating factors, potentialrisk factors that may influence survivaland quality of life, and current clinicalstatus. Patients comorbid conditions,especially active chronic conditions,may act as exacerbating factors(Table 6), affecting the planning ofpatients care and influencing thetiming and intensity of therapies. Thetreatment plan must include modifi-cation of correctable causes ofdecompensation. Examples includeeducation for sodium indiscretion,alcohol abstinence programs for over-consumption of alcohol, or revascu-larization strategies for hibernatingmyocardium (ie, viable but under-perfused myocardial tissue withdecreased contractility). In addition,risks related to heart failure must beconsidered, such as the need foranticoagulation to prevent embolicevents or the need for an implantablecardioverter-defibrillator to preventsudden cardiac death, so that appro-priate consultations and therapies are
provide a uniform plan of care basedon large, multicenter, randomizedresearch studies that focus on the pri-mary management goal of prevent-ing progression of heart failure.10
Nurses can facilitate some practi-cal assessment and managementstrategies that apply to patientsadmitted to the hospital with a pri-mary diagnosis of heart failure who
18 CRITICALCARENURSE Vol 24, No. 6, DECEMBER 2004
Table 5 Ventricular remodeling: definition and consequences
Definition
Consequences
A cascade of changes in genome expression, cells, molecules, and interstitium thatalters the size, shape, and function of the left ventricle after injury.
Alterations in heart size and shape (volume) that are not associated with preload-mediated increase in myocyte length.
Hallmarks leading to change in shape of left ventricle from a V to a U. Combination ofDilatation (myocyte lengthening and cell slippage)Cell loss/death (apoptosis)Interstitial fibrosisHeart failure after myocardial infarction: formation of a discrete collagen scarNonischemic heart failure: isolated fibrosis
Hypertrophy (see Figure 1b and c)Initially concentric (thickening of myocytes) Then becomes eccentric (thinning of the left ventricular walls)
High pressure (wall stress) in the ventricle during systole and diastole heightensmyocardial oxygen consumption, a situation that promotes further hypertrophy andactivates neurohormonal systems
Reduction in ejection fractionReduced ventricular performanceMorbidity and mortality
Figure 1 Ventricular remodeling. Cross-sectional view of left and right ventricles: a, normal; b, concentric hypertrophy; and c, eccentric hypertrophy.
Abbreviations: LV, left ventricle; RV, right ventricle.Produced and printed with permission from The Cleveland Clinic Foundation; Cleveland, Ohio.
a
RV RV RVLV LV LV
b c
by guest on June 20, 2014http://ccn.aacnjournals.org/Downloaded from
-
discussed and initiated before patientsare discharged from the hospital.
Hemodynamic Status: Volume and Perfusion
Volume and perfusion statusprovide useful clues to a patientscardiac performance and help shapethe treatment plan. Nurse caregiversmust frequently reassess the patientshemodynamic status to determinevolume and perfusion status. Volumestatus is determined by assessing ifthe patient is wet, dry, or has a bal-anced fluid level (ie, has hypervolemia,hypovolemia, or euvolemia, respec-tively), and perfusion is assessed bydetermining if the patient is cold,cool/lukewarm, or warm (ie, hasperfusion that is very low, slightlylow, or normal, respectively). Evi-dence of congestion includes thesigns of neck vein distension, ele-vated pressure in the right internaljugular vein, positive abdominal-jugular neck vein reflex, edema,ascites, and crackles (rarely) and thesymptoms of dyspnea, orthopnea,and paroxysmal nocturnal dyspnea.15
Nurses must be careful not to counton the presence of crackles as an indi-
cator of congestion because chronicmovement of fluid into the intersti-tium (common in patients with ahistory of chronic heart failure) isassociated with increased lymphaticdrainage so that crackles are absentand the alveoli remain relatively dry.16
Evidence of very low perfusionincludes symptomatic hypotension,especially in patients receivingangiotensin-converting enzyme (ACE)inhibitors, cool extremities (arms andlegs, not just hands and feet), mentalobtundation or constant sleepiness,worsening renal function (elevationin serum levels of creatinine andurea nitrogen), hyponatremia, nar-row pulse pressure, and, most impor-tant, a proportional pulse pressure of25% or less.15,16 Acute care nurses
should be educated in calculating pro-portional pulse pressure. The calcula-tion is simple to do and can provide
valuable information about cardiaccontractility and perfusion, especiallywhen trends over time are assessed.
The formula to determine pro-portional pulse pressure is (systolicblood pressure - diastolic bloodpressure)/systolic blood pressure,resulting in a proportion or percent-age.16 An example of a calculation ofproportional pulse pressure is (108 -66)/108 = 42/108 = 0.389 or 39%.
In a hemodynamic study16 of 50patients with a history of heart fail-ure, 91% of patients with a propor-tional pulse pressure of 25% or lowerhad a cardiac index (calculated ascardiac output in liters per minutedivided by body surface area insquare meters) of less than 2.2; how-ever, systolic and mean arterial bloodpressure were poorly correlated withcardiac index or stroke volume index.In a study17 of hemodynamic profiles(wet, dry, cold, and warm) and clini-cal characteristics of advanced heartfailure, a low proportional pulse pres-sure was the only predictor of wetpatients, and among wet patients,proportional pulse pressure was theonly predictor of patients in the coldcategory. A patients hemodynamicprofile should influence initiation ofpharmacological and other treat-ment strategies and also guide theadjustment of therapies during thehospitalization.
Of note, patients who are admit-ted in a congestive or wet state witha high preload (passive stretch of
CRITICALCARENURSE Vol 24, No. 6, DECEMBER 2004 19
Table 6 Exacerbating factors in chronic heart failure that lead to decompensation
Uncontrolled hypertensionAtrial fibrillation or flutter with fast ventricular responseFrequent premature ventricular contractions or ventricular tachycardiaAcute myocardial ischemiaWorsening bundle branch block or intraventricular conduction delay due to desynchro-
nized ventricular electrical cell conduction and myocyte contraction Treatment of diabetes with thiazolidinediones (Actos or Avandia)Treatment of arthritis, muscular, or pain conditions with routinely administered
nonsteroidal anti-inflammatory drugs or high doses of aspirin Concurrent infections (pneumonia, viral illnesses)ObesityHyperthyroidism or hypothyroidismUntreated anemia (hemoglobin
-
20 CRITICALCARENURSE Vol 24, No. 6, DECEMBER 2004
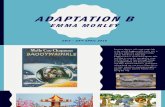
Figure 2 Acute decompensated systolic heart failure (SHF) or diastolic heart failure (DHF) in patients with chronic heart failure: initial treatment of Abbreviations: BNP, B-type natriuretic peptide; EKG, electrocardiographic; INR, international normalized ratio; IV, intravenous; PT, prothrombin time.*Treatment decisions based on serum BNP results in acute decompensated heart failure DO NOT apply to patients with chronic, stable heart failure who are not acutely dyspneic.Profiles: patient is wet, dry, or has a balanced fluid level (ie, has hypervolemia, hypovolemia, or euvolemia, respectively), and is cold, cool/ lukewarm, or warm (ie, has perfusion that isvery low, slightly low, or normal, respectively).
Dyspnea and chest pain: if cardiac markersare positive and/or EKG findings are abnormal:Follow Acute Coronary Syndrome protocol.
Admit to hospital or23-hour observation/short-
stay unit on the basis of resultsof workup and signs and
symptoms
Admitto hospital for IV
and oral pharmacologicaland nondrug therapies and
monitoring; consider cardiacresynchronization, implantable
defibrillator, and/or surgicaltherapies; treat comorbid
factors that affectheart failure
BNP >600 pg/mL*
Meets Wet and Cold profileand systolic blood pressureis 100 pg/mL but 600 pg/mL*
DyspneaWorkup: history/physical examination; oxygen saturation; laboratory tests: BNP, PT/INR, liver
function, basic metabolic profile, hematology, arterial bloodgases, troponin or other markers of cardiac injury; electrocardio-
gram, chest radiograph, and other tests on basis of history
Admit to coronary or intensive care unit
Consider invasive or noninvasivehemodynamically guided care
IV inotropic therapy may be warranted
No
Consider discharge home withinstructions to follow
up with primaryhealthcare provider
in 1-3 days
by guest on June 20, 2014http://ccn.aacnjournals.org/Downloaded from
-
myocardial fibers; reflects left ven-tricular end-diastolic pressure andvolume) often have a high afterload(pressure the heart must pumpagainst; reflects systemic vascularresistance, systolic stress, and systolicimpedance) that impairs stroke vol-ume and is reflected as a cool orlukewarm perfusion state. Whenhemodynamic measurements wererecorded in 750 patients with heartfailure before tailored therapy at alarge university teaching hospital,the mean pulmonary artery occlusivepressure was 26 mm Hg (normal is4-12 mm Hg; in heart failure treat-ment, the goal is 8-15 mm Hg) andthe mean systemic vascular resistancewas 1640 dynes sec cm-5 (normalis 800-1200 dynes sec cm-5),15
reflecting a vasoconstricted state andthe need for vasodilator therapy inaddition to diuresis and natriuresis(sodium excretion).
Diagnostic TestsIn addition to results of tests done
at the time of admission (chest radi-ographs, arterial blood gas levels,liver function tests, hematologic tests,electrocardiograms, basic metabolicprofile) and findings on physicalexamination, the results of point-of-care assays of serum levels of natri-uretic peptides can be used to guidetreatment in patients with acutedecompensated heart failure (Figure2). B-type natriuretic peptide (BNP) issecreted mainly from the ventricularmyocardium in response to elevationsin end-diastolic pressure and ventric-ular volume expansion.18 Not onlycan rapid measurement of BNP aidin diagnosis of heart failure,19-23 butBNP level can also be used to assessclinical status and the effectivenessof therapies during an admission foracute decompensation.24
Point-of-care BNP testing can bea useful adjunct in determiningwhich patients are receiving effectivecare, which patients are not progress-ing on the current treatment plan,and which patients might be candi-dates for end-of-life care. Nursesshould consider all components ofassessment of patients (etiology,aggravating factors, risks, and clini-cal status) when communicating andcollaborating with members of thehealthcare team so that patientshave the best opportunity for carestrategies that optimize outcomesand promote comfort.
Myths and Realities of Management
An algorithm provides a system-atic approach to decision making aspatients with chronic heart failureare assessed and managed during anacute exacerbation (Figure 2). Themyths associated with managementof acute heart failure are replaced withevidence-based actions that con-tribute to the best possible outcomes.
Myth 1: The Goals of Treatmentfor Acute and Chronic HeartFailure Are Different
One of the hurdles in managementof heart failure is to overcome themyth that the goals of managing acutedecompensated and stable heart fail-ure are different. Today, it is impor-tant to gear therapies toward reversalof ventricular remodeling. Reversingventricular remodeling is importantregardless of whether patients are instable condition or in a decompen-sated state. Historically, the primarygoal of treatment of acute decom-pensated heart failure was to quicklyreduce the circulating fluid volumeto relieve patients of the pulmonaryand peripheral edema. Diuretics
CRITICALCARENURSE Vol 24, No. 6, DECEMBER 2004 21
Consider discharge home
with instructions tofollow up with primary
healthcare providerin 1-3 days
Heart failure an unlikelycause; consider other causes:
pulmonary embolism, pneumothorax,pulmonary diseases, pneumonia,
arrhythmias, liver or kidneydiseases
BNP 500 mL (DHF)
or 1000 mL (SHF) with normalrenal function or >250 mL (DHF)
or 500 mL (SHF) with renal insufficiency)?
Is dyspnea resolving?
No
Yes
Yes
Consider comorbid conditions causing dyspnea If meets Wet and Cold, Dry
and Cool to Cold, Wet and Coolto Cold, or Wet and Warmprofile: treat as appropriate
dyspnea in the emergency department.
by guest on June 20, 2014http://ccn.aacnjournals.org/Downloaded from
-
have long been the standard type ofdrug used for decreasing volumeand improving hemodynamic statusand signs and symptoms.25 Throughresearch studies, however, it waslearned that acute intravenousdiuretic therapy was associated withmany hazards, including increasedmortality. Nonpotassium-sparingdiuretic therapy was associated withan increased risk of arrhythmic(sudden) death, increased cardiacmortality, aggravated renal dysfunc-tion, further activation of the renin-angiotensin and sympathetic nervoussystems with a concomitant increasein systemic vascular resistance that
was compounded by a decrease incardiac output from a reduction inpreload, and electrolyte imbalancesthat caused muscle weakness,depression, reduced contractility(from reduced conductivity), andperipheral vasoconstriction.26-31 Inpatients with acute decompensation,preventing or limiting further activa-tion of neuroendocrine systems byusing strategies that target excessintravascular and extravascular vol-ume and vascular resistance willhelp meet the overall goals of pre-venting progression of and promotingreversal of ventricular remodeling.
Myth 2: Managing Fluid Overload Equals Use of Diuretics
Administration of intravenousand oral loop diuretic agents is animportant therapy aimed at decreas-
in patients with mild to severe heartfailure, as summarized in the consen-sus guidelines.10 Researchers reportedimprovements in exercise tolerance,ejection fraction, and survival alongwith decreased rehospitalizationrates.10 Therefore, diuretics are nec-essary to relieve signs and symptomsbut should be used with ACE inhibitortherapy for survival benefit and tocounterbalance the alterations inrenal and adrenal mechanismsresponsible for sodium and waterretention. Nurses must proactivelyrecommend increases in dosage ofACE inhibitors based on the ACC/AHA practice guidelines10 during theacute hospitalization period so thatpatients dosing regimens are on tar-get before the patients are dischargedfrom the hospital.
Diuretics and Intravenous VasodilatorTherapy When patients are admit-ted with a wet and lukewarm/coolor cold profile without indications ofprofound hypoperfusion, a combi-nation of intravenous diuretics andvasodilator therapy leads to improvedacute outcomes, without the need forinotropic agents (Figure 2). Manystudies were conducted in the late1970s and early 1980s in patientswith New York Heart Associationfunctional class IV decompensatedheart failure to study the effectivenessof intravenous diuretic and vasodila-tor (nitroprusside and nitroglycerin)therapy in reducing filling pressures(preload) and systemic vascularresistance (afterload) and improvingcardiac output. The results indicatedthat nitroprusside was a clinicallyeffective and powerful agent forreducing afterload that also decreasedventricular systolic and diastolic vol-umes and improved ventricular dias-
ing preload (through initial venodi-latation and then through diuresisand natriuresis) and ultimately reliev-ing signs and symptoms, but theseagents should not be used alone toimprove overall morbidity and sur-vival in patients with heart failure. Inorder to address increased afterloadassociated with both exacerbation ofheart failure and intravenous loopdiuretic therapy, pharmacologicaltherapies must include agents thatreduce neuroendocrine activationand vasoconstriction because thesemechanisms can worsen the heartfailure syndrome by worsening ven-tricular remodeling.
Diuretics and ACE Inhibitor TherapyAlthough only limited data are avail-able, when an ACE inhibitor wascombined with loop diuretics, thecombination therapy reduced thepressor (vasoconstriction) responseof diuretics.32 ACE inhibitors reducedthe increase in plasma angiotensin II,thus decreasing the sympathetic acti-vation (and associated deteriorationin left ventricular pump function)that preceded the diuretic action ofdiuretics.32
ACE inhibitors ultimatelydecreased reabsorption of sodiumin the distal tubule and decreasedaldosterone stimulation in the adre-nal glands.33,34 Many randomized,controlled research studies wereconducted from the early 1980sthrough the mid-1990s that addedan ACE inhibitor to diuretic therapy
22 CRITICALCARENURSE Vol 24, No. 6, DECEMBER 2004
One of the hurdles in management of heartfailure is to overcome the myth that thegoals of managing acute decompensatedand stable heart failure are different.
by guest on June 20, 2014http://ccn.aacnjournals.org/Downloaded from
-
tolic properties. It provided rapidsymptomatic relief for patients andimproved, stabilized, and optimizedhemodynamic parameters.35-39
Intravenous nitroglycerin isknown predominantly as an agent forreducing preload. However, at highdoses, intravenous nitroglycerinreduces systemic and pulmonaryvascular resistance. In patients withdecompensated chronic heart failure,nitroglycerin was less powerful thannitroprusside in reducing afterloadbut was effective in reducing preload,increasing cardiac output, and con-trolling signs and symptoms andhemodynamic derangements.40-42
Table 7 is a summary of the doseranges, actions, and indications of
vasoactive medications used in themanagement of patients with acutedecompensated heart failure.43
As the overall goal of managingpatients with heart failure hasshifted from improving hemody-namic status to improving neuroen-docrine abnormalities in the hopethat ventricular remodeling will befavorably affected, researchers havestudied the effectiveness of intra-venous vasodilator therapy in modu-lating the neuroendocrine axis. In arecent study44 of 34 patients withdecompensated heart failure whoreceived intravenous diuretics andvasodilator therapies (nitroprussideand ACE inhibitors) to reduce pre-load and afterload, neurohormonal
activation (endothelin, norepinephrine, and BNP levels) decreasedrapidly and was associated withimproved hemodynamic status.Similar to results of studies con-ducted in previous decades, in thisstudy,44 the mean cardiac indexincreased from 1.70 before treat-ment to 2.58 after treatment. Pul-monary artery occlusive pressuredecreased from a mean of 31 to 18mm Hg, and systemic vascularresistance decreased from a mean of1780 to 1109 dynes sec cm-5 frombefore to after treatment. Thisresearch provided further evidencethat hemodynamic parameters inpatients at rest were significantlymodulated by improving preload
CRITICALCARENURSE Vol 24, No. 6, DECEMBER 2004 23
Table 7 Intravenous vasoactive medications indicated in acute decompensated heart failure43
Characteristic
Typical dose range
ActionVenodilatorArterial vasodilatorDiureticInotropic
Indication
Primary effectPreloadAfterloadDiuresisNatriuresisCardiac outputStroke volume
Comments
Nitroglycerin
10-200g/min
XX (coronary)
Myocardialischemia, elevatedPAOP,
hypertension
mild
Rapid onset
Nitroprusside
0.1-5 g/kg perminute
XX
Hypertensive crisis,elevated PAOP,acute aortic or
mitral regurgitation
, indirectly
Risk coronary stealfrom hypotension,
assess for thiocyanate poisoning
Nesiritide
Bolus 2 g/kg then0.01 g/kg per
minute
XXX
Congestion andvasoconstriction
from acute decompensated
heart failure
, indirectly
More rapid onsetthan nitroglycerin,minimal dosageadjustment, no
tachycardia
Milrinone
Bolus 50 g/kg* then0.375-0.75 g/kg per
minute
X
X
Very low cardiac output,high PAOP, pulmonary
hypertension
Long half-life, riskhypotension,
proarrhythmia
Dobutamine
2.5-15 g/kg per minute
X
Very low cardiac outputwith or without congestion or hypotension
Assess for tachyphylaxis,tachycardia, ischemia,
proarrhythmia
Abbreviations and symbols: PAOP, pulmonary artery occlusive pressure; X denotes that the drug has the specified action; denotes decrease; denotes increase. Noentry indicates action or effect does not occur.*Consider eliminating the bolus dose when systolic blood pressure is 100 mm Hg or less; just begin infusion and wait 2 hours to assess patient for desired effects (delayto peak effect if bolus omitted).
by guest on June 20, 2014http://ccn.aacnjournals.org/Downloaded from
-
and afterload, rather than by usingagents that increased contractilityand cardiac workload. In addition,decreased activation of neuroen-docrine hormones might improveshort- and long-term outcomes.
A newer vasodilator, nesiritide, isindicated for reducing dyspnea andimproving hemodynamic status inpatients with acute decompensatedheart failure. Nesiritide, a recombi-nant form of human BNP, hasactions identical to those of theendogenous BNP molecule.45 Nesiri-tide produced balanced arterial andvenous vasodilatation that resultedin rapid reduction in ventricular fill-ing pressures. This reduction wasmanifested clinically as a dose-dependent decrease in pulmonaryartery occlusive pressure, pul-monary artery pressures, and sys-temic blood pressure.46 Nesiritidecaused diuresis and natriuresis bysuppressing the renin-angiotensin-aldosterone system.47
When intravenous nesiritidewas compared with intravenousnitroglycerin during the first 72 hoursof signs and symptoms in patientshospitalized with acute heart failure,47
the results favored nesiritide. Nesiri-tide produced a significantly quickerand greater reduction in pulmonaryartery occlusive pressure than didnitroglycerin. Patients reported andcaregivers measured a greater reduc-tion in dyspnea when the patientsreceived nesiritide rather than nitro-glycerin. The combined actions ofvasodilatation, diuresis, and natri-uresis led to preload and afterloadreduction to achieve the goal ofenhanced cardiac output and reducedpulmonary and systemic congestion.The investigators47 concluded thatnesiritide should be the drug of choice
guidelines)10 may actually improvesigns and symptoms and quality oflife by antagonizing mechanismsthat cause excessive sodium andwater retention.
Myth 3: Low Systolic BloodPressure Requires Treatment With Intravenous Inotropic Agents
Some myths are associated withinterventions when patients withheart failure have low systolic bloodpressure. One belief is that a systolicblood pressure of less than 90 mmHg requires intravenous infusion ofinotropic agents. Unless the hypoten-sion is severe (systolic blood pressure
-
of cardiac remodeling and improveclinical outcomes. Nurses must edu-cate patients about the benefits ofmaintaining a low systolic bloodpressure and adhering to core phar-macological therapies that decreaseneuroendocrine activation anddecrease blood pressure.
Additionally, use of intravenousinotropic agents is not supported inpatients in an acute setting exceptas temporary treatment of diuretic-refractory complex decompensation.48
Intravenous inotropic therapies(continuous or intermittent infusionof milrinone or dobutamine) havebeen associated with increased mor-tality when used in patients requiringinotropic support, even though theseagents improve hemodynamic sta-tus10 (Table 7). In an effort to learn ifa short-term infusion (48 hours)might lead to short- or intermediate-term improvements in patients hos-pitalized for exacerbation of heartfailure who had a wet and cool tocold profile but in whom intravenousinotropic support was not essential,the study called Outcomes of aProspective Trial of Intravenous Mil-rinone for Exacerbations of ChronicHeart Failure (OPTIME-HF) wasconducted.49 Investigators random-ized patients to receive short-termintravenous milrinone or placebo.The 2 groups did not differ signifi-cantly in hospital and 60-day posthos-pitalization mortality or in the mediannumber of days patients were hospi-talized for cardiovascular causes inthe first 60 days after discharge. Inaddition, sustained hypotension ornew atrial arrhythmias were signifi-cantly more likely to develop in thepatients receiving milrinone than inthe patients receiving placebo. Theresults of this research, that receiving
an inotropic agent without clear evi-dence of significant hemodynamiccompromise does not enhance clini-cal or economic outcomes, led to atempering of the use of intravenousinotropic agents unless absolutelywarranted.
Further, concomitant use of -blocker (-antagonist) and intra-venous dobutamine (-agonist)therapies is controversial. The phar-macological response of dobutamineis inhibited in patients receiving highdoses of -blockers because bothdrugs compete for the same -adren-ergic receptors.48 This conflict isespecially apparent with carvedilolbecause it blocks both 1 and 2receptors.48,50
Myth 4: ACE Inhibitors and -Blocker Therapies Should BeTemporarily Decreased or Dis-continued During Decompensation
Another belief is that ACE inhibit-ors and -blocker therapies must bedecreased or discontinued or shouldnot be initiated when the patientsblood pressure is low. These agentshelp suppress maladaptive neu-roendocrine responses that lead toincreased wall stress, ventricularhypertrophy, and worsening cardiacremodeling and cardiac output.51
Unless symptomatic low blood pres-sure occurs or intravenous vasodila-tor agents are used, core oraltherapies used to manage patientswith chronic heart failure should bemaintained whenever possible.Blood pressure may not decrease orthe reduction may be self-limitingwhen vasodilator (ACE inhibitor orangiotensin-receptor blocker) and -blocker therapies are initiated andmaintained in patients with a lowbaseline blood pressure (85-90 mm
Hg). If blood pressure decreases butindications of hypoperfusion areabsent, nurses should assess patientsfor hypovolemia (from overdiuresis).In addition, nurses must communi-cate expected effects of core agentsfor treating heart failure to patientsso that patients are prepared forpotential dizziness or other symp-toms associated with drug actionsand interactions and understand theself-limiting nature of these changes.52
Myth 5: Once Core Therapies Are Unsuccessful, They ShouldNot Be Tried Again
Some may believe that once ACEinhibitor or -blocker therapy isunsuccessful in a patient because oflow blood pressure, these therapiesshould not be tried again. Assessmentand correction of mechanisms thatcause low blood pressure (such asinitiating ACE inhibition when theserum level of sodium is less than130 mmol/L) may make the precedingstatement a false claim. Core pharma-cological therapies known to improvehealth-related outcomes can be suc-cessfully implemented withoutepisodes of low blood pressure in mostpatients, as evidenced by low dropoutrates in randomized controlled stud-ies. The acute care episode is a perfectsetting for trying ACE inhibitors or-blockers again, when appropriate,because patients can be carefullymonitored and resources are readilyavailable. Low-dose, shorter-actingagents in each drug class (such ascaptopril and carvedilol) are the drugsof choice in patients with a history oflow blood pressure.
Nursing ConsiderationsIn addition to assessment of
patients, nursing actions that are cen-
26 CRITICALCARENURSE Vol 24, No. 6, DECEMBER 2004 by guest on June 20, 2014http://ccn.aacnjournals.org/Downloaded from
-
tral to patients outcomes are admin-istration of medications, evaluationof treatment effectiveness, and edu-cation and ongoing communicationwith patients, patients families, andthe healthcare team. If a patientsdyspnea improves but weight loss,urination, intake and output, orproportional pulse pressure do notimprove, nurses must be assertive inproviding timely communication ofthese findings to peers and the physi-cian team because delays can diminishhigh-quality care, hinder achievementof clinical goals, and harm the hospi-tal financially. Table 8 outlines nurs-ing actions and goals that reflectcritical thinking and foster commu-nication when managing patientswith heart failure.
Nurses often take an active rolein prompting initiation and adjust-ment of medication therapies. Nursesmust know the actions, dosing, andeffects of heart failure medicationsand must promote decisions that willaffect the overall goal of managementof heart failure (reversal of cardiacremodeling). This goal can beachieved during the acute hospital-ization by adding, maintaining, andincreasing dosages of vasodilators(ACE inhibitors) and maintaining-blocker therapy per consensusrecommendations. Nurses must notfocus on pharmacological therapiesthat simply improve symptoms (eg,diuretics), because these therapiesalso increase cardiac workload, acti-vate adverse neuroendocrine systems,and increase mortality. When indoubt about therapeutic priorities,it is always helpful to reassess thepatients clinical status. When patientshave congestion and inadequate organor peripheral perfusion (cool/luke-warm to touch), intravenous diuretic
blood pressure unless the patient hasorthostatic hypotension or othersigns and symptoms reflectinghypoperfusion or hypovolemia.Nurses must use multiple clinicalparameters, not just blood pressurevalues, to determine that withhold-ing drugs will benefit a patients clin-ical status.
Critical evaluation of eachpatients progress involves ongoingassessment of electrolyte and fluid
and vasodilator therapy (along withmaintenance of prehospital -blockertherapy) may decrease afterload andpreload to improve perfusion andcardiac index. When profoundhypoperfusion compromises organfunction, an intravenous inotropicagent may be the preferred agent ofchoice (Figure 2). It is especiallyimportant for nurses not to withholddoses of vasodilators, -blockers, ordiuretics because of a patients low
CRITICALCARENURSE Vol 24, No. 6, DECEMBER 2004 27
Table 8 Nursing considerations: critical thinking and communication
Nursing role
Critically evaluateeffectiveness ofinterventions
Communicate topatient, patientsfamily and teammembers
Actions/goals
Monitor vital signs; maintain systolic blood pressure >80 mm Hgand 1.8 mg/dL)Sodium >138 and
-
status. Such assessment is especiallyimportant in managing patientswith heart failure because activationof neuroendocrine systems, renaldysfunction, and current drug thera-pies may disrupt the fine balance ofelectrolytes and cause shifts insodium, potassium, calcium, andmagnesium.53 It is important fornurses to develop and use advancedmeasurement and cardiac ausculta-tion skills to monitor fluid status(eg, assessment of jugular venouspressure and the presence or wors-ening of systolic murmurs and S3 orS4 heart sounds) because patientsmay still have intravascular volumeoverload after obvious interstitialfluid retention (crackles, edema) dissi-pates. Freedom from congestion inthe early weeks after hospital dis-charge was an independent predictorof survival in patients hospitalizedwith New York Heart Associationfunctional class IV symptoms.54 Inorder to prevent readmission andmaintain clinical stability, patientswho have evidence of clinical andsubclinical congestion before dis-charge should be considered foraggressive follow-up (cardiologistspecializing in heart failure) andinterventions aimed at promotingeuvolemia (eg, increased restrictionin sodium diet or fluid intake, diureticself-management program, heartfailure nurse clinic).
Serum BNP values provideanother mechanism for monitoringfluid status in the early hours after
hospitalization and for assessingpatients outcomes. In patients withsymptomatic, functional class III orIV heart failure who were undergo-ing tailored therapy for their con-gested state, hourly changes in BNPlevels were significantly correlatedwith hourly changes in pulmonaryartery occlusive pressure.55 WhenBNP levels at initial hospital assess-ment and within 24 hours of dischargeor death were compared as an out-come variable,24 successfully treatedpatients (as compared with patientswho died during the index hospital-ization or were readmitted within 30days of discharge) had a meandecrease in BNP level of 216 pg/mL.Patients who were readmitted or diedhad levels that increased during thecourse of hospitalization.
Last, communication betweenhealthcare providers and patientsand patients families about thepatients clinical status and manage-ment plan is essential. Proactivelyassessing the knowledge base ofpatients and their families to promoteunderstanding of the current plan ofcare and asking if there are questionscan aid communication and infor-mation sharing. Information sharingand ongoing communication withpatients and their families enhancesperceived control, potentially decreas-ing stress.56 This communication isespecially important because loss offunctional mobility and role changesthat occur with the progression ofheart failure lead to a perceived loss
of control57 that can ultimately affectcoping, lifestyle modifications, andbehaviors. Examples of importantfactors to address in patients educa-tion are found in the first item inTable 3 and in Table 4. It is well rec-ognized that improving patientsknowledge of heart failure and pro-viding support, encouragement, andpositive reinforcement of self-carebehaviors improves outcomes inpatients with heart failure.58
References1. American Heart Association. 2003 Heart
and Stroke Statistical Update. Dallas, Tex:American Heart Association; 2002.
2. Scios Inc. ADHERE Acute DecompensatedHeart Failure National Registry: 2nd Quarter2002 Benchmark Report. San Diego, Calif:Scios Inc; 2002.
3. Graves EJ. National Hospital Discharge Sur-vey: annual summary, 1993. Vital HealthStat 13. August 1995:1-63.
4. Dauterman KW, Go AS, Rowell R, Gebret-sadik T, Gettner S, Massie BM. Congestiveheart failure with preserved systolic func-tion in a statewide sample of communityhospitals. J Card Fail. 2001;7:221-228.
5. Redfield MM, Jacobsen SJ, Burnett JC Jr,Mahoney DW, Bailey KR, Rodeheffer RJ.Burden of systolic and diastolic ventriculardysfunction in the community: appreciatingthe scope of the heart failure epidemic.JAMA. 2003;289:194-202.
6. Bennett SJ, Huster GA, Baker SL, et al.Characterization of the precipitants of hos-pitalization for heart failure decompensa-tion. Am J Crit Care. 1998;7:168-174.
7. Joshi PP, Mohanan CJ, Sengupta SP, SalkarRG. Factors precipitating congestive heartfailure: role of patient non-compliance. JAssoc Physicians India. 1999;47:294-295.
8. Tsuyuki, RT, McCelvie RS, Arnold MO, etal. Acute precipitants of congestive heartfailure exacerbations. Arch Intern Med.2001;161:2337-2342.
9. Joint Commission on Accreditation ofHealthcare Organizations. SpecificationManual for National Implementation ofHospital Core Measures Version 2.0: implementation to begin with July 2004 discharges (last updated 4/26/04). Avail-able at: http://www.jcaho.org/pms/core+measures/information+on+final+specifications.htm. Accessed September 21,2004.
10. Hunt SA, Baker DW, Chin MH, et al.ACC/AHA guidelines for the evaluation andmanagement of chronic heart failure in theadult: executive summary. A report of theAmerican College of Cardiology/AmericanHeart Association Task Force on PracticeGuidelines (Committee to revise the 1995Guidelines for the Evaluation and Manage-ment of Heart Failure). J Am Coll Cardiol.2001;38:2101-2113.
11. Jessup M, Brozena S. Heart failure. N Engl JMed. 2003;348:2007-2018.
28 CRITICALCARENURSE Vol 24, No. 6, DECEMBER 2004
Nurses must use multiple clinical parameters,not just blood pressure values, to determinethat withholding drugs will benefit apatients clinical status.
by guest on June 20, 2014http://ccn.aacnjournals.org/Downloaded from
-
12. Cohn JN, Ferrari R, Sharpe N. Cardiacremodeling: concepts and clinical implica-tionsa consensus paper from an interna-tional forum on cardiac remodeling. J AmColl Cardiol. 2000;35:569-582.
13. Kurrelmeyer K, Kalra D, Bozkurt B, et al.Cardiac remodeling as a consequence andcause of progressive heart failure. Clin Car-diol. 1998;21(12 suppl I):I14-I19.
14. Sutton MG, Sharpe N. Left ventricularremodeling after myocardial infarction:pathophysiology and therapy. Circulation.2000;101:2981-2988.
15. Stevenson LW. Tailored therapy to hemody-namic goals for advanced heart failure. Eur JHeart Fail. 1999;1:251-257.
16. Stevenson LW, Perloff JK. The limited relia-bility of physical signs for estimating hemo-dynamics in chronic heart failure. JAMA.1989;261:884-888.
17. Shah MR, Hasselblad V, Stinnett SS, et al.Hemodynamic profiles of advanced heartfailure: association with clinical characteris-tics and long-term outcomes. J Card Fail.2001;7:105-113.
18. Baughman, KL. B-type natriuretic peptide: a window to the heart. N Engl J Med.2002;347:158-159.
19. Dao Q, Krishnaswamy P, Kazanegra R, et al.Utility of B-type natriuretic peptide in thediagnosis of congestive heart failure in anurgent-care setting. J Am Coll Cardiol.2001;37:379-385.
20. Krishnaswamy P, Lubien E, Clopton P, et al.Utility of B-type natriuretic peptide levels inidentifying patients with left ventricular sys-tolic or diastolic dysfunction. Am J Med.2001;111:274-279.
21. Maisel AS, Krishnaswamy P, Nowak RN, etal. Rapid measurement of B-type natriureticpeptide in the emergency diagnosis of heartfailure. N Engl J Med. 2002;347:161-167.
22. McCullough PA, Nowak RM, McCord J, etal. B-type natriuretic peptide and clinicaljudgment in emergency diagnosis of heartfailure. Circulation. 2002;106:416-422.
23. Wieczorek SJ, Wu, AH, Christensen R, et al.A rapid B-type natriuretic peptide assayaccurately diagnoses left ventricular dys-function and heart failure: a multicenterevaluation. Am Heart J. 2002;144:834-839.
24. Cheng V, Kazanagra R, Garcia A, et al. Arapid bedside test for B-type peptide pre-dicts treatment outcomes in patients admit-ted for decompensated heart failure: a pilotstudy. J Am Coll Cardiol. 2001;37:386-391.
25. Slike B. Diuretic induced changes in symp-toms and quality of life. Br Heart J.1994;72(suppl):S57-S62.
26. Cooper HA, Dries DL, Davis CE, Shen YL,Domanski, MJ. Diuretics and risk ofarrhythmic death with left ventricular dys-function. Circulation. 1999;100:1311-1315.
27. Satorstein L. Electrophysiological impact ofdiuretics in heart failure. Br Heart J. 1994;72(suppl):S54-S56.
28. Anand IS, Florea VG. Diuretics in chronicheart failure: benefits and hazards. EurHeart J. 2001;3(suppl G):G8-G18.
29. Weinfeld MS, Chertow GM, Stevenson LW.Aggravated renal dysfunction during inten-sive therapy for advanced heart failure. AmHeart J. 1999;138:285-290.
30. Kelly DT. Vascular effects of diuretics inheart failure. Br Heart J. 1994;72(suppl):S48-S50.
31. Raftery EB. Haemodynamic effects of
48. Bristow MR, Shakar SF, Linseman JV, LowesBD. Inotropes and -blockers: is there aneed for new guidelines? J Card Fail. 2001;7(2suppl 1):8-12.
49. Cuffe MS, Califf RM, Adams Jr KF, et al.Short-term intravenous milrinone for acuteexacerbation of chronic heart failure. JAMA.2002;287:1541-1547.
50. Felker GM, OConnor CM. Inotropic ther-apy for heart failure: an evidence-basedapproach. Am Heart J. 2001;142:393-401.
51. Albert N. Heart failure: the pathophysio-logic basis for current therapeutic concepts.Crit Care Nurse. June 1999;18(suppl):2-13.
52. Albert NM. Advanced systolic heart failure:emerging pathophysiology and currentmanagement. Prog Cardiovasc Nurs. Sum-mer 1998;13:14-30.
53. Gawlinski A, McCloy K, Caswell D,Quinones-Baldrich WJ. Cardiovascular dis-orders. In: Gawlinski A, Hamwi D, ed. AcuteCare Nurse Practitioner: Clinical Curriculumand Certification Review. Philadelphia, Pa:WB Saunders Co; 1999:136-294.
54. Lucas C, Johnson W, Hamilton MA, et al.Freedom from congestion predicts good sur-vival despite previous class IV symptoms ofheart failure. Am Heart J. 2000;140:840-847.
55. Kazanegra R, Cheng V, Garcia A, et al. Arapid test for B-type natriuretic peptide corre-lates with falling wedge pressures in patientstreated for decompensated heart failure: apilot study. J Card Fail. 2001;7:21-29.
56. Miller JF. Coping With Chronic Illness: Over-coming Powerlessness. 2nd ed. Philadelphia,Pa: FA Davis Co; 1992.
57. Johnson JL, Morse JM. Regaining control:the process of adjustment after myocardialinfarction. Heart Lung. 1990;19:126-135.
58. Miranda MB, Gorski LA, LeFevre JG, LevacKA, Niederstadt JA, Toy AL. An evidence-based approach to improving care ofpatients with heart failure across the contin-uum. J Nurs Care Qual. 2002;17:1-14.
diuretics in heart failure. Br Heart J. 1994;72(suppl):S44-S47.
32. van Zwieten PA. Neuroendocrine effects ofdiuretics in heart failure. Br Heart J. 1994;72(suppl):S51-S53.
33. Hampton JR. Results of clinical trials withdiuretics in heart failure. Br Heart J. 1994;72(suppl):S68-S72.
34. Hess B. Chronic heart failure: pathophysiol-ogy and therapeutic approacheswhy isthe kidney so important? Eur Heart J. 2001;3(suppl G):G3-G7.
35. Guiha NH, Cohn JN, Mikulik E, FranciosaJA, Limas CJ. Treatment of refractory heartfailure with infusion of nitroprusside. NEngl J Med. 1974;291:587-592.
36. Leier CV, Magorien RD, Boudoulas H, LewisRP, Bambach D, Unverferth DV. The effectof vasodilator therapy on systolic and dias-tolic time intervals in congestive heart fail-ure. Chest. 1982;81:723-729.
37. Franciosa JA, Silverstein SR. Hemodynamiceffects of nitroprusside and furosemide inleft ventricular failure. Clin Pharmacol Ther.1982;32:62-69.
38. Pepine CJ, Nichols WW, Curry RC Jr, ContiCR. Aortic input impedance during nitroprus-side infusion. J Clin Invest. 1979;64:643-654.
39. Brodie BR, Grossman W, Mann T, McLau-rin LP. Effects of sodium nitroprusside onleft ventricular diastolic pressure-volumerelations. J Clin Invest. 1977;59:59-68.
40. Leier CV, Bambach D, Thompson MJ, Catte-neo SM, Goldberg RJ, Unverferth DV. Cen-tral and regional hemodynamics effects ofintravenous isosorbide dinitrate, nitroglyc-erin, and nitroprusside in patients with con-gestive heart failure. Am J Cardiol. 1981;48:1115-1123.
41. Armstrong PW, Armstrong JA, Marks GS.Pharmacokinetic-hemodynamic studies ofintravenous nitroglycerin in congestiveheart failure. Circulation. 1980;62:160-166.
42. Chatterjee K, Drew J, Parmley WW, Klaus-ner SC, Polansky J, Zacherle B. Combina-tion vasodilator therapy for severe chroniccongestive heart failure. Ann Intern Med.1976;85:467-470.
43. Greenberg BH, Hermann DD. ContemporaryDiagnosis and Management of Heart Failure.Newtown, Pa: Handbooks in Health CareCo; 2002:214-217.
44. Johnson W, Omland T, Hall C, et al. Neuro-hormonal activation rapidly decreases afterintravenous therapy with diuretics andvasodilators for class IV heart failure. J AmColl Cardiol. 2002;39:1623-1629.
45. Hobbs RE, Mills RM. Therapeutic potentialof nesiritide (recombinant B-type natri-uretic peptide) in the treatment of heart fail-ure. Expert Opin Investig Drugs. 1999;8:1063-1072.
46. Marcus LS, Hart D, Packer M, et al. Hemo-dynamic and renal excretory effects ofhuman brain natriuretic peptide infusion inpatients with congestive heart failure: adouble-blind, placebo-controlled, random-ized crossover trial. Circulation. 1996;94:3184-3189.
47. Publication Committee for the VMACInvestigators (Vasodilatation in the Man-agement of Acute CHF). Intravenous nesiri-tide vs nitroglycerin for treatment ofdecompensated congestive heart failure: arandomized controlled trial [published cor-rection appears in JAMA. 2002;288:577].JAMA. 2002;287:1531-1540.
CRITICALCARENURSE Vol 24, No. 6, DECEMBER 2004 29 by guest on June 20, 2014http://ccn.aacnjournals.org/Downloaded from
-
30 CRITICALCARENURSE Vol 24, No. 6, DECEMBER 2004
CE Test Form
Evidence-Based Practice forAcute Decompensated Heart Failure
Objectives:
1. Identify the core drug therapies for decompensated heart failure
2. Describe the role of B-type natriuretic peptide in decompensated heart failure
3. Explain the pharmacological management of decompensated heart failure
Mark your answers clearly in the appropriate box. There is only 1 correct answer. You may photocopy this form.
To receive CE credit for this test (ID C046), mark your answers on the form below, complete the enroll-ment information, and submit it with the $12 processing fee (payable in US funds) to the American Asso-ciation of Critical-Care Nurses (AACN). Answer forms must be postmarked by December 1, 2006. Within 3to 4 weeks of AACN receiving your test form, you will receive an AACN CE certificate.
This continuing education program is provided by AACN, which is accredited as a provider of continuing education in nursing by theAmerican Nurses Credentialing Centers Commission on Accreditation. AACN has been approved as a provider of continuing educa-tion by the State Boards of Nursing of Alabama (#ABNP0062), California (01036), Florida (#FBN2464), Iowa (#332), Louisiana(#ABN12), and Nevada. AACN programming meets the standards for most other states requiring mandatory continuing educationcredit for relicensure.
Program evaluationAgree Neutral Disagree
Objective 1 was met Objective 2 was met Objective 3 was met The content was appropriate My expectations were met This method of CE is effective
for this content
The level of difficulty of this test was: easy medium difficultTo complete this program, it took me
hours / minutes.
Mail this entire page to AACN, 101 Columbia, Aliso Viejo, CA 92656, (800) 899-2226
Test ID: C046Test writer: John P. Harper, RN, MSN, BC
Form expires: December 1, 2006Contact hours: 2.0
Passing score: 9 correct (75%)Category: A
Test fee: $12
Name
Address
City State ZIP
Phone ( )
E-mail address
RN license number (required)
State of licensure
AACN member number
I would like to receive my certificate via e-mail (check box)
CE Test Instructions
1. a 2. a 3. a 4. a 5. a 6. a 7. a 8. a 9. a 10. a 11. a 12. a 13. a 14. a b b b b b b b b b b b b b b c c c c c c c c c c c c c c d d d d d d d d d d d d d d
CEContinuing Education
by guest on June 20, 2014http://ccn.aacnjournals.org/Downloaded from
-
CRITICALCARENURSE Vol 24, No. 6, DECEMBER 2004 31
7. Which of the following is not a direct effect ofnesiritide?a. Decreased preloadb. Decreased afterloadc. Increased diuresisd. Increased contractility
8. What is the typical dosage range of nesiritide in thetreatment of acute decompensated HF?a. 0.001 ug/kg/minb. 0.01 ug/kg/minc. 0.1 ug/kg/mind. 1 ug/kg/min
9. Which of the following drugs inhibits renin releaseand indirectly decreases proximal reabsorption ofsodium?a. Diureticsb. -Blockersc. ACE inhibitorsd. Digitalis
10. Which one of the following medications has beenassociated with increased mortality when used inpatients requiring inotropic support?a. Dobutamineb. Dopaminec. Digoxind. Levophed
11. Which of the following goals indicates effective HFmanagement?a. Resting heart rate 4 L/min/m2
c. Pulmonary artery occlusive pressure
-
by guest on June 20, 2014http://ccn.aacnjournals.org/Downloaded from