Criminal recidivism in three models of mandatory drug treatment
11
Regular article Criminal recidivism in three models of mandatory drug treatment Douglas Young, (M.S.) a, *, Reginald Fluellen, (Ph.D.) b , Steven Belenko, (Ph.D.) c a Bureau of Governmental Research, University of Maryland, College Park, 4511 Knox Rd, Suite 301, College Park, MD 20740, USA b National Black Leadership Commission on AIDS, 105 East 22nd Street, Suite 711, New York, NY 10010, USA c Treatment Research Institute at the University of Pennsylvania, 600 Public Ledger Building, 150 South Independence Mall West, Philadelphia, PA 19106-3475, USA Received 17 November 2003; received in revised form 26 May 2004; accepted 20 August 2005 Abstract Although research has generally been supportive of compulsory treatment programs for drug abusers, findings remain mixed, and few studies have assessed the impacts of different coercive program elements. This study compared criminal recidivism outcomes of 350 clients mandated to the same long-term residential treatment facilities from three different legal sources. On several measures of recidivism, including long-term re-arrest rates that controlled for time at risk, clients mandated from two highly structured programs were found to recidivate at less than half the rate of comparison group clients. This group effect was upheld in multivariate models that controlled for pre-treatment differences and other factors related to recidivism. Combined with results of a previous retention study involving these clients, the findings provide support for the use of structured protocols for informing clients in mandatory programs about legal contingencies of participation and enforcing contingencies through frequent contact between legal agents and treatment staff. D 2004 Elsevier Inc. All rights reserved. Keywords: Mandatory treatment; Recidivism; Coercion; Courts 1. Introduction Severe budgetary constrictions caused by recent eco- nomic trends have left state and local policy makers searching for strategies to cut and contain costs. The sud- den budget-mandated release of 567 prisoners in Kentucky in December 2002 dramatically signified a growing con- sensus that sole reliance on incarceration, particularly for nonviolent crimes, is prohibitively expensive public policy. These budgetary trends will likely give new impetus to in- terest in cheaper, community-based treatment alternatives for the vast numbers of substance-abusing offenders in- volved in the criminal justice system (Arrestee Drug Abuse Monitoring Program [ADAM], 2000; Bureau of Justice Statistics, 2001; Maguire & Pastore, 1999). A number of existing models and programs aim to provide this function at different points in the criminal justice system. In opera- tion since the 1970s, Treatment Alternatives to Street Crime (TASC) programs have the most extensive history in this role (Anglin, Longshore, & Turner, 1999). TASC programs operate as a bridge between the justice and treatment systems, providing case management and brokering serv- ices. TASC may work at the bfront endQ of the system with offenders under court or probation supervision, or with parolees upon release from prison. Local TASC programs may also operate within the larger context of two other justice-based treatment models spawned largely by federal funding, Breaking the Cycle (BTC), and drug treatment courts. BTC programs target all substance-abusing offenders entering a particular legal jurisdiction, emphasizing assess- ment, treatment matching, drug testing, and graduated sanctions for non-compliance with supervision orders (Harrell, Hirst, & Mitchell, 2000). Drug courts, which now number over 1,000 nationally, typically target first- or second-time offenders charged with relatively minor crimes who have drug problems. Facilitated by court-based case 0740-5472/04/$ – see front matter D 2004 Elsevier Inc. All rights reserved. doi:10.1016/j.jsat.2004.08.007 * Corresponding author. Tel.: +1 301 403 8334; fax: +1 301 403 4404. E-mail address: [email protected] (D. Young). Journal of Substance Abuse Treatment 27 (2004) 313 – 323
-
Upload
douglas-young -
Category
Documents
-
view
213 -
download
1
Transcript of Criminal recidivism in three models of mandatory drug treatment

Journal of Substance Abuse Tre
Regular article
Criminal recidivism in three models of mandatory drug treatment
Douglas Young, (M.S.)a,*, Reginald Fluellen, (Ph.D.)b, Steven Belenko, (Ph.D.)c
aBureau of Governmental Research, University of Maryland, College Park, 4511 Knox Rd, Suite 301, College Park, MD 20740, USAbNational Black Leadership Commission on AIDS, 105 East 22nd Street, Suite 711, New York, NY 10010, USA
cTreatment Research Institute at the University of Pennsylvania, 600 Public Ledger Building, 150 South Independence Mall West,
Philadelphia, PA 19106-3475, USA
Received 17 November 2003; received in revised form 26 May 2004; accepted 20 August 2005
Abstract
Although research has generally been supportive of compulsory treatment programs for drug abusers, findings remain mixed, and
few studies have assessed the impacts of different coercive program elements. This study compared criminal recidivism outcomes of
350 clients mandated to the same long-term residential treatment facilities from three different legal sources. On several measures of
recidivism, including long-term re-arrest rates that controlled for time at risk, clients mandated from two highly structured programs were
found to recidivate at less than half the rate of comparison group clients. This group effect was upheld in multivariate models that
controlled for pre-treatment differences and other factors related to recidivism. Combined with results of a previous retention study
involving these clients, the findings provide support for the use of structured protocols for informing clients in mandatory programs about
legal contingencies of participation and enforcing contingencies through frequent contact between legal agents and treatment staff. D 2004
Elsevier Inc. All rights reserved.
Keywords: Mandatory treatment; Recidivism; Coercion; Courts
1. Introduction
Severe budgetary constrictions caused by recent eco-
nomic trends have left state and local policy makers
searching for strategies to cut and contain costs. The sud-
den budget-mandated release of 567 prisoners in Kentucky
in December 2002 dramatically signified a growing con-
sensus that sole reliance on incarceration, particularly for
nonviolent crimes, is prohibitively expensive public policy.
These budgetary trends will likely give new impetus to in-
terest in cheaper, community-based treatment alternatives
for the vast numbers of substance-abusing offenders in-
volved in the criminal justice system (Arrestee Drug Abuse
Monitoring Program [ADAM], 2000; Bureau of Justice
Statistics, 2001; Maguire & Pastore, 1999). A number of
existing models and programs aim to provide this function
0740-5472/04/$ – see front matter D 2004 Elsevier Inc. All rights reserved.
doi:10.1016/j.jsat.2004.08.007
* Corresponding author. Tel.: +1 301 403 8334; fax: +1 301 403 4404.
E-mail address: [email protected] (D. Young).
at different points in the criminal justice system. In opera-
tion since the 1970s, Treatment Alternatives to Street Crime
(TASC) programs have the most extensive history in this
role (Anglin, Longshore, & Turner, 1999). TASC programs
operate as a bridge between the justice and treatment
systems, providing case management and brokering serv-
ices. TASC may work at the bfront endQ of the system with
offenders under court or probation supervision, or with
parolees upon release from prison. Local TASC programs
may also operate within the larger context of two other
justice-based treatment models spawned largely by federal
funding, Breaking the Cycle (BTC), and drug treatment
courts. BTC programs target all substance-abusing offenders
entering a particular legal jurisdiction, emphasizing assess-
ment, treatment matching, drug testing, and graduated
sanctions for non-compliance with supervision orders
(Harrell, Hirst, & Mitchell, 2000). Drug courts, which
now number over 1,000 nationally, typically target first- or
second-time offenders charged with relatively minor crimes
who have drug problems. Facilitated by court-based case
atment 27 (2004) 313–323

D. Young et al. / Journal of Substance Abuse Treatment 27 (2004) 313–323314
management and carefully calibrated sanctions and incen-
tives, drug court participants must complete a regimen of
community-based treatment before charges are dropped or
reduced (Belenko, 1998).
Although questions have been raised about whether these
programs represent true alternatives to incarceration—drug
courts in particular may target offenders who would not be
going to jail or prison (Belenko, 2000)—they remain attrac-
tive to policy makers for other reasons. They provide an
efficient means of ensuring access to treatment for many
high-risk, high-need individuals who would not otherwise
enter treatment (Hammett, Gaiter, & Crawford, 1998;
Wenzel, Longshore, Turner, & Ridgely, 2001). Further, there
is a widespread, research-based consensus that programs that
use the coercive powers of the justice system retain clients
for the same or longer periods than clients who are not
legally mandated, leading in turn to improved employment
and criminal recidivism outcomes (Anglin, 1988; Brecht,
Anglin & Wang, 1993; Collins & Allison, 1983; Hiller,
Knight, Broome, & Simpson, 1998; Marlowe, 2001). While
not directly disputed, this conclusion has been faulted in
recent years as oversimplified, with reviewers pointing to
the imprecise terminology, poor methodology, and uneven
findings in much of the earlier research on coerced treatment
(Farabee, Prendergast, & Anglin, 1998; Marlowe, Merikle,
Kirby, Festinger, & McLellan, 2001; Wild, 1999; Young,
2002). Some of the same criticism is echoed in reviews of
the many drug court evaluations that have been spawned
by federal requirements for program funding (Gottfredson,
Najaka, & Kearley, 2003; Listwan, Sundt, Holsinger, &
Latessa, 2003). In practice, the structural and operational
characteristics of compulsory treatment models vary greatly
from one program to another (Anglin et al., 1999; Taxman &
Bouffard, 2002; Young & Belenko, 2002). Client targeting
and screening, treatment dosage and approach, case manage-
ment, monitoring, and sanctioning practices are just some
of the elements that differ among programs and are likely to
affect outcomes.
Policy makers looking for effective treatment alternatives
to incarceration need better information about the impacts of
different program mechanisms and models. The research re-
ported here is part of a small trend of recent studies that have
sought to assess the effects of specific coercive practices
and policies. It specifically builds on prior research assessing
mandated clientsT perceptions of legal pressure (PLP) in threedifferent compulsory treatment programs and the impacts of
PLP and other client factors on retention in residential treat-
ment (Young, 2002; Young & Belenko, 2002). The present
study extends the comparative analysis of the three programs
from retention outcomes to the bbottom lineQ gauge used by
policymakers—criminal recidivism.
1.1. Review of the literature
Research on compulsory treatment has evolved sub-
stantially from early studies that simply compared outcomes
of legally-involved clients and those entering treatment
voluntarily (Salmon & Salmon, 1983; Pompi & Resnick,
1987; Steer, 1983). This initial research often blurred
important distinctions—legal status, referral source, and
treatment mandate—and ignored the fact that bvoluntaryQclients are rarely self-referred, but enter treatment under other
pressures from family, peers, and employers (Marlowe et al.,
2001). Building on an ordinal index created by Anglin and
colleagues (Anglin, Brecht, & Maddahian, 1989; Brecht
et al., 1993), subsequent studies have assessed outcomes of
clients under low, medium, and high coercion, as determined
by legal status, monitoring through drug testing, and the
client reporting a legal reason for entering treatment (Hiller
et al., 1998; Hser, Maglione, Polinsky, & Anglin, 1998).
Exemplifying recent trends that extend the field, a study
by Knight , Hiller, Broome, and Simpson (2000) employs
this continuous index of legal coercion within a larger con-
text that includes assessments of engagement and motiva-
tion for treatment.
Even more detailed studies of the bblack boxQ of coer-cive program practices are evident in recent research on
drug courts, TASC programs, and other treatment diver-
sion models. These studies represent empirical tests of
themes found in theoretical and review papers supporting
the use of client contracts, swift and timely responses to
violations, and structured sanction menus (Marlowe et al.,
1996; Taxman, Soule, & Gelb, 1999; Taxman, 2000), and
the application of principles of behavioral psychology
(Marlowe & Kirby, 1999) and contingency management
(Higgins & Petry, 1999). A controlled study of a pretrial
diversion program in Washington, DC, found that grad-
uated sanctions, with or without ancillary drug treatment,
had favorable impacts on offendersT drug use (Harrell &
Cavanaugh, 1995; Harrell, 1998). The case management
model utilized by TASC—assessment, close monitoring of
treatment progress, drug testing, and reporting compliance
to legal agents—has generally been supported in evalua-
tions (Rhodes & Gross, 1997; Van Stelle, Mauser, &
Moberg, 1994), however implementation fidelity can vary
greatly across sites, moderating impacts (Anglin et al.,
1999). Applied in a broader scope in the federal Breaking
the Cycle initiatives, these same practices have received
support in an evaluation of BTC demonstrations (Harrell
et al., 2000).
Recent studies have similarly begun to test some of
the assumptions about effective coercive practices inher-
ent in the many prescriptive documents on drug courts
(e.g., NADCP, 1997). In a rare controlled evaluation of a
drug court serving offenders with serious drug histories,
Gottfredson and colleagues (2003) found that drug court
participants had lower rearrest rates than the control group
at the 2-year follow up. Results suggested this effect was
at least partially due to the courtTs success in imposing a
threat of future sanctions, which worked regardless of the
participantsT drug history (contrary to hypotheses that sanc-
tion threats would be ineffective with heavy users). The

D. Young et al. / Journal of Substance Abuse Treatment 27 (2004) 313–323 315
study findings also underscored the importance of treatment
in achieving recidivism reduction effects.
In a less rigorous design, researchers found reduced
recidivism outcomes for participants of the Douglas County
Drug Court (Omaha, NE) relative to non-equivalent com-
parison groups, and attributed at least some of this success
to the intensive judicial supervision and monitoring em-
ployed by court staff (Spohn, Piper, Martin, & Frenzel,
2001). Marlowe and colleagues (2003) have assessed the
impacts of bthe single-most defining component of a drug
court, namely, ongoing judicial status hearings with of-
fender Q (p. 145) using a controlled design. Against expec-
tations, court participants randomly assigned to attend
bi-weekly status hearings did no better than those attending
status hearings on an bas neededQ basis on several measures,
including counseling attendance, drug testing results, and
self-reported drug use or criminal activity. Clients in the
bi-weekly condition did receive more sanctions, such as
increased case management or testing, but this difference
appeared to have no impact on recidivism outcomes. A
recent study of the drug court in Cincinnati similarly found
no effects for status review hearings on re-arrests or incar-
ceration for new offenses, although attendance in hearings
was associated with a reduction in arrests for drug-related
crimes (Listwan et al., 2003).
These studies represent the latest evolution of designs
examining the effects of objective coercive program ele-
ments. Another line of recent research has emphasized the
importance of the clientTs subjective experience of coercion.Wild, Newton-Taylor, and Alletto (1998) have used a variant
of the MacArthur Perceived Coercion Scale to test hypothe-
ses generated from self-determination theory, which asserts
that personal autonomy is undermined by structural and
psychological factors (legal or employer mandates, beliefs
about substance abuse severity and interpersonal pressures to
enter treatment) that promote perceived coercion. Marlowe
et al. (1996, 2001) developed the Survey of Treatment Entry
Pressures to assess clientsT reasons for entering treatment
and motivations for quitting drug use. Consistent with the
conclusions of recent literature reviews on compulsory treat-
ment (Farabee et al., 1998; Wild, Roberts, & Cooper, 2002),
findings from both of these lines of inquiry have underscored
the multi-dimensional nature of both legal and non-legal
pressures on treatment entry, and the relatively modest role
of formal legal circumstances (legal status, referrals, and
mandates) compared to client perceptions of coercion and
other motivational factors.
In two previous studies, we explored the impacts of
coercive program elements, and clientsT perceptions of legalpressure on retention in long-term residential therapeutic
communities (TC). As in the current research, both prior
studies centered around a highly structured and coercive
program developed and operated by the Kings County
District Attorney (Brooklyn, NY), the Drug Treatment
Alternative to Prison (DTAP) program. DTAP offers repeat,
non-violent felony defendants the option of treatment in a
TC in lieu of prosecution leading, in all probability, to a
prison term (Dynia & Sung, 2000; Hynes, 1999). In the
first study, DTAP participants were compared with clients
mandated to TC treatment by other, more conventional
criminal justice sources, including probation, parole and
the courts (Young, 2002). The second study was expanded
to include another experimental group composed of par-
ticipants of the local TASC program, as well as larger
DTAP and comparison group samples (Young & Belenko,
2002). In both studies, all participants were recruited upon
admission to the same TCs used by DTAP, so treatment
was held constant in the study designs. In the second larger
study, DTAP and TASC participants had higher rates of
retention than the comparison group at the two follow-up
points, 6 and 12 months post-admission; the DTAP differ-
ence held up in multivariate analyses that controlled for an
extensive set of background factors between the groups.
Both studies also used an exploratory measure, the Per-
ception of Legal Pressure questionnaire, which assessed in-
formation provided to clients about the treatment mandate
and consequences for failure, and their perceptions of moni-
toring by DTAP, TASC, or the supervision agent, and views
on enforcement and severity of the consequence for fail-
ing. In both studies, scores on the PLP were found to be
powerful, independent predictors of retention. With a few
notable exceptions (discussed in the next section), client
perceptions as measured by PLP items were consistent
with the practices and policies of the three programs, as
indicated in a survey of program documents and observa-
tions and in-depth interviews with treatment staff, super-
vision agents, and clients. Taken together, the findings
suggested that the high retention rates in the DTAP group
was partly attributable to the priority placed on enforcement
in this program, and particularly DTAPTs use of a specializedwarrant squad and other policies that increase the certainty
of incarceration upon failure in treatment. Another program
element evident in PLP results that helped contribute to
high retention in DTAP and TASC was the practice of pro-
viding frequent and consistent messages to clients about
the contingencies of treatment participation, and informa-
tion about how participation will be regularly monitored by
legal agents.
Criminal recidivism data were not available for either of
these studies. While we would anticipate favorable recidi-
vism outcomes for the DTAP and TASC groups based on
their retention performance, this remains a hypothesis until
tested with the kind of bhard dataQ demanded by policy-
makers. Further, the scope and quality of recidivism
measures are critical methodological factors in offender
treatment research. One significant improvement in recent
years is the use of multiple measures of recidivism, in
response to problems inherent in any single indicator (e.g.,
use of re-arrest is contrary to the notion of presumptive
innocence and may be influenced by police enforcement
practices, while reconviction and reincarceration are
affected by case processing policies and practices).

D. Young et al. / Journal of Substance Abuse Treatment 27 (2004) 313–323316
Some studies, however, still do not employ survival
methods or other means of assessing the time to a recidivism
event, or to account for censoring caused by follow-up
periods that are often limited to 1 year and rarely extend
beyond 2 years (e.g., Gottfredson, Najaka, & Kearley, 2003;
Marlowe et al., 2003; Spohn et al., 2001; Van Stelle et al.,
1994; Zanis et al., 2003). Researchers also have generally
failed to employ controls for time at risk in the community,
thus limiting analyses to the single first event during the
follow-up period, despite the fact that arrest chronicity—
frequent low level arrests—is comparatively common
among substance abusing offenders. Rearrest rates (number
of arrests/follow-up period) is one of the most succinct
recidivism measures for this population, but can be biased
if time-in-custody is not subtracted from the follow-up
duration. Without this adjustment for time-in-custody, re-
arrest rates are artificially deflated, making repeat offenders
look better on this outcome (Belenko, Schiff, Phillips, &
Winterfield, 1994). Each of these improvements—multiple
recidivism measures, statistical survival techniques, and
arrest rates controlling for time-in-custody—were employed
in the present recidivism research.
1.2. Description of the mandatory treatment models
To help interpret the recidivism findings we here describe
the three mandatory models studied in the current research,
incorporating some of the description from the previous
retention paper, as well as PLP findings from that research
(Young & Belenko, 2002). Typical of mandatory treatment
programs generally, the three included here show consid-
erable variation in their coercive program elements. The
coercive policies and practices of DTAP, TASC, and the
bmandated as usualQ programs were initially assessed
through document review and interviews, observations,
and informal discussions with clients, treatment staff, and
criminal justice agents supervising study participants.
Structured interviews aimed at gathering qualitative data
on clientsT experience of coercive practices were held with
45 study participants and 36 qualitative interviews were
held with criminal justice agents and treatment staff. The
formal policies and practices, as well as clientsT experiencesof them, are organized here around the information,
monitoring, enforcement; and severity areas addressed in
the PLP. Differences in the programsT client targeting and
screening policies are discussed, and a brief description of
the treatment sites is presented.
1.2.1. Client targeting and screening
Designed to address New YorkTs second-felony offender
law, the Brooklyn DTAP program targeted defendants
charged with drug sales who had a previous non-violent
felony conviction, and typically faced a prison term of
18 months to 3 years under the new charge. TASC worked
with a more diverse set of defendants which included many
repeat felony defendants but also some first-time felons and
defendants with violent charges or convictions. Typically,
TASC participants were on probation or parole from an
earlier offense and facing a new charge. TASC did not
exclusively target defendants charged with drug crimes, but
both TASC and DTAP participants had to show evidence of
a drug problem as indicated on the Addiction Severity
Index. The third study group included probationers and
parolees charged with new crimes or who were mandated in
lieu of a technical violation of the conditions of their release
(typically positive drug tests). This comparison group also
included a few offenders referred to treatment directly from
the courts (but not drug courts, which had not yet been
implemented in New York when data collection took place).
The criminal and drug histories of this group were more
varied, reflecting the discretion allowed judges and super-
vision agents in setting treatment mandates. Any group
differences in demographics, drug and criminal history, and
other client characteristics were assessed and controlled
statistically in analyses.
1.2.2. Information
DTAP and TASC had explicit, well-implemented pro-
tocols for informing the client and defense attorney about
the legal contingencies of participation, consequences of fail-
ure, and rules and expectations of the treatment program.
DTAP required participants to sign behavioral contracts that
were reviewed in open court. TASC had a similar policy to
require written agreements by participants; however, PLP
scores indicated that, unlike DTAP, TASC did not fully im-
plement or emphasize the policy. DTAP had formal agree-
ments with the TCs requiring that treatment staff reiterate
program rules and the consequences of failure to partici-
pants, and DTAP clients were significantly more likely than
TASC clients to report that staff provided information to
them about treatment mandates and legal contingencies. The
judges, probation, and parole officers who were involved in
the comparison group cases were more variable in providing
information to mandated clients, and the comparison group
had significantly lower scores than both the DTAP and TASC
groups on all seven of the information items on the PLP
measure. It was evident from staff interviews, observations,
and PLP scores that treatment staff were less likely to know
the contingencies or consequences faced by comparison
group clients.
1.2.3. Monitoring
The TCs closely followed formal agreements they had
with DTAP and TASC to provide monthly progress reports
and to inform the program when a client had left treatment
or was to be terminated. Although TASC put greater empha-
sis on monitoring, and compared to the other programs made
more frequent contact with participants, treatment staff, and
judges, this difference did not register on the clients as
indicated by PLP scores. DTAP clients were just as or more
likely than TASC clients to report that their treatment prog-
ress was being closely monitored and that infractions or

D. Young et al. / Journal of Substance Abuse Treatment 27 (2004) 313–323 317
failure would be quickly detected. Significantly lower
scores on all five of the PLP monitoring items confirmed
that probation, parole, and court actors represented in the
third group were more variable and generally less active
in terms monitoring policies and capacities. Reports from
treatment staff about client progress or problems were re-
quested at the discretion of individual supervision agents or
judges, and treatment staff contrasted the ease of reaching
TASC and DTAP staff with that of trying to inform other
supervision agents about clients who were at risk of failing
or had left treatment.
1.2.4. Enforcement
As noted previously, DTAP emphasized enforcement
and the PLP results showed that program participants were
well aware of this. DTAP documents stressed the value of
the programTs specialized warrant enforcement squad—
former law enforcement officers who pursued clients
absconding from treatment—while TASC and the compari-
son group were left to rely on standard warrant squads
which routinely assigned violent absconders a greater pri-
ority than drug offenders. DTAP also differed from the
other mandatory models in enforcing a strict policy of
denying participants another chance if they failed once in
treatment. Although TASC case managers also delivered
stern threats to clients about the severe legal consequences
of failure, they would routinely refer clients to a second
(and sometimes a third) TC if they failed in the first pro-
gram but had made some progress and did not abscond.
Second chance referrals were also common in the com-
parison group, where judges, parole, and probation agents
would tolerate relapses and make multiple treatment re-
ferrals before enforcing any legal consequences for failure.
DTAP participants appeared to be aware of the programTsmore stringent referral policy based on responses to PLP
items that addressed this issue.
1.2.5. Severity
DTAP and TASC clients faced more severe sentences
than members of the comparison group, which included
more first-time felons and offenders facing violations of
parole and probation. PLP responses conformed to this
difference, with TASC and DTAP clients scoring higher
than the comparison group on most perceived severity
items. TASC clients scored higher than either group on one
item about the severity of the threatened consequence. Two
PLP items which assessed the respondentTs aversion to
serving time in prison showed no differences between the
three groups.
1.2.6. Therapeutic community treatment
The four TC treatment sites were all long-standing,
traditional therapeutic communities operated by large,
well-established non-profit agencies. TCs are highly struc-
tured residential treatment programs for substance abusers
that are designed to promote prosocial behavior and drug
abstinence. Communal living provides the context for con-
tinuous learning where individual change in conduct, atti-
tudes, and emotions is monitored and mutually reinforced in
the day-to-day routine. Clients must earn their way through
a series of treatment stages that bring additional status,
responsibility, and independence. In the four TC sites used
by DTAP and the other study models, clients typically spend
a year in residence at a relatively remote program campus
in upper New York State and then return to New York City
to complete a 4- to 12-month reentry phase. There, clients
participate in counseling and reside in a treatment facility,
while encouraged to obtain jobs, establish community con-
tacts, and save money for independent living upon departing
the residence.
2. Materials and methods
2.1. Sample
All DTAP and TASC clients entering the treatment pro-
grams during the data collection period were eligible to take
part in the study. Other legally-referred clients admitted
to the TCs took part in a brief screening interview. These
clients were eligible for the study if they confirmed that they
had been referred to treatment by a legal supervision agent
or the court, that someone in the justice system would be
informed if they failed in treatment, and that they had been
told or believed that there would be a legal consequence for
failure. Once confirmed as eligible, clients were recruited
using a standard informed consent protocol. Four of
154 DTAP clients and three of 203 comparison clients
recruited to take part in the study refused to participate.
Study participants were administered an intake interview as
soon as possible, typically within the first 2 weeks of their
admission to the TC (all were completed within a month
of admission). About 8% of the clients referred to the TCs
by DTAP, TASC, or other legal sources dropped out of
treatment within a few days of admission, before they could
be recruited for the study. Study participants thus included
150 DTAP clients, 124 TASC clients, and 76 clients in the
bmandated as usualQ comparison group.
As shown in Table 1, study participants were predom-
inantly male, African-American or Hispanic, and averaged
33 years old. They had extensive drug and criminal
histories, poor employment and educational histories, and
a relatively high incidence of medical and psychological
problems. On most background items the three groups were
similar. DTAP had proportionately more Hispanic clients
(62%) than TASC (50.8%) and the comparison group
(42.1%). While the groups were similar in regard to past
heroin use, TASC and comparison group clients reported
more extensive use of crack cocaine and, especially, pow-
dered cocaine. Predictably, DTAP clients averaged more
drug convictions and fewer arrests for violent offenses,
reflecting the programsT different admissions policies. These

Table 1
Sample description
Variable description
DTAP
(N = 130)
TASC
(N = 124)
Other
CJ referrals
(N = 76)
Demographics, SES
Age 33.1 32.7 33.5
% Male 88.7 88.0 90.1
Race/Ethnicity**
% Hispanic 62 50.8 42.1
% African-American 32.7 47.6 56.6
% White 5.3 1.6 1.3
% High school diploma
or GED
26 19.4 27.6
Weeks worked in past year 14.9 13.5 11.3
Medical, psychiatric problems
% Reports chronic medical
problem(s)
16.7 21 11.9
% Significant need for
medical treatment*
15.3 32.2 27.6
% Psychiatric
hospitalization, lifetime
6 6.5 7.9
% Serious depression,
lifetime
48.7 43.6 27.6
Substance abuse, criminal history
% N 1 prior admissions to
drug treatment*
37.4 45.1 59.2
Years regular use of heroin 6.9 7.1 6
Years regular use of crack
cocaine**
3.4 5.4 4.6
Years regular use
of cocaine**
4.1 7.6 8.4
% Significant need for drug
treatment
87.3 84.5 93.3
% Ever charged with
robbery**
12.7 21.8 31.6
Felony drug convictions** 3.9 3.1 2.3
* p b .05.
** p b .01.
Table 2
Recidivism results by group
Variable description
DTAP
(N = 150)
TASC
(N = 124)
Other CJ
referrals
(N = 76)
Follow-up periods
Tx. admission to
end date (months)**
44.5 41.1 42.9
Tx. termination/
completion to end date
28.1 26.8 29.9
Time-at-risk (TAR)
since admission
37.2 37.9 39
Unadjusted recidivism measures
Percent arrested** 30 28.1 55.6
Percent arrested for
felony*
16.7 17.7 22.9
Percent arrested for
misdemeanor*
18 16.1 35.5
Percent convicted of
felony
10 6.6 17.1
Percent convicted of
misdemeanor*
12 12.1 30.3
Percent arrested for
felony drug crime
10.7 13.7 18.4
Percent arrested for misd.
drug crime*
12.7 8.3 21.4
Months to first arrest 26.4 21.8 21.1
Recidivism measures, adjusted for TAR
Arrest rate (annualized)** .19 .21 .46
Arrest rate, felonies only .08 .13 .19
Arrest rate, misdemeanors
only**
.11 .08 .27
Conviction rate, felonies .04 .07 .10
Conviction rate,
misdemeanors**
.08 .07 .24
Arrest rate, drug felonies .05 .10 .12
Arrest rate, drug
misdemeanors**
.05 .03 .10
* p b .05.
** p b .01.
D. Young et al. / Journal of Substance Abuse Treatment 27 (2004) 313–323318
differences were controlled statistically in testing for group
differences in multivariate analyses.
2.2. Baseline measures
Client history and status information was gathered on
the Addiction Severity Index (ASI; McLellan, Luborsky,
Cacciola, & Griffith, 1985; McLellan et al., 1992). The ASI
questions were supplemented with several more detailed
items we created covering employment history and self-
reported criminal behavior. Official criminal history data
were obtained from the New York State Division of Criminal
Justice Services (DCJS). The research intake interview also
included the Perception of Legal Pressure questionnaire,
developed by the researchers. The 39-item measure had
respectable reliability, with a standardized internal consis-
tency coefficient (CronbachTs a) of .80. Scores on the over-
all PLP measure ranged from 32 to 73 with a mean of
52.4 (SD = 8.9); higher scores indicated greater perceived
legal pressure.
2.3. Recidivism
Recidivism was determined from official records obtained
from DCJS and the Department of Correctional Services.
The follow-up period covered by the data averaged 3.59
(SD = .43) years from the study participants’ date of ad-
mission to treatment and ranged from 2.75 to 4.47 years.
Each subjectTs time at risk was calculated by subtracting
time in custody (jail or prison) during follow-up from the
total follow-up duration. Time at risk averaged 3.16 years
(SD = .88). Several recidivism measures were assessed,
including number of re-arrests, charge types (misdemeanor,
felony, drug), time to arrest, and conviction. To control for
the variable follow-up period used in the research, we used
an arrest rate measure, calculated by dividing the total
number of arrests by time at risk, in the principal analysis.
To illustrate, the arrest rate for a client who was arrested
twice between her DTAP admission and the data cut-off
date 3 years later, and who spent 6 months in jail as a result

D. Young et al. / Journal of Substance Abuse Treatment 27 (2004) 313–323 319
of those arrests, would be calculated as follows: 2 arrests /
(1096 days�181 days) = .0021587. When annualized for
descriptive purposes, this amounts to a rate of .79 arrests
per year.
2.4. Analysis plan
Analyses progressed in three phases. Initial analyses
focused on differences among the study groups and bi-
variate tests to select variables for inclusion in subsequent
multivariate analyses of retention. One-way ANOVAs and
chi-square tests were conducted to test the equivalence of the
three groups and to identify variables which needed to be
controlled in multivariate tests involving the grouping factor.
Bi-variate analyses (t-tests and chi-square statistics) were
done to identify variables from the ASI and the official cri-
minal record that were minimally related to retention ( p b .2)
and to assess multicollinearity of the predictor variables.
Bi-variate analyses also explored group differences on the
recidivism measures.
Variables emerging from the data reduction process
were used to build multivariate models. Ordinary least
squares multiple regressions were conducted involving the
arrest rate variable. Logistic regression was used to model
arrest as a dichotomous outcome and survival analysis
and Cox hazard models examined recidivism taking into
account time to arrest and censoring. Finally, conviction as a
dichotomous outcome was assessed in a logistic regression.
Predictors were entered in the models using the forward
selection method (tests using backward likelihood ratio
elimination yielded virtually the same results). The grouping
variable, dummy coded with the comparison group serving
as the reference category, was forced into the model in
0.40
0.50
0.60
0.70
0.80
0.90
1.00
0 100 200 300 400 500 6
Days from Admiss
Cu
mu
lati
ve S
urv
ival
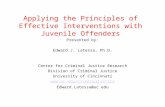
Fig 1. Survival function of ar
the final step, to assess its independent effects on the recidi-
vism outcomes.
3. Results
3.1. Bi-variate recidivism outcomes
Table 2 shows recidivism results for the three study
groups. Bi-variate tests indicate that, consistent with the
retention findings reported previously (Young & Belenko,
2002), recidivism was significantly higher among compari-
son clients than those in the other two groups on several
measures, including percent arrested, rates of arrest control-
ling for time at risk, and time to arrest. The comparison
group had higher rates of felony and misdemeanor arrests
and convictions; however, this difference was not significant
in the case of the felony arrest and conviction rates. No
differences were observed between the DTAP and TASC
samples in any of these analyses.
Differences among the groups on time to arrest are
evident in the survival curves shown in Fig. 1. Compared to
DTAP, arrests clearly occur sooner in both the comparison
and TASC groups; the first arrests in the DTAP group were
observed about 6 months after admission to the program.
After a first group of TASC clients were arrested in the
initial months after admission, very few TASC participants
were re-arrested between 3 months and 1 year post-
admission. Throughout the tracking period, the proportion
of clients bsurvivingQ (not arrested) in TASC and DTAP was
very similar—within about five percentage points. By
contrast, the proportion arrested in the comparison group
steadily diverges from the arrest rate for the other groups
00 700 800 900 1000
ion
ComparisonTASCDTAP
Study Group
rest outcome by group.

Table 3
Multiple regression with arrest rate as criterion
Predictor Variable Coefficient
Standardized
coefficient (h)t
statistic
p
value
Gender (0 = male,
1 = female)
�.153 �.09 �1.77 .077
Education level �.099 �.11 �2.16 .031
Bothered by
employment problems
�.030 �.09 �1.65 .100
Held fulltime job
at admission
�.087 �.71 �1.37 .171
Total prior theft arrests .044 .12 2.26 .024
Total prior days
incarcerated
.028 .20 3.82 .000
Total prior felony drug
convictions
�.023 �.04 �.61 .547
Last charge was probation
or paroleviolation
.218 .13 2.55 .011
Sold drugs frequently in
prior year
�.246 �.13 �2.53 .012
Total years cocaine use �.007 �.08 �1.55 .122
Prior drug treatment
admissions
.009 .04 .91 .366
Prescribed
psychiatric meds
.226 .08 1.59 .113
Chronic medical problems .138 .09 1.75 .082
Study group
DTAP= 1; comparison
group = 0
�.216 �.19 �2.43 .015
TASC = 1; comparison
group = 0
�.229 �.19 �2.85 .005
Model Statistics R2 = .21
F = 5.64 (df = 15, 325)
p b .0001
Table 4
Cox regression results on re-arrest
Predictor variable Wald m2 h (p)
odds
ratio
Gender (0 =male, 1 = female) 9.55 �1.08 (.002) .334
Education level 6.13 �.367 (.01) .692
Bothered by employment
problems
8.25 �.165 (.004) .848
Employed full time past
3 years
8.61 �.673 (.003) .510
Total prior felony drug
convictions
.130 �.020 (.88) .980
Last charge was
probation/parole violation
12.83 .881 (.000) 2.41
Sold drugs frequently in
prior year
8.52 �.822 (.004) .440
Total years cocaine use 5.37 �.034 (.021) .967
Prior drug treatment
admissions
3.02 .057 (.08) 1.06
Chronic medical
problems
7.14 .670 (.007) 1.95
Study group 20.33 (.000)
DTAP= 1; comparison
group = 0
6.04 �.383 (.014) .682
TASC=1; comparison
group = 0
3.38 �.264 (.066) .768
Model Statistics m2 = 71.35 ( p b .001)
df / N = 12 / 342
�2 Log L= 1311.73
D. Young et al. / Journal of Substance Abuse Treatment 27 (2004) 313–323320
beginning about 8 months after admission. By 3 years post-
admission, the proportion of comparison group clients who
were re-arrested is about 25% greater than that rate for
TASC and DTAP groups.
3.2. Multivariate models
A number of multivariate analyses tested whether the
differences among the study groups on the recidivism
outcomes would hold up controlling for other factors.
Table 3 presents the OLS multiple regression results on
the arrest rate variable. The R2 for this overall model was
.21 (F = 5.64; df = 15, 325; p b .001). This analysis showed
that DTAP and TASC clients had significantly lower arrest
rates than the comparison group while holding constant pre-
admission group differences on prior drug convictions,
cocaine use, treatment admissions, and medical problems, as
well as other factors which met the criteria for entry in the
stepwise model.
Although the history variables on which the groups
differed were unrelated to subsequent arrests, other criminal
history variables were selected for the model, including total
time incarcerated, prior thefts, and prior probation or parole
violation. All three of these are traditionally associated with
arrest chronicity, particularly low level property crime and
violations while on supervision. Surprisingly, clients who
self-reported that they had sold drugs frequently in the prior
year had lower arrest rates. Education level was inversely
related to recidivism in the regression model, as were two
marginally related employment measures. Experiencing
chronic medical problems was also marginally positively
related to arrest rate.
Logistic regression and Cox hazard models of arrest
showed generally similar results. In the logistic analysis the
overall model had a pseudo R2 of .24 (model v 2 = 65.19;
p b .001) and the differences between the comparison group
and DTAP (h=�1.15, p b .001) and the comparison group
and TASC (h=�1.31, p b .001) on the dichotomous arrest
outcome were upheld as significant, yielding odds ratios of
.317 and .269 respectively. The Cox results showed the
same significant effect for the DTAP group, while the effect
for TASC group membership was marginal ( p = .069, see
Table 4). As in the OLS analysis, a prior parole or probation
violation was associated with arrest and time to arrest;
however, the prior theft and time incarcerated variables did
not contribute to the Cox model. Being female, having a
higher education level, steadily holding a full time job in
recent years, and reporting concern about employment
problems were inversely related to arrest and time to arrest
in the model. Mirroring findings in the multiple regression
analyses, frequent prior drug sales, as well as years of
regular cocaine use were negatively associated with the

D. Young et al. / Journal of Substance Abuse Treatment 27 (2004) 313–323 321
arrest outcome, while having chronic medical problems was
a positive predictor.
To further test the robustness of the group differences, an
additional analysis examined conviction as a variant of
recidivism. We also considered performing an analysis
involving time incarcerated during follow-up, but rejected
this as an outcome of interest because it is as much a re-
flection of the varying sanctioning policies of the mandatory
treatment models as it is the behavior of the client. In the
conviction analysis, logistic regression was chosen over a
hazard model, since time to conviction is often influenced by
case processing practices and legal maneuvering. The
conviction results generally replicated those found for
arrest, with a pseudo R2 of .21 (model v2 = 51.90;
p b .003) and significant effects for DTAP (h =�1.20,
p b .002) and TASC (h =�1.28, p b .001), with odds ratios
of .303 and .278 respectively.
4. Discussion
State and local policymakers, faced with the worst
budget crises in a generation, are searching for safe and
effective ways to reduce criminal justice system costs
(Campbell, 2003). Treatment diversion programs are
attractive because of their potential cost efficiencies (Lang
& Belenko, 2000), but much more must be known about the
impacts of different compulsory treatment models and the
constituent policies and practices that make them work.
Extending a line of research on two such programs that had
been shown to have high retention rates (Young, 2002;
Young & Belenko, 2002), the present study showed that
criminal recidivism of participants in the Brooklyn DTAP
and TASC programs were substantially below those of a
matched comparison group of offenders who were man-
dated to treatment from conventional criminal justice
sources—sources that had similar clients but lacked the
more formal monitoring and sanctioning procedures of
DTAP and TASC. The value of these findings are enhanced
by the comparatively long follow-up period used in the
research, which averaged 3.6 years from the study partici-
pantsT date of admission to the program and 2.3 years from
the point these clients either completed or were terminated
from treatment. The capacity to assess recidivism through
arrest rates by calculating participantsT time at risk during
the follow-up period was another strength of the study
design. Taking time in custody into account helped level the
playing field between the groups, and arrest rate provided a
more accurate index of recidivism than more typical arrest
outcomes (e.g., probability of arrest, number of arrests).
The proportion of comparison group participants that
were rearrested (55.6%) was similar to that reported for
prison releasees nationally (Langan & Levin, 2002) but
almost twice the proportion rearrested in DTAP and TASC
(30% and 28.1% respectively). This pattern of group
differences was robust across multiple measures of recidi-
vism. Significantly more comparison group clients were re-
arrested for both misdemeanors and felonies during the
tracking period, and the reconviction rates in this group
were 1.7 to 2.5 greater than those for DTAP and TASC. The
fact that the felony reconviction differences were not
significant may have been due to the restricted range in
their distributions. The overall annual arrest rate for the
comparison group (.46) was over twice the rate for DTAP
(.19) or TASC (.21).
These recidivism results were tested in four different
multivariate analyses that controlled for the small number of
variables on which the groups differed pre-treatment, and
other factors found to be associated with the recidivism
outcomes. With these factors held constant, three of the
analyses assessed a variation of the overall re-arrest rate
outcome measure (OLS regression), any arrest (logistic
regression), and time to re-arrest accounting for censoring
(survival analysis and Cox hazard regression)—and a fourth
assessed any conviction (logistic regression). With the
exception of a marginal finding for the TASC group in
one analysis, results consistently showed that DTAP and
TASC clients had significantly more favorable outcomes on
these measures than the comparison group. As expected,
criminal history measures were also significant predictors
across the multiple models. An offense that included a
parole or probation violation was the history item most
predictive in all of the models assessing re-arrest. Other
significant criminal record items in the OLS model included
total prior thefts and days incarcerated—both indicators of
the kind of chronic pattern of frequent, low level arrests that
typically comprise criminal records with high arrest rates.
Most of the other factors that were significant in these
models had also been found in past research. Higher levels
of education, fulltime employment, and expressing concern
about employment problems were consistently associated
with less recidivism. Having chronic medical problems
was shown to be a risk factor for re-arrest. It was some-
what unexpected to find that female participants in the
TCs were less likely to recidivate, given concerns raised
by some reviewers about the effectiveness of confronta-
tional, group-oriented approaches with women substance
abusers (Lockwood, McCorkel, & Inciardi, 1998; Peugh &
Belenko, 1999). Additional research exploring the ability
of these TCs to address the unique needs of women
clients—their sensitivity to clientsT traumatic experiences
and psychological distress, and social support, child care,
and transitional issues (Bouffard & Taxman, 2000)—are
suggested by these results.
The key findings of reduced recidivism for the DTAP
and TASC groups provide potentially valuable support for
compulsory treatment and these models in particular. For all
the drawbacks of individual measures, recidivism is the
benchmark sought by policymakers and the public for
assessing correctional interventions. The need for studies
involving recidivism was further evidenced in a recent,
extensive review of research on compulsory treatment (Wild

D. Young et al. / Journal of Substance Abuse Treatment 27 (2004) 313–323322
et al., 2002). Of 161 articles that met their initial review
criteria, the authors identified only 18 studies that were
adequate methodologically to assess the effectiveness of a
compulsory treatment program, and only six of these
assessed recidivism as an outcome. Moreover, while more
than half of the studies that tracked other outcomes (entry
and retention in treatment) showed favorable effects for
clients in the compulsory treatment group, only two of the
six recidivism studies demonstrated lower recidivism rates
for this group. This review did not include the most recent
studies discussed in the background section of the present
paper, but it is notable that even the most rigorous of these
studies—controlled evaluations of drug court programs that
track recidivism outcomes (Gottfredson & Exum, 2002;
Listwan et al., 2003)—continue to show mixed results.
In this regard, it is instructive to review findings from the
Perception of Legal Pressure measure and from our obser-
vations and qualitative interviews with staff and clients,
which point to the specific coercive program policies and
practices that likely account for the success of DTAP and
TASC. Providing information to mandated clients about
the conditions of treatment participation and consequences
for failure—and convincing them those conditions will be
enforced—stood out as effective coercive strategies in this
research. DTAPTs use of a warrant enforcement squad, and
TASCTs strategy of mixing support for clients with frequent
cajoling and threats appears to create the perception of en-
forcement. Monthly progress reports to the legal agent, case
managersT phone calls, program visits, and the use of court
appearances and graduated responses to early signs of failure
likely reinforce this perception (Young, 2002; Young &
Belenko, 2002).
A major caveat to this research is that the findings may
be specific to compulsory models employing long-term
residential treatment, and/or to offenders with compara-
tively serious criminal records. The PLP was developed for
use in these community-based TCs, with these kinds of
clients, and studies must be done to assess whether these
findings can be replicated in the much more ubiquitous
outpatient settings and client profiles that predominate in
drug courts and most TASC programs. More generally, self-
reported perceptions of the presence and strength of
coercive program components is at best an indirect indicator
of their causal role in client retention and recidivism
outcomes. Future research should be aimed at expanded
use of both perceptual tools like the PLP as well as
objective indicators of program practices and policies in
study designs that can isolate and identify their impact on
client outcomes in the full range of compulsory models now
operating nationally.
Acknowledgments
This research was funded by a grant from the National
Institute of Drug Abuse (R01-DA09075) to Steven Belenko.
We much appreciate the support of our colleagues at the
Vera Institute of Justice, where much of this research was
conducted; Susan Powers and Paul Dynia, formerly of the
Office of the Kings County District Attorney; Kenneth Linn
of EAC-TASC; and the clients, administrators, and staff of
the treatment programs involved in the study.
References
Arrestee Drug Abuse Monitoring Program (ADAM). (2000). 1999 annual
report on drug use among adult and juvenile arrestees. Washington,
DC7 National Institute of Justice.
Anglin, M. D. (1988). The efficacy of civil commitment in treating narcotic
addiction. In C. Leukefeld & F. Tims (Eds.), Compulsory treatment of
drug abuse: research and clinical practice. NIDA research Monograph
Series #86 (pp. 8–34). Washington, DC7 Government Printing Office.
Anglin, M. D., Brecht, M. L., & Maddahian, E. (1989). Pretreatment
characteristics and treatment performance of legally coerced versus
voluntary methadone maintenance admissions. Criminology, 27,
537–557.
Anglin, M. D., Longshore, D., & Turner, S. (1999). Treatment alternatives
to street crime: an evaluation of five programs. Criminal Justice and
Behavior, 26, 168–195.
Belenko, S. (1998). Research on drug courts: a critical review. New York7
The National Center on Addiction and Substance Abuse at Columbia
University.
Belenko, S. (2000). The challenges of integrating drug treatment into the
criminal justice process. Albany Law Review, 63, 833–876.
Belenko, S., Schiff, M. F., Phillips, M. T., & Winterfield, L. (1994).
Modeling the prison displacement effects of alternative sanctions
programs: A case study. Prison Journal, 73, 167–197.
Bouffard, J. A., & Taxman, F. S. (2000). Client gender and the imple-
mentation of jail-based therapeutic community programs. Journal of
Drug Issues, 30, 881–900.
Brecht, M. L., Anglin, M. D., &Wang, J. C. (1993). Treatment effectiveness
for legally coerced versus voluntary methadone maintenance clients.
American Journal of Drug and Alcohol Abuse, 19, 89–106.
Bureau of Justice Statistics. (2001). Trends in state parole, 1990–2000.
Washington, DC7 Author.
Campbell, R. (2003). Dollars and sentences: legislators views on prisons,
punishment, and the budget crisis. New York7 Vera Institute of Justice.
Collins, J. J., & Allison, M. (1983). Legal coercion and retention in drug
abuse treatment. Hospital and Community Psychiatry, 34, 1145–1149.
Dynia, P., & Sung, H. (2000). The safety and effectiveness of diverting
felony drug offenders to residential treatment as measured by
recidivism. Criminal Justice Policy Review, 11, 299–311.
Farabee, D., Prendergast, M., & Anglin, D. (1998). The effectiveness of
coerced treatment for drug-abusing offenders. Federal Probation, 62,
3–10.
Gottfredson, D. C., & Exum, M. L. (2002). The Baltimore City drug
treatment court: one-year results from a randomized study. Journal of
Research in Crime and Delinquency, 39, 337–356.
Gottfredson, D. S., Najaka, S. S., & Kearley, B. (2003). Effectiveness of
drug treatment courts: evidence from a randomized trial. Criminology
and Public Policy, 2, 171–196.
Hammett, T. M., Gaiter, J. L., & Crawford, C. (1998). Researching
seriously at-risk populations: health interventions in criminal justice
settings. Health Education and Behavior, 1, 99–120.
Harrell, A. (1998). Drug courts and the role of graduated sanctions.
National Institute of Justice research preview. Washington, DC7
Government Printing Office.
Harrell, A., & Cavanaugh, S. (1995). Compliance with drug abstinence
requirements during pretrial release: a comparison of graduated
sanctions and treatment for drug felony defendants. Paper presented

D. Young et al. / Journal of Substance Abuse Treatment 27 (2004) 313–323 323
at the 47th Annual Meeting of the American Society of Criminology,
Boston, MA.
Harrell, A. V., Hirst, A., & Mitchell, O. (2000). Implementing system-wide
interventions for drug-involved offenders in Birmingham, Alabama:
evaluation of the breaking the cycle demonstration. Washington, DC7
Urban Institute.
Higgins, S. T., & Petry, N. M. (1999). Contingency management: incentives
for sobriety. Alcohol Research and Health, 23, 122–127.
Hiller, M. L., Knight, K., Broome, K. M., & Simpson, D. D. (1998). Legal
pressure and treatment retention in a national sample of long-term
residential programs. Criminal Justice and Behavior, 25, 463–481.
Hser, Y. I., Maglione, M., Polinsky, M. L., & Anglin, M. D. (1998).
Predicting drug treatment entry among treatment-seeking individuals.
Journal of Substance Abuse Treatment, 15, 213–220.
Hynes, C. J. (1999). Drug treatment alternative-to-prison program:
ninth annual report. Brooklyn, NY7 Kings County District Attor-
ney’s Office.
Knight, K., Hiller, M. L., Broome, K. M., & Simpson, D. D. (2000). Legal
pressure, treatment readiness, and engagement in long-term residential
programs. Journal of Offender Rehabilitation, 31, 101–115.
Lang, M. A., & Belenko, S. (2000). Predicting retention in a residential
drug treatment alternative to prison program. Journal of Substance
Abuse Treatment, 19, 145–160.
Langan, P. A., & Levin, D. J. (2002). Recidivism of prisoners released in
1994. Bureau of Justice Statistics special report. Washington, DC7
Government Printing Office.
Listwan, S. J., Sundt, J. L., Holsinger, A. M., & Latessa, E. J. (2003). The
effect of drug court programming on recidivism: the Cincinnati ex-
perience. Crime and Delinquency, 49, 389–411.
Lockwood, D., McCorkel, J., & Inciardi, J. A. (1998). Developing
comprehensive prison-based therapeutic community treatment for
women. In S. J. Stevens & H. K. Wexler (Eds.), Women and substance
abuse: gender transparency. Binghamton, NY7 Haworth Press.
Maguire, K., & Pastore, A. L. (Eds.) (1999). Sourcebook of criminal justice
statistics—1998. Washington, DC7 Bureau of Justice Statistics.
Marlowe, D. B., Festinger, D. S., Lee, P. A., Schepise, M. M., Hazzard, J.,
Merrill, J. C., Mulvaney, F. D., & McClellan, A. T. (2003). Are judi-
cial status hearings a key component of drug court: during-treatment data
from a randomized trial. Criminal Justice and Behavior, 30, 141–162.
Marlowe, D. B. (2001). Coercive treatment of substance abusing criminal
offenders. Journal of Forensic Psychology Practice, 1, 65–73.
Marlowe, D. B., Merikle, E. P., Kirby, K. C., Festinger, D. S., & McLellan,
A. T. (2001). Multidimensional assessment of perceived treatment-entry
pressures among substance abusers. Psychology of Addictive Behaviors,
15, 97–108.
Marlowe, D. B., Kirby, K. C., Bonieskie, L. M., Glass, D. J., Dodds, L. D.,
Husband, S. D., Platt, J. J., & Festinger, D. S. (1996). Assessment of
coercive and noncoercive pressures to enter drug abuse treatment. Drug
and Alcohol Dependence, 42, 77–84.
Marlowe, D. B., & Kirby, K. C. (1999). Effective use of sanctions in drug
courts: lessons from behavioral research. National Drug Court Institute
Review, 2, 1–32.
McLellan, A. T., Kushner, H., Metzger, D., Peters, F., Smith, I., Grissom,
G., Pettinati, H., & Argeriou, M. (1992). The fifth edition of the
Addiction Severity Index. Journal of Substance Abuse Treatment, 9,
199–213.
McLellan, A. T., Luborsky, L., Cacciola, J., & Griffith, J. E. (1985).
New data from the Addiction Severity Index: reliability and validity
in three centers. The Journal of Nervous and Mental Disease, 173,
412–423.
National Association of Drug Court Professionals. (1997). Defining drug
courts: the key components. Washington, DC7 U.S. Department of
Justice, Office of Justice Programs.
Peugh, J., & Belenko, S. (1999). Substance-involved women inmates:
challenges to providing effective treatment. Prison Journal, 79, 23–44.
Pompi, K. F., & Resnick, J. (1987). Retention of court-referred adolescents
and young adults in the therapeutic community. American Journal of
Drug and Alcohol Abuse, 13, 309–325.
Rhodes, W., & Gross, M. (1997). Case management reduces drug use and
criminality among drug-involved arrestees: an experimental study of
an HIV prevention intervention. Washington, DC7 National Institute
of Justice.
Salmon, R. W., & Salmon, R. J. (1983). The role of coercion in rehabi-
litation of drug abusers. International Journal of the Addictions, 18,
9–21.
Spohn, C., Piper, R. K., Martin, T., & Frenzel, E. D. (2001). Drug courts
and recidivism: the results of an evaluation using two comparison
groups and multiple indicators of recidivism. Journal of Drug Issues,
31, 149–176.
Steer, R. A. (1983). Retention in drug-free counseling. The International
Journal of the Addictions, 18, 1109–1114.
Taxman, F. (2000). Unraveling bwhat worksQ for offenders in substance
abuse treatment services. National Drug Court Institute Review, 2,
91–132.
Taxman, F. S., & Bouffard, J. (2002). Assessing therapeutic integrity in
modified therapeutic communities for drug-involved offenders. Prison
Journal, 82, 189–212.
Taxman, F. S., Soule, D., & Gelb, A. (1999). Graduated sanctions: stepping
into accountable systems and offenders. Prison Journal, 79, 182–204.
Van Stelle, K. R., Mauser, E., & Moberg, D. P. (1994). Recidivism to the
criminal justice system of substance-abusing offenders diverted into
treatment. Crime and Delinquency, 40, 175–196.
Wenzel, S. L., Longshore, D., Turner, S., & Ridgely, M. S. (2001). Drug
courts: a bridge between criminal justice and health services. Journal
of Criminal Justice, 29, 241–253.
Wild, T. C. (1999). Compulsory substance-user treatment and harm
reduction: a critical analysis. Substance Use and Misuse, 34, 83–102.
Wild, T. C., Newton-Taylor, B., & Alletto, R. (1998). Perceived coercion
among clients entering substance abuse treatment: Structural and
psychological determinants. Addictive Behaviors, 23, 81–95.
Wild, T. C., Roberts, A., & Cooper, E. L. (2002). Compulsory substance
abuse treatment: an overview of recent findings and issues. European
Addiction Research, 8, 84–93.
Young, D. (2002). Impacts of perceived legal pressure on retention in drug
treatment. Criminal Justice and Behavior, 29, 27–55.
Young, D., & Belenko, S. (2002). Program retention and perceived coercion
in three models of mandatory drug treatment. Journal of Drug Issues,
32, 297–328.
Zanis, D. A., Mulvaney, F., Coviello, D., Alterman, A. I., Savitz, B., &
Thompson, W. (2003). The effectiveness of early parole to substance
abuse treatment facilities on 24-month criminal recidivism. Journal of
Drug Issues, 22, 223–236.