Creating and Sustaining a Patient Safety Program · Creating and Sustaining a Patient Safety...
37
Creating and Sustaining a Patient Safety Program August 29, 2019 11:00 am – 12:00 noon PDT
Transcript of Creating and Sustaining a Patient Safety Program · Creating and Sustaining a Patient Safety...

Creating and Sustaining a Patient Safety Program
August 29, 201911:00 am – 12:00 noon PDT

Moderator/Host
Barbara Abeling, PhD, RNSafety & Reliability Clinical [email protected]
Asma [email protected]

Housekeeping Items
• All lines will be muted. Raise your hand if you wish to be unmuted.
• The presentation slides and recording will be available within 1-3 business days.
• 1 CE unit will be provided to CHPSO/HQI/CHA Members:– Complete the survey by September 6, 2019– CE certs will be emailed within five business days

How to ask a question

Speakers
Stephanie Bailey, MPH, CJCPInpatient Director – Quality & Patient Safety
John Muir Health
Melissa McRae, MS-HCAManager – Quality & Patient Safety
John Muir Health

• 3 Hospital System
–Two acute care hospitals (798 licensed beds)
–Behavioral Health Center
• John Muir Physician Network
–Over 1,000 primary care and specialty physicians
–Five major outpatient centers
–Comprehensive selection of primary care, urgent care and specialty care
Concord Medical Center
Walnut Creek Medical Center
Behavioral Health Center
Ambulatory Clinic
JMH System Overview

CA Health & Safety Code §1279.6 Requirements: Patient Safety Plan
• Patient Safety Committee including at least physicians, RNs, pharmacist, administrators
• System for reporting patient safety events• A safety culture that encourages reporting• Process for analyzing safety events• Ongoing patient safety training

CA Health & Safety Code §1279.6 Requirements: Patient Safety Committee
• Review and approve patient safety plan at least annually
• Receive and review safety event reports• Monitor corrective actions related to events• Make recommendations to eliminate future
patient safety events

Internal Data
Safety Event Response &
Analysis
Pro-active Risk Assessments
External DataCulture of Trust
Organization-Wide Learning
Patient & Family Engagement
Communication with Patients &
Families after Harm
Essential Elements of a Successful Patient Safety Program

1. Internal Data1. Reporting by staff and physicians Patient Safety Alerts
2. Reports at Daily Safety Huddles3. Culture of safety surveys4. Patient complaints and grievances5. Physician Peer Review

Patient Safety Alert (PSA) Reports• 723 event reports/month; 24/day (ADC=450)Physicians may use a mobile app to reportLink to reporting system embedded within Epic
• 79% of files are “closed” within 30 daysApparent Cause Analysis prompts embeddedOperational leader must “sign-off”Risk Manager closes the file
• Front line staff may view actions taken on an event they reported

2. Safety Event Response & Analysis•Apparent Cause Analysis (ACA)•Root cause Analysis (RCA)•Safety Event Classification (SEC)•Measuring our Serious Safety Event Rate (SSER) over time

Analysis of Safety EventsSerious Safety Event Precursor or
Near-Miss Event
Risk Manager coordinates a Root-Cause Analysis
(RCA)
Operational Leader conducts an Apparent Cause Analysis
(ACA), when indicated
Serious Safety Event Precursor or Near-Miss Event

Serious Safety Event Rate (SSER)
Reviewed as Potential SSEs & Classified by Safety Event Review Team (SERT)
Some HAIs and
HAPIs
Patient Safety Alerts
Physician Peer
ReviewFor Patient Safety Alerts and HAIs/HAPIs:
Operational Leaders assess events for deviations in care
Risk Managers confirm deviations + impact of at least moderate harm
For Physician Peer Review
Peer Review RNs prepare the case
Physician Reviewers confirm deviations + impact of at least moderate harm

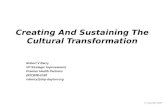
SSER Over Time
Our highest point SSER was in April 2016
As of June 2019, our SSER has reduced by 67.5%

3. Pro-Active Risk Assessments4. External Data
•FMEAs•Risk Assessments by medical malpractice insurer•Sentinel Event Alerts•External data helps inform risk assessmentsCHPSOISMPECRI
TJCHIIN

5. Culture of Trust• Fair & Just Culture (including documented
use when reviewing safety events)• Closing the loop on reported safety events• Care for the Caregiver


Fair & Just Culture• How do you know leaders are using it? • Data captured in Patient Safety Alert system:
“Was the F&J Culture Decision Tree used to evaluate the actions of the staff member?”
• Leader expectation: Decision Tree reviewed together with the employee
• Jan-Jun data: 55% of the time

Culture of Trust
Employees willingly report safety
concerns
Employees receive feedback from
leaders
Employees have confidence leaders
will take action

Closing the Loop• Follow-up to those
who report issues• Communication to
hospital staff and clinicians about events and actions taken

Care for the Caregiver• “JMH is committed to providing support and
care for our caregivers, workforce members and medical staff impacted by emotionally traumatic events”
• Includes trained peer supporters available for individual care after harm, error or traumatic events

6. Organization-wide Learning• HRO & Error Prevention Error Prevention Tools Rounding to Influence (RTI)COE Ambassador Program
• Organization-wide publications Great Catch/HeRO AwardsOne Patient’s StoryLessons Learned

Organization-Wide Learning
24
Serious Safety Events (SSEs)
Precursor Safety Events (PSEs)
Near Miss Events, Great Catches (NME)
Lessons Learned
One Patient’s Story
Great Catch/HeROAwards

Organization-Wide Learning
Distributed to all staff and physicians across JMH

Lessons Learned Publication•Format:Case SummaryLessons Learned (why it happened)Action Taken (to prevent a recurrence)What is a Root Cause Analysis?
•Process:Approved by the operational owner, Safety
Committee, Privacy Officer, Legal


Error Prevention Tools that may have prevented an Error
0
50
100
150
200
250
300
Validate and Verify STAR Team Checking Ask Clarifying Questions

7. Patient & Family Engagement• Patient & Family Advisory Committee (PFAC)Originally, one committee for acute care
hospitalsExpanding now to Ambulatory and Behavioral
Health PFACs• PFAC members on our safety committee,
involved with PI projects

8. Communication with Patients and Families after Harm
• Early, transparent, empathic• Goal = first discussion within 1 hour• Risk Managers generally facilitate• Includes appropriate physician & other
leader(s) • Checklist is used to prepare• One contact person for patient/family

Policies & Procedures• Patient Safety Plan• Patient Safety Alerts• Root Cause Analysis (RCAs)• Fair & Just Culture Response to Errors and Patient Safety
Events• Early Communication with Patient/Family After a Harm
Event or Error• Support for Caregivers After Harm, Error or Traumatic
Events

How to ask a question

Upcoming Safe Table ForumsCHPSO Members only
Date Time Topic
September 12 10:00 am – 11:00 am PDT Workplace Bullying and Unprofessional Behavior
September 26 10:00 am – 11:00 am PDT Smart Pump Issues
October 9 10:00 am – 11:00 am PDT Safe Pathology Specimen Management
October 23 10:00 am – 11:00 am PDT TBD
November 7 10:00 am – 11:00 am PDT TBD
November 20 10:00 am – 11:00 am PDT TBD
December 11 10:00 am – 11:00 am PDT TBD

Upcoming HQI-CHPSO Webinars
Patient Safety Work Product - Privileged and Confidential
Date Time Topic
September 18 11:00 am – 12:00 pm PDT
Three “Stepps” to Enhance Teamwork and Prevent Adverse Events
October 24 11:00 am – 12:00 pm PST Supporting Natural Birth and Decreasing Cesarean Birth Rates
November 19 10:00 am – 11:00 am PST How to Create an Effective Patient Safety Evaluation System
December 12 10:00 am – 11:00 am PST Patient Safety Act Case Law under the Patient Safety Act

2019 Annual Conference
October 14 - 15, 2019SacramentoOctober 14 - 15, 2019 Sacramento
https://www.hqinstitute.org/event/2019-hqi-annual-conference

Follow-up Email• Feel free to share articles, tools, policies,
or other resources for fellow members to [email protected]
– We will de-identify your hospital and provider names
• Click here for the survey link – Please share potential topics for future
meetings

Thank You!
• Follow us on Twitter!@CHPSO and @HQInstitute