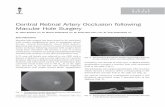
CRAO and BRAO
28
-
Upload
chacha-mashinka -
Category
Health & Medicine
-
view
1.537 -
download
5
Transcript of CRAO and BRAO



Epidemiology
Mean age – mid 60”s
Men > women
Bilateral in 1 – 2%
May have other retinal vascular disease

Etiology Systemic hypertension seen in two thirds of patients
Diabetes mellitus
Cardiac valvular disease seen in one fourth of patients
Cardiac anomalies, such as patent foramen ovale
Embolism
Embolism is the most common cause. The carotid artery and the heart are the most common sources.

There are 3 types of
emboli
1. Cholestrol
Hollenhorst plaques
Minute , bright , refractile,
Golden to yellow orange
crystals, often at
bifurcation

2. Fibrin platelet
Dull grey , elongated
particles which are
usually multiple

3. Calcific emboli
Single , white , non
scintillating particles

PathophysiologyEmboli artery narrowing atheroma turbulent blood flow
break off atheroma lodge small caliber arteryt block
Ischemia Retinal artery occlusion

Characteristics
Sudden severe visual loss in 1 eye
Painless
Retinal appearance
Opaque and edematous
Retina artery narrow,mild hemorrhage
Most prominent in posterior pole
Thickest ganglion cell layer
Cherry-red spot


With time
Artery re-canalizes
Edema clears
Visual loss is
devastating and
permanent
Irreversible damage to
neural tissue after 90
minutes

Diagnosis Ocular examintain
Cardiovascular examination
Labortory studies are helpful / blood sugar , cholesterol , triglycerid /
Carotid ultrasound
Fluorescein angiography
Electroretinogram
ECG and echocardiogram

Dislodge the Embolus
“Burst the Dam”
Digital massage to dislodge embolus
A/C paracentesis
IV acetazolamide
Retrobulbar vasodilators
Inject fibrinolytic in supraorbital artery
Retrobulbar vasodilators
YAG laser embolysis
Surgical embolysis
Keep the Retina Alive
Carbogen inhalation
Oxygen inhalatioN
Hyperbaric oxygen therapy
Emergent TPPV with or without perfluorocarbonliquid infusion

Ocular massage

Sudden profound altitudinal or sectoral VF loss
VA – variable
Fundus – narrowing of arteries and veins with sludging and segmentation of the blood column / cattle trucking , box carrying/
One or more emboli may seen
Cloudy white retina that corresponds to the area of ischaemia.
Sign may sometimes be subtle.

Management is directed toward determining systemic etiology factors. No specific ocular therapy has been found to be effective in improving the visual progmosis.pressureon the globe may dislodge an embolus from a large central vessel toward a more peripheral location , but the efficacy of this maneuver in improving visual outcomes is unknown

Atherosclerosis is
the most common
etiology
but possible causes
include
Eisenmenger
syndrome , giant cell
arteritis , and other
inflammatory
conditions.

A severe form of chronic ischemia of both anterior and posterior segments of the eye as well as other orbital structures supplied by the ophthalmic artery.
Usually unilateral
Age: 50-80 yrs
M&F 2:1

Anterior Segment Dilated Episcleral
vessels Pain in orbit
Corneal edema AC Cells
Iris neovascularisation
NeovasuclarGlaucoma


Proliferative diabetic
retinopathy
Ischemic CRVO
Carotid artery
ultrasoundCarotid occlusion, usually
90% or more
ERG
Diminished b- and a- waves

Full scater PRP
Carotid artery stenting
Endarterectomy


On fundusfluoresceinangiography, there was a delay in arterial filling and AV transit time was 70 sec


fundus fluorescein
angiography showed
normal retinal
perfusion with AV
transit time of 12
seconds
One day after IAT, his
vision improved to
20/40

Fundus photography 2
weeks after
thrombolysis . There is
no more retinal edema