Cranial treatment and the infant - Leon Chaito · 2013-04-22 · The cranial bones are unconnected...
8
This text has deliberately concentrated attention on the adult skull. The skull of the infant, and more so in the neonate by necessity, is immensely malleable, with the pliability of a milk carton. As a mainly cartilaginous structure at birth, the infant skull is ultraresponsive to direct molding pressures. The evolution of the neurocranium, through different growth centers, as well as the main sutural features of the skull and face are shown in Figure A2.1. The cranial bones are unconnected by sutures at birth and some of the cranial bones, known as composite bones (e.g. occiput, sphenoid, temporal) comprise several parts, allowing scope for the rapid growth of the brain (Carreiro 2003). The neo- natal cranium is remarkably soft and unstructured, to allow folding of the cranium as it passes through the birth canal, where it is particularly vulnerable to deformation during the birth process (see Figs A2.2 and A2.3). Cranial distortion can be created by prebirth influences, via trauma (seat-belt compression during an automobile accident, for example) or if the womb is crowded (perhaps by a twin) or if chemical influences distort development (drugs, toxins and/or nutritional deficits). Far more likely to produce damage, however, are the influences of the powerful forces acting upon the supple skull during the birth process. Among the factors which can produce cranial damage during birth are (Biedermann 1992, 2001): 399 Appendix 2 Cranial treatment and the infant APPENDIX CONTENTS The craniocervical link 400 Sleeping position and cranial deformity 401 Other reasons for serious cranial distortion in infants, according to medical authorities 402 What are the long-term effects of deformational plagiocephaly? 402 Different cranial approaches 403 Ear disease and cranial care 404 Conclusion 406 References 406 Appendix 2.qxd 24/03/05 12:53 PM Page 399
Transcript of Cranial treatment and the infant - Leon Chaito · 2013-04-22 · The cranial bones are unconnected...

This text has deliberately concentrated attentionon the adult skull. The skull of the infant, andmore so in the neonate by necessity, is immenselymalleable, with the pliability of a milk carton. As amainly cartilaginous structure at birth, the infantskull is ultraresponsive to direct molding pressures.
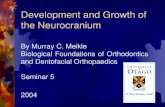
The evolution of the neurocranium, throughdifferent growth centers, as well as the mainsutural features of the skull and face are shown inFigure A2.1.
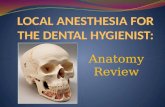
The cranial bones are unconnected by suturesat birth and some of the cranial bones, known ascomposite bones (e.g. occiput, sphenoid, temporal)comprise several parts, allowing scope for therapid growth of the brain (Carreiro 2003). The neo-natal cranium is remarkably soft and unstructured,to allow folding of the cranium as it passesthrough the birth canal, where it is particularlyvulnerable to deformation during the birthprocess (see Figs A2.2 and A2.3).
Cranial distortion can be created by prebirthinfluences, via trauma (seat-belt compressionduring an automobile accident, for example) or ifthe womb is crowded (perhaps by a twin) or ifchemical influences distort development (drugs,toxins and/or nutritional deficits). Far more likelyto produce damage, however, are the influences ofthe powerful forces acting upon the supple skullduring the birth process.
Among the factors which can produce cranial damage during birth are (Biedermann1992, 2001):
399
Appendix 2
Cranial treatment and the infant
APPENDIX CONTENTS
The craniocervical link 400
Sleeping position and cranial deformity 401
Other reasons for serious cranial distortion in infants, according to medical authorities 402
What are the long-term effects of deformationalplagiocephaly? 402
Different cranial approaches 403
Ear disease and cranial care 404
Conclusion 406
References 406
Appendix 2.qxd 24/03/05 12:53 PM Page 399

• too rapid a transit through the birth canalwhich precludes the opportunities for ‘normal’molding to occur
• too extended a period in the birth canal withexcessive compression forces operating on thedelicate membranes, sometimes for many hours(Magoun 1976)
• anomalous prenatal positioning and/orcrowding (as in twins or triplets)
• the application of mechanical force to extractthe infant via inappropriate use of forceps orthe stress of vacuum suction delivery (Noret1993).
As Milne (1995) explains:
A newborn baby has no sutural interlocking orinterdigitation between adjacent cranial bones.The bony plates of the cranial vault are free tofloat like icebergs in an elastic sea of membranousdura. The mechanism of the fontanells, pliantcartilage, tender membrane, open sutures,cerebrospinal fluid and falx and tentorium has
evolved so that what is, evolutionarily, a hugehead can pass through a small birth canal intact.This is achieved by progressive and controlledcranial implosion.
The craniocervical link
Biedermann (2001) suggests that the commondenominator in all of these negative influences isundue mechanical stress impinging on vulnerablecerebral tissues and the craniocervical area. The result may include asymmetrical posture,morphology or movement patterns, as well asinappropriate responses to external stimuli.
Under normal conditions any minor distortionsimposed during birth will resolve as a result of theinfluences of the reciprocal tension membraneswithin a matter of days, greatly assisted by theforces involved in suckling and crying (Frymann
CRANIAL TREATMENT AND THE INFANT400
A
B
C
D
E
FFigure A2.1 The neurocranium increases through variousgrowth centers: (A) the synchondroses in the skull base; (B)the sutures in the cranium. The growing brain (C) is amechanical entity with a stable skull base. (D) The sutures inthe cranium allow movement of the dura mater (E). (F) Thebrain growth is buffered by the skull base and makes thecranium reform at the sutures. (Redrawn from von Piekartz& Bryden (2001) with permission from Elsevier.)
Figure A2.2 Anteroposterior view of the neonatalcranium. The periosteum has been removed from the rightfrontal bone but is still in place on the left. The sutures canbe seen to comprise thickened connective tissue. (Reproducedwith permission from the Willard & Carreiro Collection.)
Appendix 2.qxd 24/03/05 12:53 PM Page 400

1966). In many instances, however, such arecovery is not achieved due to the degree ofdistortion created, with sometimes disastrousconsequences in health terms (Arbuckle 1948,Frymann 1976).
Distortions and deformities are often easilynoted and may be the reason the parent(s) seekassistance. Behavioral problems such as incessantcrying, feeding difficulties, ‘head banging’ orfrank illness might cause parents to attempt tofind appropriate professional help. Clearly if thehealth-care provider consulted is ignorant of theinfluence of cranial function on health, whateveris offered will be less than satisfactory.
After birth the pliability of the infant craniumcontinues to allow damage to occur more easilythan once ossification has taken place. Falls andblows are obvious possibilities, and indeedprobabilities, during the early years of life. If severeenough, these may produce problems similar tothose which can occur during childbirth.
Biedermann (2001) describes what he terms‘KISS’ children in whom the main clinical feature
is torticollis, often combined with an asymmetricalcranium, postural asymmetry and a range ofdysfunctional symptoms (see Fig. A2.4). KISS is anacronym for kinematic imbalances due tosuboccipital strain. Biedermann notes: ‘(KISSimbalances) can be regarded as one of the mainreasons for asymmetry in posture andconsequently asymmetry of the osseous structuresof the cranium and the spine’.
Among the many symptoms reported byBiedermann in KISS children are torticollis,reduced range of head/neck motion, cervicalhypersensitivity, opisthotonos, restlessness, in-ability to control head movement and one upperlimb underused (based on statistical records of 263 babies treated in one calendar year up to June 1995).
Biedermann (2001) is convinced that the mosteffective treatment for such infants is removal ofsuboccipital strain by manual treatment and notdirect treatment of cranial asymmetry, as this isconsidered to be a symptom of the underlyingproblem (most commonly suboccipital strain).Following appropriate treatment to re-establishfull range of upper cervical motion, functionalimprovement is reported to be common within2–3 weeks, although normalization of cranialasymmetry takes many months.
How much treatment is required? According toBiedermann, of the 263 babies treated, 213required only one treatment, 41 were treated twiceand the remainder more often, with just tworequiring 4–5 treatment sessions.
Sleeping position and cranial deformity
One of the reasons for KISS-like problems seemsto relate to infant sleeping position. A researchstudy by plastic and reconstructive surgeons hasconcluded that the almost universal acceptance ofpositioning neonates on their backs to avoid SIDSmay well increase the incidence of abnormalitiesof the occipital cranial sutures, causing significantposterior cranial asymmetry, malposition of the ears,distortion of the cranial base, deformation of theforehead and facial structures (Argenta et al 1996).
The study reported that there had been adramatic increase in the incidence of deformationof the occipital structures, although the patient
Sleeping position and cranial deformity 401
Typical strain pattern
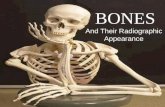
Figure A2.3 Schematic diagram depicting the typicalcone-shaped, rotational strain seen at the sight of vacuumplacement. The depth of extension into deeper tissuesappears to be dependent upon the duration and intensity ofapplication of the device. (Reproduced with permission fromCarreiro 2003.)
Appendix 2.qxd 24/03/05 12:53 PM Page 401

referral base has not changed appreciably. Argentaet al note that the timing of this increase correlatesclosely with the acceptance of recommendedchanges in sleeping position to supine or sidepositioning for infants because of the fear of
sudden infant death syndrome (SIDS). Theyreport that older infants were treated withcontinuous positioning by the parent, keeping theinfant off the involved side, while younger infantsand those with poor head control were treatedwith a soft-shell helmet. Only three of 51 patientshave required surgical intervention and otherpatients demonstrated spontaneous improvementof all measured parameters.
The researchers report:
We believe that most occipital plagiocephalydeformities are deformations rather than truecranio-synostoses. Despite varying amounts ofsuture abnormality evidenced on computed tomo-graphic scans, most deformities can be correctedwithout surgery. In cases where progression ofthe cranial deformity occurs, despite conservativetherapy, surgical intervention should be under-taken at approximately 1 year of age. (Argenta et al1996)
Other reasons for serious cranial distortion ininfants, according to medical authorities
It is reported (Miller & Clarren 2001) thatdeformational plagiocephaly (cranial distortion or‘crooked head shape’) can result from threedifferent etiologic processes.
• Abnormalities in brain shape and subsequentaberrant directions in brain growth
• Premature fusion of a single coronal orlambdoidal suture
• Prenatal or postnatal external constraint.
What are the long-term effects ofdeformational plagiocephaly?
A study was conducted to determine whetherthere was an increased rate of later developmentaldelay in school-aged children who presented asinfants with deformational plagiocephaly, withoutobvious signs of delay at the time of initialevaluation (Miller & Clarren 2001).
A total of 181 families from the medical recordreview were notified about the study and63 families agreed to participate in a telephoneinterview. The sample of participants for thetelephone interview was random to, and
CRANIAL TREATMENT AND THE INFANT402
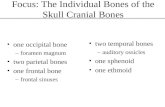
Figure A2.4 Two KISS babies with their cranial asymmetries.Both pictures were taken by the parents and are reproducedhere with their kind permission. They show in both cases aright-convex KISS situation with the accompanying cranialscoliosis, microsomy of the left side of the face, flatteningof the right occipital region and a seemingly asymmetricalpositioning of the ears. All these morphological asymmetriesneed many months to subside. The important sign at thecontrol 3 weeks after the initial treatment is the freemovement of the cervical spine. (Reproduced from vonPiekartz & Bryden (2001) with permission from Elsevier.)
Appendix 2.qxd 24/03/05 12:53 PM Page 402

representative of, the group as a whole. Thefamilies reported that 25 of the 63 children (39.7%)with persistent deformational plagiocephaly hadrequired special help in primary school includingspecial education assistance, physical therapy,occupational therapy and speech therapy, generallythrough an Individual Education Plan. Onlyseven of 91 siblings (7.7%), serving as controls,required similar services. One useful finding wasthat affected males whose deformity was due touterine constraint were at the highest risk forsubsequent school problems.
It was also noted that the use of helmet therapyto correct the distortion (a standard medicalapproach) did not seem to affect the rate of develop-mental delay, almost half of the delayed patientshaving worn helmets (Miller & Clarren 2001).
Different cranial approaches
This text is not an appropriate place in which tooffer precise details of infant cranial care, as themethods needed for application on such delicatestructures need to be learned in closely supervisedclinical and classroom settings. Suffice it to saythat the method of application of cranial mani-pulation in infants is usually direct rather thanindirect, i.e. the barriers of resistance are engagedand molding is applied to normalize distortions,utilizing very gentle and sensitive holdingpatterns.
Biedermann (a physiotherapist, whose work onKISS children is reported earlier in this appendix)applies a direct approach in cervical treatment ofKISS children, using what is described as ‘minimalimpulse manipulation’, commonly in a lateraldirection but with a rotational component in somecases.
We measured the force used in treatment of babiesand adults [and found] the force used for treatingbabies is 15–20% of that used in adults. In mostcases the direction of the impulse is determined byradiological findings (85%). … The manipulationitself consists of a short thrust with minimal forceof the proximal phalanx of the medial edge of thesecond finger.
The amount of force involved, tested with acalibrated pressure gauge, required no more effort
than would be needed to ‘push a bell-buttonenergetically’.
Clinical researchers and authors such as ViolaFrymann (1976) and John Upledger (Upledger &Vredevoogd 1983) record many instances ofsuccess in treating dysfunctional children, somewith severe learning and behavioral problems aswell as a host of physical complaints, utilizingcranial techniques (Upledger 1978). Some researchhas been undertaken, notably by these twopioneers but also by others such as Californianosteopathic physician Carlisle Holland (1991),whose video evidence of the benefits of cranialmanipulation is well worth study.
Holland discusses mainstream methods whichattempt to address infant cranial distortion(largely from a cosmetic perspective). Some of themethods currently employed by orthopedicsurgeons to ‘correct’ cranial distortions involvesurgical removal of plates of bone from the skull,fusion of sutures and the imposition ofirreversible damage to the cranial mechanism. Analternative is to inflict growing infants with thewearing, for years, day and night, of a ‘helmet’which forcibly molds deviant skulls intocosmetically acceptable shapes, with no regard forfunctional integrity (and with an enormousdegree of discomfort).
Visual evidence is available via videos (such asthose produced by physicians such as CarlisleHolland) of the possibility of returning the growingskull to a degree of normality, structurally, withbenefits aplenty in terms of symptom relief, fromassociated wry neck, visual and acoustic problems,as well as behavioral and learning difficulties. Theyounger a baby’s head is treated the better as,once ossification commences, normalizationbecomes more difficult.
Should cranial distortion occur in infancy andchildhood, when plasticity allows for a degree ofmovement not available in the adult skull, inparticular in relation to the sphenobasilar syn-chondrosis (see especially Chs 1 and 2), theresulting distortion patterns, with their associatedsoft tissue imbalances of the reciprocal tensionmembranes in particular, will become ‘set’ andwill be largely impervious to ‘corrective’ treatmentin adult life. Some modification of the associatedstress patterns can still be initiated via cranial and
Different cranial approaches 403
Appendix 2.qxd 24/03/05 12:53 PM Page 403

other therapeutic measures, even in adult life, butrestoration of structural ‘normality’ and symmetrybecomes a virtual impossibility after childhood.
Moving away from cranial distortion to farmore common patterns of ill health affectinginfants leads inevitably to the topic of chronic earinfection.
Ear disease and cranial care
Spermon-Marijnen & Spermon (2001) have treatedmany children with chronic middle ear disease,using cranial techniques. They report that: ‘60children [with otitis media with effusion] wereinspected and treated with passive movements ofthe craniofacial region over the past 6 years; 49children were treated successfully and 11 showedno change’.
These children had been referred by generalphysicians because standard treatments such asinsertion of grommets, paracentesis, surgery and/or antibiotic usage had failed. Spermon-Marijnen& Spermon (2001) suggest that ‘passive movementof the cranium can restore the circulation andmotion by which drainage of the middle ear isstimulated’.
It is worth reflecting that this model of carerepresents one of the therapeutic choices, discussedin Chapter 12, in which the objective is enhancingfunction so that the adaptation load (inflam-mation, congestion, etc.) can be better handled viaenhanced drainage and circulation, with homeo-static/self-regulating mechanisms effecting therecovery.
As discussed in Chapter 12, these clinicianscommence the process of treatment by observation,palpation and motion palpation.
Look at symmetry or deformity, paying specialattention to asymmetry, the orbital line, the levelof ears related to the level of eyes, and themastoids. Palpate the vault and position of thesutures, noting swelling, overlap and mobility.Test the condylar parts of the occiput and examinethe occipito-atlantal mobility.
As has been repeated throughout this book,palpation and motion palpation merge readilyinto treatment: ‘The techniques of passive motiontesting are, in our opinion, also effective as
therapeutic movements, with the application ofadditional or sustained pressure’.
In earlier chapters it has been suggested thattreatment of the adult cranium frequently involvesindirect methods (‘exaggerate distortion’), althoughdirect methods can also be useful (springingmethods, decompression, V-spread, etc.). In contrast,when treating infants, direct approaches are mostcommonly utilized, reflecting the far more pliablenature of the tissues involved.
The following list is a summary of the methodsdescribed by Spermon-Marijnen & Spermon(2001) as relevant techniques used for childrenwith chronic ear conditions. Some of these methods,as well as similar but not identical approaches,have been outlined in previous chapters, mostnotably in Chapters 6 and 7.
1. Transverse movement of the sphenoid. Sittingat the head of the supine patient, one indexfinger and middle finger on the sphenoid andthe other index and middle finger on thecontralateral zygoma and frontal bone,pressure is used to gently shunt the sphenoidinto a translation. Hand positions then reverseand translation to the other side is introduced.In this same opposition rotation of thesphenoid is also achievable. Note: this issimilar to the method described in Exercises6.5a and b and 7.8. See also method 10 inChapter 10, describing Jones’s method fortreatment of the sphenoid tender point.
2. Longitudinal movements of the nasofrontalregion. Standing to the side of the supinepatient, one hand over the crown of the head,the index finger contacts and stabilizes thesupraorbital region on one side, while theother hand uses a pincer contact on thesuperior aspect of the nose to introduce adistraction force. This may be sustained or canrhythmically ‘pump’ the area. One side is treatedand then the other to ‘influence the frontal andmaxillary sinuses’. While not identical, themethods described in Exercises 7.10 and 7.11will achieve similar results.
3. Transverse movement of the zygomatemporaland zygomamaxilla region. The patient issupine and the practitioner is seated at the
CRANIAL TREATMENT AND THE INFANT404
Appendix 2.qxd 24/03/05 12:53 PM Page 404

head. One side is treated at a time. (a) Usingfinger and thumb contacts of each hand, onecontact closer to the zygomamaxilla junctionand the other closer to the zygomatemporaljunction, a gentle distraction/separation isintroduced as the patient’s head is rotatedcontralaterally. (b) Thumb and index finger ofone hand is placed on the zygoma and thesame contacts of the other hand are placed onthe maxilla, allowing distraction that eases thezygoma laterally and cephalad and the maxillamedially and caudad. The distraction is appliedand released synchronous with the breathingof the patient several times. Spermon-Marijnen& Spermon suggest that these methods influencethe maxillary and frontal sinuses. See Exercises6.5c and 7.37 for variations on these approaches.See Figures A2.5 and A2.6.
4. Longitudinal movement of the petrous bone(mastoid lift). The patient is supine and thepractitioner is seated at the head. With fingercontact on the petrous portion of the mastoidbone, rhythmic repetitive longitudinal tractionis applied cephalad, synchronous with breath-ing. This decompression approach is thoughtto influence the craniocervical region. See alsoExercises 7.32 and 7.34 for rhythmic approachesutilizing leverage of the mastoid processes.
5. Rotation of the forehead on hindhead. Theforehead is held with one hand, while the other
cradles the occipital region, to act as astabilizing force. The frontal bone is gentlyrotated clockwise then anticlockwise severaltimes to influence sinus drainage. See also method 9 in Chapter 10, describing Jones’s treatment of the sphenobasilar tenderpoint, which uses similar mechanics (see Fig. 10.10).
6. Distractions of relevant sutures. A gappingpressure is applied at right angles acrosssutures. See Exercise 7.6 for a description of theV-spread technique, as well as method 11 inChapter 10 describing Jones’s treatment of thesquamosal tender point, which distracts theparietal bone from the temporal, gapping thesuture between them (see Fig. 10.10).
7. Opening external auditory meatus. Thepatient is sidelying, head on a firm pillow. Thepractitioner places two fingers of one hand onthe mastoid process and two fingers of theother hand anterior and superior to the externalauditory meatus. A rhythmic separation stretchis introduced, with the patient being asked toeither swallow after each stretch, swallowduring the stretch or perform a Valsalvamaneuver during the stretch (i.e. inhale, holdthe nose and attempt to exhale through thenose, creating increased pressure in the naso-pharynx, in an attempt to open the Eustachiantubes).
Ear disease and cranial care 405
Figure A2.5 Movement of the zygomatemporal region.(Reproduced from von Piekartz & Bryden (2001) withpermission from Elsevier.)
Figure A2.6 Movement of the zygomamaxilla region.(Reproduced from von Piekartz & Bryden (2001) withpermission from Elsevier.)
Appendix 2.qxd 24/03/05 12:53 PM Page 405

CONCLUSION
Cranial treatment of infants differs from themethodology applied to adults in that it usuallyinvolves direct approaches. Pressures used areeven lighter for infants than the gentle methodssuggested for adults. Whether problems aredevelopmental or distortional or treatment isaimed at improving drainage (as in otitis orsinusitis), there are a range of effective treatment
methods, examples of which have been describedin this chapter.
It is essential that appropriate training is undertaken before infants are treated using cranialmethods.
CRANIAL TREATMENT AND THE INFANT406
! CAUTION
REFERENCES
Arbuckle B 1948 Cranial aspect of emergencies of thenewborn. Journal of the American OsteopathicAssociation 47(5): 507–511
Argenta L et al 1996 An increase in infant cranial deformitywith supine sleeping position. Journal of CraniofacialSurgery 7(1): 5–11
Biedermann H 1992 Kinematic imbalances due tosuboccipital strain. Journal of Manual Medicine 31: 92–95
Biedermann H 2001 Primary and secondary cranialasymmetry in KISS children. In: von Piekartz H, BrydenL (eds) Craniofacial dysfunction and pain. ButterworthHeinemann, Oxford
Carreiro J 2003 An osteopathic approach to children.Churchill Livingstone, Edinburgh
Frymann V 1966 Relation of disturbances of craniosacralmechanism to symptomatology of the newborn. A studyof 1250 infants. Journal of the American OsteopathicAssociation 65(6): 1059
Frymann V 1976 The trauma of birth. Osteopathic Annals4(22): 8–14
Holland C 1991 The biophysics of cranial osteopathy(viscoelastic/viscoplastic axes of motion in the cranium).Video Medicine Labs Inc, Scottsdale, AZ
Magoun H 1976 Osteopathy in the cranial field. CranialAcademy, Kirksville, MO
Miller R, Clarren S 2001 Long-term developmentaloutcomes in patients with deformational plagiocephaly.Pediatrics 105(2): 26
Milne H 1995 The heart of listening. North Atlantic Books,Berkeley, CA
Noret R 1993 Craniosacral therapy. In: Chaitow L (ed)Alternative medicine – the definitive guide. BurtonGoldberg Group, Puyallup, Washington
Spermon-Marijnen H, Spermon J 2001 Manual therapymovements of the craniofascial region as a therapeuticapproach to children with long-term ear disease. In: vonPiekartz H, Bryden L (eds) Craniofacial dysfunction andpain. Butterworth Heinemann, Oxford
Upledger J 1978 The relationship of craniosacralexamination findings in grade school children withdevelopmental problems. Journal of the AmericanOsteopathic Association 77(72): 760–776
Upledger J, Vredevoogd J 1983 Craniosacral therapy.Eastland Press, Seattle
von Piekartz H, Bryden L 2001 (eds) Craniofacialdysfunction and pain. Butterworth Heinemann, Oxford
Appendix 2.qxd 24/03/05 12:53 PM Page 406