CQR Breast Cancer · 2018-09-11 · 292 CQ Researcher force (uSpStf) emphasized that each woman...
24
Breast cancer Is mammography being oversold and overused? B reast cancer is the second most common cancer among women in the United States, after skin can- cer, and the second-leading cause of cancer death, after lung cancer. Yet breast cancer mortality rates have been declining, most probably the result of early detection and better treatment. advances in hormone therapy and discoveries of antibody treatments have markedly improved the outcome for breast cancer patients, along with the development of genetic tests on tumor tissue to determine which patients will best benefit from chemotherapy. While progress is being made, some debates seem never to fade. There continue to be disagreements about the age at which women should begin mammography screening, how to treat the increasing number of “zero stage” breast cancers that screening detects and the extent to which environmental pollutants cause breast cancer. In addition, disparities in treatment and racial outcomes continue to be documented. I N S I D E THe I SSUeS ....................291 BacKGROUNd ................298 cHRONOLOGY ................299 cURReNT SITUaTION ........304 aT I SSUe ........................305 OUTLOOK ......................307 BIBLIOGRaPHY ................310 THe NeXT STeP ..............311 T HIS R ePORT Singer/actress Olivia Newton-John, a breast cancer survivor who was diagnosed at age 43, is a critic of a scientific panel’s recent recommendation against routine mammography screening for women in their 40s. An advocate of early detection, she poses with the pink ribbon symbol of breast cancer awareness. CQ R esearcher Published by cQ Press, a division of SaGe www.cqresearcher.com CQ Researcher • April 2, 2010 • www.cqresearcher.com Volume 20, Number 13 • Pages 289-312 RecIPIeNT Of SOcIeTY Of PROfeSSIONaL JOURNaLISTS a WaRd fOR eXceLLeNce ◆ aMeRIcaN BaR aSSOcIaTION SILVeR GaVeL a WaRd
Transcript of CQR Breast Cancer · 2018-09-11 · 292 CQ Researcher force (uSpStf) emphasized that each woman...

Breast cancerIs mammography being oversold and overused?
Breast cancer is the second most common cancer
among women in the united States, after skin can-
cer, and the second-leading cause of cancer death,
after lung cancer. yet breast cancer mortality rates
have been declining, most probably the result of early detection
and better treatment. advances in hormone therapy and discoveries
of antibody treatments have markedly improved the outcome for
breast cancer patients, along with the development of genetic tests
on tumor tissue to determine which patients will best benefit from
chemotherapy. while progress is being made, some debates seem
never to fade. there continue to be disagreements about the age
at which women should begin mammography screening, how to
treat the increasing number of “zero stage” breast cancers that
screening detects and the extent to which environmental pollutants
cause breast cancer. in addition, disparities in treatment and racial
outcomes continue to be documented.
I
N
S
I
D
E
tHe iSSueS ....................291
BacKGRound ................298
cHRonoloGy ................299
cuRRent Situation ........304
at iSSue........................305
outlooK ......................307
BiBlioGRapHy ................310
tHe next Step ..............311
tHiSRepoRt
Singer/actress Olivia Newton-John, a breast cancersurvivor who was diagnosed at age 43, is a critic of ascientific panel’s recent recommendation againstroutine mammography screening for women in their40s. An advocate of early detection, she poses with thepink ribbon symbol of breast cancer awareness.
CQResearcherpublished by cQ press, a division of SaGe
www.cqresearcher.com
CQ Researcher • April 2, 2010 • www.cqresearcher.comVolume 20, Number 13 • Pages 289-312
Recipient of Society of pRofeSSional JouRnaliStS awaRd foR
excellence � ameRican BaR aSSociation SilveR Gavel awaRd

290 CQ Researcher
THE ISSUES
291 • is the value of mam-mography being oversold?• Should “stage zero” cancer be watched andnot treated?• do chemicals in the environment cause breastcancer?
BACKGROUND
298 Radical SurgeryRadical mastectomy was the standard of care for decades in the20th century.
298 Mastectomy to LumpectomyRadiation and simple mastectomy were moreaccepted by century’s end.
301 Non-surgical Break-throughsthe holy grail of treatmentis personalized medicine.
CURRENT SITUATION
304 Task Force Authoritythe new health care lawempowers a panel of pre-ventive medicine experts.
304 Task Force Accountabilityincreased transparencywould quiet some critics.
306 Breast Cancer EducationKey changes were madein a controversial plan.
OUTLOOK
307 Personalized Treatmenta new test marks a treat-ment breakthrough.
SIDEBARS AND GRAPHICS
292 Breast Cancer Hits Whiteand Black Women Hardestasian-americans are the leastaffected.
293 Most Victims Are WomenOver 45nearly 40,000 died frombreast cancer in 2009.
294 A Breast Cancer GlossaryHere are several key breastcancer terms and a list ofthe most common types ofbreast cancer.
299 ChronologyKey events since 1882.
300 Few High-Risk WomenGet Genetic Testingtests can spot genetic muta-tions to genes that suppressbreast cancer tumors.
302 Risk Factors for BreastCancerSome factors are not pre-ventable, such as genetics,and some are, such as recentuse of birth control pills.
303 Do Social Isolation, StressLead to Breast Cancer?experiments with mice andrats suggest a possible link.
305 At IssueShould the courts overturnpatents for genes linked toelevated breast cancer risk?
FOR FURTHER RESEARCH
309 For More Informationorganizations to contact.
310 BibliographySelected sources used.
311 The Next Stepadditional articles.
311 Citing CQ ResearcherSample bibliography formats.
BReaSt canceR
credit: ap photo/Ronald Zak
MANAGING EDITOR: thomas J. [email protected]
ASSISTANT MANAGING EDITOR: Kathy [email protected]
ASSOCIATE EDITOR: Kenneth Jost
STAFF WRITERS: thomas J. Billitteri, marcia clemmitt, peter Katel
CONTRIBUTING WRITERS: Rachel cox, Sarah Glazer, alan Greenblatt, Reed Karaim
Barbara mantel, patrick marshall, tom price, Jennifer weeks
DESIGN/PRODUCTION EDITOR: olu B. davis
ASSISTANT EDITOR: darrell dela Rosa
EDITORIAL INTERNS: dagny leonard, Julia Russell
FACT-CHECKING: eugene J. Gabler, michelle Harris
A Division of SAGE
PRESIDENT AND PUBLISHER:John a. Jenkins
copyright © 2010 cQ press, a division of SaGe.
SaGe reserves all copyright and other rights herein,
unless pre vi ous ly spec i fied in writing. no part of this
publication may be reproduced electronically or
otherwise, without prior written permission. un -
au tho rized re pro duc tion or trans mis sion of SaGe copy -
right ed material is a violation of federal law car ry ing
civil fines of up to $100,000.
cQ press is a registered trademark of congressional
Quarterly inc.
CQ Researcher (iSSn 1056-2036) is printed on acid-
free paper. pub lished weekly, except; (Jan. wk. 1)
(may wk. 4) (July wks. 1, 2) (aug. wks. 2, 3) (nov.
wk. 4) and (dec. wks. 4, 5), by cQ press, a division
of SaGe publications. annual full-service subscriptions
start at $803. for pricing, call 1-800-834-9020. to pur-
chase a CQ Researcher report in print or electronic
format (pdf), visit www. cqpress.com or call 866-427-
7737. Single reports start at $15. Bulk purchase dis-
counts and electronic-rights licensing are also avail-
able. pe ri od i cals post age paid at wash ing ton, d.c.,
and ad di tion al mailing of fic es. poSt maS teR: Send
ad dress chang es to CQ Re search er, 2300 n St., n.w.,
Suite 800, wash ing ton, dc 20037.
April 2, 2010Volume 20, Number 13
CQRe search er
April 2, 2010 291www.cqresearcher.com
Breast cancer
tHe iSSueSn early everyone knows
somebody with breastcancer. Kathy Kivel-
son Hecht of west windsor,n.J., knows two women withthe disease — her sisters.
Her mother died of can-cer in 1989, but doctors couldnot identify the originatingsite. a year later, her 37-year-old middle sister was diag-nosed with breast cancer andopted for a lumpectomy.
“we’d had a very traumat-ic year,” says Kivelson Hecht,who was at her sibling’s bed-side after the surgery, alongwith their older sister. “i wasjust 35, and when the sur-geon walked into my sister’sroom, she insisted he speakto us about our chances ofbreast cancer.”
“He strongly recommend-ed that we go home and talkwith our own gynecologists,”she recalls. She did and hashad annual mammogramsever since.
But seven years later, the middle sis-ter’s cancer spread to her other breast,requiring a mastectomy, and her oldestsister also eventually got breast cancer.
not a year goes by, says KivelsonHecht, that she doesn’t say to herself:“ ‘oK, it’s going to be there.’ But sofar i’ve been lucky.”
changes in dna can cause normalbreast cells to become cancerous. about2 percent of adult women in the unit-ed States inherit mutations that are as-sociated with a high risk of the dis-ease — Kivelson Hecht tested negative— but most dna changes that canlead to cancer are not inherited andoccur in a woman’s breast cells dur-ing her lifetime. 1 (a small number ofmen also get breast cancer.)
Researchers do not know exactlywhat causes those mutations or thealterations in surrounding tissue thatmight allow cancer cells to spread, butthere are known risk factors, includ-ing dense breasts, early menstruationand late menopause, alcohol use, obe-sity and use of menopausal hormonetherapy. (See box, p. 302.)
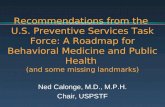
Breast cancer is the most frequent-ly diagnosed cancer in women, nextto skin cancer. (See glossary and a listof common types of breast cancer, pp.294-295.) that’s despite a 2.2 percentdrop in the incidence rate each yearfrom 1999 through 2005 — the mostrecent figures available — after in-creasing for more than two decades.the decline in the incidence rate
may reflect the sharp reduc-tion in the use of hormone-replacement therapy formenopausal women follow-ing a well-publicized reportin 2002 that tied hormonereplacement to increased riskof heart disease and breastcancer. 2 the drop in breastcancer cases may also reflecta small decline in detection,as the percentage of women40 and older who opted formammography declinedfrom 70.1 percent in 2000 to66.4 percent in 2005. 3
Breast cancer is also thesecond-leading cause of can-cer death in women; only lungcancer kills more. yet deathrates from breast cancer havesteadily decreased since 1990,the result of advances in bothearlier detection and improvedtreatment. 4 for instance,drugs have been developedthat help prevent breast can-cer in women at high risk,and therapies that disrupt hor-mones are now prescribed forbreast cancers with hormonereceptors. antibodies have
also been developed to target cancercells with too much of the proteinHer2/neu. finally, genetic testing oftumor tissue is helping oncologistsdetermine which patients will mostbenefit from chemotherapy.
amidst these advances in treatment,however, one thing seems to neverchange: the long-running debate aboutthe efficacy of mammography screen-ing for women in their 40s.
last november, an independent panelof doctors and scientists recommend-ed against routine screening mam-mography for most women in this agebracket, a reversal from its recom-mendation of seven years earlier. inboth announcements, however, the unit-ed States preventive Services task
By BARBARA MANTEL
ass
oci
ated
pre
ss/p
ress
ass
oci
atio
n
A physician examines a mammogram for signs of breastcancer, the most frequently diagnosed cancer in women,next to skin cancer, and the second-leading cause ofcancer death in women. In a controversial move lastNovember, an independent panel of doctors and
scientists reversed its own mammogram advice fromseven years ago and recommended against routinemammography for most women in their 40s.

292 CQ Researcher
force (uSpStf) emphasized that eachwoman should weigh the benefits andharms of screening mammography andmake her own decision. 5
this is not the first time that scien-tists have changed course on breastscreening. in 1987, the national cancerinstitute (nci) recommended that healthywomen, beginning at age 40, should getmammograms every one to two years.in 1993, it dropped that recommenda-tion, only to adopt it again in 1997. witheach switch, confusion and debate fol-lowed. this time was no different.
a media storm erupted almost im-mediately. celebrities lined up to denouncethe task force’s new guidelines, includingsinger/actress olivia newton-John, diag-nosed at 43, who said, “we are not data,we are human beings.” 6 the americancancer Society and the american con-gress of obstetricians and Gynecologistsissued statements continuing to recom-mend screening for women in their 40s,as did the american college of Radiolo-gy, which issued a press release titled“uSpStf mammography recommenda-tions will result in countless unnecessarybreast cancer deaths each year.” 7
even Secretary of Health andHuman Services (HHS) Kathleen Se-belius, to whom the task force re-ports, distanced herself and the obamaadministration from the panel. “theydo not set federal policy, and theydon’t determine what services arecovered by the federal government,”Sebelius said in a statement. “indeed,i would be very surprised if any pri-vate insurance company changed itsmammography coverage decisions asa result of this action.” 8
Gail wilensky, a former official inGeorge w. Bush’s HHS, called Sebelius’sstatement “appalling and outrageousand a very good reminder of how hardit is going to be to move to evidence-based medicine whenever it goesagainst a sacred cow.” 9
meanwhile, several leading women’shealth groups endorsed the task force’srecommendation, including the nationalBreast cancer coalition, Breast canceraction and the national women’s Healthnetwork, all of which had been say-ing for years that the benefits of mam-mograms for younger women havebeen oversold and do not outweigh
the potential harms, such as false pos-itives and unnecessary biopsies.
the timing of the uSpStf an-nouncement further complicated thepublic reaction. a hyper-emotionaland increasingly heated debate wasraging over democrats’ proposedhealth-care reform legislation, and Re-publicans had claimed the plan wouldamount to the rationing of health carebased on cost. in early december,when a subcommittee of the Houseenergy and commerce committeeasked task force members to comeand explain their mammography rec-ommendations, chairman Henry a.waxman, d-calif., felt compelled todefend the uSpStf’s motives.
“while that judgment may be con-tentious, i have no doubt it was drivenby science and by the interpretation ofscience — and not by cost or insur-ance coverage or the ongoing healthreform debate,” waxman said. 10
advocates for african-americanwomen raised particular concerns.“these recommendations completelyignore the impact of well-knownbreast cancer disparities affecting us,”said eleanor Hinton-Hoytt, presidentand ceo of washington-based Blackwomen’s Health imperative. 11 african-american women are more often diag-nosed with breast cancer at a later stagethan whites and also are more likelyto die of the disease.
african-american women — for un-known reasons — account for a dis-proportionate number of “triple nega-tive” breast cancer, a particularlyaggressive form of the disease. But lackof medical coverage, barriers to earlydetection and screening and unequalaccess to treatment may also contributeto black women’s higher mortality rate,according to the nci. 12
for instance, a recent study showedthat black women are less likely thanwhite women to receive radiation ther-apy after a lumpectomy, the standardof care for early stage breast cancer.the authors did not know if fewer
BReaSt canceR
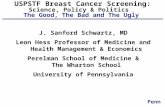
White and Black Women Are Hit Hardest
While white women have the highest incidence of breast cancer, African-American women have the highest mortality rates. Asian-American women are the least affected, with a mortality rate of a little more than a third of that of black women.
Source: “Breast Cancer Facts and Figures 2009-2010,” American Cancer Society
Female Breast Cancer Incidence andMortality Rates by Race and Ethnicity
(U.S., 2002-2006)
0
30
60
90
120
150
American Indian/Alaskan Native
Hispanic/Latina
Asian-American/Pacific Islander
African-American
White
(Rate per 100,000)
123.5
23.9
113.0
33.0
81.6
12.5
90.2
15.5
91.7
14.3
Incidence
Mortality

April 2, 2010 293www.cqresearcher.com
black women are receiving radiation“simply because it is not offered tothem, because they decline the treat-ment or perhaps because they are un-able to complete a whole course oftreatment due to other health prob-lems.” 13 more studies are needed,they said.
Here are some of the questions thatbreast cancer sufferers, physicians, re-searchers, advocacy groups and politi-cians are debating:
Is mammography oversold?early detection is the key to sav-
ing the lives of cancer victims.that’s been the message from muchof the medical community fordecades. But research is calling thatnotion into question.
physicians are debating the useful-ness of prostate cancer screening formiddle-aged men, and new guidelinesfor cervical cancer screening now saywomen should start having papsmears at age 21; the medical com-munity had previously recommendedyoung women start screening threeyears after beginning to have inter-course, even if a teenager. 14 But per-haps most contentious of all was lastnovember’s recommendation by theinfluential united States preventiveServices task force (uSpStf) that mostwomen under 50 should no longerhave routine breast cancer screeningand that women between 50 and 74should no longer have mammogramsevery year but rather every other year.the new recommendation does notapply to the small number of womenwho are at high risk for the disease.
the task force’s guidelines are in-tended to reduce potential harms fromscreening, like overtreatment of non-invasive cancer and the anxiety andunnecessary biopsies that result fromfalse positives.
But the uproar that erupted imme-diately following their release caughtthe task force and its supporters bysurprise.
“i’m not sure why it created sucha firestorm,” says fran visco, presidentof the national Breast cancer coali-tion. “i was taken aback.” Her groupsupports the task force’s findings and,like several other women’s health or-ganizations, has been vocal for yearsabout the limitations of screening mam-mography for younger women.
opposition to the task force’schange of course ranged from mea-sured to outraged. “this is one screen-ing test i recommend unequivocally. . . to any woman 40 and over, beshe a patient, a stranger or a familymember,” said otis Brawley, the amer-ican cancer Society’s chief medicalofficer, who also acknowledged thatreasonable experts can disagree. 15
the american congress of obstetri-cians and Gynecologists said it “main-tains its current advice” that womenin their 40s continue mammographyscreening 16 while the american So-ciety of Breast Surgeons “strongly op-posed” the new guidelines. 17 andthe american college of Radiologysaid flatly if the guidelines became
policy, “countless american womenmay die needlessly from breast can-cer each year.” 18
perhaps the angriest challenges camefrom individual women, like GenaKnutson, a 13-year breast cancer sur-vivor diagnosed at age 35, who wrotea letter to the editor of her local news-paper: “with my history, you canimagine my shock regarding the fed-eral recommendation that mammo-grams before age 50 are not medicallynecessary. this recommendation putslives at risk.” 19
task force members believe theirtrue message got obscured in the mediastorm. “if you really look at what thetask force was saying in 2002 [the lasttime it issued guidelines], it’s not a lotdifferent from what they were sayingin 2009,” says Russell Harris, a pro-fessor of medicine at the university ofnorth carolina in chapel Hill and aformer task force member.
in 2002, the task force had rec-ommended that women get screenedevery one to two years beginning atage 40, but it went on to say that the
Most Victims Are Women Over 45
An estimated 40,000 women died from breast cancer in 2009, and more than 192,000 invasive cases were diagnosed.
Source: “Breast Cancer Facts and Figures 2009-2010,” American Cancer Society
Estimated New Female Breast Cancer Cases andDeaths by Age Group, 2009
Age In situ Invasive Deaths cases cases
Younger than 45 6,460 18,640 2,820
45 and older 55,820 173,730 37,350
Younger than 55 24,450 62,520 8,890
55 and older 37,830 129,850 31,280
Younger than 65 40,940 120,540 17,200
65 and older 21,340 71,830 22,970
All ages 62,280 192,370 40,170

294 CQ Researcher
precise age at which the benefits (areduced death rate) justify the poten-tial harms (false positive results andunnecessary biopsies) is a “subjectivejudgment” and that clinicians shouldtell women that the balance improveswith age. in other words, women shouldmake up their own minds.
“But very few people read or tookto heart that message,” says Harris,“and because of that, organizationsand physicians assumed the task forcesaid screen everybody over 40, and
that’s not really what they said.”So in 2009, after reviewing the data
again, the task force decided to change“the tone” of its recommendation, ac-cording to Harris, saying it could nolonger recommend screening for womenin their 40s but continuing to stress thatthe judgment was subjective and up toeach individual and her doctor.
Some of the panel’s critics said taskforce members underestimated the po-tential benefit of screening mammog-raphy. the panel ignored information
from more recent population-basedstudies, says carol lee, a radiologistat memorial Sloan Kettering cancercenter in new york city and the chairof the american college of Radiolo-gy’s commission on Breast imaging.“where the older, randomized trialsshowed a 15 percent reduction inmortality with screening for womenin their 40s, the newer population tri-als show a 30 to 40 percent reduc-tion in mortality.”
Randomized controlled clinical trialsenroll patients and then randomly as-sign them to various treatments, fol-lowing up for years to determine theresults. population studies compare dif-ferent parts of a country with differentmammography rates, and if there is achange in mortality in one area versusanother, they attribute it to screening.
Harris says that the new populationstudies were taken into account butthat they are “methodologically weak.”for instance, there could be manyother differences between the twogroups aside from screening that couldaccount for variations in mortality.
lee and other critics of the task forcealso say it overstated the potential harmsfrom screening mammography. it’s truethat 1,900 women in their 40s need tobe screened for 10 years in order toprevent one cancer death, and morethan 1,000 false positive results will begenerated in the process, leading tosome unnecessary biopsies. 20 But leepoints to studies showing that the anx-iety from receiving a false positive isshort-lived. “and biopsy these days ismuch less invasive than it used to be,”says lee. “a needle biopsy can take aslittle as 15 minutes.”
But vasco says biopsies create scartissue, which can mask problems thatwould show up in a mammographylater, “when women are supposed tohave routine screening in their 50s.”
Besides false positives, the task forcesaid that the increasing use of mam-mography has also resulted in thediagnosis and treatment of cancers that
BReaSt canceR
A Breast Cancer Glossary
Here are key breast cancer terms and a list of the most common types of breast cancer. Many other types of less common breast cancer are not listed here. Sometimes a breast tumor can be a mix of these types or a mixture of invasive and in situ cancer.
Understanding Key TermsAdenocarcinoma — A type of cancer that starts in gland tissue (tissue that makes and secretes a substance). The ducts and lobules of the breast are gland tissues because they make breast milk, so cancers starting in these areas are often called adenocarcinomas.
Breast lumps — Most breast lumps are benign (not cancerous). Benign breast tumors are abnormal growths, but they do not spread outside of the breast and are not life threatening. But some benign lumps can increase the risk of getting breast cancer. Most lumps are caused by fluid-filled sacs known as cysts, which can cause breast swelling and pain. They often happen just before a woman’s period is about to start. The breasts may feel lumpy, and sometimes there is a clear or slightly cloudy nipple discharge.
Carcinoma — A cancer that begins in the lining layer of organs such as the breast. Nearly all breast cancers are carcinomas (either ductal carcino-mas or lobular carcinomas).
Carcinoma in situ — The early stage of cancer, when it is still only in the layer of cells where it began. In breast cancer, in situ means that the cancer cells are only in the ducts or lobules and have not spread into deeper tissues in the breast or to other organs. Sometimes called non-invasive or pre-invasive breast cancers.
Duct — Small tubes in the breast that carry milk to the nipple.
Invasive (infiltrating) carcinoma — A cancer that has already grown beyond the layer of cells where it started. Most breast cancers are invasive carcinomas — either invasive ductal carcinoma or invasive lobular carci-noma.
Lobule — Glands that make breast milk.
Sarcoma — Sarcomas are cancers that start from connective tissues such as muscle tissue, fat tissue or blood vessels. Sarcomas of the breast are rare.

April 2, 2010 295www.cqresearcher.com
would never have become invasive andof slow-growing cancers that wouldnot have shortened a woman’s life.
and while the magnitude of over-diagnosis is unknown, Harris says, itis not trivial, as task force critics claim.“it is not zero, and it may be as muchas 20 to 25 percent of all the breastcancers diagnosed,” he says. 21
to date, the new guidelines do notseem to have had an impact on in-surance coverage, but it has openedup a divide between doctors and pa-tients, if a recent survey in the An-nals of Internal Medicine is any indi-cation. most doctors who respondedsaid they would no longer offer rou-tine screening to women in their 40s,while most women who respondedsaid they would not give up their an-nual mammogram. 22
“what this whole debate under-scores is the urgent need to come upwith better screening tools,” says ericwiner, director of the breast oncolo-gy center at the dana-farber cancerinstitute in Boston. if oncologists bet-ter understood who is most at risk,he says, then mammograms and mRis[magnetic resonance imaging] couldbe devoted to those women. “whenyou do that, the false positives godown, and the true positives go up.”
Should “stage zero” cancer bewatched and not treated?
the increase in mammographyscreening since the late 1970s has ledto a surge in diagnoses for ductal car-cinoma in situ (dciS), a kind of breastcancer rarely seen before 1980 but thatnow accounts for about 25 percent ofall breast cancers diagnosed. 23
individual dciS cells look just likeinvasive cancer under a pathologist’smicroscope, but unlike invasive can-cer they are confined to the inside ofthe milk ducts. Some doctors call dciS“zero stage” breast cancer, and the sur-vival rate is high: ten years after di-agnosis, 96 to 98 percent of womenare alive. 24
However, the disease is typically treat-ed much like early-stage invasive breastcancer — with a lumpectomy and ra-diation or even a mastectomy and oftenhormone treatment. and that bothersmany clinicians and researchers.
many dciS patients do not needtreatment since a significant numberof cases will never progress to inva-sive cancer. analysis of autopsy resultsand studies of dciS that were missedat biopsy “suggest that the lifetime riskof progression must be considerablyless than 50 percent.” 25 that meansthousands of women each year are
actually harmed by treatment, suffer-ing disfiguring surgery and the sideeffects of radiation and hormone treat-ment for no reason, most oncologistsagree. the problem is that physicianshave no sure way of distinguishing be-tween the dciS cases that will remaindormant and those that will spread.
with so much uncertainty, dciS pa-tients tend to overestimate their riskof invasive breast cancer, one studyshowed, and suffer unnecessary anxietyas a result. “you think you’re going todie,” said 40-year-old Barbara laufer,a woman from Burbank, calif., who
Source: American Cancer Society, Sept. 29, 2009
Major Types of Breast CancerDuctal carcinoma in situ (DCIS) — The most common type of non-invasive breast cancer, where the cancer is only in the ducts and has not spread into the breast tissue. Nearly all women with cancer at this stage can be cured. Often the best way to find DCIS early is with a mammo-gram. If there are areas of dead or dying cancer cells (called tumor necrosis) within the biopsy sample (when tissue is taken out to be looked at in the lab), the tumor is likely to grow and spread quickly (become more aggressive).
Lobular carcinoma in situ (LCIS) — Begins in the milk-making glands (lobules) but does not go through the wall of the lobules. It is not a true cancer, but having LCIS increases a woman’s risk of getting cancer later, so it’s important that women with LCIS should have regular mammograms and doctor visits.
Invasive (or infiltrating) ductal carcinoma (IDC) — The most common breast cancer, it starts in a duct, breaks through the duct wall and invades the tissue of the breast. From there it may spread (metastasize) to other parts of the body. IDC accounts for about eight out of 10 invasive breast cancers.
Invasive (infiltrating) lobular carcinoma (ILC) — Starts in the milk glands (lobules) and can spread (metastasize) to other parts of the body. About one out of 10 invasive breast cancers are ILCs.
Inflammatory breast cancer (IBC) — An uncommon type of invasive breast cancer that accounts for about 1 percent to 3 percent of all breast cancers. Usually there is no single lump or tumor. Instead, IBC makes the skin of the breast look red and feel warm. It also makes the skin look thick and pitted, something like an orange peel. The breast may get bigger, hard, tender or itchy. In its early stages, IBC is often mistaken for infection. Because there is no defined lump, it may not show up on a mammogram, which may make it even harder to catch it early. It usually has a higher chance of spreading and a worse outlook than invasive ductal or lobular cancer.

296 CQ Researcher
was diagnosed with dciS three yearsago and had two lumpectomies andradiation and is taking the hormonetreatment tamoxifen. 26
Some physicians have proposedchanging the name and removing theword “carcinoma” to reduce that anx-iety. “cancer usually implies invasion,and dciS is specifically not invasive,”says carmen allegra, chair of a na-tional institutes of Health panel ondciS and chief of hematology andoncology at the uni-versity of florida’sShands cancer cen-ter. “to call it can-cer is probably anoverstatement.”
“you could re-name it , for in-stance, in ductalintra-epithelial neo-plasia,” says StephenBauer, president ofthe college of amer-ican pathologists anddirector of laborato-ries at mercy SanJuan medical center,near Sacramento,calif. “it’s been donewith cervical cancer.”cervical intraepithe-lial neoplasia is thelabel now used in-stead of carcinomain situ.
But the biggest harm is not anxietybut overtreatment, and a few physicianspropose scaling back therapy.
“i’ve come to a very different ap-proach to talking to patients with dciS,”says Shelley Hwang, a breast surgeonat the university of california, San fran-cisco, “and it’s more of an evaluationof tradeoffs. So i present as one op-tion active surveillance.” that includesa mammogram every six months, pos-sibly alternating with an mRi, and nosurgery and no radiation. “But the pa-tient has to know that the possibilityof having invasive cancer will increase,”
explains Hwang, “although with sur-veillance the likelihood is that theywould have a curable cancer. Hwangacknowledges that she is “definitelyon the fringe” when it comes to herapproach to dciS treatment.
“it would be hard to not at leastintervene surgically,” says allegra.
pat whitworth, a breast surgeon innashville, tenn., and former chairmanof the board at the american Societyof Breast Surgeons, says he would con-
sider active surveillance only rarely,with the following hypothetical patient:“She’s physiologically elderly and frail.She’s not going to tolerate a haircutwell let alone a surgical procedure, andthe biopsy appears to have removedthe problem, and it was low-grade dciS.”But most of his patients would still optfor a little more surgery, whitworth says.
Hwang says 90 percent of her pa-tients also opt for some surgery. Butmary Jane lapinski did not. the 55-year-old, single woman from northernvirginia was diagnosed with dciS sevenyears ago. Because she had dciS in
two locations, her surgeon recom-mended a mastectomy. “it was mind-boggling,” she says. “i’m thinking,‘How can you tell me that i need amastectomy for a noninvasive cancerwhen women with invasive cancer aregetting lumpectomies?’ it truly did notmake any sense to me at all.”
lapinski went on the internet, whereall she read pointed to mastectomy,and she was about to schedule hersurgery when she came across an ar-
ticle about a study con-ducted by Hwang. inthe study, dciS patientswhose cancer cells haveestrogen receptors weregiven the hormone treat-ment tamoxifen forthree months before sub-mitting to surgery.
lapinski flew to Sanfrancisco, signed up,and after three monthsand a discussion withHwang about the prosand cons, opted to nothave surgery and toleave the study. She re-mains on tamoxifen andreturns to San francis-co every six months foran mRi. “over the years,the whole area in mybreast that was affectedhas shrunk significant-ly,” says lapinski.
Hwang published the results of thestudy last year, reporting that cancercells under the microscope look shriv-eled, and tissue markers that show howfast cells are dividing indicated that thegrowth rate had slowed down. 27 “itdoesn’t happen to the same extent inall patients, but it does happen to somepatients big time,” says Hwang. thosepatients may benefit from longer-termhormonal therapy instead of surgeryand instead of just pure active surveil-lance, she says. Hwang is also plan-ning a study of six months of hor-monal treatment before surgery.
BReaSt canceR
Cancer survivors sit for a portrait in pink before the annual KomenRace for the Cure in Tyler, Texas. Susan B. Komen for the Cure is a leading national grassroots advocacy organization
that raises money for breast cancer research.
ap p
hoto
/Tyler Morning Telegraph
/d.J. pet
ers

April 2, 2010 297www.cqresearcher.com
what would it take for other breastsurgeons to consider discussing activesurveillance with their dciS patients?whitworth says he would need to seea published study of post-menopausalwomen randomized to either standardtreatment or active surveillance andfollowed afterward for five to 10 years.if data on recurrence and mortality“were fairly comparable, then i thinkwe would see some shifting in treat-ment,” he says.
Do chemicals in the environmentcause breast cancer?
there is no single cause of breastcancer. yet understanding the etiolo-gy of this complex disease is essen-tial to understanding how to preventit. while 5 to 10 percent of breast can-cer cases are thought to be hereditary,the majority of women who developthe disease will never know why.
Scientists have identified certain riskfactors, like early menstruation and latemenopause, alcohol consumption andobesity, but “most of these risk factorsaccount for very small increases or de-creases in a woman’s chances of de-veloping breast cancer,” according tothe national Breast cancer coalition. 28
environmental chemicals may playa role, say some researchers, by dam-aging dna, by mimicking hormonesthat signal tumor cells to grow or byaltering mammary gland develop-ment early in life. they say the sizeof the dose may not be what mat-ters most but how early in life andfor how long the exposure occursand to whom; some women may bemore susceptible than others. “Breastcancer rates increased enormouslyover the decades since world war iiat the same time that we have hadincreasing exposure to a wide vari-ety of chemicals and radiation in theenvironment,” says Janet Gray, direc-tor of the program in science, tech-nology and society at vassar collegein poughkeepsie, n.y., who wrote anextensive review of the research on
breast cancer and the environmentfor the Breast cancer fund, an ad-vocacy group in San francisco, calif.
But correlation does not prove alink. for that, scientists turn to ani-mal and human studies. one team ofresearchers reviewed hundreds of an-imal studies and found that 216chemicals have been shown to causemammary gland tumors, mostlythrough dna mutations. there couldbe many others, since only a smallfraction of the more than 80,000 chem-icals used in the united States todayhave been tested in animals for car-cinogenic potential. 29
“the laboratory evidence is verystrong that there are environmentalchemicals that affect biological process-es linked to breast cancer,” says JuliaG. Brody, who participated in the re-view of chemicals and is the execu-tive director of the Silent Spring insti-tute in newton, mass., which researchesthe environment and women’s health.the chemicals include benzene, foundin gasoline; polycyclic aromatic hy-drocarbons, found in vehicle exhaust,air pollution, tobacco smoke andcharred foods; methylene chloride, acommon solvent in paint strippers andglues; and some pharmaceuticals, likefurosemide, a diuretic, and griseofulvin,an anti-fungal. 30
most of the 216 chemicals alsocaused tumors in multiple organs, notjust mammary tissue, and in multiplespecies of animals. “these character-istics are generally believed to indi-cate likely carcinogenicity in humans,”Brody’s team reported. 31
a growing number of animal stud-ies also implicate endocrine-disruptingcompounds (edcs) — found in cer-tain plastics, pesticides, flame retar-dants and personal care products —which mimic or block hormones. “thereare literally hundreds of studies demon-strating that low doses of endocrinedisruptors in early development haveprofound effects on mammary tissue,breast development and incidence of
breast cancer, especially in a varietyof rodent models,” says Gray. 32
But extrapolating from animal stud-ies to the human experience is tricky.“we’re on very thin ice inferring fromanimal models that there’s a high prob-ability that a chemical is a carcinogenin humans,” says david Hunter, a pro-fessor of epidemiology at Harvard uni-versity in cambridge, mass. “there isa relatively low correlation betweenexposures that cause cancer in ani-mals and those exposures causing can-cer in humans,” says Hunter. “and ifthere is a relationship, it’s a differenttype of cancer in the human com-pared to the animal.”
the gold standard would be humanstudies, but there haven’t been many,and most that have been done havenot found a link. perhaps that’s be-cause human studies have mostly mea-sured levels of a single chemical inadult women, while the critical peri-od of exposure might be puberty, orearly childhood, or even in utero. inaddition, it might be exposure to amix of chemicals that is important.
But it is extremely difficult to studyearly exposure to multiple chemicals.most people don’t know what chem-icals they are exposed to now, letalone decades ago. and when inter-viewing women with breast cancer,“How do you know the diagnosis it-self isn’t influencing their recall ofevents?” asks James lacey, a cancerepidemiologist at city of Hope, a com-prehensive cancer center in duarte,calif. “people want to put a narrativeto their experiences,” he says. Re-searchers also may not be able to findan unexposed control group, sincemany chemicals are pervasive. and fi-nally, chemicals may increase breastcancer risk only for women with cer-tain genetic mutations.
instead, some researchers havecombed through state environmentaldata and medical records looking forreliable information. one group foundblood samples taken from young

298 CQ Researcher
women at the time they gave birth,measured their levels of the pesticideddt, and then followed the womenfor two decades. early exposure toddt was associated with a fivefoldincrease in risk of developing breastcancer before age 50. 33 ddt, thoughbanned in 1972, continues to linger inthe environment.
“that is an important study, and itprovides the kind of evidence that isvery difficult to get,” says Brody.
four human studies show higherbreast cancer risk from exposure topolychlorinated bipheyls (pcBs) inwomen with a gene mutation thataffects how they metabolize thesenow banned chemicals that wereonce used in electrical equipment,but still linger.
But Hunter cautions that no singleepidemiological study is definitive.“we only accept something as likelyto be causal if the majority of studiespoint in the same direction,” he says.Brody also calls the number of humanstudies sparse and says there are “hugeknowledge gaps.”
experts say more chemicals must betested — both in the lab and in ani-mals and in forward-looking humanstudies — not dependent on memory.for instance, the federal national chil-dren’s Study will examine the effects ofenvironmental influences on the healthand development of 100,000 childrenin the united States, following themfrom before birth until age 21. 34
“However, that doesn’t help us rightnow,” says Gray. that’s why she andBrody both advocate relying on theanimal data to propel action in theshort term. “i don’t think most fami-lies want to take unnecessary riskswith their daughters,” says Brody. aprogressive policy, she says, would ac-knowledge that we know enough nowto start reducing those exposures.
for michael thun, emeritus vicepresident of epidemiology and sur-veillance at the american cancer So-ciety, it’s not so clear. “the precau-
tionary principle says that if you havesome evidence you should take ac-tion — you don’t need conclusive ev-idence — but the question that re-mains unresolved is where do youdraw the line?” says thun.
Brody says the u.S. should look toeurope and canada for a model ofhow to implement the precautionaryprinciple. these countries have devel-oped systematic programs for assess-ing the health consequences of syn-thetic chemicals — both old and new— as a prerequisite for use. 35
BacKGRoundRadical Surgery
i n the late 19th century, the amer-ican surgeon william Stewart Hal-
sted offered “an alternative, a choice,a possibility for breast cancer patientsin a surgical world bereft of hope,”writes James S. olson in his bookBathsheba’s Breast: Women, Cancer &History. 36 at the time, women, terri-fied of a breast cancer diagnosis,typically delayed consulting a doctor,who would then not see the canceruntil it was large and often inopera-ble. when they did operate, tumorsoften returned, and most women dieda brutal and painful death.
Halsted believed that cancer slowlyspread through the body’s lymphatic sys-tem, and he embraced the technique ofremoving lymph nodes during cancersurgery. But he also knew that cancerwas a cellular disease, and he worriedthat “a careless surgeon who cut intothe tumor with the scalpel, lifted thebreast away with his hands, then . . .scooped out lymph nodes with hisfingers probably scattered tumor cellsall over.” 37 using the hands this waywas advised in textbooks and wascommon practice at the time.
instead, in the early 1890s Halstedcalled for removing the breast, lymphnodes and chest muscles in a singleprocedure, “cutting widely aroundthe tumor, removing all the tissue inone piece.” 38
over the next two decades, Hal-sted, his students and colleagues per-formed tens of thousands of theseradical mastectomies, and Halstedbegan to collect a database on the210 surgeries he himself had per-formed. of the 60 women whosecancer had not spread to the lymphnodes, more than 85 percent werealive three years later. of the 110women whose cancer had spread tothe lymph nodes, just 31 percent sur-vived for three years. and for the 40women with cancer in more remotelymph nodes, only 10 percent sur-vived that long.
olson writes that Halsted’s con-clusion was clear: “women who re-ceived a radical mastectomy beforethe tumor spread to regional lymphnodes had excellent odds. womenwho de layed t rea tment weredoomed.” 39 Halsted’s results laid thefoundation for a massive campaign70 years later for early detectionthrough mammography.
Mastectomy to Lumpectomy
B ut radical mastectomy was dis-figuring and at times led to per-
sistent pain and arm swelling knownas lymphedema. as surgeons gainedan appreciation of its side effectsand learned more about the biolo-gy of cancer, the procedure attract-ed critics.
among the most vocal was englishphysician Geoffrey Keynes, who ques-tioned Halsted’s basic assumption —that breast cancer “spread slowlythrough the lymph nodes, hypothe-sizing that the disease in fact entered
BReaSt canceR
Continued on p. 300

April 2, 2010 299www.cqresearcher.com
chronology1800s Surgical tech-niques are refined; radiationis introduced.
1882american william Stewart Halsteddevelops the radical mastectomy.
1896chicago physician emil Grubbetreats breast cancer patients withx-rays. . . . Scotsman thomas Beat-son reports that removing ovariesresults in improvement of breastcancer patients, laying foundationfor modern hormone therapy.
•
1930s-1970sAdvances are made in breastcancer treatment and diagnosis.
1939congress establishes national cancerinstitute (nci).
1969mammography machines introduced.
1975-76Studies demonstrate that adjuvantchemotherapy — treatment aftersurgery — prolongs survival forbreast cancer patients.
1978tamoxifen is approved as adjuvanttherapy to prevent cancer recurrence.
•
1980s-1990sScientists begin to understandthe genetics of breast cancer;mammography debate begins.
1980-83Studies show combining treatments,
like chemotherapy and radiation,helps certain breast cancers, chang-ing the standard of care.
1987nci and the american cancer Soci-ety (acS) recommend that beginningat age 40, women should beginscreening every one-to-two years.
1990national institutes of Health (niH)says lumpectomy plus radiation isas effective as mastectomy.
1992Study finds no evidence that low-fat or high-fiber diets protectagainst breast cancer. . . . taxol,derived from yew tree bark, is ap-proved to treat breast cancer afterother drugs have failed.
1993nci drops its recommendation thatwomen in their 40s get mammo-grams, saying no clear scientificevidence exists that regular screen-ing reduces risk of dying; acScontinues to recommend screeningfor women in their 40s.
1997mutations to the BRca1 and BRca2tumor-suppressing genes are linkedto high lifetime chance of develop-ing breast cancer. . . . after review-ing updated screening studies, ncireverses course and recommendsmammograms for women in their40s every one-to-two years.
1998daily tamoxifen treatment isshown to reduce the incidence ofinvasive breast cancer by 45 per-cent and noninvasive breast cancerby 50 percent in high-risk women.. . . food and drug administration(fda) approves an antibody forwomen with certain types ofmetastatic breast cancer.
2000-PresentGenetic tests of breast tumorsare developed while mammog-raphy debate continues.
2002Hormone replacement therapy forpostmenopausal women is shownto increase the risk of breast can-cer and increase the odds of heartattack, stroke and blood clots.
2002u.S. preventive Services task force(uSpStf) recommends routinemammography for women in their40s every one-to-two years, empha-sizing that each woman mustweigh potential benefits and harms.
2002-2004test for gene activity in breasttumor tissue is shown to predictrecurrence likelihood and benefitof chemotherapy.
2005Herceptin is shown to cut risk oftumors returning in women withearly stage HeR2-positive breastcancer by 50 percent; approvedfor this use in 2006.
2007Studies describe common variationsin dna sequences associated withsmall increased breast cancer risk.
November 2009after reviewing studies about falsepositives and overtreatment of non-invasive breast cancer, uSpStf nolonger recommends routine mam-mography for women in their 40s.the task force also says thatwomen between 50 and 74 shouldhave mammograms every otheryear rather than every year andrecommends against breast cancerself-exams because harms, like falsepositives, outweight the benefits.

300 CQ Researcher
the bloodstream and spread through-out the body early in its course,” writesBarron lerner, in The Breast CancerWars. 40 if this were true, then re-moving lymph nodes would not re-duce mortality.
other critics suggested that themortality of breast cancer patients de-pended less on early detection andsurgery than on the innate aggres-siveness of the cancer itself. one newyork surgeon wrote that “cures de-pend . . . on a mystical somethingthat pathologists are now exploringand which is spoken of as the biolo-gy of the tumor.”
By the late 1920s, a few of thesecritics had begun to argue that radia-tion, “either by itself or accompaniedby surgical removal of the tumor orbreast alone, was as or more effective
than radical mastectomy.” Studies beganto show survival rates comparable toradical mastectomy. 41
yet radical mastectomy remained thestandard of care for decades. in fact fol-lowing world war ii and the develop-ment of potent antibiotics that prevent-ed postoperative infections, a few surgeonswent “superradical.” university of min-nesota surgeon owen H. wangensteenbelieved that breast cancers that hadreached the lymph nodes required evenmore aggressive surgery, which entailed“the splitting of a patient’s clavicle, ribsand sternum (breast bone) in pursuit ofcancer cells,” writes lerner. 42
meanwhile, more voices were chal-lenging the notion of early treatmentand curability, including biometricianswho studied the statistical record.these new studies claimed, like thefew lone voices 20 years earlier, that
the biology of each breast cancerdetermined a woman’s chances ofsurvival. for instance, a canadianbiometrician, neil mcKinnon, pub-lished studies showing that breastcancer mortality in ontario, england,wales, denmark and five u.S. stateshad remained stable from 1909 to1947, despite surgery and greaterpublic awareness of the benefits ofearly intervention, thanks to publicityby cancer societies. 43
By the late 1950s, many researchersbegan to argue that the only way tocompare the efficacy of differentbreast cancer therapies was to con-duct randomized controlled clinicaltrials, which many surgeons interpret-ed as a direct assault on their authorityand expertise. Roald Grant, a surgeonwith the american cancer Society, com-pared physicians who relied on such
BReaSt canceR
Continued from p. 298
Karen Kramer, a 45-year-old mother of three in mary-land, spent most of her adult life worried about breastcancer. “for me, it was not if i get it but when i get
it,” she says. three generations of women on her father’s sidehave had the disease, and her mother’s sister as well.
fifteen months ago, a mammography technician told Kramerthat she had dense breasts, making detection more difficult. al-ready nervous about her family history, Kramer asked for ad-vice, and the technician recommended a genetic counselor. Kramerwent the same day and soon chose to be tested for harmfulmutations in two tumor-suppresor genes, BRca1 and BRca2.
about 60 percent of women who have inherited BRca mu-tations will develop breast cancer, compared to 12 percent ofwomen in the general population. and 15 to 40 percent willdevelop ovarian cancer, compared to less than 2 percent ofmost women. 1
But the dreaded mutations are rare. “if you are looking atnon-Hispanic whites in the u.S., 1 in 800 carries a mutation,”says oncologist marc Robson, clinic director of the clinicalGenetics Service at memorial Sloan-Kettering cancer center innew york. But for women of ashkenazi Jewish descent, likeKramer, the chance is much higher: 1 in 40.
three weeks after testing, Kramer sat in an oncologist’s of-fice with the counselor as they opened the results. “when they
said it was positive, the oncologist handed me tissues,” re-counted Kramer. “and i said, ‘you know what, i don’t needtissues.’ Honestly, i have not cried about it. i’m actually grate-ful because now i have choices.”
the american Society of clinical oncology (aSco) recom-mends testing for BRca1 and BRca2 mutations only if an in-dividual has “a personal or family history suggestive of genet-ic cancer susceptibility.” 2 But most high-risk women do not gettested. Kramer almost didn’t. “i had told every gynecologistthroughout the years what my family history was,” says Kramer,“and nobody seemed to worry about it.”
according to a recent study, about half of the women iden-tified as high risk in a national survey knew about genetic test-ing, about 10 percent had discussed it with a health profes-sional and less than 2 percent had been tested. 3
a woman who tests positive has several options: She cantake a medication like tamoxifen, which can reduce the riskof developing breast cancer; have more frequent cancer screen-ings and clinical exams; or have preventive surgery.
Kramer decided to have surgery to remove her ovaries,fallopian tubes, uterus and both breasts. “i did not want to liveon pins and needles,” she says. Her sister, who also tested pos-itive, chose hysterectomy, no mastectomy and frequent breastscreening.
few High-Risk women Get Genetic testingTests can spot mutations in genes that suppress breast cancer tumors.

April 2, 2010 301www.cqresearcher.com
trials and statistics to nazi physicianswho experimented on humans duringworld war ii. 44
yet in 1966, in a series of papersfollowing several clinical trials, uni-versity of pittsburgh surgeon andpathologist Bernard fisher “turned up-side down the prevailing logic of ma-lignancy and metastasis.” He arguedthat from the very beginning of abreast tumor’s life, cancer cellsslough off into the lymphatic systemand the blood stream. “cells withouta future succumbed to the immunesystem, but others . . . waited to takeroot somewhere else in the body.”olson writes that the papers had enor-mous impact, removing the rationalefor emergency surgery — to catchthe cancer quickly before it can spread— and giving women time to ex-plore their options. 45
fisher’s research also set the stagefor the expanded use of chemothera-py — chemical agents that destroycancer cells throughout the body. Heargued that the only hope for cancerwas for surgeons to reduce the tumorso any remaining cancer cells couldbe destroyed by the patient’s immunesystem and anticancer drugs.
ten years later, fisher was respon-sible for delivering the obituary onradical mastectomy. He tracked near-ly 2,000 women in canada and theunited States for six years, who eitherhad had a radical mastectomy or asimple mastectomy (removal of thebreast that leaves the lymph nodesand chest muscles intact) followed byradiation. the survival rates were vir-tually the same. 46
in 1990, the national institutes ofHealth announced that lumpectomy
(removing the tumor but leaving mostof the breast intact) plus radiation isas effective as simple mastectomy. Butthe ensuing debate about lumpectomydid not completely subside until 2002,when fisher and colleagues publishedthe results of a randomized trial show-ing that women with relatively smallbreast cancers treated with lumpecto-my plus radiation were as likely to bealive and disease-free 20 years later aswomen treated with mastectomy. 47
Non-surgical Breakthroughs
d espite advances in surgery andchemotherapy, mortality rates for
breast cancer barely budged from1950-1990 — remaining at about 28deaths per 100,000 people. 48 Since
testing for BRca1 and BRca2 mutations clearly can leadto intervention, but experts say some new types of dna analy-sis being offered to consumers have no clear clinical utility.
Researchers have found minor variations in dna — called SnpS(single nucleotide polymorphisms) — that are associated with breastcancer. unlike BRca mutations, Snps are fairly common, but theincreased risk associated with each Snp is low — the equivalent,say, of postponing childbearing from age 30 to 35.
Robson doesn’t favor testing for Snps, because “it is not atall clear that Snps indicate any change in intervention.” andaSco recommends that Snp testing be given only through clin-ical trials. 4 moreover, a government advisory panel has calledfor the creation of a public registry of genetic tests so their va-lidity can be studied. 5
in the meantime, dozens of companies now offer genomictesting to individuals, who swab their cheeks or spit into a testtube and mail it in with a check.
for instance, navigenics, a genetics-testing firm in fostercity, calif., tests for markers associated with 28 health condi-tions, including seven different Snps associated with breast can-cer. consumers can order their genomic profile directly orthrough a physician.
“many of the physicians we work with use this to help re-fine screening recommendations for their patients,” says elissa
levin, navigenics’ director of genomic services. But aSco saysthere are no scientific studies, at least so far, that validate thisuse of the tests.
nevertheless, genomic screening may have some personal util-ity. positive results, levin says, may help motivate some womento make lifestyle changes that could lower their risk of cancer.But critics say it could make others anxious and confused.
to avoid that, navigenics offers its customers genetic coun-seling by phone, and levin says most of its clients use the ser-vice. But not all companies offer genetic counseling. in fact,neither do all physicians.
— Barbara Mantel
1 “BRca1 and BRca2: cancer Risk and Genetic testing,” national cancerinstitute fact sheet, may 2009, p. 2.2 marc e. Robson, et al., “american Society of clinical oncology policy State-ment update: Genetic and Genomic testing for cancer Susceptibility,” Jour-nal of Clinical Oncology, Jan. 11, 2010, p. 3, http://jco.ascopubs.org/cgi/doi/10.1200/Jco.2009.27.0660.3 douglas e. levy, et al., “Guidelines for Genetic Risk assessment of Heredi-tary Breast and ovarian cancer: early disagreements and low utilization,”abstract, Journal of General Internal Medicine, July 2009.4 Robson, et al., op. cit.5 “u.S. System of oversight of Genetic testing: a Response to the chargeof the Secretary of Health and Human Services,” department of Health andHuman Services, april 2008, p. 8.

302 CQ Researcher
then, however, the death rate has de-clined steadily, thanks to earlier de-tection, improved treatment and abetter understanding of the geneticsof breast cancer.
in 1990, while teaching at the uni-versity of california, Berkeley, geneti-cist mary-claire King determined that5-10 percent of breast cancer cases re-sulted from an inherited mutant geneon the long arm of chromosome 17,later identified as BRca1, a tumor sup-pressor gene. the mutations allowtumor cells to grow.
King — who had spent 15 yearsstudying Jewish women of ashke-nazi decent, who have a high inci-dence of breast cancer — later dis-covered a second, similar gene calledBRca2. Since her breakthroughs,scientists have developed drugs thathelp prevent breast cancer in womenof high risk. 49
But not all women with the mu-tations go on to develop breast can-cer. Since a woman inherits twocopies of the gene, one from eachparent, perhaps the normal copymust also mutate during a patient’slifetime for cancer to grow. Someresearchers have speculated that en-vironmental toxins may cause thatmutation.
as scientists made strides in un-derstanding the biology of breastcancer, they began to develop ther-apies geared to the particular char-acteristics of tumor tissue. for in-stance, drugs like tamoxifen aregiven to patients who have early-stage breast cancer with estrogen re-ceptors on the cells’ surfaces. thedrugs block the receptors, prevent-ing estrogen from binding to the celland causing the cancer to grow. tak-ing tamoxifen after surgery for fiveyears cuts the chances of recurrenceby about half, but the drug has sideeffects and may increase a woman’schance of developing endometrialcancer and blood clots. 50
BReaSt canceR
Continued on p. 304
Risk Factors for Breast Cancer
Several factors affect women’s likelihood to get breast cancer, includ-ing age and family history. Several other risk factors are preventable, such as a woman’s recent use of birth control pills.
Source: “What Causes Breast Cancer?” American Cancer Society
Risk Factors That Aren’t Preventable:
Gender: Women are 100 times more likely than men to get breast cancer.
Age: About two-thirds of women with invasive breast cancer are at least 55.
Genetics: About 5 to 10 percent of breast cancers may be linked to mutations in certain genes.
Family history: A woman with a mother, sister or daughter with breast cancer is twice as likely to get it.
Personal history: A woman with breast cancer is more likely to get a new cancer in her other breast or elsewhere in the same breast.
Race: White women are most likely to get breast cancer. African-American women are most likely to die from it. Asian, Hispanic and Native American women are less likely to get breast cancer.
Breast tissue density: Women with denser breast tissue have more gland tissue and less fatty tissue and are at a higher risk for breast cancer.
Menstrual periods: Women who began having periods before age 12 or who began menopause after age 55 have been exposed to more estrogen and progesterone.
Earlier breast radiation: Women treated for another cancer with radiation to the chest have a greatly increased risk of getting breast cancer.
Risk Factors That May Be Preventable:
Not having children or having them later in life: Women who haven’t had children or had their first child after age 30 are more likely to get breast cancer.
Recent use of birth control pills: Women using birth control pills are at a higher risk for breast cancer, but that risk subsides once they stop taking them.
Using post-menopausal hormone therapy: Some doctors prescribe estrogen and progesterone to relieve menopause symptoms, which may make women more likely to get breast cancer and die from it.
Not breast-feeding: Because breast-feeding lowers a woman’s total number of menstrual periods, it slightly lowers her risk of breast cancer.
Alcohol: Women who have between two and five drinks per day are one-and-a-half times more likely to get breast cancer than women who don’t drink alcohol.
Being overweight: Women who are overweight or obese have a greater risk of breast cancer, especially after beginning menopause or if they became overweight or obese during adulthood.
Lack of exercise: A study found that only an hour-and-a-quarter to two-and-a-half hours of brisk walking weekly reduced risk of breast cancer by 18 percent.

April 2, 2010 303www.cqresearcher.com
S uzanne Conzen is an associate professor of hematology/oncology at the University of Chicago’s Pritzker School ofMedicine. She and behavioral biologist Martha McClintock
are studying the link between stress, social isolation and breastcancer in mice and rats. They also have teamed up with soci-ologists to study socially isolated African-American women onChicago’s South Side who are newly diagnosed with breast can-cer. Here are highlights from cQR contributing writer BarbaraMantel’s recent interview with Conzen.
CQR: What happens to femalemice and rats when they are isolat-ed, compared to rats living in groups?SC: for reasons that are not com-
pletely understood, this strain of ratshas been known in older age to de-velop breast cancer. we have found thatthese rats develop tumors much earli-er, and the tumors end up being larg-er when the rats are socially isolated.
CQR: Why?SC: martha noticed that these iso-
lated rats were much more jumpyand vigilant than those in groups andwondered if they have differences intheir stress response brought on bytheir social isolation. She found thelevels of the stress hormone corti-costerone [cortisol in humans] weremuch higher and lasted much longerin reaction to a superimposed, un-expected stress in the isolated rats.
CQR: What do you mean by su-perimposed unexpected stress?SC: this was [physical] restraint; it is supposed to mimic a
burrow collapsing.CQR: So you did the same experiment with mice that
are designed to get cancer, known as transgenic mice?SC: yes, we separated the female mice at weaning into iso-
lation or group housing. and indeed these socially isolatedtransgenic mice develop earlier and larger tumors.
CQR: Did you also measure the stress hormones?SC: yes, and we found a very similar response to a super-
imposed stressor. their corticosterone levels increased signifi-cantly more rapidly and to a higher degree than the group-housed mice. this is interesting because this is a geneticallyinbred strain of mice that are used for cancer biology experi-ments, and the only difference had been their housing.
CQ: How would stress hormone affect the develop-ment of breast cancer?
SC: one possibility is that chronic social isolation is caus-ing an increase in the circulating stress hormones, and this maybe related to changes in the gene expression that we see inthe mouse mammary gland. this hormone, corticosterone, isactually known to turn genes on and off.
CQR: Do you know which genes?SC: what surprised us is that we thought the genes that
would be regulated in association with this stress would beprimarily cell survival genes, genes that affect whether a cell
lives or dies. what we found, in fact,was that they were genes more closelyassociated with the metabolism of sug-ars and fats.
CQR: So how did the increase instress make these tumors grow fasterand larger?SC: that’s what we don’t know. all
we know is that it has changed the geneexpression in the mammary gland so thatthere is more efficient production of fattyacids, which are absolutely critical forcancer cells to grow.
CQR: Does this research in the labhave much to say about women, stressand breast cancer?SC: i think it is not directly translat-
able at this point, except to say it raisesthe possibility that the social environmentis a player in changing the physiologythat is relevant to cancer development. inthat way, it is paradigm shifting.
CQR: you’ve teamed up with soci-ologists, in particular Sarah Gehlert of Washington Uni-versity in St. Louis, to study African-American womennewly diagnosed with breast cancer who live on the SouthSide of Chicago. Why?SC: my interest was instigated by my patients, many of
whom are from the South Side of chicago, who were con-vinced that stress played a role in their cancer.
CQR: Gehlert’s team is interviewing the women, ana-lyzing crime statistics and neighborhood conditions, mea-suring their stress hormone and studying tumor biop-sies. How does it all work?SC: Sarah measures the women’s cortisol levels to see if
their history of stress — for instance, divorce, murders in thefamily — associate with abnormal cortisol secretion. what we’dlike to do is get a sense of what happens to these patients.How does the cortisol correlate with the kinds of breast can-cers that they get?
do Social isolation and Stress lead to Breast cancer?Experiments with mice and rats suggest a possible link.
Suzanne Conzen.
Suza
nne
conze
n

304 CQ Researcher
BReaSt canceR
the antibody trastuzumab is givento breast cancer patients with too muchHeR2 protein in the cancer cell mem-brane, which causes cells to repro-duce uncontrollably. the drug bindsto the protein, effectively deactivatingit. Studies have shown that the drugin combination with chemotherapy im-proves survival, but patients have oftendeveloped resistance. Heart problemscan also result.
the holy grail of treatment is per-sonalized medicine, and the intro-duction in 2004 of a new genetictest called oncotype dx is a startdown that path for breast cancer pa-tients. the test measures the ex-pression of 21 genes in breast tumortissue and generates a prediction ofrecurrence. clinicians have begun touse the test to determine who bestbenefits from chemotherapy aftersurgery in hopes of avoiding un-necessary toxic treatment.
cuRRentSituation
Task Force Authority
t he historic health care legisla-tion signed into law by presi-
dent obama on march 23 includesa controversial — but little discussed— provision that expands the au-thority of the u.S. preventive Ser-vices task force. created in 1984,the independent panel of private-sector experts evaluates the scientif-ic evidence for the effectiveness ofpreventive services, like mammogra-phy. until march 23, its recommen-dations were considered authorita-tive, but primarily advisory.
now uSpStf guidelines will havethe weight of law. under health care
reform, all insurance plans eventuallywill have to cover at little or no costto patients all preventive services thatthe task force rates as “a” or “B,” in-dicating that science shows the ser-vice provides a net benefit that is mod-erate to substantial.
late last year, when this provisionwas inserted into both the Senate andthe House versions of health care re-form, opposition was vigorous.
critics quickly warned that thetask force would ration care. “we’restarting down a path, in my opin-ion, of socialization of medicine inthis country,” said Rep. Joe l. Bar-ton, R-texas, at a congressional hear-ing. “we don’t want rationing of healthcare in america. we don’t want tointervene between the doctor-patientrelationship.” 51
task force supporters disputed thatcharge. “nothing could be further fromthe truth,” said Rep. waxman. the leg-islation simply established a minimumcoverage, and insurers would be freeto cover services given a lower rating,said waxman. 52 in fact, the exactwording of the legislation is quite clear:
“nothing in this subsection shall beconstrued to prohibit a plan or issuerfrom providing coverage for servicesin addition to those recommended byunited States preventive Services taskforce or to deny coverage for servicesthat are not recommended by suchtask force.” 53
But critics worried the task force’sratings would serve as a benchmark,tempting insurers to withdraw cover-age of lower-rated services, like mam-mograms for women in their 40s, whichgot a c rating last november.
So in early december, the Senatesprang into action and carved outan exception for mammography, de-livering a significant blow to thecredibility of the uSpStf. Becausethe Senate bill was eventuallypassed by the House and signed bythe president into law, this excep-tion now stands.
“as i reviewed the bill, i felt we coulddo more to enhance and improvewomen’s healthcare,” said Sen. Barbaramikulski, d-md., at the time. 54
mikulski and olympia Snow, R-maine, sponsored, and the Senatepassed, an amendment requiring in-surers to cover, without any costs topatients, preventive care and screen-ings for women approved by a fed-eral agency, the Health Resources andServices administration.
But an amendment offered bySen. david vitter, R-la., and passedby the Senate specifically set asidethe uSpStf’s november guidelinesfor the purposes of insurance cov-erage. “the current recommenda-tions of the united States preven-tive Services task force regardingbreast cancer screening, mammog-raphy, and prevention shall be con-sidered the most current other thanthose issued in or around novem-ber 2009.” 55 in other words, thetask force’s B rating from 2002 is theone that counts. So insurers will haveto cover screening mammographyfor women in their 40s.
Task Force Accountability
B esides expanding the authority ofthe uSpStf, the original House
version of the health care reform mea-sure had tried to make the panel’s pro-ceedings more transparent and its mem-bers more diverse.
the measure would have expandedthe task force from 16 to 30 mem-bers, including specialists in women’shealth and geriatrics, for instance. itsmeetings would have been made morepublic, and it would have had toconsult a “stakeholder’s board” madeup of representatives from the pub-lic, advocacy groups and the insur-ance industry. 56
“people who follow the uSpStf havelong recognized some of the problems
Continued on p. 306
Continued from p. 302

no
April 2, 2010 305www.cqresearcher.com
at issue:Should the courts overturn patents for genes linked to elevatedbreast cancer risk?*yes
yesJEFFREy A. KANTDIRECTOR, DIVISION OF MOLECULARDIAGNOSTICS, UNIVERSITY OF PITTSBURGHMEDICAL CENTER; MEMBER, COLLEGE OFAMERICAN PATHOLOGISTS MOLECULARPATHOLOGY WORKGROUP
WRITTEN FOR CQ RESEARCHER, APRIL 2010
l awyers from the american civil liberties union (aclu)have laid out legal arguments challenging patents issuedto myriad Genetics for the genes known as BRca1 and
BRca2. mutations of the two genes provide a significanthereditary predisposition for breast and ovarian cancer. thecase could set a landmark precedent. the college of americanpathologists is among 19 plaintiffs, representing thousands ofmedical researchers, physicians and patients who oppose theissuance of patents on human genes.
the college believes patents on genes, genetic variants andgenotype-phenotype correlations — when enforced to restrictdiagnostic genetic testing — violate longstanding prohibitionsagainst patenting natural phenomena and laws of nature. thecollege’s opposition to gene patents is rooted in principle andpractice. Genes including their range of dna sequence vari-ants are naturally occurring products of nature, hence issuinga patent on an isolated gene — including mutations of thatgene — violates legal principles restricting patents on productsor laws of nature. as the law is currently written, patentinghuman genes limits patient access to medical care, jeopardizesthe ability to practice medicine in the best interest of patientsand raises the cost of care.
a patent holder may authorize a single lab to test a patentedgene or require such high licensing fees that a wider range oflaboratories are prevented from providing diagnostic services,second opinions or developing improved tests. as medicalspecialists in the diagnosis of disease, pathologists have anabiding interest in ensuring that gene patents do not restrictthe ability of physicians to provide quality diagnostic servicesto the patients they serve. multiple surveys have indicated thatgene patents limit laboratory offerings as well as a patient’saccess to testing for specific genes and disorders.
Recently, the department of Health and Human ServicesSecretary’s advisory committee on Genetics, Health and Societyvoted to recommend exemptions from certain patents, whichwould allow medical researchers to study more genes and de-velop more diagnostic tests based on already patented humangenes without the threat of a patent-infringement lawsuit.Recognition by this prestigious advisory group underscores theimportance of addressing gene patents for the future of med-ical research, genetic testing and personalized health care.no
KEVIN E. NOONANPATENT ATTORNEY AND MOLECULARBIOLOGIST, CHICAGO, ILL.
WRITTEN FOR CQ RESEARCHER, APRIL 2010
p atents for any invention do two things: protect fromcopiers (thereby promoting commercialization) and fa-cilitate disclosure. u.S. patent law fulfills both these goals. patent rights are granted for only 20 years from
the application’s filing date; after a patent expires, the inventionis freely available to all — forever — and cannot be repatentedor its availability otherwise restricted. also, a patent applicantmust provide a complete description of how to make and usethe invention, ensuring that it is fully disclosed.
isolated dna is patentable for several reasons that contradictsome of the misinformation spread by those opposed to thepractice. first, patented dna must be isolated from a cell, sothat no one owns “your” dna. Second, patented dna ischanged from its chemical form in the body, and this chemicalconversion is more extensive than the types of purification ofnaturally occurring compounds, such as antibiotics and anti-cancer drugs, which are clearly patentable. third, the genetic in-formation contained in a patented gene is unpatentable and canbe freely used. fourth, gene patents do not prevent basic re-search on genes: the research database pubmed contains morethan 7,000 research papers on the BRca1 and BRca2 genes,most of them published after the patents on these genes weregranted. finally, without patent protection, university researcherswould be performing uncompensated research and developmentfor corporations that would be able to use their inventionsfreely, since university scientists publish their work.
most diseases are not like BRca-linked breast or ovariancancer; more than one gene is affected during the develop-ment of the disease. imagine a world where isolated dnawas not patentable. Researchers could survey tissue samples toidentify genes and alterations involved in common diseaseslike diabetes and cancer. Bio-informatics methods using “genechips” containing 10,000 genes could then be used to providea diagnosis without identifying the specific genes or mutationsinvolved. the complexity of such systems would make themvery hard to reverse-engineer, so developers could keep thema trade secret. the public would not benefit from the expirationof a patent or the disclosures that accompany patenting.
critics of gene patenting do not take these disadvantages ofbanning such patenting into account. in addition, the relianceon emotional — and in some cases dishonest — appealsshould raise serious questions about the motivations and co-gency of these arguments.no
* Editor’s note: On March 29, 2010, U.S. District Judge Robert W. Sweet struck down patents on two genes linked to breast and ovarian cancer,BRCA1 and BRCA2. Myriad Genetics, the patent holder, said it would appeal the decision.

306 CQ Researcher
with it,” says dick woodruff, senior di-rector of federal relations for the amer-ican cancer Society’s cancer action net-work, which opposed the task force’srevised mammographyguidelines. “they oper-ate several levels downin the bureaucracy, themeetings are closed andthe membership is small,”he adds.
transparency andpublic trust are worthygoals, says former taskforce member Harris,“and i think there aregood ways and badways to do it.” it wouldhelp to allow for pub-lic comments on pro-posed task force guide-lines before the paneltakes its final votes, hesaid. But making everymeeting public, he says,“would turn the pro-ceedings into a circus.”
expanding the sizeof the task force couldmake meetings un-wieldy, and the mem-bership is already di-verse, he says. “thereare physicians, healtheconomists, nursing spe-cialists, pediatric peo-ple and ob-gyn,” Harrissays, and all of themhave been trained inbiostatistics. they knowhow to summarize, ex-amine, and critically ap-praise the thousands ofpublished studies of pre-ventive services forwhich the task force is-sues guidelines, he says.
“we need to make sure the task force’sevaluations remain free from advocacy,politics and economics,” said ned ca-longe, the task force’s chairman. 57
although the House provisions didnot make it into the final health carereform legislation, supporters hopethey will eventually become law. “con-gress is legislating all the time,” says
woodruff. “Hopefully, there will beopportunities in the future to improveupon the bill.”
Breast Cancer Education
t he health care reform law con-tains the Breast cancer education
and awareness learningyoung act, or eaRly act.its controversial originalversion, introduced a yearago, directed the federalgovernment to conduct apublic education campaignto teach young womenhow to detect and preventbreast cancer, by encour-aging breast exams, genet-ic counseling and lifestylechanges.
But critics worried thatsuch a campaign would domore harm than good byraising unnecessary alarmamong younger women, es-pecially those in their 20sand 30s for whom breastcancer is a rare disease.Breast self exams might leadto false alarms and to un-needed mammograms andbiopsies. and makinglifestyle changes to reducerisk, these critics say, is notalways feasible.
two professors of med-icine at the dartmouth in-stitute for Health policyand clinical practice point-ed out that the most com-mon risk factor for breastcancer is delaying childbirth,and the risk begins to riseif a woman has not hadher first full-term pregnan-cy by age 20. in addition,some evidence indicatesthat young women with in-creased body mass have alower risk of breast cancer.
“it is hard to believe that the eaRlyact’s sponsors would want to launcha public health campaign encouragingteens to become pregnant or gain
BReaSt canceR
Continued from p. 304
Debate over the efficacy of regular mammography screening forwomen in their 40s has been going on for decades, and shows nosign of ending. Last November, an independent scientific panelrecommended against routine screening for most women in thisage bracket, reversing its recommendation of seven years earlier.In 1987, the National Cancer Institute recommended that
healthy women, beginning at age 40, should get mammogramsevery one to two years. In 1993, it dropped that recommendation, only to adopt it again in 1997.
Stock
photo

April 2, 2010 307www.cqresearcher.com
weight,” the professors wrote in anewspaper opinion piece. 58
Susan love, a breast cancer sur-geon in Santa monica, calif., andpresident of the dr. Susan love Re-search foundation, argued againstpassage of the eaRly act. youngwomen may be led to overestimatetheir risk of dying from the disease,she said, and “once you have madewomen more ‘aware’ of their po-tential risk, you will have nothing totell them to do,” she wrote in a letterto the bill’s sponsors. 59
the american cancer Society andits cancer action network also op-posed the eaRly act, and the orga-nization proposed revisions, which wereeventually adopted.
“the key to the rewrite,” sayswoodruff, “was to give the secretary[of Health and Human Services] muchbroader authority to look at the evi-dence and the science and figure outhow best to communicate to youngwomen about breast health in gen-eral.” Gone were specific recommen-dations for dietary changes, geneticcounseling and breast self-exam.
But is the bill so watered downas to be unnecessary? “our job is tolook at the legislation and help todevelop a bill that makes the mostsense under the circumstances,” sayswoodruff.
outlooKPersonalized Treatment
m ore than half of americanwomen diagnosed with breast
cancer each year have estrogen re-ceptor positive cancer that has notspread to the lymph nodes. the stan-dard treatment is surgery, plus radia-tion and hormonal therapy, whichcures about 80 to 85 percent of pa-
tients. yet most women with thisdiagnosis are also advised to receiveoften toxic chemotherapy to preventthe cancer’s return. 60
“the vast majority of people thatwe are treating with chemotherapy arenot benefiting from the treatment” be-cause they don’t need it, says JosephSparano, md, the director of the Breastevaluation center at the montefiore-einstein cancer center in the Bronx.doctors are still refining the tools thatwould identify the minority of patientsat risk of recurrence.
one of those tools is oncotypedx, which marks a breakthrough inpersonalized medicine for breast can-cer patients. it is a test that measuresthe activity of 21 genes in tumor tis-sue and allows doctors to customizetreatment. the test generates a scoreranging from 0 to 100; the higherthe score, the greater the chance awoman has of a recurrence withoutchemotherapy. according to the na-tional cancer institute, oncotype dxis more accurate at estimating recur-rence risk than standard measures,like tumor size. 61
Since oncotype dx came on themarket in 2004, physicians have or-dered it for more than 100,000 patients,and the american Society of clinicaloncology has recently endorsed it. 62
in one study published this year, on-cologists changed treatment recom-mendations for 31.5 percent of patientsbased on the oncotype dx recurrencescore, with the most common changefrom chemotherapy plus hormonaltherapy to hormonal therapy alone. 63
But the test’s benefit is unclear forthe majority of women receiving it,those whose scores fall in the 11 to25 range. for women with scores belowor above, Sparano says the treatmentdirection after surgery is clear: hor-monal therapy alone for those withlow scores and hormonal therapy pluschemotherapy when the score is high.But, he says, “we don’t have really de-finitive information that a woman with
a score in the mid-range really bene-fits from chemotherapy.”
Sparano is recruiting patients intoa nationwide study called tailoRx,designed to determine the benefit ofchemotherapy to those women. womenwith low or high scores will receivethe accepted treatment for their scores,but women with a recurrence scoreof 11 to 25 will be randomly assignedto receive hormonal therapy, with orwithout chemotherapy. a total of 11,000women are expected to be enrolledby mid-2011. the women will be stud-ied for 10 years.
personalized medicine is also beingtested for women with high risk, fastgrowing breast cancers. in march, apublic-private partnership led by thefoundation for the national institutesof Health launched a national trial thatwould administer promising newdrugs to women based on geneticmarkers in their tumors. the drugswould be given, along with chemother-apy, prior to surgery to help shrinktumors. 64
“personalized treatment of cancer isthe future,” says dr. edith perez, di-rector of the mayo clinic’s Breast pro-gram in Jacksonville, fla., who is alsorecruiting patients for the tailoRxstudy. perez runs the clinic’s Breastcancer translational Genomics pro-gram, whose purpose, she says, “is toeventually be able to do a completegenomic profiling of tissue from awoman’s tumor, look for abnormalitiesand then customize treatment.”
Notes
1 “can Breast cancer Be prevented?” ameri-can cancer Society, September 2009, p. 1,www.cancer.org.2 for background, see david masci, “women’sHealth,” CQ Researcher, nov. 7, 2003, pp. 941-964.3 “cancer facts & figures 2009,” americancancer Society, p. 9, www.cancer.org.4 Ibid.

308 CQ Researcher
BReaSt canceR
5 “Screening for Breast cancer,” united Statespreventive Services task force, agency forHealthcare Research and Quality, departmentof Health & Human Services, november 2009,updated december 2009, www.ahrq.gov/clinic/uSpstf/uspsbrca.htm#summary.6 “Hollywood Breast cancer Survivors Speakout against new mammogram Guidelines,”“access Hollywood,” nov. 18, 2009, www.accesshollywood.com.7 “uSpStf mammography Recommendationswill Result in countless unnecessary Breastcancer deaths each year,” american collegeof Radiology, nov. 16, 2009, www.medicalnewstoday.com/articles/171247.php.8 “Secretary Sebelius Statement on newBreast cancer Recommendations,” dept. ofHealth and Human Services, news release,nov. 18, 2009, www.hhs.gov/news/press/2009pres/11/20091118a.html.9 alice park and Kate pickert, “the mam-mogram melee,” Time, dec. 7, 2009, p. 40.10 “opening Statement of Rep. Henry a. wax-man,” Hearing on Breast cancer ScreeningRecommendations, Subcommittee on Health,dec. 2, 2009, http://energycommerce.house.gov./press_111/20091202/waxman_opening.pdf.11 “new mammography Guidelines, a deathSentence for Black women,” nov. 19, 2009,http://breakingoursilence.com.12 “cancer Health disparities,” national can-cer institute, march 11, 2008, www.cancer.gov/cancertopics/factsheet/cancer-health-disparities/disparities.13 “m.d. anderson Study finds Racial dis-parities exist in Radiation therapy Rates forearly Stage Breast cancer,” news release, mdanderson cancer center, dec. 14, 2009,www.mdanderson.org/newsroom.
14 Sandra young, “new cervical cancerscreening guidelines released,” cnn, nov. 20,2009, www.cnn.com/2009/HealtH/11/20/cervical.cancer.guidelines/.15 “american cancer Society Responds tochanges to uSpStf mammography Guide-lines,” american cancer Society, nov. 16, 2009,www.cancer.org.16 “acoG Statement on Revised uS preven-tive Services task force Recommendationson Breast cancer Screening,” american con-gress of obstetricians and Gynecologists,nov. 16, 2009, www.acog.org.17 “Society Responds to uSpStf changes inmammography Guidelines,” american Societyof Breast Surgeons, www.breastsurgeons.org.18 “uSpStf mammography Recommendationswill Result in countless unnecessary Breastcancer deaths each year,” op. cit.19 “new mammography guidelines a disser-vice,” letter to the editor, The San Diego Union-Tribune, dec. 27, 2009, p. B7.20 Robert aronowitz, “addicted to mammo-grams,” The New York Times, op-ed., nov. 20,2009.21 “Screening for Breast cancer, Recommen-dation Statement,” agency for Healthcare Re-search and Quality, u.S. department of Health& Human Services, december 2009, p. 2.22 Roni caryn Rabin, “doctor-patient divideon mammograms,” The New York Times,feb. 16, 2010, p. d7.23 Beth a. virnig, et al., “diagnosis and man-agement of ductal carcinoma in Situ (dciS),”agency for Healthcare Research and Quali-ty, u.S. department of Health and HumanServices, September 2009, p. 1.24 liz Szabo, “ ‘new’ type of breast cancerstops women in their tracks; mystery condi-
tion called dciS sparks treatment debate,”USA Today, oct. 12, 2009, p. 5d.25 H. Gilbert welch, et al., “the Sea of un-certainty Surrounding ductal carcinoma inSitu: the price of Screening mammography,”Journal of the National Cancer Institute,feb. 20, 2008, p. 228.26 Szabo, op. cit.27 y. y. chen, et al., “pathologic and biologicresponse to preoperative endocrine therapyin patients with eR-positive ductal carcinomain situ,” BMC Cancer, aug. 18, 2009.28 “environmental Risk factors for Breast can-cer,” national Breast cancer coalition, Sep-tember 2006, p. 2, www.stopbreastcancer.org.29 Ruthann a. Rudel, et al., “chemicals caus-ing mammary Gland tumors in animals Sig-nal new directions for epidemiology, chem-ical testing, and Risk assessment for Breastcancer prevention,” Environmental Factorsin Breast Cancer, supplement to Cancer,June 15, 2007, pp. 2635-2636.30 Julia Green Brody and Ruthann a. Rudel,“environmental pollutants and Breast cancer:the evidence from animal and Human Stud-ies,” Breast Diseases: A Year Book Quarterly,vol. 19, no. 1, 2008, p. 17.31 Rudel, et al., op. cit.32 Julia G. Brody, “everyday exposures andBreast cancer,” Reviews on EnvironmentalHealth, vol. 25, no. 1, 2010, p. 3.33 Janet Gray, ed., “State of the evidence: theconnection Between Breast cancer and theenvironment,” Breast cancer fund, 2008, p. 9.34 “what is the national children’s Study?”www.nationalchildrensstudy.gov/pages/default.aspx.35 Brody, op. cit., p. 4.36 James S. olson, Bathsheba’s Breast: Women,Cancer & History (2002), p. 61.37 Ibid.38 Ibid.39 Ibid., pp. 62-63.40 Barron H. lerner, The Breast Cancer Wars(2001), p. 33.41 Ibid., pp. 33-35.42 Ibid., p. 69.43 Ibid., p. 101.44 Ibid., p. 115.45 olson, op. cit., p. 129.46 Bernard fisher, “united States trials of con-servative surgery,” World Journal of Surgery,vol. 1, no. 3, may 1977, www.springerlink.com/content/j1313t7453876666/.47 B. fisher, et al., “twenty-year follow-up ofa randomized trial comparing total mastec-
About the AuthorBarbara Mantel is a freelance writer in new york citywhose work has appeared in The New York Times, the Jour-nal of Child and Adolescent Psychopharmacology and MammMagazine. She is a former correspondent and senior pro-ducer for national public Radio and has won several jour-nalism awards, including the national press club’s Best con-sumer Journalism award and the front page award fromthe newswomen’s club of new york for her april 18, 2008,CQ Researcher report “public defenders.” She holds a B.a.in history and economics from the university of virginia andan m.a. in economics from northwestern university.

April 2, 2010 309www.cqresearcher.com
tomy, lumpectomy, and lumpectomy plus ir-radiation for the treatment of invasive breastcancer,” New England Journal of Medicine,oct. 17, 2002.48 aronowitz, op. cit.49 “Gene BRca1,” the chemical Heritagefoundation, 2001, www.chemheritage.org/educationalServices/pharm/chemo/readings/brca1.htm.50 “Hormone therapy,” american cancer So-ciety, Sept. 18, 2009, www.cancer.org.51 Rob Stein, “in wake of mammographyguidelines, u.S. health task force faces newscrutiny,” The Washington Post, dec. 20, 2009,p. a3.52 Ibid.53 patient protection and affordable care act,Sec. 2713, http://thomas.loc.gov/cgi-bin/query/f?c111:7:./temp/~c111kvSix:e51492.54 emily p. walker, “Senate affirms Screeningmammography for 40-year-olds,” MedPageToday, dec. 3, 2009.55 “patient protection and affordable careact,” Sec. 2713, op. cit.56 Stein, op. cit.57 Ibid.58 Steven woloshin and lisa m. Schwartz,“the eaRly act is not what the doctor or-dered,” Los Angeles Times, July 31, 2009,http://articles.latimes.com/2009/jul/31/opinion/oe-woloshin31.59 natasha Singer, “in push for cancer Screen-ing, limited Benefits,” The New York Times,July 17, 2009, p. a1.60 “new Genetic test for personalized treat-ment of Breast cancer,” montefiore medicalcenter, www.montefiore.org/whoweare/stories/Sparano/.61 “personalized treatment trial for Breastcancer launched,” national cancer institute,www.cancer.gov/newscenter/pressreleases/tailoRxRelease.62 Susan Jenks, “Gene tests avert chemother-apy,” Florida Today, June 2, 2009, p. 1d.63 Shelly S. lo, et al., “prospective multicenterStudy of the impact of the 21-Gene Recur-rence Score assay on medical oncologist andpatient adjuvant Breast cancer treatment Se-lection,” Journal of Clinical Oncology, abstract,Jan. 11, 2009, jco.ascopubs.org/cgi/content/abstract/Jco.2008.20.2119v1.64 “the Biomarkers consortium launches i-Spy 2 Breast cancer clinical trial,” foundationfor the national institutes of Health, march 17,2010, www.biomarkersconsortium.org/images/stories/docs/ispypress031710.pdf.
FOR MORE INFORMATIONAgency for Healthcare Research and Quality, 540 Gaither Road, Suite 2000,Rockville, md 20850; (301) 427-1364; www.ahrq.gov. a department of Health andHuman Services agency that uses research to improve health care practice and policy.
American Cancer Society, 250 williams St., n.w., atlanta, Ga 30303; (404) 320-3333; www.cancer.org. a nationwide, community-based health organization thatsponsors cancer research, educates the public and advocates for policies and laws.
Breast Cancer Action, 55 new montgomery St., San francisco, ca 94105; (415)243-9301; http://bcaction.org. advocates for policy changes in treatment, environ-mental exposures and health care inequities.
Breast Cancer Fund, 1388 Sutter St., Suite 400, San francisco, ca 94109; (415)346-8223; www.breastcancerfund.org. advocates for elimination of environmentaland other preventable causes of breast cancer.
Centers for Disease Control and Prevention, Division of Cancer Preventionand Control, 4770 Buford Hwy, n.e., mS K-64, atlanta, Ga 30341; (800) 232-4636;www.cdc.gov/cancer/breast. federal agency that collects information about cancer,including who gets it, at what stage it is diagnosed and how it is treated.
Dr. Susan Love Research Foundation, 811 wilshire Blvd., Suite 500, Santa monica,ca 90403; (310) 828-0060; www.dslrf.org. works to eradicate breast cancer and im-prove the quality of women’s health through research, education and advocacy.
National Breast Cancer Coalition, 1101 17th St., n.w., Suite 1300, washington,dc 20036; (202) 296-7477; www.stopbreastcancer.org. lobbies national, state andlocal governments for increased funding for cancer research and improved healthcare access for women.
National Breast Cancer Foundation, 2600 network Blvd., Suite 300, frisco, tx75034; (469) 252-0075; www.nationalbreastcancer.org. funds free mammograms forwomen in need.
National Cancer Institute, 6116 executive Blvd., Bethesda, md 20892; (301) 496-6641; www.cancer.gov. the principal federal agency for cancer research and training.
National Women’s Health Network, 1413 K St., n.w., 4th floor, washington,dc 20005; (202) 682-2640; http://nwhn.org. promotes a critical analysis of healthissues in order to affect policy and support consumer decision-making.
RxList, c/o webmd, 111 8th ave, 7th floor, new york, ny 10011; (212) 624-3700;www.rxlist.com. an online medical resource providing detailed and current phar-maceutical information on brand and generic drugs.
Silent Spring Institute, 29 crafts St., newton, ma 02458; (617) 332-4288;www.silentspring.org. investigates research into the links between the environmentand women’s health, with particular emphasis on breast cancer.
Susan G. Komen for the Cure, 5005 lBJ freeway, Suite 250, dallas, tx 75244;(877) 465-6636; www.komen.org. a worldwide grassroots network of breast cancersurvivors and activists that raises money for research through its Race for the cure.
FOR MORE INFORMATION

310 CQ Researcher
Selected Sources
Bibliography
Books
Lerner, Barron H., The Breast Cancer Wars: Hope, Fear,and the Pursuit of a Cure in Twentieth-Century America,Oxford University Press, 2001.a columbia university professor of medicine examines the
medical and cultural history of the battle against breast can-cer in the united States.
Olson, James S., Bathsheba’s Breast: Women, Cancer &History, The Johns Hopkins University Press, 2002.a history professor at Sam Houston State university in Huntsville,
texas, describes the history of breast cancer through the storiesof historical figures like abigail adams and Betty ford.
Articles
Park, Alice, and Kate Pickert, “The Mammogram Melee,”Time, Dec. 7, 2009.the furor over the new breast cancer screening guidelines
from the u.S. preventive Services task force could be a signof things to come.
Rabin, Roni Caryn, “Doctor-Patient Divide on Mammograms,”The New York Times, Feb. 16, 2010.many doctors are inclined to accept the new breast can-
cer screening guidelines, while many patients reject them.
Stein, Rob, “In wake of mammography guidelines, U.S.health task force faces new scrutiny,”The Washington Post,Dec. 20, 2009.members of the u.S. preventive Services task force testify
before congress about breast cancer screening and the taskforce’s expanded role under health care reform.
Szabo, Liz, “ ‘New’ type of breast cancer stops women intheir tracks,” USA Today, Oct. 12, 2009.doctors are treating ductal carcinoma in situ (dciS) aggres-
sively even though not all cases will develop into invasivebreast cancer.
Welch, H. Gilbert, Steven Woloshin and Lisa M. Schwartz,“The Sea of Uncertainty Surrounding Ductal Carcinomain Situ —The Price of Screening Mammography,” Journalof the National Cancer Institute, Feb. 20, 2008.a journal editorial argues it may be time to consider re-
serving biopsy for lesions that can be palpated.
Reports and Studies
“Screening for Breast Cancer: Recommendation Statement,”U.S. Preventive Services Task Force, November 2009,
updated December 2009, www.ahrq.gov/clinic/uspstf09/breastcancer/brcanrs.htm.the task force no longer recommends routine screening
for most women in their 40s and recommends screening forwomen 50-74 only every other year.
Allegra, Carmen J., “National Institutes of Health State-of-the-Science Conference Statement: Diagnosis and Man-agement of Ductal Carcinoma In Situ Sept. 22-24, 2009,”Journal of the National Cancer Institute, Vol. 102, Issue3, Feb. 6, 2010.the statement assesses the current data on diagnosis and
management of dciS.
Brody, Julia Green, et al., “Environmental Pollutants andBreast Cancer: Epidemiologic Studies,” Cancer, May 14,2007, www3.interscience.wiley.com/cgi-bin/fulltext/114261513/PDFSTART.the authors review the limited research on links between
environmental pollutants and breast cancer risk in humans.
Gray, Janet, ed., “State of the Evidence: The ConnectionBetween Breast Cancer and the Environment,” BreastCancer Fund, 2008, www.breastcancerfund.org/media/publications/state-of-the-evidence.the author summarizes hundreds of studies examining links
between breast cancer and chemicals and radiation in theenvironment.
Robson, Mark E., et al., “American Society of ClinicalOncology Policy Statement Update: Genetic and GenomicTesting for Cancer Susceptibility,” Journal of ClinicalOncology, Jan. 11, 2010, http://jco.ascopubs.org/cgi/doi/10.1200/JCO.2009.27.0660.the professional group revises its testing recommendations for
genetic mutations associated with breast cancer risk and raisesconcerns about genetic tests marketed directly to consumers.
Rudel, Ruthann A., et al., “Chemicals Causing MammaryGland Tumors in Animals Signal New Directions forEpidemiology, Chemicals Testing, and Risk Assessmentfor Breast Cancer Prevention,” Environmental Factorsin Breast Cancer, Supplement to Cancer, May 14, 2007.the authors identify 216 chemicals associated with increases
in mammary gland tumors in animals.
Virnig, Beth A., “Diagnosis and Management of DuctalCarcinoma In Situ (DCIS),” Agency for Healthcare Re-search and Quality, AHRQ Publication No. 09-E018, Sep-tember 2009, www.ahrq.gov/clinic/tp/dcistp.htm.the authors review the literature on the incidence and treat-
ment of dciS and recommend further avenues for research.

April 2, 2010 311www.cqresearcher.com
Early Detection
Begley, Sharon, “The Myth of Early Detection,”Newsweek,April 6, 2009, p. 44.many breast cancer survivors say early detection saved their
lives, but early detection does not necessarily produce clearand unquestionable benefits.
Frellick, Marcia, “Breast Cancer Research Advancing,”Chicago Tribune, Oct. 4, 2009, p. A24.mammograms are still vital to fighting breast cancer, but
new tools for detection are more promising than ever.
Tatum, Cheryl, “New HMC MRI Aids Breast Cancer De-tection,” The Tennessean, March 30, 2009.a tennessee hospital has installed new mRi technology
that can detect previously undetectable breast cancers.
Health Care Proposals
Park, Alice, and Kate Pickert, “The Mammogram Melee,”Time, Dec. 7, 2009, p. 40.new breast cancer recommendations from the u.S. preventive
Services task force may be difficult for americans to accept.
Pear, Robert, and David M. Herszenhorn, “Senate BacksPreventive Health Care for Women,” The New York Times,Dec. 4, 2009, p. A21.the Senate has voted to require health insurance compa-
nies to provide free mammograms for women while reject-ing a Republican challenge to medicare savings that wouldfinance most of the bill.
Yamamura, Kevin, “Health Policy Very Personal forFiorina,” Sacramento Bee, Nov. 26, 2009, p. A1.u.S. Senate candidate carly fiorina, R-calif., is a breast can-
cer survivor and opposes any health policy recommendingthat women get fewer mammograms.
Mammography
Brawley, Otis W., “Cancer Society: Let’s Stick With Mam-mograms,” News Journal (Delaware), Nov. 23, 2009.many women would not be candidates for breast-conserving
therapy without mammograms, according to the americancancer Society.
Brinker, Nancy, “Debating Mammograms,” Newsweek,Dec. 21, 2009, p. 20.mammograms are not perfect, but they are still the best
breast cancer screening tool widely available.
Rabin, Roni Caryn, “Benefits of Mammogram Under Debatein Britain,” The New York Times, March 31, 2009, p. D5.
mammograms diagnose breast cancer in many women thatis so slow-growing that it would never threaten their lives.
Smith, Stephen, “Breast Screening Advice Upended,”The Boston Globe, Nov. 17, 2009, p. 30.the u.S. preventive Services task force has concluded that
mammograms save the lives of very few women ages 40 to 49.
Voskuil, Scott, “Digital Mammography Offers Many Ad-vantages,” Herald Times Reporter (Wisconsin), Oct. 19,2009, p. 1B.digital mammography offers several advantages over reg-
ular mammography largely because images can be manip-ulated after they are recorded.
Risk Factors
Charles-Harris, Hakan, “Black Women More Likely to DieFrom Breast Cancer,”Miami Times, April 1, 2009, p. 15B.Breast cancer is the leading cancer among white and black
women, but black women are more likely to die from thedisease.
Fahrner, Mari Anne, “Medications Decrease Risk ofBreast Cancer, Studies Find,” St. Louis Post-Dispatch,Aug. 27, 2009, p. B2.Several prevention trials provide evidence that women with
above average risks for breast cancer can decrease the riskswith medication.
Simmons, Shannon, “Diet, Exercise May Help Prevent BreastCancer,” Statesman Journal (Oregon), Oct. 8, 2009, p. 1.a healthy diet and regular exercise can help reduce a woman’s
weight, which in turn reduces her risk for breast cancer.
the next Step:Additional Articles from Current Periodicals
CITING CQ RESEARCHER
Sample formats for citing these reports in a bibliography
include the ones listed below. preferred styles and formats
vary, so please check with your instructor or professor.
mla StyleJost, Kenneth. “Rethinking the death penalty.” cQ Researcher
16 nov. 2001: 945-68.
apa Style
Jost, K. (2001, november 16). Rethinking the death penalty.
CQ Researcher, 11, 945-968.
cHicaGo Style
Jost, Kenneth. “Rethinking the death penalty.” CQ Researcher,
november 16, 2001, 945-968.

ACCESSCQ Researcher is available in print and online. for access, visit your libraryor www.cqresearcher.com.
STAY CURRENTfor notice of upcoming CQ Researcher reports or to learn more about CQResearcher products, subscribe to the free e-mail newsletters, CQ ResearcherAlert! and CQ Researcher News: http://cqpress.com/newsletters.
PURCHASEto purchase a CQ Researcher report in print or electronic format (pdf),visit www.cqpress.com or call 866-427-7737. Single reports start at$15. Bulk purchase discounts and electronic-rights licensing are alsoavailable.
SUBSCRIBEannual full-service CQ Researcher subscriptions—including 44 reports ayear, monthly index updates, and a bound volume—start at $803. add$25 for domestic postage.
CQ Researcher Online offers a backfile from 1991 and a number of toolsto simplify research. for pricing information, call 800-834-9020, or [email protected].
Upcoming Reportsearthquakes, 4/9/10 education Standards, 4/16/10 caring for veterans, 4/23/10
In-depth Reports on Issues in the News
?Are you writing a paper?
Need backup for a debate?
Want to become an expert on an issue?
for more than 80 years, students have turned to CQ Researcher for in-depth reporting onissues in the news. Reports on a full range of political and social issues are now available.following is a selection of recent reports:
Civil Libertiescybersecurity, 2/10press freedom, 2/10Government and Religion, 1/10closing Guantánamo, 2/09affirmative action, 10/08
Crime/Lawprosecuting terrorists, 3/10prisoner Reentry, 12/09interrogating the cia, 9/09examining forensics, 7/09legalizing marijuana, 6/09
EducationHousing the Homeless, 12/09Bilingual education, 12/09value of a college education, 11/09financial literacy, 9/09
Environment/Societyteen pregnancy, 3/10youth violence, 3/10Sex Scandals, 1/10animal Rights, 1/10women in the military, 11/09conspiracy theories, 10/09
Health/Safetymodernizing the Grid, 2/10Sleep deprivation, 2/10professional football, 1/10medication abuse, 10/09nuclear disarmament, 10/09Health-care Reform, 8/09
Politics/Economytea party movement, 3/10State Budget crisis, 9/09Business Bankruptcy, 4/09future of the Gop, 3/09