CPR for Administrative Staff - · PDF fileThe mnemonic for the primary survey is “DRS...
25
1 | Page CPR for Administrative Staff
-
Upload
vuongtuyen -
Category
Documents
-
view
219 -
download
3
Transcript of CPR for Administrative Staff - · PDF fileThe mnemonic for the primary survey is “DRS...

1 | P a g e
CPR for Administrative Staff

2 | P a g e
Welcome to the Wellington Free
Ambulance
CPR Refresher Course
This booklet has been designed for administration staff working in practices.
During the course of your refresher, you will be given many opportunities to practise the skills
associated with this booklet. Additionally, there are large blank areas in your workbooks where we
encourage you to write your own notes.
Remember that you can take the booklet home with you. Any notes you make will be a great resource
to refresh your memory as you read over the booklet later.
Have fun and enjoy your course!
Wellington Free Ambulance
© 2016 Wellington Free Ambulance Service Inc.
The right of Wellington Free Ambulance Service
Inc. to be identified as the author of this
document under section 96 of the Copyright Act
(1994) is hereby asserted.

3 | P a g e
CONTENTS
PRIMARY SURVEY .................................................................................................................................... 4
DANGER .................................................................................................................................................. 5
RESPONSE ............................................................................................................................................... 6
AIRWAY ................................................................................................................................................... 9
BREATHING ........................................................................................................................................... 10
CPR ........................................................................................................................................................ 11
DEFIBRILLATION .................................................................................................................................... 12
CHOKING ............................................................................................................................................... 14
CHEST PAIN ........................................................................................................................................... 19
STROKE .................................................................................................................................................. 23

4 | P a g e
PRIMARY SURVEY The primary survey is the first step in patient assessment. The purpose is to detect potentially life-
threatening conditions or injuries that are immediately treatable.
The mnemonic for the primary survey is “DRS ABCD” (“Doctors ABCD”).

5 | P a g e
DANGER It is not uncommon for a rescuer to be hurt or even die while attempting to provide help. Don’t rush into
a scene. Instead, take a moment to think and decide whether you need to make it safe before
proceeding. It is important that you do not place yourself or others at greater risk than the patient.
If it’s not safe, make it safe
If you can’t make it safe, stay at a safe distance
Never move a patient if moving them could cause
them further injury unless they are in immediate
danger
6 | P a g e
RESPONSE Level of consciousness reflects how normally the brain is functioning. Anything that disrupts the normal
working of the brain will result in an altered level of consciousness.
Call out loudly to the patient and give an instruction
Tap them on the clavicle or, if necessary, you can use a pen and press it firmly into their nail
bed
This will give you an initial level of consciousness (LOC) for the patient on a scale called “AVPU”
(Alert, responds to Voice, responds to Pain, Unresponsive).
A
V
P
U

7 | P a g e
Figure 2
Figure 1
SEND FOR HELP For any serious illness or injury, rapid transport to hospital and advanced care will be required.
Dialling 111 is one of the
most important tasks in a
medical emergency. It is
especially important in cardiac
arrest. Cardiac arrest is when the heart suddenly and unexpectedly stops beating.
It is preferable that you get another person to make the call for you, allowing you to stay with the
patient. Sometimes, however, this is not possible and you must make a decision to either remain with
the patient and administer care or leave them unattended while you go for help.
Situations where you must immediately go for help:
Where it is impossible to approach the casualty because of the dangers to yourself
In adult cardiac arrest where a defibrillator is needed. In
childhood collapse with no signs of breathing and for adult
immersion victims, you would stay and perform CPR for 2 minutes
before going to the phone.
Did you know…?
People who are deaf, hearing or speech
impaired can register with police to join the 111
txt service.
Go to http://www.police.govt.nz/111-txt
and follow the steps in “How to Register”.
8 | P a g e
Speaking to the call taker:
The very first piece of information the call taker will ask you is the location of your emergency. Whilst
this can be frustrating for you, it enables us to send you an ambulance even if the call drops or your cell
phone goes flat.
If we don’t know where you are, we can’t send any help!
The call taker will then begin a sequence of questions that helps us dispatch the best resources for
your emergency. This will not delay the dispatch of the ambulance if you require one. Our ambulances
are dispatched by someone other than the call taker you are speaking too – a dispatcher. All this
happens simultaneously while you are on the phone.
Staying on the line:
Sometimes the call taker will keep you on the line or ask you more detailed questions. This information
is transmitted to the responding ambulance crew as they head toward your emergency.
Giving information:
Try to be specific when speaking to the call taker – remember, they cannot see what is happening and
are reliant on your information. Here is a list of helpful information you could pass on.
Your name
Number that you are calling from
Nearby landmarks e.g. shop names
Number of casualties
If it is a crash, whether anyone is trapped and whether power lines are down
9 | P a g e
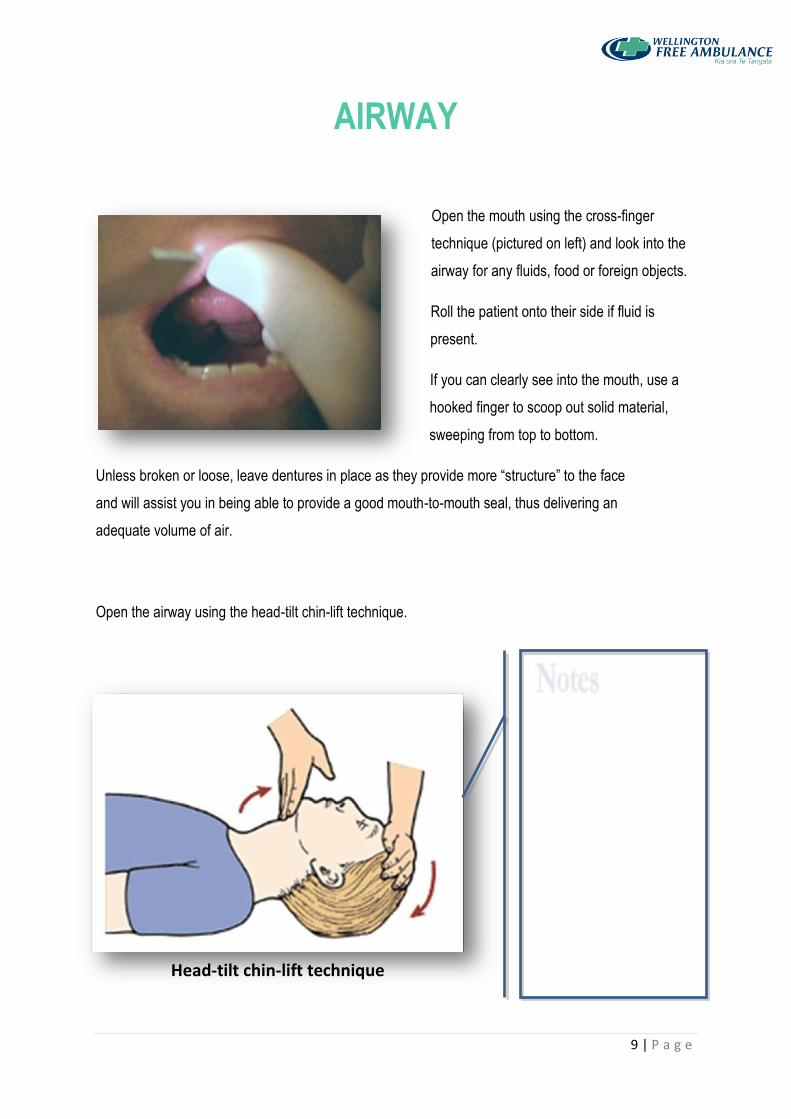
AIRWAY
Open the mouth using the cross-finger
technique (pictured on left) and look into the
airway for any fluids, food or foreign objects.
Roll the patient onto their side if fluid is
present.
If you can clearly see into the mouth, use a
hooked finger to scoop out solid material,
sweeping from top to bottom.
Unless broken or loose, leave dentures in place as they provide more “structure” to the face
and will assist you in being able to provide a good mouth-to-mouth seal, thus delivering an
adequate volume of air.
Open the airway using the head-tilt chin-lift technique.
Head-tilt chin-lift technique
10 | P a g e
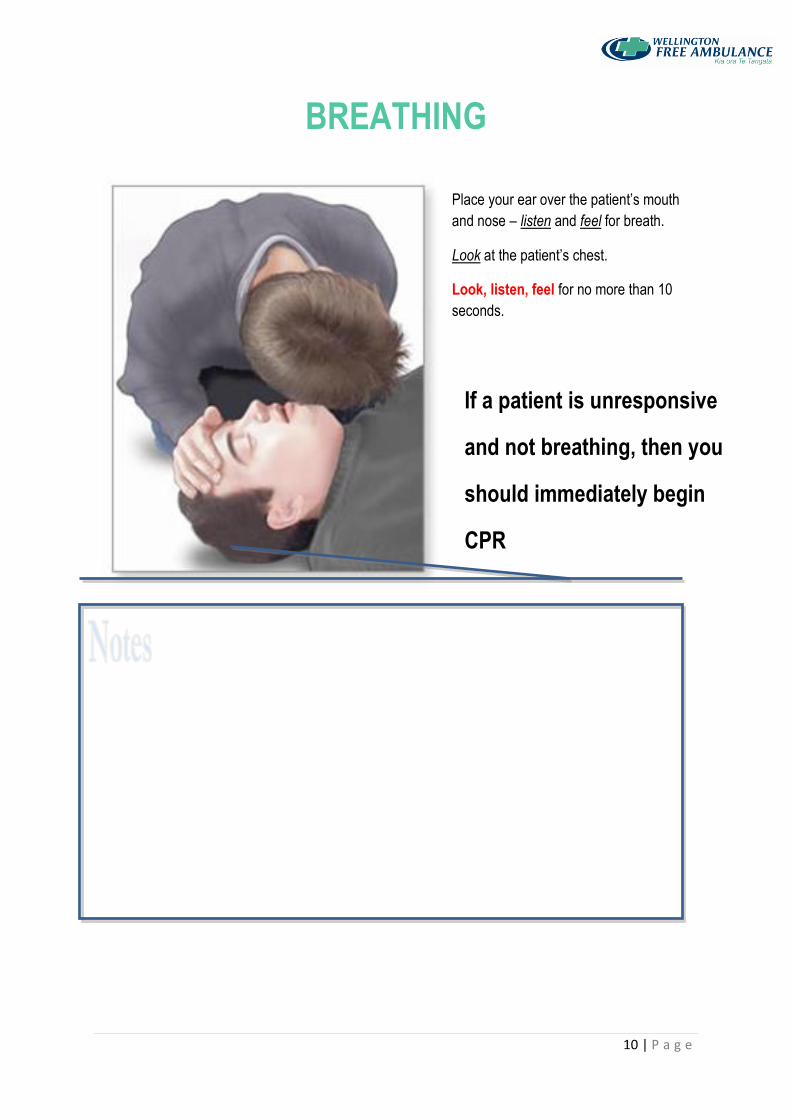
BREATHING
Place your ear over the patient’s mouth
and nose – listen and feel for breath.
Look at the patient’s chest.
Look, listen, feel for no more than 10
seconds.
If a patient is unresponsive
and not breathing, then you
should immediately begin
CPR

11 | P a g e
CPR It is a well-established fact that if a patient is unresponsive and not breathing, then they will have no
pulse.
Don’t waste time looking for something you know will not be there.
Adult
Child
Infant
AGE >8 yrs. 1 – 8 yrs. < 1 yr.
INITIAL BREATH 0 0 0
RATIO 30:2 30:2 30:2
RATE 100 100 100
DEPTH 1/3 of chest 1/3 of chest 1/3 of chest
2
Figure 3

12 | P a g e
DEFIBRILLATION The Automatic External Defibrillator (AED) is only opened and attached to a patient under the following
circumstances. The patient must be:
• Unconscious
• Not breathing normally
Children who have a cardiac arrest often fall into a
rhythm which is not shockable. If this is the case, you
need to continue CPR and follow the voice prompts.
You may use an AED on children. Paediatric pads are preferable, but if there are no paediatric pads,
you may use the adult pads. Pad placement for
children is front/back.
Finally, current research on CPR training tells
us that most lay rescuers and even some
professional rescuers find it very difficult to find
a pulse under emergency conditions. This is
why we start CPR on anyone who is
unconscious and non-breathing. If you have the ability to check for a pulse, then do so, but remember
that the AED is to be attached to any patients who are non-breathing.
13 | P a g e
Safety Considerations
AEDs are very safe, but most rescuers worry about either inappropriately shocking a patient who is not
in cardiac arrest or accidentally shocking another person.
• Inappropriate Shocks – the AED uses a complex set of computer algorithms and needs to be
99% certain that the patient is in cardiac arrest – that is, in VF or VT – before a shock is delivered.
• Occasionally, movement or electrical interference when analysing the cardiac rhythm can
confuse an AED. It is very important to ensure that no one touches the patient while the AED is
analysing the cardiac rhythm and it is also important that cell phones and other electronic
devices are not used within 2 metres of the AED.
Accidental Shocks – the risk of electrical shock to rescuers is very low, provided that there is someone
in overall command of the AED and the resuscitation situation. This person, who may not necessarily
be the most senior or qualified person present, is responsible for ensuring that everyone is clear of the
patient before defibrillating. This involves performing a visual check of bystanders and then self, and
then issuing the warning: “EVERYONE CLEAR” before pressing the SHOCK button and defibrillating.
Advanced rescuers using oxygen therapy to help resuscitate the patient should ensure that it is turned
away from the patient’s chest whilst defibrillation is taking place.
Avoid defibrillating a patient with wet clothing.
Avoid defibrillating a patient who is lying in a puddle of liquid or is in contact with any other
conductive surface e.g. metal.

14 | P a g e
CHOKING Choking is defined as a blocked airway. Anything that blocks an airway causes choking. It can be the
tongue or vomit in an unconscious person lying flat on their back. Normally it refers to an airway that
has been blocked by a solid obstruction.
Normal swallowing
The epiglottis acts as a flap to seal the entrance to the lungs (trachea) and direct food to the stomach
via the food pipe.
Choking
A choking person cannot gasp because food lodged in the trachea blocks the passage of air. The red
arrow shows where the food should have gone to prevent choking.

15 | P a g e
Management
The aim of choking management is to dislodge the obstruction by delivering back blows and/or chest
thrusts which push the obstruction out using pressure from the air trapped in the lungs. Abdominal
thrusts (“Heimlich Manoeuvre”) are no longer used.
Choking can be either partial or complete,
depending on whether the airway is partially or
completely blocked. With partial choking, the
patient can still make noise and will try to get rid of
the obstruction using their cough, gag and swallow
reflex. Encourage them to continue coughing to try
to dislodge the obstruction.
A patient with a complete airway obstruction will
remain silent. Step in and help them immediately.

16 | P a g e
Adults and Children
Ask the patient, “Are you choking?”
If the patient can make a noise, encourage them to
cough.
If the patient is silent or unable to dislodge the obstruction, bend them forward and give them
5 firm back blows between the shoulders.
If this does not dislodge the airway obstruction, give 5 chest thrusts.
Repeat the cycle of back blows and
chest thrusts until they expel the
obstruction or become unconscious.
If the patient becomes unconscious,
place them on the ground and
immediately start CPR.

17 | P a g e
Infants
Give 5 firm back blows between the infant’s
shoulders while supporting the infant on your arm,
with their head down.
Turn the infant over and give 5 chest thrusts while
supporting the infant on your arm, with its head down.
Check airway; scoop any visible obstruction out with a
hooked little finger.
Repeat back blows and chest thrusts until obstruction is removed or infant becomes
unconscious.
Begin CPR immediately if the infant becomes unconscious.

18 | P a g e

19 | P a g e
CHEST PAIN Every time the heart beats, the muscles that make up the walls of the heart
contract, emptying out the chambers. This muscle is fed by coronary
arteries which supply blood that is carrying oxygen and nutrients.
When the heart beats at its normal rate (60-100 beats per minute), the blood
getting through the artery is enough to adequately supply the heart.
If somebody has heart disease (coronary atherosclerosis),
arteries get clogged up with a waxy deposit that makes
them narrow. This process happens over a long period of
time and occurs all over the body. As the arteries get
narrower, less blood flows through them. When the heart
rate increases, the decreased amount of blood flow is
insufficient for the heart. Therefore, the area of muscle
being deprived will start to starve.
As this starvation occurs, the patient gets characteristic
pain in the centre of the chest, known as angina.
Usually this pain will resolve with rest or medication that
specifically targets angina. The most common medication
is GTN or Nitrolingual spray.

20 | P a g e
Sometimes, however, a blood clot can wedge itself into an area
that has already been narrowed, thereby completely occluding
blood flow. This prevents the muscle downstream from receiving
any blood and it starts to die. That area of the heart converts to
scar tissue and is no longer able to contract. This is what is
known as a ‘heart attack’.

21 | P a g e
Signs and symptoms
Chest pain described as heavy, crushing or tight (may have no pain at all)
Shortness of breath
Sense of impending doom
Nausea
Pain radiating down arm or up neck into jaw
Sweating
22 | P a g e
If the signs of a heart attack can be identified quickly enough, we can treat it. The blockage in the
coronary artery can sometimes be removed. This restores blood flow to the starving area of the heart
and stops more heart muscle dying.
Any patient with unrelieved chest pain is having a heart attack until proven otherwise.
Management
Encourage the patient to rest – place them in a sitting position.
Call an ambulance.
Provide reassurance.
Monitor the patient closely – heart attacks are our leading cause of cardiac arrest.
Encourage the patient to take their medication if they have some.

23 | P a g e
STROKE
A cerebrovascular accident (CVA),
commonly known as a stroke, causes
the death of an area of brain by oxygen
starvation due to a blocked or ruptured
blood vessel.
There are two types of CVA. A bleeding
or ‘hemorrhagic’ stroke is caused by a
ruptured blood vessel (usually from an
aneurysm and causes 15% of all CVAs).
The brain beyond the bleed is starved of
blood and oxygen.
A blockage or ‘ischaemic’ stroke is caused by a clot blocking an artery (85% of CVAs). The brain
beyond the obstruction is prevented from receiving blood and oxygen.
Transient ischaemic attack (TIA), also known as a ‘mini stroke’, has symptoms which often resolve
within an hour and will not last more than 24 hours. They are caused by a temporary blockage, often as
a result of high blood pressure. When the blockage is removed or when blood pressure drops, the
syptoms resolve. Until proven otherwise, treat this as a CVA rather than a TIA.
Figure 4

24 | P a g e
Signs and Symptoms
Weakness or paralysis down one side of the body
Very rarely the paralysis can include the whole body
Facial droop
Noisy breathing
Difficulty swallowing
Confusion
Headache (usually only haemorrhagic)
Visual disturbances
Possibly a red flushed face
Slurred or muddled speech
Altered level of consciousness
Management
A patient should be classed as ‘FAST positive’ if they display any or all of the above ‘FAST
symptoms’. If a patient can be transported to an appropriate hospital in less than 2.5 hours of symptom
onset, treatment (known as thrombolysis) may be able to dissolve the clot of an ischaemic stroke and
prevent irreparable damage. Therefore, it is essential to call 111 as soon as you notice any warning
signs and take note of the time of onset so you can communicate this information to emergency
personnel.
Figure 5

25 | P a g e
References
Figure 1 Retrieved from http://www.nsupport.co.nz/?page_id=78
Figure 2 Retrieved from http://www.stjohn.org.nz/What-we-do/When-to-call-111/
Figure 3 Retrieved from http://www.nzrc.org.nz/assets/Uploads/Guidelines/guideline-6dec10.pdf
Figure 4 Retrieved from http://floydmemorial.com/healthscope/understanding-stroke-the-basics/
Figure 5 Retrieved from http://www.health.govt.nz/your-health/conditions-and-
treatments/diseases-and-illnesses/stroke