CPHQ Secrets - phtrainee.comphtrainee.com/wp-content/uploads/2018/12/CPHQ-SECRETS.pdf · the CPHQ...
190
ProductID: CPHQ C C P P H H Q Q S S e e c c r r e e t t s s Your Key to Certified Professional In Healthcare Quality Test Success
Transcript of CPHQ Secrets - phtrainee.comphtrainee.com/wp-content/uploads/2018/12/CPHQ-SECRETS.pdf · the CPHQ...
ProductID: CPHQ
CCPPHHQQ SSeeccrreettss
Your Key to Certified Professional In Healthcare Quality Test Success
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
2
From the Director of Test-Taking Strategy-
Dear future CPHQ Success Story:
Congratulations on your purchase of the most advanced test-taking manual
for the CPHQ certification test. Notice I did not say study guide- there are
plenty of decent study guides on the market, but that was not our objective in
writing this manual. Our goal is to seek and exploit specific weaknesses in
the CPHQ assessment, and then share those secrets with our customers.
Let’s be perfectly honest here- you’ve worked hard enough in college, and if
you want to spend hours in a study guide to boost your score, that’s a great
thing to do. In fact, we recommend at least a brief review of some of the
better study guides on the market. But that’s simply not enough to do well in
the high-pressure high-stakes environment of the test day. How well you do
on this test will have a significant impact on your future- and we have the
research and practical advice to help you execute on test day.
The product you’re reading now is much more than a study guide- it is a
tactical weapon designed to exploit weaknesses in the test itself, and help
you avoid the most common errors test takers make when taking the CPHQ
test.
How to use this manual
We don’t want to waste your time. This manual is fast-paced and fluff-free.
We suggest going through it a number of times, trying out its methods on a
number of practice tests.
First, read through the manual completely to get a feel for the content and
organization. Read the general success strategies first, and then proceed to
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
3
the individual test sections. Each tip has been carefully selected for its
effectiveness.
Second, read through the manual again, and take notes in the margins and
highlight those sections where you may have a particular weakness (we
strongly suggest printing the manual out on a high-quality printer).
Finally, bring the manual with you on test day and study it before the exam
begins.
Your success is our success
We would be delighted to hear your CPHQ Success Story. Send us an email
and tell us your story. Thanks for your business and we wish you continued
success-
Sincerely,
The CPHQ Certification Secrets Team

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
4
Table of Contents Table of Contents..................................................................................................4
Secret Key #1 – Time is Your Greatest Enemy ....................................................8
Pace Yourself ................................................................................................8
Secret Key #2 – Guessing is not Guesswork......................................................10
Monkeys Take the CPHQ................................................................................10
Success Strategy #2 .......................................................................................11
Secret Key #3 – Practice Smarter, Not Harder ...................................................13
Success Strategy #3 .......................................................................................13
Secret Key #4 – Prepare, Don’t Procrastinate ....................................................14
Secret Key #5 – Test Yourself ............................................................................15
Success Strategy #5 .......................................................................................15
Top 20 Test Taking Tips .....................................................................................16
General Strategies ..............................................................................................17
Make Predictions .........................................................................................17
Answer the Question ...................................................................................17
Benchmark...................................................................................................18
Valid Information..........................................................................................18
Avoid “Fact Traps” .......................................................................................18
Milk the Question .........................................................................................19
The Trap of Familiarity.................................................................................19
Eliminate Answers .......................................................................................20
Tough Questions .........................................................................................20
Brainstorm ...................................................................................................20
Read Carefully .............................................................................................21
Face Value...................................................................................................21
Prefixes........................................................................................................21
Hedge Phrases ............................................................................................22
Switchback Words .......................................................................................22
New Information...........................................................................................22
Time Management.......................................................................................22
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
5
Contextual Clues .........................................................................................23
Don’t Panic ..................................................................................................23
Pace Yourself ..............................................................................................23
Answer Selection .........................................................................................23
Check Your Work.........................................................................................24
Beware of Directly Quoted Answers ............................................................24
Slang ...........................................................................................................24
Extreme Statements ....................................................................................25
Answer Choice Families ..............................................................................25
Why Certify? .......................................................................................................26
Score...............................................................................................................26
Seven Pillars of Quality.......................................................................................28
Emphasis on Outcomes......................................................................................31
Managed Care ....................................................................................................35
Medical Management Terms...........................................................................37
Organizational Effectiveness ..............................................................................42
What are Ethics?.................................................................................................47
What is Organizational Structure? ......................................................................49
Healthcare Organizations and Data Banks .........................................................51
HQCB/NAHQ...................................................................................................51
Health Care Quality Improvement Program ....................................................53
National Practitioner Data Bank (NPDB) .........................................................54
Healthcare Integrity and Protection Data Bank ...............................................56
Key Thinkers and Management Tools ................................................................58
Dr. Kaoru Ishikawa ..........................................................................................58
Dr. Joseph Juran .............................................................................................59
Affinity Diagram...............................................................................................62
Brainstorming ..................................................................................................63
Prioritization Matrix..........................................................................................64
Gantt charts.....................................................................................................65
Delphi Technique ............................................................................................67

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
6
Other Tools .....................................................................................................71
Quality Management Principles ..........................................................................73
Uniform Hospital Discharge Data Set (UHDDS) .................................................79
Individual Differences in Organizations - Personality ..........................................84
Attitudes & Behaviors..........................................................................................87
The Perceptual Process......................................................................................90
Training & Development .....................................................................................92
Managing Work Motivation .................................................................................95
Business and Its Environment ............................................................................97
Accounting/Budgets ..........................................................................................102
Budgets .........................................................................................................104
Communication in Organizations ......................................................................108
Leadership ........................................................................................................111
Stress Management..........................................................................................113
What is Decision Making?.................................................................................115
Compensation & Benefits .................................................................................119
Managing Teams ..............................................................................................126
Occupational Safety and Health .......................................................................129
Emergency Preparedness.............................................................................133
Key Legal Acts ..................................................................................................134
Safe Medical Device Act of 1990...................................................................134
Clinical Laboratory Improvement Amendments Act of 1988..........................136
Americans with Disabilities Act......................................................................136
Medicare changes from the Balanced Budget Refinement Act (BBRA) of 1999
......................................................................................................................138
Distribution of Increased Payments to Medicare + Choice Organizations under
the Medicare, Medicaid, and SCHIP Benefits Improvement and Protection Act
of 2000 ..........................................................................................................140
COBRA .........................................................................................................145
Medicare Conditions of Participation For Hospitals .......................................151

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
7
The Malcolm Baldrige National Quality Improvement Act of 1987 - Public Law
100-107 .........................................................................................................156
Organizational Exit............................................................................................159
Statistics ...........................................................................................................162
Special Report: Which Study Guides and Practice Tests Are Worth Your Time
..........................................................................................................................166
Practice Tests................................................................................................166
Study Guides.................................................................................................166
Special Report: Retaking the Test: What Are Your Chances at Improving Your
Score? ..............................................................................................................167
Special Report: Ethics Research and Websites................................................170
Special Report: Key Formulas ..........................................................................171
Special Report: What is Test Anxiety and How to Overcome It? ......................175
Lack of Preparation .......................................................................................175
Physical Signals ............................................................................................176
Nervousness .................................................................................................177
Study Steps...................................................................................................180
Helpful Techniques........................................................................................182
Special Report: Additional Bonus Material........................................................190
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
8
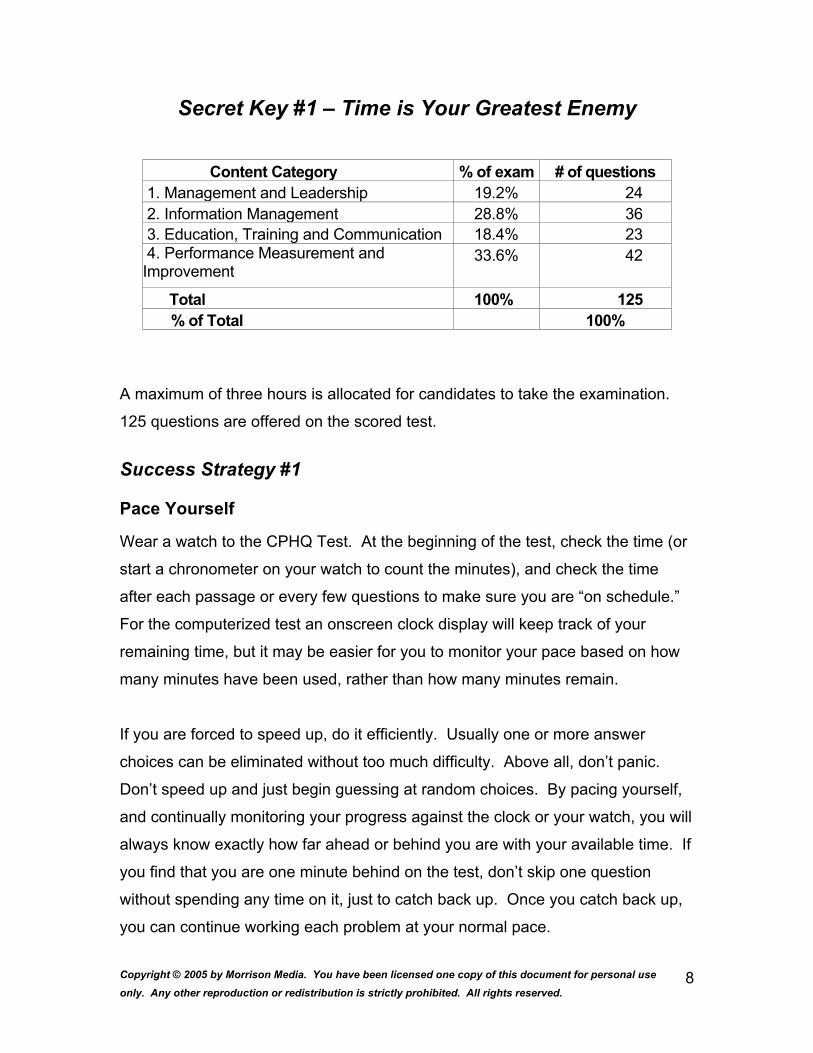
Secret Key #1 – Time is Your Greatest Enemy
Content Category % of exam # of questions1. Management and Leadership 19.2% 24 2. Information Management 28.8% 36 3. Education, Training and Communication 18.4% 23 4. Performance Measurement and Improvement
33.6% 42
Total 100% 125 % of Total 100%
A maximum of three hours is allocated for candidates to take the examination.
125 questions are offered on the scored test.
Success Strategy #1
Pace Yourself
Wear a watch to the CPHQ Test. At the beginning of the test, check the time (or
start a chronometer on your watch to count the minutes), and check the time
after each passage or every few questions to make sure you are “on schedule.”
For the computerized test an onscreen clock display will keep track of your
remaining time, but it may be easier for you to monitor your pace based on how
many minutes have been used, rather than how many minutes remain.
If you are forced to speed up, do it efficiently. Usually one or more answer
choices can be eliminated without too much difficulty. Above all, don’t panic.
Don’t speed up and just begin guessing at random choices. By pacing yourself,
and continually monitoring your progress against the clock or your watch, you will
always know exactly how far ahead or behind you are with your available time. If
you find that you are one minute behind on the test, don’t skip one question
without spending any time on it, just to catch back up. Once you catch back up,
you can continue working each problem at your normal pace.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
9
Furthermore, don’t dwell on the problems that you were rushed on. If a problem
was taking up too much time and you made a hurried guess, it must be difficult.
The difficult questions are the ones you are most likely to miss anyway, so it isn’t
a big loss. It is better to end with more time than you need than to run out of
time. You can always go back and work the problems that you skipped. If you
have time left over, as you review the skipped questions, start at the earliest
skipped question, spend at most another minute, and then move on to the next
skipped question.
Lastly, sometimes it is beneficial to slow down if you are constantly getting ahead
of time. You are always more likely to catch a careless mistake by working more
slowly than quickly, and among very high-scoring test takers (those who are
likely to have lots of time left over), careless errors affect the score more than
mastery of material.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
10
Secret Key #2 – Guessing is not Guesswork
You probably know that guessing is a good idea on the CPHQ test- unlike other
standardized tests, there is no penalty for getting a wrong answer. Even if you
have no idea about a question, you still have a 20-25% chance of getting it right.
Most test takers do not understand the impact that proper guessing can have on
their score. Unless you score extremely high, guessing will significantly
contribute to your final score.
KEY POINT: THERE IS NO PENALTY FOR GUESSING ON THE CPHQ.
Monkeys Take the CPHQ
What most test takers don’t realize is that to insure that 20-25% chance, you
have to guess randomly. If you put 20 monkeys in a room to take this test,
assuming they answered once per question and behaved themselves, on
average they would get 20-25% of the questions correct. Put 20 test takers in
the room, and the average will be much lower among guessed questions. Why?
1. This test intentionally writes deceptive answer choices that “look” right. A test
taker has no idea about a question, so picks the “best looking” answer, which
is often wrong. The monkey has no idea what looks good and what doesn’t,
so will consistently be lucky about 20-25% of the time.
2. Test takers will eliminate answer choices from the guessing pool based on a
hunch or intuition. Simple but correct answers often get excluded, leaving a
0% chance of being correct. The monkey has no clue, and often gets lucky
with the best choice.
This is why the process of elimination endorsed by most test courses is flawed
and detrimental to your performance- test takers don’t guess, they make an
ignorant stab in the dark that is usually worse than random.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
11
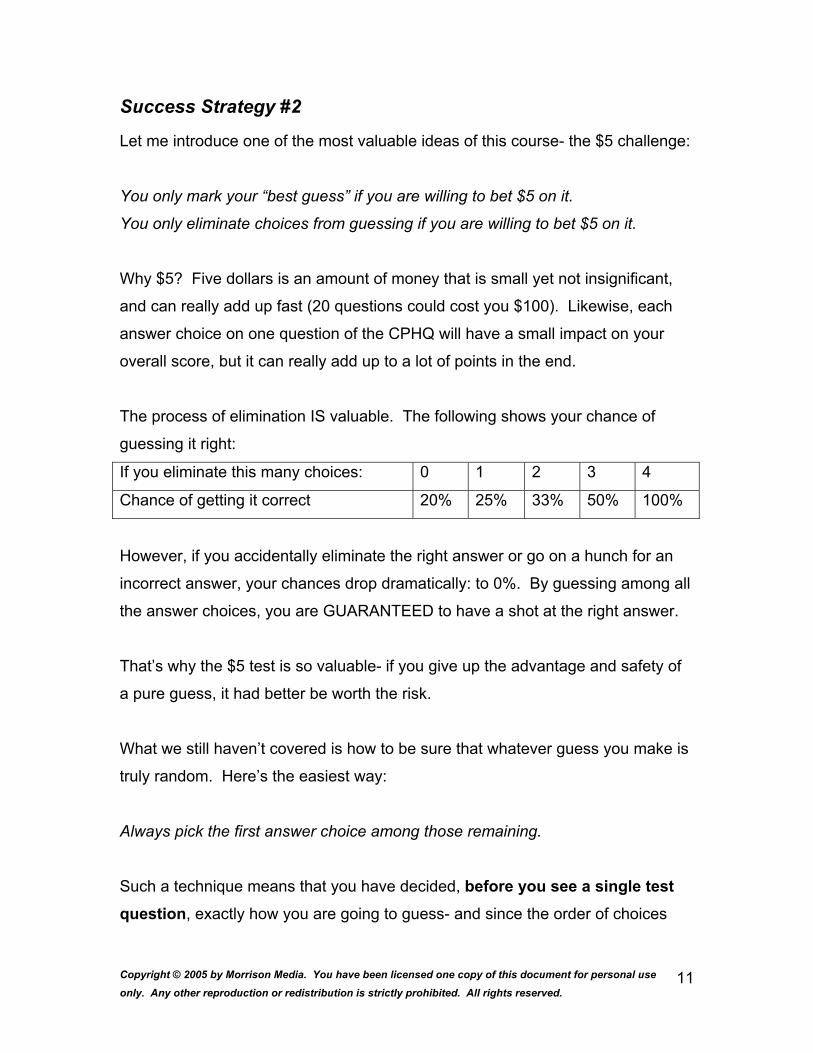
Success Strategy #2
Let me introduce one of the most valuable ideas of this course- the $5 challenge:
You only mark your “best guess” if you are willing to bet $5 on it.
You only eliminate choices from guessing if you are willing to bet $5 on it.
Why $5? Five dollars is an amount of money that is small yet not insignificant,
and can really add up fast (20 questions could cost you $100). Likewise, each
answer choice on one question of the CPHQ will have a small impact on your
overall score, but it can really add up to a lot of points in the end.
The process of elimination IS valuable. The following shows your chance of
guessing it right:
If you eliminate this many choices: 0 1 2 3 4
Chance of getting it correct 20% 25% 33% 50% 100%
However, if you accidentally eliminate the right answer or go on a hunch for an
incorrect answer, your chances drop dramatically: to 0%. By guessing among all
the answer choices, you are GUARANTEED to have a shot at the right answer.
That’s why the $5 test is so valuable- if you give up the advantage and safety of
a pure guess, it had better be worth the risk.
What we still haven’t covered is how to be sure that whatever guess you make is
truly random. Here’s the easiest way:
Always pick the first answer choice among those remaining.
Such a technique means that you have decided, before you see a single test question, exactly how you are going to guess- and since the order of choices

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
12
tells you nothing about which one is correct, this guessing technique is perfectly
random.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
13
Secret Key #3 – Practice Smarter, Not Harder
Many test takers delay the test preparation process because they dread the
awful amounts of practice time they think necessary to succeed on the test. We
have refined an effective method that will take you only a fraction of the time.
There are a number of “obstacles” in your way on the CPHQ test. Among these
are answering questions, finishing in time, and mastering test-taking strategies.
All must be executed on the day of the test at peak performance, or your score
will suffer. The CPHQ is a mental marathon that has a large impact on your
future.
Just like a marathon runner, it is important to work your way up to the full
challenge. So first you just worry about questions, and then time, and finally
strategy:
Success Strategy #3
1. Find a good source for practice tests.
2. If you are willing to make a larger time investment, consider using more
than one study guide- often the different approaches of multiple authors
will help you “get” difficult concepts.
3. Take a practice test with no time constraints, with all study helps “open
book.” Take your time with questions and focus on applying strategies.
4. Take a practice test with time constraints, with all guides "open book."
5. Take a final practice test with no open material and time limits
If you have time to take more practice tests, just repeat step 5. By gradually
exposing yourself to the full rigors of the test environment, you will condition
your mind to the stress of test day and maximize your success.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
14
Secret Key #4 – Prepare, Don’t Procrastinate
Let me state an obvious fact: if you take the CPHQ exam three times, you will get
three different scores. This is due to the way you feel on test day, the level of
preparedness you have, and, despite CPHQ exam’s claims to the contrary, some
tests WILL be easier for you than others.
Since your future depends so much on your score, you should maximize your
chances of success. In order to maximize the likelihood of success, you’ve got to
prepare in advance. This means taking practice tests and spending time learning
the information and test taking strategies you will need to succeed.
Since you have to pay a registration fee each time you take the CPHQ exam,
don’t take it as a “practice” test. Feel free to take sample tests on your own, but
when you go to take the CPHQ exam, be prepared, be focused, and do your best
the first time!
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
15
Secret Key #5 – Test Yourself
Everyone knows that time is money. There is no need to spend too much of your
time or too little of your time preparing for the CPHQ exam. You should only
spend as much of your precious time preparing as is necessary for you to pass it.
Success Strategy #5
Once you have taken a practice test under real conditions of time constraints,
then you will know if you are ready for the test or not.
If you have scored extremely high the first time that you take the practice test,
then there is not much point in spending countless hours studying. You are
already there.
Benchmark your abilities by retaking practice tests and seeing how much you
have improved. Once you score high enough to guarantee success, then you
are ready.
If you have scored well below where you need, then knuckle down and begin
studying in earnest. Check your improvement regularly through the use of
practice tests under real conditions. Above all, don’t worry, panic, or give up.
The key is perseverance!
Then, when you go to take the CPHQ exam, remain confident and remember
how well you did on the practice tests. If you can score high enough on a
practice test, then you can do the same on the real thing.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
16
Top 20 Test Taking Tips
1. Carefully follow all the test registration procedures
2. Know the test directions, duration, topics, question types, how many
questions
3. Setup a flexible study schedule at least 3-4 weeks before test day
4. Study during the time of day you are most alert, relaxed, and stress free
5. Maximize your learning style; visual learner use visual study aids, auditory
learner use auditory study aids
6. Focus on your weakest knowledge base
7. Find a study partner to review with and help clarify questions
8. Practice, practice, practice
9. Get a good night’s sleep; don’t try to cram the night before the test
10. Eat a well balanced meal
11. Know the exact physical location of the testing site; drive the route to the
site prior to test day
12. Bring a set of ear plugs; the testing center could be noisy
13. Wear comfortable, loose fitting, layered clothing to the testing center;
prepare for it to be either cold or hot during the test
14. Bring at least 2 current forms of ID to the testing center
15. Arrive to the test early; be prepared to wait and be patient
16. Eliminate the obviously wrong answer choices, then guess the first
remaining choice
17. Pace yourself; don’t rush, but keep working and move on if you get stuck
18. Maintain a positive attitude even if the test is going poorly
19. Keep your first answer unless you are positive it is wrong
20. Check your work, don’t make a careless mistake

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
17
General Strategies
The most important thing you can do is to ignore your fears and jump into the test
immediately- do not be overwhelmed by any strange-sounding terms. You have
to jump into the test like jumping into a pool- all at once is the easiest way.
Make Predictions
As you read and understand the question, try to guess what the answer will be.
Remember that several of the answer choices are wrong, and once you begin
reading them, your mind will immediately become cluttered with answer choices
designed to throw you off. Your mind is typically the most focused immediately
after you have read the question and digested its contents. If you can, try to
predict what the correct answer will be. You may be surprised at what you can
predict.
Quickly scan the choices and see if your prediction is in the listed answer
choices. If it is, then you can be quite confident that you have the right answer.
It still won’t hurt to check the other answer choices, but most of the time, you’ve
got it!
Answer the Question
It may seem obvious to only pick answer choices that answer the question, but
the test writers can create some excellent answer choices that are wrong. Don’t
pick an answer just because it sounds right, or you believe it to be true. It MUST
answer the question. Once you’ve made your selection, always go back and
check it against the question and make sure that you didn’t misread the question,
and the answer choice does answer the question posed.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
18
Benchmark
After you read the first answer choice, decide if you think it sounds correct or not.
If it doesn’t, move on to the next answer choice. If it does, mentally mark that
answer choice. This doesn’t mean that you’ve definitely selected it as your
answer choice, it just means that it’s the best you’ve seen thus far. Go ahead
and read the next choice. If the next choice is worse than the one you’ve already
selected, keep going to the next answer choice. If the next choice is better than
the choice you’ve already selected, mentally mark the new answer choice as
your best guess.
The first answer choice that you select becomes your standard. Every other
answer choice must be benchmarked against that standard. That choice is
correct until proven otherwise by another answer choice beating it out. Once
you’ve decided that no other answer choice seems as good, do one final check
to ensure that your answer choice answers the question posed.
Valid Information
Don’t discount any of the information provided in the question. Every piece of
information may be necessary to determine the correct answer. None of the
information in the question is there to throw you off (while the answer choices will
certainly have information to throw you off). If two seemingly unrelated topics are
discussed, don’t ignore either. You can be confident there is a relationship, or it
wouldn’t be included in the question, and you are probably going to have to
determine what is that relationship to find the answer.
Avoid “Fact Traps”
Don’t get distracted by a choice that is factually true. Your search is for the
answer that answers the question. Stay focused and don’t fall for an answer that
is true but incorrect. Always go back to the question and make sure you’re
choosing an answer that actually answers the question and is not just a true
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
19
statement. An answer can be factually correct, but it MUST answer the question
asked. Additionally, two answers can both be seemingly correct, so be sure to
read all of the answer choices, and make sure that you get the one that BEST
answers the question.
Milk the Question
Some of the questions may throw you completely off. They might deal with a
subject you have not been exposed to, or one that you haven’t reviewed in years.
While your lack of knowledge about the subject will be a hindrance, the question
itself can give you many clues that will help you find the correct answer. Read
the question carefully and look for clues. Watch particularly for adjectives and
nouns describing difficult terms or words that you don’t recognize. Regardless of
if you completely understand a word or not, replacing it with a synonym either
provided or one you more familiar with may help you to understand what the
questions are asking. Rather than wracking your mind about specific detailed
information concerning a difficult term or word, try to use mental substitutes that
are easier to understand.
The Trap of Familiarity
Don’t just choose a word because you recognize it. On difficult questions, you
may not recognize a number of words in the answer choices. The test writers
don’t put “make-believe” words on the test; so don’t think that just because you
only recognize all the words in one answer choice means that answer choice
must be correct. If you only recognize words in one answer choice, then focus
on that one. Is it correct? Try your best to determine if it is correct. If it is, that is
great, but if it doesn’t, eliminate it. Each word and answer choice you eliminate
increases your chances of getting the question correct, even if you then have to
guess among the unfamiliar choices.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
20
Eliminate Answers
Eliminate choices as soon as you realize they are wrong. But be careful! Make
sure you consider all of the possible answer choices. Just because one appears
right, doesn’t mean that the next one won’t be even better! The test writers will
usually put more than one good answer choice for every question, so read all of
them. Don’t worry if you are stuck between two that seem right. By getting down
to just two remaining possible choices, your odds are now 50/50. Rather than
wasting too much time, play the odds. You are guessing, but guessing wisely,
because you’ve been able to knock out some of the answer choices that you
know are wrong. If you are eliminating choices and realize that the last answer
choice you are left with is also obviously wrong, don’t panic. Start over and
consider each choice again. There may easily be something that you missed the
first time and will realize on the second pass.
Tough Questions
If you are stumped on a problem or it appears too hard or too difficult, don’t
waste time. Move on! Remember though, if you can quickly check for obviously
incorrect answer choices, your chances of guessing correctly are greatly
improved. Before you completely give up, at least try to knock out a couple of
possible answers. Eliminate what you can and then guess at the remaining
answer choices before moving on.
Brainstorm
If you get stuck on a difficult question, spend a few seconds quickly
brainstorming. Run through the complete list of possible answer choices. Look
at each choice and ask yourself, "Could this answer the question satisfactorily?"
Go through each answer choice and consider it independently of the other. By
systematically going through all possibilities, you may find something that you
would otherwise overlook. Remember that when you get stuck, it’s important to
try to keep moving.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
21
Read Carefully
Understand the problem. Read the question and answer choices carefully. Don’t
miss the question because you misread the terms. You have plenty of time to
read each question thoroughly and make sure you understand what is being
asked. Yet a happy medium must be attained, so don’t waste too much time.
You must read carefully, but efficiently.
Face Value
When in doubt, use common sense. Always accept the situation in the problem
at face value. Don’t read too much into it. These problems will not require you to
make huge leaps of logic. The test writers aren’t trying to throw you off with a
cheap trick. If you have to go beyond creativity and make a leap of logic in order
to have an answer choice answer the question, then you should look at the other
answer choices. Don’t overcomplicate the problem by creating theoretical
relationships or explanations that will warp time or space. These are normal
problems rooted in reality. It’s just that the applicable relationship or explanation
may not be readily apparent and you have to figure things out. Use your common
sense to interpret anything that isn’t clear.
Prefixes
If you're having trouble with a word in the question or answer choices, try
dissecting it. Take advantage of every clue that the word might include. Prefixes
and suffixes can be a huge help. Usually they allow you to determine a basic
meaning. Pre- means before, post- means after, pro - is positive, de- is negative.
From these prefixes and suffixes, you can get an idea of the general meaning of
the word and try to put it into context. Beware though of any traps. Just because
con is the opposite of pro, doesn’t necessarily mean congress is the opposite of
progress!

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
22
Hedge Phrases
Watch out for critical “hedge” phrases, such as likely, may, can, will often,
sometimes, often, almost, mostly, usually, generally, rarely, sometimes.
Question writers insert these hedge phrases to cover every possibility. Often an
answer choice will be wrong simply because it leaves no room for exception.
Avoid answer choices that have definitive words like “exactly,” and “always”.
Switchback Words
Stay alert for “switchbacks”. These are the words and phrases frequently used to
alert you to shifts in thought. The most common switchback word is “but”.
Others include although, however, nevertheless, on the other hand, even though,
while, in spite of, despite, regardless of.
New Information
Correct answer choices will rarely have completely new information included.
Answer choices typically are straightforward reflections of the material asked
about and will directly relate to the question. If a new piece of information is
included in an answer choice that doesn't even seem to relate to the topic being
asked about, then that answer choice is likely incorrect. All of the information
needed to answer the question is usually provided for you, and so you should not
have to make guesses that are unsupported or choose answer choices that
require unknown information that cannot be reasoned on its own.
Time Management
On technical questions, don’t get lost on the technical terms. Don’t spend too
much time on any one question. If you don’t know what a term means, then
since you don’t have a dictionary, odds are you aren’t going to get much further.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
23
You should immediately recognize terms as whether or not you know them. If
you don’t, work with the other clues that you have, the other answer choices and
terms provided, but don’t waste too much time trying to figure out a difficult term.
Contextual Clues
Look for contextual clues. An answer can be right but not correct. The
contextual clues will help you find the answer that is most right and is correct.
Understand the context in which a phrase or statement is made. This will help
you make important distinctions.
Don’t Panic
Panicking will not answer any questions for you. Therefore, it isn’t helpful. When
you first see the question, if your mind goes blank, take a deep breath. Force
yourself to mechanically go through the steps of solving the problem and using
the strategies you've learned.
Pace Yourself
Don’t get clock fever. It’s easy to be overwhelmed when you’re looking at a page
full of questions, your mind is full of random thoughts and feeling confused, and
the clock is ticking down faster than you would like. Calm down and maintain the
pace that you have set for yourself. As long as you are on track by monitoring
your pace, you are guaranteed to have enough time for yourself. When you get
to the last few minutes of the test, it may seem like you won’t have enough time
left, but if you only have as many questions as you should have left at that point,
then you’re right on track!
Answer Selection
The best way to pick an answer choice is to eliminate all of those that are wrong,
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
24
until only one is left and confirm that is the correct answer. Sometimes though,
an answer choice may immediately look right. Be careful! Take a second to
make sure that the other choices are not equally obvious. Don’t make a hasty
mistake. There are only two times that you should stop before checking other
answers. First is when you are positive that the answer choice you have
selected is correct. Second is when time is almost out and you have to make a
quick guess!
Check Your Work
Since you will probably not know every term listed and the answer to every
question, it is important that you get credit for the ones that you do know. Don’t
miss any questions through careless mistakes. If at all possible, try to take a
second to look back over your answer selection and make sure you’ve selected
the correct answer choice and haven’t made a costly careless mistake (such as
marking an answer choice that you didn’t mean to mark). This quick double
check should more than pay for itself in caught mistakes for the time it costs.
Beware of Directly Quoted Answers
Sometimes an answer choice will repeat word for word a portion of the question
or reference section. However, beware of such exact duplication – it may be a
trap! More than likely, the correct choice will paraphrase or summarize a point,
rather than being exactly the same wording.
Slang
Scientific sounding answers are better than slang ones. An answer choice that
begins “To compare the outcomes…” is much more likely to be correct than one
that begins “Because some people insisted…”

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
25
Extreme Statements
Avoid wild answers that throw out highly controversial ideas that are proclaimed
as established fact. An answer choice that states the “process should used in
certain situations, if…” is much more likely to be correct than one that states the
“process should be discontinued completely.” The first is a calm rational
statement and doesn’t even make a definitive, uncompromising stance, using a
hedge word “if” to provide wiggle room, whereas the second choice is a radical
idea and far more extreme.
Answer Choice Families
When you have two or more answer choices that are direct opposites or
parallels, one of them is usually the correct answer. For instance, if one answer
choice states “x increases” and another answer choice states “x decreases” or “y
increases,” then those two or three answer choices are very similar in
construction and fall into the same family of answer choices. A family of answer
choices is when two or three answer choices are very similar in construction, and
yet often have a directly opposite meaning. Usually the correct answer choice
will be in that family of answer choices. The “odd man out” or answer choice that
doesn’t seem to fit the parallel construction of the other answer choices is more
likely to be incorrect.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
26
Why Certify?
CPHQ: Certified Professional In Healthcare Quality
• Raise the standards in your field and distinguish your experience.
• Use your credentials to further your career.
• Improve your skills and abilities to manage workers
Candidate Handbook
http://www.cphq.org/examin.html
Score
In addition to the 125 scored questions, CPHQ examinations also include an
additional 15 pretest questions. You will be asked to answer these questions,
however, they will not be included in the scored examination result.
The CPHQ uses the following percentage guidelines in selecting the three types
of questions that appear on each examination: 32% recall, 53% application, and
15% analysis. Recall questions test the candidate’s knowledge of specific facts
and concepts. Application questions require the candidate to interpret or apply
information to a situation. Analysis questions test the candidate’s ability to
evaluate, problem solve or integrate a variety of information and/or judgment
into a meaningful whole.
Scores are reported in written form only, in person or by U.S. mail. The score
report will reflect either “pass” or “fail,” followed by a raw score indicating the
number of questions you answered correctly. Additional detail is provided in the
form of raw scores by each of the four major content categories. This

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
27
information is provided as feedback to help you understand your performance
within the major content categories. Your pass/fail status is determined by your
overall raw score for the entire examination.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
28
Seven Pillars of Quality
1. Efficacy
This deals with a controlled environment and examines what is possible. It sets
an upper boundary for quality and establishes the ideal to which all should aspire.
However, as we know, the real world is very different to the laboratory. It is likely
that the less control that is exerted over the environment, the less probable it is
that practitioners are able to meet these standards.
2. Effectiveness
The second pillar of quality is "effectiveness" i.e. to what extent does the service
achieve its intended outcomes in a real world environment? Social, economic
and individual factors influence the selection of quality indicators. Various
indicators have been developed such as cost effective, socially effective and
individually effective although the way in which they are measured is not always
universally agreed.
3. Efficiency
The third pillar of quality is "efficiency". This examines the extent to which scarce
resources are used to derive the greatest benefits with the least waste. This is
usually measured by examining the ratio between the costs and benefits of a
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
29
service and comparing these with others who are providing the same or similar
services. This measure is typically used by socio-economic forces seeking to
select a service which will result in reduced costs. The assumption is made that
the benefit stays the same, an assumption that is frequently not tested.
4. Acceptability
The fourth pillar is acceptability. This concentrates on the usefulness of the
service to the patient and its perceived impact on his/ her quality of life. It takes
into consideration patient preferences regarding access to the service (eg.
advice), relationship with health service providers (eg trust, confidentiality), the
amenities in which the service is provided and the cost utility relationship.
5. Optimality
The fifth pillar is optimality. From the point of view of society and the economic
system, it is necessary to ensure that the optimum allocation of resources is
achieved relative to the benefits derived from the services provided. Techniques
such as cost benefit analysis and marginal costing are used to identify the
optimum point of resource allocation: benefits. Quality indicators are usually of a
global socio-economic nature. Neither the individual service provider nor patient
are concerned with these indicators. However, data collection starts at the
interface between the two and these desire for maximal rather than optimal
benefits may adversely influence the selection of appropriate indicators.
6. Equity
The sixth pillar is equity. Society is concerned that every person should receive
equal treatment, or at best fair treatment. Equity is compromised when the quality
of service or even the range of services is determined by the patient's ability to
pay for the service. Since third party payers play a significant role in the health
care system, equity would be affected by the extent to which a third party payer
includes a fee for the service in the benefits that it offers it members.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
30
7. Legitimacy
The seventh and final pillar is legitimacy. This is similar to the concept of
acceptability except that "the preferences and values for legitimacy are
expressed through a societal rather than an individual perspective". Clearly,
society requires evidence upon which to make these judgements.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
31
Emphasis on Outcomes
1. Accountability for Outcomes
Amongst all this disruption, there has been an increase in focus on the
accountability of health professionals. They are being challenged to improve
quality with the major emphasis on outcomes based medicine. Social and
economic institutions are demanding that standards be set and quality measured
as a condition of professional recognition. As Holdford and Smith (1997) state
"Outcome measures have emerged as a primary research focus for medical
disciplines as a result of demand by health care payers and the public for
justification of the rising costs of care. Health care consumers demand that
providers report the outcomes achieved for the health care dollars spent, whilst
providers realize that they must demonstrate the value of their services and
products".
2. Outcome models
Health outcomes have been variously defined and classified. Lohr (1988) defined
health outcomes in terms of the result of medical care. She characterized these
as one or more of the five D's: death, disease, disability, discomfort, and
dissatisfaction.
Kozma et al ( 1993) described three outcomes in terms of their ECHO model.
Economic outcomes are based on a comparison between the costs of what was
received and the benefit derived from alternatives. Clinical outcomes are
changes to morbidity and mortality rates which result from health care
interventions. Humanistic outcomes are the psychological consequences of
health care which include patient measures of functional status, quality of life and
satisfaction with care. This model is useful because it incorporates measures of
value, not merely costs, and it urges health care providers to take all three
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
32
outcome measures into account when considering alternative intervention
strategies.
3. RELATIONSHIP BETWEEN OUTCOMES AND QUALITY
In 1994 Mount wrote:
"If the past four years are typical of the next six, the 1990's may come to be
called the "quality" decade. Whether one looks at health care specifically or
society generally, no concept has received more attention than quality has.
Quality assurance, quality improvement ... these terms and the processes they
entail signal the quality revolution in health care organizations."
1. Some Quality basics
Quality refers to characteristics which are associated with excellence, and these
characteristics form the criteria for assessing the quality of a specific service.
Assurance implies a guarantee that a product or service meets certain standards.
Quality assurance (QA) is therefore a formal system that assures that products or
services meet the characteristics associated with excellence.
In other words, it is a deliberate process of identifying and evaluating the quality
of patient care services to ensure that a predetermined standard is being met.
Audits identify deficiencies and deficiencies are rectified - this remedial step is a
key feature of QA.
On the other hand quality improvement (QI) is based on the assumption that
quality can never be completely assured and a sustained programme for
identifying opportunities to improve quality is necessary. Coltin and Aronow
(1993) define QI as "the application of scientific methods to understand and
continuously improve the ability of all processes to meet the needs of
customers." The QI approach is a process of improving the whole system as

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
33
opposed to the QA approach of identifying and overcoming defects. QI focuses on the positive whilst QA highlights the negative.
2. Measuring quality
Donabedian (1980) introduced the well known structure, process, outcomes
(SPO) model of quality assessment. Although he believed outcomes to be the
ultimate measure of quality, he argued that in addition to outcomes, measures
should be made of structure and process. Structure refers to the systems and
facilities deemed to be essential for quality care. Processes are those actions
which occur in order to deliver health care products and services.
Thus the quality of outcomes can be inferred if structural and process variables
are in accordance with standards and/or guidelines. Similarly, if the structural
variables and processes do not conform with norms, standards and protocols, it
is unlikely that outcomes of acceptable quality would be achieved.
3. Structural and process measures and their limitations
Structural and process indicators are much easier to measure than outcomes
and for this reasons they are usually selected ahead of outcome indicators.
4. Outcome measures and their limitations
The outcome of an intervention must be the most reliable way of measuring its
quality. However, from the point of health care, it makes good sense to assess
structure and process since a fixation with outcomes is not always in the best
interests of the patient.
Outcomes measures have other limitations. It is difficult to show a causal link
between the health care intervention and an outcome since many environmental
influences exist which are difficult to control (eg. diet, lifestyle). Meaningful
outcomes are often difficult to define and measure, and require large samples to
ensure that valid results are obtained - eg. quality of life studies.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
34
In conclusion, any measure of quality should take into consideration appropriate
structural, process and outcome indicators.
4. QUALITY INDICATORS
The United States Office of Technology Assessment defined quality health care
as "the degree to which the process of care increases the probability of outcomes
desired by patients and reduces the probability of undesired outcomes give the
current state of knowledge" (Holdford and Smith: 1997). Whilst the emphasis is
on outcomes, this is closely linked with processes.
1. The existence of a health care service on its own does not provide a reliable
indicator of quality unless there are appropriate process indicators linked to that
service.
2. Process indicators on their own are not acceptable measures of quality health
care unless there is a clear link between the process and the outcome and the
causal relationship between the two has been validated.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
35
Managed Care
What is Managed Care?
• Managed care is a complex system that involves the active coordination of, and the arrangement for, the provision of health services and coverage of health benefits.
• The most common types of Managed Care Organizations (MCOs) include Health Maintenance Organizations (HMOs), Preferred Provider Organizations (PPOs) and Exclusive Provider Organizations (EPOs.)
• Managed care usually involves three key components: oversight of the medical care given; contractual relationships and organization of the providers giving care; and the covered benefits tied to managed care rules.
In contrast, what is traditional health care?
• Traditional health care is most identified with freedom of choice for patients and physicians. Patients can choose whatever physician they want to see, physicians can choose to order whatever services they feel are necessary.
• Health Plans are mostly passive third parties, paying for all the services a physician orders, at the provider’s usual charges.
• A Health Plan’s costs and premiums are based on prior experience and covered benefits of the population insured. There is no way to fix medical costs or know exactly what they’ll be in the future.
• After medical services are rendered by providers, the health plan is billed, and patients must pay the difference between provider’s charges and what their health plan pays.
What is Defined Care?
• Defined Care is the model that describes the health care system with employer sponsored Defined Contribution health plans.
• Defined Contribution health plans involve employers and other traditional purchasers of care providing an allowance, that empowers consumers to purchase and select from a wide menu of benefit options that are arranged by the employer or a purchasing administrator.
• Under Defined Care, the consumer is more empowered, informed and enabled, and consumer, provider, plan and employer roles and requirements change accordingly.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
36
In managed care each patient with insurance coverage under a health plan is
called a member. Other terms used include enrollees and covered lives.
Each person who has the health plan policy in his/her name, whether the policy
is bought just for the individual or for the whole family, is called the subscriber or
the insured.
If the subscriber has coverage for other family members, they are called
dependents. Subscribers and dependents are all members. A subscriber with a
covered spouse and three children would equal five members.
Purchasers, providers and others often refer to how many members (how much
enrollment) a health plan has or a provider serves.
Membership is typically classified by type of MCO, such as HMO, PPO or EPO
(Exclusive Provider Organization). Membership is also broken down by
Purchaser category, including Medicare, Medicaid and Commercial. Commercial
means non-government program members. Commercial members with
employment-based coverage are called Group members (because they have
group coverage).
Per Member Per Month is the relative measure, the ratio, by which most
expense and revenue, and many utilization comparisons are made.
Member Months: Some people do get hung up on member months. But there
isn't any magic to it: whatever period of time you wish to measure (let's take three
months for example) you add up the members for each month for the total period
of time (so if you have 1,000 members in month one; 1,500 members in month
two; and 2,000 members in month three, you get 4,500 member months for the
period.) Divide the member months (4,500 in our example) by the elapsed
months in the period (three in our example) and you get the average members
for the period (1,500 in our example.)
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
37
Medical Management Terms
Quality Management Quality Management (also referred to as Quality Assurance) involves ensuring
members are getting accessible & available care, delivered within community
standards; and ensuring a system exists to identify and correct problems, and to
monitor ongoing performance. Tools include: profiling of data, audits of health
plan and provider records and facilities, surveys of providers and members and
recording of problem incidents as they occur.
Utilization Management Utilization Management involves coordinating how much or how long care is
given for each patient, as well as the level of care. The goal is to ensure care is
delivered cost-effectively, at the right level, and doesn't use unnecessary
resources. Tools include authorization requirements to approve services before
they occur, concurrent review for continuing cases, and profiling of cases after
they occur for analysis.
Outcomes Management A program used to determine the clinical end-results according to defined various
categories (by provider, by procedure, by clinical guideline, etc.) and then
promote use of those categories which yield improved outcomes.
Demand Management A program administered provider organizations to monitor and process many
types of initial member requests for clinical information and services. The
program may involve operating an extended hours nursing telephone triage
service for members, or patient education materials and resources.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
38
Disease Management Disease management involves aspects of case and outcomes management, but
the approach focuses on specific diseases, looking at what creates the costs,
what treatment plan works, educating patients and providers, and coordinating
care at all levels: hospital, pharmacy, physician, etc.
Sharing Financial Risk
In Managed Care Organization (MCO) provider contracts, providers often bear
some level of financial risk. In paying providers, capitation and salaries involve
the highest levels of provider risk, and are usually just allowed under HMOs. Per
Case payments also involve some risk, as costs could exceed the case payment.
Capitation: Capitation means paying a fixed amount of money per person (per
capita). Capitation puts a lid on payments per person that otherwise might
change under a fee-for-service system. Providers are at full financial risk for the
services capitated. The provider is paid a fixed amount per member enrolled,
regardless of the number of services delivered to that member.
Contact capitation is a relatively newer capitation methodology based on
experience. Under a contact capitation arrangement, the managed care
organization typically pays a provider a capitated amount per qualifying patient,
as opposed to an entire member population. There are a number of alternative
structures for contact capitation. Payments can be a global fee for entire episode
of care, or it may be a monthly payment for the period of time that the patient is
referred or has been diagnosed with a specific condition. With contact capitation,
the provider is only at risk for the cost per referral. The MCO retains the risk for
the number of referrals, as opposed to conventional capitation, which places
providers at risk for both the number of referrals and the cost per referral.
Other types of risk sharing include withholds, when a portion of the provider
payment is held back and only paid later if certain criteria are met. Also, there are
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
39
shared risk funds, where physician groups share in a portion of the financial risk
and potential profit of hospital or prescription costs.
How shared risk funds work: Typically, in a shared risk arrangement, a fund gets
"paid" the capitation rate. Medical expenses are paid from this fund, and
periodically, profits or losses are distributed to the participants.
Shared risk funds often allocate the risk between physicians and institutional
providers, or between physicians and health plans. Occasionally, there are three
or more parties involved (Health Plan, Physicians, Hospital and a management
company could all be involved). Hospital and Pharmacy services are the most
prevalent examples of shared risk funds. However, there are many other types of
services that involve shared risk arrangements as well.
Incurred but not reported claims or encounters involve covered services that
have been rendered, but have not been received or captured by you to process.
You to need to consider this issue
when:
You pay claims from sub-contracted or outside providers. You capitate sub-contracted providers and collect encounter data from
them. You provide internal services and capture your encounter data, or even
pay yourself from a shared risk fund.
Premium Pricing Cycle
Premiums drive profits: medical management is critical, but: too low of a premium
will not fund even the best managed plan, while a very high premium might fund
a poorly managed plan. The cycle is a 40 year old phenomenon.
How the cycle works- during profitable periods:
1. plans want to expand market share- 2. start to lower price to do so- 3. other plans match lower prices to keep pace and not lose share
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
40
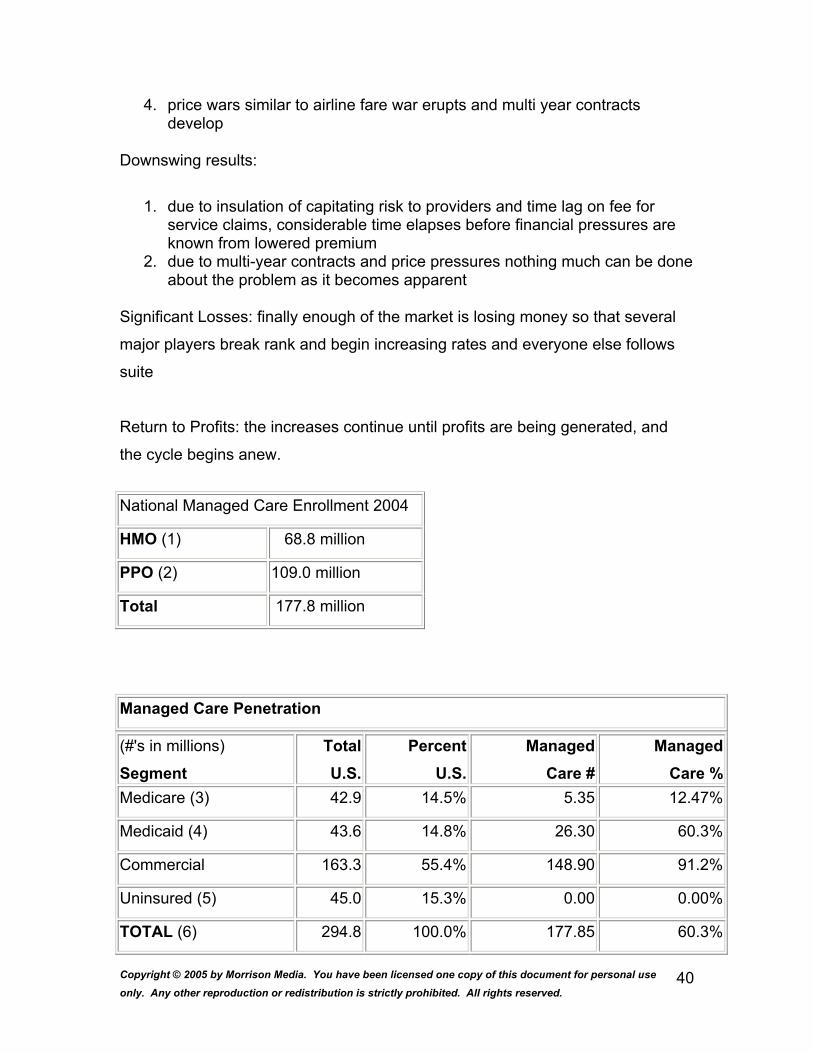
4. price wars similar to airline fare war erupts and multi year contracts develop
Downswing results:
1. due to insulation of capitating risk to providers and time lag on fee for service claims, considerable time elapses before financial pressures are known from lowered premium
2. due to multi-year contracts and price pressures nothing much can be done about the problem as it becomes apparent
Significant Losses: finally enough of the market is losing money so that several
major players break rank and begin increasing rates and everyone else follows
suite
Return to Profits: the increases continue until profits are being generated, and
the cycle begins anew.
National Managed Care Enrollment 2004
HMO (1) 68.8 million
PPO (2) 109.0 million
Total 177.8 million
Managed Care Penetration
(#'s in millions)
Segment TotalU.S.
PercentU.S.
Managed Care #
ManagedCare %
Medicare (3) 42.9 14.5% 5.35 12.47%
Medicaid (4) 43.6 14.8% 26.30 60.3%
Commercial 163.3 55.4% 148.90 91.2%
Uninsured (5) 45.0 15.3% 0.00 0.00%
TOTAL (6) 294.8 100.0% 177.85 60.3%

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
41
Key HMO Performance Measures
Commercial Medicare
Inpatient Days Per 1,000 Per Year (7) 240.9 N/A
Physician Encounters Per Member Per
Year (8) 3.1 8.0
Rx's Utilization Per Member Per Month
(7) 0.7 N/A
Plan Medical Loss Ratio (9) 87.50%
Average PMPM Rates - Physician (10) $53.35 $209.43
Average PMPM Rates - Hospital (10) $53.15 $252.43
Health Plan Total Managed Care Enrollment*
Anthem/WellPoint 28.0 million
Aetna U.S. Healthcare 13.6 million
United Health Group 10.8 million
Cigna HealthCare 9.9 million
Kaiser Foundation Health Plans 8.4 million
HealthNet 7.3 million
Humana 7.0 million
Coventry Health Care 3.1 million
PacifiCare Health Systems 3.0 million
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
42
Organizational Effectiveness
Organizational Effectiveness
Collins’s Profile of Great Organizations (“Good to Great”)
Disciplined People
Level 5 Leadership (professional will and humility)
First Who Then What (the “right” people are your most important asset”)
Collins’s Profile of Great Organizations (“Good to Great”)
Disciplined Thought
Confront the Brutal Facts (dialogue and debate, conducting autopsies,
creating red flag mechanisms)
Hedgehog Concept (what you are deeply passionate about, what you can
be the best in the world at, and what drives your economic engine)
Organizational Effectiveness
Collins’s Profile of Great Organizations (“Good to Great”)
Disciplined Action
Culture of Discipline (Adherence to the Hedgehog Concept)
Technology Accelerators (accelerate momentum)
Organizational Effectiveness
Collins’s Profile of Great Organizations (“Good to Great”)
The Flywheel and the Doom Loop
Consistency and sustaining positive changes.
Total Quality Management (TQM)
• TQM refers to a set of methods and tools that are used to help
organizations better manage business processes in order to enhance
quality, productivity, customer satisfaction.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
43
“McDonald’s”
How does an Egg McMuffin demonstrate fundamental
elements of TQM?
Typical Elements of an Effective TQM Program
1. Process Orientation
• Cross-Functional Teams
• Customer Focus
• Benchmarking
• Investment in Employee Training
• Data-Based Decision Making
2. Employee Empowerment
• Continuous Improvement
• Open Communication
• Quality-Driven Culture
Outcomes of Total Quality Management
• Reduced costs • Increased productivity • Higher customer satisfaction and retention • Fewer defects in products and services • Shorter product development cycles • Greater profitability
What is Strategy? Why is it Important?
Strategy is a broad plan of action (“roadmap”) for pursuing and achieving the
firm’s objectives and satisfying its mission.
Strategy is important because it aligns an organization with its external
environment.
Questions:
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
44
• Purpose of the organization? • Who are the customers or stakeholders? • Which products or services? • What are the core values of the organization?
The Strategic Planning Process
Examples of Organizational Mission Statements
“To solve unsolved problems innovatively” (3M)
“Empowering people through great software” (Microsoft)
“To give ordinary folks the chance to buy the same thing as rich people.”
(Wal-Mart)
“Crush Reebok” (Nike)
The Strategic Planning Process
Perform an External Environmental Scan.
• Competitors • Customers • Technology • Economic Conditions • Laws and Regulations
Outcome: ID Opportunities and Threats
The Strategic Planning Process
Perform an Internal Environmental Scan.
• Processes • Structure • People • Culture • Product/Service Portfolio • Past Performance
Outcome: ID Organizational Strengths and Weaknesses.
The Strategic Planning Process
• Develop strategic objectives to support the mission.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
45
• “Critical Measures of Success” (e.g., revenue growth, profits, customer satisfaction, customer retention, cost reduction, product quality, service quality, employee satisfaction.
• Develop strategies to support strategic objectives. • Develop operational goals and strategies. • Implement the strategic plan.
Execution:
• Bossidy and Charan’s Key Points About Execution • Execution is a discipline. • Execution is the job of the business leader. • Execution has to be in the culture.
The Strategic Planning Process
Evaluate results and modify as needed.
• Bossidy and Charan’s Diagnostic Questions for Conducting a Strategy Review
• How well versed is each business unit team about the competition? • How strong is the organizational capability to execute the strategy? • Is the plan scattered or sharply focused? • Are we choosing the right ideas? • Are the linkages with people and operations clear?
The Four Perspectives of the Balanced Scorecard
• Financial (e.g., operating income, return on capital employed) • Customer (e.g., customer satisfaction, new customer acquisition) • Internal Business Process (e.g., defects, efficiency) • Learning and Growth (e.g., new individual or organizational competencies)
Practical Guidelines for Effective
Strategic Planning
1. Involve everyone you need to carry out your plan.
2. Work collaboratively with those whose help you need.
3. Schedule a full-day retreat.
4. Document your plan.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
46
5. Make it as simple as possible.
6. Develop an action plan for each strategic objective.
7. Keep the process alive by updating it continuously.
8. Make sure that your plan fits senior management’s goals.
9. Don’t undertake too much – prioritize your objectives.
10. Keep your plan visual.
11. Communicate the plan down the line.
12. Create an accountability document.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
47
What are Ethics?
Ethics are principles of morality or rules of conduct.
Business ethics are rules about how businesses and their employees
ought to behave.
Key Point: What is ethical or unethical may vary widely across cultures.
Benefits of Managing Ethics in the Workplace
1. Attention to business ethics has improved society.
2. Ethics programs help maintain a moral cause in turbulent times.
3. Ethics programs integrate ethical guidelines in to decision making.
4. Ethics programs help manage values associated with other initiatives such
asa TQM, strategic planning, and diversity.
5. Ethics programs promote a strong public image.
6. Ethics programs show employees that management truly supports
attention to ethics.
7. Ethics programs are an insurance policy that help ensure that policies are
legal.
8. Ethics programs align organizational behaviors with operating values.
9. Ethics programs develop an awareness and sensitivity to ethical issues.
Causes of Unethical Employee Behavior
A. Organizational Reward Systems
B. A Bottom-Line Mentality
C. Lack of Operational Controls
D. Machiavellian Personality Type
E. Darwinian Organizational Culture
F. Weak Leadership
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
48
Strategies for Enhancing Ethical Behavior in Organizations
A. Obtain support of top management.
B. Develop a code of ethics.
Example: Policy
The Company is committed to the highest ethical standards and to
compliance with all applicable laws and regulations. It is the obligation of
our employees to:
• Conduct themselves honestly and ethically; • Avoid conflicts of interest, and disclose to their immediate superiors any
relationship that appears to constitute a conflict of interest; and • Comply with applicable governmental laws, rules and regulations.
C. Accomplish preferred behaviors in the workplace.
D. Provide ethics training for all managers and employees.
E. Integrate ethics into other management practices.
F. Implement a whistle-blowing process.
G. Consider establishing an ethics management committee.
H. Assign a high-ranking member of management to become an “ethics
officer.”
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
49
What is Organizational Structure?
Organizational structure refers to the formal definition and relationships among
tasks, jobs, work units, people, and resources in a firm. It addresses questions
regarding the formation of jobs, processes, systems, work units, divisions, etc.
and the relationships between them that are created to support the overall
objectives of the organization.
Structure is important because it must support the strategic plan of the
organization. Structure shapes the effectiveness of an organization in terms of
inter-departmental working relationships, product and service development lead
times, quality, efficiency, and responsiveness to customer demands.
Structure greatly influences individual and group morale, motivation,
commitment, and satisfaction.
Characteristics of Functional Structures
1. Advantages
Efficiency
Specialization
2. Disadvantages
Narrow Perspectives (i.e., a “functional mindset”)
Lack of Innovation
Characteristics of Divisional Structures
1. Advantages
Autonomy
Customization of strategies
2. Disadvantages
Lower efficiency
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
50
Coordination
Characteristics of Matrix Structures
1. Advantages
Flexibility
Responsiveness to environment
Enhanced communication
2. Disadvantages
Frustration/stress from two boss system
Risk of one system overwhelming the other
Need for high levels of cooperation
Characteristics of Decentralized Structures
1. Advantages of High Decentralization (Flat Organizations)
Eliminates layers of management
Decisions can be made by people closer to the problem
2. Advantages of Low Decentralization (Tall Organizations)
Eliminates additional responsibility not desired by some people
performing routine jobs
Permits crucial decisions to be made by individuals with the big
picture
Contemporary Organizational Forms
A. Virtual Organizations – Temporary organization composed of multiple
organizations formed for a specific purpose.
B. Boundary less Organizations – Open system approach where jobs and
formalization are de-emphasized.
C. Modular Organizations – Organizations where non-core functions are
outsourced.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
51
Healthcare Organizations and Data Banks
The National Committee for Quality Assurance (NCQA) http://www.ncqa.org/
HQCB/NAHQ
The Healthcare Quality Certification Board (HQCB) of the National Association
for Healthcare Quality (NAHQ) was formed in 1976 to advance the profession of
healthcare quality management through the development of a certification
program. The HQCB is the certifying arm of NAHQ. The HQCB establishes
policies, procedures, and standards for certification and recertification in the field
of healthcare quality management. The granting of Certified Professional in Healthcare Quality (CPHQ) status recognizes professionals and academic
achievement through the individual’s participation in this international voluntary
certification program. The commitment by the HQCB to advance the profession is
reflected in its five-year vision statement:
The HQCB adopted a name change in 1992 consistent with terminology changes
in the field. Prior to 1992, the HQCB was known as the Quality Assurance
Certification Board (CPQA). This designation also changed. All current certified
professionals and new successful candidates are identified by the designation
Certified Professional in Healthcare Quality (CPHQ).
National Association for Healthcare Quality: The National Association for
Healthcare Quality (NAHQ), HQCB’s parent association, is a leading organization
for healthcare quality management professionals. NAHQ comprises more than
5,000 individual members and numerous institutional members. Its goal is to
promote the continuous improvement of quality in healthcare by providing
educational and development opportunities for professionals at all management
levels and within numerous healthcare settings.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
52
NAHQ maintains formal affiliation with quality associations in almost every state,
along with numerous affiliate societies from countries outside of the United
States.
Accreditation: The HQCB was granted full accreditation by NCCA during the
first initial review and has undergone the required reaccreditation process in
1993, 1998 and 2003. HQCB received a full five-year accreditation on each
occasion.
NCCA accredits certification entities that are national in scope using standards
developed originally in early 1978 with funding provided by the U.S. Department
of Health and Human Services.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
53
Health Care Quality Improvement Program
For more than two decades, HSAG has served as the Center for Medicare and
Medicaid Services (CMS) contracted Quality Improvement Organization (QIO) in
various states. As the QIO, HSAG works with providers to review and improve
the quality of health care for Medicare beneficiaries statewide.
In 1992, CMS launched Medicare’s first multi-state quality improvement pilot
project. The project demonstrated that QIOs working with providers improved
hospital-based AMI care. CMS subsequently expanded the QIO program to
include national quality improvement projects in the hospital and physician office
settings.
New National Initiatives CMS has augmented these quality improvement activities with major new
national initiatives to widely disseminate select quality measures for Medicare-
certified nursing homes, home health agencies, hospitals, and physicians offices.
In November 2001, DHHS Secretary Tommy G. Thompson announced the
Quality Initiative – the Department’s commitment to assure quality health care for
all Americans through accountability and public disclosure.
The Initiative aims to:
• empower consumers with quality of care information to make more informed decisions about their healthcare; and
• stimulate and support providers and clinicians to improve the quality of care.
HSAG promotes awareness, understanding and use of this information by
working directly with beneficiaries and providers, and with intermediaries such as
discharge planners, community organizations, and the media.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
54
National Practitioner Data Bank (NPDB)
Why the NPDB Was Created
The legislation that led to the creation of the NPDB was enacted because the
U.S. Congress believed that the increasing occurrence of medical malpractice
litigation and the need to improve the quality of medical care had become
nationwide problems that warranted greater efforts than any individual State
could undertake. The intent is to improve the quality of health care by
encouraging State licensing boards, hospitals and other health care entities, and
professional societies to identify and discipline those who engage in
unprofessional behavior; and to restrict the ability of incompetent physicians,
dentists, and other health care practitioners to move from State to State without
disclosure or discovery of previous medical malpractice payment and adverse
action history. Adverse actions can involve licensure, clinical privileges,
professional society membership, and exclusions from Medicare and Medicaid.
The NPDB is primarily an alert or flagging system intended to facilitate a
comprehensive review of health care practitioners' professional credentials. The
information contained in the NPDB is intended to direct discrete inquiry into, and
scrutiny of, specific areas of a practitioner's licensure, professional society
memberships, medical malpractice payment history, and record of clinical
privileges. The information contained in the NPDB should be considered together
with other relevant data in evaluating a practitioner's credentials; it is intended to
augment, not replace, traditional forms of credentials review.
Access to Information
Access to information in the NPDB is available to entities that meet the eligibility
requirements defined in the provisions of P.L. 99-660 and the NPDB regulations.
In order to access information, entities must first register with the Data Bank.
NPDB information is not available to the general public. However, information in
a form that does not identify any particular entity or practitioner is available.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
55
Confidentiality
Information reported to the NPDB is considered confidential and shall not be
disclosed except as specified in the NPDB regulations. The Privacy Act of 1974,
protects the contents of Federal systems of records such as those contained in
the NPDB from disclosure, unless the disclosure is for a routine use of the
system of records as published annually in the Federal Register. The published
routine uses of NPDB information do not allow for disclosure of information to the
general public.
The Office of Inspector General (OIG), Health and Human Services (HHS), has
the authority to impose civil money penalties on those who violate the
confidentiality provisions of Title IV. Persons, organizations, or entities that
receive information either directly or indirectly are subject to the confidentiality
provisions and the imposition of a civil money penalty of up to $11,000 for each
offense if they violate those provisions.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
56
Healthcare Integrity and Protection Data Bank
Why the HIPDB Was Created
The Secretary of the U.S. Department of Health and Human Services, acting
through the Office of Inspector General (OIG), was directed by the Health
Insurance Portability and Accountability Act of 1996 to create the Healthcare
Integrity and Protection Data Bank (HIPDB) to combat fraud and abuse in health
insurance and health care delivery. Health care fraud burdens the nation with
enormous financial costs and threatens the quality of health care and patient
safety. Estimates of annual losses due to health care fraud range from 3 to
10 percent of all health care expenditures--between $30 billion and $100 billion
based on estimated 1997 expenditures of over $1 trillion.
The HIPDB is primarily a flagging system that may serve to alert users that a
comprehensive review of a practitioner's, provider's, or supplier's past actions
may be prudent. The HIPDB is intended to augment, not replace, traditional
forms of review and investigation, serving as an important supplement to a
careful review of a practitioner's, provider's, or supplier's past actions.
Access to Information
Access to information in the HIPDB is available to entities that meet the eligibility
requirements defined in Section 1128E of the Social Security Act and the HIPDB
regulations. In order to access information, eligible entities must first register with
the Data Bank.
HIPDB information is not available to the general public. However, information in
a form that does not identify any particular entity or practitioner is available.
Confidentiality
Information reported to the HIPDB is considered confidential and shall not be
disclosed except as specified in the HIPDB regulations. The Privacy Act of 1974,
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
57
protects the contents of Federal systems of records such as those contained in
the NPDB from disclosure, unless the disclosure is for a routine use of the
system of records as published annually in the Federal Register.
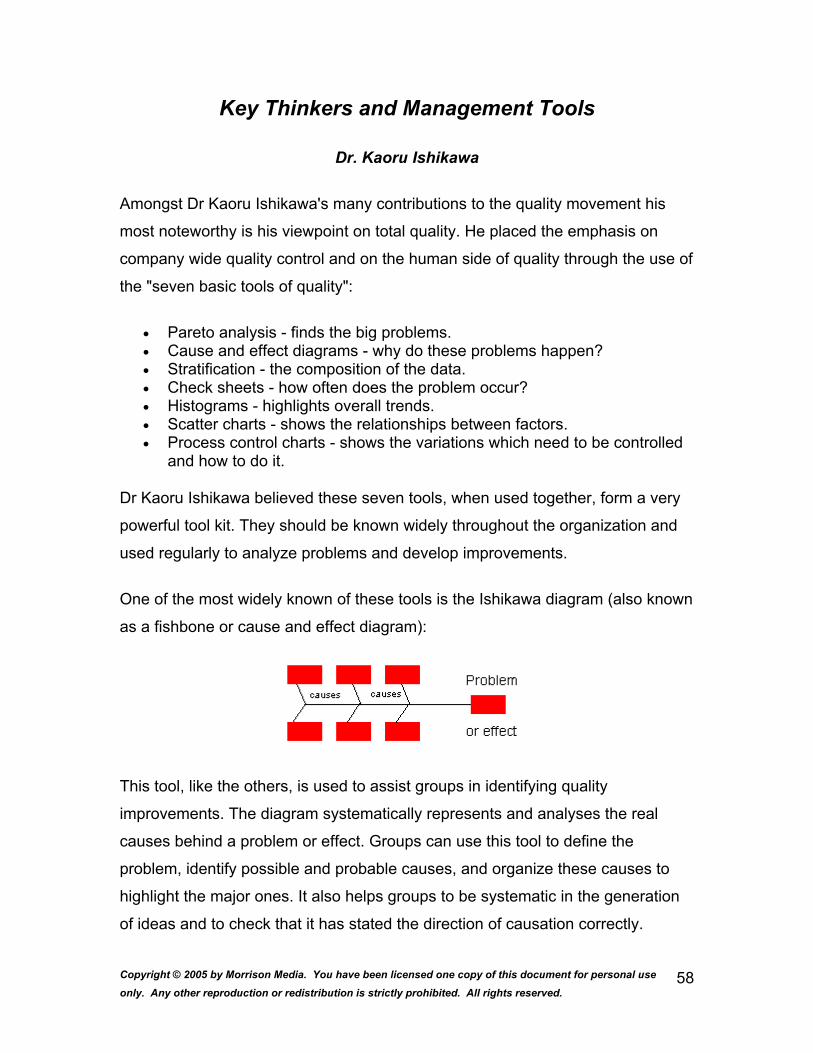
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
58
Key Thinkers and Management Tools
Dr. Kaoru Ishikawa
Amongst Dr Kaoru Ishikawa's many contributions to the quality movement his
most noteworthy is his viewpoint on total quality. He placed the emphasis on
company wide quality control and on the human side of quality through the use of
the "seven basic tools of quality":
• Pareto analysis - finds the big problems. • Cause and effect diagrams - why do these problems happen? • Stratification - the composition of the data. • Check sheets - how often does the problem occur? • Histograms - highlights overall trends. • Scatter charts - shows the relationships between factors. • Process control charts - shows the variations which need to be controlled
and how to do it.
Dr Kaoru Ishikawa believed these seven tools, when used together, form a very
powerful tool kit. They should be known widely throughout the organization and
used regularly to analyze problems and develop improvements.
One of the most widely known of these tools is the Ishikawa diagram (also known
as a fishbone or cause and effect diagram):
This tool, like the others, is used to assist groups in identifying quality
improvements. The diagram systematically represents and analyses the real
causes behind a problem or effect. Groups can use this tool to define the
problem, identify possible and probable causes, and organize these causes to
highlight the major ones. It also helps groups to be systematic in the generation
of ideas and to check that it has stated the direction of causation correctly.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
59
The diagrammatic format is immensely useful when the findings need to be
presented to others.
Dr. Joseph Juran
Dr.Joseph Juran born Romania 24 Dec 1904, emigrated to America 1912 and
began as an engineer in 1924 publishing "Quality Control Handbook" in 1951 and
a professor at New York University. Like Demning, traveled to Japan in the mid
50's to conduct top and middle level executive seminars on planning,
organizational issues, management responsibilities for quality and the need to
set and monitor improvement target goals.
His concepts of "Breakthrough", "The internal customer" and the "Quality Trilogy"
did much to build on the foundation of business improvement established by the
other quality gurus. Expanded on the use of Pareto analysis for effective problem
targeting, "cost of quality" and the concept of company "quality councils".
Juran maintained that quality was intrinsically linked to product satisfaction and
dissatisfaction. Satisfaction in this context was the superior performance or
features, where as the dissatisfaction was the deficiencies or defects in the
product or service. These two distinct areas were concerned with matching
customer requirements (the external dimension) and building the product or
service correctly (the internal dimension).
Juran's well known definition, "Fit for purpose" needs further clarification. For
whose purpose and what's the real purpose. As there are many customers both
internal and external to the business, Juran maintained that quality begins with
who, how and why these customers will use it, without this information any
improvement will be guesswork. Illustrating this point by stating a dangerous
product could meet all specifications and still not be fit for use. More recently, his
"Big Q" concept of quality not being just about manufacturing but extends across
organizational links and onto the customers.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
60
Internal customer
Juran realized that the customer was not just the end customer and that each
person along the chain has an internal customer, and as such is supplier to the
next in the chain. Therefore Juran maintained that at each stage was a "Three
role model": supplier, process and customer. The "three role model" represents a
breaking down of the complete cycle into numerous opportunities for ongoing
process and business improvement. Emphasizing that quality improvements can
be identified and achieved throughout the complete cycle from the original
customer need through to the receiving external customer.
By exploring the complete lifecycle, Juran points out that the "big picture" must
include suppliers and in so doing brings into the equation Purchasing and Sub-
contract as prime elements to maintaining product quality (essential when prime
contractor ships are involved). Expanding this argument, he rightly states that, "a
single source can more easily neglect to sharpen its competitive edge, cost and
service", but goes on to temper it with a hands-on team approach to vendors
being more productive than a adversarial one.
Cost of quality
The cost of quality, or not getting it right first time, Juran maintained should be
recorded and analyzed and classified into failure costs, appraisal costs and
prevention costs.
Failure costs
Scrap, rework, corrective actions, warranty claims, customer complaints and loss of custom
Appraisal costs
Inspection, compliance auditing and investigations
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
61
Prevention costs
Training, preventive auditing and process improvement implementation
Quality trilogy
Juran's view is that, "Quality does not happen by accident it must be
planned". Seeing quality planning as the three elements of Quality Planning,
Quality Control and Quality Improvement running parallel to budgeting, cost
control and cost reduction. Stating that planning's key elements required to
implement a company-wide strategy were to identify customer needs, define
quality goals, identify and implement quality metrics, planning process capability,
and continually monitor results to reduced manufacturing and non-manufacturing
errors. All this supports his theory that quality is not free and there is a point
where conformance is more costly than the value of the quality obtained.
Quality Planning Road Map
1. Identify customers.
2. Determine customer needs.
3. Translate customer needs into specifications.
4. Develop product or service to meet customer needs.
5. Optimize product or service features and characteristics.
6. Develop process capabilities to produce product or service.
7. Prove process.
8. Production process.
Quality Council
A body typically comprising senior management with the responsibility for project
managing the quality improvements. The council would set targets, run needs
analysis for training and equipment, cost of quality measurement, co-ordination

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
62
and liaise between groups and management levels. Essentially become the focal
point of the quality improvement culture within the business organization as they
improve communication and breakdown interdepartmental or functional
boundaries.
The breakthrough concept
Like the Deming cycle, Juran's breakthrough concerns itself with the
product/service life cycle. In essence this splits it up into two areas: the "journey
from symptom to cause" and the "journey from cause to remedy".
However, Juran's message is not always well received. The view that training
should start at the top often provokes a senior management reaction that training
is for others as they either know it all or should do. Logically, and speaking from
experience, this belief needs to be reassessed. It is often seen that good quality
initiatives and improvements are dead before they have got off the ground due to
lack of understanding, poor launch, bad presentation, inadequate buy-in and
more often restrictions on the time to adequately assess them. "Fire fighting" is a
poor excuse for improvement and indicative of the lack of planning and risk
management. In his view less than 20% of quality problems are due to
operators, the remainder lies a little higher up the salary structures.
Affinity Diagram
The affinity diagram, or KJ method (after its author, Kawakita Jiro), wasn't
originally intended for quality management. Nonetheless, it has become one of
the most widely used of the Japanese management and planning tools. The
affinity diagram was developed to discovering meaningful groups of ideas within
a raw list. In doing so, it is important to let the groupings emerge naturally, using
the right side of the brain, rather than according to preordained categories.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
63
Usually, an affinity diagram is used to refine a brainstorm into something that
makes sense and can be dealt with more easily. In Seven New QC Tools,
Ishikawa recommends using the affinity diagram when facts or thoughts are
uncertain and need to be organized, when preexisting ideas or paradigms need
to be overcome, when ideas need to be clarified, and when unity within a team
needs to be created.
A sample affinity diagram is show below. On the left side of the window is a
brainstormed list of ideas. On the right side is the affinity diagram, in which ideas
have been grouped into affinity sets. In this case, the sorting is in an advanced
state, and affinity sets have already been given titles. It's important not to add the
titles early in the sorting process.
Brainstorming
Creative thinking requires tools such as the brainstorm and the affinity diagram.
Brainstorming is simply listing all ideas put forth by a group in response to a
given problem or question. In 1939, a team led by advertising executive Alex
Osborn coined the term "brainstorm." According to Osborn, " Brainstorm means
using the brain to storm a creative problem and to do so "in commando fashion,
each stormer audaciously attacking the same objective." Creativity is encouraged
by not allowing ideas to be evaluated or discussed until everyone has run dry.
Any and all ideas are considered legitimate and often the most far-fetched are
the most fertile. Structured brainstorming produces numerous creative ideas
about any given "central question". Done right, it taps the human brain's capacity
for lateral thinking and free association.
Brainstorms help answer specific questions such as:
• What opportunities face us this year? • What factors are constraining performance in Department X? • What could be causing problem Y? • What can we do to solve problem Z?
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
64
However, a brainstorm cannot help you positively identify causes of problems, rank ideas in a meaningful order, select important ideas, or check solutions.
To conduct a successful brainstorm:
1. Make sure everyone understands and is satisfied with the central question before you open up for ideas.
2. You may want to give everyone a few seconds to jot down a few ideas before getting started.
3. Begin by going around the table or room, giving everyone a chance to voice their ideas or pass. After a few rounds, open the floor.
4. More ideas are better. Encourage radical ideas and piggybacking. 5. Suspend judgment of all ideas. 6. Record exactly what is said. Clarify only after everyone is out of ideas. 7. Don't stop until ideas become sparse. Allow for late-coming ideas. 8. Eliminate duplicates and ideas that aren't relevant to the topic.
A brainstorm starts with a clear question, and ends with a raw list of ideas. That's
what it does well - give you a raw list of ideas. Some will be good, and some
won't. But, if you try to analyze ideas in the brainstorming session, you will ruin
the session. Wait. Later, you can analyze the results of a brainstorm with other
quality improvement tools. In particular, affinity diagramming is designed to sort a
raw list, using "gut feel" to begin to categorize the raw ideas. It is most often the
next step beyond brainstorming.
Prioritization Matrix
What is it?
A Prioritization Matrix is a useful technique you can use with your team members
or with your users to achieve consensus about an issue. The Matrix helps you
rank problems or issues (usually generated through brainstorming) by a
particular criterion that is important to your organization. Then you can more
clearly see which problems are the most important to work on solving first.
When to use it?
When you need to prioritize problems, or to achieve consensus about an issue.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
65
How to use it:
1. Brainstorm--Conduct a brainstorming session on problems users or team members have with your program or service.
2. Fill out the Prioritization Matrix chart with the group:
Problem Frequency Importance Feasibility Total Points
3. In the first column, write down the problems that were mentioned in the brainstorming session.
4. In the second to fourth columns, define your criteria. Examples of some typical criteria are:
o Frequency: How frequent is the problem? Does it occur often or only on rare occasions?
o Importance: From the point of view of the users, what are the most important problems? What are the problems that you want to resolve?
o Feasibility: How realistic is it that we can resolve the problem? Will it be easy or difficult?
You can choose other criteria if they better fit the situation you are discussing. For example, for a more quantitative comparison, you could use cost, amount of time, or other numerical indicators as the criteria.
5. Rank/Vote--Each participant now votes three times for each criteria. Each participant votes nine times in total.
6. Total all the votes together. The totals help you see clearly how to prioritize the problems.
Gantt charts
Developed by Harry Gantt in 1916, these charts give a timeline for each activity.
They are used for planning, scheduling and then recording progress against
these schedules.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
66
Basically there are two basic types of Gantt Charts: Load Charts and Project
Planning Charts.
* Load Charts:
This type of chart is useful for manufacturing projects during peak or heavy load
periods. The format of the Gantt Load Chart is very similar to the Gantt Project
Planning Chart but, in this case, uses time as well as departments, machines or
employees that have been scheduled.
* Project Planning Chart
It addresses the time of individual work elements giving a time line for each
activity of a project. This type of chart is the predecessor of the following tool:
PERT. As it can be seen in the figure, it is really easy to understand the graph,
but in developing it you need to take into consideration certain precedence
relationships between the different activities of the project. On the chart,
everyone is able to see when each activity starts and finishes but there is no
possibility to determine when each activity may start or if we can start a particular
activity before finishing the immediate predecessor activity. Therefore, we need
somehow know the precedence relationships between activities. This is the main
reason for using the following tools instead of using exclusively Gantt Charts.
PERT/CPM (Critical path Method)
Both methods show precedence relationships explicitly. Although the two
methods were developed independently during the fifties, they are surprisingly
similar. Both methods, PERT and CPM, use a graphic representation of a project
that it is called "Project Network" or "CPM diagram", and it is used to portray
graphically the interrelatioships of the elements of a project and to show the
order in which the activities must be performed.
PERT
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
67
We have a high degree of uncertainty in regard to the completion time of many
activities. It makes sense in the real world that you do not really know how long a
particular activity will take, specially talking about certain activities such as
research and development. In this case, we can look at the project completion
time in a probabilistic fashion and for each activity we can define:
a. Optimistic time estimate: an estimate of the minimum time an activity will require.
b. Most likely time estimate: an estimate of the normal time an activity will require.
c. Pessimistic time estimate: an estimate of the maximum time an activity will require.
Delphi Technique
The Delphi technique was developed by the RAND Corporation in the late 1960's
as a forecasting methodology. Later, the U.S. government enhanced it as a
group decision-making tool with the results of Project HINDSIGHT, which
established a factual basis for the workability of Delphi. That project produced a
tool in which a group of experts could come to some consensus of opinion when
the decisive factors were subjective, and not knowledge-based.
Delphi is particularly appropriate when decision-making is required in a political
or emotional environment, or when the decisions affect strong factions with
opposing preferences. The tool works formally or informally, in large or small
contexts, and reaps the benefits of group decision making while insulating the
process from the limitations of group decision-making; e.g., over-dominant group
members, political lobbying, or "bandwagonism".
Delphi has worked well when trying to prioritize national funding for projects
among different states with conflicting goals, or if the scale of the decision-
making problem is very large:
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
68
"The size of the budget for ASSIST, and the large number of proposals
submitted, generated a complex decision problem. For example, the number of
possible ways of funding is far more than could be considered individually. In
view of this, and the need to identify secondary criteria and allow them to
influence the funding decision, decision makers at [National Cancer Institute]
decided that a formal modeling approach should be used."
Delphi has the added advantage that it works as an informal, subjective model
when the decisions are based on opinion, and can be directly converted to a
formal model, when the data is more knowledge-based.
Delphi Prioritization Procedure
The prioritization process enumerated below will allow the stakeholders and
subject matter experts to produce a list of project rankings, or several lists, from
which the decision-makers in upper management may apply other criteria to
make a decision. The process can be completed in a few short meetings by a
panel of experts, by the corporate associates at large in a series of
questionnaires, or by a hybrid of the two. The description below is vague when
company policy or facilitator discretion may be used to invoke a variation.
1. Pick a facilitation leader. Select a person that can facilitate, is an expert in research data collection,
and is not a stakeholder. An outsider is often the common choice.
2. Select a panel of experts. The panelists should have an intimate knowledge of the projects, or be
familiar with experiential criteria that would allow them to prioritize the
projects effectively. In this case, the department managers or project
leaders, even though stakeholders, are appropriate.
3. Identify a strawman criteria list from the panel. In a brainstorming session, build a list of criteria that all think appropriate
to the projects at hand. Input from non-panelists are welcome. At this
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
69
point, there is no "correct" criteria. However, technical merit and cost are
two primary criteria; secondary criteria may be project-specific.
4. The panel ranks the criteria. For each criterion, the panel ranks it as 1 (very important), 2 (somewhat
important), or 3 (not important). Each panelist ranks the list individually,
and anonymously if the environment is charged politically or emotionally.
5. Calculate the mean and deviation. For each item in the list, find the mean value and remove all items with a
mean greater than or equal to 2.0. Place the criteria in rank order and
show the (anonymous) results to the panel. Discuss reasons for items with
high standard deviations. The panel may insert removed items back into
the list after discussion.
6. Rerank the criteria. Repeat the ranking process among the panelists until the results stabilize.
The ranking results do not have to have complete agreement, but a
consensus such that the all can live with the outcome. Two passes are
often enough, but four are frequently performed for maximum benefit. In
one variation, general input is allowed after the second ranking in hopes
that more information from outsiders will introduce new ideas or new
criteria, or improve the list.
7. Identify project constraints and preferences. Projects as a whole are often constrained by total corporate budget, or
mandatory requirements like regulatory impositions. These "hard
constraints" are used to set boundaries on the project ranking. More
flexible, "soft constraints" are introduced as preferences. Typically, hard
constraints apply to all projects; preferences usually apply to only some
projects. Each panelist is given a supply of preference points, about 70%
of the total number of projects. (For example, give each panelist 21
preference points if 30 projects have been defined.)
8. Rank projects by constraint and preference.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
70
a. Each panelist ranks the projects first by the hard constraints. Which
project is most important to that panelist? Some projects may be
ignored. For example, if the total corporate budget is 100 million,
the panelist allocates each project a budget, up to the maximum
requested for that particular project, and such that the total of all
budgets does not exceed the $100 million. Some projects may not
be allocated any funding.
b. Next each panelist spreads their preference points among the
project list as desired. Some projects may get 10 points, others
may get none, but the total may not exceed the predefined
maximum (21 in our example above).
9. Analyze the results and feedback to panel. Find the median ranking for each project and distribute the projects into
quartiles of 25, 50, and 75-percentiles (50-percentile being the median).
Produce a table of ranked projects, with preference points, and show to
the panel. Projects between the 25th and 75th quartile may be considered
to have consensus (depending on the degree of agreement desired);
projects in the outer-quartiles should be discussed. Once the reason for
the large difference in ranking is announced, repeat the ranking process.
10. Rerank the projects until it stabilizes. After discussing why some people (minority opinion) ranked their projects
as they did, repeat the rankings. Eventually the results will stabilize:
projects will come to a consensus, or some will remain in the outlier range.
Not everyone may be persuaded to rank the same way, but discussion is
unnecessary when the opinions stay fixed. Present the ranking table to the
decision makers, with the various preferences as options, for their final
decision.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
71
Other Tools
Check sheet
The function of a check sheet is to present information in an efficient, graphical
format. This may be accomplished with a simple listing of items. However, the
utility of the check sheet may be significantly enhanced, in some instances, by
incorporating a depiction of the system under analysis into the form.
Pareto Chart
Pareto charts are extremely useful because they can be used to identify those
factors that have the greatest cumulative effect on the system, and thus screen
out the less significant factors in an analysis. Ideally, this allows the user to focus
attention on a few important factors in a process.
They are created by plotting the cumulative frequencies of the relative frequency
data (event count data), in descending order. When this is done, the most
essential factors for the analysis are graphically apparent, and in an orderly
format.
Flowchart
Flowcharts are pictorial representations of a process. By breaking the process
down into its constituent steps, flowcharts can be useful in identifying where
errors are likely to be found in the system.
Cause and Effect Diagram
This diagram, also called an Ishikawa diagram (or fish bone diagram), is used to
associate multiple possible causes with a single effect. Thus, given a particular
effect, the diagram is constructed to identify and organize possible causes for it.
The primary branch represents the effect (the quality characteristic that is
intended to be improved and controlled) and is typically labeled on the right side
of the diagram. Each major branch of the diagram corresponds to a major cause
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
72
(or class of causes) that directly relates to the effect. Minor branches correspond
to more detailed causal factors. This type of diagram is useful in any analysis, as
it illustrates the relationship between cause and effect in a rational manner.
Histogram
Histograms provide a simple, graphical view of accumulated data, including its
dispersion and central tendency. In addition to the ease with which they can be
constructed, histograms provide the easiest way to evaluate the distribution of
data.
Scatter Diagram
Scatter diagrams are graphical tools that attempt to depict the influence that one
variable has on another. A common diagram of this type usually displays points
representing the observed value of one variable corresponding to the value of
another variable.
Control Chart
The control chart is the fundamental tool of statistical process control, as it
indicates the range of variability that is built into a system (known as common
cause variation). Thus, it helps determine whether or not a process is operating
consistently or if a special cause has occurred to change the process mean or
variance.
The bounds of the control chart are marked by upper and lower control limits that
are calculated by applying statistical formulas to data from the process. Data
points that fall outside these bounds represent variations due to special causes,
which can typically be found and eliminated. On the other hand, improvements in
common cause variation require fundamental changes in the process.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
73
Quality Management Principles
Introduction
This document introduces the eight quality management principles on which the
quality management system standards of the revised ISO 9000:2000 series are
based. These principles can be used by senior management as a framework to
guide their organizations towards improved performance.
Principle 1 Customer focus
Organizations depend on their customers and therefore should understand
current and future customer needs, should meet customer requirements and
strive to exceed customer expectations.
Key benefits:
• Increased revenue and market share obtained through flexible and fast responses to market opportunities.
• Increased effectiveness in the use of the organization's resources to enhance customer satisfaction.
• Improved customer loyalty leading to repeat business.
Applying the principle of customer focus typically leads to:
• Researching and understanding customer needs and expectations. • Ensuring that the objectives of the organization are linked to customer
needs and expectations. • Communicating customer needs and expectations throughout the
organization. • Measuring customer satisfaction and acting on the results. • Systematically managing customer relationships. • Ensuring a balanced approach between satisfying customers and other
interested parties (such as owners, employees, suppliers, financiers, local communities and society as a whole).
Principle 2 Leadership
Leaders establish unity of purpose and direction of the organization. They should
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
74
create and maintain the internal environment in which people can become fully
involved in achieving the organization's objectives.
Key benefits:
• People will understand and be motivated towards the organization's goals and objectives.
• Activities are evaluated, aligned and implemented in a unified way. • Miscommunication between levels of an organization will be minimized.
Applying the principle of leadership typically leads to:
• Considering the needs of all interested parties including customers, owners, employees, suppliers, financiers, local communities and society as a whole.
• Establishing a clear vision of the organization's future. • Setting challenging goals and targets. • Creating and sustaining shared values, fairness and ethical role models at
all levels of the organization. • Establishing trust and eliminating fear. • Providing people with the required resources, training and freedom to act
with responsibility and accountability. • Inspiring, encouraging and recognizing people's contributions.
Principle 3 Involvement of people
People at all levels are the essence of an organization and their full involvement
enables their abilities to be used for the organization's benefit.
Key benefits:
• Motivated, committed and involved people within the organization. • Innovation and creativity in furthering the organization's objectives. • People being accountable for their own performance. • People eager to participate in and contribute to continual improvement.
Applying the principle of involvement of people typically leads to:
• People understanding the importance of their contribution and role in the organization.
• People identifying constraints to their performance.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
75
• People accepting ownership of problems and their responsibility for solving them.
• People evaluating their performance against their personal goals and objectives.
• People actively seeking opportunities to enhance their competence, knowledge and experience.
• People freely sharing knowledge and experience. • People openly discussing problems and issues.
Principle 4 Process approach
A desired result is achieved more efficiently when activities and related resources
are managed as a process.
Key benefits:
• Lower costs and shorter cycle times through effective use of resources. • Improved, consistent and predictable results. • Focused and prioritized improvement opportunities.
Applying the principle of process approach typically leads to:
• Systematically defining the activities necessary to obtain a desired result. • Establishing clear responsibility and accountability for managing key
activities. • Analyzing and measuring of the capability of key activities. • Identifying the interfaces of key activities within and between the functions
of the organization. • Focusing on the factors such as resources, methods, and materials that
will improve key activities of the organization. • Evaluating risks, consequences and impacts of activities on customers,
suppliers and other interested parties.
Principle 5 System approach to management
Identifying, understanding and managing interrelated processes as a system
contributes to the organization's effectiveness and efficiency in achieving its
objectives.
Key benefits:
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
76
• Integration and alignment of the processes that will best achieve the desired results.
• Ability to focus effort on the key processes. • Providing confidence to interested parties as to the consistency,
effectiveness and efficiency of the organization.
Applying the principle of system approach to management typically leads to:
• Structuring a system to achieve the organization's objectives in the most effective and efficient way.
• Understanding the interdependencies between the processes of the system.
• Structured approaches that harmonize and integrate processes. • Providing a better understanding of the roles and responsibilities
necessary for achieving common objectives and thereby reducing cross-functional barriers.
• Understanding organizational capabilities and establishing resource constraints prior to action.
• Targeting and defining how specific activities within a system should operate.
• Continually improving the system through measurement and evaluation.
Principle 6 Continual improvement
Continual improvement of the organization's overall performance should be a
permanent objective of the organization.
Key benefits:
• Performance advantage through improved organizational capabilities. • Alignment of improvement activities at all levels to an organization's
strategic intent. • Flexibility to react quickly to opportunities.
Applying the principle of continual improvement typically leads to:
• Employing a consistent organization-wide approach to continual improvement of the organization's performance.
• Providing people with training in the methods and tools of continual improvement.
• Making continual improvement of products, processes and systems an objective for every individual in the organization.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
77
• Establishing goals to guide, and measures to track, continual improvement.
• Recognizing and acknowledging improvements.
Principle 7 Factual approach to decision making
Effective decisions are based on the analysis of data and information
Key benefits:
• Informed decisions. • An increased ability to demonstrate the effectiveness of past decisions
through reference to factual records. • Increased ability to review, challenge and change opinions and decisions.
Applying the principle of factual approach to decision making typically leads to:
• Ensuring that data and information are sufficiently accurate and reliable. • Making data accessible to those who need it. • Analysing data and information using valid methods. • Making decisions and taking action based on factual analysis, balanced
with experience and intuition.
Principle 8 Mutually beneficial supplier relationships
An organization and its suppliers are interdependent and a mutually beneficial
relationship enhances the ability of both to create value
Key benefits:
• Increased ability to create value for both parties. • Flexibility and speed of joint responses to changing market or customer
needs and expectations. • Optimization of costs and resources.
Applying the principles of mutually beneficial supplier relationships typically leads
to:
• Establishing relationships that balance short-term gains with long-term considerations.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
78
• Pooling of expertise and resources with partners. • Identifying and selecting key suppliers. • Clear and open communication. • Sharing information and future plans. • Establishing joint development and improvement activities. • Inspiring, encouraging and recognizing improvements and achievements
by suppliers.
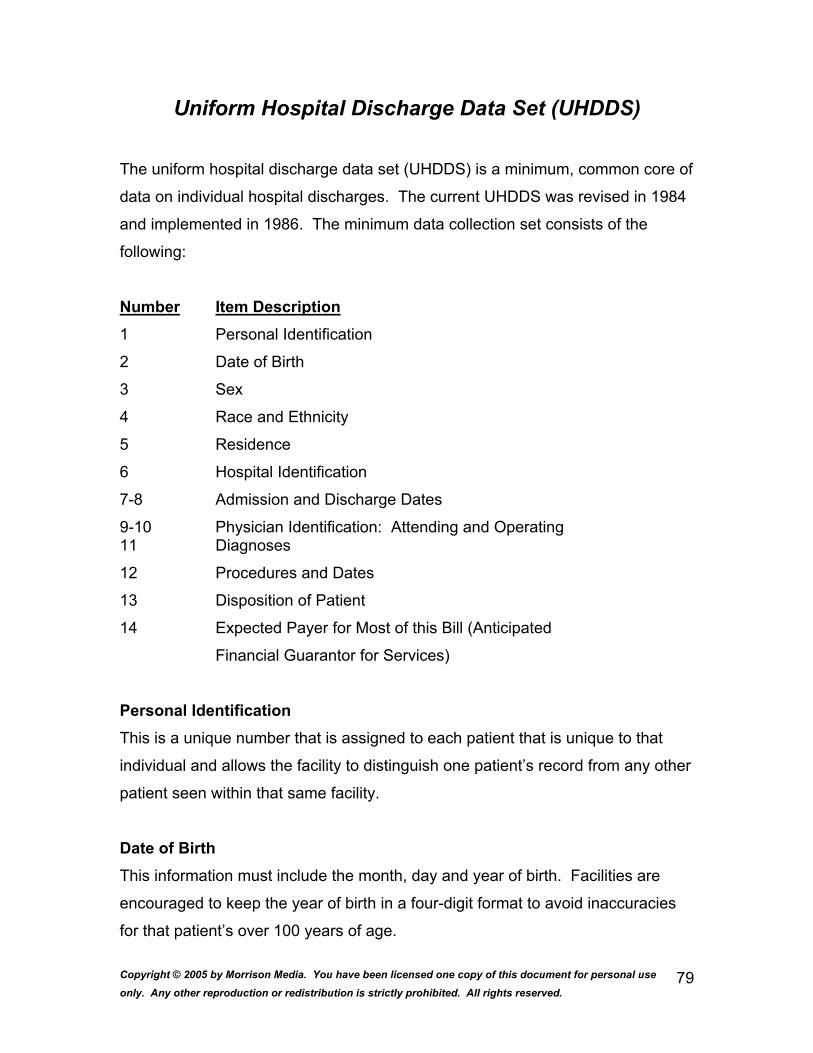
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
79
Uniform Hospital Discharge Data Set (UHDDS)
The uniform hospital discharge data set (UHDDS) is a minimum, common core of
data on individual hospital discharges. The current UHDDS was revised in 1984
and implemented in 1986. The minimum data collection set consists of the
following:
Number Item Description 1 Personal Identification
2 Date of Birth
3 Sex
4 Race and Ethnicity
5 Residence
6 Hospital Identification
7-8 Admission and Discharge Dates
9-10 Physician Identification: Attending and Operating 11 Diagnoses
12 Procedures and Dates
13 Disposition of Patient
14 Expected Payer for Most of this Bill (Anticipated
Financial Guarantor for Services)
Personal Identification This is a unique number that is assigned to each patient that is unique to that
individual and allows the facility to distinguish one patient’s record from any other
patient seen within that same facility.
Date of Birth This information must include the month, day and year of birth. Facilities are
encouraged to keep the year of birth in a four-digit format to avoid inaccuracies
for that patient’s over 100 years of age.
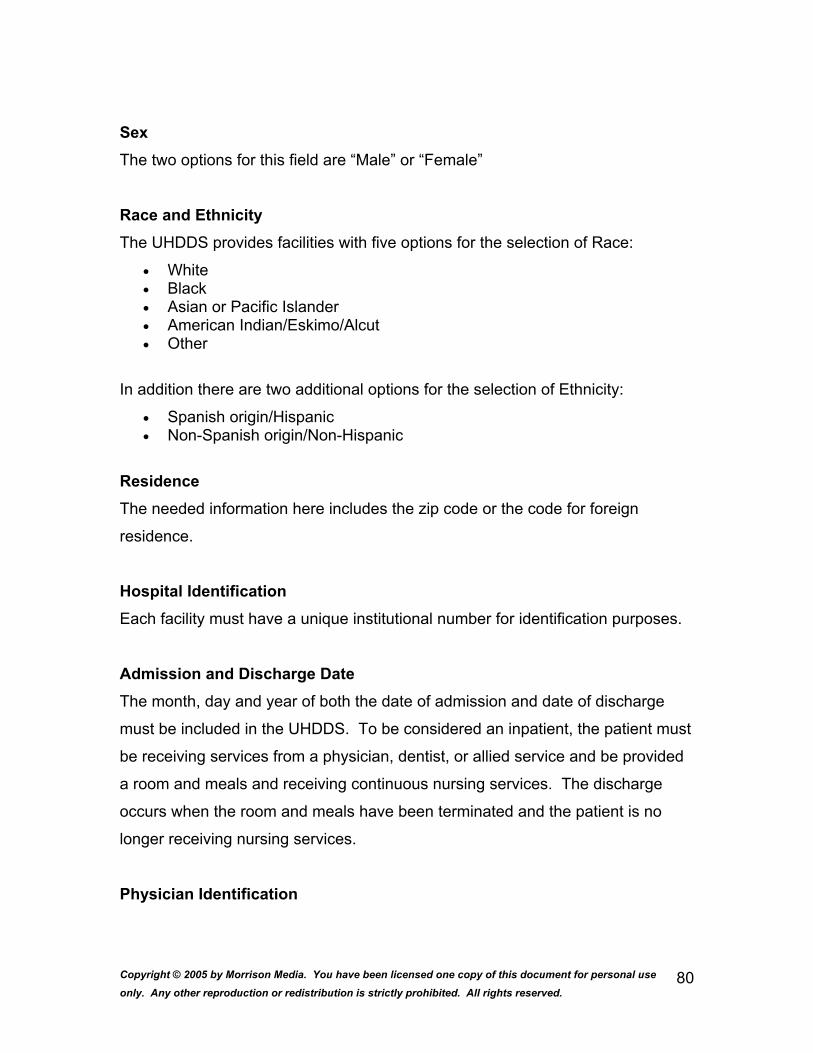
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
80
Sex The two options for this field are “Male” or “Female”
Race and Ethnicity The UHDDS provides facilities with five options for the selection of Race:
• White • Black • Asian or Pacific Islander • American Indian/Eskimo/Alcut • Other
In addition there are two additional options for the selection of Ethnicity:
• Spanish origin/Hispanic • Non-Spanish origin/Non-Hispanic
Residence The needed information here includes the zip code or the code for foreign
residence.
Hospital Identification Each facility must have a unique institutional number for identification purposes.
Admission and Discharge Date The month, day and year of both the date of admission and date of discharge
must be included in the UHDDS. To be considered an inpatient, the patient must
be receiving services from a physician, dentist, or allied service and be provided
a room and meals and receiving continuous nursing services. The discharge
occurs when the room and meals have been terminated and the patient is no
longer receiving nursing services.
Physician Identification
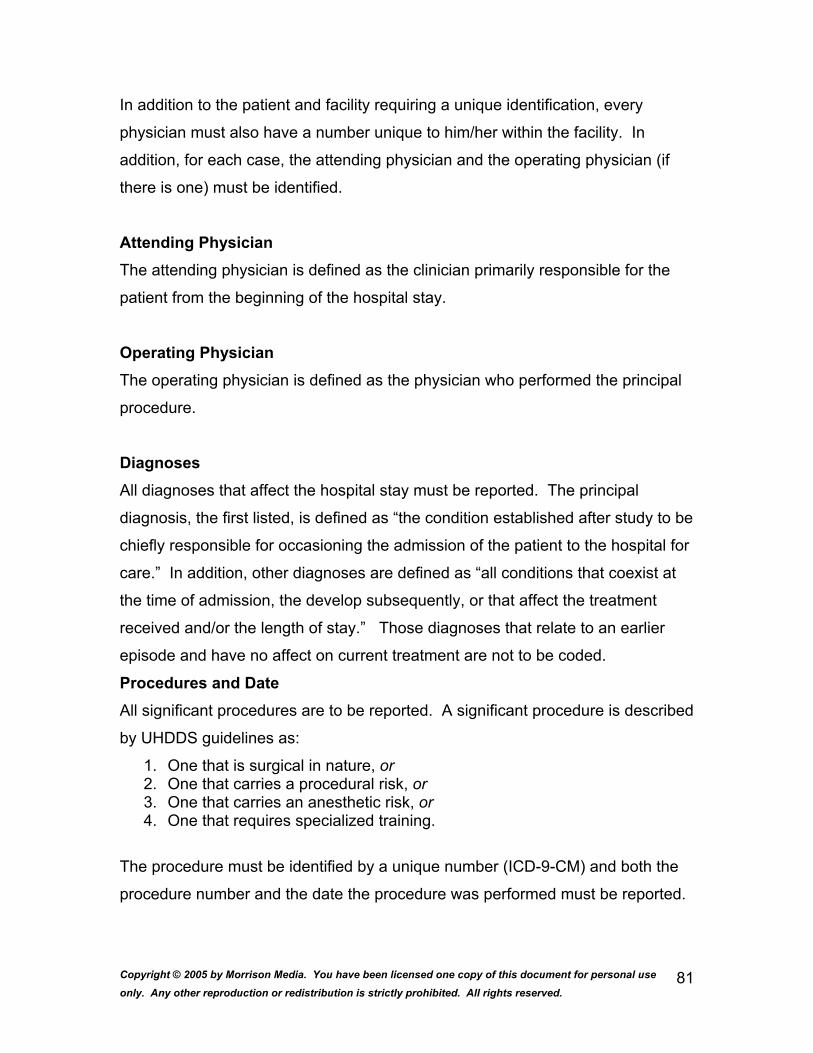
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
81
In addition to the patient and facility requiring a unique identification, every
physician must also have a number unique to him/her within the facility. In
addition, for each case, the attending physician and the operating physician (if
there is one) must be identified.
Attending Physician The attending physician is defined as the clinician primarily responsible for the
patient from the beginning of the hospital stay.
Operating Physician The operating physician is defined as the physician who performed the principal
procedure.
Diagnoses All diagnoses that affect the hospital stay must be reported. The principal
diagnosis, the first listed, is defined as “the condition established after study to be
chiefly responsible for occasioning the admission of the patient to the hospital for
care.” In addition, other diagnoses are defined as “all conditions that coexist at
the time of admission, the develop subsequently, or that affect the treatment
received and/or the length of stay.” Those diagnoses that relate to an earlier
episode and have no affect on current treatment are not to be coded.
Procedures and Date All significant procedures are to be reported. A significant procedure is described
by UHDDS guidelines as:
1. One that is surgical in nature, or 2. One that carries a procedural risk, or 3. One that carries an anesthetic risk, or 4. One that requires specialized training.
The procedure must be identified by a unique number (ICD-9-CM) and both the
procedure number and the date the procedure was performed must be reported.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
82
When more than one procedure is performed, one procedure must be designated
as the principal procedure defined by UHDDS as: “is one that was performed for
definitive treatment rather than one performed for diagnostic or exploratory
purposes, or was necessary to take care of a complication. If there appear to be
two procedures that are principal, then the one most related to the principal
diagnosis should be selected as the principal procedure.”
Procedural risk is also defined by UHDDS and is as stated: “a professionally
recognized risk that a given procedure may induce some functional impairment,
injury, morbidity, or even death. This risk may arise from direct trauma,
physiologic disturbances, interference with natural defense mechanisms, or
exposure of the body to infection or other harmful agents.”
An anesthetic risk is defined as “Any procedure that either requires or is
regularly performed under general anesthesia carries anesthetic risk, as do
procedures under local, regional, or other forms of anesthesia that induce
sufficient functional impairment necessitating special precautions to protect the
patient from harm.”
And specialized training refers to procedures that can only be performed by
specialized professional, qualified technicians or clinical team that are specifically
trained to carry out the procedure, or whose main purpose is to perform the
procedure.
Disposition of Patient The disposition of a patient must be reported to include any of the following:
1. Discharged to home (routine discharge) 2. Left against medical advice 3. Discharged to another short-term hospital 4. Discharged to a long-term care institution 5. Died 6. Other (allows “disposition of patient” to be all inclusive)
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
83
Expected Payer for Most of this Bill (Anticipated financial Guarantor for Services) The following is a list of options for reporting:
1. Blue Cross 2. Other insurance companies 3. Medicare 4. Medicaid 5. Workers’ Compensation 6. Other government payers 7. Self-pay 8. No charge (free, charity, special research, or teaching) 9. Other
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
84
Individual Differences in Organizations - Personality
What is Personality? Why is it Important?
Personality refers to the relatively stable and unique combination of attitudes,
beliefs, values which each individual possesses.
Personality shapes how we work and manage others in organizations (i.e., our
management and work style).
Goleman’s Emotional Intelligence - Self-Awareness
Definition
Refers to the ability to recognize and understand your moods, emotions, drives
as well as their effect on others.
• Hallmarks • Self-confidence • Realistic self-Assessment • Self-deprecating sense of humor
Goleman’s Emotional Intelligence - Self-Regulation
Definition
The ability to control or redirect disruptive impulses and moods.
The propensity to suspend judgment - to think before acting.
• Hallmarks • Trustworthiness and integrity • Comfort with ambiguity • Openness to change
Goleman’s Emotional Intelligence – Motivation
Definition
A passion to work for reasons that go beyond money or status.
A propensity to pursue goals with energy and persistence.
• Hallmarks • Strong drive to achieve • Optimism even in the face of failure
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
85
• Organizational commitment
Goleman’s Emotional Intelligence – Empathy
Definition
The ability to understand the emotional makeup of other people.
Skill in treating people according to their emotional reactions.
• Hallmarks • Expertise in building and retaining talent • Cross-cultural sensitivity
• Service to clients and customers
Goleman’s Emotional Intelligence - Social Skill
Definition
Proficiency in managing relationships and building networks.
An ability to find common ground and build rapport.
• Hallmarks • Effectiveness in leading change • Persuasiveness • Expertise in building and leading teams
Techniques for Boosting Emotional Intelligence
1. Manage emotions instead of suppressing them.
2. Recognize your “hot buttons.”
3. Become an optimist.
4. Read the emotions of others.
5. Use your EI to help others boost theirs.
The Abrasive Personality Type
1. Extremely Intelligent 2. Impatient 3. Intimidates Others 4. Perfectionist 5. Highly Analytical 6. Domineering

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
86
7. Inability to Delegate 8. Competitive 9. Lacks Tact
Techniques for Handling Abrasive Individuals
1. Understand the causes of the person’s behavior.
2. Report your observations to the person.
3. Recognize the person’s desire to achieve but manage his/her
expectations and goals.
4. Refuse to argue.
5. Expect to repeat the process.
Covey’s Seven Habits of Highly Effective People
1. Be proactive
2. Begin with the end in mind
3. Put first things first
4. Think win/win
5. Seek first to understand and then to be understood
6. Synergize
7. Sharpen the sword
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
87
Attitudes & Behaviors
What are Attitudes?
Attitudes refer to stable clusters of feelings, beliefs and behavioral intentions
toward specific objects, people or institutions.
Why are Attitudes Important?
1. Attitudes have important managerial implications because they are related
to subsequent employee behaviors.
2. Many companies hire for attitude and train for skills.
The General Attitude Model
Theories of Job Satisfaction-Locke’s Value Theory of Satisfaction
1. Determinants of Facet Satisfaction
a. Have-Want Discrepancy for a Facet
b. Importance of the Facet
2. Overall job satisfaction depends in the degree to which a person’s
MOST IMPORTANT job facets are being satisfied.
Managerial Implications: Locke’s Value Theory
1. Identify which facets are most important to your employees.
2. Assess the extent to which a have-want discrepancy exists for the most
important facets.
3. Identify and implement steps to reduce or eliminate have-want
discrepancies for the most important facets.
Mobley’s Satisfaction-Turnover Model
Key Components of the Model
1. Perceived Desirability of Movement
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
88
a. Job Satisfaction
b. Opportunities for Internal Organizational Transfer
2. Perceived Ease of Movement
a. Level of Business Activity
b. Visible Organizations
c. Personal Characteristics
Managerial Implications
1. If your objective is to retain employees within a specific work unit, seek to
achieve high employee job satisfaction and few perceived opportunities for
internal and external organizational transfer.
2. If your objective is to retain employees within an overall organization, seek
to achieve high job satisfaction, many opportunities for internal
organizational transfer and few opportunities for external organizational
transfer.
Steers and Rhodes Satisfaction-Attendance Model
Key Components of the Model
1. Job Satisfaction
2. Pressure to Attend
3. Ability to Attend
Steers and Rhodes Satisfaction-Attendance Model
Managerial Implications
1. Achieve and maintain high employee job satisfaction.
2. Enhance pressure to attend through organizational policies and practices.
3. Eliminate barriers that inhibits employees’ ability to come to work.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
89
Emerging Trend and Challenge – “Presenteeism”
• Presenteeism refers to employees who go to work despite the fact that they are sick or injured.
• Presenteeism can include migraines, colds/flu, back pain, hypertension, and allergies.
• Based on recent surveys, more 40% of employers reported that presenteeism is a major problem.
• Presenteeism costs U.S. companies more than $150 billion.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
90
The Perceptual Process
Perception: What is it and why is it important?
1. Perception is critical because it can vary widely by person.
2. Perception is the “reality” that individuals respond to in terms of
organizational behavior.
3. Differences in perception can erect barriers between people and work
units, cause conflict, undermine teamwork, and create resistance to
organizational change.
Fundamental Attribution Error
The tendency to attribute the causes of others’ behavior to internal rather than
external causes.
Example: District Manager at a Retailer
Perceptual Factors
• Halo Effect The tendency to create an overall negative or positive impression of someone
based on one dominant characteristic of that person.
• Similar-to-Me Effect The tendency to view others who are similar to us more favorably than those who
are not similar to us.
• Primacy/Recency Effects The tendency to place a disproportionate weight on what happens at the very
beginning and very end of an event or interaction.
Example: “Business Presentations, Performance Appraisals”
• Selective Perception The tendency to focus on certain information related to a person or issue.
Example: “The Good News Culture”
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
91
• Stereotypes The tendency to place people or issues into categories and to assume that every
person or issue in that category possesses certain attributes.
Examples: Perceptions of Americans, Professions
Perceptual Readiness
The tendency to perceive people or issues in a way which confirms our
expectations.
Example: Teamwork Experiences, Task Performance
Perceptual Defense
The tendency to maintain our perceptions of people or issues despite
disconfirming evidence.
Example: “Analog vs. Digital Phones at Motorola”
Guidelines for Reducing Perceptual Factors
1. Recognize external causes of behavior.
2. Be aware of stereotypes, biases and assumptions.
3. Reality test your understanding of a situation.
4. Emphasize objective information.
5. Avoid making rash judgments.
6. Seek information from a variety of sources.
7. Be empathetic (“Walk in the shoes of another for a mile”).
8. Actively manage the perceptions of others.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
92
Training & Development
What are Training and Development?
Training refers to the process of providing employees with specific skills or
helping them correct deficiencies in their performance.
Development refers to an effort to provide employees with the abilities the
organization will need in the future.
The Needs Assessment Phase
1. The primary activity in this phase is conducting a training needs analysis.
2. The key outcome of this phase is the identification of training objectives.
3. Levels of Training Needs Analysis
• Organizational Level • Task Level • Person Level
Guidelines for Effective Training Needs Analysis
• Use multiple-choice or yes/no question formats (survey) to make it easier for employees to respond.
• Use a 360 degree approach to collecting data. • Obtain information about the ideal conditions for delivering the training. • Use a 1-3 rating scale to elicit specific responses. • Leave room for respondents to write comments. • Ask employees about barriers to training and how to overcome them. • Limit questions to 25 or less. • Interview a cross-section of managers to obtain input into the process.
The Training Phase
1. The objective of this phase is to develop appropriate training content and
methods given the training objectives.
Audience Characteristics – Adult Learners
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
93
• Need to be involved and consulted. • Need feedback regarding how they are doing. • Learn in a variety of ways. • Want to be able to challenge the content and the process. • Enjoy being able to answer questions. • Are interested in obtaining practical solutions to their problems. • Like to be treated as equals. • Need to be challenged. • Want to be able to practice in a risk-free environment. • Need to build on their own knowledge and experience.
Guidelines for Effective Presentation of Training
• Stick to your agenda. • Listen to your trainees. • Deal with dysfunctional behavior. • Focus on your training objectives. • Provide a safe and appropriate learning environment. • Ensure equal participation. • Vary your training methods and delivery to maintain interest. • Have fun. • Review your agenda.
Guidelines for On-the-Job Training
• Decide on the best method for providing on-the-job training. • Provide developmental feedback for trainees on a regular basis. • Clearly define training objectives. • Formally evaluate the training program. • Develop appropriate training materials to support the process. • Train the trainer. • Block out specific time for training.
Guidelines for Effective Training Evaluation
• Base the training evaluation on the training objectives. • Assess trainee perceptions of the value of the training. • Assess trainee mastery of the training content. • Conduct a follow-up evaluation to assess the impact of the training on
employee performance and organizational effectiveness. • Obtain specific, quantifiable results that demonstrate the value of the
training.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
94
Common Reasons for the Failure of Training
• The reason for the training has not been identified. • The training tries to be everything to all people. • The needs of trainees were ignored or not taken into account. • The training is impractical. • Examples are unrealistic or unrelated. • The training is concentrated. • The supervisor is not involved. • The training is not reinforced back on the job.
Creating a Learning Organization that Supports Training
• Design hiring systems to assess capacity to learn and commitment to ongoing learning.
• Promotion criteria should include contributions to personal and team learning.
• Compensation systems should reward new skill acquisition. • Formal managerial responsibilities should include coaching and
mentoring. • Performance appraisal systems should include learning-related activities
and results as a criterion of performance. • Business plans and organizational goals should emphasize continuous
learning as a key source of competitive advantage.
Measures of Training Effectiveness
• Knowledge Change = Ka/Kb • Skill Change = Sa/Sb • Attitude Change = Aa/Ab • Performance Change = Pa/Pb • Training Hours Per Employee • Percentage of Employees Completing a Training Program • Training Investment Factor = Total Training Cost/Total Number of
Employees
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
95
Managing Work Motivation
What is Motivation?
Motivation is composed of two basic components:
1. Intensity - The amount of desire generated.
2. Direction - How intensity is channeled.
The FISH! Philosophy
Element #1 – Play!
Element #2 – Make Their Day
Element #3 – Choose Your Attitude
Element #4 – Be There
Practical Implications – Content Theories of Motivation
• Assess employee needs and identify those that are most active. • Develop and implement appropriate strategies to enable employees to
satisfy their active needs. • Use a variety of strategies to satisfy employee needs. • Conduct regular evaluations of your strategies for satisfying active
employee needs.
The Operant Conditioning Process
1. Stimulus (S) or Antecedent (A) – A signal, cue or specific context.
2. Response (R) or Behavior (B) - The target behavior that you want to
change.
3. Consequences (C) - Outcomes which occur based on a behavior.
Guidelines for Increasing Desired Employee Behaviors
• Make sure that you understand the S-R-C linkage. • Make sure that the consequence is positively valued by the employee. • Link positive consequences with the desired behavior more frequently to
facilitate acquisition of behavior. • Vary the frequency of using positive consequences to maintain the desired
behavior.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
96
• Vary the type of positive consequences used. • Watch the costs associated with administering positive consequences.
Guidelines for Eliminating Undesired Employee Behaviors
• Make sure that you understand the S-R-C. • Make sure that the consequence is negatively valued by the employee. • Make sure to explain the desired behavior to the employee. • Be aware of other negative consequences that may result from the use of
punishment. • Use punishment only when there is a real need to do so.
Locke and Latham’s
Goal-Setting Theory
• Goal-Directed Effort • Goal Difficulty • Goal Specificity • Goal Acceptance • Goal Commitment
Goal-Setting Theory: Managerial Implications
1. Set good goals.
2. Provide support.
3. Link appropriate outcomes to goal achievement.
Adams’s Equity Theory
Motivation Resulting From Equity Comparisons
a. Equitable Payment
b. Underpayment Inequity
c. Overpayment Inequity
Managerial Implications of Equity Theory
Monitor and manage employee perceptions of equity with the objective of
achieving perceived payment equity.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
97
Business and Its Environment
Statute of Frauds- Deception deliberately practiced with a view to gaining an
unlawful or unfair advantage; artifice by which the right or interest of another is
injured; injurious stratagem; deceit; trick
Duress-
a. Coercion illegally applied.
b. Forcible confinement
In law an agent is a person authorized to do some act or acts in the name of
another, who is called his principal.
Be familiar with different types of insurance and laws pertaining to consigned
goods.
Torts In the common law, a tort is a wrong for which the law provides a remedy. The
term comes from Law French and means, literally, 'a wrong'. The "law of torts" is
a body of civil law or private law that covers the various legal (money damages
and equity remedy) which the law provides for civil wrongs arising from extra-
contractual liability, i.e., other than those wrongs which arise from a breach of
contractual obligations.
Under United States law, torts are generally divided into two categories:
intentional torts and non-intentional torts. Intentional torts include those actions
that are intentional and voluntary and that are made with knowledge by the
tortfeasor (i.e. the person who committed the tort) upon the plaintiff (the one who
brings the complaint seeking relief). Intentional torts include: battery, assault
(apprehension of harmful or offensive contact), false imprisonment, intentional
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
98
infliction of emotional distress, the real property tort of trespass to land, and the
personal property torts of conversion and trespass to chattels.
Amongst unintentional torts one finds negligence as being the most common
source of litigation in most American courts. It is a form of extracontractual
liability that is based upon a duty of care of a reasonable person, who, being the
proximate cause of damages, and but for the tortfeasor's act, is the cause of
damages to the plaintiff. Other non-intentional torts include negligent infliction of
emotional harm.
There is some overlap between tort law and criminal law -- some acts may at
once constitute both a tort and a crime -- and many crimes may be viewed as
particularly egregious torts. A cause of action in tort can also be distinguished
from a criminal prosecution which may arise from the alleged violation of a
criminal statute. The former is typically prosecuted by a private citizen, whereas
the latter is prosecuted by the state, and one or both may be brought forth
independently. Moreover, remedies for torts can take the form of compensation
for damages or injunctive relief. A criminal prosecution usually results in the
imposition of a sentence, such as a fine and/or incarceration
Res ipsa loquitur
[Latin: the thing speaks for itself]. An expression used in tort to refer to situations
where negligence is presumed on the defendant since the object causing injury
was in his or her control. This is a presumption that can be rebutted by showing
that the event was an inevitable accident and had nothing to do with the
defendant's responsibility of control or supervision.
Contributory negligence
The negligence of the claimant which, while not being the primary cause of a tort,
nevertheless combined with the act or omission of the defendant to cause the
tort, and without which the tort would not have occurred
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
99
Employment Laws
• Civil Rights Act of 1991 • Put burden of proof on employers. • Quotas are illegal. • Permitted trials by jury where punitive and compensatory damages are
sought. • Expanded the right to bring actions challenging discriminatory seniority
systems. • Limited the extent to which reverse discrimination lawsuits could be
brought.
Major Employment Laws and Regulations
• Sexual Harassment • Quid Pro Quo Sexual Harassment - A manager who gives an employee
preferential treatment in exchange for “sexual favors.” • Hostile Work Environment Sexual Harassment - When the behavior of
someone in the work setting is sexual in nature and is perceived by an employee to be offensive and undesirable.
Behaviors that May Constitute Sexual Harassment
• Touching • Telling sexually-oriented jokes • “Elevator Eyes” • Allowing pin-up calendars, sexually-oriented images in the workplace • Making sexually-oriented comments. • Repeatedly making unwanted sexual advances toward another employee • Making conditions of employment based on “sexual favors” • Physical assaults (e.g., grabbing)
Sexual Harassment – Practical Guidelines
• Create a zero tolerance policy. • Provide training. • Provide support for the person who filed the complaint (e.g., EAP). • Conduct periodic employee attitude surveys to gauge the effectiveness of
the policy. • Implement a grievance procedure. • Follow the company policy. • Conduct a thorough investigation and document the timeline of events. • Evaluate managers based on their effectiveness in implementing the
policy.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
100
• Work with your HR representative. • Treat every complaint seriously. • Do not transfer or fire anyone based on a sexual harassment complaint
alone. • Obtain support of top management.
Major Employment Laws and Regulations
Pregnancy Discrimination Act of 1978
• Protects pregnant employees from discrimination in employment. • Employers must allow pregnant employees to work until it affects their
performance and the disability is at a level that is comparable to other conditions where workers could not continue.
• Employers must allow women to return to work after childbirth on the same basis as for other disabilities.
Employers may not do the following:
• Refuse to hire a pregnant employee. • Terminate an employee after discovering the employee’s pregnancy. • Fail to permit the employee to be part of the normal cycle of office culture. • Refuse to provide lighter duty, if the employee needs it.
Religious Discrimination
• Employers cannot question the acceptability of an employee’s religion. • The employer should be conscious of potential religious conflicts in
developing and implementing workplace policies. • The employer must make a good faith effort to make reasonable
accommodations for employees based on religion so long as they do not constitute an “undue hardship” to the employer.
Age Discrimination in Employment Act of 1967
• Prohibits discrimination against individuals who are 40 years-old or older. • Guidelines for overcoming or preventing age discrimination include: • Audit organizational culture. • Rethink and change attitudes about older workers. • Assess and modify HR practices that may discriminate against older
workers. • Include older workers in diversity task forces.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
101
Major Employment Laws
The Americans with Disabilities Act (ADA) prohibits discrimination in employment
practices against an individual with a physical or mental disability who is
otherwise qualified.
1. Key issue is whether a disabled person can perform the "essential functions of a job." 2. The employer is obligated to make "reasonable accommodations“ for
employees who are otherwise qualified. 3. Accommodations may not present an "undue hardship” to the employer.
Examples of Reasonable Accommodations
• Lap boards • Voice responsive computers • Robotic devices • Telephone amplifiers • Flexible work arrangements • Walking canes • Computer screen magnifiers • Delivered lunches • Automatic page turners • Affirmative Action • Purpose
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
102
Accounting/Budgets
Asset-
a. The entries on a balance sheet showing all properties, both tangible
and intangible, and claims against others that may be applied to
cover the liabilities of a person or business. Assets can include
cash, stock, inventories, property rights, and goodwill.
b. The entire property owned by a person, especially a bankrupt, that
can be used to settle debts.
Liability- A financial obligation, debt, claim, or potential loss
Income- The amount of money or its equivalent received during a period of time
in exchange for labor or services, from the sale of goods or property, or as profit
from financial investments.
Cost- An amount paid or required in payment for a purchase; a price
Expense- An expenditure of money; a cost
Debit-
a. An item of debt as recorded in an account.
b. The left-hand side of an account or accounting ledger where
bookkeeping entries are made.
c. An entry of a sum in the left-hand side of an account.
d. The sum of such entries
Credit-
a. The deduction of a payment made by a debtor from an amount due.
b. The right-hand side of an account on which such amounts are
entered.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
103
c. An entry or the sum of the entries on this side.
d. The positive balance or amount remaining in a person's account.
e. A credit line
Net Income- the excess of revenues over outlays in a given period of time
Balance Sheet- A statement of a business or institution that lists the assets,
debts, and owners' investment as of a specified date
Income Statement- a financial statement that gives operating results for a
specific period
Depreciation- An allowance made for a loss in value of property
Know the basic accounting cycle and the components of a journal entry that uses
double-entry accounting methods. Know how to prepare a end of fiscal period
statement accounts.
Inventory methods: Average cost LIFO- Last in first out FIFO- First in first out
Know the types of depreciation:
Declining Balance Straight Line Sum of the year’s digits
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
104
Budgets
The budget is one of the manager's most important tools. Carefully crafting a
budget can be key to obtaining additional resources. There are three ways to
improve the budgeting process to ensure sufficient control over expenditure of
resources.
1. Develop clear formal budget organization. Know who is responsible for the budget in each department.
2. Set up financial accounts for each department. (Expenses and income that are traceable to specific staff members for more efficient control.)
3. Plan well in advance and anticipate unexpected windfalls; or on the downside, emergencies that require reallocation of funds.
Because gaining resources is a very competitive process, the manager needs to
be high in the administrative hierarchy, eloquent in articulating budget needs, and
persistent in following thorough with questions or concerns from the budget
granting agency.
As a planning document, the budget is a presentation of the organization's
objectives in terms of specific programs to be carried out during a specified
period of time -- usually one year. Following is a simple overview of major kinds
of budgets.
I. Line Item Budget
Line item budgets are the most common type of budget and are often called
incremental budgets, because typically just a small amount of funding is added
each year. The advantages of a line item budget are:
• Easy to prepare • Easy to understand • Easy to justify.
People understand that costs always go up! The big disadvantage is that there is
no relationship between the budget request and objectives and priorities, and it is
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
105
different to transfer from one line item to another. Finally, the line item budget
negates change. It tends to project the past into the future.
II. Formula Budget
The formula budget is sometimes used in large library systems, and state or
federal agencies. It uses predetermined standards for allocation of resources.
Budget criteria are established and then applied across the board to all units
within the system. This type of budget is focused on input rather than activities.
III. Program Budget
Program budget is concerned with the organization's activities, as opposed to
expenditures - goes hand-in-hand with strategic planning. Based on establishing
costs of individual programs, so one can look at the total costs of a program and
decide whether to continue, modify and delete.
The advantages of a program budget are:
• easier to evaluate programs since costs are tied to results • priorities can be changed quickly • smaller more manageable budget units
IV. Performance Budgets
Performance budgets are similar to program budgets, but here the emphases are
on costing out functions. All fixed costs are added in. Emphasis is on quantity
not quality.
V. Planning, Programming, Budgeting Systems (PPBS)
PPBS is a form of planning a combination of program budgeting and
performance budgeting. First, goals and measurable objectives are established.
Then develop costs of achieving each of the objectives including alternate ways
to achieve the objectives with cost benefit rations presented for each.
VI. Zero Based Budgeting

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
106
Focus on two basic questions
1. Are current activities efficient and effective? 2. Should current activities be eliminated or reduced to fund higher-priority
new programs or to reduce the current budget?
With ZBB each unit of the budget must be justified, and placed in a hierarchy.
Activities are broken into packages and funds are allocated by priority until all
funds have been expended, and the cut off point is reached.
This process requires the identification of goals and objectives, the reason for the
activity, consequences of not implementing the package, detailed measurement
of performance and costs of the activity. Ranking decision packages focuses
decisions about the most important activities in each unit of the organization.
After each unit identifies its priorities, the priorities of all units are amalgamated
into one pool in light of the decision package's importance to the total
organization.
Basically, ZBB is not concerned with the past, but with what should be done in
the future. By forcing staff to identify areas of greater and lesser importance, it
emphasizes standing among all units of the organization. ZBB can be threatening
to staff - the fact that each program starts in the lineup at zero base every year.
The advantages of ZBB are:
• combines planning, budgeting, and decision making into one process; • more involvement by staff can be good for morale; • may save money; • conducive to change; • easier to justify budget.
The disadvantages of ZBB are:
• threatening • time consuming • requires more paperwork • requires extensive training in the techniques • prioritizing process can be highly political.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
107
VII. Allocation Revision Accountability Systems (ADAP)
ADAP combines aspects of PPBS and ZBB. Normally, the organization or unit submits three budgets
1. Budget increase 2. Modest increase 3. Budget below which organization cannot function.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
108
Communication in Organizations
What is Communication?
Communication is the process through which messages are transmitted and
interpreted by two or more individuals.
Why is Communication Important?
1. It’s not just WHAT you say, but also HOW you say it that matters!!
2. If you can’t communicate, don’t expect others to do what you want them to
do.
3. Communication skills are one of the best predictors of “success” in the
business world.
The Basic Communication Process
The Sender
IDEA – ENCODING OF IDEA – Taking an idea and translating it into an
appropriate message. The Basic Communication Process
The Receiver
DECODING – IDEA RECEIVED – Interpreting a message and receiving it.
The Roles of Noise and Feedback
There are many barriers to communication. Feedback is the reply or return
message from the receiver.
“Gender Differences in Communication”
MALES
Emphasize status Nonverbals (less eye contact)
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
109
Use “I” Ritual opposition Offer advice or solutions Direct style of giving orders
FEMALES
Downplay their status Nonverbals (more direct eye contact) Focus on social connections (“we”) Ritual apology Offer social support Indirect style of giving orders
General Guidelines for Managing the Grapevine
• Take the attitude that it is better to give too much information than not enough.
• Never deny or lie about the truth – your credibility will suffer and mistrust will increase.
• Hold regular meetings to provide updates and to answer questions. • Go to the source of the rumor, collect information about the “truth” and
share the facts with employees. • Anticipate issues that might provoke gossip and deal with them right away.
General Guidelines for Effective Upward Communication
• Always keep your boss informed of the situation. • Focus on solutions not problems. • Follow the chain of command. • If you have a pressing issue, make an appointment with your boss. Be
sure to state your objective and the amount of time needed. • Play close attention to how you frame your message. • If you are unsure how your boss will respond to an issue, run it by him/her
in writing first. • When presenting information, be sure to provide written documentation. • Be as concise as possible.
General Guidelines for Effective Employee Communication
• Encourage communication from your people (e.g., open door policy, walking around).
• Don’t just tell employees what to do – tell them why. • Ask for employee opinions (e.g., suggestion systems, brown bag lunches).

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
110
• Maintain a positive approach (look, smile, and act interested). • Demonstrate respect for your associates by listening to them and showing
interest in their ideas. • Don’t voice disagreement with your boss’s instructions to your employees.
Voice them to your boss.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
111
Leadership
House's Path-Goal Theory Practical Implications
• Change the situation. • Train the leader to match the situation. • Replace the leader.
Hersey-Blanchard's Situational Leadership Theory Practical Implications
• Train the leader to match the situation • Replace the leader • Change the situation
Ciampa and Watkins Leadership Theory Practical Implications
• A new leader has 2-3 years to make measurable progress in changing the culture and improving financial performance.
• A new leader should understand the organization's current strategy and goals.
• During the first six months, the leader must develop and test hypotheses about operating priorities.
• New leaders must balance an intense, single-minded focus on a few priorities with flexibility about when and how they are implemented.
• New leaders must make key decisions about the organizational architecture of the firm. The leader must decide whether the composition of the inherited team is appropriate.
• After six months, the leader must have some personal credibility and momentum for sustained improvements in performance.
• The new leader must earn the right to transform the • organization. It is critical to build coalitions supportive of change. • TThere is no best way to manage a leadership transition.
Charney’s Guidelines for Effective Leadership
• Have a clear vision of what you are working towards. • Give credit to those who have earned it. • Be flexible. • Be consistent in terms of your principles and values. • Confront issues as they arise.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
112
• Reflect on and learn from mistakes – admit when you are wrong. • Walk the talk – be willing to do what you expect of others. • Let people know how they are doing. • Treat staff as individuals.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
113
Stress Management
What is Stress?
Stress refers to the pattern of emotional states, cognitions, and physiological
reactions occurring in response to stressors.
The PRIMARY attribute of stress is that it is physiological in nature.
Why is Stress Important?
• 43% of all adults suffer adverse effects from stress. • 75-90% of all physician office visits are for stress-related ailments. • Stress costs U.S. industry more than $300 billion dollars per year, or
$7,500 per worker. • U.S. workers put in an average of 47 hrs./week. On an annual basis, U.S.
workers work one month more than Japanese and three months more than German workers.
• Incidents of “going postal,” “desk rage,” and “office rage” continue to increase in the workplace.
The Stress Process Model
The Major Components
1. Stressors 2. Stress 3. Stress Reactions 4. Personality Characteristics
Stressors - Causes of Stress
Types of Stressors
1. Role Conflict 2. Role Ambiguity 3. Underload Stressors
a. Qualitative Underload b. Quantitative Underload
4. Overload Stressors
a. Qualitative Overload b. Quantitative Overload
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
114
5. Responsibility for Others 6. Lack of Social Support 7. Sexual Harassment 8. Unpleasant Physical Working Conditions 9. Causes of Stress Outside Work
Stress Management Techniques
1. Reduce or eliminate stressors. • Job Redesign • Flexible Work Arrangements • Work-Life Balance Programs • “Fighting Stress on the Job” and • “Pets to Work”
2. Treat the person’s reactions to stress. • Employee Wellness Programs
3. Modify the person’s ability to cope with stress. • Stress Management Workshops • Employee Assistance Programs • Wellness Programs
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
115
What is Decision Making?
Why is Decision Making Important?
1. Managers make many decisions each day.
2. Managerial decisions have a real and significant impact on work unit and
organizational effectiveness.
3. A systematic and thorough decision making process will enhance the
likelihood of managerial and organizational effectiveness (i.e., “your
batting average”).
Why is Decision Making NOT Just an Issue of Common Sense?
1. Real world problems are often highly complex and dynamic.
2. The information available to support decision making is often unavailable
or unreliable and invalid.
3. Time and resource constraints make it extremely difficult to effectively
identify and evaluate decision alternatives.
4. Political factors constrain the ability of a decision maker to “do the right
thing.”
5. The “bias for action” and concern for efficiency as primary criteria of
success short circuit the decision making process.
6. Making the right decision is linked with weak implementation or execution.
Decision Making Models
The Rational-Economic Model of Decision Making
1. Identify the problem.
A discrepancy between a current condition and a desired end.
2. Define objectives.
Identify evaluation criteria for decision.
3. Make a pre-decision.
Amount of participation
How to decide

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
116
4. Generate alternatives.
Think “outside the box”
5. Evaluate alternatives.
Evaluate each alternative using the same criteria.
6. Make a choice.
7. Implement choice.
8. Follow-up.
Evaluate outcome against evaluation criteria.
Assumptions of the
Rational-Economic Model
1. Perfect information
2. Ability to generate all alternatives
3. Objective criteria for ranking alternatives
4. Unlimited time to make the decision
5. Choice of alternatives will maximize outcomes
Decision Making Styles
The Directive Style
Prefers simple, clear solutions
Makes decisions rapidly
Does not consider many alternatives
Relies on existing rules
The Analytical Style
Prefers complex problems
Carefully analyzes alternatives
Enjoys solving problems
Willing to use innovative methods

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
117
The Conceptual Style
Socially-oriented
Humanistic and artistic approach
Solves problems creatively
Enjoys new ideas
The Behavioral Style
Concern for their organization
Interest in helping others
Open to suggestions
Relies on meetings
Practical Guidelines for Preventing or Overcoming Groupthink
• Do a critical evaluation of group ideas “openly.” • Have key members take a neutral stance on solutions. • Hold discussions with outsiders to obtain reactions. • Assign the role of devil’s advocate to a group member. • Form subgroups to develop alternative solutions. • Hold second chance meetings to reconsider major decisions.
Barriers to Making Effective Decisions
• Reliance on Heuristics Availability (convenience)
Example: Making scholarship or admissions decisions based on GPA.
• Representative ness (stereotype) -1 Example: Medical diagnosis
Barriers to Making Effective Decisions
Bias Toward Implicit Favorites
Example: Creating a committee, run a focus group, throwing more money
at an initiative
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
118
Escalation of Commitment
Example: NBA basketball players,
Organizational Barriers to Decision Making
• Time Constraints • Political “Face Saving” • Bounded Discretion
Strategies for Improving Decision Making
• Recognize your personal decision making biases. • Vary the decision making style (degree of participation) depending on the
situation. • Involve colleagues who see the world differently from you. • Fight the temptation to solve today’s problem with yesterday’s solution. • Make sure that you are solving the right problem. • Consider as many solutions as possible. • Analyze the “worst case scenario” associated with implementing your
solution and what to do about it. • When making a decision that affects others, share the reasoning behind
the decision.
Strategies for Improving Decision Making
• Ask lots of questions. • Learn from prior decisions. • Prioritize decisions into short-term and long-term priorities. • Use a “Plan-Do-Check-Act Cycle” of decision making. • Focus on decision effectiveness and not just decision efficiency.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
119
Compensation & Benefits
What is Compensation?
1. Compensation refers to the total value of outcomes given to employees in
exchange for their membership in the organization and for performing the
tasks, duties and responsibilities associated with their jobs.
2. Total compensation = Base Pay + Performance-Based Pay + Indirect
Compensation
Objectives of an Effective Compensation System
1. Employee attraction, motivation and retention
2. Externally competitive
3. Equitable, fair and rewarding
4. Legal compliance
5. Cost-effective
6. Compatible with mission and culture
Steps in the Development of a Compensation System
1. Conduct a job analysis.
2. Write job descriptions.
3. Determine job specifications.
4. Rate worth of jobs. (job evaluation)
5. Create a job hierarchy.
6. Classify jobs by grade levels.
7. Price jobs. (market-based salary)
8. Develop pay structures (salary ranges)
What is Job Evaluation?
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
120
Job evaluation is the process through which the relative worth of jobs in an
organization is determined. Job evaluation provides the foundation for
determining the salary ranges for jobs.
External Equity - Examples
Battle of Network News Magazines
Tom Brokaw - $7 million per year with NBC
Diane Sawyer - Above $7 million per year with ABC
Barbara Walters - More than all peers with ABC
Steps in Conducting a Market/Salary Survey
1. Identify benchmark or key jobs.
2. Collect salary data based on market surveys for key jobs.
3. Complete the structure for non-benchmark jobs.
4. Establish a pay policy.
a. Lead Strategy
b. Match Strategy
c. Lag Strategy
Key Considerations in Formulating a Total Compensation Strategy
• What is the organization’s vision/mission? • What are the organization’s objectives and strategic priorities? • What are the demographics of the work force? What benefits do they need
and want? • Who are the organization’s competitors for labor? Does it want to lead,
match, or lag? • Is compensation an entitlement or based on merit? • How cost effective is the administration of the system? • How much flexibility can be included in the system? • What are the legal requirements and how can they be met? • What is the best way to communicate options to employees and
management?
Purposes of Broadbanding
• To provide wider salary ranges.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
121
• To reduce the number of distinctions made based on job value. • To provide more autonomy to managers. • To enhance employee mobility.
Special Cases in Compensation
• Red Circle Rate – A situation in which an employee’s pay is above the maximum salary for the salary range associated with his/her job.
• Green Circle Rate – A situation in which an employee’s pay is below the minimum salary for the salary range associated with his/her job.
Types of Base Pay Systems
1. Flat or Single-Rate System
2. Time-Based Step Rate System
3. Combination Step-Rate and Performance System
What is Performance-Based Compensation? Why is it Important?
Performance-based pay refers to that part of an employee’s total compensation
which is based on job performance.
Performance-based pay is important because it has a significant impact on key
HR outcomes such as attraction, motivation, and retention of employees.
Types of Performance-Based Pay Systems
Merit Pay Systems
Salary Ranges
Maximum $60,000 Midpoint $50,000 Minimum $40,000
Guidelines for Making Merit Pay Systems Effective
• Develop accurate performance appraisal systems. • Train supervisors in performance appraisal.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
122
• Tie rewards closely to performance ratings. • Use a wide range of increases to differentiate between performance levels
Types of Performance-Based Pay Systems
Individual Incentive Pay Systems
1. Piece Rate Systems
2. Commissions
3. Bonuses
a. Discretionary
b. Performance-Based
Types of Performance-Based Pay Systems
Group Incentive Pay Plans - Gainsharing
• Teamwork is enhanced and coordinated within work groups. • Employees focus their attention on business operations and goals. • Employees become knowledgeable about the entire business. • Employees work harder and smarter. • Individuals and groups generate ideas for working more effectively. • Work assignments are more flexible.
Group Incentive Pay Plans – Scanlon Plans
• Participative Management • Joint Administration by Management and Employees • Formulas Used to Calculate Amount of the Bonus
Types of Performance-Based Pay Systems
Group Incentive Pay Plans – Improshare Plans
50/50 division of productivity gains between the organization and
employees.
Example: Improshare System
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
123
Types of Performance-Based Pay Systems
Organization-Based Pay Systems
1. Cash Profit Sharing Plans 2. Deferred Profit-Sharing Plans 3. Stock Bonuses or Stock Options
Guidelines for an Effective Incentive System
• Tie the plan to the organization’s business strategies. • Relate pay increases to organizational performance, both bottom-line and
quality driven. • Involve employees as partners. • Transfer from the concept of pay as reward entitlement. • Transfer more risk to employees. • Award incentives on both individual and team bases. • Use the compensation professional as an internal consultant.
Challenges Associated with Performance-Based Pay Systems
1. Lack of control over drivers of performance 2. Difficulties in measuring performance 3. Rewards are too small 4. Managers who are unwilling to differentiate pay based on performance 5. Employees who think that they are "above average"
What is Indirect Compensation? Why is it Important?
Objectives
1. To reward continued employment. 2. To promote loyalty. 3. To enable employees to live healthier, less worrisome lives. 4. To create a “social contract” to protect the financial and physical well-
being of employees.
Types of Employee Benefits (1,2)
Statutory Benefits
A. Social Security/Medicare
1. Provides retirement, disability, death and survivor’s benefits.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
124
2. Medicare covers hospital insurance (Medicare A) and optional medical insurance (Medicare B) for people after age 65. 3. This is a matching program with employers and employees paying same
taxes (6.2% on first $62,700 for Social Security and 1.45% on all earnings for Medicare.
4. For individuals born 1960 or later, 67 is the age for eligibility to receive full benefits.
5. Disability benefits are paid to workers (and dependents) if they have a physical/psychiatric impairment that prevents them from working for at least 5 months and is expected to continue for 12 months or result in death.
6. Survivor’s benefits paid to eligible dependents including: surviving spouse 60 or older (50 if disabled), unmarried children under age 18, and dependent parents age 62 or older.
7. Challenges Facing Social Security • Boomers and younger generation are paying more than they receive. • People are living longer. • Retirement age will not shift from 65 to 67 until 2027. • Fewer workers to support each retiree. • The earnings test penalizes those that must work but not those who have
other non-wage sources. • Means testing results in some people receiving more than they need,
while others receive less than they need.
Statutory Benefits
B. Unemployment Insurance 1. This is a mandatory program that provides a subsistence payment to employees between jobs. 2. This program is funded primarily by employers. C. Worker’s Compensation 1. This is a state insurance program that protects workers in case of a work-
related injury or disease that results from employment. 2. It is funded by a payroll tax that is paid to an insurance company or state
fund based on experience. D. Family and Medical Leave 1. FMLA states that employers with 50 or more employees are required to
grant up to 12 weeks of unpaid leave in order to care for new children, to care for a sick family member, or for a serious health condition.
2. Employers are required to maintain health care benefits, to reinstate the employee, and to post appropriate notices.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
125
Work-Life and Work-Family Balance Programs
• Flextime • Alternative Work Schedules • Flexible Benefits • Telecommuting • Job Sharing • On-Site Child Care • Wellness Programs • Tuition Reimbursement • Leave Policies • EAPs • Elder Care Benefits
Characteristics of Effective Benefit Programs
1. Specific objectives 2. Employee involvement 3. Flexibility 4. Willingness to modify benefit mix 5. Communication of benefits information 6. Administrative cost controls 7. Promote wellness programs
Measures for Evaluating the Effectiveness of Compensation
and Benefits
• Job Evaluation Factor = JE/J • Salary Range Exception Factor = EX/E • Cost to Supervise = TSS/TS • Benefit to Payroll Ratio = TBC/TPC • Percentage of Sick Leave to Total Pay • Percent of Employees Who Use a Plan (Utilization)
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
126
Managing Teams
What are Groups vs. Teams?
A group is a collection of two or more individuals who maintain stable patterns of
relationships, share common goals and perceive themselves as a group.
A team is a group whose members have complementary skills and are
committed to a common purpose to which they hold themselves mutually
accountable.
Why Managing Teams is NOT Common Sense
1. Some employees do not like having their job performance dependent
on others.
2. Each member of a team has a unique personality and work style that may
not be compatible with those of other team members.
3. Political factors create barriers to teamwork.
4. The team cannot obtain clarity regarding its primary objectives.
5. A lot of teams do not understand how to define teamwork given the task.
6. The roles of respective team members are not clearly defined.
7. The culture of the organization may not support teamwork.
8. Effective team management requires ongoing planning, coordination, and
communication that become very time consuming.
McCaskey Framework for Analyzing Teams
Examples of Analyzing Team Systems Using McCaskey
A team that is given the task of designing innovative new products (task
requirements) does not possess the right mix of individuals to get the job done
(people).
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
127
A team given the responsibility for running one of a company’s business lines
(task) possesses extremely bright and competent individuals (people) but does
not have a value system and norms that encourage cooperation and teamwork
(culture).
The strategy and structure of the organization (context) do not support the
objectives, strategies and structures of a team (formal organization).
McCaskey Framework for Analyzing Teams
Practical Implications
1. Monitor each dimension of the model on an ongoing basis.
2. Evaluate the degree of fit or alignment between various dimensions of the
model.
3. Take action to modify specific dimensions of the model in order to achieve
better fit or alignment. This will enhance the effectiveness of the overall
team.
Characteristics of Hot Groups
1. Total preoccupation with task
2. Intellectual intensity, integrity and exchange
3. Emotional intensity
4. Fluid structure/small size
Practical Guidelines for Creating Hot Groups
• Make room for spontaneity. • Break down barriers. • Encourage intellectual exchange. • Select talented people and respect their self-motivation and ability. • Use information technology to build relationships. • Value truth and the speaking of it.
Maxwell’s 17 Indisputable Laws of Teamwork
1. “The Law of Significance” – One is too small to achieve greatness
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
128
2. “The Law of the Big Picture” – The goal is more important than the role
3. “The Law of the Niche” – All players have a place where they add the
most value
4. “The Law of Mount Everest” – As the challenge escalates, the need for
teamwork elevates
5. “The Law of the Chain” – The strength of a team is impacted by its
weakest link
6. “The Law of the Catalyst” – Winning teams have players who make things
happen
7. “The Law of the Compass” – Vision gives team members direction and c
confidence
8. “The Law of the Bad Apple” – Rotten attitudes ruin a team.
9. “The Law of Accountability” – Team members must be able to count on
each other when it counts
10. “The Law of the Price Tag” – The team fails to reach its potential when it
fails to pay the price
11. “The Law of the Scoreboard” – The team can make adjustments when it
knows where it stands
12. “The Law of the Bench” – Great teams have great depth
13. “The Law of Identity” – Shared values define the team
14. “The Law of Communication” – Interaction fuels action
15. “The Law of the Edge” – The difference between two equally talented
teams is leadership
16. “The Law of High Morale” – When you are winning, nothing hurts
17. “The Law of Dividends” – Investing in the team compounds over time
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
129
Occupational Safety and Health
What are Occupational Safety and Health?
1. Occupational Safety refers to a work environment which is free from
danger, risk and injury.
2. Occupational Health refers to a worker who experiences a state of well-
being, free from illness or disease.
3. Occupational Security refers to the protection of an organization’s assets.
The Occupational Safety and Health Act (1970) – Employee Rights
• The right to safety and health on the job. • The right to accompany an inspection. • The right to be informed of workplace hazards. • The right to request inspections. • The right to file a complaint.
The Occupational Safety and Health Act (1970) – Employer Responsibilities
• Meet the general duty responsibilities to provide a safe and healthful workplace.
• Notify employees of their rights under OSHA. • Provide training mandated under OSHA. • Comply with all industry-specific standards. • Maintain accurate records (e.g., OSHA no. 200 log) of work-related
injuries, accidents and deaths. • Abate cited violations within the period prescribed by OSHA. • Provide employees with protective equipment needed for a job. • Maintain records of employee exposures to workplace hazards.
Key OSHA Standards
• General Duty Clause • Emergency Exit Procedures • Occupational Noise Exposure • Machine Guarding • Hazard Communication • Personal Protective Equipment • Confined Space Entry
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
130
• Bloodborne pathogens
Safety Committee Activities
• Investigate serious or dangerous accidents. • Conduct safety inspections. • Review and evaluate protective equipment need. • Review safety programs and recommend improvement. • Send information gained in training sessions to all employees. • Communicate safety information and results to management and
employees.
Characteristics of Effective Safety Programs
• Specific safety rules and procedures • Hazard recognition activities • Top management support • Safety Committees • Safety Training
Strategies for Management to Show Support for Safety and Health
• Appoint safety coordinators with high-level responsibility and authority • Regularly review safety activity results against predetermined objectives • Evaluate supervisors based on the safety performance of their employees • Include safety results in communications to corporate officers or board of
directors • Provide financial support for safety program
Contemporary Trends in Occupational Safety and Health
Substance Abuse
• Five times more medical claims • Three times more sick leave • Five times more compensation claims • Twice as many mistakes • Six times more absences
Symptoms
• Careless Work Habits • Absenteeism • Drop in Performance

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
131
• Emotional Outbursts • Impaired memory and logical thinking • Difficulty getting along with co-workers
Strategies for Handling Substance
Abuse in the Workplace
1. Develop a zero tolerance substance abuse policy. 2. Be assertive in dealing with substance abusers. 3. Refer the employee to a professional to deal with related personal
problems. 4. Clarify performance standards and inform the employee of the
consequences of poor performance. 5. Consider implementing a drug testing program to identify substance
abuse. 6. Train managers to identify substance abusers.
Workplace Violence
Examples
• Columbine High School • Taxi Cab Drivers • Convenience Stores • U.S. Post Office • Universities • Delivery Drivers
Conditions Associated with Workplace Violence
• Widespread Layoffs • Rigid, authoritarian management styles • Insensitive terminations • Pressure for increased productivity • Working late at night • Working with the public • Increased workloads
Profile of a Workplace Killer
• Socially Isolated • Experiencing personal stressors • Low self-esteem and no outlet for anger • Difficulty dealing with frustration and criticism
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
132
• Fascinated with weapons and the military • Temper-control problems • Drug and alcohol abuse • History of conflict • Paranoia • Making threats or intimidating others
Strategies for Reducing Workplace Violence
• Establish policy of zero tolerance. • Administer severe negative consequences for those who violate the
policy. • Encourage reporting of incidents. • Develop a plan for workplace security. • Provide training for handling workplace violence. • Ensure management commitment • Hold employee meetings to discuss workplace violence issues.
General Management Guidelines for Promoting Health and Safety
• Deal with unsafe work practices immediately. • Plan based on the assumption that what can happen will happen. • Post health and safety rules in a prominent place. • Beware of fatigue caused by excessive work demands. • Provide appropriate safety training. • Report and record all accidents. • Review safety results on a regular basis with your team. • Don’t let new employees start until they understand all health and safety
rules.
Measures of Effectiveness – Occupational Safety and Health
• Number of safety and health meetings • Number of internal safety meetings • Number of internal safety inspections conducted • Number of accidents • Accident severity rate • Number of lost time accidents • Number of near-misses • Number of violations found in safety • Total citations from OSHA • Average cost per accident • Cost of OSHA fines • Total lost time costs
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
133
• Average time to correct a citation
Emergency Preparedness
Emergencies can range from unintentional natural disasters, such as floods or
snowstorms, to intentional events, such as bioterrorism. To ensure local public
health is prepared to respond to potential emergency situations in the
community, hospitals have an emergency preparedness program. As part of the
commitment to the health and safety of the community, the goal of the
Emergency Preparedness Program is to provide efficient, effective public health
response in emergency situations.
The Emergency Preparedness Program works to:
• Assess local public health's readiness to respond to emergencies. • Develop and maintain plans for responding to possible future
emergencies. • Create and maintain the infrastructure for responding to emergencies. • Ensure proper disaster-response equipment and resources are readily
available. • Develop and maintain a strong network with first responders in the
community.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
134
Key Legal Acts
Safe Medical Device Act of 1990
The Safe Medical Devices Act of 1990 (SMDA) imposed significant new reporting
requirements on the medical device industry and users of medical devices like
the VA. SMDA requires that user facilities report to the Food and Drug
Administration (FDA) and/or the manufacturer any deaths and serious injuries
which a device may have caused or contributed to. SMDA also requires user
facilities to establish and maintain adverse event files.
Definitions:
Device user facility: a hospital, ambulatory surgical facility, nursing home,
outpatient treatment facility, or an outpatient diagnostic facility which is not a
physician's office.
Medical device: any item that is used for the diagnosis, treatment, or prevention
of a disease, injury, or other condition and is not a drug or biologic. This is not
just equipment.
Serious injury: an injury or illness that is:
life threatening, results in permanent impairment of a body function or permanent damage
to a body structure, or necessitates medical or surgical intervention to preclude permanent
damage or impairment.
A device may have "caused or contributed to" a patient's death or serious injury,
if the death or serious injury was or may have been attributed to the device or the
device may have been a factor in the death or serious injury because of:
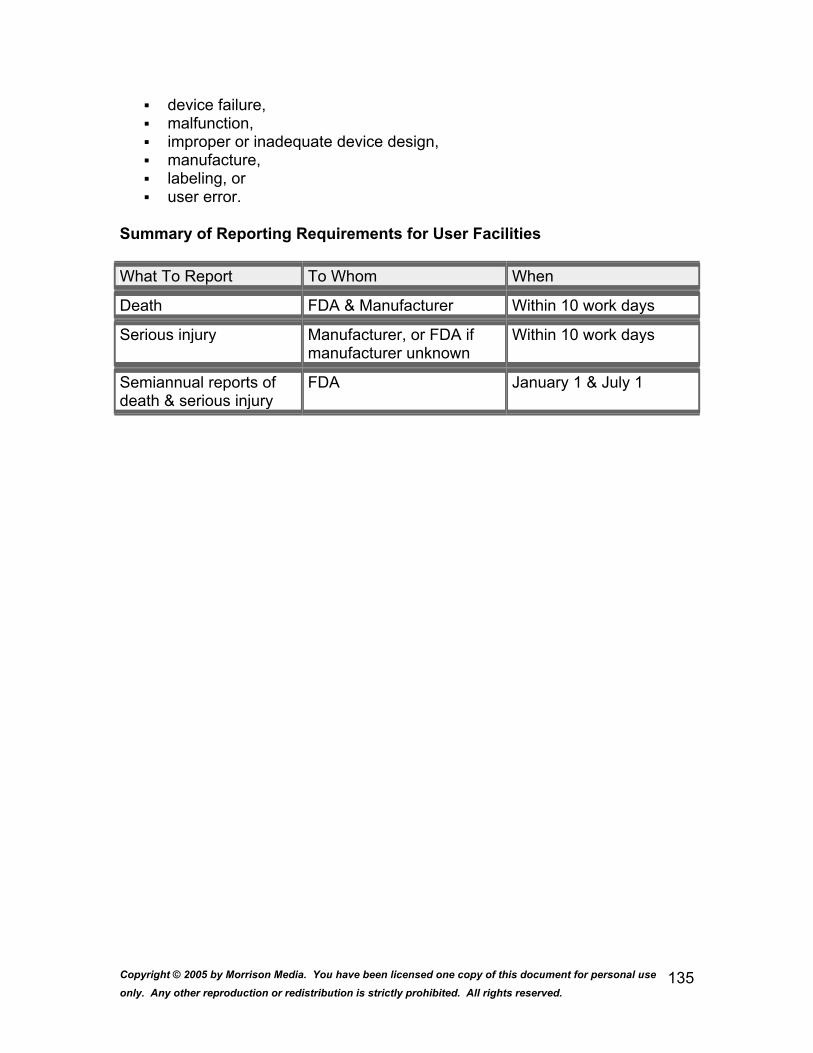
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
135
device failure, malfunction, improper or inadequate device design, manufacture, labeling, or user error.
Summary of Reporting Requirements for User Facilities What To Report To Whom When
Death FDA & Manufacturer Within 10 work days
Serious injury Manufacturer, or FDA if manufacturer unknown
Within 10 work days
Semiannual reports of death & serious injury
FDA January 1 & July 1
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
136
Clinical Laboratory Improvement Amendments Act of 1988
The Clinical Laboratory Improvement Amendments Act of 1988, or CLIA, sprang
to life following reports of problems with Pap smear testing that is performed
mostly in large independent laboratories. The goal of CLIA is to improve the
quality of testing in virtually all laboratories where tests on human specimens are
performed.
Americans with Disabilities Act
Title I of the Americans with Disabilities Act of 1990, which took effect July 26,
1992, prohibits private employers, state and local governments, employment
agencies and labor unions from discriminating against qualified individuals with
disabilities in job application procedures, hiring, firing, advancement,
compensation, job training, and other terms, conditions and privileges of
employment. An individual with a disability is a person who:
• Has a physical or mental impairment that substantially limits one or more major life activities;
• Has a record of such an impairment; or • Is regarded as having such an impairment.
A qualified employee or applicant with a disability is an individual who, with or
without reasonable accommodation, can perform the essential functions of the
job in question. Reasonable accommodation may include, but is not limited to:
• Making existing facilities used by employees readily accessible to and usable by persons with disabilities.
• Job restructuring, modifying work schedules, reassignment to a vacant position;
• Acquiring or modifying equipment or devices, adjusting modifying examinations, training materials, or policies, and providing qualified readers or interpreters.
An employer is required to make an accommodation to the known disability of a
qualified applicant or employee if it would not impose an "undue hardship" on the
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
137
operation of the employer's business. Undue hardship is defined as an action
requiring significant difficulty or expense when considered in light of factors such
as an employer's size, financial resources and the nature and structure of its
operation.
An employer is not required to lower quality or production standards to make an
accommodation, nor is an employer obligated to provide personal use items such
as glasses or hearing aids.
Medical Examinations and Inquiries
Employers may not ask job applicants about the existence, nature or severity of a
disability. Applicants may be asked about their ability to perform specific job
functions. A job offer may be conditioned on the results of a medical examination,
but only if the examination is required for all entering employees in similar jobs.
Medical examinations of employees must be job related and consistent with the
employer's business needs.
Drug and Alcohol Abuse
Employees and applicants currently engaging in the illegal use of drugs are not
covered by the ADA, when an employer acts on the basis of such use. Tests for
illegal drugs are not subject to the ADA's restrictions on medical examinations.
Employers may hold illegal drug users and alcoholics to the same performance
standards as other employees.
EEOC Enforcement of the ADA
The U.S. Equal Employment Opportunity Commission issued regulations to
enforce the provisions of Title I of the ADA on July 26, 1991. The provisions
originally took effect on July 26, 1992, and covered employers with 25 or more
employees. On July 26, 1994, the threshold dropped to include employers with
15 or more employees.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
138
Medicare changes from the Balanced Budget Refinement Act (BBRA)
of 1999
Before the BBRA, beneficiaries were required to pay 20% of the entire amount
charged for an outpatient hospital service, with no limit. The new provision caps
this amount at the inpatient hospital deductible amount, currently $776. This
provision is effective as if included in the Balanced Budget Act of 1997(1997).
Moratorium on Therapy Caps Before the BBRA, there was a $1,500 annual limit on physical, occupational and
speech therapies. The new provision suspends these annual payments limits for
2 years, 2000 and 2001. This provision was effective for services furnished on or
after January 2, 2000.
Extension of Immunosuppressive Drug Benefit
Before the BBRA, immunosuppressive drug therapy for post-transplant
beneficiaries was limited to 36 months following organ transplant. The new
provision extends this coverage from 36 to 44 months, for the year 2000. This
coverage will not apply to those beneficiaries eligible for Medicare solely for end-
stage renal disease (ERSD), since those beneficiaries’ entire Medicare coverage
ends 36 months after kidney transplant. This provision was effective January 1,
2000.
Changes in Medicare+Choice (Medicare HMO) Enrollment Rules
Before the BBRA, a Medicare HMO could terminate its services in a particular
area, and enrollees’ "guaranteed issue" rights to Medigap policies did not apply
until their coverage terminated (generally January 1). The new provision gives
these enrollees the option of exercising their "guaranteed issue" rights either
within 63 days of when the coverage terminates or within 63 days of receiving
notice of their plan’s termination of services. This provision was effective with
enactment of the BBRA: 11/29/99.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
139
Before the BBRA, an enrollee could not continue to be enrolled in a Medicare
HMO if the HMO terminated services in the area in which the enrollee lived. The
new provision states that HMOs may choose to continue enrollment for those
enrollees who live in the plan’s terminated service area, as long as those
enrollees agree to receive services in the HMO’s continued service area. This
provision applies to service area reductions before, on, or after 11/29/99.
Changes in Effective Date of Enrollment/Disenrollment in Medicare+Choice
Plans
Before the BBRA, whenever a beneficiary enrolled or disenrolled with a
Medicare+Choice plan, the enrollment change would become effective the first
day of the next calendar month. The new provision states that any changes
made before or on the 10th of any month will be effective the first day of the first
calendar month after the change is requested. Any changes made after the 10th
of any month will be effective the first day of the second month after the change
is requested. This provision applies to any changes in elections of coverage
made on or after January 1, 2000.
Extending Medicare Coverage for Disabled Medicare Beneficiaries
Before the BBRA, when a Medicare beneficiary eligible due to disability returned
to work for 4 years at $700/month or more, they lost their premium-free Medicare
Part A. The new provision extends this time limit to 8 ½ years. This provision will
be effective October 1, 2000.
Option for Disabled Medicare Beneficiaries to Suspend Medigap Insurance
Before the BBRA, there was no current law regarding suspension of Medigap
insurance coverage when a disabled beneficiary was employed and covered
under that employer’s group health plan. The new provision allows those
Medicare beneficiaries eligible due to disability to suspend Medigap benefits and
premiums if they become employed and are covered under the employer’s group
health plan. This provision was effective on the date of enactment of the BBRA
(11/29/99).

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
140
Distribution of Increased Payments to Medicare + Choice Organizations under the Medicare, Medicaid, and SCHIP Benefits Improvement and
Protection Act of 2000
Background: Of the 39 million people with Medicare, about 5.6 million are
enrolled in a Medicare+Choice organization. The Medicare+Choice program was
established under the Balanced Budget Act (BBA) of 1997 to permit contracts
between HCFA and a variety of different managed care and fee-for-service
entities. In addition, the program sets federal reimbursement rates for
Medicare+Choice organizations (including HMOs and other private health plans).
The BBA set the payment rate per enrollee per month. Payment is based on the
rate in the county in which an enrolled beneficiary lives, adjusted for factors
associated with health care costs, such as age. The county payment rate
established by the BBA is the highest of three amounts:
• A minimum two percent increase over the prior year's rate;
• A minimum dollar amount called a "floor". This was $402 in 2000;
• An amount derived from blending the local rate with a national rate
based on historic spending under the "fee-for-service" Medicare
program.
Floor payments and the blended rate were intended to reduce the variation in
Medicare+Choice payment rates by raising payments in low-payment counties.
With The Medicare, Medicaid, and SCHIP Benefits Improvement and Protection
Act (BIPA), enacted in December, 2000, Congress increased both the minimum
percentage increase for 2001 (from 2 percent to 3 percent) and the floor amount.
In addition to the basic floor of $475, the legislation established another, new
floor of $525 for counties in urban areas with populations over 250,000. The
legislation also extended bonus payments set by the Balanced Budget
Refinement Act of 1999. The bonus is for Medicare+Choice organizations that
enter a county where no other plan has been offered since 1997, or where
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
141
coverage was terminated as of January 1, 2001. That bonus increases payments
by an additional 5 percent the first year a plan is offered, and by an additional 3
percent for the second year. The BIPA legislation invited Medicare+Choice
organizations, which had given notice of their intent to terminate coverage for
Medicare beneficiaries, to rescind that decision by January 18, 2000. Finally, the
BIPA legislation contains a provision that phases in risk adjustment payments
over the next seven years. Risk adjustment pays plans more for treating sicker,
and therefore more costly, beneficiaries.
These changes to payment rates are expected to increase aggregate payments
to Medicare+Choice organizations by about $11 billion over the next five years
(about $1 billion for 2001). The new rates are effective March 1, 2001.
Medicare+Choice organizations were required to submit new benefit information:
To qualify for the higher payments under BIPA, the legislation required
Medicare+Choice organizations to submit revised Adjusted Community Rate
Proposals (ACRPs) by January 18, 2001. These proposals detail
Medicare+Choice organizations’ premiums, benefit packages, and the costs and
payments associated with providing benefits. (The consumer oriented portions of
each Medicare+Choice organization's premiums and benefit packages can be
found on www. medicare.gov, under "Medicare Health Care Compare.")
Under BIPA, the new payments must be used by Medicare+Choice organizations
in only four ways:
• Reduce beneficiary premiums or cost sharing (e.g. co-pays);
• Enhance benefits;
• Enhance the network of health care providers available to
beneficiaries;
• Reserve funds to help offset premium increases or benefit reductions
in the future through contributions to a benefit stabilization fund.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
142
Because the BIPA was enacted late in the year -- it was signed December 21,
2000 -- the Health Care Financing Administration worked rapidly to implement its
new provisions. New payment rates were published on January 4, 2001. Since
Medicare+Choice organizations were required by BIPA to submit new ACRPs
within two weeks of that date, HCFA consulted extensively with representatives
of Medicare+Choice organizations to enable those organizations to understand
the new legislation and submit their new benefit plans.
650 proposals from 177 Medicare+Choice organizations
HCFA received about 650 revised ACRPs from 177 Medicare+Choice
organizations. HCFA staff worked to review and approve all of them, and the
many marketing and advertising materials that describe them, in time for any
Medicare+Choice plans that wished to market to beneficiaries to enroll them by
March 1, 2001, when the new payment rates begin.
The largest payment rate increases (based on BIPA) went to floor counties; plans
in these counties were less likely to use new funds exclusively for enhanced
provider networks.
The distribution of the new funds varies by whether or not the counties served by
the Medicare+Choice organization are floor counties, and which type of floor
applies (Chart 2).
• The highest increases in rates are in counties that receive the new $525
floor for urban areas of 250,000 or more. Medicare+Choice organizations
serving these counties will see, on average, increases of 9.7 percent
above pre-BIPA rates for 2001. Nearly one-quarter of all Medicare+Choice
enrollees live in these counties.
• The $475 floor raises rates in these counties by 8.3 percent above pre-
BIPA rates for 2001. A small proportion (less than 2 percent) of enrollees
live in these counties.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
143
• All other counties receive just 1 percent increases above pre-BIPA rates
for 2001—rates rise 3 percent above the 2000 rate. However, these
counties have had the highest payment rates historically. About 75
percent of Medicare+Choice organization enrollees live in these counties.
Medicare+Choice organizations' use of the new funds varies by the amount of
the payment increases under BIPA (Chart 3).
• In counties with the $525 and $475 floor, Medicare+Choice organizations
using all funds to enhance provider networks represent the largest share
of enrollees, 44 and 49 percent, respectively. About 8-9 percent of
enrollees in these counties will be in plans where the BIPA funds were
used only to reduce cost sharing or premiums.
• In non-floor counties, about 72 percent of enrollees are in
Medicare+Choice organizations that put all of the BIPA funds into
enhancing provider networks. (Non-floor counties had the smallest
percentage increase in their pre-BIPA 2001 rates, but have the highest
historical payments).
Premiums dropped about $2/month nationally as a result of the BIPA changes.
Looking at national average, premiums for basic plans will go down an average
of $2 per month relative to pre-BIPA 2001 premiums as a result of the choices
made by Medicare+Choice organizations in using the BIPA funds (Chart 4).
(Premiums have tended to be highest in counties where Medicare payment rates
have been historically lowest, i.e., the floor counties.)
• Relative to pre-BIPA 2001 premiums, post-BIPA premiums are reduced
more in the $525 floor counties. There, premiums will fall an average of
about $6.
• In the $475 floor counties, relative to pre-BIPA premiums, post-BIPA
premiums will drop an average of about $4, from about $52 to $48.
• Post-BIPA premiums will be about $1 less than pre-BIPA 2001 premiums
in non-floor counties.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
144
Without BIPA, almost 21 percent of Medicare+Choice enrollees would have had
premiums for basic plans greater than $50 in 2001, compared with just 7 percent
of Medicare+Choice enrollees the prior year (Chart 5). In counties with $525 floor
payments, premiums of more than $50 per month will be less common than
before BIPA--dropping from 40 percent of all enrollees to 24 percent. With BIPA,
almost 16 percent of enrollees will see premiums beginning in March of 2001
above $50 (a 5 percentage point decrease). There was almost no change in the
share of enrollees in Medicare+Choice organizations with $0 premium basic
plans in 2001 as a result of BIPA (about 45 percent).
Adding drug coverage was rare.
The proportion of enrollees with drug coverage in Medicare+Choice
organizations’ basic packages has declined over the past several years--from 84
percent in 1999 to 72 percent in 2000 (Chart 6). Drug coverage is most common
in counties with the highest payment rates.
Few Medicare+Choice organizations used the BIPA funds to add a drug benefit
(Chart 6). Without BIPA, about 69 percent of beneficiaries would have had drug
coverage in their basic plan in 2001. With BIPA, the percent of enrollees in
Medicare+Choice plans with drug coverage in the basic packages beginning in
March of 2001 rises one percentage point to 70 percent. That is, about 61,000
Medicare+Choice enrollees will have access to new drug coverage in basic
packages beginning in March of 2001 (Chart 7).
• About three-fourths of enrollees with a new drug benefit who lacked drug
coverage in 2001 pre-BIPA and will have drug coverage post-BIPA (i.e.,
effective March 1, 2001) live in counties with the $525 floor.
• The largest increase in the percentage of enrollees who lacked drug
coverage in 2001 pre-BIPA and will have drug coverage post-BIPA (i.e.,
effective March 1, 2001) is in counties with the $475 floor, from 31 percent
to 38 percent.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
145
COBRA
COBRA is an acronym for the Consolidated Budget Reconciliation Act. Budget
reconciliation Acts used to be an accounting exercise by Congress -- with pages
and pages of columns and columns of numbers. One day in 1985, lawmakers
discovered that they could use a Budget Reconciliation Act to make law. Here's
what they came up with:
The COBRA law, first enacted in 1985, has been amended by subsequent tax
bills and other legislation, most importantly the Health Insurance Portability and
Accountability Act (HIPAA).
Most employers with group health plans are required to offer employees the
opportunity to temporarily continue their group health care coverage under their
employer's plan if their coverage otherwise would cease due to a termination,
layoff, or other change in employment status.
These "COBRA" health care continuation requirements -- were enacted as part
of the Consolidated Omnibus Budget Reconciliation Act of 1985 -- generally
entitle employees (as well as covered spouses and dependents) to extend (at
their own expense) their employer-provided health care coverage for a period of:
Up to 18 months for covered employees, as well as their spouses and
dependents, when employees otherwise would lose coverage because of a
termination or reduction of hours;
Up to 36 months for spouses and dependents facing a loss of employer-
provided coverage due to an employee's death, a divorce or legal separation,
or certain other "qualifying events.'
The range of employers affected by COBRA is very broad, with exemptions
available only for employers that normally employ fewer than 20 employees, and
church plans, and plans maintained by the U.S. government.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
146
Although employers are permitted to charge COBRA beneficiaries a premium for
continuation coverage of up to 102 percent of the cost of the coverage to the plan
(150 percent in the case of certain disabled employees), the 2 percent "mark up'
usually does not cover the full cost of administering COBRA.
Employers that violate the COBRA requirements are subject to a penalty of $100
per affected employee for each day that the violation continues. And plan
administrators who fail to provide required COBRA notices to employees may be
personally liable for a civil penalty of up to $100 a day for each day the notice is
not provided.
COBRA is one of the more administratively complex pieces of legislation in the
employee benefits area. This complexity is underscored by the fact that COBRA
has been subject to numerous legislative changes in recent years, which have
outdated parts of the proposed regulations originally issued by IRS in 1987.
These modifications to COBRA's requirements are noted in this summary.
Basic Terms and Concepts
COBRA requires an employer to offer employees and their dependents the
opportunity to continue their group health coverage under the employer's plan
when certain events occur that otherwise would cause them to lose their job-
related health plan coverage. Important terms used for COBRA administration
purposes include:
* "Qualifying event", which refers to the specific events (an employee's
termination, layoff, or death) that would cause a loss of employer-provided
coverage and thus trigger the coverage-continuation option.
* "Qualified beneficiary", is the term used to refer to an employee or a employee's
spouse or dependent who is or was covered under the employer-provided health
plan and has experienced a qualifying event.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
147
COBRA imposes a host of rules governing the obligations and duties of both
employers and qualified beneficiaries involved in coverage-continuation
situations.
Specific rules under COBRA deal with issues like: the length of the required
coverage period; notification requirements for employers and plan administrators;
procedures for electing continuation coverage; premiums the employer may
require beneficiaries to pay; and the circumstances under which an employer
may terminate COBRA coverage short of the full continuation period.
How COBRA Rights Are Triggered
An employer's obligation to offer COBRA coverage is triggered by the occurrence
of a qualifying event. Specifically, COBRA recognizes a qualifying event as a loss
of employer-provided health coverage due to one of the following reasons:
* The death of a covered employee.
* Divorce or legal separation of the employee.
* The employee's entitlement to Medicare.
* Dependent child's loss of eligibility under the plan.
* Bankruptcy of the employer.
* The employee's change in employment status, including termination or
reduction in working hours.
An employee called to military duty also has COBRA continuation rights. The
Internal Revenue Service has ruled that the termination of health coverage
arising from an employee's being called to active military duty triggers an
employer's obligation to offer health care continuation coverage, unless the
employer continues normal coverage while the employee is on military leave.
Coverage Periods: Basic Rules
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
148
The normal COBRA coverage continuation period is either 18 or 36 months.
Special coverage periods are available to qualified beneficiaries who are
disabled at the time of a qualifying event or are retirees (or are a retiree's widow
or widower) and would lose their health plan coverage due to the bankruptcy of
the sponsoring employer.
An 18-month period of continuation coverage is available to covered employees
and their spouses and dependents in cases where coverage is lost due to the
employee's termination or reduction of hours. A special 29-month period of
coverage (the basic 18-month period of continuation coverage, plus an additional
11 months) is available for beneficiaries who are disabled at the time of the
qualifying event.
A 36-month period of continuation coverage is available for spouses and
dependents where coverage is lost due to circumstances such as the employee's
entitlement to Medicare, divorce or legal separation, or death. The 36-month
continuation period also applies to cases where dependent children reach the
maximum age for coverage under an employer's plan.
Special "multiple qualifying event" rules permit qualified beneficiaries who receive
COBRA continuation coverage upon a covered employee's termination or
reduction in hours to extend the length of their coverage if a second qualifying
event -- divorce or death of the covered employee -- occurs during the initial 18
month period. In general, the extension cannot exceed 36 months from the date
of the first qualifying event. When an employer files for bankruptcy and the
company's retirees -- or their widows or widowers -- lose health coverage under
the employer's health care plan within a year before or after the event, the
employer must make available the coverage-continuation option to these people
and any covered spouses or dependents until the retiree or widow/widower dies.
Upon the death of the covered retiree or widow/widower, spouses and
dependents may continue coverage for an additional 36 months.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
149
Qualified Beneficiaries
A "qualified beneficiary" is as any person who, on the day before a qualifying
event, is covered under an employer's group health plan by virtue of being either
a covered employee, the spouse of a covered employee, or the dependent child
of a covered employee.
COBRA defines "covered employee" as a person who is or was covered under a
group health plan as a result of having performed services for one or more
persons maintaining the plan. Although COBRA continuation coverage rights
generally arise out of an employment relationship, COBRA's definition of
"covered employee" is designed to be sufficiently broad so that independent
contractors, partners, and other non-employees may have continuation coverage
rights if they are covered by a plan as a result of services performed for the plan
sponsor.
Dependents acquired by a COBRA beneficiary during a period of continuation
coverage (a spouse who marries a qualified beneficiary after they have already
started to receive continuation coverage), must be permitted to elect coverage for
the remaining period of the qualified beneficiary's coverage period, if this is
allowed for the "acquired" dependents of active employees. Dependents
acquired after a qualifying event do not gain status as a "qualified beneficiary.'
Military Duty
Employers are not obligated to continue benefits to employees who serve in the
National Guard or a military reserve unit when they are called to active duty.
Employers that terminate the health care coverage of Guard members or
reservists who are called to active duty must offer these employees and their
dependents the opportunity to elect COBRA continuation coverage and notify
them of their COBRA rights. Military benefit plans do not constitute group health
insurance plans within the meaning of COBRA. Therefore, employers may not

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
150
terminate COBRA coverage even though reservists or their dependents become
covered under military plans.
"Gross Misconduct" Exception
COBRA permits employers to deny continuation coverage to employees who are
terminated for gross misconduct. The problem for employers is: neither the law
nor the IRS regulations specifically define what constitutes "gross misconduct". In
view of COBRA's costly penalties and the absence of any legal definition or
guidelines on what constitutes "gross misconduct," employers should apply the
"gross-misconduct" exception only in very clear-cut cases of egregious or
outrageous misconduct.
The "gross misconduct" exception was intended for use in only extreme cases of
employee misconduct. Consult your attorney to see if they can defend a COBRA
denial on the basis of what YOU think is "gross misconduct". Assault and theft
are "gross misconduct" talking back to a supervisor is not.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
151
Medicare Conditions of Participation For Hospitals
On December 19, 1997, the Health Care Financing Administration ("HCFA")
issued a proposed rule revising the "Conditions of Participation" ("COP") for
hospitals that participate in the Medicare and Medicaid programs. (62 Fed. Reg.
66726) As part of President Clinton’s Reinventing Government Initiative, the
proposed regulations attempt to focus on the outcome of patient care and
eliminate unnecessary procedural requirements for hospitals. HCFA is currently
seeking public comment on these proposed COP. Health care providers
participating in the Medicare/Medicaid programs should take this opportunity to
review the proposed standards accordingly.
HCFA noted that the current standards adopted in 1986, which stress structures
and process, no longer represent the best available method for assessing and
improving the quality of care in hospitals. According to HCFA, the "patient-
centered" proposed COP are intended to mirror its approach for all COP and
stimulate improvement in processes, outcomes and overall patient satisfaction.
Additionally, they are intended to foster an interdisciplinary approach to the
delivery of patient care.
While the proposed rule contains nineteen (19) separate COP, which revise or
eliminate many of the existing requirements, the proposed rule essentially adopts
the basic structure of the Joint Commission on Accreditation of Health Care
Organizations’ "Agenda for Change" and incorporates critical requirements into
the four core conditions discussed below.
I. Patient Rights
As part of a hospital’s obligation to protect and promote the rights of patients, the
proposed COP would require a hospital to inform patients of their rights before
furnishing care and to establish a grievance process which specifies the person a
patient should contact to express a grievance. Included within the delineated list
of patients rights are: (i) a patient’s right to participate in the development and

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
152
implementation of his/her plan of care; (ii) the right to formulate an advanced
directive and have hospital staff comply with the directive; (iii) the right to
personal privacy and safety, including the right to be free of verbal and physical
abuse; (iv) the right to confidentiality of patient clinical records and the right to
access such records within a reasonable time frame; and (v) the right to be free
from the use of seclusion or restraints as a means of coercion, convenience or
retaliation by staff.
In an attempt to allow a hospital flexibility in determining how it ensures that
restraints and seclusion are not inappropriately used, HCFA has not currently
included detailed requirements in the proposed rule regarding seclusion and
restraints. However, HCFA has indicated that it will consider whether further
requirements are necessary to ensure patient health and safety. Examples of
detailed requirements that HCFA is considering are whether written orders for
restraints and seclusion should be valid for a specific period of time and whether
patients in seclusion should be checked every fifteen (15) minutes.
II. Patient Admission, Assessment and Plan of Care
This proposed COP would require a hospital to conduct a comprehensive
assessment of the needs of each patient and establish a coordinated plan of care
to address how all relevant hospital disciplines would meet such needs. A
comprehensive assessment must identify not only the patient’s condition and
necessary care at the time of admission, but would also need to contain an initial
estimate of post-hospital needs. The plan of care addressing the needs identified
in the comprehensive assessment must specify the care to be delivered by all
relevant disciplines. It would further need to be modified to address the changing
requirements of the patient. The proposed standard calls for both the
comprehensive assessment and plan of care to be included in the medical record
within 24 hours of a patient’s admission. HCFA maintains that the proposed rule
creates more flexibility for hospitals than the current standards in determining

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
153
what disciplines should be involved in planning a patient’s care because such
plan shall be based on a patient’s clinical picture.
III. Patient Care
In an attempt to integrate the way a patient experiences care in a hospital, the
proposed rule establishes a single unified patient care condition which requires
that care and treatment for the patient be coordinated by all relevant disciplines
and conform to the plan of care. The proposed standard requires that not only
the plan of care be modified as needed, but also that the actual care provided be
modified as appropriate, establishing, according to HCFA, "the linkage between
evolution of treatment results and care plan modification." If the hospital provides
care to outpatients, the proposed standard requires that such care must meet the
same requirements that apply to inpatient care.
IV. Quality Assessment/Performance Improvement
Under the proposed rule, hospitals would be required to develop, implement,
maintain, and evaluate an effective data-driven quality assessment ("QA") and
performance improvement ("PI") program, which must reflect the complexity of
the hospital’s organization and services. The proposed rule has identified twelve
elements for inclusion in the assessment.
As part of the overhaul of the QA process, hospitals would be required to use
hospital specific data as well as Peer Review Organization ("PRO") data and
other available data as an integral part of the QA/PI strategy. As part of the QA
process, the proposed COP would require a hospital to set priorities for PI based
on prevalence and severity of identified problems. Actions taken by a hospital
would need to be measurable and tracking would need to demonstrate sustained
improvement.
According to HCFA, the new QA/PI COP focuses on a hospital’s performance in
improving patient outcomes and satisfaction instead of the current "problem
focus" approach to identifying and correcting problems in patient care. Although

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
154
the proposed COP do not currently set a specific number of QA studies that a
hospital must undertake, HCFA has indicated that it is considering developing
such a requirement which could possibly be tied to the number of patient
discharges or hospital beds.
Streamlining
As noted above, the proposed regulations attempt to focus on patient care
outcomes and to eliminate unnecessary procedural requirements for hospitals.
Most notably, the proposed COP eliminate specific requirements related to the
structure and organization of both the governing body and medical staff.
Additionally specific staffing requirements have been greatly reduced as well as
other narrowly focused standards, such as the requirement that post anesthesia
evaluations be done by the same individual who administered the anesthesia. Of
interest to medical staffs, will be the elimination of the ambiguous requirement
that prohibited a hospital from requiring specialty board certification as a
necessary condition for medical staff membership.
Considerations
Some hospitals may not consider the adoption of the proposed COP a significant
problem as they are, in part, consistent with recently revised JCAHO standards
and certain states’ regulations. However, with the adoption of new COP comes
unfamiliar surveyors who are likewise attempting to understand the new
requirements. Moreover hospitals still must comply with state regulations and
may have some difficulty integrating the requirements of the new COP with
existing policies and procedures drafted in accordance with the former COP and
state law.
Furthermore, despite HCFA’s attempts to use process oriented requirements
only where it believes such requirements remain highly predictive of specific
desired outcomes or where necessary to deter fraud and abuse, the proposed
rule still contains process oriented requirements which should be closely
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
155
scrutinized by hospitals. For example, the comments to the proposed rule
emphasize that the comprehensive assessment need be only done in a timely
manner. However, it also requires that the assessment be placed in the medical
record within twenty four (24) hours of admission. This time frame could pose a
problem to physicians who rely on dictation services, as frequently, such services
do not have a rapid turnaround.
Outlined below are the primary issues of the COPs that effect hospitals:
1. The hospital must incorporate an agreement with an organ/tissue and eye
bank.
2. The hospital must notify, in a timely manner, the Organ Procurement
Organization (OPO) of individuals whose death is imminent or who have
died in the hospital. The OPO determines medical suitability for organ
donation. The tissue bank and eye bank determine suitability for tissue
and eye donation.
3. The hospital must ensure, in collaboration with the designated OPO,
tissue bank or eye bank, that the family of each potential donor is informed
of their options for donation of organs, tissues or eyes.
4. The hospital must encourage discretion and sensitivity with respect to the
circumstances, views, and beliefs of the families of potential donors.
The hospital must have and implement written protocols that ensure that the
hospital works cooperatively with the designated OPO, tissue bank and eye bank
in educating staff on donation issues, reviewing death records to improve
identification of potential donors, and maintaining potential donors while
necessary testing and placement of potential donated organs, tissues and eyes
take place.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
156
The Malcolm Baldrige National Quality Improvement Act of 1987 - Public Law 100-107
The Malcolm Baldrige National Quality Award was created by Public Law 100-
107, signed into law on August 20, 1987. The Award Program, responsive to the
purposes of Public Law 100-107, led to the creation of a new public-private
partnership. Principal support for the program comes from the Foundation for the
Malcolm Baldrige National Quality Award, established in 1988.
The Award is named for Malcolm Baldrige, who served as Secretary of
Commerce from 1981 until his tragic death in a rodeo accident in 1987. His
managerial excellence contributed to long-term improvement in efficiency and
effectiveness of government. The Findings and Purposes Section of Public Law
100-107 states that:"
1. the leadership of the United States in product and process quality has been
challenged strongly (and sometimes successfully) by foreign competition, and
our Nation's productivity growth has improved less than our competitors' over
the last two decades.
2. American business and industry are beginning to understand that poor quality
costs companies as much as 20 percent of sales revenues nationally and that
improved quality of goods and services goes hand in hand with improved
productivity, lower costs, and increased profitability.
3. strategic planning for quality and quality improvement programs, through a
commitment to excellence in manufacturing and services, are becoming more
and more essential to the well-being of our Nation's economy and our ability to
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
157
compete effectively in the global marketplace.
4. improved management understanding of the factory floor, worker involvement
in quality, and greater emphasis on statistical process control can lead to
dramatic improvements in the cost and quality of manufactured products.
5. the concept of quality improvement is directly applicable to small companies as
well as large, to service industries as well as manufacturing, and to the public
sector as well as private enterprise.
6. in order to be successful, quality improvement programs must be
management-led and customer-oriented, and this may require fundamental
changes in the way companies and agencies do business.
7. several major industrial nations have successfully coupled rigorous private-
sector quality audits with national awards giving special recognition to those
enterprises the audits identify as the very best; and
8. a national quality award program of this kind in the United States would help
improve quality and productivity by:
a. helping to stimulate American companies to improve quality and
productivity for the pride of recognition while obtaining a competitive edge
through increased profits;
b. recognizing the achievements of those companies that improve the quality
of their goods and services and providing an example to others;
c. establishing guidelines and criteria that can be used by business,
industrial, governmental, and other organizations in evaluating their own
quality improvement efforts; and
d. providing specific guidance for other American organizations that wish to
learn how to manage for high quality by making available detailed

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
158
information on how winning organizations were able to change their
cultures and achieve eminence."
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
159
Organizational Exit
What are the Goals of Downsizing and Layoffs?
1. Reducing costs
2. Increasing profitability
3. Increasing shareholder return
4. Increasing quality and productivity
Strategies for Downsizing
How Effective Have Downsizing and Layoffs Been?
1. Cost Reduction: <50% Success
2. Increased Profitability: <33% Success
3. Increased Shareholder Return: <25% Success
4. Increased Quality and Productivity: <50% Success
Biggest Mistakes Made in Downsizing/Layoffs
1. Lack of a strategic vision.
2. Lack of consideration for alternatives.
3. HR held completely responsible for the downsizing.
4. Lack of consideration for feelings of people affected.
5. Lack of training.
Approaches to Making Layoff Decisions - Seniority
Advantages
• Legally defensible • Easy to implement • Objective-Perceived as being fair
Disadvantages
• Loss of good employees • Loss of minorities and women

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
160
Approaches to Making Layoff Decisions - Merit
Advantages
• Rewards performance. • Enables you to keep your best employees.
Disadvantages
• May be less legally defensible. • Alternatives to Layoffs • Hiring Freezes
Alternatives: Employee Transfers Job Sharing Pay Freezes Pay Cuts Retraining
Guidelines for Employee Layoffs
• Give as much advance warning as possible – have a clear vision of the “post-layoff” organization.
• Complete a termination in 15 minutes or less. • Give the employee a written statement of his/her severance benefits. • Express appreciation for what the employee has contributed to the
organization. • Don’t beat around the bush. • Don’t allow time for debate. • Do not make any personal comments – keep it at a professional level. • Don’t rush the employee off-site unless security is a concern. • Provide outplacement services (e.g., EAPs. career services). • Consider timing issues – don’t layoff an employee on a significant date. • Make sure that the employee receives the news directly from his/her boss. • Take care of morale and trust issues among survivors.
Guidelines for Managing the Aftermath of an Employee Layoff
1. Hold a meeting with survivors.
2. Provide access to EAP services for survivors.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
161
3. Provide a vision for the future.
4. Avoid signs of extravagant spending following a layoff.
5. Maintain open channels of communication with employees.
6. Set realistic expectations among survivors regarding the possibility of
future layoffs.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
162
Statistics
Probability: A number expressing the likelihood that a specific event will occur
expressed as the ratio of the number of actual occurrences to the number of
possible occurrences.
Statistics: The mathematics of the collection, organization, and interpretation of
numerical data, especially the analysis of population characteristics by inference
from sampling
Histogram: A bar graph of a frequency distribution in which the widths of the
bars are proportional to the classes into which the variable has been divided and
the heights of the bars are proportional to the class frequencies
Know how to solve probability problems by using the following:
Counting Techniques
Independent Trials
Binomial Distribution: The frequency distribution of the probability of a specified
number of successes in an arbitrary number of repeated independent Bernoulli
trials
Joint Probability: The probability that two or more specific outcomes will occur
in an event
Measures of Central Tendency
Average (mean): The sum of a set of values divided by the number of values
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
163
Weighted Average: An average that takes into account the proportional
relevance of each component, rather than treating each component equally
Range: The difference or interval between the smallest and largest values in a
frequency distribution
Median: Relating to or constituting the middle value in a distribution
Mode: The value or item occurring most frequently in a series of observations or
statistical data
Standard deviation: A statistic used as a measure of the dispersion or variation
in a distribution, equal to the square root of the arithmetic mean of the squares of
the deviations from the arithmetic mean
Variance: The square of the standard deviation
Balance Scale: One definition of central tendency is the point at which the distribution is in
balance.
Smallest Absolute Deviation: Another way to define the center of a distribution is based on the concept of the
sum of the absolute differences.
Smallest Squared Deviation: We shall discuss one more way to define the center of a distribution. It is based
on the concept of the sum of squared differences.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
164
Central Tendency: The center or middle of a distribution. There are many
measures of central tendency. The most common are the mean, median, and
mode. Others include the trimea, trimmed mean, and geometric mean.
Class Frequency: One of the components of a histogram, the class frequency is the number of
observations in each class interval.
Class Interval: Bin Width: Also known as bin width, the class interval is a division of data for use
in a histogram.
Discrete: Variables that can only take on a finite number of values are called "discrete
variables." All qualitative variables are discrete. Some quantitative variables are
discrete, such as performance rated as 1, 2, 3, 4, or 5, or temperature rounded to
the nearest degree.
Distribution: Frequency Distribution: The distribution of empirical data is called a frequency
distribution and consists of a count of the number of occurrences of each value. If
the data are continuous, then a grouped frequency distribution is used. Typically,
a distribution is portrayed using a frequency polygon or a histogram.
Frequency Polygon: A frequency polygon is a graphical representation of a distribution. It partitions
the variable on the x-axis into various contiguous class intervals of (usually)
equal widths. The heights of the polygon's points represent the class frequencies.
Grouped Frequency Distribution:

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
165
A grouped frequency distribution is a frequency distribution in which frequencies
are displayed for ranges of data rather than for individual values. For example,
the distribution of heights might be calculated by defining one-inch ranges.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
166
Special Report: Which Study Guides and Practice Tests Are Worth Your Time
We believe the following practice tests and guide present uncommon value to our
customers who wish to “really study” for the CPHQ tests. While our manual
teaches some valuable tricks and tips that no one else covers, learning the basic
coursework tested on the exam is also necessary.
Practice Tests
Practice Test Questions
http://www.jbqualitysolutions.com/About/handbook.php
Study Guides
1. “A Dash through the Data! Using Data for Improvement”, a two-hour videotape on the basics of using data for QI by Sandra K. Murray, available through the National Association for Healthcare Quality (NAHQ), 4700 W. Lake Avenue, Glenview, IL 60025-1485, 800-966-9392, international 847-375-4720, FAX 847-375-6320, www.nahq.org.
2. Handbook for Improvement, a Reference Guide for Tools & Concepts, Second Edition, published by Executive Learning, Inc., 7101 Executive Center Drive, Ste. 160, Brentwood, TN 37027, international 615-373-8483, 800-929-7890, FAX 615-373-8635, www.elinc.com.
3. The Healthcare Quality Handbook: A Professional Resource and Study Guide, published by Janet A. Brown, RN, CPHQ, JB Quality Solutions, Inc., 2309 Paloma Street, Pasadena, CA 91104, international 626-797-3074, FAX 626-797-3864, e-mail: [email protected], www.jbqualitysolutions.com. Workshop audio tapes or CDs also available.
4. Hospital Peer Review published by American Health Consultants, Inc., 3525 Piedmont Road, Building Six, Suite 400, Atlanta, GA 30305, international 404-262-7436, 800-688-2421, FAX 404-262-7837, www.ahcpub.com.
5. Journal for Healthcare Quality published by the National Association for Healthcare Quality (NAHQ), 4700 W. Lake Avenue, Glenview, IL 60025-1485, 800-966-9392, international 847-375-4720, FAX 847-375-6320, www.nahq.org.
6. Managing Performance Measurement Data in Health Care, published by Joint Commission Resources, One Renaissance Blvd., Oakbrook Terrace, IL 60181, 630-792-5800, Library of Congress Catalog Card No. 00-110892, International Standard Book No. 0-86688-693-1, www.jcrinc.com.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
167
Special Report: Retaking the Test: What Are Your Chances at Improving Your Score?
After going through the experience of taking a major test, many test takers
feel that once is enough. The test usually comes during a period of transition
in the test taker’s life, and taking the test is only one of a series of important
events. With so many distractions and conflicting recommendations, it may
be difficult for a test taker to rationally determine whether or not he should
retake the test after viewing his scores.
The importance of the test usually only adds to the burden of the retake
decision. However, don’t be swayed by emotion. There a few simple
questions that you can ask yourself to guide you as you try to determine
whether a retake would improve your score:
1. What went wrong? Why wasn’t your score what you expected?
Can you point to a single factor or problem that you feel caused the low
score? Were you sick on test day? Was there an emotional upheaval in your
life that caused a distraction? Were you late for the test or not able to use the
full time allotment? If you can point to any of these specific, individual
problems, then a retake should definitely be considered.
2. Is there enough time to improve?
Many problems that may show up in your score report may take a lot of time
for improvement. A deficiency in a particular math skill may require weeks or
months of tutoring and studying to improve. If you have enough time to
improve an identified weakness, then a retake should definitely be
considered.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
168
3. How will additional scores be used? Will a score average, highest score,
or most recent score be used?
Different test scores may be handled completely differently. If you’ve taken
the test multiple times, sometimes your highest score is used, sometimes
your average score is computed and used, and sometimes your most recent
score is used. Make sure you understand what method will be used to
evaluate your scores, and use that to help you determine whether a retake
should be considered.
4. Are my practice test scores significantly higher than my actual test score?
If you have taken a lot of practice tests and are consistently scoring at a much
higher level than your actual test score, then you should consider a retake.
However, if you’ve taken five practice tests and only one of your scores was
higher than your actual test score, or if your practice test scores were only
slightly higher than your actual test score, then it is unlikely that you will
significantly increase your score.
5. Do I need perfect scores or will I be able to live with this score? Will this
score still allow me to follow my dreams?
What kind of score is acceptable to you? Is your current score “good
enough?” Do you have to have a certain score in order to pursue the future
of your dreams? If you won’t be happy with your current score, and there’s
no way that you could live with it, then you should consider a retake.
However, don’t get your hopes up. If you are looking for significant
improvement, that may or may not be possible. But if you won’t be happy
otherwise, it is at least worth the effort.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
169
Remember that there are other considerations. To achieve your dream, it is
likely that your grades may also be taken into account. A great test score is
usually not the only thing necessary to succeed. Make sure that you aren’t
overemphasizing the importance of a high test score.
Furthermore, a retake does not always result in a higher score. Some test
takers will score lower on a retake, rather than higher. One study shows that
one-fourth of test takers will achieve a significant improvement in test score,
while one-sixth of test takers will actually show a decrease. While this shows
that most test takers will improve, the majority will only improve their scores a
little and a retake may not be worth the test taker’s effort.
Finally, if a test is taken only once and is considered in the added context of
good grades on the part of a test taker, the person reviewing the grades and
scores may be tempted to assume that the test taker just had a bad day while
taking the test, and may discount the low test score in favor of the high
grades. But if the test is retaken and the scores are approximately the same,
then the validity of the low scores are only confirmed. Therefore, a retake
could actually hurt a test taker by definitely bracketing a test taker’s score
ability to a limited range.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
170
Special Report: Ethics Research and Websites
Business Ethics Resources on WWW
Links to sites in the areas of codes of ethics, organizations, publications, specific
topics, and papers.
http://www.ethics.ubc.ca/resources/business
Discussions of Ethics on the Net
List of Internet discussion groups with links and subscription addresses.
http://frank.mtsu.edu/~jpurcell/Ethics/ethics.html
Ethics Resources on the Net
Links to sites in areas of business ethics such as codes of conduct, reference
sources, organizations, issues, corporations, consultants, and commentaries.
Also includes links to other types of ethics sites
(human rights, environment, etc.)
http://www.depaul.edu/ethics/
The On-Line Journal of Ethics
http://condor.depaul.edu/ethics/ethg1.html
The Newsletter of DePaul University's Institute for Business & Professional
Ethics
http://www.depaul.edu/ethics/newslet.html
Center for Ethical Business Cultures
Assists business leaders in developing practical, productive and responsible
relationships with key stakeholders.
http://www.stthomas.edu/www/mccr_http/index.html
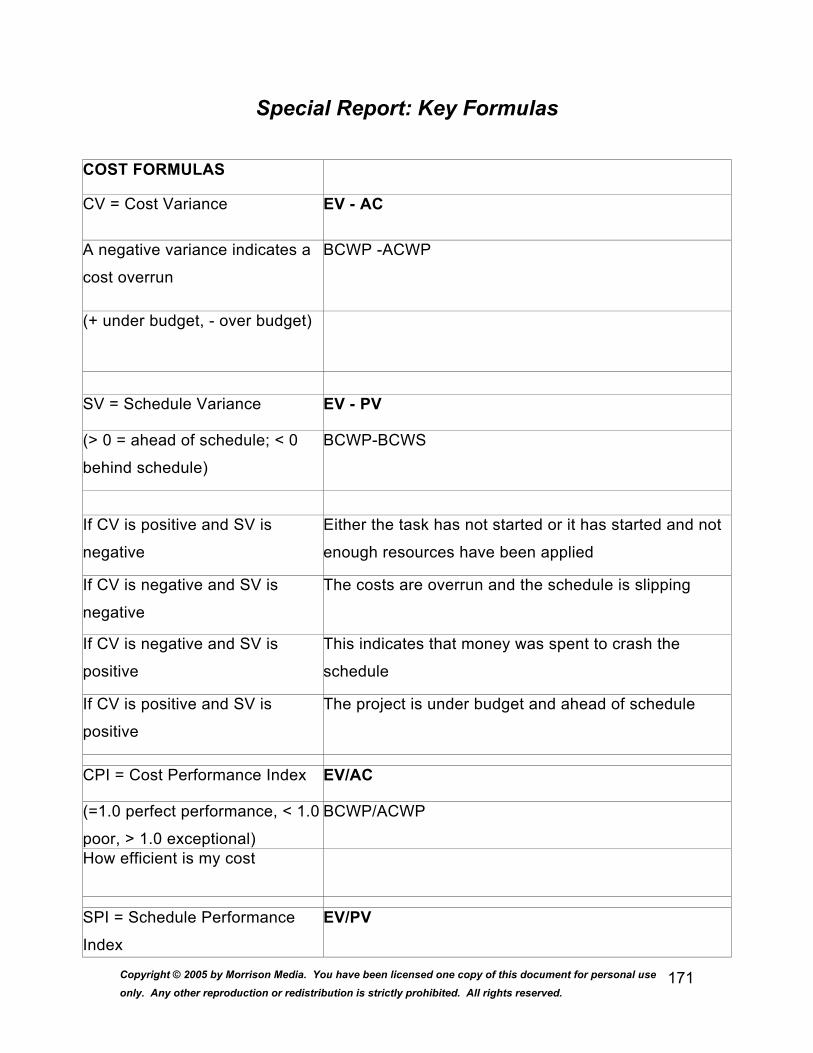
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
171
Special Report: Key Formulas
COST FORMULAS
CV = Cost Variance EV - AC
A negative variance indicates a
cost overrun
BCWP -ACWP
(+ under budget, - over budget)
SV = Schedule Variance EV - PV
(> 0 = ahead of schedule; < 0
behind schedule)
BCWP-BCWS
If CV is positive and SV is
negative
Either the task has not started or it has started and not
enough resources have been applied
If CV is negative and SV is
negative
The costs are overrun and the schedule is slipping
If CV is negative and SV is
positive
This indicates that money was spent to crash the
schedule
If CV is positive and SV is
positive
The project is under budget and ahead of schedule
CPI = Cost Performance Index EV/AC
(=1.0 perfect performance, < 1.0
poor, > 1.0 exceptional)
BCWP/ACWP
How efficient is my cost
SPI = Schedule Performance
Index
EV/PV
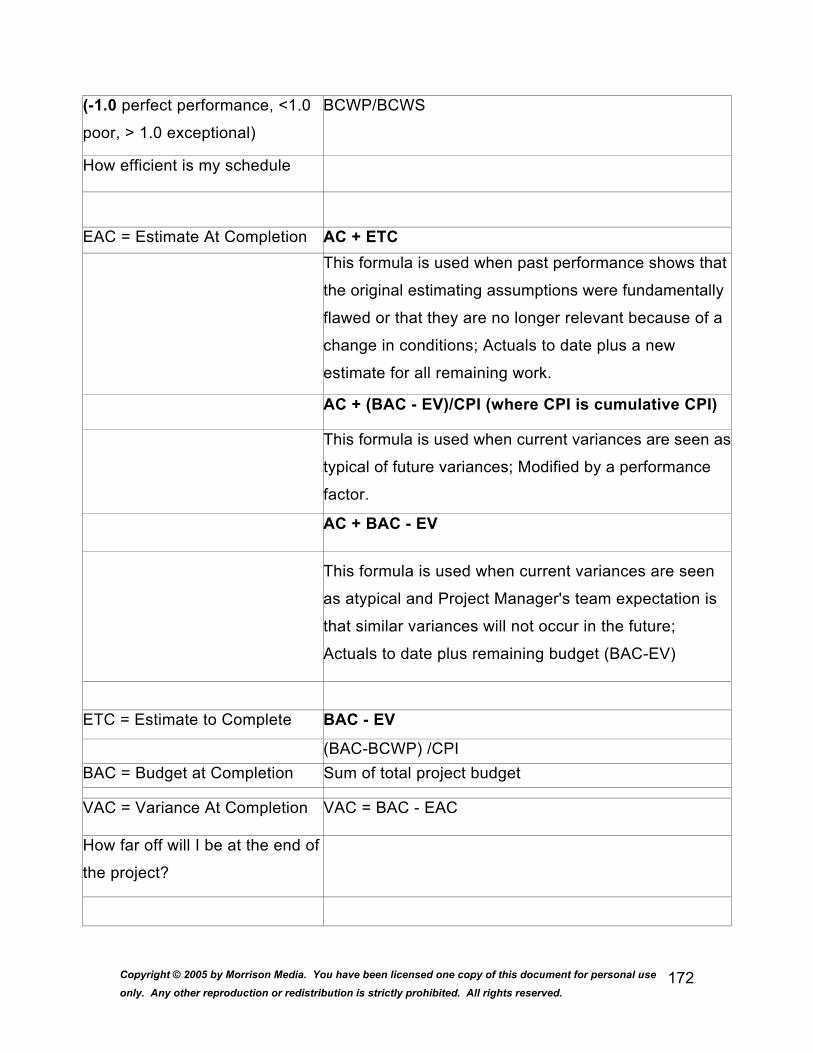
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
172
(-1.0 perfect performance, <1.0
poor, > 1.0 exceptional)
BCWP/BCWS
How efficient is my schedule
EAC = Estimate At Completion AC + ETC This formula is used when past performance shows that
the original estimating assumptions were fundamentally
flawed or that they are no longer relevant because of a
change in conditions; Actuals to date plus a new
estimate for all remaining work.
AC + (BAC - EV)/CPI (where CPI is cumulative CPI)
This formula is used when current variances are seen as
typical of future variances; Modified by a performance
factor.
AC + BAC - EV
This formula is used when current variances are seen
as atypical and Project Manager's team expectation is
that similar variances will not occur in the future;
Actuals to date plus remaining budget (BAC-EV)
ETC = Estimate to Complete BAC - EV
(BAC-BCWP) /CPI BAC = Budget at Completion Sum of total project budget
VAC = Variance At Completion VAC = BAC - EAC
How far off will I be at the end of
the project?

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
173
CV% = Cost Variance
Percentage
CV% = CV/EV*100
How far off is my cost?
SV% = Schedule Variance
Percentage
SV% = SV/PV*100
How far off is my schedule?
VAC% = Variance At
Completion Percentage
VAC% = VAC/BAC*100
Variable and Type Earned Value Description
PV = Planned Value (BCWS) The cost of what I planned to get done
EV = Earned Value (BCWP) The value of the work actually done
AC = Actual Cost (ACWP) The totals of costs incurred in a given period
Other Formulas
Straight Line Depreciation Cost- Salvage/Time Double Declining Balance Double the SL Depreciation; $ X original cost -
accumulated depreciation
Sum of Years (SOY) (Cost-Salvage) X year/sum of years (3-2-1/6)
Future Value D(r+1) to the # of periods
Simple Interest Interest = Principle X Rate X Time Compound Interest FV (Future Value) = Deposit (1 + rate) ; Principle/ (r+1)
to the # of periods
Communication Channels # Of Team Members (t) X (t-1)/2
Expected Value Optimistic + (4XMost Likely) + Pessimistic/6
Standard Deviation Optimistic-Pessimistic/6 (one deviation is the difference
between EV and SD)
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
174
Standard Deviations 68.26, 95.46, 99.73
Variance Planned - Actual; % Variance = Variance/Planned
EMV = Expected Monetary
Value
probability X amount of Stake (probability is
frequency/# of possible; amount at stake = cost of loss
and least
cost to restoreNPV = Net Present Value Initial payment of 12,000, annual discount rate of 10-%
cost or revenue/(1-r) to the t
Sometimes called discounted cash flows, assumes that
there is a minimum desired rate of return and that all
future cash flows are discounted to the present time. It is
the sum of all the discounted cash flows, both outgoing
and incoming, over the life of the project.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
175
Special Report: What is Test Anxiety and How to Overcome It?
The very nature of tests caters to some level of anxiety, nervousness or
tension, just as we feel for any important event that occurs in our lives. A little
bit of anxiety or nervousness can be a good thing. It helps us with motivation,
and makes achievement just that much sweeter. However, too much anxiety
can be a problem; especially if it hinders our ability to function and perform.
“Test anxiety,” is the term that refers to the emotional reactions that some
test-takers experience when faced with a test or exam. Having a fear of
testing and exams is based upon a rational fear, since the test-taker’s
performance can shape the course of an academic career. Nevertheless,
experiencing excessive fear of examinations will only interfere with the test-
takers ability to perform, and his/her chances to be successful.
There are a large variety of causes that can contribute to the development
and sensation of test anxiety. These include, but are not limited to lack of
performance and worrying about issues surrounding the test.
Lack of Preparation
Lack of preparation can be identified by the following behaviors or situations:
Not scheduling enough time to study, and therefore cramming the night
before the test or exam
Managing time poorly, to create the sensation that there is not enough time to
do everything
Failing to organize the text information in advance, so that the study material
consists of the entire text and not simply the pertinent information
Poor overall studying habits

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
176
Worrying, on the other hand, can be related to both the test taker, or many
other factors around him/her that will be affected by the results of the test.
These include worrying about:
Previous performances on similar exams, or exams in general
How friends and other students are achieving
The negative consequences that will result from a poor grade or failure
There are three primary elements to test anxiety. Physical components,
which involve the same typical bodily reactions as those to acute anxiety (to
be discussed below). Emotional factors have to do with fear or panic. Mental
or cognitive issues concerning attention spans and memory abilities.
Physical Signals
There are many different symptoms of test anxiety, and these are not limited
to mental and emotional strain. Frequently there are a range of physical
signals that will let a test taker know that he/she is suffering from test anxiety.
These bodily changes can include the following:
Perspiring
Sweaty palms
Wet, trembling hands
Nausea
Dry mouth
A knot in the stomach
Headache
Faintness
Muscle tension

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
177
Aching shoulders, back and neck
Rapid heart beat
Feeling too hot/cold
To recognize the sensation of test anxiety, a test-taker should monitor
him/herself for the following sensations:
The physical distress symptoms as listed above
Emotional sensitivity, expressing emotional feelings such as the need to cry
or laugh too much, or a sensation of anger or helplessness
A decreased ability to think, causing the test-taker to blank out or have racing
thoughts that are hard to organize or control.
Though most students will feel some level of anxiety when faced with a test or
exam, the majority can cope with that anxiety and maintain it at a manageable
level. However, those who cannot are faced with a very real and very serious
condition, which can and should be controlled for the immeasurable benefit of
this sufferer.
Naturally, these sensations lead to negative results for the testing experience.
The most common effects of test anxiety have to do with nervousness and
mental blocking.
Nervousness
Nervousness can appear in several different levels:
The test-taker’s difficulty, or even inability to read and understand the
questions on the test
The difficulty or inability to organize thoughts to a coherent form

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
178
The difficulty or inability to recall key words and concepts relating to the
testing questions (especially essays)
The receipt of poor grades on a test, though the test material was well known
by the test taker
Conversely, a person may also experience mental blocking, which involves:
Blanking out on test questions
Only remembering the correct answers to the questions when the test has
already finished.
Fortunately for test anxiety sufferers, beating these feelings, to a large
degree, has to do with proper preparation. When a test taker has a feeling of
preparedness, then anxiety will be dramatically lessened.
The first step to resolving anxiety issues is to distinguish which of the two
types of anxiety are being suffered. If the anxiety is a direct result of a lack of
preparation, this should be considered a normal reaction, and the anxiety
level (as opposed to the test results) shouldn’t be anything to worry about.
However, if, when adequately prepared, the test-taker still panics, blanks out,
or seems to overreact, this is not a fully rational reaction. While this can be
considered normal too, there are many ways to combat and overcome these
effects.
Remember that anxiety cannot be entirely eliminated, however, there are
ways to minimize it, to make the anxiety easier to manage. Preparation is
one of the best ways to minimize test anxiety. Therefore the following
techniques are wise in order to best fight off any anxiety that may want to
build.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
179
To begin with, try to avoid cramming before a test, whenever it is possible.
By trying to memorize an entire term’s worth of information in one day, you’ll
be shocking your system, and not giving yourself a very good chance to
absorb the information. This is an easy path to anxiety, so for those who
suffer from test anxiety, cramming should not even be considered an option.
Instead of cramming, work throughout the semester to combine all of the
material which is presented throughout the semester, and work on it gradually
as the course goes by, making sure to master the main concepts first, leaving
minor details for a week or so before the test.
To study for the upcoming exam, be sure to pose questions that may be on
the examination, to gauge the ability to answer them by integrating the ideas
from your texts, notes and lectures, as well as any supplementary readings.
If it is truly impossible to cover all of the information that was covered in that
particular term, concentrate on the most important portions, that can be
covered very well. Learn these concepts as best as possible, so that when
the test comes, a goal can be made to use these concepts as presentations
of your knowledge.
In addition to study habits, changes in attitude are critical to beating a struggle
with test anxiety. In fact, an improvement of the perspective over the entire
test-taking experience can actually help a test taker to enjoy studying and
therefore improve the overall experience. Be certain not to overemphasize
the significance of the grade - know that the result of the test is neither a
reflection of self worth, nor is it a measure of intelligence; one grade will not
predict a person’s future success.
To improve an overall testing outlook, the following steps should be tried:
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
180
Keeping in mind that the most reasonable expectation for taking a test is to
expect to try to demonstrate as much of what you know as you possibly can.
Reminding ourselves that a test is only one test; this is not the only one, and
there will be others.
The thought of thinking of oneself in an irrational, all-or-nothing term should
be avoided at all costs.
A reward should be designated for after the test, so there’s something to look
forward to. Whether it be going to a movie, going out to eat, or simply visiting
friends, schedule it in advance, and do it no matter what result is expected on
the exam.
Test-takers should also keep in mind that the basics are some of the most
important things, even beyond anti-anxiety techniques and studying. Never
neglect the basic social, emotional and biological needs, in order to try to
absorb information. In order to best achieve, these three factors must be held
as just as important as the studying itself.
Study Steps
Remember the following important steps for studying:
Maintain healthy nutrition and exercise habits. Continue both your
recreational activities and social pass times. These both contribute to your
physical and emotional well being.
Be certain to get a good amount of sleep, especially the night before the test,
because when you’re overtired you are not able to perform to the best of your
best ability.
Keep the studying pace to a moderate level by taking breaks when they are
needed, and varying the work whenever possible, to keep the mind fresh
instead of getting bored.

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
181
When enough studying has been done that all the material that can be
learned has been learned, and the test taker is prepared for the test, stop
studying and do something relaxing such as listening to music, watching a
movie, or taking a warm bubble bath.
There are also many other techniques to minimize the uneasiness or
apprehension that is experienced along with test anxiety before, during, or
even after the examination. In fact, there are a great deal of things that can
be done to stop anxiety from interfering with lifestyle and performance.
Again, remember that anxiety will not be eliminated entirely, and it shouldn’t
be. Otherwise that “up” feeling for exams would not exist, and most of us
depend on that sensation to perform better than usual. However, this anxiety
has to be at a level that is manageable.
Of course, as we have just discussed, being prepared for the exam is half the
battle right away. Attending all classes, finding out what knowledge will be
expected on the exam, and knowing the exam schedules are easy steps to
lowering anxiety. Keeping up with work will remove the need to cram, and
efficient study habits will eliminate wasted time. Studying should be done in
an ideal location for concentration, so that it is simple to become interested in
the material and give it complete attention. A method such as SQ3R (Survey,
Question, Read, Recite, Review) is a wonderful key to follow to make sure
that the study habits are as effective as possible, especially in the case of
learning from a textbook. Flashcards are great techniques for memorization.
Learning to take good notes will mean that notes will be full of useful
information, so that less sifting will need to be done to seek out what is
pertinent for studying. Reviewing notes after class and then again on
occasion will keep the information fresh in the mind. From notes that have
been taken summary sheets and outlines can be made for simpler reviewing.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
182
A study group can also be a very motivational and helpful place to study, as
there will be a sharing of ideas, all of the minds can work together, to make
sure that everyone understands, and the studying will be made more
interesting because it will be a social occasion.
Basically, though, as long as the test-taker remains organized and self
confident, with efficient study habits, less time will need to be spent studying,
and higher grades will be achieved.
To become self confident, there are many useful steps. The first of these is
“self talk.” It has been shown through extensive research, that self-talk for
students who suffer from test anxiety, should be well monitored, in order to
make sure that it contributes to self confidence as opposed to sinking the
student. Frequently the self talk of test-anxious students is negative or self-
defeating, thinking that everyone else is smarter and faster, that they always
mess up, and that if they don’t do well, they’ll fail the entire course. It is
important to decreasing anxiety that awareness is made of self talk. Try
writing any negative self thoughts and then disputing them with a positive
statement instead. Begin self-encouragement as though it was a friend
speaking. Repeat positive statements to help reprogram the mind to
believing in successes instead of failures.
Helpful Techniques
Other extremely helpful techniques include:
Self-visualization of doing well and reaching goals
While aiming for an “A” level of understanding, don’t try to “overprotect” by
setting your expectations lower. This will only convince the mind to stop
studying in order to meet the lower expectations.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
183
Don’t make comparisons with the results or habits of other students. These
are individual factors, and different things work for different people, causing
different results.
Strive to become an expert in learning what works well, and what can be
done in order to improve. Consider collecting this data in a journal.
Create rewards for after studying instead of doing things before studying that
will only turn into avoidance behaviors.
Make a practice of relaxing - by using methods such as progressive
relaxation, self-hypnosis, guided imagery, etc - in order to make relaxation an
automatic sensation.
Work on creating a state of relaxed concentration so that concentrating will
take on the focus of the mind, so that none will be wasted on worrying.
Take good care of the physical self by eating well and getting enough sleep.
Plan in time for exercise and stick to this plan.
Beyond these techniques, there are other methods to be used before, during
and after the test that will help the test-taker perform well in addition to
overcoming anxiety.
Before the exam comes the academic preparation. This involves establishing
a study schedule and beginning at least one week before the actual date of
the test. By doing this, the anxiety of not having enough time to study for the
test will be automatically eliminated. Moreover, this will make the studying a
much more effective experience, ensuring that the learning will be an easier
process. This relieves much undue pressure on the test-taker.
Summary sheets, note cards, and flash cards with the main concepts and
examples of these main concepts should be prepared in advance of the
actual studying time. A topic should never be eliminated from this process.
By omitting a topic because it isn’t expected to be on the test is only setting
up the test-taker for anxiety should it actually appear on the exam. Utilize the
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
184
course syllabus for laying out the topics that should be studied. Carefully go
over the notes that were made in class, paying special attention to any of the
issues that the professor took special care to emphasize while lecturing in
class. In the textbooks, use the chapter review, or if possible, the chapter
tests, to begin your review.
It may even be possible to ask the instructor what information will be covered
on the exam, or what the format of the exam will be (for example, multiple
choice, essay, free form, true-false). Additionally, see if it is possible to find
out how many questions will be on the test. If a review sheet or sample test
has been offered by the professor, make good use of it, above anything else,
for the preparation for the test. Another great resource for getting to know the
examination is reviewing tests from previous semesters. Use these tests to
review, and aim to achieve a 100% score on each of the possible topics.
With a few exceptions, the goal that you set for yourself is the highest one
that you will reach.
Take all of the questions that were assigned as homework, and rework them
to any other possible course material. The more problems reworked, the
more skill and confidence will form as a result. When forming the solution to
a problem, write out each of the steps. Don’t simply do head work. By doing
as many steps on paper as possible, much clarification and therefore
confidence will be formed. Do this with as many homework problems as
possible, before checking the answers. By checking the answer after each
problem, a reinforcement will exist, that will not be on the exam. Study
situations should be as exam-like as possible, to prime the test-taker’s system
for the experience. By waiting to check the answers at the end, a
psychological advantage will be formed, to decrease the stress factor.
Another fantastic reason for not cramming is the avoidance of confusion in
concepts, especially when it comes to mathematics. 8-10 hours of study will

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
185
become one hundred percent more effective if it is spread out over a week or
at least several days, instead of doing it all in one sitting. Recognize that the
human brain requires time in order to assimilate new material, so frequent
breaks and a span of study time over several days will be much more
beneficial.
Additionally, don’t study right up until the point of the exam. Studying should
stop a minimum of one hour before the exam begins. This allows the brain to
rest and put things in their proper order. This will also provide the time to
become as relaxed as possible when going into the examination room. The
test-taker will also have time to eat well and eat sensibly. Know that the brain
needs food as much as the rest of the body. With enough food and enough
sleep, as well as a relaxed attitude, the body and the mind are primed for
success.
Avoid any anxious classmates who are talking about the exam. These
students only spread anxiety, and are not worth sharing the anxious
sentimentalities.
Before the test also involves creating a positive attitude, so mental
preparation should also be a point of concentration. There are many keys to
creating a positive attitude. Should fears become rushing in, make a
visualization of taking the exam, doing well, and seeing an A written on the
paper. Write out a list of affirmations that will bring a feeling of confidence,
such as “I am doing well in my English class,” “I studied well and know my
material,” “I enjoy this class.” Even if the affirmations aren’t believed at first, it
sends a positive message to the subconscious which will result in an
alteration of the overall belief system, which is the system that creates reality.
If a sensation of panic begins, work with the fear and imagine the very worst!
Work through the entire scenario of not passing the test, failing the entire

Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
186
course, and dropping out of school, followed by not getting a job, and pushing
a shopping cart through the dark alley where you’ll live. This will place things
into perspective! Then, practice deep breathing and create a visualization of
the opposite situation - achieving an “A” on the exam, passing the entire
course, receiving the degree at a graduation ceremony.
On the day of the test, there are many things to be done to ensure the best
results, as well as the most calm outlook. The following stages are suggested
in order to maximize test-taking potential:
Begin the examination day with a moderate breakfast, and avoid any coffee
or beverages with caffeine if the test taker is prone to jitters. Even people
who are used to managing caffeine can feel jittery or light-headed when it is
taken on a test day.
Attempt to do something that is relaxing before the examination begins. As
last minute cramming clouds the mastering of overall concepts, it is better to
use this time to create a calming outlook.
Be certain to arrive at the test location well in advance, in order to provide
time to select a location that is away from doors, windows and other
distractions, as well as giving enough time to relax before the test begins.
Keep away from anxiety generating classmates who will upset the sensation
of stability and relaxation that is being attempted before the exam.
Should the waiting period before the exam begins cause anxiety, create a
self-distraction by reading a light magazine or something else that is relaxing
and simple.
During the exam itself, read the entire exam from beginning to end, and find
out how much time should be allotted to each individual problem. Once
writing the exam, should more time be taken for a problem, it should be
abandoned, in order to begin another problem. If there is time at the end, the
unfinished problem can always be returned to and completed.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
187
Read the instructions very carefully - twice - so that unpleasant surprises
won’t follow during or after the exam has ended.
When writing the exam, pretend that the situation is actually simply the
completion of homework within a library, or at home. This will assist in
forming a relaxed atmosphere, and will allow the brain extra focus for the
complex thinking function.
Begin the exam with all of the questions with which the most confidence is
felt. This will build the confidence level regarding the entire exam and will
begin a quality momentum. This will also create encouragement for trying the
problems where uncertainty resides.
Going with the “gut instinct” is always the way to go when solving a problem.
Second guessing should be avoided at all costs. Have confidence in the
ability to do well.
For essay questions, create an outline in advance that will keep the mind
organized and make certain that all of the points are remembered. For
multiple choice, read every answer, even if the correct one has been spotted -
a better one may exist.
Continue at a pace that is reasonable and not rushed, in order to be able to
work carefully. Provide enough time to go over the answers at the end, to
check for small errors that can be corrected.
Should a feeling of panic begin, breathe deeply, and think of the feeling of the
body releasing sand through its pores. Visualize a calm, peaceful place, and
include all of the sights, sounds and sensations of this image. Continue the
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
188
deep breathing, and take a few minutes to continue this with closed eyes.
When all is well again, return to the test.
If a “blanking” occurs for a certain question, skip it and move on to the next
question. There will be time to return to the other question later. Get
everything done that can be done, first, to guarantee all the grades that can
be compiled, and to build all of the confidence possible. Then return to the
weaker questions to build the marks from there.
Remember, one’s own reality can be created, so as long as the belief is there,
success will follow. And remember: anxiety can happen later, right now,
there’s an exam to be written!
After the examination is complete, whether there is a feeling for a good grade
or a bad grade, don’t dwell on the exam, and be certain to follow through on
the reward that was promised…and enjoy it! Don’t dwell on any mistakes that
have been made, as there is nothing that can be done at this point anyway.
Additionally, don’t begin to study for the next test right away. Do something
relaxing for a while, and let the mind relax and prepare itself to begin
absorbing information again.
From the results of the exam - both the grade and the entire experience, be
certain to learn from what has gone on. Perfect studying habits and work
some more on confidence in order to make the next examination experience
even better than the last one.
Learn to avoid places where openings occurred for laziness, procrastination
and day dreaming.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
189
Use the time between this exam and the next one to better learn to relax,
even learning to relax on cue, so that any anxiety can be controlled during the
next exam. Learn how to relax the body. Slouch in your chair if that helps.
Tighten and then relax all of the different muscle groups, one group at a time,
beginning with the feet and then working all the way up to the neck and face.
This will ultimately relax the muscles more than they were to begin with.
Learn how to breath deeply and comfortably, and focus on this breathing
going in and out as a relaxing thought. With every exhale, repeat the word
“relax.”
As common as test anxiety is, it is very possible to overcome it. Make
yourself one of the test-takers who overcome this frustrating hindrance.
Copyright © 2005 by Morrison Media. You have been licensed one copy of this document for personal use only. Any other reproduction or redistribution is strictly prohibited. All rights reserved.
190
Special Report: Additional Bonus Material
Due to our efforts to try to keep this book to a manageable length, we’ve
created a link that will give you access to all of your additional bonus material.
Please visit http://www.mo-media.com/cphq/bonuses to access the
information.