CPG Medical Students

of 33
-
Upload
kalichandren-arumugam -
Category
Documents
-
view
229 -
download
0
Transcript of CPG Medical Students
-
8/10/2019 CPG Medical Students
1/33
GuidelinesforMedicalStud
Gynaecological&
obstetric
history
ta
andphysicalexamination
Department of Obstetrics & GynaecologUniversity of Malta Medical School
Malta
2011
-
8/10/2019 CPG Medical Students
2/33
2
Published byDepartment of Obstetrics & GynaecologyUniversity of Malta Medical School, Malta
Department of Obstetrics & Gynaecology, UMMS, 2011
No part of this publication may be reproduced, stored in a retrieval systemor transmitted to any form by any means, electronic, mechanical,
photocopying, recording or otherwise, without the previous permission ofthe publisher and author.
-
8/10/2019 CPG Medical Students
3/33
-
8/10/2019 CPG Medical Students
4/33
4
INTRODUCTION
Female reproductive health is an important component of medical education. Regardless of the
specialitythatthemedicalstudentswillultimatelychoosetopursue,asmedicalpractitionerstheyneed
tohaveabasicknowledgeandskillspertinenttothecareofthefemalepatient.Theyneedtonotonly
needtoknowhowtoperformtheclinicalassessment,buthowtodothisinasensitive,competent,and
ethical manner. The principles of history taking and physical examination in obstetric and
gynaecologicalpatientsaresimilartothose inotherbranchesofmedicine,butthereareaspectsthat
arespecifictothespeciality.
Ingeneral,history taking andphysicalexamination shouldbe carriedout in a logical sequence. The
medicalstudentshouldunderstandthepurposeofeachposedquestionandeachobservationalaspect
oftheexamination.Whilethereismarkedoverlapbetweentheclinicalassessmentoftheobstetricand
thegynaecologicalpatient,itwillbeappreciatedthattheemphasisdiffersinthetwoclinicalsituations.
HISTORYTAKING
The scope of taking a clinical history in any situation is to identify the clinical problem and obtain
sufficientdetailtoallow forthe formulationofaprovisionaldiagnosissothatthesubsequentclinical
examinationand
investigations
are
targeted
to
narrow
down
the
diagnostic
possibilities
further.
The
eventualpresentationoftheclinicalhistory,whetherthisispresentedverballyorinthewrittenformat,
shouldfollowalogicalandchronologicalsequencepreferablyinparagraphformat[asinastory]see
example.
-
8/10/2019 CPG Medical Students
5/33
5
Duringhistorytaking,themedicalstudentshouldatalltimesshowthepatienttherespectthatisdueto
her;while full confidentialitymustbemaintained at all timesbearing inmind that the relationship
betweentheprofessionalandhisclient isbasedonmutualtrustandrespect.Themedicalprofession
haslong
identified
the
need
for
confidentiality
with
the
classical
Hippocratic
Oath
stating:
All
that
may
cometomyknowledgeintheexerciseofmyprofessionorindailycommercewithmen,whichoughtnot
to be spread abroad, Iwill keep secret andwill never reveal. The concept of professional secrecy
relatingtothemedicalprofessionwassostronglyfeltthatitwasincorporatedwithintheCriminalCode
ofMalta[Ch.9:257].Thelawreadsasfollows:Ifanyphysician,surgeon,obstetricianorapothecaryor,
ingeneral,
any
other
person
who,
by
reason
of
his
calling
or
profession,
becomes
the
depository
of
any
secretconfidedtohim1,shall,exceptwhencompelledbylawtogiveinformationtothepublicauthority,
disclosesuchsecret,heshall,onconvictionbeliabletoafine.Furthermore,anyconvictionunderthis
headingmayalsoinvolvedisciplinaryactiononthepartoftheMedicalCouncil.
History taking should follow a logical and chronological sequence. Each clinician has his particular
preference.Ageneralusefulschemeforagynaecologicalhistoryisoutlinedbelow.
Introduce
yourself
and
obtain
consent
to
take
history
Hello.IamMr/Ms****,amedicalstudent.DoyoumindifIaskyousome
questionsaboutyourmedicalcondition?
1This
includes
the
medical
student
and
any
other
paramedical
professional.
-
8/10/2019 CPG Medical Students
6/33
6
Personalhistory Name,age,address[ifrelevant],maritalstatus,occupation.
Presentingcomplaint
Whatistheproblemthatbroughtyoutothehospital/clinic?Besttorecordthisinthepatientsownwords.
Were you referred by your doctor or did you selfrefer yourself to the
hospital/clinic?
Patientmaynotfurnishsufficientdetails,inwhichcaseitwillbenecessary
toamplify
with
specific
directed
questions.
E.g.
SOCRATES
relating
to
pain:
o
Site:where,local/diffuse
o Onset:rapid/gradual,pattern,worse/bettersinceonset
o Character:sharp/dull/stabbing,burning/cramp/crushing
o
Radiation:Doesthepainaffectyouanywhereelse?[to
thigh/loin/elsewhere]
o Alleviatingfactors:Whatdoyoudotomakeyourselfcomfortable?
Isthepainbetteraftermenstruation?
o
Timecourse:Whendidthepainstart?;ifpainischronicWhat
madeyouseekattentionnow?Isthepainworseatanyparticular
timeofthecycle?
o
Exacerbatingfactors:Isthereanythingthatbringsonthepainor
makesitworse?
o
Severity&Impactonlife:Onascaleof1to10,atwhatlevelwould
youclassifythepain?"Doesitinterruptyourlife?"
-
8/10/2019 CPG Medical Students
7/33
-
8/10/2019 CPG Medical Students
8/33
8
Associated
Symptoms
Systemic
enquiry
Isthereanythingelsethatyouhavenoticedrelatingtothepain?vaginal
discharge [colour, consistency, amount, smell] or bleeding [amount,
colour];weight
changes;
fever,
bowel
problems
[constipation,
diarrhoea,
etc]; urinary problems [dysuria, frequency, hesitancy, nocturia, colour
change,incontinence,feelingofincompleteemptying,etc.];etc.
Menstrual
history
Lengthandregularityofcycles
Severityofmenses lengthofmenses,heavy,flooding,presenceofclots,
numberof
tampons/pads
used
Painduringmensestimingofpaininrelationtomenses[beginning,end];
characterofpain[dullpersistent,coliky]
Lastmenstrualperiod[firstday]
Presenceofspellsofnoperiodsinabsenceofpregnancy;bleedingbetween
periods;afterintercourse.
Timeofmenarcheandmenopause.Ifmenopausal:assessforassociated
symptoms[hotflushes,nightsweats];historyofpostmenopausalbleeding.
Sexualhistory
Sexuallyactive;numberofpartners[bediscreet!].
Contraceptionbeingusedcurrentlyandanyusedpreviously.
Physicalorotherdifficultiesduringintercourseifpaincheckwhether
deep/superficial,always/
sometimes.
Papsmear:date&resultoflastsmear.
-
8/10/2019 CPG Medical Students
9/33
9
Obstetrichistory
Anydifficultyinconceiving;Whattreatmentwasusedtoassistthe
infertility?
Possibilityof
current
pregnancy.
Numberofpreviouschildren gender,antenatalproblems,birthweights,
modeofdelivery,postpartumcomplications[bleeding,thrombosis,
infection].
Numberofmiscarriages,terminationsand/orectopicswhatmonththey
occurred,pattern
of
miscarriage
[spontaneous,
induced],
surgery
performed.
Past
medical
&
surgicalhistory
Doyoucurrentlysufferfromanyillnesseshypertension,diabetes,
epilepsy,asthma,bleedingdisorders,etc?;Haveyoueverbeenseriouslyill
beforecardiovascularepisodes,jaundice,STDPID,etc.?
Haveyouundergoneanysurgeryappendicitis,gynaecologicalsurgery
abdominalorvaginal[inclusiveD&C]?;Didyouhaveanyproblemswith
anaesthesia?;Didyourequirebloodtransfusion?
Haveyoueverseenagynaecologistbeforeforwhatreason?
Haveyoureceivedallthechildhoodvaccinationsrubella,HPV,TB?
Drug
history
Areyouonanymedicationsatpresentlist?
Areyou
allergic
to
any
medications
what
happened
when
you
took
the
medication? [ensureallergysincepatientsoftenassociatedevelopmentof
vaginalthrushasanadversereactiontoantibioticuse].
-
8/10/2019 CPG Medical Students
10/33
10
Familyhistory
Areyourparentsstillalive?Dotheysufferfromanyillness?ifdead
Whatwasthecauseofdeath?
Doyou
have
any
brothers
or
sisters?
ifyes
What
is
their
state
of
health?
Isthereanyfamilyrelateddiseaseinyourfamilythatyouareawareof?
diabetes,hypertension,malignancy,twins
Whatisthestateofhealthofyourspouse?Yourchildren?
Socialhistory
Race&
migration
ifrelevant
Presentandpastoccupations
Diet,physicalactivity
Smoking,alcohol,entertainmentdrugs
Wholiveswithyouathome?supportofotherhouseholdmembers;
Anypets?
Haveyoutravelledoverseasrecently?Where?
Atthispointoneshouldbe inapositionto identifythePRESENTINGCOMPLAINTandtoformulatea
workingprovisionaldiagnosis.
-
8/10/2019 CPG Medical Students
11/33
11
CLINICALEXAMINATION
Thescopeoftheclinicalexaminationistogatherfurthercluestosupplementtheinformationgathered
fromthe
clinical
history
to
help
identify
the
clinical
problem
and
narrow
down
the
differential
diagnosis.
Withthisaiminmind,theexaminationshouldbeacomprehensivebuttargetedone.Alwaysobtainthe
patientconsenttoallowyoutoperformtheexaminationandexplainatalltimestothepatientwhat
youplantodo.
REMEMBERTO
ALWAYS
PUT
THE
PATIENT
AT
EASE
AND
ENSURE
COMFORT.
BESENSITIVETOTHEPATIENTSFEELINGSANDDECENCY.
Obtaining
consent
toexamine
patient
Doyou
mind
ifIexamine
you?
You
can
ask
me
to
stop
at
any
time
you
feel
uncomfortable?
-
8/10/2019 CPG Medical Students
12/33
12
SystemicExamination
A systemic examination is always useful since it can identify conditions that may predispose or
aggravatethe
presenting
complaint.
Generalappearance Weight:anorexic,cachectic,orobese.
Hydrationlevel,Hyperventilation,Hiccupping,Twitching,spasms
Hands
&
Arms Examinenails:koilonychias,leuconychia[whitetransversebands],
Muehrcke'snails
[white
paired
lines
near
fingernail
tip];
finger
clubbing;
nicotinestains
Checkpalmsforpalmarcrease,anaemiaorerythemia
Wrists:checkpulsererate,regularity,andcharacter.
Checkforscratchmarks,injectionmarks,spidernaevi,bruising.
Checkbloodpressure
Face,
neck,
chest
Checkeyes:jaundice,anaemia,considerfundoscopywhenindicated.
Mouth:fetor.ulcers,infections,hypertrophicgums/gingivitis.
Face:cloasma,rash.
Checkheartsounds:rate,rhythm,extrasounds/murmurs
Checklungs:wheezing,bronchialsounds,crepitations[basal],etc.
Legs
Checkfor
oedema
[pitting
till
what
level:
ankle/shin];
Presenceofvaricosities+/ thrombosis[superficial/deepunilateral
swelling,tenderness]
Checkperipheralvasculature:pulses
Checktoes&foot:signsofdiscolouration,gangrene,tophi.
-
8/10/2019 CPG Medical Students
13/33
13
AbdominalExamination
Anabdominalexaminationisanessentialpartofthegynaecologicalexaminationandshouldpreferably
precede the genital examination. The adage of INSPECTION PALPATION PERCUSSION
AUSCULTATIONshould
always
be
adhered
to.
Duringtheexamination,ensurethattheabdomen issufficientlyexposedtoallowaclearoverallview
from the symphysispubis to thecostalmargin.Aspartof theabdominalexamination, remember to
always include the supraclavicular region [check for Virchov lymph nodes]; and the inguinal region
[checkfor
lymph
nodes/hernia].
o REMEMBERTOAGAINOBTAINCONSENTTOEXAMINETHEPATIENTSABDOMEN.
o
REMEMBERTOINFORMANDEXPLAINTOTHEPATIENTWHATYOUINTENDTODOAT
ALLTIMES.
o
WARN
PATIENT
TO
INFORM
YOU
IF
THE
EXAMINATION
BECOMES
UNCOMFORTABLE
ATANYTIME.
o
ALWAYSLOOKATTHEPATIENTSFACEDURINGTHEEXAMINATIONTOIDENTIFYANY
SIGNSOFPAINORDISCOMFORTELICITEDDURINGTHEEXAMINATION.
o MAKESURETHATTHEPATIENTHASRECENTLYEMPTIEDHERBLADDER.
-
8/10/2019 CPG Medical Students
14/33
14
Inspection Assessthegeneralappearanceoftheabdomendistended[fat,foetus,
faeces,flatus,fluid,fullsizedtumours],umbilicus[flattened,possible
presenceof
hernae,
Sister
Joseph
nodule,
Cullens
discolouration],
superficialveinprominence,telangectasia/caputmedusae,
discolouration,pigmentation,scars[onemayneedtorollthepatientto
theside],striae,presenceofstoma,anyobviouslyvisible
masses/peristalsis/movements/pulsations.
Palpation
ensurewarmcleanhands;
ensurerelaxationof
abdominal
muscles.
Startwith
light
palpation
first
and
go
systematically
through
all
the
six
divisionsoftheabdomenRIF,rightHypochondrium,epigastrium,left
hypochondrium,LIF,hypogastrium.[Startfromnontenderlocationfirst]
o Lookforanymasses,tendernesswith/outguarding
Proceedwithdeeperpalpation,warningthepatientthatthismaybe
uncomfortableinwhichcaseistotellyouandyouwillstopthe
examination.Keepavisuallookoutforandfacialgrimacethatreflectdiscomfort.Gothroughthesixdivisionsoftheabdomen.
o Lookforanymasses,tendernesswith/outguarding
o Ifanytendernesscheckforthepresenceofrebound
tendernesswarningthepatientfirst.Also,assessforany
referredpain
during
palpation.
o Ifamassispalpable,assesssize[measurediameterin
centimetreorgestationalageequivalence],form
[regular/irregular],consistency[hard,soft,cystic],mobility,
tenderness,relationshiptoabdominalwall[superficial,intra
abdominal],etc.
-
8/10/2019 CPG Medical Students
15/33
15
Proceedtoexaminespecificallyforanenlargedortenderliver[check
Murphyssign],spleenandkidneys.Remembertoalsocheckthebackfor
tendernessoverbaseofspineoroverloin[kidneypunch],sacral
oedema.
Percussion PercussforthetopborderofliverdownRightmidclavicularline[normally
at5th
rib]andcontinuedowntoabdominaledgecalculatingspan
[generally12.5
cm].
Percussion
of
liver
border
for
loss
of
dullness
in
presenceofairinabdomen.
Percussspleentoassesssizewhensplenomegalysuspect.
Percussforkidneysizeestimationwhenenlarged;toassessanenlarged
bladderorextentofabdominalmass.
Checkforthepresenceofascites
o
Shiftingdullnessthedoctorspercussingfingerisplacedvertically
sothatfingertipispointingtowardsthepatientslegs;start
percussingatmidlineandcontinueleftlaterallyuntildullness
noted.Levelmarkedandpatientrolledovertorightforafew
minutes,thenrepercuss.Ascitespresentifthedullnessmoves
mediallyand
previous
point
of
dullness
is
now
resonant.
o
Fluidthrilldoctorplaceshandsoneachofthepatientsflanks,
whilethepatientisaskedtoplaceherleftlateraledgeofthehand
verticallyonthemidlineattheumbilicus;doctorflickshandon
rightflank,acorrespondingthrillisfeltbythecontralateralhand.
-
8/10/2019 CPG Medical Students
16/33
16
Auscultation
Belowumbilicustoassessbowelsoundsfor:
o
Rushingsoundcalled"borborygmi";
o Nosoundfor3minutes;
o
"Tinkling"sound.
Aboveumbilicusfor:AAAbruit;Venushum.
RightandLeftaboveumbilicusforrenalarterystenosis.
Overliverfor:Frictionrub[gratingduringbreathing];Bruit.
Overspleenforsplenicrub.
-
8/10/2019 CPG Medical Students
17/33
17
ObstetricExamination
Theobstetricexaminationcanbeconsideredaspecialisedadditiontotheexaminationoftheabdomen,
itsscopebeingtoassessthepregnancycharacteristics. Examinationoftheabdomen isaccomplished
withthe
patient
supine.
Late
in
pregnancy,
care
must
be
taken
to
have
the
patient
lie
slightly
to
one
side,lestthepregnantuterusimpedevenacava bloodflow,leadingtosyncope.
Inspection Assessthegeneralappearanceoftheabdomen
o
Distendedconsistentwithpregnancy;flatteningoreversionof
umbilicus;presence
of
striae
gravidarum;
presence
of
linea
nigra;
presenceofscars[notegynaecological/obstetricsurgeryscars,
laparoscopy,etc].
o
Observeregularityofuterineshape[maybepartiallyrotatedtoone
sideortheother];lookforpresenceoffoetalmovements.
Palpation
ensure
warmcleanhands;
ensurerelaxationof
abdominalmuscles.
Assess
fundal
height
starting
from
the
xiphisterum
and
working
ones
way
downwardsuntilfundusispalpated.Measuresymphysisfundalheightin
cmequivalenttogestationalageinweeks.
Bylateralpalpationusingbothhandoneithersideoftheabdomen,
assessthelieofthefoetus[longitudinal/transverse/oblique],thelocality
oftheback[right/left]andthepresentation [cephalic/breech].
Iflongitudinal,
assess
the
degree
of
the
descent
of
the
presenting
part
throughthepelvicbrimassessedinthenumberoffingersonecanplace
overfoetalheadsuprapubically[infifths2/5th
isconsideredengaged;
3/5th
unengaged].
Auscultation Listenoverthefoetalheartwherethescapulaislocated.Assessheart
rateto
maternal
pulse
-
8/10/2019 CPG Medical Students
18/33
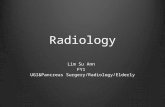
18
Assessingengagementofhead
-
8/10/2019 CPG Medical Students
19/33
19
GynaecologicalExamination
Thepelvicexaminationisanintegralcomponentofanygynaecologicalconsultationandfundamentalto
planninganygynaecologicalintervention.Inallsettings,thepatientsconsentmustalwaysbeobtained
beforeapelvic
examination
is
undertaken.
BLADDERMUSTBEEMPTIEDPRIORTOEXAMINATION
PERFORMED IN LITHOTOMY POSITION [on back, legs apart, knees bent], OR LEFT LATERAL
POSITION
INFORMTHE
PATIENT
OF
WHAT
YOU
PLAN
TO
DO
AND
INFORM
HER
OF
YOUR
OBSERVATIONS.
Inspection Examinetheexternalgenitalianotingandrashes,swellings,ulcerations,
lesions.
Separate
labia
with
forefinger
and
thumb
and
examine
clitoris.
Lookforanydischargeandnotecharacteristics[purulent/clear/blood
stained]
Tellpatienttobeardownandcoughlookforanyvaginalwallor
introitalbulges[prolapsedvaginalwallsoruterinedescent] orpassage
ofurine[stressincontinenceideallyherebladderwouldbefull]
-
8/10/2019 CPG Medical Students
20/33
20
Speculuminspection. InsertCuscos[bivalve]speculumlubricate,insertinupwards
directionwithbladesclosedusingonehandwhilelabiaareseparated
withother
hand;
open
blades
gently
to
visualise
cervix
and
vaginal
walls.Closebladesslowingduringwithdrawal.
o
Lookforanycervicallesions[ectopy,polyps,cysts,tears,etc],
vaginaldischarge[purulent/clear/bloodstained];cervical
inflammation;etc.
o
Perform
a
Cervical
smear
using
spatula
and/or
brush
rotaing
both
through360o andsmearingsampleslightlyonasmear.
o
Mayperformhighvaginalswab,cervicalswabs,wetslidesfor
infection.
-
8/10/2019 CPG Medical Students
21/33
21
Bimanualpalpation. PalpateBartholin'sglands[posterioroflabiamajor].
Lubricateindexandmiddlefingerifnecessary.Whiletheleftindex
fingerand
thumb
separate
labia,
the
right
index
and
middle
finger
areInsertintovagina.Thecervixislocated[assess:size,shape,
position,tenderness,mobility].
Thenperformabimanualexamination:keepingthevaginal
finderspushingupwardsandbackwards,pushthelefthanddown
back
onto
the
symphysis
pubis.
o
Palpatetheuterus[assesspositionantevertedorretroverted;
size;consistency;mobility;tenderness,cervicalexcitation.
oPalpatetheforniceswhileusingthelefthandtopushdownfrom
theiliacfossaetothesuprapubicregion[assessovariansize;
adnexialmasses,tenderness].
-
8/10/2019 CPG Medical Students
22/33
22
In the obstetric patient, a pelvic examination can help assess progress of labour by assess certain
specificcriteriarelatedtothestateofthecervix.AlltheseparametersareincludedinBishopScoreto
giveanoverallnumericalscoreofthestateofthecervix.
Score 0 1 2 3
Dilatation 0 12 34 >5
Effacement 80%
Consistency Firm Moderate Soft
Position
Posterior
Middle
AnteriorStation 3 3 1,0 +1,+2
BishopScoreCriteria
Effacement Descentofhead[station]inpelvis
-
8/10/2019 CPG Medical Students
23/33
23
EXAMPLEPRESENTATIONOFANANTENATALHISTORY&EXAMINATION
Seehttp://www.clinicalexam.com/pda/o_obs_antenatal_history_exam.htm
PresentationoftheHistory
Introduction
This is , a
baby.
The
reason
she
is
in
hospital
is
.
CurrentPregnancy
Focusingourattentiononthispregnancy,thefirstdayof. The current pregnancy was
and
taking
periconceptual
folic
acid.
She had a positive pregnancy test at weeks. She visited her doctor at .Duringthefirsttrimesterofpregnancy,she
. She booked into hospital at
-
8/10/2019 CPG Medical Students
24/33
24
-
8/10/2019 CPG Medical Students
25/33
-
8/10/2019 CPG Medical Students
26/33
26
alcohol||hasrestrictedherselfto...unitsofalcoholperweek>sincefindingoutshewaspregnant.She
takingironandfolicacidsupplements.
Summaryof
history
In summary, therefore, this is , a baby. Thereasonshe is inhospital is. isbeingkeptin
thehospital.
PresentationoftheExamination
General
looks . Her temperature is . Her pulse is
. Her blood pressure is .
Herrespiratoryrateis.Herurinesampleis
-
8/10/2019 CPG Medical Students
27/33
27
Onpalpation,Imeasuredthesymphysiofundalheightontheinchessidetoreduceobservererror,and
foundittobe,whichcompatiblewithgestation.ThefoetalpartsthatI
feelinthefundusappeartobetheastheyare.Thelieis
and
the
back
would
appear
to
be
on
the
as
it
offers more resistance to palpation and I feel small parts on the opposite side. The presentation
appearstobe.Theheadengaged.The foetusappears
clinicallyinsize.Theliquorvolumeappearsclinically.Thefoetalheartisbestheardovertheandoftheumbilicus,andis
.
SummaryofExamination
This is apregnancy, lie,presentation,thehead,thefoetusisclinically
insize,theliquorvolumeisclinically,andthefoetalheartis.
-
8/10/2019 CPG Medical Students
28/33
28
EXAMPLEANTENATALCASEWRITEUP
CaseSummary
Ms.Xis
a28
year
old
secondagravida
Rhesus
negative
woman
who
presented
to
the
emergency
departmentwithpainlessmoderatevaginalbleedingat34weeksofgestation.
HistoryofPresentPregnancy
Mrs.Xhadherlastmenstrualperiodonthe14th
January2008,computingherexpecteddateofdelivery
tothe
21
st
October
2008;
her
cycles
having
been
previously
normal
and
regular
every
28
30
days.
She
didnotgiveahistoryofanymenstrualproblems.
Mrs.Xhadnoproblemsduringthefirsttrimesterotherthanslightnauseaandoccasionalvomiting.This
sheacceptedasnormal,since itdidnotparticularlydistressher.Thepregnancywasplannedandshe
hadstartedfolicacidtwomonthsprevioustoconception.Shecontinuedtotakefolicacidthroughout
the first trimester. Shedidnot giveanyhistoryof vaginalbleedingduring the first threemonthsof
pregnancy.Sheattendedher familydoctorateightweeksofpregnancy,whenaclinicalexamination
wasreportedasnormal.
SheattendedtheantenatalclinicandbookedherconfinementatMaterDeiHospitalduringthesecond
trimesterat
14
weeks
of
gestation.
All
routine
investigations
taken
[complete
blood
count;
TORCH
SyphilisHepatitisCHIVscreen;bloodglucose]atthatvisitwerenormal.HerbloodgroupwasARhesus
negative;antibodytitreforantiDwasnegative.Ageneralclinicalexaminationwasnormal.Uterinesize
corresponded to dates; foetal heart was audible using a doptone stethoscope. She had her first
ultrasoundscanat18weeksofgestation.Shewastoldthatwhilethefoetuswasnormal,theplacenta
waslow
lying
and
that
she
will
need
afurther
scan
in
the
third
trimester
to
correctly
assess
the
-
8/10/2019 CPG Medical Students
29/33
29
significance of this. She had no problems during the second trimester and gave no history of any
episodesofvaginalbleeding.Shewasstartedonhaematinicsat14weeksofgestation.
Mrs.Xhad
no
problems
during
the
early
part
of
the
third
trimester
until
32
weeks
of
pregnancy.
All
routineantenatalvisitswerereportedlynormalwithadequatefoetalgrowthandbloodpressure.She
wasgivenaprophylacticantiDinjection[500IU]at28weeksofpregnancy.Ultrasoundscandoneat32
weeksofgestationconfirmedthepersistenceofalowplacentation;foetalgrowthandwellbeingwas
normal; foetalpresentationwastransverse. Inretrospectshementionedthatatabout31weeks,she
hadanepisodeofmildvaginalspottingthemorningafterhavinghadsexualintercourse.Thebleeding
was slight lasting only onemorning and she did not particularly alarm herself. She was advised to
refrainfromhavingsexualintercourse.
Historyofpresentingcomplaint
Shepresentedat34weeksofgestationwithpainlessvaginalbleedingof suddenonset.Thepresent
episodeof
bleeding
was
sudden
in
onset
and
severe
enough
for
the
blood
to
trickle
down
her
thighs.
Therewerenoassociatedfeaturessuchaspainoranydiscomfort.
Onadmission, thebleedinghad settled toonlya slight vaginal loss. The foetuswaseasilypalpable;
presentationwascephalicobliquewiththebacktotheleft.Foetalheartwasaudibleandofnormalrate.
Symphysealfundal
height
was
about
34
cm
corresponding
to
the
gestational
age.
There
was
no
tendernessovertheuterus.Therewerenosignsofmaternalcardiovascularshock;thepatientspulse
was 80 beats perminute, blood pressure 110/70mmHg.An ultrasound scan confirmed the clinical
findings;theplacentawaspraevia,apparentlymarginalandposterior(Type2placentapraevia).Foetal
growthcorrespondedtogestation.
-
8/10/2019 CPG Medical Students
30/33
30
Anintravenousinfusionwassetup,whilebloodwastakenforhaemoglobinestimationandcrossmatch.
An antiD injection was administered. Regular monitoring of vaginal blood loss, pulse and blood
pressurewerecarriedout;while foetalheartratemonitoringwasalsocarriedout intermittently.The
motheralso
received
two
doses
of
dexamethasone
[12
mg
every
12
hours]
to
assist
foetal
lung
maturity.
Thepatientwas reviewedafter24hours.Thevaginalbleedinghad stopped completely, therebeing
only a slight browning staining on the vaginal pad. All parameters had remained normal. The
intravenousinfusionwasstopped.ShewastransferredtotheAntenatalWardandtoldthatsheneeded
to remain inhospital throughout the remainingantenatalperiod.Shehada repeatepisodeof slight
bleeding at 35 weeks of gestation, which was managed conservatively. Foetal monitoring with
cardiotocographyandultrasoundshowednoabnormality.AnantiDimmunoglobulindose[500IU]was
repeated.
PastObstetricHistory
Thepatient
had
had
aprevious
pregnancy
four
years
earlier.
The
antenatal
period
had
run
anormal
course.Onsetof labourwas induced since thepatientspregnancyhad run tooveraweekpasther
estimateddates.Labourhadprogressedeffectively,but foetaldistresswasdiagnosedatabout5cm
cervical dilatation. An Emergency Caesarean section was thus performed. A live born male infant,
weighing3400gmwasdelivered.Shegavenohistoryofmiscarriages.
PastMedical&SurgicalHistory
Thepatientgavenohistoryofanysignificantmedicalevents.Shehadhadanappendectomyperformed
attheageof15years.
-
8/10/2019 CPG Medical Students
31/33
31
PastGynaecologicalHistory
Thepatienthadnorelevantgynaecologicalevents.Hermenarcheoccurredaroundtheageof10years;
hercyclesstabilisingwithinaboutayear.Shehadhadregularsmeartestsaftershebecamesexually
active;these
having
been
always
normal.
Her
last
smear
test
was
performed
about
six
months
before
embarking on this current pregnancy. During the interpregnancy period she used the oral
contraceptivepill[Yasmine]forcontraception.
DrugHistory
Thepatientwasonnolongtermmedication,exceptforthehaematinicsreceivedduringherpregnancy.
Shedidnot reportanydrugallergies.Shedidnotsmokecigarettesanddidnotabusealcoholatany
timeduringherpregnancy.
SocialHistory
Thepatientwasinastablerelationship.Shemarriedattheageof20years;andlivedwithherhusband
andchild.
She
worked
as
aclerk
in
an
industrial
manufacturing
setting.
She
intended
to
apply
for
parentalleavetocareforherchildren.
Examinationat36weeksofpregnancy
Thepatientwasexaminedat36weeksofpregnancy.Atthispointintime,shewasaninpatientinthe
hospital.There
were
no
acute
symptoms.
On examination the patientwas in good general health. She did not appear anaemic and was not
distressed inanyway.Cardiovascularsystemwasnormal;herbloodpressureandpulsebeing110/60
mmHg and 70 beats/min respectively. There was no lower limb oedema. Abdominal examination
conformedtoa36weeksofpregnancy.Onvisualexaminationtherewasadistendedabdomenwitha
f i li i d i id O l i h h i f d l h i h d 37
-
8/10/2019 CPG Medical Students
32/33
32
faint lineanigraandsomestriaegravidarum.Onpalpation,thesymphysisfundalheightmeasured37
cm;thefoetallieappearedtobeobliquewithacephalicpresentationandthebacktotheleftside.The
foetalheartwasaudibleontheleftlowerquadrant.
Followupofthispregnancy
At37weeksofpregnancy,thepatientsufferedasuddenonsetofseverevaginalbleedingwhilehaving
a shower. She was transferred to the Central Delivery Suite. Assessment at this stage, showed a
persistingunstablelieofthefoetus.Inviewoftheseverityofbleedingandthematurityoftheinfant,a
decisionwasmadetoundertakedeliverybyurgentCaesareansection.Thiswascarriedoutunderspinal
anaesthesia.Atsurgery,theplacentawasconfirmedtobeaposteriorType2placentapraevia.Afemaleinfant,weighing 3540 gm,was bornwith anApgar score of 8 at 1minute. The infant required no
resuscitation.TheCaesareansectionproceededwithoutanycomplications.
Thepatientwas treatedwithasyntocinon infusion (40units in500mls infusion)during the first24
hourspost
operatively.
She
also
received
intra
operative
prophylactic
antibiotics
three
eight
hourly
dosesofintravenousAugmentin(amoxycillin250mgandclavulanicacid125mg)oninductionhasbeen
comparedwiththree8hourlydosesin900patients.ThefoetusbloodgroupwasreportedasGroupO
Rhesus negative; Coombs test was negative. No antiD prophylaxis was thus administered to the
mother.Shewasdischargedwithherchildfourdaysaftersurgerywithapostoperativehaemoglobin
levelof
10.5
g/dl;
she
was
advised
to
continue
her
haematinics
for
afurther
six
weeks.
CaseDiscussion
Thiscase involvedapregnancy ina secondagravidawomancomplicatedbyType2Placentapraevia.
ThesituationwasfurthercomplicatedbyaRhesusnegativebloodgroup.
Th ti t t d t h ibl b l l t ti t h fi t lt d t 18
-
8/10/2019 CPG Medical Students
33/33
33
The patientwas noted to have a possible abnormal placentation at her first ultrasound scan at 18
weeksofgestationwhentheplacentawasnotedtobelowlying.Whilethisobservationissuggestiveof
an eventualplacentapraevia at term,not all casesof lowlyingplacentaediscovered in the second
trimesterremain
so
in
the
third
trimester
when
the
lower
segment
actually
develops.
The
patient,
by
virtueofherpreviouscaesareansection,wasathighriskofabnormalplacentation.
The clinical course was typical of the condition with warning bleeding occurring at 32 weeks of
gestation[aftersexual intercourse],followedbymoreseverebleedingat34weeksandsubsequently.
Theinitialmanagementfollowedinthiscaseincludedanexpectantregimenawaitingfoetalmaturity.In
anticipationof thepossibleneed foraprematurebirth, foetal lungmaturitywasaugmentedby theadministration of dexamethasone. Blood was crossmatched and kept in reserve to enable timely
transfusionshouldtheneedarise.At37weeksofgestation,thebleedingincreasedsignificantly,andin
viewofthedegreeoffoetalmaturity,adecisiontoterminatethepregnancywastaken.Becauseofthe
persistingunstablelie,aCaesareansectionwasdecidedupon.
ThecasewasfurthercomplicatedbyamaternalRhesusnegativebloodgroup.Toobviatethepossibility
of subsequent immunization, aprophylacticdoseof antiD immunoglobulinwas administered at 28
weeks is linewith currentguidelines. Inanticipationofpossible fetomaternal transfusion, a further
dosewasgivenwheneverthepatientexperiencedepisodesofbleeding.Theseprophylacticmeasures
provedneedless
since
the
foetus
was
eventually
found
to
have
been
Rhesus
negative.