COVID-19 Mortality from Secondary Acquired Infections · 2020. 10. 19. · Infections Ho w life has...
9
COVID-19 Mortality from Secondary Acquired Infections Ho w life has changed: COVID-19 and AMR Presidential Advisory Council on Combating Antibiotic-Resistant Bacteria 9 September 2020 Cornelius J. Clancy, M.D. Chief, Infectious Diseases VA Pittsburgh Healthcare System Associate Chief, Infectious Diseases Director, XDR Pathogen Lab and Mycology Research Unit University of Pittsburgh
Transcript of COVID-19 Mortality from Secondary Acquired Infections · 2020. 10. 19. · Infections Ho w life has...

COVID-19 Mortality from Secondary Acquired Infections
How life has changed: COVID-19 and AMRPresidential Advisory Council on Combating Antibiotic-Resistant Bacteria9 September 2020
Cornelius J. Clancy, M.D.Chief, Infectious Diseases VA Pittsburgh Healthcare SystemAssociate Chief, Infectious DiseasesDirector, XDR Pathogen Lab andMycology Research UnitUniversity of Pittsburgh

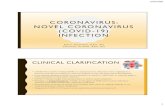
Why do COVID-19 patients die?
Postmortem histopathology images from Sekulic et al. Am J Clin Path 2020; Hanley et al. Lancet Microbe 2020.
Diffuse alveolar damage causing acute respiratory distress syndrome (ARDS)
Thromboembolic disease
Multisystem organ failure Immune depletion and dysregulation

Do patients die of secondary infections?
of COVI-19 autopsies have histopathologic findings in lungs that are consistent with superimposed bronchopneumonia or pulmonary infection137%
● Findings due to superimposed infection or COVID-19?● Very limited microbiology and AMR data● More often focal process rather than diffuse disease● Often not recognized or treated with antimicrobials ante-mortem
Images from Sekulic et al. Am J Clin Path 2020; Hanley et al. Lancet Microbe 2020. 1. Histopathologic findings: Intra-alveolar PMN infiltrates or abscess/empyema, in absence of classic viral pneumonia histopathology. N=106/289, from review of data from 51 peer-reviewed publications through 28 August 2020, includes hospital- and community-based deaths
Sizeable minority of COVID-19 decedents die with, but not necessarily from, superimposed bacterial
or (less often) fungal infections

Types of COVID-19 secondary infections
Microbiology and AMR will reflect local epidemiology
and host risk factors
Lung: P. aeruginosa, K. pneumoniae, C. koseri, S. maltophiliaUrine: E. Coli, Proteus, K. pneumoniae
● MDR, ESBL, CRE infections diagnosedBlood: S. aureus, coag negative Staph, Strep spp., Candida
Bloodstream infections● Endocarditis, septic emboli, abscesses
Urinary tract infectionsSkin and soft tissue infectionsClostridiodes difficile infections
Co-infections● Community acquired pneumonia, urinary tract infection, skin/soft tissue
infection, C difficile infection, febrile neutropeniaSecondary infections
● Hospital/ventilator pneumonia, bloodstream infection, urinary tract infection, C. difficile infection
VAPHS experience, through 7/31/20
No co- or secondary infxn, 72%
Present w co-infxn, 9%
Develop secondary infxn, 19%
Buehrle et al. Antimicrob Agents Chemother 2020

COVID-19: Antimicrobial stewardship strategies
Gp 1. No antimicrobials
41%
Gp 2. Empiric treatment, no infxn diagnosed
31%
Gp 3. Treat for co-infxn
9%
Gp 4. Treat for secondary infxn, 19%
Stewardship group Stewardship objectives1. No treatment Limit unnecessary use, include rapid
diagnostics (negative predictive values)2. Empiric treatment
Target most likely pathogens, rapid de-escalation, limit duration, aggressive diagnostic testing (NPVs)
3. Treat co-infection Promote narrow spectrum, short course, oral
4. Treat secondary infection
Target nosocomial pathogens, promote narrow spectrum, short course
Buehrle et al. Antimicrob Agents Chemother 2020

1400
1600
1800
2000
2200
2400
Antib
iotic
Day
s of
The
rapy
(DO
T)
1/18 3/18 5/18 7/18 9/1811/181/19 3/19 5/19 7/19 9/1911/191/20 3/20 5/20
Actual Predicted
2000
2500
3000
3500
4000
Bed
days
of c
are
1/18 3/18 5/18 7/18 9/1811/181/19 3/19 5/19 7/19 9/1911/191/20 3/20 5/20
Actual Predicted
Impact of COVID-19 on hospital antibiotic use
580
600
620
640
660
Day
s of
The
rapy
per
100
0 Be
d D
ays
of C
are
1/18 3/18 5/18 7/18 9/1811/181/19 3/19 5/19 7/19 9/1911/191/20 3/20 5/20
Actual Predicted
7080
9010
011
0D
OT/
1000
BD
OC
3/18
6/18
9/18
12/18 3/1
96/1
99/1
912
/19 3/20
6/20
Actual Predicted
3040
5060
70D
OT/
1000
BD
OC
3/18
6/18
9/18
1218 3/1
96/1
99/1
912
/16 3/20
6/20
Actual Predicted
VAPHS Days of therapy (DOT) VAPHS bed days of care (BDOC) VAPHS DOT/1,000 BDOC
Non-antipseudomonal PNCsDOT/1,000 BDOC
MacrolidesDOT/1,000 BDOC
Significantly increased DOT/1000 BDOC of agents vs. CAP ● Patients with CAP/suspected CAP disproportionately presenting to hospital?● Over-treatment of suspected CAP?
Buehrle et al. Antimicrob Agents Chemother 2020

0
200
400
600
800
1000
1200
1400
1600VAPHS outpatient prescriptions, Nov 2017-July 2020
510
1520
Pres
crip
tions
per
100
0 pe
rson
s
Aug 2014 Aug 2015 Aug 2016 Aug 2017 Aug 2018 Aug 2019
Amoxicillin
510
1520
Pres
crip
tions
per
100
0 pe
rson
s
Aug 2014 Aug 2015 Aug 2016 Aug 2017 Aug 2018 Aug 2019
Azithromycin
02
46
810
Pres
crip
tions
per
100
0 pe
rson
s
Aug 2014 Aug 2015 Aug 2016 Aug 2017 Aug 2018 Aug 2019
Amoxicillin/Clavulanate
Outpatient antibiotic useUS prescription fills, 2014-July 2020 (IQVIA NPA data)
Significant reductions in prescription fills in April 2020 for the ten most commonly prescribed outpatient antibiotics
● No significant rebound, April-July 2020: Azithromycin, amoxicillin-clavulanate, levofloxacin ● Rebound April-July 2020, but still below baseline: Amoxicillin, doxycycline
Prescription fills for outpatient antibiotics recommended against CAP or commonly used against respiratory tract infections remain significantly below baseline
● Patients not seeking care? Clinicians less likely to prescribe (unnecessary) agents?

Will COVID-19 result in increased AMR? Pro• Antibiotic prescribing in excess of secondary
infections, suggesting inappropriate use• Many COVID-19 epicentres also AMR epicentres• Burden of antibiotic use in hospitalized patients
increased, even outside of epicentres• Reports of HAI outbreaks associated with
breakdowns in infection prevention• Effects of COVID-19 on public health infrastructure,
sanitation, healthcare delivery, governance may indirectly impact AMR and transmission
• Secondary infections may increase as COVID-19 treatment evolves (e.g., dexamethasone)
• Co-circulation of SARS-CoV-2 and influenza may fuel inappropriate antibiotic prescribing
• Overall antibiotic use in humans has decreased in many places
• Major determinant of AMR rates is spread, which may be decreased with COVID-19 travel restrictions, enhanced attention to infection prevention, etc.
• Better COVID-19 outcomes may decrease pools of high risk critically ill patients, including those on ventilators, receiving hemodialysis, etc.
• Increased emphasis on diagnosing respiratory viral infections may decrease inappropriate antibiotic treatment
• Data from southern hemisphere suggest that impact of influenza may be lessened by COVID-19 precautions
Clancy, Buehrle and Nguyen. J Antimicrob Chemother-AMR 2020; Collignon and Beggs. J Antimicrob Chemother-AMR 2020
COVID-19 and AMR story will be dynamic, and likely to differ from region to region, hospital to hospital, and unit to unit within hospitals
● AMR was a major problem before COVID-19, and it will remain a problem
Con

COVID-19 and AMR: Needs moving forward
• Report our experiences and data• More rigorous microbiology and
definitions of superimposed infections in clinical and postmortem studies
• Surveillance data on antimicrobial use and AMR
• Education• It’s OK not to get/give an antibiotic• AMR has not gone away